What Differentiates Poor and Good Outcome Psychotherapy? A Statistical-Mechanics-Inspired Approach to Psychotherapy Research

 , , ,
, , ,
Abstract
:1. Introduction
2. Material and Methods
2.1. Sample
2.2. Measures
2.3. Data Analysis
- (1)
- Three independent PCAs are performed: (a) PCA of poor-outcome cases (6 variables); (b) PCA of good-outcome cases (6 variables); and (c) PCA of good-and-poor-outcome cases taken together with 12 (6 + 6) variables.
- (2)
- The component scores of the 24-variable case (i.e., 12 + 6 + 6) are scrutinized by means of mutual Pearson correlations. This procedure allows us to gather two pieces of crucial information. On the one hand, the component scores pertaining to (a) or (b) (subset) cases that scale with the same component scores of (c) (whole set) point to latent factors common to good and poor outcome cases (below called “mixed”). On the other hand, the component scores pertaining to (c) that scale only with one of the (a) and (b) subsets are peculiar to either poor or good outcome cases (below called “pure”).
3. Results
3.1. Static Analyses
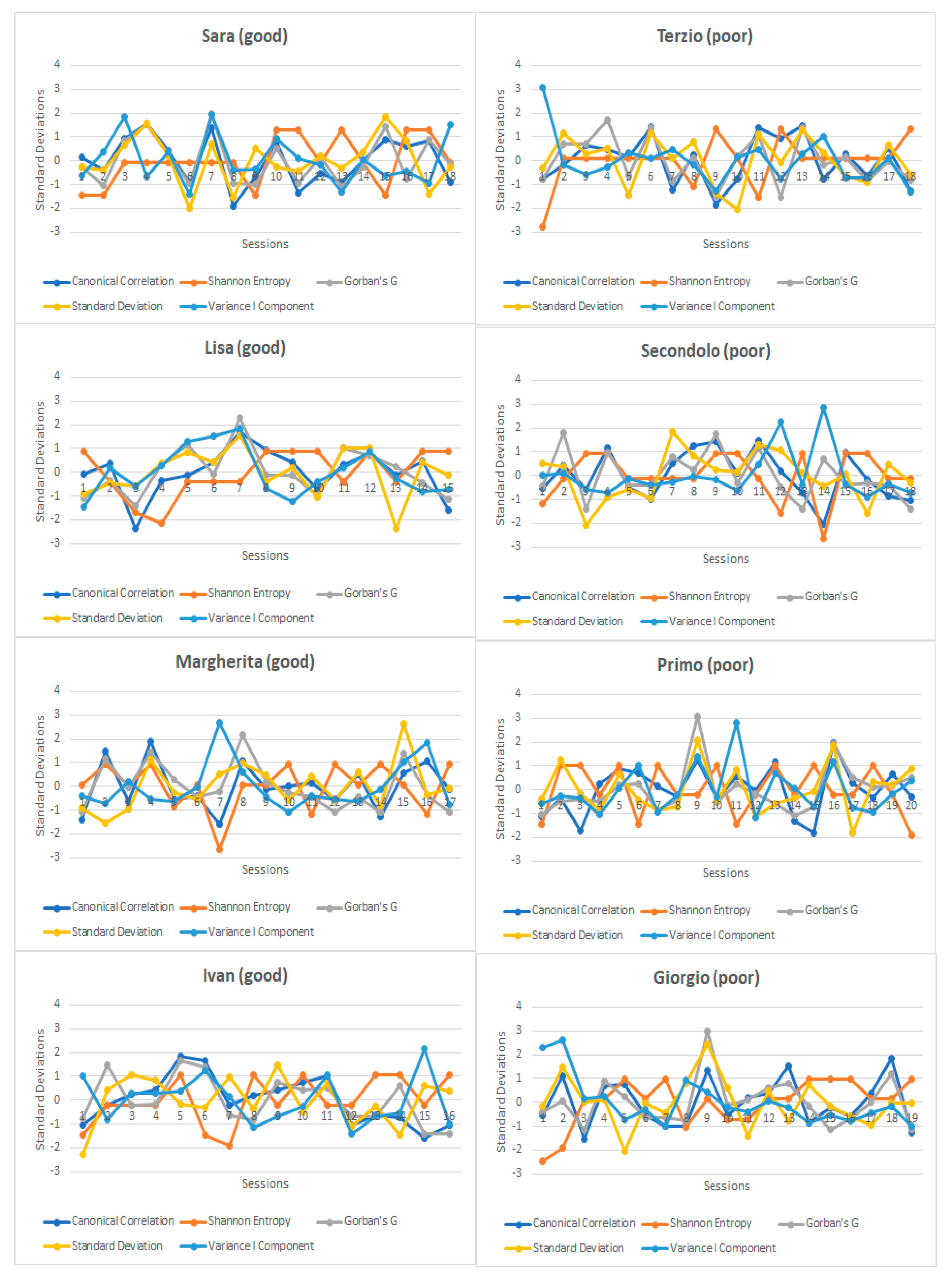
3.2. Dynamic Analyses
- Component 1: The higher the component score, the higher the relational consistency between therapist and patient (canonical correlation), its correlation robustness and variability. A dimension described with the polarities of order-variability.
- Component 2: The higher the component score, the higher the complexity of the system (the more negative the correlation with the amount of variance explained by the first component, the flatter the spectrum of eigenvalues). A dimension described with the polarities of elementary-complex.
- Component 3: The higher the component score, the higher the emergence of “low” and “high” correlation phases along the process.
4. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A
- (1)
- Canonical correlation coefficients between patient and therapist descriptors. Canonical Correlation is a way of inferring information from cross-covariance matrices. In the case we have two vectors X = (X1, …, Xn) and Y = (Y1, …, Ym) of random variables, and there are correlations among the variables, then canonical-correlation analysis finds linear combinations of the Xi and Yj which have maximum correlation with each other. Briefly, it measures the maximum interrelation between patient and therapist in a given time point. It is a “correlational-spectrum” analysis.
- (2)
- Percentage of explained variance by the first principal component. Very broadly used measure of order in a given system.
- (3)
- Sum of Pearson correlation coefficients higher than |0.25|. It turned out to be very effective in measuring the system’s robustness and in predicting change and crises in economics [2].
- (4)
- Standard deviation of Pearson coefficients. The 2nd and 3rd are measures of order: the higher the measures (i.e., “% of Explained Variance” and “Gorban’s G”), the more robust and connected the system’s network. This (i.e., “Standard Deviation”), on the other hand, is a measure of dispersion. The higher the standard deviation, the more variable and flexible the system’s network. The literature identifies extreme rigid or flexible network as dysfunctional systems.
- (5)
- Shannon Entropy on Eigenvalues. A commonly used measure of system order/disorder. A negative peak indicates a peak of system order and vice versa. It is a measure of “flatness” of the scree plot once a Principal Component Analysis is performed. A negative peak, on the other hand, indicates a steep slope on the scree plot [3].

References
- Hill, T.L. An Introduction to Statistical Thermodynamics; Courier Corporation: Chelmsford, MA, USA, 1986. [Google Scholar]
- Gorban, A.N.; Smirnova, E.V.; Tyukina, T.A. Correlations, risk and crisis: From physiology to finance. Phys. A Stat. Mech. Appl. 2010, 389, 3193–3217. [Google Scholar] [CrossRef]
- Sabatini, A.M. Analysis of postural sway using entropy measures of signal complexity. Med. Biol. Eng. Comput. 2000, 38, 617–624. [Google Scholar] [CrossRef] [PubMed]
- Scheffer, M.; Carpenter, S.R.; Lenton, T.M.; Bascompte, J.; Brock, W.; Dakos, V.; Van de Koppel, J.; Van de Leemput, I.A.; Levin, S.A.; Van Nes, E.H.; et al. Anticipating critical transitions. Science 2012, 338, 344–348. [Google Scholar] [CrossRef] [PubMed]
- Rybnikov, S.R.; Rybnikova, N.A.; Portnov, B.A. Public Fears in Ukrainian Society: Are Crises Predictable? Psychol. Dev. Soc. 2017, 29, 98–123. [Google Scholar] [CrossRef]
- Giuliani, A.; Tsuchiya, M.; Yoshikawa, L. Self-Organization of Genome Expression from Embryo to Terminal Cell Fate: Single-Cell Statistical Mechanics of Biological Regulations. Entropy 2018, 20, 13. [Google Scholar] [CrossRef]
- Mojtahedi, M.; Skupin, A.; Zhou, J.; Castano, I.G.; Leong-Quong, R.Y.; Chang, H.; Giuliani, A.; Huang, S. Cell fate-decision as high-dimensional critical state transition. PLoS Biol. 2016, 14, e2000640. [Google Scholar] [CrossRef]
- Pagani, M.; Giuliani, A.; Oberg, J.; Chincarini, A.; Morbelli, S.; Brugnolo, A.; Amaldi, D.; Picco, A.; Bauckneht, M.; Buschiazzo, A.; et al. Predicting the transition from normal aging to Alzheimer’s disease: A statistical mechanistic evaluation of FDG-PET data. NeuroImage 2016, 141, 282–290. [Google Scholar] [CrossRef]
- Giuliani, A.; Filippi, S.; Bertolaso, M. Why network approach can promote a new way of thinking in biology. Front. Genet. 2014, 5, 83. [Google Scholar] [CrossRef]
- Laughlin, R.; Pines, D.; Schmalian, J.; Stojković, B.; Wolynes, P. The middle way. Proc. Natl. Acad. Sci. USA 2000, 97, 32–37. [Google Scholar] [CrossRef]
- Schiepek, G.; Strunk, G. The identification of critical fluctuations and phase transitions in short term and coarse-grained time series—A method for the real-time monitoring of human change processes. Biol. Cybern. 2010, 102, 197–207. [Google Scholar] [CrossRef]
- Gelo, O.C.G.; Salvatore, S. A dynamic systems approach to psychotherapy: A meta-theoretical framework for explaining psychotherapy change processes. J. Couns. Psychol. 2016, 63, 379–395. [Google Scholar] [CrossRef] [PubMed]
- Gumz, A.; Bauer, K.; Brähler, E. Corresponding instability of patient and therapist process ratings in psychodynamic psychotherapies. Psychother. Res. 2012, 22, 26–39. [Google Scholar] [CrossRef]
- Watson, J.C.; Greenberg, L.S.; Lietaer, G. The experiential paradigm unfolding: Relationship & experiencing in therapy. In Handbook of Experiential Psychotherapy; Greenberg, L.S., Watson, J.C., Lietaer, G., Eds.; Guilford Press: New York, NY, USA, 1998; pp. 3–27. [Google Scholar]
- Tschacher, W.; Ramseyer, F. Modelling psychotherapy process by time-series panel analysis (TSPA). Psychother. Res. 2009, 19, 469–481. [Google Scholar] [CrossRef] [PubMed]
- Gelo, O.; Ramseyer, F.; Mergenthaler, E.; Tschacher, W. Verbal coordination between patient and therapist speech: Hints for psychotherapy process research. In Annual Meeting of the Society for Psychotherapy Research; Ulmer Textbank: Ulm, Germany, 2008; pp. 90–91. [Google Scholar]
- Gumz, A.; Kästner, D.; Geyer, M.; Wutzler, U.; Villmann, T.; Brähler, E. Instability and discontinuous change in the experience of therapeutic interaction: An extended single-case study of psychodynamic therapy processes. Psychother. Res. 2010, 20, 398–412. [Google Scholar] [CrossRef]
- Jacobson, N.S.; Truax, P. Clinical significance: A statistical approach defining meaningful change in psychotherapy research. J. Consult. Clin. Psychol. 1991, 59, 12–19. [Google Scholar] [CrossRef]
- Beck, A.T.; Steer, R.A.; Garbin, M.G. Psychometric properties of the Beck Depression Inventory: Twenty-five years of evaluation. Clin. Psychol. Rev. 1988, 8, 77–100. [Google Scholar] [CrossRef]
- Mendes, I.; Ribeiro, A.P.; Angus, L.; Greenberg, L.S.; Sousa, I.; Gonçalves, M.M. Narrative change in emotion-focused therapy: How is change constructed through the lens of the innovative moments coding system? Psychother. Res. 2010, 20, 692–701. [Google Scholar] [CrossRef]
- Spitzer, R.; Williams, J.; Gibbons, M.; First, M. Structured Clinical Interview for DSM-III-R; American Psychiatric Association: Washington, DC, USA, 1989. [Google Scholar]
- Greenberg, L.; Rice, L.; Watson, J. Manual for Client-Centered Therapy; York University: Toronto, ON, Canada, 1994. [Google Scholar]
- Mergenthaler, E. Emotion-abstraction patterns in verbatim protocols: A new way of describing psychotherapeutic processes. J. Consult. Clin. Psychol. 1996, 64, 1306–1315. [Google Scholar] [CrossRef]
- Mergenthaler, E. Resonating minds: A school-independent theoretical conception and its empirical application to psychotherapeutic processes. Psychother. Res. 2008, 18, 109–126. [Google Scholar] [CrossRef]
- Mergenthaler, E. The Cycles Model (CM) Software; University of Ulm: Ulm, Germany, 2011. [Google Scholar]
- Jolliffe, I.T.; Cadima, J. Principal component analysis: A review and recent developments. Philos. Trans. R. Soc. A Math. Phys. Eng. Sci. 2016, 374, 20150202. [Google Scholar] [CrossRef]
- Giuliani, A.; Ghirardi, O.; Caprioli, A.; Di Serio, S.; Ramacci, M.T.; Angelucci, L. Multivariate Analysis of behavioral aging highlights some unexpected features of complex systems organization. Behav. Neural Biol. 1994, 61, 110–122. [Google Scholar] [CrossRef]
- Orsucci, F.F.; Musmeci, N.; Aas, B.; Schiepek, G.; Reda, M.A.; Canestri, L.; Giuliani, A.; de Felice, G. Synchronization analysis of language and physiology in human dyads. Nonlinear Dyn. Psychol. Life Sci. 2016, 20, 167–191. [Google Scholar]
- Halfon, S.; Çavdar, A.; Orsucci, F.; Schiepek, G.K.; Andreassi, S.; Giuliani, A.; de Felice, G. The non-linear trajectory of change in play profiles of three children in psychodynamic play therapy. Front. Psychol. 2016, 7, 1494. [Google Scholar] [CrossRef]
- Guastello, S.J.; Koopmans, M.; Pincus, D. Chaos and Complexity in Psychology; Cambridge University: Cambridge, UK, 2009. [Google Scholar]
- Orsucci, F.F. Human Dynamics: A Complexity Science Open Handbook; Nova Science Publishers, Incorporated: Hauppauge, NY, USA, 2015. [Google Scholar]

{kind=link}
| Component | PCA Good-Outcome Cases. Eigenvalues, % of Variance Explained. | PCA Poor-Outcome Cases. Eigenvalues, % of Variance Explained. |
|---|---|---|
| 1 | 23.192 | 20.742 |
| 2 | 18.112 | 18.303 |
| 3 | 17.114 | 16.896 |
| 4 | 15.707 | 15.752 |
| 5 | 14.393 | 15.360 |
| 6 | 11.482 | 12.947 |
| Components PCA (c) | Good-comp1 | Good-comp2 | Good-comp3 | Good-comp4 | Good-comp5 | Good-comp6 | Poor-comp1 | Poor-comp2 | Poor-comp3 | Poor-comp4 | Poor-comp5 | Poor-comp6 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 0.991 ** | 0.008 | 0.003 | 0.004 | 0.012 | 0.004 | 0.088 ** | 0.127 ** | −0.015 | 0.025 | −0.010 | 0.081 ** |
| 2 | 0.075 ** | −0.029 | −0.010 | 0.045 ** | −0.008 | −0.051 ** | 0.995 ** | 0.020 | −0.006 | 0.014 | −0.006 | 0.015 |
| 3 | −0.070 ** | 0.710 ** | 0.015 | 0.055 ** | 0.058 ** | −0.011 | 0.013 | 0.694 ** | 0.143 ** | −0.137 ** | 0.063 ** | −0.024 |
| 4 | −0.076 ** | −0.568 ** | −0.194 ** | 0.201 ** | 0.067 ** | −0.012 | −0.033 * | 0.658 ** | −0.341 ** | 0.200 ** | −0.051 ** | 0.023 |
| 5 | −0.015 | −0.254 ** | 0.800 ** | 0.062 ** | −0.047 ** | −0.030 | −0.005 | 0.177 ** | 0.495 ** | 0.139 ** | −0.085 ** | 0.049 ** |
| 6 | −0.001 | 0.170 ** | 0.560 ** | 0.047 ** | 0.077 ** | 0.023 | 0.007 | −0.064 ** | −0.779 ** | −0.103 ** | 0.027 | 0.020 |
| 7 | −0.018 | 0.241 ** | −0.044 ** | 0.708 ** | −0.134 ** | −0.047 ** | −0.025 | −0.163 ** | −0.011 | 0.630 ** | −0.047 ** | 0.131 ** |
| 8 | 0.010 | −0.058 ** | 0.030 | −0.001 | 0.302 ** | 0.079 ** | 0.006 | −0.017 | 0.051 ** | 0.158 ** | 0.940 ** | −0.025 |
| 9 | −0.001 | 0.119 ** | 0.026 | −0.642 ** | −0.154 ** | −0.021 | 0.017 | 0.063 ** | −0.102 ** | 0.683 ** | −0.058 ** | −0.174 ** |
| 10 | 0.015 | 0.037 * | −0.021 | −0.002 | 0.914 ** | −0.030 | 0.005 | −0.068 ** | 0.058 ** | 0.144 ** | −0.307 ** | −0.130 ** |
| 11 | −0.042 * | 0.024 | −0.027 | −0.174 ** | 0.103 ** | −0.274 ** | −0.006 | 0.005 | −0.008 | 0.037 * | 0.004 | 0.933 ** |
| 12 | −0.005 | 0.002 | −0.010 | −0.047 ** | 0.030 | 0.953 ** | 0.027 | 0.011 | 0.016 | 0.042 * | −0.069 ** | 0.238 ** |
| Control Variables (Good-comp2, 3 and 4) | AB Therapist (Good Cases) | POS Therapist (Good Cases) | NEG Therapist (Good Cases) | AB Patient (Good Cases) | POS Patient (Good Cases) | NEG Patient (Good Cases) |
| AB therapist | 1.000 | −0.259 ** | −0.460 ** | −0.463 ** | −0.114 ** | 0.780 ** |
| POS therapist | 1.000 | −0.541 ** | −0.714 ** | −0.183 ** | −0.583 ** | |
| NEG therapist | 1.000 | 0.918 ** | −0.346 ** | 0.186 ** | ||
| AB patient | 1.000 | 0.046 ** | 0.078 ** | |||
| POS patient | 1.000 | −0.473 ** | ||||
| NEG patient | 1.000 | |||||
| Control Variables (Poor-comp2, 3 and 4) | AB therapist (poor cases) | POS therapist (poor cases) | NEG therapist (poor cases) | AB patient (poor cases) | POS patient (poor cases) | NEG patient (poor cases) |
| AB therapist | 1.000 | −0.170 ** | −0.064 ** | −0.637 ** | −0.323 ** | 0.977 ** |
| POS therapist | 1.000 | −0.424 ** | 0.831 ** | −0.559 ** | −0.296 ** | |
| NEG therapist | 1.000 | −0.072 ** | −0.343 ** | 0.148 ** | ||
| AB patient | 1.000 | −0.418 ** | −0.680 ** | |||
| POS patient | 1.000 | −0.354 ** | ||||
| NEG patient | 1.000 |
| Component | Eigenvalue | Difference | Proportion | Cumulative |
| 1 | 2.36 | 0.73 | 0.47 | 0.47 |
| 2 | 1.62 | 1.11 | 0.32 | 0.79 |
| 3 | 0.50 | 0.21 | 0.10 | 0.89 |
| 4 | 0.29 | 0.08 | 0.05 | 0.95 |
| 5 | 0.21 | 0.04 | 1.00 | |
| Components’ Loadings | ||||
| Component 1 | Component 2 | Component 3 | ||
| Canonical Correlation | 0.77 | 0.46 | −0.31 | |
| Shannon Entropy | −0.30 | 0.86 | 0.11 | |
| Gorban’s G | 0.86 | 0.29 | −0.18 | |
| Standard Deviation | 0.79 | 0.05 | 0.60 | |
| Variance I Component | 0.52 | −0.75 | −0.08 | |
| The GLM Procedure | |||||
|---|---|---|---|---|---|
| Dependent Variable: Component 1 | |||||
| Source | DF | Sum of Squares | Mean Square | F Value | Pr > F |
| Model | 7 | 35.47 | 5.06 | 6.45 | <0.0001 |
| Error | 133 | 104.52 | 0.78 | ||
| Corrected Total | 140 | 140 | |||
| R-Square | Coeff. Var. | Root MSE | Mean Component 1 | ||
| 0.25 | −5.4 × 1014 | 0.88 | 0 | ||
| Dependent Variable: Component 2 | |||||
| Source | DF | Sum of Squares | Mean Square | F Value | Pr > F |
| Model | 7 | 17.79 | 2.54 | 2.77 | 0.010 |
| Error | 133 | 122.21 | 0.91 | ||
| Corrected Total | 140 | 140 | |||
| R-Square | Coeff. Var. | Root MSE | Mean Component 2 | ||
| 0.12 | −4.47 × 1015 | 0.95 | 0 | ||
| Dependent Variable: Component 3 | |||||
| Source | DF | Sum of Squares | Mean Square | F Value | Pr > F |
| Model | 7 | 8.47 | 1.21 | 1.22 | 0.29 |
| Error | 133 | 131.53 | 0.99 | ||
| Corrected Total | 140 | 140 | |||
| R-Square | Coeff. Var. | Root MSE | Mean Component 3 | ||
| 0.06 | −2.85 × 1015 | 0.99 | 0 | ||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
de Felice, G.; Orsucci, F.F.; Scozzari, A.; Gelo, O.; Serafini, G.; Andreassi, S.; Vegni, N.; Paoloni, G.; Lagetto, G.; Mergenthaler, E.; et al. What Differentiates Poor and Good Outcome Psychotherapy? A Statistical-Mechanics-Inspired Approach to Psychotherapy Research. Systems 2019, 7, 22. https://0-doi-org.brum.beds.ac.uk/10.3390/systems7020022
de Felice G, Orsucci FF, Scozzari A, Gelo O, Serafini G, Andreassi S, Vegni N, Paoloni G, Lagetto G, Mergenthaler E, et al. What Differentiates Poor and Good Outcome Psychotherapy? A Statistical-Mechanics-Inspired Approach to Psychotherapy Research. Systems. 2019; 7(2):22. https://0-doi-org.brum.beds.ac.uk/10.3390/systems7020022
Chicago/Turabian Stylede Felice, Giulio, Franco F. Orsucci, Andrea Scozzari, Omar Gelo, Gabriele Serafini, Silvia Andreassi, Nicoletta Vegni, Giulia Paoloni, Gloria Lagetto, Erhard Mergenthaler, and et al. 2019. "What Differentiates Poor and Good Outcome Psychotherapy? A Statistical-Mechanics-Inspired Approach to Psychotherapy Research" Systems 7, no. 2: 22. https://0-doi-org.brum.beds.ac.uk/10.3390/systems7020022