Effectiveness of the Early Response to COVID-19: Data Analysis and Modelling

 ,
,  ,
, 

Abstract
:1. Introduction
2. Results
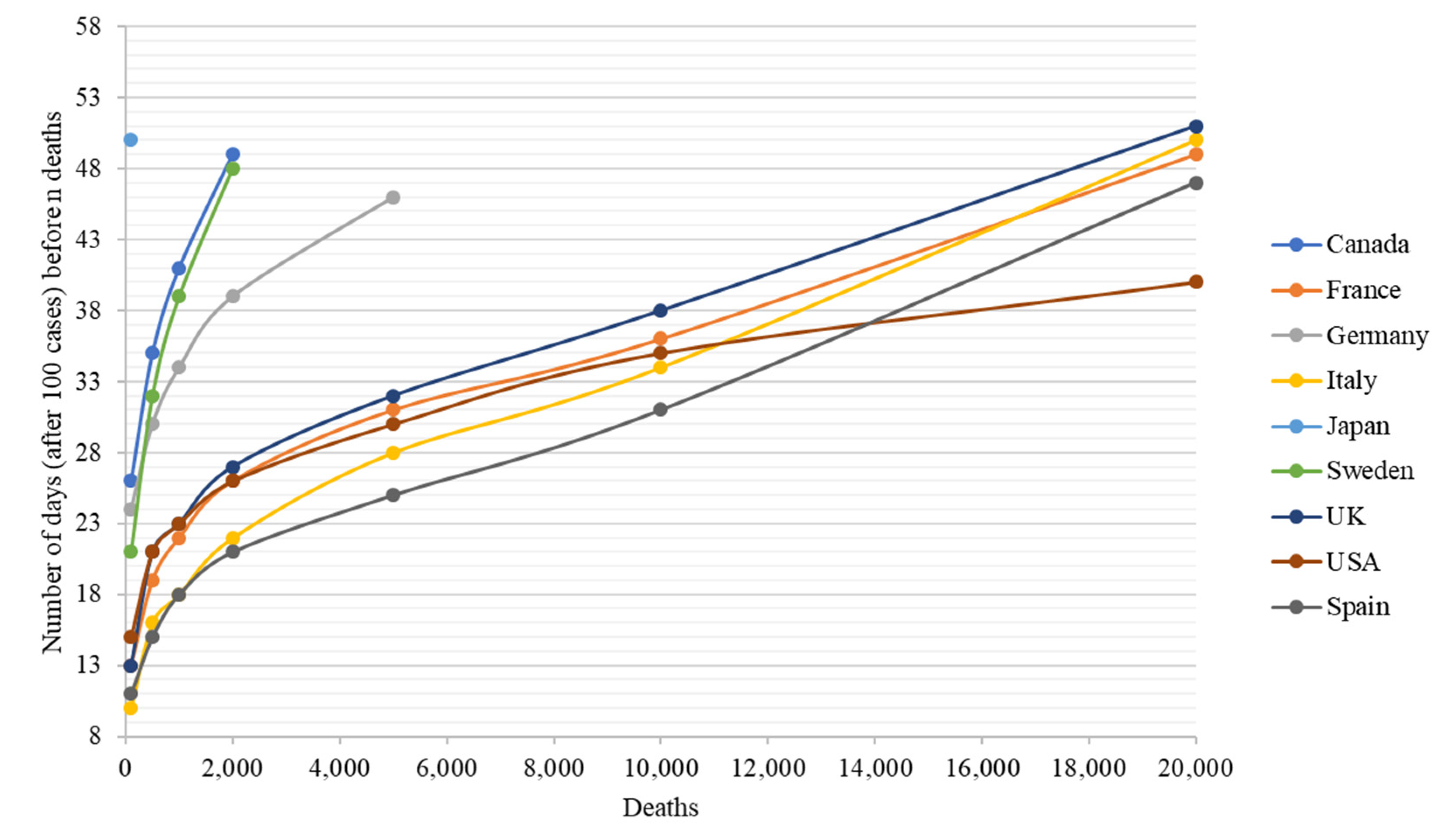
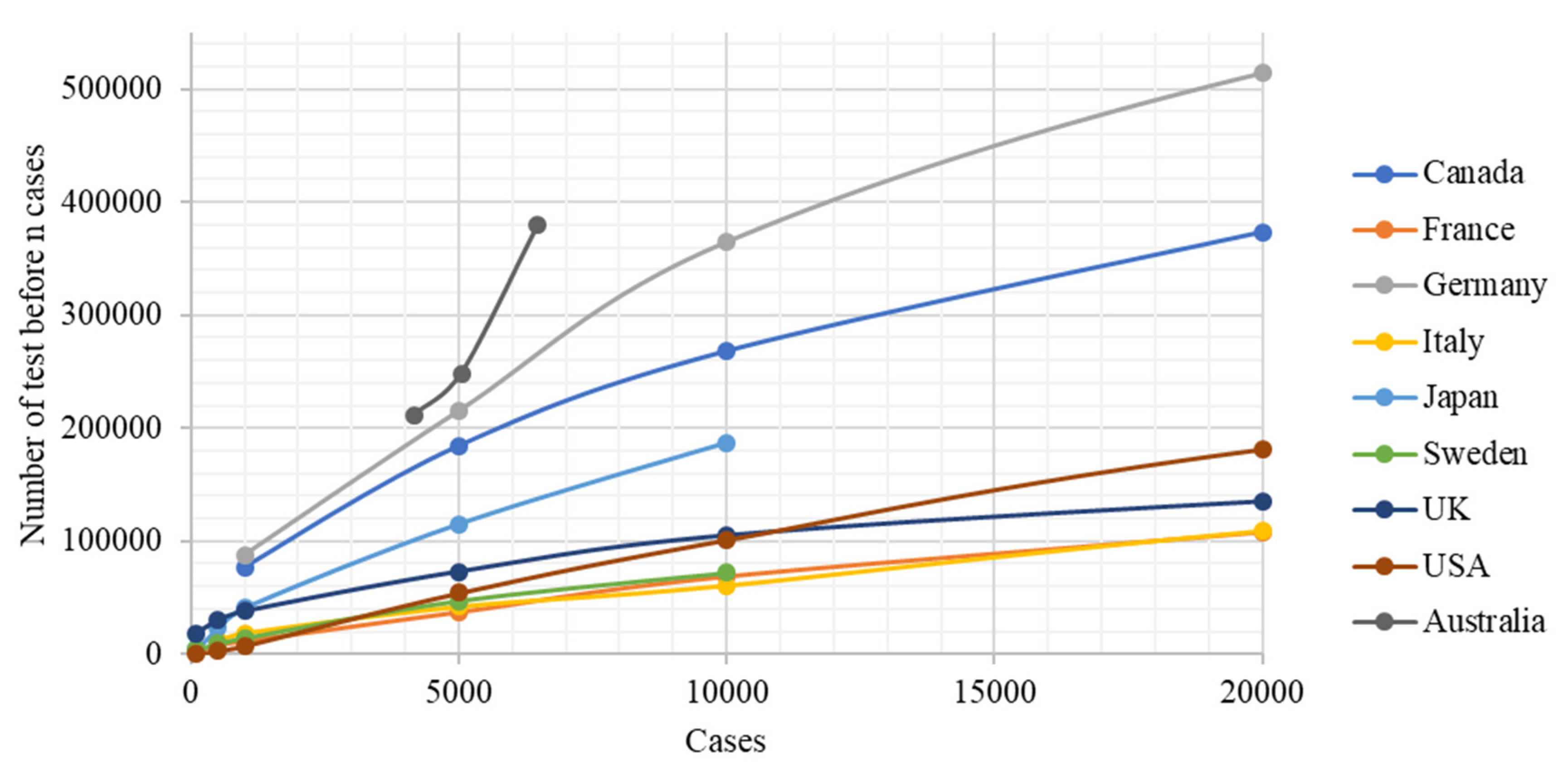
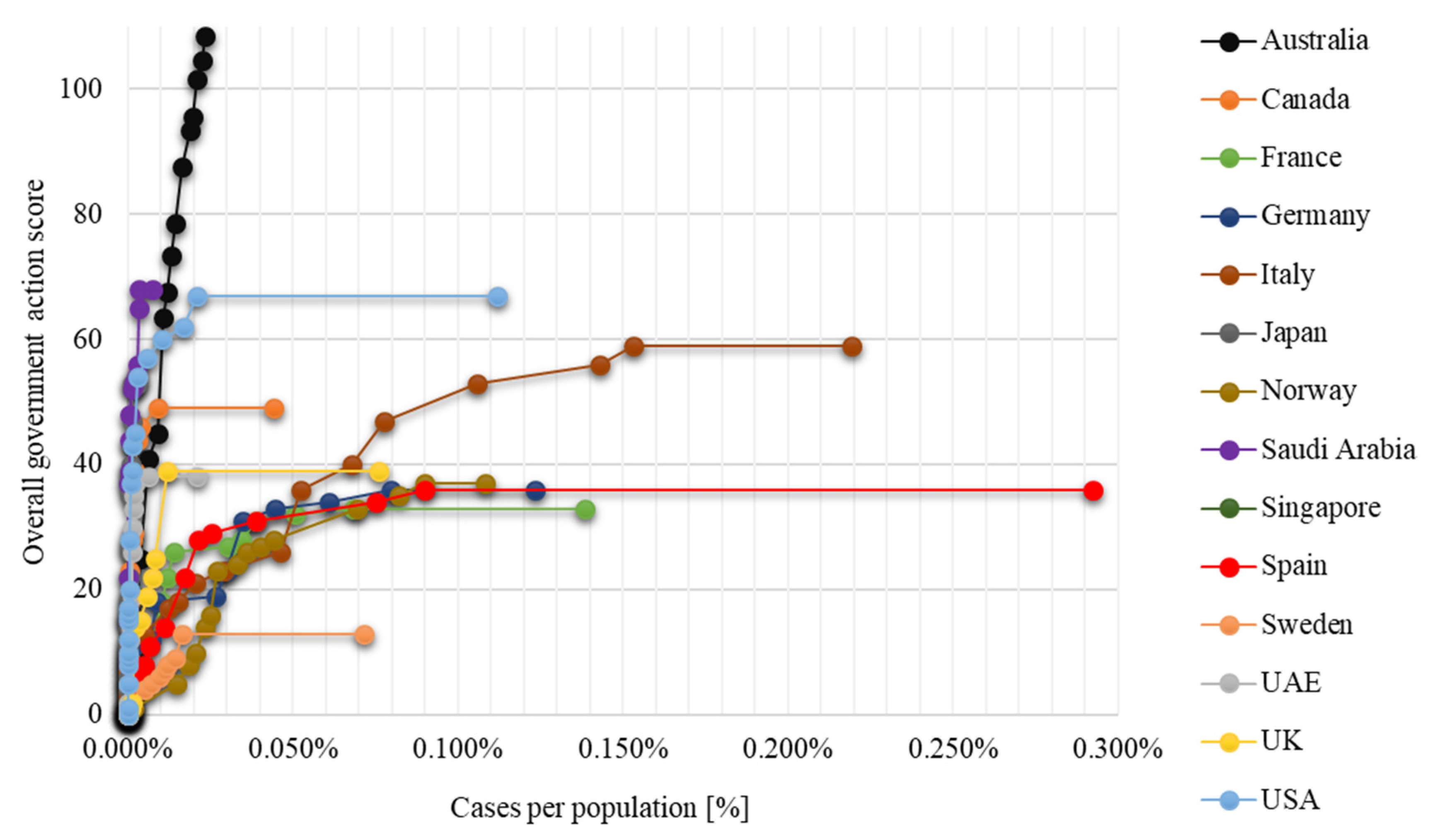
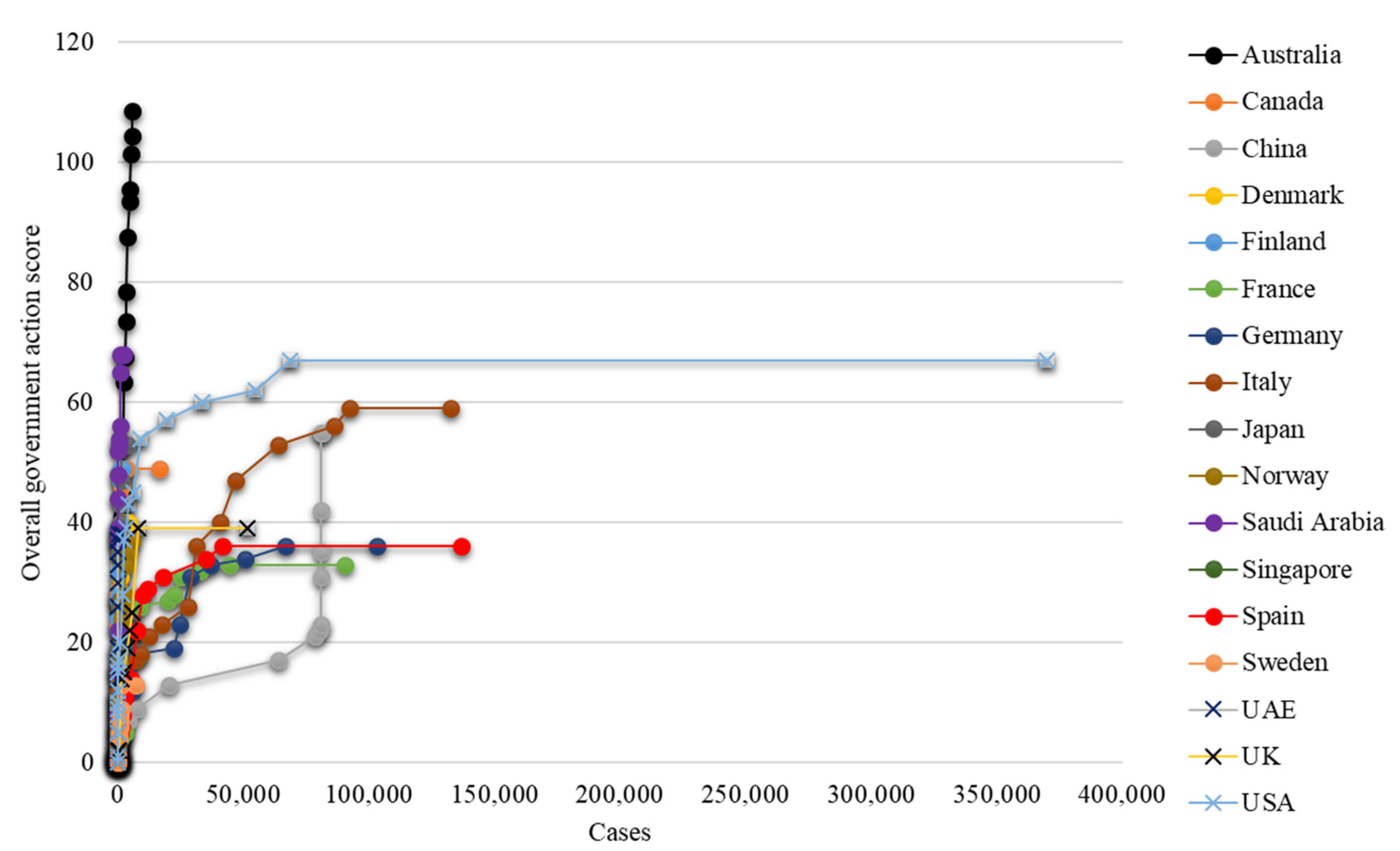
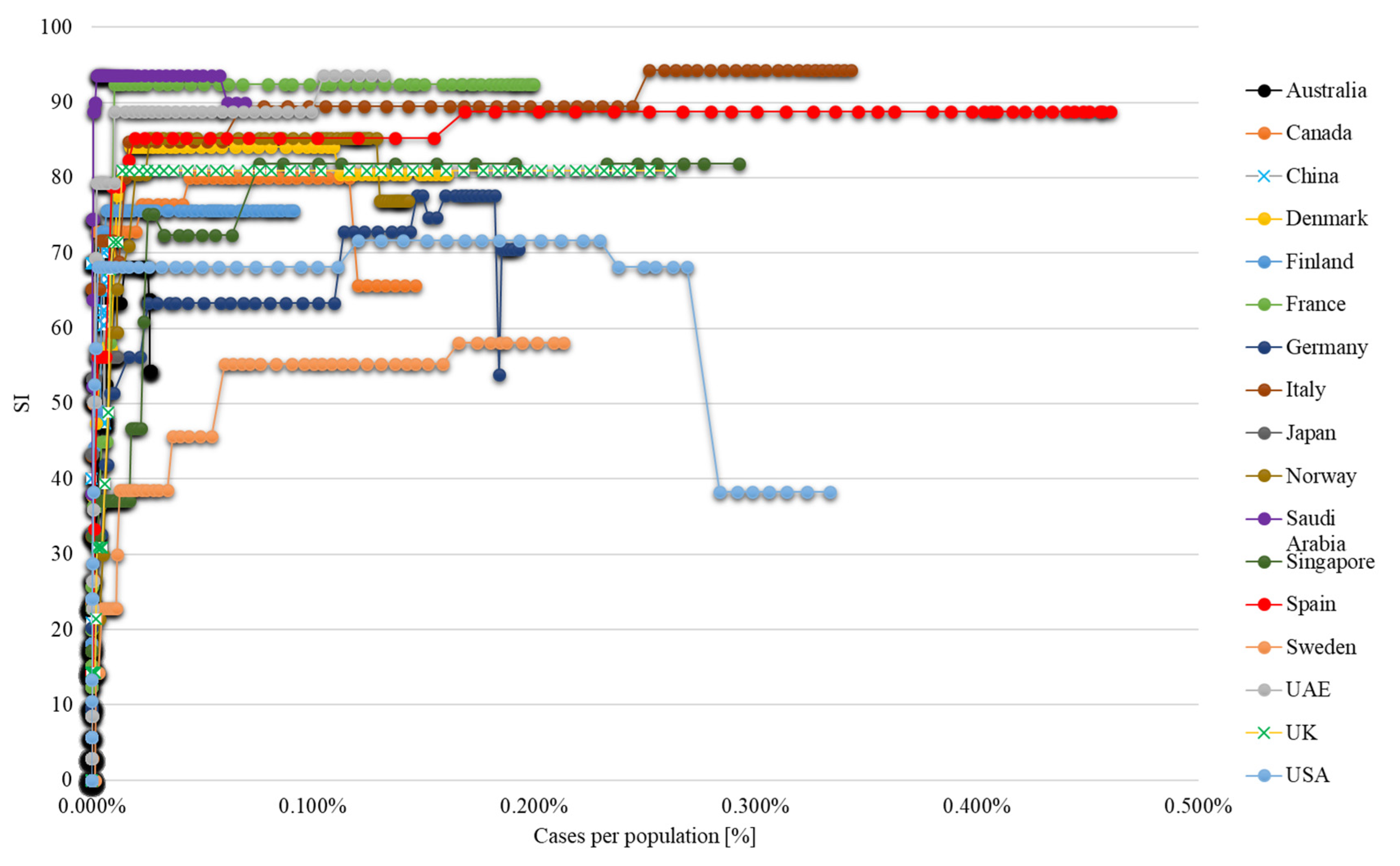
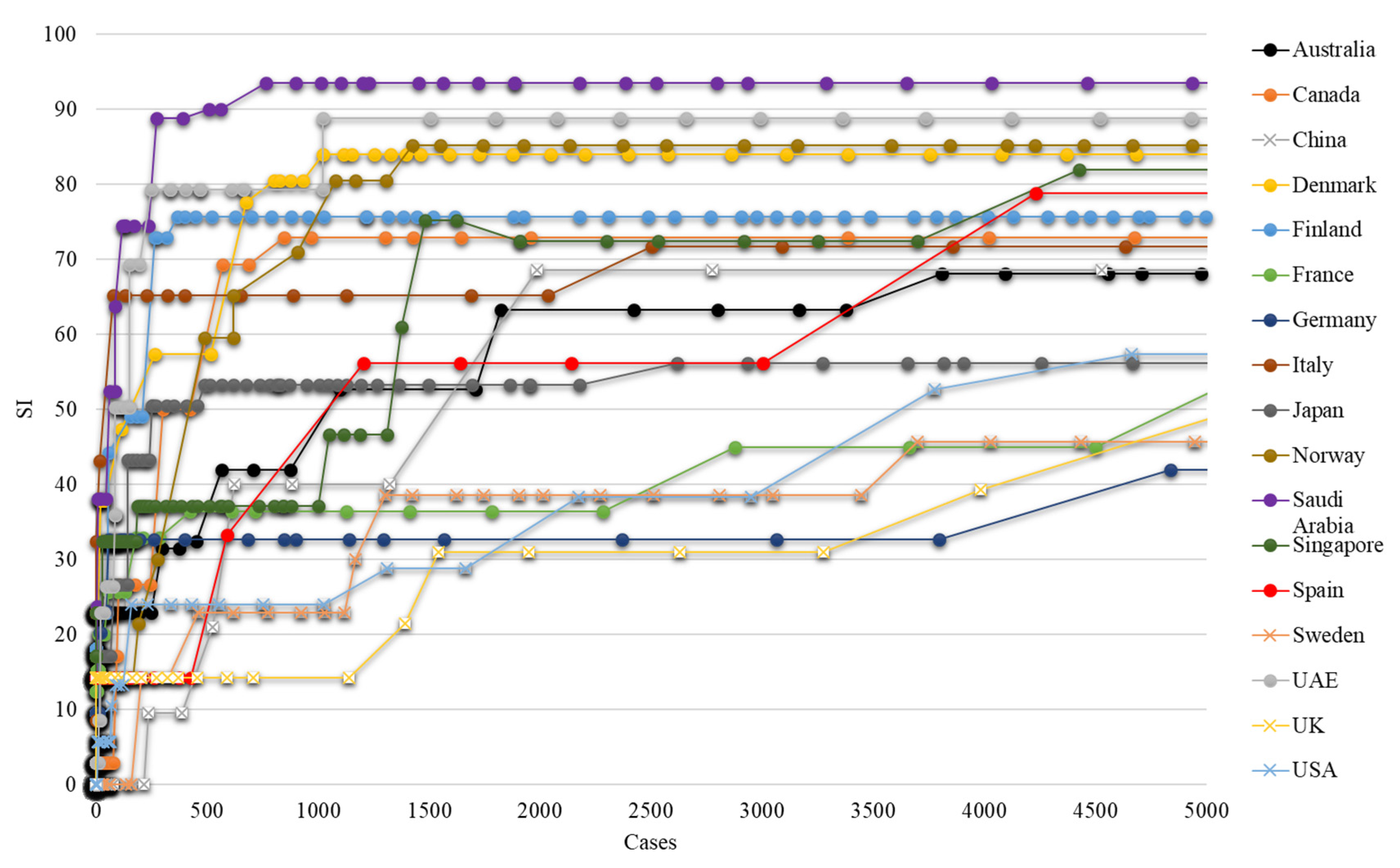
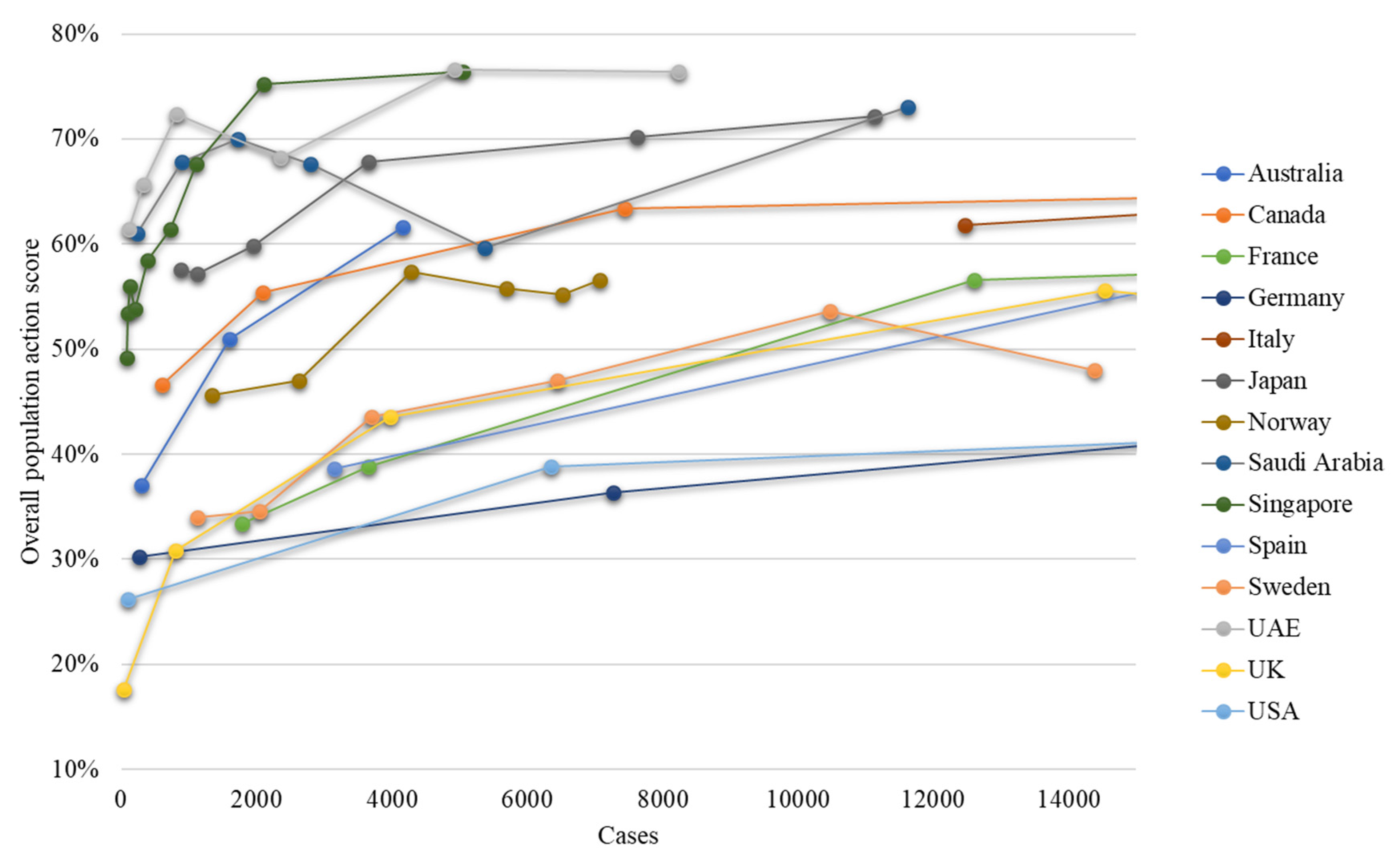
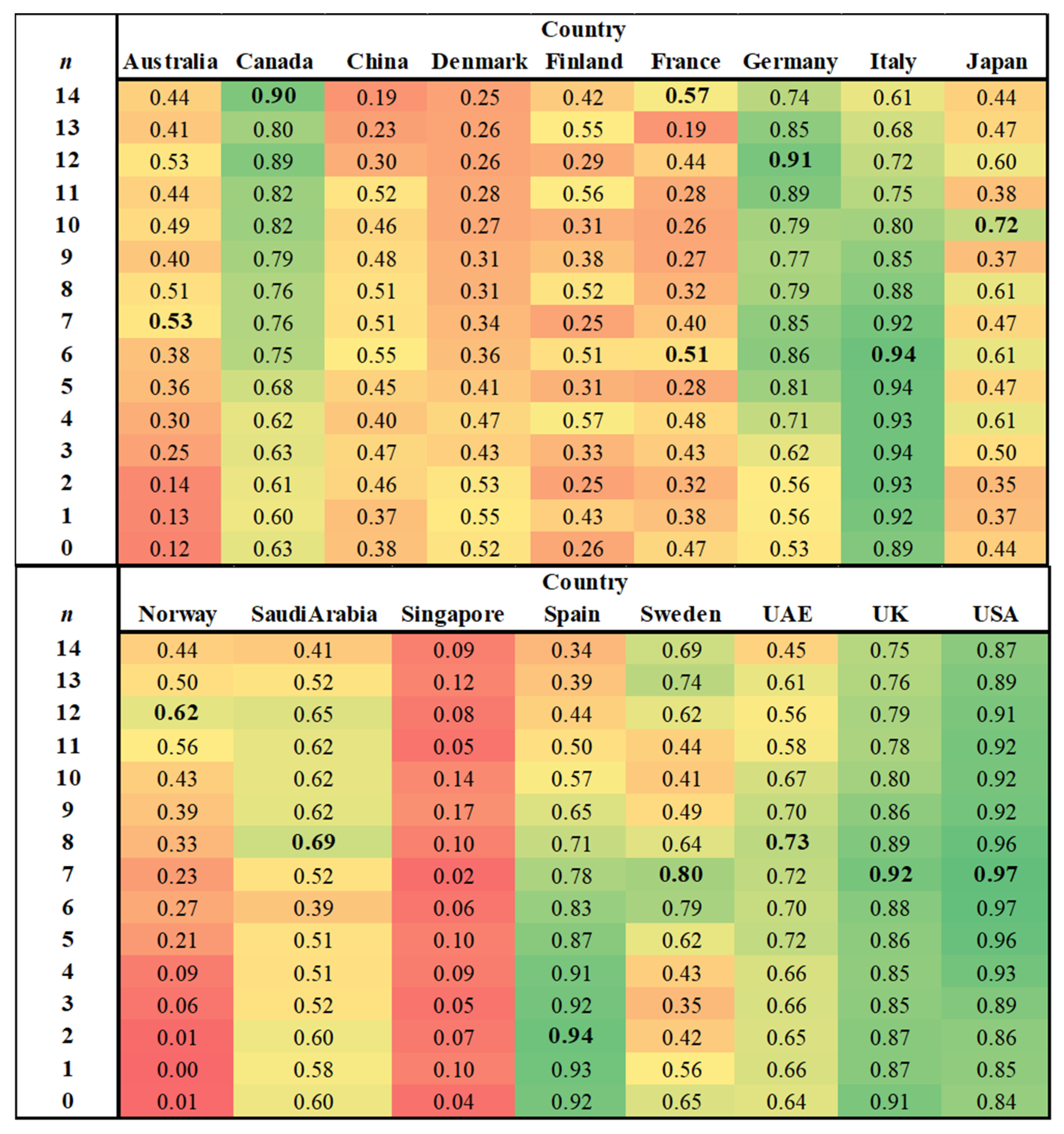
2.1. Data Analysis Outputs
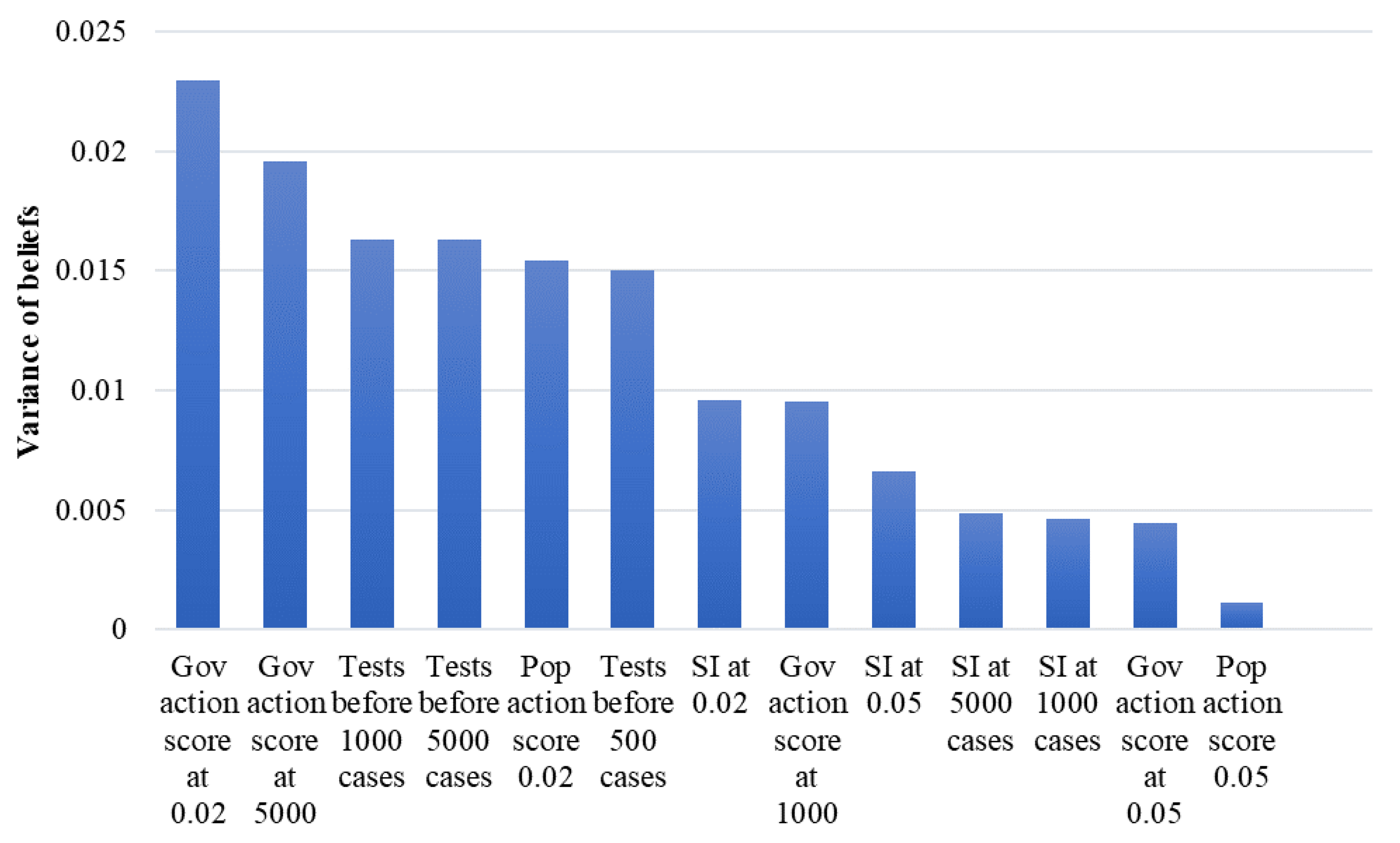
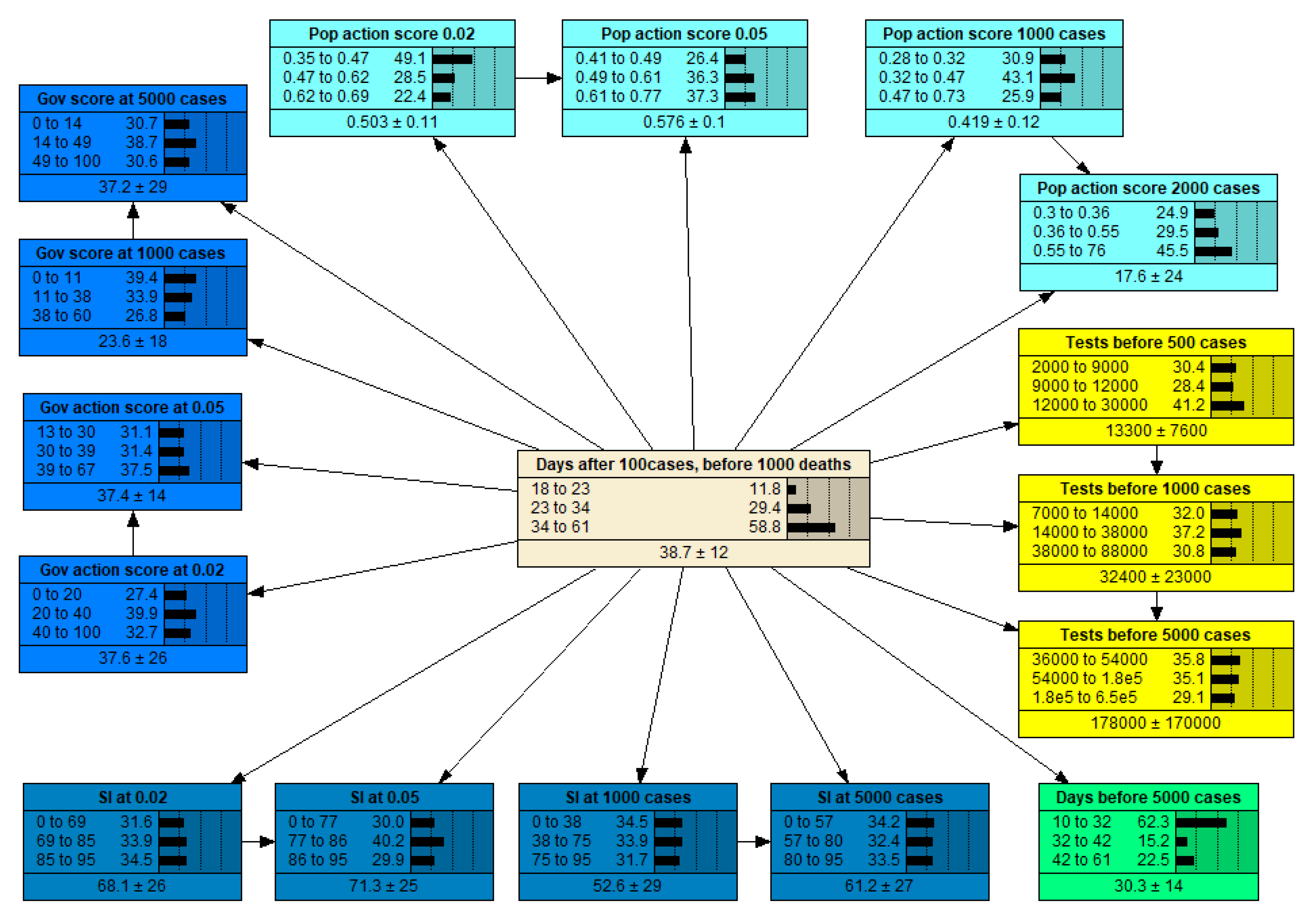
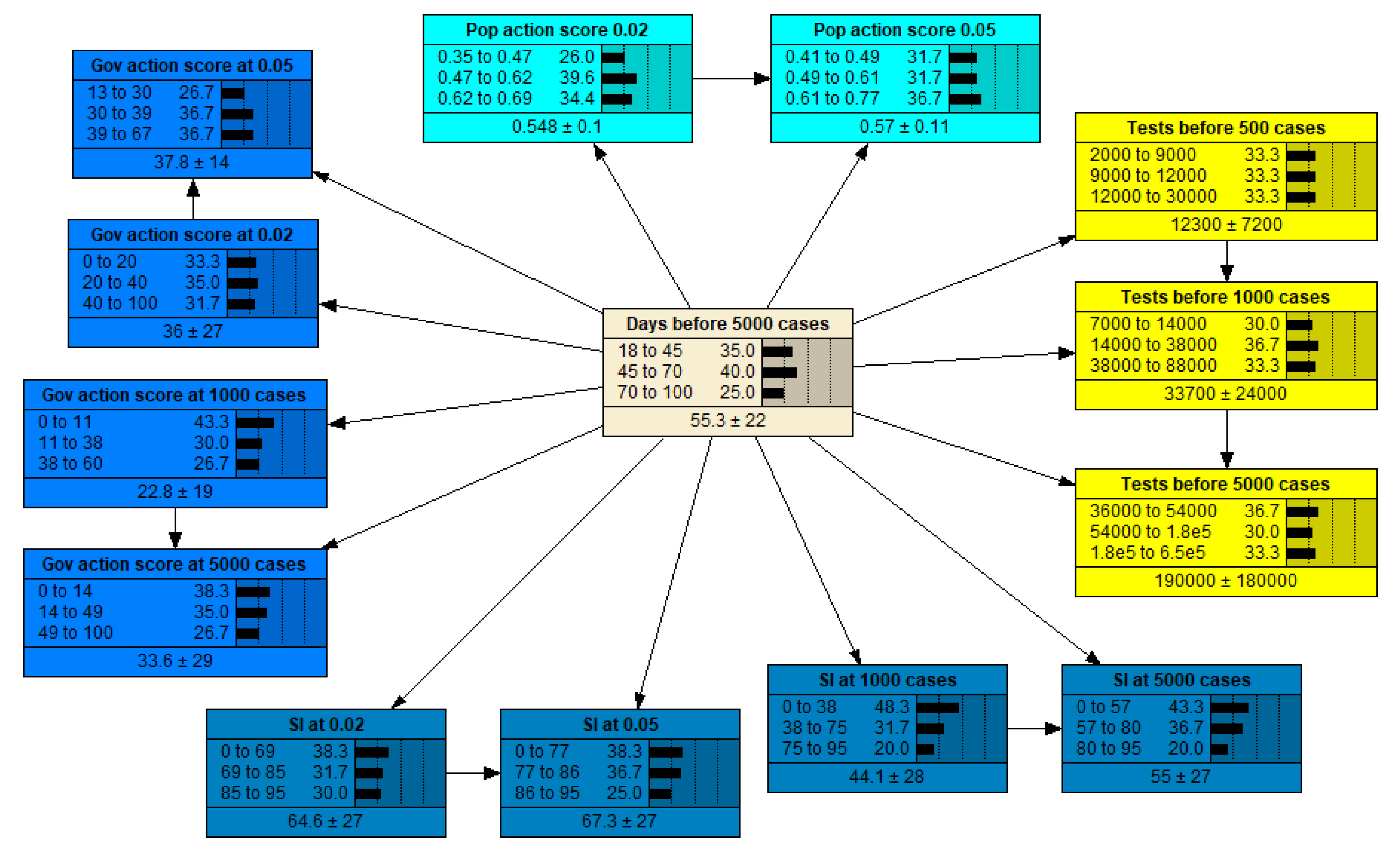
2.2. Bayesian Network Outputs
3. Discussion
4. Materials and Methods
4.1. Data Collection
4.2. Data Pre-Processing and Analysis
4.3. Model Development and Application
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A









References
- Gates, B. Responding to Covid-19—A once-in-a-century pandemic? N. Engl. J. Med. 2020, 382, 1677–1679. [Google Scholar] [CrossRef] [PubMed]
- Hoehl, S.; Rabenau, H.; Berger, A.; Kortenbusch, M.; Cinatl, J.; Bojkova, D.; Behrens, P.; Böddinghaus, B.; Götsch, U.; Naujoks, F.; et al. Evidence of SARS-CoV-2 infection in returning travelers from Wuhan, China. N. Engl. J. Med. 2020, 382, 1278–1280. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Pan, R.; Wan, X.; Tan, Y.; Xu, L.; Ho, C.S.; Ho, R.C. Immediate psychological responses and associated factors during the initial stage of the 2019 coronavirus disease (COVID-19) epidemic among the general population in China. Int. J. Environ. Res. Public Health 2020, 17, 1729. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brzezinski, A.; Deiana, G.; Kecht, V.; Van Dijcke, D. The COVID-19 Pandemic: Government vs. Community Action across the United States. Covid Econ. Vetted Real-Time P. 2020, 7, 115–156. [Google Scholar]
- Sterman, J.D. Business Dynamics: Systems Thinking and Modeling for a Complex World; The McGraw-Hill Companies: New York, NY, USA, 2000. [Google Scholar]
- Bertone, E.; Sahin, O.; Richards, R.; Roiko, A. Extreme events, water quality and health: A participatory Bayesian risk assessment tool for managers of reservoirs. J. Clean. Prod. 2016, 135, 657–667. [Google Scholar] [CrossRef] [Green Version]
- Bertone, E.; Sahin, O.; Stewart, R.A.; Zou, P.X.; Alam, M.; Hampson, K.; Blair, E. Role of financial mechanisms for accelerating the rate of water and energy efficiency retrofits in Australian public buildings: Hybrid Bayesian Network and System Dynamics modelling approach. Appl. Energy 2018, 210. [Google Scholar] [CrossRef] [Green Version]
- Sahin, O.; Suprun, E.; Richards, R.; Salim, H.; MacAskill, S.; Heilgeist, S.; Stewart, R.; Rutherford, S.; Beal, C. Navigating the Wicked Complexity of the COVID-19 Pandemic. Syst. Commun. 2020. accepted for publication. [Google Scholar]
- Fenton, N.; Neil, M. Risk Assessment and Decision Analysis with Bayesian Networks; CRC Press: New York, NY, USA, 2013. [Google Scholar]
- Hale, T.; Webster, S.; Petherick, A.; Phillips, T.; Kira, B. Oxford COVID-19 Government Response Tracker, Blavatnik School of Government. 2020. Available online: https://www.bsg.ox.ac.uk/research/research-projects/coronavirus-government-response-tracker (accessed on 5 June 2020).
- Hale, T.; Petherick, A.; Kira, B.; Angrist, N.; Phillips, T. Variation in Government Responses to COVID-19; BSG Working Paper Series; Blavatnik School of Government: Oxford, UK, 2020. [Google Scholar]
- Wilson, N.; Kvalsvig, A.; Barnard, L.T.; Baker, M. Estimating the Case Fatality Risk of COVID-19 using Cases from Outside China. medRxiv 2020. [Google Scholar] [CrossRef] [Green Version]
- Bendavid, E.; Mulaney, B.; Sood, N.; Shah, S.; Ling, E.; Bromley-Dulfano, R.; Lai, C.; Weissberg, Z.; Saavedra, R.; Tedrow, J.; et al. COVID-19 Antibody Seroprevalence in Santa Clara County, California. medRxiv 2020. [Google Scholar] [CrossRef]
- Volpato, S.; Landi, F.; Incalzi, R.A. Frail Health Care System for an Old Population: Lesson form the COVID-19 Outbreak in Italy. J. Gerontol. Ser. A 2020. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pueyo, T. Coronavirus: The Hammer and the Dance. Available online: https://medium.com/@tomaspueyo/coronavirus-the-hammer-and-the-dance-be9337092b56 (accessed on 5 May 2020).
- Hensvik, L.; Skans, O. COVID-19 Crisis Response Monitoring; IZA Institute of Labor Economics: Bonn, Germany, 2020. [Google Scholar]
- Wang, J.; Tang, K.; Feng, K.; Lv, W. High temperature and high humidity reduce the transmission of COVID-19. SSRN 2020. [Google Scholar] [CrossRef] [Green Version]
- Rocklöv, J.; Sjödin, H. High population densities catalyse the spread of COVID-19. J. Travel Med. 2020, 27. [Google Scholar] [CrossRef] [PubMed]
- YouGov. YouGov International COVID-19 Tracker. 2020. Available online: https://yougov.co.uk/topics/international/articles-reports/2020/03/17/YouGov-international-COVID-19-tracker (accessed on 5 June 2020).
- Acaps. #COVID19 Government Measures Dataset. 2020. Available online: https://www.acaps.org/covid19-government-measures-dataset (accessed on 5 June 2020).
- Bayes, M.; Price, M. An essay towards solving a problem in the doctrine of chances. By the late Rev. Mr. Bayes, F.R.S. communicated by Mr. Price, in a letter to John Canton, A.M.F.R.S. Philos. Trans. 1763, 53, 370–418. [Google Scholar]
- Chen, S.; Pollino, C. Good practice in Bayesian network modelling. Environ. Model. Softw. 2012, 37, 134–145. [Google Scholar] [CrossRef]
- Uusitalo, L. Advantages and challenges of Bayesian networks in environmental modelling. Ecol. Model. 2007, 203, 312–318. [Google Scholar] [CrossRef]
- Langarizadeh, M.; Moghbeli, F. Applying naive bayesian networks to disease prediction: A systematic review. Acta Inform. Med. 2016, 24, 364. [Google Scholar] [CrossRef] [PubMed]
- Solares, C.; Sanz, A.M. Different Bayesian network models in the classification of remote sensing images. In Proceedings of the Intelligent Data Engineering and Automated Learning-IDEAL 2007, Birmingham, UK, 16–19 December 2007. [Google Scholar]
- Friedman, N.; Geiger, D.; Goldszmidt, M. Bayesian network classifiers. Mach. Learn. 1997, 29, 131–163. [Google Scholar] [CrossRef] [Green Version]
- Norsys. Netica APIs (Application Programmer Interfaces). Available online: https://www.norsys.com/netica_api.html (accessed on 6 March 2020).
- Neapolitan, R. Probabilistic Reasoning in Expert Systems: Theory and Algorithms; John Wiley: New York, NY, USA, 1990. [Google Scholar]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Country | Days Before 10,000 Deaths | Early ICU | Early Gov Action | Early SI | Early Pop Action | Early Testing | Lag to Death |
|---|---|---|---|---|---|---|---|
| (R2) | |||||||
| Australia | L | H | M | L but + | H | 7 (0.53) | |
| Canada | M | H | H | M | H | 14 (0.9) | |
| France | 36 | H | L | M | L | L | 6, 14 (~0.5) |
| Germany | L | L | L | L | H | 12 (0.91) | |
| Italy | 34 | H | L | H | H | L | 6 (0.94) |
| Japan | M | L but + | M | H | M | 10 (0.71) | |
| Norway | M | M | L but + | L | 12 (0.62) | ||
| Saudi Arabia | H | H | H but − | 8 (0.69) | |||
| Spain | 31 | L | M | L | 2 (0.94) | ||
| Sweden | H | L | L | L | L | 7 (0.79) | |
| UAE | L | M | H | H | H | 8 (0.74) | |
| UK | 38 | H | M | M | L | L | 7 (0.92) |
| USA | 35 | L | H | M | L | L | 7 (0.97) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bertone, E.; Luna Juncal, M.J.; Prado Umeno, R.K.; Peixoto, D.A.; Nguyen, K.; Sahin, O. Effectiveness of the Early Response to COVID-19: Data Analysis and Modelling. Systems 2020, 8, 21. https://0-doi-org.brum.beds.ac.uk/10.3390/systems8020021
Bertone E, Luna Juncal MJ, Prado Umeno RK, Peixoto DA, Nguyen K, Sahin O. Effectiveness of the Early Response to COVID-19: Data Analysis and Modelling. Systems. 2020; 8(2):21. https://0-doi-org.brum.beds.ac.uk/10.3390/systems8020021
Chicago/Turabian StyleBertone, Edoardo, Martin Jason Luna Juncal, Rafaela Keiko Prado Umeno, Douglas Alves Peixoto, Khoi Nguyen, and Oz Sahin. 2020. "Effectiveness of the Early Response to COVID-19: Data Analysis and Modelling" Systems 8, no. 2: 21. https://0-doi-org.brum.beds.ac.uk/10.3390/systems8020021