
Effects of Ibuprofen Use on Lymphocyte Count and Oxidative Stress in Elite Paralympic Powerlifting

 ,
, 
 , , , ,
, , , ,  , ,
, ,  ,
,  , , and
, , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
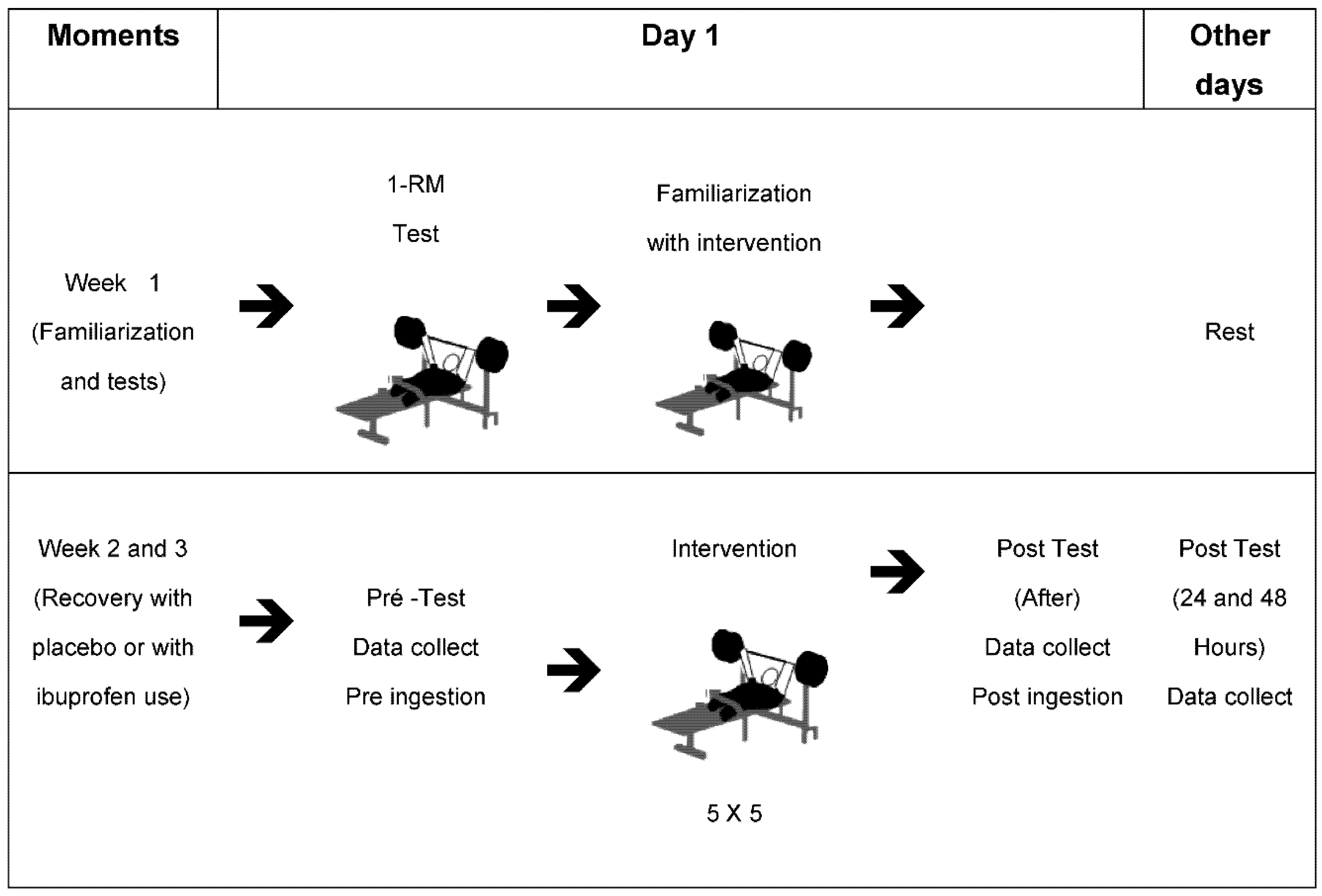
2.1. Study Design
2.2. Sample
2.3. Ethics
2.4. Body Mass Analysis
2.5. Maximum Training Load Analysis
2.6. Upper Limbs Muscle Strength
2.7. Blood Sample Collection
2.8. Blood Cell and Leukocyte Count (HEMOGRAM)
2.9. Oxidative Stress
2.10. Post-Workout Recovery Using a Placebo
2.11. Post-Workout Recovery Using Ibuprofen
2.12. Statistical Analysis
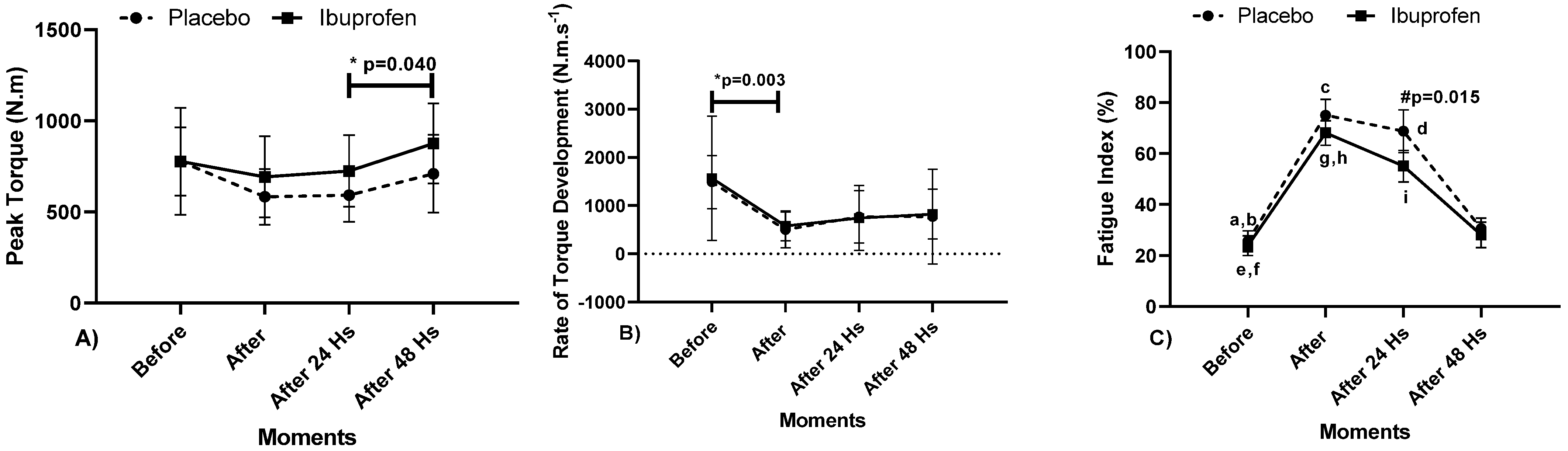
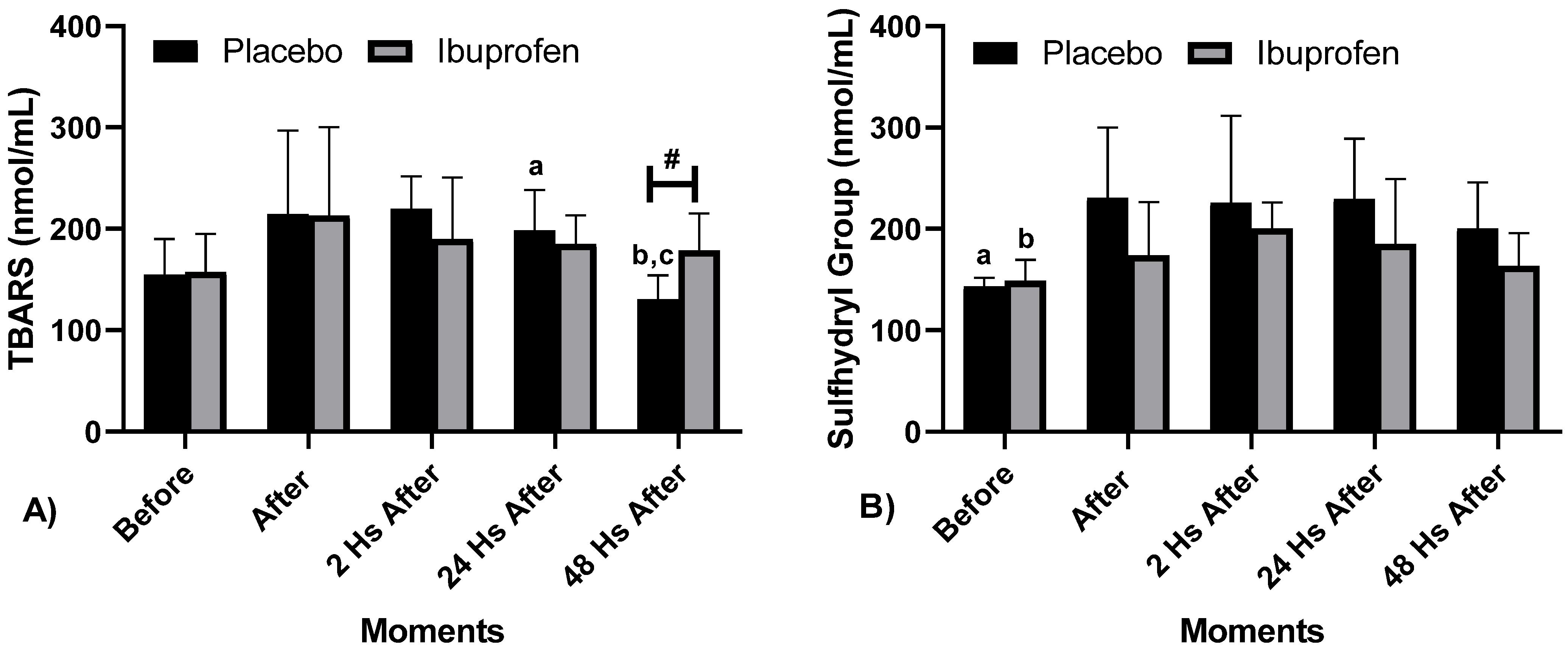
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fraga, G.S.; Aidar, F.J.; Matos, D.G.; Marçal, A.C.; Santos, J.L.; Souza, R.F.; Carneiro, A.L.; Vasconcelos, A.B.; Da Silva-Grigoletto, M.E.; Tillaar, R.V.D.; et al. Effects of Ibuprofen Intake in Muscle Damage, Body Temperature and Muscle Power in Paralympic Powerlifting Athletes. Int. J. Environ. Res. Public Health 2020, 17, 5157. [Google Scholar] [CrossRef]
- Hecksteden, A.; Skorski, S.; Schwindling, S.; Hammes, D.; Pfeiffer, M.; Kellmann, M.; Ferrauti, A.; Meyer, T. Blood-Borne Markers of Fatigue in Competitive Athletes—Results from Simulated Training Camps. PLoS ONE 2016, 11, e148810. [Google Scholar] [CrossRef] [PubMed]
- Sampaio, C.R.S.F.; Aidar, F.J.; Ferreira, A.R.P.; Santos, J.L.D.; Marçal, A.C.; Matos, D.G.; Souza, R.F.; Moreira, O.C.; Guerra, I.; Fernandes Filho, J.; et al. Can Creatine Supplementation Interfere with Muscle Strength and Fatigue in Brazilian National Level Paralympic Powerlifting? Nutrientes 2020, 12, 2492. [Google Scholar] [CrossRef] [PubMed]
- Bessa, A.L.; Oliveira, V.N.; Agostini, G.G.; Oliveira, R.J.; Oliveira, A.C.; White, G.E.; Wells, G.D.; Teixeira, D.N.; Espindola, F.S. Exercise Intensity and Recovery. J. Strength Cond. Res. 2016, 30, 311–319. [Google Scholar] [CrossRef]
- Nunes-Silva, A.; Bernardes, P.T.T.; Rezende, B.M.; Lopes, F.; Gomes, E.C.; Marques, P.E.; Lima, P.M.A.; Coimbra, C.C.; Menezes, G.B.; Teixeira, M.M.; et al. Treadmill Exercise Induces Neutrophil Recruitment into Muscle Tissue in a Reactive Oxygen Species-Dependent Manner. An Intravital Microscopy Study. PLoS ONE 2014, 9, e96464. [Google Scholar] [CrossRef]
- Gonçalves, C.A.M.; Dantas, P.M.S.; Dos Santos, I.K.; Dantas, M.P.; Da Silva, D.C.P.; Cabral, B.G.D.A.T.; Guerra, R.O.; Júnior, G.B.C. Effect of Acute and Chronic Aerobic Exercise on Immunological Markers: A Systematic Review. Front. Physiol. 2020, 10, 1602. [Google Scholar] [CrossRef]
- Macedo, N.C.D.; Iessi, I.L.; Gallego, F.Q.; Netto, A.O.; Sinzato, Y.K.; Volpato, G.T.; Zambrano, E.; Damasceno, D.C. Swimming Program on Mildly Diabetic Rats in Pregnancy. Reprod. Sci. 2021, 28, 2223–2235. [Google Scholar] [CrossRef]
- Yang, D.K.; Lee, S.-J.; Adam, G.O.; Kim, S.-J. Aralia continentalis kitagawa Extract Attenuates the Fatigue Induced by Exhaustive Exercise through Inhibition of Oxidative Stress. Antioxidants 2020, 9, 379. [Google Scholar] [CrossRef]
- Speer, H.; D’Cunha, N.M.; Alexopoulos, N.I.; McKune, A.J.; Naumovski, N. Anthocyanins and Human Health—A Focus on Oxidative Stress, Inflammation and Disease. Antioxidants 2020, 9, 366. [Google Scholar] [CrossRef] [PubMed]
- Varamenti, E.; Nikolovski, Z.; Elgingo, M.I.; Jamurtas, A.Z.; Cardinale, M. Training-induced variations in haematological and bio-chemical variables in adolescent athletes of arab origin throughout an entire athletic season. J. Hum. Kinet. 2018, 64, 123–135. [Google Scholar] [CrossRef] [Green Version]
- Ammar, A.; Turki, M.; Hammouda, O.; Chtourou, H.; Trabelsi, K.; Bouaziz, M.; Abdelkarim, O.; Hoekelmann, A.; Ayadi, F.; Souissi, N.; et al. Effects of Pomegranate Juice Supplementation on Oxidative Stress Biomarkers Following Weightlifting Exercise. Nutritients 2017, 9, 819. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ammar, A.; Chtourou, H.; Souissi, N. Effect of Time-of-Day on Biochemical Markers in Response to Physical Exercise. J. Strength Cond. Res. 2017, 31, 272–282. [Google Scholar] [CrossRef] [PubMed]
- Ammar, A.; Chtourou, H.; Hammouda, O.; Turki, M.; Ayedi, F.; Kallel, C.; Abdelkarim, O.; Hoekelmann, A.; Souissi, N. Relationship between biomarkers of muscle damage and redox status in response to a weightlifting training session: Effect of time-of-day. Acta Physiol. Hung. 2016, 103, 243–261. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Finaud, J.; Lac, G.; Filaire, E. Oxidative stress: Relationship with exercise and training. Sports Med. 2006, 36, 327–358. [Google Scholar] [CrossRef] [PubMed]
- Ammar, A.; Chtourou, H.; Hammouda, O.; Trabelsi, K.; Chiboub, J.; Turki, M.; Abdelkarim, O.; El Abed, K.; ben Ali, M.; Hoekelmann, A.; et al. Acute and delayed responses of C-reactive protein, malondialdehyde and antioxidant markers after resistance training session in elite weightlifters: Effect of time of day. Chronobiol. Int. 2015, 32, 1211–1222. [Google Scholar] [CrossRef]
- De Souza, R.F.; de Matos, D.G.; Ferreira, A.R.P.; Chilibeck, P.; Barros, N.D.A.; Oliveira, A.S.; Cercato, L.M.; da Silva, D.S.; Aidar, F.J. Effect of Ibuprofen on Muscle, Hematological and Renal Function, Hydric Balance, Pain, and Performance During Intense Long-Distance Running. J. Strength Cond. Res. 2020, 34, 2076–2083. [Google Scholar] [CrossRef]
- Mishra, D.K.; Fridén, J.; Schmitz, M.C.; Lieber, R.L. Anti-inflammatory medication after muscle injury. A treatment resulting in short-term improvement but subsequent loss of muscle function. J. Bone Jt. Surg. Am. 1995, 77, 1510–1519. [Google Scholar] [CrossRef]
- Bondesen, B.A.; Mills, S.T.; Kegley, K.M.; Pavlath, G.K. The COX-2 pathway is essential during early stages of skeletal muscle re-generation. Am. J. Physiol. Cell Physiol. 2004, 56, C475–C483. [Google Scholar] [CrossRef]
- Bondesen, B.A.; Mills, S.T.; Pavlath, G.K. The COX-2 pathway regulates growth of atrophied muscle via multiple mechanisms. Am. J. Physiol. Cell Physiol. 2006, 290, C1651–C1659. [Google Scholar] [CrossRef] [Green Version]
- International Paralympic Committee (IPC). World Para Powerlifiting. Rules & Regulations. Available online: https://www.paralympic.org/sites/default/files/document/180215210800620_World%2BPara%2BPowerlifting%2BRules%2Band%2BRegulations_Feb%2B2018_0.pdf (accessed on 13 October 2020).
- Resende, M.; Resende, R.V.; Reis, G.; Barros, L.; Bezerra, M.; Matos, D.; Marçal, A.; Almeida-Neto, P.; Cabral, B.; Neiva, H.; et al. The Influence of Warm-Up on Body Temperature and Strength Performance in Brazilian National-Level Paralympic Powerlifting Athletes. Medicina 2020, 56, 538. [Google Scholar] [CrossRef]
- Ball, R.; Weidman, D. Analysis of USA Powerlifting Federation Data From 1 January 2012–11 June 2016. J. Strength Cond. Res. 2018, 32, 1843–1851. [Google Scholar] [CrossRef]
- Souza, R.F.; Nogueira, A.C.; Ferreira, A.R.P.; Matos, D.G.; Oliveira, L.S.L.; Zanona, A.F.; Aidar, F.J. Analysis of muscle recovery time after acute stretching at peak torque of the hamstring muscles. Med. Dello Sport 2019, 72, 171–180. [Google Scholar]
- Lapenna, D.; Ciofani, G.; Pierdomenico, S.D.; Giamberardino, M.A.; Cuccurullo, F. Reaction conditions affecting the relationship between thiobarbituric acid reactivity and lipid peroxides in human plasma. Free Radic. Biol. Med. 2001, 31, 331–335. [Google Scholar] [CrossRef]
- Faure, P.; Lafond, J.L. Measurement of plasma sulfhydryl and carbonyl groups as a possible indicator of protein oxidation. In Analysis of Free Radicals in Biological Systems; Favier, A.E., Cadet, J., Kalyanaraman, B., Fontecave, M., Pierre, J.L., Eds.; Birkhäuser Verlag: Basel, Switzerland, 1995; pp. 237–248. [Google Scholar]
- Lakens, D. Calculating and reporting effect sizes to facilitate cumulative science: A practical primer for t-tests and ANOVAs. Front. Psychol. 2013, 4, 863. [Google Scholar] [CrossRef] [Green Version]
- Lakens, D. Equivalence tests: A practical primer for t tests, correlations, and meta-analyses. Soc. Psychol. Personal. Sci. 2017, 8, 355–362. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cohen, J. Statistics a power primer. Psychol. Bull. 1992, 112, 155–159. [Google Scholar] [CrossRef] [PubMed]
- Elshafei, M.; Shihab, E. Towards Detecting Biceps Muscle Fatigue in Gym Activity Using Wearables. Sensors 2021, 21, 759. [Google Scholar] [CrossRef]
- Mushtaq, W.; Hamdani, N.; Noohu, M.M.; Raghavan, S. Effect of Modified Constrain Induced Movement Therapy on Fatigue and Motor Performance in Sub Acute Stroke. J. Stroke Cerebrovasc. Dis. 2020, 29, 105378. [Google Scholar] [CrossRef] [PubMed]
- Kerhervé, H.A.; Stewart, D.G.; McLellan, C.; Lovell, D. Fatigue Indices and Perceived Exertion Highlight Ergometer Specificity for Repeated Sprint Ability Testing. Front. Sports Act. Living 2020, 2, 45. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.-Y.; Chou, W.-Y.; Ko, J.-Y.; Lee, M.S.; Wu, R.-W. Early Recovery of Exercise-Related Muscular Injury by HBOT. BioMed Res. Int. 2019, 2019, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stolk, R.F.; Van Der Pasch, E.; Naumann, F.; Schouwstra, J.; Bressers, S.; Van Herwaarden, A.E.; Gerretsen, J.; Schambergen, R.; Ruth, M.M.; Van Der Hoeven, J.G.; et al. Norepinephrine Dysregulates the Immune Response and Compromises Host Defense during Sepsis. Am. J. Respir. Crit. Care Med. 2020, 202, 830–842. [Google Scholar] [CrossRef]
- Basile, U.; Bruno, C.; Napodano, C.; Vergani, E.; Pocino, K.; Brunetti, A.; Gulli, F.; Santini, S.A.; Mancini, A. Plasmatic free light chains as inflammatory marker in insulin resistance: Comparison of metabolic syndrome with adult growth hormone deficiency. BioFactors 2018, 44, 480–484. [Google Scholar] [CrossRef] [PubMed]
- Moro, T.; Tinsley, G.; Longo, G.; Grigoletto, D.; Bianco, A.; Ferraris, C.; Guglielmetti, M.; Veneto, A.; Tagliabue, A.; Marcolin, G.; et al. Time-restricted eating effects on performance, immune function, and body composition in elite cyclists: A randomized controlled trial. J. Int. Soc. Sports Nutr. 2020, 17, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Barbouti, A.; Vasileiou, P.V.S.; Evangelou, K.; Vlasis, K.G.; Papoudou-Bai, A.; Gorgoulis, V.G.; Kanavaros, P. Implications of Oxidative Stress and Cellular Senescence in Age-Related Thymus Involution. Oxid. Med. Cell. Longev. 2020, 2020, 7986071. [Google Scholar] [CrossRef] [PubMed]
- Sun, W.; Wang, Z.; Sun, M.; Huang, W.; Wang, Y.; Wang, Y. Aloin antagonizes stimulated ischemia/reperfusion-induced damage and inflammatory response in cardiomyocytes by activating the Nrf2/HO-1 defense pathway. Cell Tissue Res. 2021, 384, 735–744. [Google Scholar] [CrossRef] [PubMed]
- Barili, A.; Corralo, V.D.S.; Cardoso, A.M.; Mânica, A.; Bonadiman, B.D.S.R.; Bagatini, M.D.; Da Silva-Grigoletto, M.E.; De Oliveira, G.G.; De Sá, C.A. Acute responses of hemodynamic and oxidative stress parameters to aerobic exercise with blood flow restriction in hypertensive elderly women. Mol. Biol. Rep. 2018, 45, 1099–1109. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.-S.; Lee, T.; Chow, S.-E. Role of exercise intensities in oxidized low-density lipoprotein-mediated redox status of monocyte in men. J. Appl. Physiol. 2006, 101, 740–744. [Google Scholar] [CrossRef] [PubMed]
- Miyazaki, H.; Oh-Ishi, S.; Ookawara, T.; Kizaki, T.; Toshinai, K.; Ha, S.; Haga, S.; Ji, L.L.; Ohno, H. Strenuous endurance training in humans reduces oxidative stress following exhausting exercise. Eur. J. Appl. Physiol. 2001, 84, 1–6. [Google Scholar] [CrossRef]
- Yokota, T.; Kinugawa, S.; Hirabayashi, K.; Yamato, M.; Takada, S.; Suga, T.; Nakano, I.; Fukushima, A.; Matsushima, S.; Okita, K.; et al. Systemic oxidative stress is associated with lower aerobic capacity and impaired skeletal muscle energy metabolism in heart failure patients. Sci. Rep. 2021, 11, 1–8. [Google Scholar] [CrossRef]
- Souza, A.V.; Giolo, J.S.; Teixeira, R.R.; Vilela, D.D.; Peixoto, L.G.; Justino, A.B.; Caixeta, D.C.; Puga, G.M.; Espindola, F.S. Salivary and plas-matic antioxidant profile following continuous, resistance, and high-intensity interval exercise: Preliminary study. Oxid. Med. Cell. Longev. 2019, 2019, 5425021. [Google Scholar] [CrossRef]
- Bouzid, M.A.; Hammouda, O.; Matran, R.; Robin, S.; Fabre, C. Influence of physical fitness on antioxidant activity and malondialdehyde level in healthy older adults. Appl. Physiol. Nutr. Metab. 2015, 40, 582–589. [Google Scholar] [CrossRef]
- Gram, M.; Vigelsø, A.; Yokota, T.; Helge, J.W.; Dela, F.; Hey-Mogensen, M. Skeletal muscle mitochondrial H2O2 emission increases with immobilization and decreases after aerobic training in young and older men. J. Physiol. 2015, 593, 4011–4027. [Google Scholar] [CrossRef] [Green Version]
- Koubaa, A.; Triki, M.; Trabelsi, H.; Baati, H.; Sahnoun, Z.; Hakim, A. The Effect of a 12-Week Moderate Intensity Interval Training Program on the Antioxidant Defense Capability and Lipid Profile in Men Smoking Cigarettes or Hookah: A Cohort Study. Sci. World J. 2015, 2015, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Nobari, H.; Nejad, H.; Kargarfard, M.; Mohseni, S.; Suzuki, K.; Adsuar, J.C.; Pérez-Gómez, J. The Effect of Acute Intense Exercise on Activity of Antioxidant Enzymes in Smokers and Non-Smokers. Biomolecules 2021, 11, 171. [Google Scholar] [CrossRef]
- Pingitore, A.; Lima, G.P.P.; Mastorci, F.; Quinones, A.; Iervasi, G.; Vassalle, C. Exercise and oxidative stress: Potential effects of anti-oxidant dietary strategies in sports. Nutrition 2015, 31, 916–922. [Google Scholar] [CrossRef]
- Bogdanis, G.; Stavrinou, P.; Fatouros, I.; Philippou, A.; Chatzinikolaou, A.; Draganidis, D.; Ermidis, G.; Maridaki, M. Short-term high-intensity interval exercise training attenuates oxidative stress responses and improves antioxidant status in healthy hu-mans. Food Chem. Toxicol. 2013, 61, 171–177. [Google Scholar] [CrossRef]
- De Souza, R.F.; Augusto, R.L.; De Moraes, S.R.A.; De Souza, F.B.; Gonçalves, L.V.D.P.; Pereira, D.D.; Moreno, G.M.M.; De Souza, F.M.A.; Andrade-Da-Costa, B.L.D.S. Ultra-Endurance Associated with Moderate Exercise in Rats Induces Cerebellar Oxidative Stress and Impairs Reactive GFAP Isoform Profile. Front. Mol. Neurosci. 2020, 13, 157. [Google Scholar] [CrossRef]
- De Araújo, S.S.; Aidar, F.J.; De Matos, D.G.; Santos, J.L.; Souza, L.M.V.; Silva, A.N.; Marçal, A.C.; Mourão, D.M.; Júnior, A.L.; Durães, G.M.; et al. Does Croton Argyrophyllus Extract Has an Effect on Muscle Damage and Lipid Peroxidation in Rats Submitted to High Intensity Strength Exercise? Int. J. Environ. Res. Public Health 2019, 16, 4237. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Korivi, M.; Chen, C.-T.; Yu, S.-H.; Ye, W.; Cheng, I.-S.; Chang, J.-S.; Kuo, C.-H.; Hou, C.-W. Seaweed Supplementation Enhances Maximal Muscular Strength and Attenuates Resistance Exercise-Induced Oxidative Stress in Rats. Evid. Based Complement. Altern. Med. 2019, 2019, 3528932-9. [Google Scholar] [CrossRef] [PubMed]
- Mastaloudis, A.; Yu, T.-W.; O’Donnell, R.P.; Frei, B.; Dashwood, R.H.; Traber, M.G. Endurance exercise results in DNA damage as detected by the comet assay. Free Radic. Biol. Med. 2004, 36, 966–975. [Google Scholar] [CrossRef] [PubMed]
- Azizbeigi, K.; Azarbayjani, M.A.; Atashak, S.; Stannard, S.R. Effect of Moderate and High Resistance Training Intensity on Indices of Inflammatory and Oxidative Stress. Res. Sports Med. 2015, 23, 73–87. [Google Scholar] [CrossRef]
- Ryrsø, C.K.; Thaning, P.; Siebenmann, C.; Lundby, C.; Lange, P.; Pedersen, B.K.; Hellsten, Y.; Iepsen, U.W. Effect of endurance versus resistance training on local muscle and systemic inflammation and oxidative stress in COPD. Scand. J. Med. Sci. Sports 2018, 28, 2339–2348. [Google Scholar] [CrossRef]
- Koozehchian, M.S.; Daneshfar, A.; Fallah, E.; Agha-Alinejad, H.; Samadi, M.; Kaviani, M.; B., M.K.; Jung, Y.P.; Sablouei, M.H.; Moradi, N.; et al. Effects of nine weeks L-Carnitine supplementation on exercise performance, anaerobic power, and exercise-induced oxidative stress in resistance-trained males. J. Exerc. Nutr. Biochem. 2018, 22, 7–19. [Google Scholar] [CrossRef]
- Jürgenson, J.; Serg, M.; Kampus, P.; Kals, J.; Zagura, M.; Viru, M.; Zilmer, K.; Zilmer, M.; Eha, J.; Unt, E. Oxidative Stress Parameters and Its Associations with Arterial Stiffness in Competitive Powerlifting Athletes After 12-Week Supervised Strength Training. J. Strength Cond. Res. 2019, 33, 1816–1822. [Google Scholar] [CrossRef] [Green Version]
- Prasertsri, P.; Boonla, O. Upper and lower limb resistance training program versus high-intensity interval training on oxidative stress markers in university athletes. J. Exerc. Rehabil. 2021, 17, 198–206. [Google Scholar] [CrossRef] [PubMed]
- Alves, N.F.; Porpino, S.K.; Monteiro, M.M.; Gomes, E.; Braga, V.A. Coconut oil supplementation and physical exercise improves baroreflex sensitivity and oxidative stress in hypertensive rats. Appl. Physiol. Nutr. Metab. 2015, 40, 393–400. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lima, F.D.; Stamm, D.N.; Della Pace, I.D.; Ribeiro, L.R.; Rambo, L.M.; Bresciani, G.; Ferreira, J.; Rossato, M.F.; Silva, M.A.; Pereira, M.E.; et al. Ibuprofen intake increases exercise time to exhaustion: A possible role for pre-venting exercise-induced fatigue. Scand. J. Med. Sci. Sports 2016, 26, 1160–1170. [Google Scholar] [CrossRef]
- McAnulty, S.R.; Owens, J.T.; McAnulty, L.S.; Nieman, D.C.; Morrow, J.D.; Dumke, C.L.; Milne, G.L. Ibuprofen use during extreme exercise: Effects on oxidative stress and PGE2. Med. Sci. Sports Exerc. 2007, 39, 1075–1079. [Google Scholar] [CrossRef] [PubMed]
- López-Durán, J.L.; Frías-Iniesta, J. Drug synergism in analgesia treated with ibuprofen and codeine. SEMERGEN-Med. Fam. 2014, 38, 24–32. [Google Scholar] [CrossRef]
- Trappe, T.A.; White, F.; Lambert, C.P.; Cesar, D.; Hellerstein, M.; Evans, W.J. Effect of ibuprofen and acetaminophen on post exercise muscle protein synthesis. Am. J. Physiol. 2002, 282, E551–E556. [Google Scholar]
- Trappe, T.A.; Fluckey, J.D.; White, F.; Lambert, C.P.; Evans, W.J. Skeletal Muscle PGF2α and PGE2 in Response to Eccentric Resistance Exercise: Influence of Ibuprofen and Acetaminophen. J. Clin. Endocrinol. Metab. 2001, 86, 5067–5070. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peterson, J.; Trappe, T.A.; Mylona, E.; White, F.; Lambert, C.P.; Evans, W.J.; Pizza, F.X. Ibuprofen and Acetaminophen: Effect on Muscle Inflammation after Eccentric Exercise. Med. Sci. Sports Exerc. 2003, 35, 892–896. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Almqvist, P.M.; Ekström, B.; Kuenzig, M.; Haglund, U.; Schwartz, S.I. Increased survival of endotoxin-injected dogs treated with methylprednisolone, naloxone, and ibuprofen. Circ. Shock 1984, 14, 129–136. [Google Scholar] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variables | (Mean ± Standard Deviation) |
|---|---|
| n | 10 |
| Age (years) | 27.13 ± 5.57 |
| Body Weight (kg) | 79.25 ± 25.51 |
| Experience (years) | 2.99 ± 0.51 |
| 1-RM/Bench press (kg) | 137.13 ± 30.53 * |
| 1-RM/Body Weight | 1.80 ± 0.31 ** |
| Variables | Placebo | Ibuprofen | p | Cohen’s d |
| CPR (mg/dL) | 1.80 ±1.47 | 3.55 ± 2.37 | 0.031 * | 1.80 d |
| Urea (mg/dL) | 28.88 ± 6.66 | 24.38 ± 6.74 | 0.074 | 3.35 d |
| Uric acid (mg/dL) | 5.14 ± 1.10 | 5.50 ± 1.21 | 0.140 | 1.41 d |
| Leukocytes (mm3) | 7.41 ± 1.80 | 6.64 ± 1.67 | 0.415 | 2.08 d |
| Neutrophils (%) | 3.72 ± 1.22 | 4.88 ± 1.14 | 0.151 | 4.66 d |
| Lymphocytes (%) | 2.43 ± 0.58 | 3.48 ± 0.78 | 0.001 * | 4.36 d |
| Erythrocytes (million/mm3) | 5.06 ± 0.39 | 5.13 ± 0.46 | 0.221 | 0.64 b |
| Hemoglobin (g/mL) | 15.08 ± 1.12 | 15.00 ± 1.43 | 0.767 | 0.20 a |
| Hematocrit (%) | 42.63 ± 3.30 | 43.95 ± 4.00 | 0.019 * | 1.31 d |
| MCV (U3) | 84.29 ± 2.21 | 85.67 ± 3.36 | 0.090 | 1.08 c |
| MCH (UUG) | 29.79 ± 0.52 | 29.23 ± 0.89 | 0.123 | 1.42 d |
| MCHC (%) | 35.36 ± 0.94 | 34.12 ± 1.14 | 0.007 * | 4.31 d |
| RDW (%) | 10.24 ± 3.35 | 11.50 ± 0.54 | 0.305 | 0.45 b |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aidar, F.J.; Fraga, G.S.; Getirana-Mota, M.; Marçal, A.C.; Santos, J.L.; de Souza, R.F.; Ferreira, A.R.P.; Neves, E.B.; Zanona, A.d.F.; Bulhões-Correia, A.; et al. Effects of Ibuprofen Use on Lymphocyte Count and Oxidative Stress in Elite Paralympic Powerlifting. Biology 2021, 10, 986. https://0-doi-org.brum.beds.ac.uk/10.3390/biology10100986
Aidar FJ, Fraga GS, Getirana-Mota M, Marçal AC, Santos JL, de Souza RF, Ferreira ARP, Neves EB, Zanona AdF, Bulhões-Correia A, et al. Effects of Ibuprofen Use on Lymphocyte Count and Oxidative Stress in Elite Paralympic Powerlifting. Biology. 2021; 10(10):986. https://0-doi-org.brum.beds.ac.uk/10.3390/biology10100986
Chicago/Turabian StyleAidar, Felipe J., Guacira S. Fraga, Márcio Getirana-Mota, Anderson Carlos Marçal, Jymmys L. Santos, Raphael Fabricio de Souza, Alexandre Reis Pires Ferreira, Eduardo Borba Neves, Aristela de Freitas Zanona, Alexandre Bulhões-Correia, and et al. 2021. "Effects of Ibuprofen Use on Lymphocyte Count and Oxidative Stress in Elite Paralympic Powerlifting" Biology 10, no. 10: 986. https://0-doi-org.brum.beds.ac.uk/10.3390/biology10100986