
Effect of Computer-Aided Navigation Techniques on the Accuracy of Endodontic Access Cavities: A Systematic Review and Meta-Analysis

 , and
, and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
Study Design
3. Results
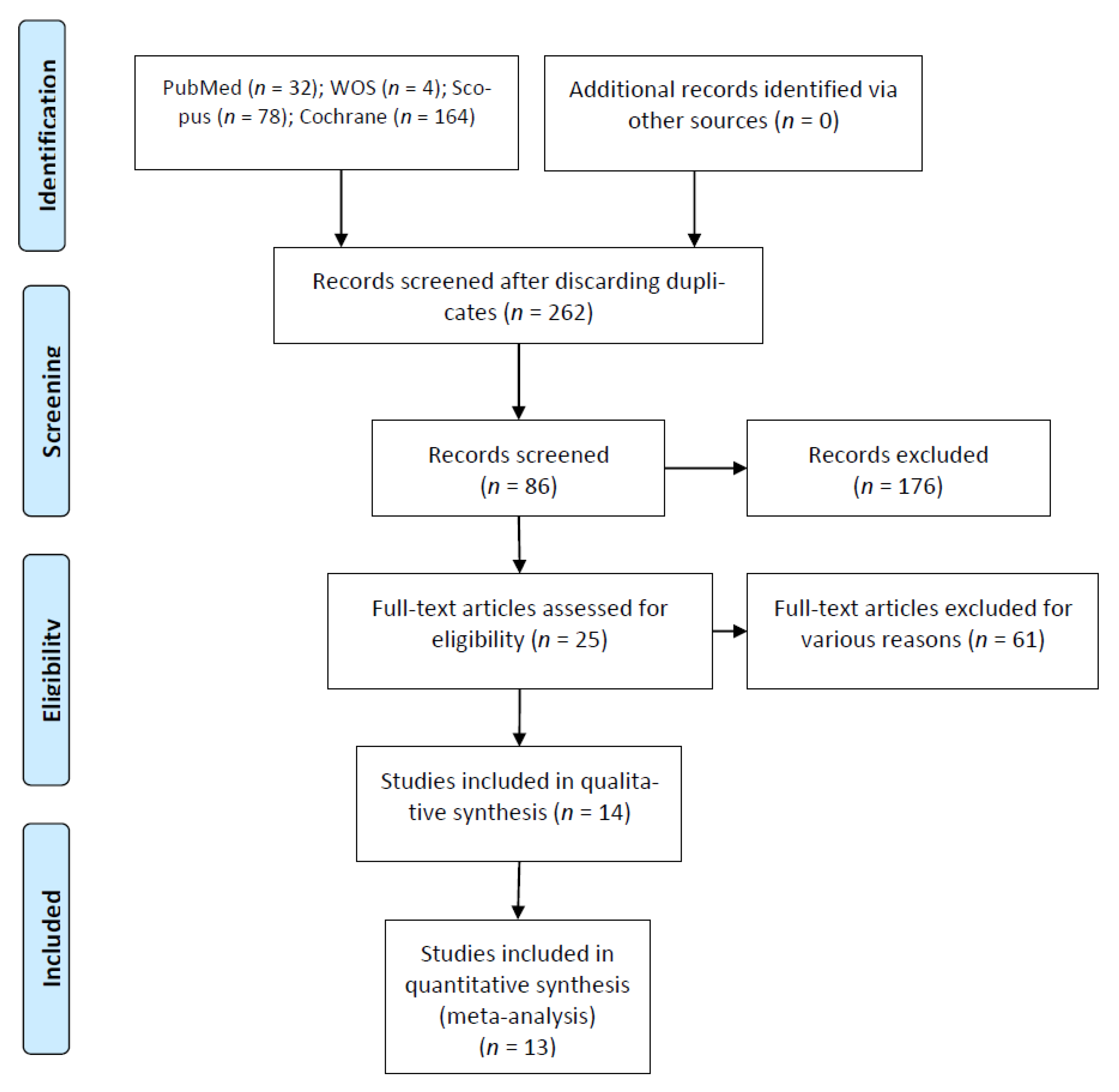
3.1. Flow Diagram
3.2. Qualitative Analysis
3.3. Quality Assessment
3.4. Quantitative Analysis
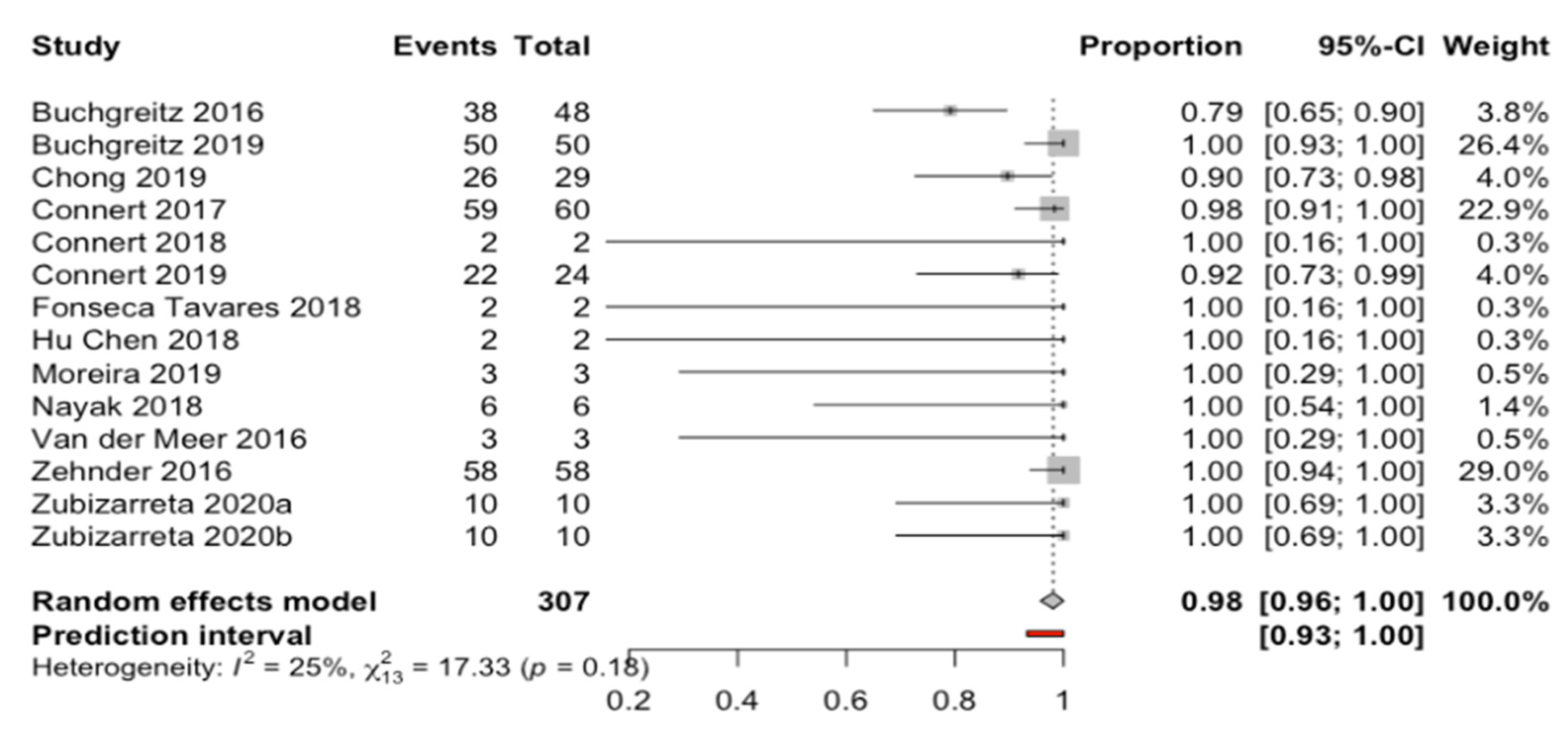
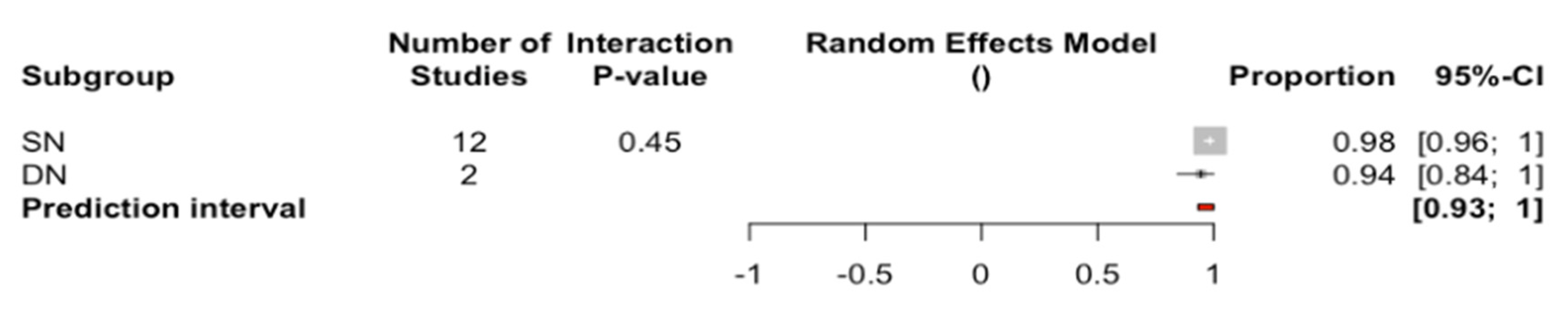
3.4.1. Root Canal Location Success Rate
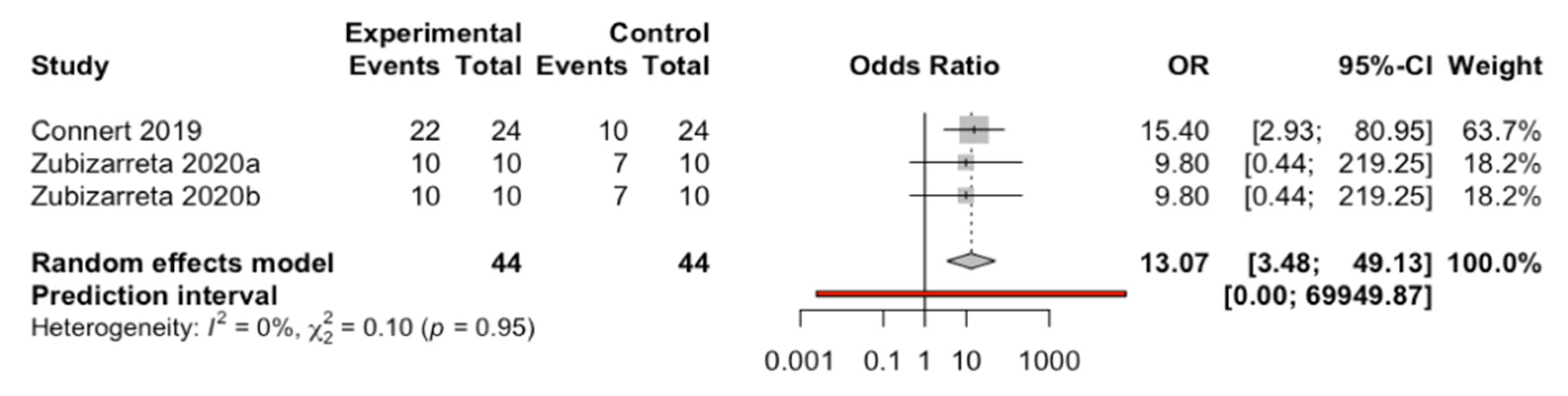
3.4.2. Comparison Between Computer-Aided Navigation Techniques and Control Group
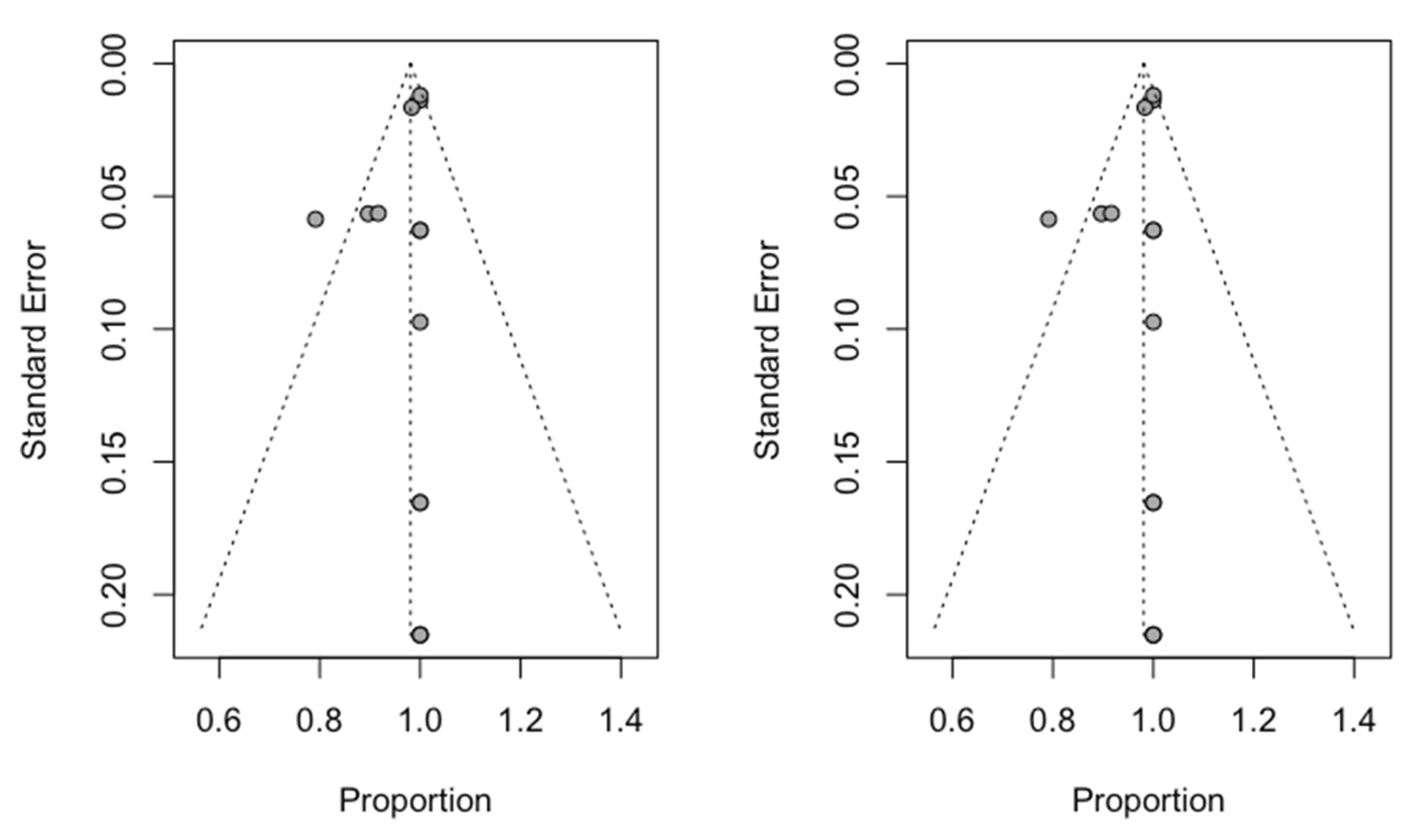
3.5. Publication Bias
4. Discussion
5. Conclusions
Funding
Conflicts of Interest
References
- Baruwa, A.O.; Martins, J.N.R.; Meirinhos, J.; Pereira, B.; Gouveia, J.; Quaresma, S.A.; Monroe, A.; Ginjeira, A. The Influence of Missed Canals on the Prevalence of Periapical Lesions in Endodontically Treated Teeth: A Cross-sectional Study. J. Endod. 2020, 46, 34–39. [Google Scholar] [CrossRef] [PubMed]
- Karabucak, B.; Bunes, A.; Chehoud, C.; Kohli, M.R.; Setzer, F. Prevalence of apical periodontitis in endodontically treated premolars and molars with untreated canal: A cone - beam computed tomography study. J. Endod. 2016, 42, 538–541. [Google Scholar] [CrossRef] [PubMed]
- Zender, M.S.; Connert, T.; Weiger, R.; Krastl, G.; Kühl, S. Guided endodontics: Accuracy of a novel method for guided access cavity preparation and root canal location. Int. Endod. J. 2016, 49, 966–972. [Google Scholar] [CrossRef] [PubMed]
- Venskutonis, T.; Plotino, G.; Juodzbalys, G.; Mickevičiene, L. The importance of cone-beam computed tomography in the management of endodontic problems: A review of the literature. J. Endod. 2014, 40, 1895–1901. [Google Scholar] [CrossRef] [PubMed]
- Zubizarreta-Macho, Á.; Muñoz, A.P.; Deglow, E.R.; Agustín-Panadero, R.; Álvarez, J.M. Accuracy of Computer-Aided Dynamic Navigation Compared to Computer-Aided Static Procedure for Endodontic Access Cavities: An in Vitro Study. J. Clin. Med. 2020, 9, 129. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Plotino, G.; Grande, N.M.; Isufi, A.; Ioppolo, P.; Pedulla, E.; Bedini, R.; Gambarini, G.; Testarelli, L. Fracture Strength of Endodontically Treated Teeth with Different Access Cavity Designs. J. Endod. 2017, 43, 995–1000. [Google Scholar] [CrossRef] [PubMed]
- Liberati, A.; Banzi, R.; Moja, L. Measuring the impact of evidence: The Cochrane systematic review of organized stroke care. Intern. Emerg. Med. 2009, 4, 507–510. [Google Scholar]
- Nagendrababu, V.; Duncan, H.F.; Tsesis, I.; Sathorn, C.; Pulikkotil, S.J.; Dharmarajan, L.; Dummer, P.M.H. PRISMA for abstracts: Best practice for reporting abstracts of systematic reviews in Endodontology [published online ahead of print, 2019 Mar 19]. Int. Endod. J. 2019, 52, 1096–1107. [Google Scholar]
- Nagendrababu, V.; Dilokthornsakul, P.; Jinatongthai, P.; Veettil, S.K.; Pulikkotil, S.J.; Duncan, H.F.; Dummer, P.M.H. Glossary for systematic reviews and meta-analyses. Int. Endod. J. 2020, 53, 232–249. [Google Scholar] [CrossRef] [Green Version]
- Krithikadatta, J.; Gopikrishna, V.; Datta, M. CRIS Guidelines (Checklist for Reporting In-vitro Studies): A concept note on the need for standardized guidelines for improving quality and transparency in reporting in-vitro studies in experimental dental research. J. Conserv. Dent. 2014, 17, 301–304. [Google Scholar] [CrossRef] [Green Version]
- Jadad, A.R.; Moore, R.A.; Carroll, D.; Jenkinson, C.; Reynolds, D.J.M.; Gavaghan, D.J.; McQuay, H.J. Assessing the quality of reports of randomized clinical trials: Is blinding necessary? Control. Clin. Trials 1996, 17, 1–12. [Google Scholar] [CrossRef]
- Buchgreitz, J.; Buchgreitz, M.; Mortensen, D.; Bjørndal, L. Guided access cavity preparation using cone-beam computed tomography and optical surface scans - an ex vivo study. Int. Endod. J. 2016, 49, 790–795. [Google Scholar] [CrossRef]
- Chong, B.S.; Dhesi, M.; Makdissi, J. Computer-aided dynamic navigation: A novel method for guided endodontics. Quintessence Int. 2019, 50, 196–202. [Google Scholar] [PubMed]
- Connert, T.; Zehnder, M.S.; Weiger, R.; Kühl, S.; Krastl, G. Microguided Endodontics: Accuracy of a Miniaturized Technique for Apically Extended Access Cavity Preparation in Anterior Teeth. J. Endod. 2017, 43, 787–790. [Google Scholar] [CrossRef] [PubMed]
- Connert, T.; Krug, R.; Eggmann, F.; Emsermann, I.; ElAyouti, A.; Weiger, R.; Kühl, S.; Krastl, G. Guided Endodontics versus Conventional Access Cavity Preparation: A Comparative Study on Substance Loss Using 3-dimensional-printed Teeth. J. Endod. 2019, 45, 327–331. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Li, H.; Lin, F.; Zhao, Y.J.; Guo, Y.J.; Zhang, X.-Y.; Wang, Y.; Lyu, P. 3D printing of drill guide template for access cavity preparation in human molars: A preliminary study. Rapid Prototyp. 2018, 24, 914–919. [Google Scholar] [CrossRef]
- Nayak, A.; Jain, P.K.; Kankar, P.K.; Jain, N. Computer-aided design-based guided endodontic: A novel approach for root canal access cavity preparation. Proc. Inst. Mech. Eng. H 2018, 232, 787–795. [Google Scholar] [CrossRef] [PubMed]
- Connert, T.; Zehnder, M.S.; Amato, M.; Weiger, R.; Kühl, S.; Krastl, G. Microguided Endodontics: A method to achieve minimally invasive access cavity preparation and root canal location in mandibular incisors using a novel computer-guided technique. Int. Endod. J. 2018, 51, 247–255. [Google Scholar] [CrossRef]
- Fonseca Tavares, W.L.; Diniz Viana, A.C.; de Carvalho Machado, V.; Feitosa Henriques, L.C.; Ribeiro Sobrinho, A.P. Guided Endodontic Access of Calcified Anterior Teeth. J. Endod. 2018, 44, 1195–1199. [Google Scholar] [CrossRef]
- Maia, L.M.; de Carvalho Machado, V.; da Silva, N.R.F.A.; Brito Júnior, M.; da Silveira, R.R.; Moreira Júnior, G.; Ribeiro Sobrinho, A.P. Case Reports in Maxillary Posterior Teeth by Guided Endodontic Access. J. Endod. 2019, 45, 214–218. [Google Scholar] [CrossRef] [PubMed]
- van der Meer, W.J.; Vissink, A.; Ng, Y.L.; Gulabivala, K. 3D Computer aided treatment planning in endodontics. J. Dent. 2016, 45, 67–72. [Google Scholar] [CrossRef]
- Buchgreitz, J.; Buchgreitz, M.; Bjørndal, L. Guided root canal preparation using cone beam computed tomography and optical surface scans - an observational study of pulp space obliteration and drill path depth in 50 patients. Int. Endod. J. 2019, 52, 559–568. [Google Scholar] [CrossRef] [PubMed]
- Jain, S.D.; Carrico, C.K.; Bermanis, I. 3-Dimensional Accuracy of Dynamic Navigation Technology in Locating Calcified Canals. J. Endod. 2020, 46, 839–845. [Google Scholar] [CrossRef]
- Van Assche, N.; Vercruyssen, M.; Coucke, W.; Teughels, W.; Jacobs, R.; Quirynen, M. Accuracy of computer-aided implant placement. Clin. Oral Implants Res. 2012, 23, 112–123. [Google Scholar] [CrossRef] [PubMed]
- Sicilia, A.; Botticelli, D. Computer-guided implant therapy and soft- and hard- tissue aspects. The Third EAOConsensus Conference 2012. Clin. Oral Implants Res. 2012, 23, 157–161. [Google Scholar] [CrossRef] [PubMed]
- Gambarini, G.; Galli, M.; Morese, A.; Stefanelli, L.V.; Abduljabbar, F.; Giovarruscio, M.; Di Nardo, D.; Seracchiani, M.; Testarelli, L. Precision of Dynamic Navigation to Perform Endodontic Ultraconservative Access Cavities: A Preliminary In Vitro Analysis. J. Endod. 2020, 46, 1286–1290. [Google Scholar] [CrossRef]
- Block, M.; Emery, R.; Lank, K.; Ryan, J. Implant Placement Accuracy Using Dynamic Navigation. Int. J. Oral Maxillofac. Implants 2016, 32, 92–99. [Google Scholar] [CrossRef]
- Stefanelli, L.V.; DeGroot, B.S.; Lipton, D.I.; Mandelaris, G.A. Accuracy of a Dynamic Dental Implant Navigation System in a Private Practice. Int. J. Oral Maxillofac. Implants 2019, 34, 205–213. [Google Scholar] [CrossRef] [PubMed]
- Mediavilla Guzmán, A.; Riad Deglow, E.; Zubizarreta-Macho, Á.; Agustín-Panadero, R.; Hernández Montero, S. Accuracy of Computer-Aided Dynamic Navigation Compared to Computer-Aided Static Navigation for Dental Implant Placement: An In Vitro Study. J. Clin. Med. 2019, 8, 2123. [Google Scholar] [CrossRef] [Green Version]
- Chen, C.K.; Yuh, D.Y.; Huang, R.Y.; Fu, E.; Tsai, C.F.C.C. Accuracy of implant placement with a navigation system, a laboratory guide, and freehand drilling. Int. J. Oral Maxillofac. Implants 2018, 33, 1213–1218. [Google Scholar] [CrossRef] [PubMed]
- Tchorz, J.P.; Wrbas, K.T.; Hellwig, E. Guided endodontic access of a calcified mandibular central incisor using a software-based three-dimensional treatment plan. Int. J. Comput. Dent. 2019, 22, 273–281. [Google Scholar]
- Torres, A.; Shaheen, E.; Lambrechts, P.; Politis, C.; Jacobs, R. Microguided Endodontics: A case report of a maxillary lateral incisor with pulp canal obliteration and apical periodontitis. Int. Endod. J. 2019, 52, 540–549. [Google Scholar] [CrossRef] [PubMed]
- Lara-Mendes, S.T.O.; Barbosa, C.F.M.; Machado, V.C.; Santa-Rosa, C.C. A New Approach for Minimally Invasive Access to Severely Calcified Anterior Teeth Using the Guided Endodontics Technique. J. Endod. 2018, 44, 1578–1582. [Google Scholar] [CrossRef] [PubMed]
- Zubizarreta-Macho, Á.; Ferreiroa, A.; Agustín-Panadero, R.; Rico-Romano, C.; Lobo-Galindo, A.B.; Mena-Álvarez, J. Endodontic re-treatment and restorative treatment of a dens invaginatus type II through new technologies. J. Clin. Exp. Dent. 2019, 11, e570–e576. [Google Scholar] [CrossRef] [PubMed]
- Zubizarreta Macho, Á.; Ferreiroa, A.; Rico-Romano, C.; Alonso-Ezpeleta, L.Ó.; Mena-Álvarez, J. Diagnosis and endodontic treatment of type II dens invaginatus by using cone-beam computed tomography and splint guides for cavity access: A case report. J. Am. Dent. Assoc. 2015, 146, 266–270. [Google Scholar] [CrossRef]
- Mena-Álvarez, J.; Rico-Romano, C.; Lobo-Galindo, A.B.; Zubizarreta-Macho, Á. Endodontic treatment of dens evaginatus by performing a splint guided access cavity. J. Esthet. Restor. Dent. 2017, 29, 396–402. [Google Scholar] [CrossRef]
- Mena-Álvarez, J.; Riad-Deglow, E.; Quispe-López, N.; Rico-Romano, C.; Zubizarreta-Macho, A. Technology at the service of surgery in a new technique of autotransplantation by guided surgery: A case report. BMC Oral Health 2020, 20, 99. [Google Scholar] [CrossRef] [PubMed]
- Tavares, W.L.F.; Fonseca, F.O.; Maia, L.M.; de Carvalho Machado, V.; França Alves Silva, N.R.; Junior, G.M.; Ribeiro Sobrinho, A.P. 3D Apicoectomy Guidance: Optimizing Access for Apicoectomies. J. Oral Maxillofac. Surg. 2020, 78, 357.e1–357.e8. [Google Scholar] [CrossRef] [PubMed]
- Sutter, E.; Lotz, M.; Rechenberg, D.K.; Stadlinger, B.; Rücker, M.; Valdec, S. Guided apicoectomy using a CAD/CAM drilling template. Int. J. Comput. Dent. 2019, 22, 363–369. [Google Scholar] [PubMed]
- Gargallo-Albiol, J.; Barootchi, S.; Salomó-Coll, O.; Wang, H.L. Advantages and disadvantages of implant navigation surgery. A systematic review. Anat. Anz. 2019, 225, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Pellegrino, G.; Mangano, C.; Mangano, R.; Ferri, A.; Taraschi, V.; Marchetti, C. Augmented reality for dental implantology: A pilot clinical report of two cases. BMC Oral Health 2019, 19, 158. [Google Scholar] [CrossRef] [PubMed]
- Suebnukarn, S.; Hataidechadusadee, R.; Suwannasri, N.; Suprasert, N.; Rhienmora, P.; Haddawy, P. Access cavity preparation training using haptic virtual reality and microcomputed tomography tooth models. Int. Endod. J. 2011, 44, 983–989. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author (Year) | Study Type | Sample (n) | Measurement Procedure | Computer-Aided Navigation Technique | Root Canal Location Rate | Computer-Aided Navigation Technique Results |
|---|---|---|---|---|---|---|
| Buchgreitz et al. (2016) [13] | In vitro | 48 | Clinical and radiographic | SN | 38/48 | Apical horizontal deviation: 0.46 (0.69–0.32) mm |
| Buchgreitz et al. (2019) [23] | CT | 50 | Clinical and radiographic | SN | 50/50 | Root canal location success: 100% |
| Chong et al. (2019) [14] | In vitro | 29 | Clinical and radiographic | DN | 26/29 | Root canal location success: 89.7% |
| Connert et al. (2017) [15] | In vitro | 60 | Clinical and radiographic | SN | 59/60 | Base of the bur (angle) deviation: 1.59 ± 1.22° |
| Base of the bur (mesio–distal) deviation: 0.12 ± 0.12 mm | ||||||
| Base of the bur (buccal–oral) deviation: 0.13 ± 0.13 mm | ||||||
| Base of the bur (apical–coronal) deviation: 0.12 ± 0.12 mm | ||||||
| Tip of the bur (mesio–distal) deviation: 0.14 ± 0.18 mm | ||||||
| Tip of the bur (buccal–oral) deviation: 0.34 ± 0.28 mm | ||||||
| Tip of the bur (apical–coronal) deviation: 0.12 ± 0.11 mm | ||||||
| Connert et al. (2018) [19] | CS | 2 | Clinical and radiographic | SN | 2/2 | Root canal location success: 100% |
| Connert et al. (2019) [16] | In vitro | 48 | Clinical and radiographic | Control | 10/24 | Root canal location success: 41.7% |
| Substance loss: 49.9 mm3 | ||||||
| SN | 22/24 | Root canal location success: 91.7% | ||||
| Substance loss: 9.8 mm3 | ||||||
| Fonseca Tavares et al. (2018) [20] | CS | 2 | Clinical and radiographic | SN | 2/2 | Root canal location success: 100% |
| Hu Chen et al. (2018) [17] | In vitro | 2 | Clinical and radiographic | SN | 2/2 | Root canal location success: 100% |
| Jain et al. (2020) [23] | In vitro | 138 | Clinical and radiographic | DN | NAv | Apical horizontal deviation 2D: 0.9 |
| Apical horizontal deviation 3D: 1.3 | ||||||
| Angular deviation 3D: 1.7 | ||||||
| Moreira Maia et al. (2019) [21] | CS | 3 | Clinical and radiographic | SN | 3/3 | Root canal location success: 100% |
| Nayak et al. (2018) [18] | In vitro | 6 | Clinical and radiographic | SN | 6/6 | Buccal–lingual deviation: 0.07–0.20 mm |
| Mesio–distal deviation: 0.08–0.19 mm | ||||||
| Total deviation: 0.15–0.26 mm | ||||||
| Van der Meer et al. (2016 [22] | CS | 3 | Clinical and radiographic | SN | 3/3 | Root canal location success: 100% |
| Zhender et al. (2016) [4] | In vitro | 58 | Clinical and radiographic | SN | 58/58 | Angle deviation: 1.81° |
| Mesio–distal deviation: 0.21 mm | ||||||
| Buccal–palatal deviation: 0.2 mm | ||||||
| Apical–coronal deviation: 0.16 mm | ||||||
| Zubizarreta et al. (2020) [6] | In vitro | 30 | Clinical and radiographic | Control | 7/10 | Coronal deviation: 4.03 ± 1.93 mm |
| Apical deviation: 2.43 ± 1.23 mm | ||||||
| Angular deviation: 14.95 ± 11.15° | ||||||
| a: SN | 10/10 | Coronal deviation: 7.44 ± 1.57 mm | ||||
| Apical deviation: 7.13 ± 1.73 mm | ||||||
| Angular deviation: 10.04 ± 5.2° | ||||||
| b: DN | 10/10 | Coronal deviation: 3.14 ± 0.86 mm | ||||
| Apical deviation: 2.48 ± 0.94 mm | ||||||
| Angular deviation: 5.58 ± 3.23° |
| Author (Year) | Sample Preparation and Handling | Allocation Sequence and RanDomization Process | Whether the Evaluators Were Blinded | Statistical Analysis | Score |
|---|---|---|---|---|---|
| Buchgreitz et al. (2016) [13] | Yes | No | No | Yes | 2 |
| Chong et al. (2019) [14] | Yes | No | No | No | 1 |
| Connert et al. (2017) [15] | Yes | No | No | Yes | 2 |
| Connert et al. (2019) [16] | Yes | No | No | Yes | 2 |
| Hu Chen et al. (2018) [17] | Yes | No | No | Yes | 2 |
| Nayak et al. (2017) [18] | Yes | No | No | Yes | 2 |
| Zehnder et al. (2017) [4] | Yes | No | No | Yes | 2 |
| Zubizarreta et al. (2020) [6] | Yes | Yes | No | Yes | 3 |
| Jadad Criteria | ||||||
|---|---|---|---|---|---|---|
| Author (Year) | Is the Study Randomized? | Is the Study Double-Blinded? | Were Withdrawals and Dropouts Described? | Adequate Method of Randomization? | Appropriate Blinding Method? | Score |
| Buchgreitz et al. (2019) [23] | 0 | 0 | 0 | 0 | 0 | 0 |
| Connert et al. (2018) [19] | NA | NA | NA | NA | NA | NA |
| Fonseca Tavares et al. (2018) [20] | NA | NA | NA | NA | NA | NA |
| Moreira Maia et al. (2019) [21] | NA | NA | NA | NA | NA | NA |
| Van der Meer et al. (2016) [22] | NA | NA | NA | NA | NA | NA |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zubizarreta-Macho, Á.; Valle Castaño, S.; Montiel-Company, J.M.; Mena-Álvarez, J. Effect of Computer-Aided Navigation Techniques on the Accuracy of Endodontic Access Cavities: A Systematic Review and Meta-Analysis. Biology 2021, 10, 212. https://0-doi-org.brum.beds.ac.uk/10.3390/biology10030212
Zubizarreta-Macho Á, Valle Castaño S, Montiel-Company JM, Mena-Álvarez J. Effect of Computer-Aided Navigation Techniques on the Accuracy of Endodontic Access Cavities: A Systematic Review and Meta-Analysis. Biology. 2021; 10(3):212. https://0-doi-org.brum.beds.ac.uk/10.3390/biology10030212
Chicago/Turabian StyleZubizarreta-Macho, Álvaro, Sara Valle Castaño, José María Montiel-Company, and Jesús Mena-Álvarez. 2021. "Effect of Computer-Aided Navigation Techniques on the Accuracy of Endodontic Access Cavities: A Systematic Review and Meta-Analysis" Biology 10, no. 3: 212. https://0-doi-org.brum.beds.ac.uk/10.3390/biology10030212