
Can Telemedicine Optimize the HCV Care Cascade in People Who Use Drugs? Features of an Innovative Decentralization Model and Comparison with Other Micro-Elimination Strategies

 , ,
, ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. PWUDs: Characteristics of a Special Population
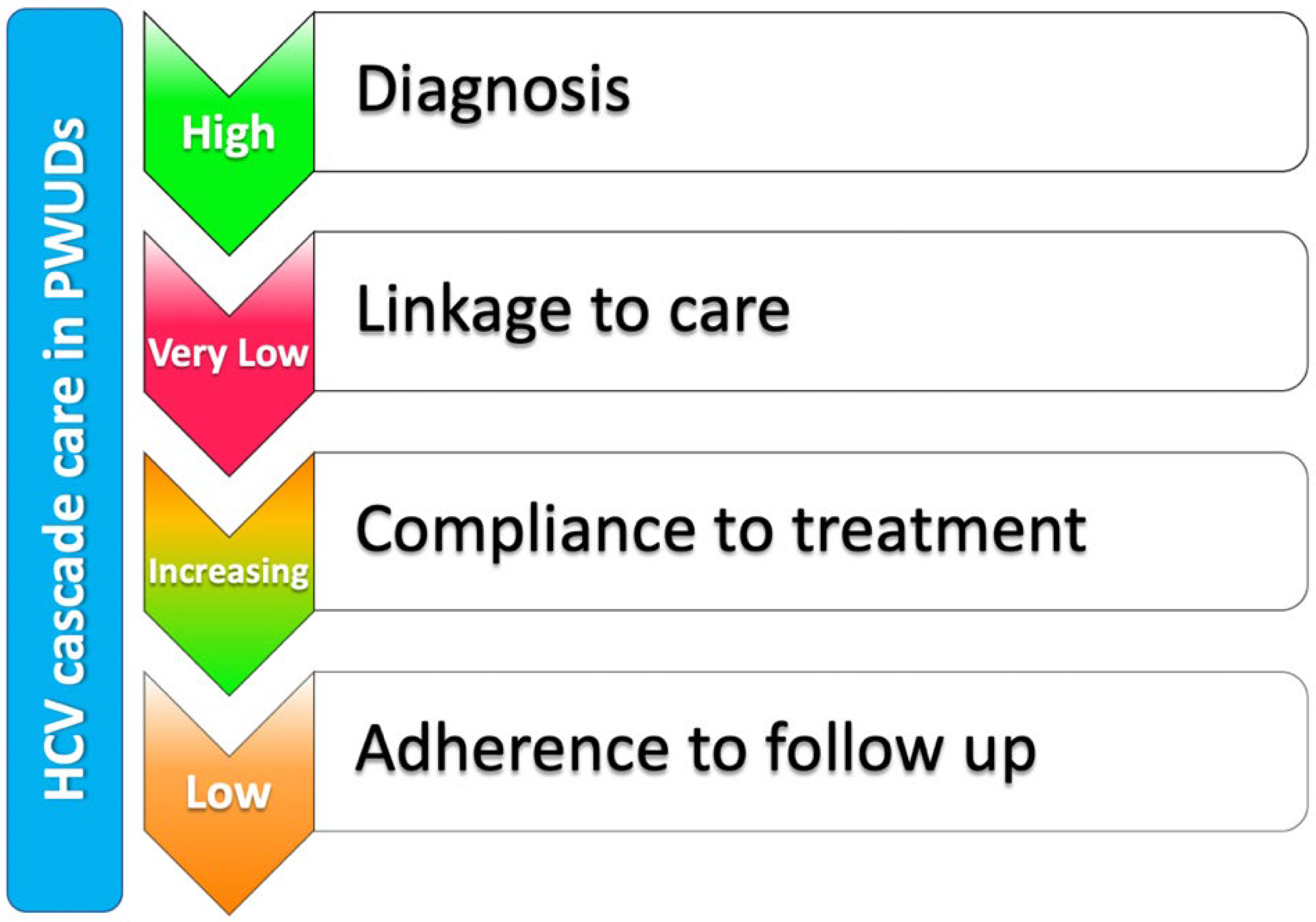
3. HCV Care Cascade in PWUDs
4. Treatment Models
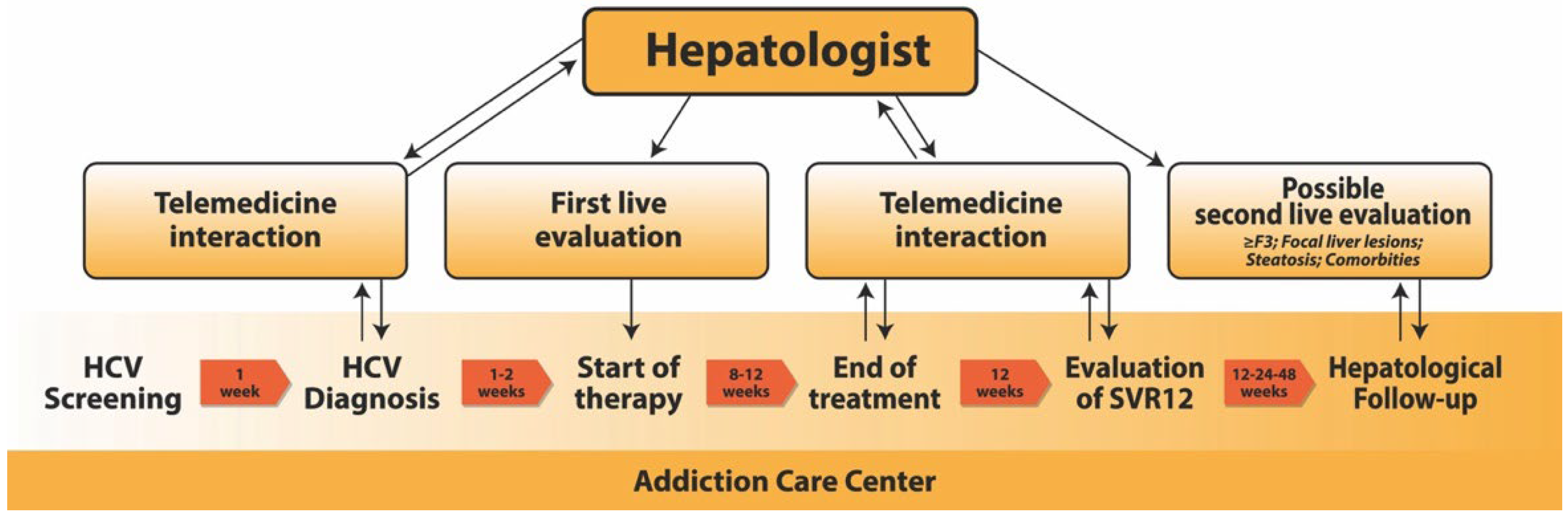
4.1. Our Telemedicine-Based Model
4.2. Other Telemedicine-Based Models
4.3. Other Treatment Models
4.3.1. Decentralization Models
4.3.2. Integrated Care
4.3.3. Directly Observed Therapy
4.3.4. Peer Support
4.3.5. Economic Incentives
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Polaris Observatory HCV Collaborators. Global change in hepatitis C virus prevalence and cascade of care between 2015 and 2020: A modelling study. Lancet Gastroenterol. Hepatol. 2022, 7, 396–415. [Google Scholar] [CrossRef]
- World Health Organization. Global Hepatitis Report 2017; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Kondili, L.A.; Craxì, A.; Aghemo, A. Absolute targets for HCV elimination and national health policy paradigms: Foreseeing future requirements. Liver Int. 2021, 41, 649–655. [Google Scholar] [CrossRef] [PubMed]
- Blach, S.; Kondili, L.A.; Aghemo, A.; Cai, Z.; Dugan, E.; Estes, C.; Gamkrelidze, I.; Ma, S.; Pawlotsky, J.-M.; Razavi-Shearer, D.; et al. Impact of COVID-19 on global HCV elimination efforts. J. Hepatol. 2021, 74, 31–36. [Google Scholar] [CrossRef]
- Nevola, R.; Messina, V.; Marrone, A.; Coppola, N.; Rescigno, C.; Esposito, V.; Sangiovanni, V.; Claar, E.; Pisaturo, M.; Fusco, F.M.; et al. Epidemiology of HCV and HBV in a High Endemic Area of Southern Italy: Opportunities from the COVID-19 Pandemic—Standardized National Screening or One Tailored to Local Epidemiology? Biology 2022, 11, 609. [Google Scholar] [CrossRef] [PubMed]
- Degenhardt, L.; Peacock, A.; Colledge, S.; Leung, J.; Grebely, J.; Vickerman, P.; Stone, J.; Cunningham, E.B.; Trickey, A.; Dumchev, K.; et al. Global prevalence of injecting drug use and sociodemographic characteristics and prevalence of HIV, HBV, and HCV in people who inject drugs: A multistage systematic review. Lancet Glob. Health 2017, 5, e1192–e1207. [Google Scholar] [CrossRef] [Green Version]
- Cousien, A.; Tran, V.C.; Deuffic-Burban, S.; Jauffret-Roustide, M.; Dhersin, J.-S.; Yazdanpanah, Y. Hepatitis C treatment as prevention of viral transmission and liver-related morbidity in persons who inject drugs. Hepatology 2016, 63, 1090–1101. [Google Scholar] [CrossRef]
- Rosato, V.; Nevola, R.; Conturso, V.; Perillo, P.; Mastrocinque, D.; Pappalardo, A.; Le Pera, T.; Del Vecchio, F.; Claar, E. Telemedicine improve HCV elimination among Italian people who use drugs: An innovative therapeutic model to increase the adherence to treatment into addiction care centers evaluated before and during the COVID-19. Biology, 2022; accepted. [Google Scholar]
- Rosato, V.; Nevola, R.; Conturso, V.; Perillo, P.; Le Pera, T.; Del Vecchio, F.; Claar, E. Telemedicine improve HCV elimination among Italian people who use drugs: An innovative therapeutic model to increase the adherence to treatment into addiction care centers. J. Hepatol. 2021, 75, S657–S658. [Google Scholar]
- Rashti, R.; Sharafi, H.; Alavian, S.M.; Moradi, Y.; Bolbanabad, A.M.; Moradi, G. Systematic Review and Meta-Analysis of Global Prevalence of HBsAg and HIV and HCV Antibodies among People Who Inject Drugs and Female Sex Workers. Pathogens 2020, 9, 432. [Google Scholar] [CrossRef]
- Doerrbecker, J.; Behrendt, P.; Mateu-Gelabert, P.; Ciesek, S.; Riebesehl, N.; Wilhelm, C.; Steinmann, J.; Pietschmann, T.; Steinmann, E. Transmission of Hepatitis C Virus among People Who Inject Drugs: Viral Stability and Association with Drug Preparation Equipment. J. Infect. Dis. 2013, 207, 281–287. [Google Scholar] [CrossRef] [Green Version]
- Eckhardt, B.; Winkelstein, E.R.; Shu, M.A.; Carden, M.R.; McKnight, C.A.; Jarlais, D.C.D.; Glesby, M.J.; Marks, K.; Edlin, B.R. Risk factors for hepatitis C seropositivity among young people who inject drugs in New York City: Implications for prevention. PLoS ONE 2017, 12, e0177341. [Google Scholar] [CrossRef] [PubMed]
- Larney, S.; Kopinski, H.; Beckwith, C.G.; Zaller, N.D.; Jarlais, D.D.; Hagan, H.; Rich, J.D.; van den Bergh, B.J.; Degenhardt, L. Incidence and prevalence of hepatitis C in prisons and other closed settings: Results of a systematic review and meta-analysis. Hepatology 2013, 58, 1215–1224. [Google Scholar] [CrossRef] [PubMed]
- Blouin, K.; Leclerc, P.; Morissette, C.; Roy, É.; Blanchette, C.; Parent, R.; Serhir, B.; Alary, M. Sex Work as an Emerging Risk Factor for Human Immunodeficiency Virus Seroconversion Among People who Inject Drugs in the SurvUDI Network. Sex Transm. Dis. 2016, 43, 648–655. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Robaeys, G.; Bielen, R.; Azar, D.G.; Razavi, H.; Nevens, F. Global genotype distribution of hepatitis C viral infection among people who inject drugs. J. Hepatol. 2016, 65, 1094–1103. [Google Scholar] [CrossRef] [Green Version]
- Foster, G.R.; Afdhal, N.; Roberts, S.K.; Bräu, N.; Gane, E.J.; Pianko, S.; Lawitz, E.; Thompson, A.; Shiffman, M.L.; Cooper, C.; et al. Sofosbuvir and Velpatasvir for HCV Genotype 2 and 3 Infection. N. Engl. J. Med. 2015, 373, 2608–2617. [Google Scholar] [CrossRef] [Green Version]
- Pawlotsky, J.M.; Negro, F.; Aghemo, A.; Berenguer, M.; Dalgard, O.; Dusheiko, G.; Marra, F.; Puoti, M.; Wedemeyer, H.; European Association for the Study of the Liver. EASL recommendations on treatment of hepatitis C: Final update of the series. J. Hepatol. 2020, 73, 1170–1218. [Google Scholar] [CrossRef]
- Fattovich, G.; Stroffolini, T.; Zagni, I.; Donato, F. Hepatocellular carcinoma in cirrhosis: Incidence and risk factors. Gastroenterology 2004, 127, S35–S50. [Google Scholar] [CrossRef]
- Macdonald, D.-C.; Nelson, M.; Bower, M.; Powles, T. Hepatocellular carcinoma, human immunodeficiency virus and viral hepatitis in the HAART era. World J. Gastroenterol. 2008, 14, 1657–1663. [Google Scholar] [CrossRef] [Green Version]
- Marino, A.; Zafarana, G.; Ceccarelli, M.; Cosentino, F.; Moscatt, V.; Bruno, G.; Bruno, R.; Benanti, F.; Cacopardo, B.; Celesia, B.M. Immunological and Clinical Impact of DAA-Mediated HCV Eradication in a Cohort of HIV/HCV Coinfected Patients: Monocentric Italian Experience. Diagnostics 2021, 11, 2336. [Google Scholar] [CrossRef]
- Shih, Y.-F.; Liu, C.-J. Hepatitis C Virus and Hepatitis B Virus Co-Infection. Viruses 2020, 12, 741. [Google Scholar] [CrossRef]
- Latham, N.H.; Doyle, J.S.; Palmer, A.Y.; Vanhommerig, J.W.; Agius, P.; Goutzamanis, S.; Li, Z.; Pedrana, A.; Gottfredsson, M.; Bouscaillou, J.; et al. Staying hepatitis C negative: A systematic review and meta-analysis of cure and reinfection in people who inject drugs. Liver Int. 2019, 39, 2244–2260. [Google Scholar] [CrossRef] [PubMed]
- Schwarz, T.; Horváth, I.; Fenz, L.; Schmutterer, I.; Rosian-Schikuta, I.; Mårdh, O. Interventions to increase linkage to care and adherence to treatment for hepatitis C among people who inject drugs: A systematic review and practical considerations from an expert panel consultation. Int. J. Drug Policy 2022, 102, 103588. [Google Scholar] [CrossRef] [PubMed]
- Grebely, J.; Dalgard, O.; Conway, B.; Cunningham, E.B.; Bruggmann, P.; Hajarizadeh, B.; Amin, J.; Bruneau, J.; Hellard, M.; Litwin, A.H.; et al. Sofosbuvir and velpatasvir for hepatitis C virus infection in people with recent injection drug use (SIMPLIFY): An open-label, single-arm, phase 4, multicentre trial. Lancet Gastroenterol. Hepatol. 2018, 3, 153–161. [Google Scholar] [CrossRef] [Green Version]
- Iversen, J.; Grebely, J.; Topp, L.; Wand, H.; Dore, G.; Maher, L. Uptake of hepatitis C treatment among people who inject drugs attending Needle and Syringe Programs in Australia, 1999–2011. J. Viral Hepat. 2014, 21, 198–207. [Google Scholar] [CrossRef]
- Messina, V.; Onorato, L.; Di Caprio, G.; Claar, E.; Iovinella, V.; Russo, A.; Rosato, V.; Salzillo, A.; Nevola, R.; Simeone, F.; et al. Directly Acting Antiviral-Based Treatment for HCV-Infected Persons Who Inject Drugs: A Multicenter Real-Life Study. Life 2020, 11, 17. [Google Scholar] [CrossRef] [PubMed]
- Christensen, S.; Buggisch, P.; Mauss, S.; Böker, K.H.W.; Schott, E.; Klinker, H.; Zimmermann, T.; Weber, B.; Reimer, J.; Serfert, Y.; et al. Direct-acting antiviral treatment of chronic HCV-infected patients on opioid substitution therapy: Still a concern in clinical practice? Addiction 2018, 113, 868–882. [Google Scholar] [CrossRef]
- Ghany, M.G.; Morgan, T.R.; AASLD-IDSA Hepatitis C Guidance Panel. Hepatitis C Guidance 2019 Update: American Association for the Study of Liver Diseases–Infectious Diseases Society of America Recommendations for Testing, Managing, and Treating Hepatitis C Virus Infection. Hepatology 2020, 71, 686–721. [Google Scholar] [CrossRef] [Green Version]
- Jordan, A.E.; Perlman, D.C.; Reed, J.; Smith, D.J.; Hagan, H. Patterns and Gaps Identified in a Systematic Review of the Hepatitis C Virus Care Continuum in Studies among People Who Use Drugs. Front. Public Health 2017, 5, 348. [Google Scholar] [CrossRef] [Green Version]
- Corcorran, M.A.; Tsui, J.I.; Scott, J.D.; Dombrowski, J.C.; Glick, S.N. Age and gender-specific hepatitis C continuum of care and predictors of direct acting antiviral treatment among persons who inject drugs in Seattle, Washington. Drug Alcohol Depend. 2021, 220, 108525. [Google Scholar] [CrossRef]
- Messina, V.; Russo, A.; Parente, E.; Russo, G.; Raimondo, T.; Salzillo, A.; Simeone, F.; Onorato, L.; Di Caprio, G.; Pisaturo, M.; et al. Innovative procedures for micro-elimination of HCV infection in persons who use drugs. J. Viral Hepat. 2020, 27, 1437–1443. [Google Scholar] [CrossRef]
- Gonzalez, S.A.; Fierer, D.S.; Talal, A.H. Medical and Behavioral Approaches to Engage People Who Inject Drugs into Care for Hepatitis C Virus Infection. Addict. Disord. Their Treat. 2017, 16, S1–S23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oru, E.; Trickey, A.; Shirali, R.; Kanters, S.; Easterbrook, P. Decentralisation, integration, and task-shifting in hepatitis C virus infection testing and treatment: A global systematic review and meta-analysis. Lancet Glob. Health 2021, 9, e431–e445. [Google Scholar] [CrossRef]
- Talal, A.H.; Andrews, P.; McLeod, A.; Chen, Y.; Sylvester, C.; Markatou, M.; Brown, L.S. Integrated, Co-located, Telemedicine-based Treatment Approaches for Hepatitis C Virus Management in Opioid Use Disorder Patients on Methadone. Clin. Infect. Dis. 2019, 69, 323–331. [Google Scholar] [CrossRef] [PubMed]
- Dhiman, R.K.; Grover, G.S.; Premkumar, M.; Roy, A.; Taneja, S.; Duseja, A.; Arora, S. Outcomes of real-world integrated HCV microelimination for people who inject drugs: An expansion of the punjab model. eClinicalMedicine 2021, 41, 101148. [Google Scholar] [CrossRef]
- Sivakumar, A.; Madden, L.; DiDomizio, E.; Eller, A.; Villanueva, M.; Altice, F.L. Treatment of Hepatitis C virus among people who inject drugs at a syringe service program during the COVID-19 response: The potential role of telehealth, medications for opioid use disorder and minimal demands on patients. Int. J. Drug Policy 2022, 101, 103570. [Google Scholar] [CrossRef] [PubMed]
- Norton, B.L.; Bachhuber, M.A.; Singh, R.; Agyemang, L.; Arnsten, J.H.; Cunningham, C.O.; Litwin, A.H. Evaluation of contingency management as a strategy to improve HCV linkage to care and treatment in persons attending needle and syringe programs: A pilot study. Int. J. Drug Policy 2019, 69, 1–7. [Google Scholar] [CrossRef]
- Ward, K.M.; Falade-Nwulia, O.; Moon, J.; Sutcliffe, C.G.; Brinkley, S.; Haselhuhn, T.; Katz, S.; Herne, K.; Arteaga, L.; Mehta, S.H.; et al. A Randomized Controlled Trial of Cash Incentives or Peer Support to Increase HCV Treatment for Persons with HIV Who Use Drugs: The CHAMPS Study. Open Forum Infect. Dis. 2019, 6, ofz166. [Google Scholar] [CrossRef]
- Akiyama, M.J.; Norton, B.L.; Arnsten, J.H.; Agyemang, L.; Heo, M.; Litwin, A.H. Intensive Models of Hepatitis C Care for People Who Inject Drugs Receiving Opioid Agonist Therapy. Ann. Intern. Med. 2019, 170, 594–603. [Google Scholar] [CrossRef]
- Schmidbauer, C.; Schubert, R.; Schütz, A.; Schwanke, C.; Luhn, J.; Gutic, E.; Pirker, R.; Lang, T.; Reiberger, T.; Haltmayer, H.; et al. Directly observed therapy for HCV with glecaprevir/pibrentasvir alongside opioid substitution in people who inject drugs—First real world data from Austria. PLoS ONE 2020, 15, e0229239. [Google Scholar] [CrossRef]
- Wade, A.J.; Doyle, J.S.; Gane, E.; Stedman, C.; Draper, B.; Iser, D.; Roberts, S.K.; Kemp, W.; Petrie, D.; Scott, N.; et al. Outcomes of Treatment for Hepatitis C in Primary Care, Compared to Hospital-based Care: A Randomized, Controlled Trial in People Who Inject Drugs. Clin. Infect. Dis. 2020, 70, 1900–1906. [Google Scholar] [CrossRef]
- Rinaldi, L.; Messina, V.; Di Marco, V.; Iovinella, V.; Claar, E.; Cariti, G.; Sacco, R.; De Luca, M.; Scifo, G.; Gatti, P.; et al. Factors Enhancing Treatment of Hepatitis C Virus–Infected Italian People Who Use Drugs: The CLEO-GRECAS Experience. Am. J. Gastroenterol. 2021, 116, 1248–1255. [Google Scholar] [CrossRef] [PubMed]
- Mangia, A.; Rina, M.F.; Canosa, A.; Piazzolla, V.; Squillante, M.M.; Agostinacchio, E.; Cocomazzi, G.; Visaggi, E.; Augello, N.; Iannuzziello, C.; et al. Increased Hepatitis C virus screening, diagnosis and linkage to care rates among people who use drugs through a patient-centered program from Italy. United Eur. Gastroenterol. J. 2021, 9, 1109–1118. [Google Scholar] [CrossRef] [PubMed]
- Byrne, C.J.; Beer, L.; Inglis, S.K.; Robinson, E.; Radley, A.; Goldberg, D.J.; Hickman, M.; Hutchinson, S.; Dillon, J.F. Real-world outcomes of rapid regional hepatitis C virus treatment scale-up among people who inject drugs in Tayside, Scotland. Aliment. Pharmacol. Ther. 2022, 55, 568–579. [Google Scholar] [CrossRef] [PubMed]
- Talal, A.H.; McLeod, A.; Andrews, P.; Nieves-McGrath, H.; Chen, Y.; Reynolds, A.; Sylvester, C.; Dickerson, S.S.; Markatou, M.; Brown, L.S. Patient Reaction to Telemedicine for Clinical Management of Hepatitis C Virus Integrated into an Opioid Treatment Program. Telemed. J. e-Health 2019, 25, 791–801. [Google Scholar] [CrossRef] [PubMed]
- Radley, A.; de Bruin, M.; Inglis, S.K.; Donnan, P.T.; Hapca, A.; Barclay, S.T.; Fraser, A.; Dillon, J. Clinical effectiveness of pharmacist-led versus conventionally delivered antiviral treatment for hepatitis C virus in patients receiving opioid substitution therapy: A pragmatic, cluster-randomised trial. Lancet Gastroenterol. Hepatol. 2020, 5, 809–818. [Google Scholar] [CrossRef]
- Syed, T.A.; Cherian, R.; Lewis, S.; Sterling, R.K. Telemedicine HCV treatment in department of corrections results in high SVR in era of direct-acting antivirals. J. Viral Hepat. 2020, 28, 209–212. [Google Scholar] [CrossRef]
- Cuadrado, A.; Cobo, C.; Mateo, M.; Blasco, A.J.; Cabezas, J.; Llerena, S.; I Fortea, J.; Lázaro, P.; Crespo, J. Telemedicine efficiently improves access to hepatitis C management to achieve HCV elimination in the penitentiary setting. Int. J. Drug Policy 2020, 88, 103031. [Google Scholar] [CrossRef]
- Galán, G.J.; Alia, C.A.; González, M.V.; Berriguete, R.M.G.; González, F.F.; Rodríguez, C.M.F.; Fernández, M.G.; García, M.L.G.; Losa, J.E.; Velasco, M.; et al. The contribution of telemedicine to hepatitis C elimination in a correctional facility. Rev. Esp. Enferm. Dig. 2019, 111, 550–555. [Google Scholar] [CrossRef]
- Sterling, R.K.; Cherian, R.; Lewis, S.; Genther, K.; Driscoll, C.; Martin, K.; Goode, M.B.; Matherly, S.; Siddiqui, M.S.; Luketic, V.A.; et al. Treatment of HCV in the Department of Corrections in the Era of Oral Medications. J. Correct. Health Care 2018, 24, 127–136. [Google Scholar] [CrossRef]
- Morey, S.; Hamoodi, A.; Jones, D.; Young, T.; Thompson, C.; Dhuny, J.; Buchanan, E.; Miller, C.; Hewett, M.; Valappil, M.; et al. Increased diagnosis and treatment of hepatitis C in prison by universal offer of testing and use of telemedicine. J. Viral Hepat. 2019, 26, 101–108. [Google Scholar] [CrossRef] [Green Version]
- Halder, A.; Li, V.G.; Sebastian, M.; Nazareth, S.; Tuma, R.; Cheng, W.; Doyle, A. Use of telehealth to increase treatment access for prisoners with chronic hepatitis C. Intern. Med. J. 2021, 51, 1344–1347. [Google Scholar] [CrossRef] [PubMed]
- Papaluca, T.; McDonald, L.; Craigie, A.; Gibson, A.; Desmond, P.; Wong, D.; Winter, R.; Scott, N.; Howell, J.; Doyle, J.S.; et al. Outcomes of treatment for hepatitis C in prisoners using a nurse-led, statewide model of care. J. Hepatol. 2019, 70, 839–846. [Google Scholar] [CrossRef] [PubMed]
- Allah, M.A.; Wahed, S.; Ammar, I.; Kamal, E.; Alboraie, M.; Abdel-Razek, W.; Hassany, M.; El-Serafy, M.; Waked, I.; Doss, W. Utility of telemedicine in the treatment of patients with chronic HCV infection using DAAs in remote areas with limited resources. Liver Int. 2021, 41, 1979–1980. [Google Scholar] [CrossRef] [PubMed]
- Hernandez, J.L.P.; Mendoza, R.L.; Martinez, J.L.; Roldan, J.F.T.; Rosales, P.A.C.; Arredondo, H.A.M.; Gonzalez, V.R.; Silva, L.D.L.C.; Santana-Vargas, D.; Tijera, M.D.F.H.D.L.; et al. Chronic viral hepatitis C micro-elimination program using telemedicine. The Mexican experience. Rev. Esp. Enferm. Dig. 2021, 113, 432–435. [Google Scholar] [CrossRef]
- Du, P.; Wang, X.; Kong, L.; Jung, J. Can Telementoring Reduce Urban-Rural Disparities in Utilization of Direct-Acting Antiviral Agents? Telemed. J. e-Health 2021, 27, 488–494. [Google Scholar] [CrossRef]
- Mashru, J.; Kirlew, M.; Saginur, R.; Schreiber, Y.S. Management of infectious diseases in remote northwestern Ontario with telemedicine videoconference consultations. J. Telemed. Telecare 2017, 23, 83–87. [Google Scholar] [CrossRef]
- Stephens, D.; Leston, J.; Terrault, N.A.; Gailloux, K.; Mera, J.; Essex, W.; Reilley, B. An Evaluation of Hepatitis C Virus Telehealth Services Serving Tribal Communities: Patterns of Usage, Evolving Needs, and Barriers. J. Public Health Manag. Pract. 2019, 25, S97–S100. [Google Scholar] [CrossRef]
- Doica, I.P.; Florescu, D.N.; Oancea, C.N.; Turcu-Stiolica, A.; Subtirelu, M.-S.; Dumitra, G.; Rogoveanu, I.; Gheonea, D.I.; Ungureanu, B.S. Telemedicine Chronic Viral Hepatitis C Treatment during the Lockdown Period in Romania: A Pilot Study. Int. J. Environ. Res. Public Health 2021, 18, 3694. [Google Scholar] [CrossRef]
- Morales-Arraez, D.; Hernández-Bustabad, A.; Medina-Alonso, M.J.; Santiago-Gutiérrez, L.G.; García-Gil, S.; Diaz-Flores, F.; Pérez-Pérez, V.; Nazco, J.; de Rota Martin, P.F.; Gutiérrez, F.; et al. Telemedicine and decentralized hepatitis C treatment as a strategy to enhance retention in care among people attending drug treatment centres. Int. J. Drug Policy 2021, 94, 103235. [Google Scholar] [CrossRef]
- Cooper, C.L.; Hatashita, H.; Corsi, D.J.; Parmar, P.; Corrin, R.; Garber, G. Direct-Acting Antiviral Therapy Outcomes in Canadian Chronic Hepatitis C Telemedicine Patients. Ann. Hepatol. 2017, 16, 874–880. [Google Scholar] [CrossRef]
- Haridy, J.; Iyngkaran, G.; Nicoll, A.; Hebbard, G.; Tse, E.; Fazio, T. eHealth Technologies for Screening, Diagnosis, and Management of Viral Hepatitis: A Systematic Review. Clin. Gastroenterol. Hepatol. 2021, 19, 1139–1150.e30. [Google Scholar] [CrossRef] [PubMed]
- Ho, S.B.; Bräu, N.; Cheung, R.; Liu, L.; Sanchez, C.; Sklar, M.; Phelps, T.E.; Marcus, S.G.; Wasil, M.M.; Tisi, A.; et al. Integrated Care Increases Treatment and Improves Outcomes of Patients with Chronic Hepatitis C Virus Infection and Psychiatric Illness or Substance Abuse. Clin. Gastroenterol. Hepatol. 2015, 13, 2005–2014.e3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bajis, S.; Dore, G.J.; Hajarizadeh, B.; Cunningham, E.B.; Maher, L.; Grebely, J. Interventions to enhance testing, linkage to care and treatment uptake for hepatitis C virus infection among people who inject drugs: A systematic review. Int. J. Drug Policy 2017, 47, 34–46. [Google Scholar] [CrossRef] [PubMed]
- Zhou, K.; Fitzpatrick, T.; Walsh, N.; Kim, J.Y.; Chou, R.; Lackey, M.; Scott, J.; Lo, Y.-R.; Tucker, J.D. Interventions to optimise the care continuum for chronic viral hepatitis: A systematic review and meta-analyses. Lancet Infect. Dis. 2016, 16, 1409–1422. [Google Scholar] [CrossRef] [Green Version]
- Socías, M.E.; Karamouzian, M.; Parent, S.; Barletta, J.; Bird, K.; Ti, L. Integrated models of care for people who inject drugs and live with hepatitis C virus: A systematic review. Int. J. Drug Policy 2019, 72, 146–159. [Google Scholar] [CrossRef]
- Delile, J.-M.; De Ledinghen, V.; Jauffret-Roustide, M.; Roux, P.; Reiller, B.; Foucher, J.; Dhumeaux, D. Hepatitis C virus prevention and care for drug injectors: The French approach. Hepatol. Med. Policy 2018, 3, 7. [Google Scholar] [CrossRef] [Green Version]
- Coffin, P.O.; Santos, G.-M.; Behar, E.; Hern, J.; Walker, J.; Matheson, T.; Kinnard, E.N.; Silvis, J.; Vittinghoff, E.; Fox, R.; et al. Randomized feasibility trial of directly observed versus unobserved hepatitis C treatment with ledipasvir-sofosbuvir among people who inject drugs. PLoS ONE 2019, 14, e0217471. [Google Scholar] [CrossRef]
- McDermott, C.L.; Lockhart, C.M.; Devine, B. Outpatient directly observed therapy for hepatitis C among people who use drugs: A systematic review and meta-analysis. J. Virus Erad. 2018, 4, 118–122. [Google Scholar] [CrossRef]
- Surey, J.; Menezes, D.; Francis, M.; Gibbons, J.; Sultan, B.; Miah, A.; Abubakar, I.; Story, A. From peer-based to peer-led: Redefining the role of peers across the hepatitis C care pathway: HepCare Europe. J. Antimicrob. Chemother. 2019, 74, v17–v23. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
|
First Authors | References | Year of Publication | Country | Study Design | Description of the Intervention | Telemedicine-Based Models? | HCV-RNA Positive Evaluated Patients, n | HCV-RNA Positive Treated Patients, n | Linkage to Care, % | Patients Who Have Completed Treatment, n/tot (%) | Adherence to Treatment, % | Overall SVR, n/tot (%) | Reinfection Rate, n/tot (%) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Our model | [8] | 2022 ‡ | Italy | Observational prospective monocentric | Decentralization “patient-tailored” model at SerDs | Yes | 135 | 135 | 100 | 129/135 (95.6) | 93.4 | 133/135 (98.5) | 1/133 (0.75) |
| Talal | [34] | 2019 | USA | Prospective | Decentralization model in OST program | Yes | 61 | 45 | 73.8 | 44/45 (97.8) | 10–20% missed ≥ 1 dose | 42/45 (93.3) | 2/42 (4.8) |
| Dhiman | [35] | 2021 | India | RCT | Integrated care | Yes | n.s. | 2826 * | n.s. | 2280/2826 (80.7) | n.e. | 1398/1552 evaluated (91.1) | n.e. |
| Sivakumar | [36] | 2022 | USA | NRS | Minimization of face-to-face visits | Yes | 35 | 31 | 88.6 | 31 (100) | n.e. | 29/31 (93.5) | n.e. |
| Grebely | [24] | 2018 | Several country | Multicentre open-label phase IV trial | Electronic blister packs | No | n.s. | 103 | n.s. | 100/103 (97.1) | 94 | 97/103 (94.2) | 1/98 (1) |
| Norton | [37] | 2019 | USA | NRS | Financial incentives | No | 12 | 9 | 75 | 9/9 (100) | 74 | 9/9 (100) | n.e. |
| Ward | [38] | 2019 | USA | RCT | Financial incentives | No | 54 | 41 | 76 | 39/41 (95.1) | 97.6 | 37/41 (90.2) | 1/38 (2.6) |
| Peer mentors | No | 54 | 45 | 83 | 42/45 (93.3) | 97.8 | 41/45 (91.1) | 0/41 (0) | |||||
| Akiyama | [39] | 2019 | USA | RCT | Directly observed therapy | No | n.s. | 51 | n.s. | 50/51 (98) | 86 | 50/51 (98) | n.e. |
| Self-administered treatment | n.s. | 51 | n.s. | 48/51 (94) | 75 | 46/51 (90.2) | n.e. | ||||||
| Messina | [31] | 2020 | Italy | Prospective | Training and partial decentralization | no | n.s. | 45 | 84 | 45/45 (100) | n.e. | 45/45 (100) | n.e. |
| Schmidbauer | [40] | 2020 | Austria | n.s. | Directly observed therapy | No | n.s. | 74 | n.s. | 74/74 (100) | 94.6 | 70/74 (94.6) | 1/70 (1.4) |
| Wade | [41] | 2020 | Australia/New Zealand | RCT | Primary care | No | 48 | 43 | 89.6 | 39/43 (90.7) | n.e. | 28/43 (65.1) | n.e. |
| hospital-based specialist care | 29 | 18 | 62.1 | 17/18 (94.4) | n.e. | 16/18 (88.9) | n.e. | ||||||
| Rinaldi | [42] | 2021 | Italy | Retrospective/prospective, multicenter | SerD | No | n.s. | 1460 | n.s. | 1451/1460 (99.4) | n.e. | 1404/1460 (96.2) | n.e. |
| non-SerD | No | n.s. | 249 | n.s. | 241/249 (96.8) | n.e. | 228/249 (91.6) | n.e. | |||||
| Mangia | [43] | 2021 | Italy | n.s. | Training, fast-track screening, dedicated transportation service | No | 231 | 226 | 97.8 | 220/226 (97.3) | 97.7 | 217/220 (98.6) | 1/217 (0.5) |
| Byrne | [44] | 2022 | Scotland | Retrospective | Community pharmacies | No | n.s. | 144 | n.s. | 140/144 (97.2) | n.e. | 131/144 (91) | 12/131 (9.2) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nevola, R.; Rosato, V.; Conturso, V.; Perillo, P.; Le Pera, T.; Del Vecchio, F.; Mastrocinque, D.; Pappalardo, A.; Imbriani, S.; Delle Femine, A.; et al. Can Telemedicine Optimize the HCV Care Cascade in People Who Use Drugs? Features of an Innovative Decentralization Model and Comparison with Other Micro-Elimination Strategies. Biology 2022, 11, 805. https://0-doi-org.brum.beds.ac.uk/10.3390/biology11060805
Nevola R, Rosato V, Conturso V, Perillo P, Le Pera T, Del Vecchio F, Mastrocinque D, Pappalardo A, Imbriani S, Delle Femine A, et al. Can Telemedicine Optimize the HCV Care Cascade in People Who Use Drugs? Features of an Innovative Decentralization Model and Comparison with Other Micro-Elimination Strategies. Biology. 2022; 11(6):805. https://0-doi-org.brum.beds.ac.uk/10.3390/biology11060805
Chicago/Turabian StyleNevola, Riccardo, Valerio Rosato, Vincenza Conturso, Pasquale Perillo, Teresa Le Pera, Ferdinando Del Vecchio, Davide Mastrocinque, Annalisa Pappalardo, Simona Imbriani, Augusto Delle Femine, and et al. 2022. "Can Telemedicine Optimize the HCV Care Cascade in People Who Use Drugs? Features of an Innovative Decentralization Model and Comparison with Other Micro-Elimination Strategies" Biology 11, no. 6: 805. https://0-doi-org.brum.beds.ac.uk/10.3390/biology11060805