
Blood and Salivary Inflammatory Biomarkers Profile in Patients with Chronic Kidney Disease and Periodontal Disease: A Systematic Review

 ,
,  , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Focal Question
2.2. Information Sources and Search Strategy
2.3. Inclusion and Exclusion Criteria
2.4. Study Selection
2.5. Data Extraction and Assessment of Bias
3. Results
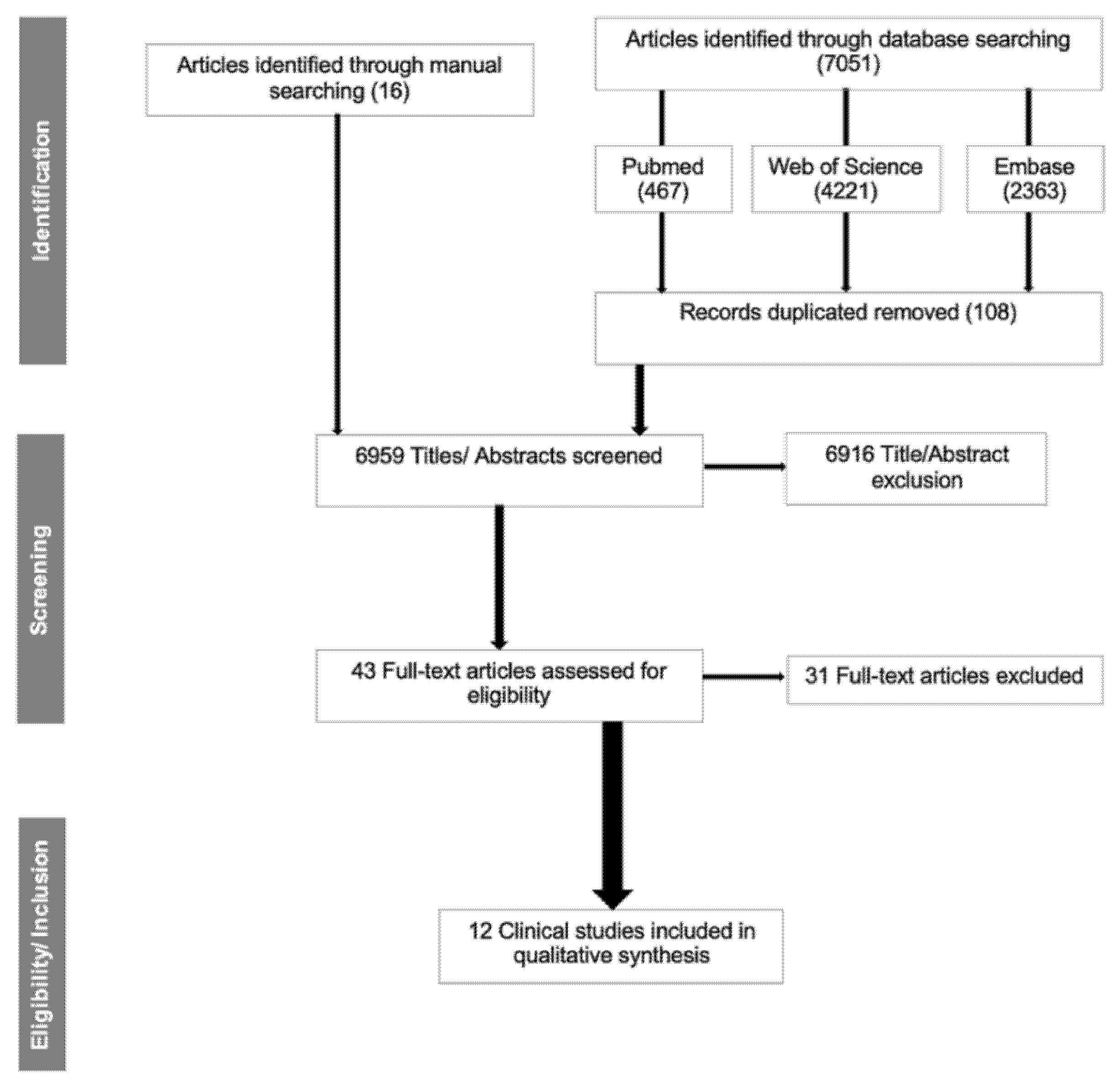
3.1. Study Selection
3.2. Study Characteristics
3.3. Chronic Kidney Disease (CKD) and Periodontal Disease
3.4. Biomarkers
3.5. Other Health Risk Factors (Smoking and Diabetes)
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Frazão, C.M.F.Q.; Delgado, M.F.; Araújo, M.G.A.; Silva, F.B.B.L.; Sá, J.D.; Lira, A.L.B.C. Nursing care for chronic renal patients on hemodialysis. Rev. Rene. 2014, 15, 701–709. [Google Scholar] [CrossRef]
- Schmalz, G.; Schiffers, N.; Schwabe, S.; Vasko, R.; Müller, G.A.; Haak, R.; Mausberg, R.F.; Ziebolz, D. Dental and periodontal health, and microbiological and salivary conditions in patients with or without diabetes undergoing haemodialysis. Int. Dent. J. 2017, 67, 186–193. [Google Scholar] [CrossRef] [PubMed]
- Altamimi, A.; AlBakr, S.; Alanazi, T.; Alshahrani, F.; Chalisserry, E.; Anil, S. Prevalence of Periodontitis in Patients Undergoing Hemodialysis: A Case Control Study. Mater. Sociomed. 2018, 30, 58–61. [Google Scholar] [CrossRef] [PubMed]
- Schmalz, G.; Kauffels, A.; Kollmar, O.; Slotta, J.E.; Vasko, R.; Müller, G.A.; Haak, R.; Ziebolz, D. Oral behavior, dental, periodontal and microbiological findings in patients undergoing hemodialysis and after kidney transplantation. BMC Oral Health 2016, 16, 72. [Google Scholar] [CrossRef]
- Bostanci, N.; Selevsek, N.; Wolski, W.; Grossmann, J.; Bao, K.; Wahlander, A.; Trachsel, C.; Schlapbach, R.; Öztürk, V.Ö.; Afacan, B.; et al. Targeted proteomics guided by label-free quantitative proteome analysis in saliva reveal transition signatures from health to periodontal disease. Mol. Cell. Proteom. 2018, 17, 1392–1409. [Google Scholar] [CrossRef]
- Ramirez, J.; Higuera, N.; Mancilla, M.; Coronilla, G.; Bustamante, J.; López, A. Use of Biomarkers for the Diagnosis of Periodontitis. In Periodontal Disease-Diagnostic and Adjunctive Non-Surgical Considerations; IntechOpen: London, UK, 2019; pp. 1–21. [Google Scholar]
- Kaczor-Urbanowicz, K.E.; Martin Carreras-Presas, C.; Aro, K.; Tu, M.; Garcia-Godoy, F.; Wong, D.T.W. Saliva diagnostics—Current views and directions. Exp. Biol. Med. 2017, 242, 459–472. [Google Scholar] [CrossRef]
- Tomás, I.; Marinho, J.S.; Limeres, J.; Santos, M.J.; Araújo, L.; Diz, P. Changes in salivary composition in patients with renal failure. Arch. Oral Biol. 2008, 53, 528–532. [Google Scholar] [CrossRef]
- Donato, H.; Donato, M. Stages for undertaking a systematic review. Acta Med. Port. 2019, 32, 227–235. [Google Scholar] [CrossRef]
- Poli, F.E.; Gulsin, G.S.; McCann, G.P.; Burton, J.O.; Graham-Brown, M.P. The assessment of coronary artery disease in patients with end-stage renal disease. Clin. Kidney J. 2019, 12, 721–734. [Google Scholar] [CrossRef]
- Prasad, S.; Tyagi, A.K.; Aggarwal, B.B. Detection of inflammatory biomarkers in saliva and urine: Potential in diagnosis, prevention, and treatment for chronic diseases. Exp. Biol. Med. 2016, 241, 783–799. [Google Scholar] [CrossRef]
- Klassen, J.T.; Krasko, B.M. The dental health status of dialysis patients. J. Can. Dent. Assoc. 2002, 68, 34–38. [Google Scholar] [PubMed]
- Duran, I.; Erdemir, E.O. Periodontal treatment needs of patients with renal disease receiving haemodialysis. Int. Dent. J. 2004, 54, 274–278. [Google Scholar] [CrossRef] [PubMed]
- Souza, C.R.; Liberio, S.A.; Guerra, R.N.; Monteiro, S.; Silveira, E.J.; Pereira, A.L. Assessment of periodontal condition of kidney patients in hemodialysis. Rev. Assoc. Med. Bras. 2005, 51, 285–289. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.P.; Chiang, C.K.; Chan, C.P.; Hung, K.Y.; Huang, C.S. Does periodontitis reflect inflammation and malnutrition status in hemodialysis patients? Am. J. Kidney Dis. 2006, 47, 815–822. [Google Scholar] [CrossRef] [PubMed]
- Craig, R.G. Interactions between chronic renal disease and periodontal disease. Oral Dis. 2008, 14, 1–7. [Google Scholar] [CrossRef]
- Kinney, J.S.; Morelli, T.; Braun, T.; Ramseier, C.A.; Herr, A.E.; Sugai, J.V.; Shelburne, C.E.; Rayburn, L.A.; Singh, A.K.; Giannobile, W.V. Saliva/Pathogen Biomarker Signatures and Periodontal Disease Progressio. J. Dent. Res. 2011, 90, 752–758. [Google Scholar] [CrossRef] [PubMed]
- Malamud, D. Saliva as a Diagnostic Fluid. Dent. Clin. N. Am. 2011, 55, 159–178. [Google Scholar] [CrossRef]
- Siddaway, A.P.; Wood, A.M.; Hedges, L.V. How to Do a Systematic Review: A Best Practice Guide for Conducting and Reporting Narrative Reviews, Meta-Analyses, and Meta-Syntheses. Annu. Rev. Psychol. 2018, 70, 747–770. [Google Scholar] [CrossRef]
- Celec, P.; Tóthová, L.; Šebeková, K.; Podracká, L.; Boor, P. Salivary markers of kidney function—Potentials and limitations. Clin. Chim. Acta 2016, 453, 28–37. [Google Scholar] [CrossRef]
- Maciejczyk, M.; Szulimowska, J.; Skutnik, A.; Taranta-Janusz, K.; Wasilewska, A.; Wiśniewska, N.; Zalewska, A. Salivary Biomarkers of Oxidative Stress in Children with Chronic Kidney Disease. J. Clin. Med. 2018, 7, 209. [Google Scholar] [CrossRef]
- Kim, J.J.; Kim, C.J.; Camargo, P.M. Salivary biomarkers in the diagnosis of periodontal diseases. J. Calif. Dent. Assoc. 2013, 41, 119–124. [Google Scholar] [PubMed]
- Lee, J.Y.; Antoniazzi, M.C.C.; Perozini, C.; Ruivo, G.F.; Pallos, D. Prevalence of carotid artery calcification in patients with chronic renal disease identified by panoramic radiography. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2014, 118, 612–618. [Google Scholar] [CrossRef] [PubMed]
- Pallos, D.; Leao, M.V.; Togeiro, F.C.; Alegre, L.; Ricardo, L.H.; Perozini, C.; Ruivo, G.F. Salivary markers in patients with chronic renal failure. Arch. Oral Biol. 2015, 60, 1784–1788. [Google Scholar] [CrossRef] [PubMed]
- Costantinides, F.; Castronovo, G.; Vettori, E.; Frattini, C.; Artero, M.L.; Bevilacqua, L.; Berton, F.; Nicolin, V.; Di Lenarda, R. Dental care for patients with end-stage renal disease and undergoing hemodialysis. Int. J. Dent. 2018, 2018, 9610892. [Google Scholar] [CrossRef]
- Rysz, J.; Gluba-Brzózka, A.; Franczyk, B.; Jablonowski, Z.; Cialkowska-Rysz, A. Novel biomarkers in the diagnosis of chronic kidney disease and the prediction of its outcome. Int. J. Mol. Sci. 2017, 18, 1702. [Google Scholar] [CrossRef]
- Akar, H.; Akar, G.C.; Carrero, J.J.; Stenvinkel, P.; Lindholm, B. Systemic consequences of poor oral health in chronic kidney disease patients. Clin. J. Am. Soc. Nephrol. 2011, 6, 218–226. [Google Scholar] [CrossRef]
- Nylund, K.M.; Ruokonen, H.; Sorsa, T.; Heikkinen, A.M.; Meurman, J.H.; Ortiz, F.; Tervahartiala, T.; Furuholm, J.; Bostanci, N. Association of the Salivary Triggering Receptor Expressed on Myeloid Cells/ its Ligand Peptidoglycan Recognition Protein 1 Axis with Oral Inflammation Kidney Disease. J. Periodontol. 2018, 89, 117–129. [Google Scholar] [CrossRef] [PubMed]
- Nylund, K.M.; Meurman, J.H.; Heikkinen, A.M.; Honkanen, E.; Vesterinen, M.; Furuholm, J.O.; Tervahartiala, T.; Sorsa, T.; Ruokonen, H.M. Periodontal Inflammatory Burden and Salivary MMP-8 Concentration Among Chronic Kidney Disease Patients at Predialysis Stage. J. Periodontol. 2015, 86, 1212–1220. [Google Scholar] [CrossRef]
- Ebersole, J.L.; Nagarajan, R.; Akers, D.; Miller, C.S. Targeted salivary biomarkers for discrimination of periodontal health and disease(s). Front. Cell. Infect. Microbiol. 2015, 5, 1–12. [Google Scholar] [CrossRef]
- Ji, S.; Choi, Y. Point-of-care diagnosis of periodontitis using saliva: Technically feasible but still a challenge. Front. Cell. Infect. Microbiol. 2015, 5, 1–9. [Google Scholar] [CrossRef]
- Akram, Z.; Abduljabbar, T.; Abu Hassan, M.I.; Javed, F.; Vohra, F. Cytokine profile in chronic periodontitis patients with and without obesity: A systematic review and meta-analysis. Dis. Markers. 2016, 2016, 4801418. [Google Scholar] [CrossRef] [PubMed]
- Ksiazek, K.; Blaszczak, J.; Buraczynska, M. IL4 gene VNTR polymorphism in chronic periodontitis in end-stage renal disease patients. Oral Dis. 2019, 25, 258–264. [Google Scholar] [CrossRef] [PubMed]
- Cotič, J.; Ferran, M.; Karišik, J.; Jerin, A.; Pussinen, P.J.; Nemec, A.; Pavlica, Z.; Buturović-Ponikvar, J.; Petelin, M. Oral health and systemic inflammatory, cardiac and nitroxid biomarkers in hemodialysis patients. Med. Oral Patol. Oral Cir. Bucal. 2017, 22, e432–e439. [Google Scholar] [CrossRef] [PubMed]
- Garneata, L.; Slusanschi, O.; Preoteasa, E.; Corbu-stancu, A.; Mircescu, G. Periodontal status, inflammation, and malnutrition in hemodialysis patients—Is there a link? J. Ren. Nutr. 2014, 25, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Perozini, C.; Ruivo, G.F.; Ricardo, L.H.; Pavesi, L.A.; Kim, Y.J.; Pallos, D. Medical and periodontal clinical parameters in patients at different levels of chronic renal failure. Int. J. Dent. 2017, 2017, 9858073. [Google Scholar] [CrossRef]
- Hou, Y.; Wang, X.; Zhang, C.X.; Wei, Y.D.; Jiang, L.L.; Zhu, X.Y.; Du, Y.J. Risk factors of periodontal disease in maintenance hemodialysis patients. Medicine 2017, 96, 1–5. [Google Scholar] [CrossRef]
- Veisa, G.; Tasmoc, A.; Nistor, I.; Segall, L.; Siriopol, D.; Solomon, S.M.; Donciu, M.D.; Voroneanu, L.; Nastasa, A.; Covic, A. The impact of periodontal disease on physical and psychological domains in long-term hemodialysis patients: A cross-sectional study. Int. Urol. Nephrol. 2017, 49, 1261–1266. [Google Scholar] [CrossRef]
- Rodrigues, V.P.; Libério, S.A.; Lopes, F.F.; Thomaz, E.B.; Guerra, R.N.; Gomes-Filho, I.S.; Pereira, A.L. Periodontal status and serum biomarkers levels in haemodialysis patients. J. Clin. Periodontol. 2014, 41, 862–868. [Google Scholar] [CrossRef]
- Grubbs, V.; Garcia, F.; Vittinghoff, E.; Jue, B.L.; Ryder, M.; Lovett, D.H.; Offenbacher, S.; Taylor, G.; Ganz, P.; Bibbins-Domingo, K.; et al. Nonsurgical Periodontal Therapy in CKD: Findings of the Kidney and Periodontal Disease (KAPD) Pilot Randomized Controlled Trial. Kidney Med. 2019, 2, 49–58. [Google Scholar] [CrossRef]
- Yoshihara, A.; Iwasaki, M.; Miyazaki, H.; Nakamura, K. Bidirectional relationship between renal function and periodontal disease in older Japanese women. J. Clin. Periodontol. 2016, 43, 720–726. [Google Scholar] [CrossRef]
- Ausavarungnirun, R.; Wisetsin, S.; Rongkiettechakorn, N.; Chaichalermsak, S.; Udompol, U.; Rattanasompattikul, M. Association of dental and periodontal disease with chronic kidney disease in patients of a single, tertiary care centre in Thailand. BMJ Open 2016, 6, e011836. [Google Scholar] [CrossRef] [PubMed]
- Arenius, I.; Ruokonen, H.; Ortiz, F.; Furuholm, J.; Välimaa, H.; Bostanci, N.; Eskola, M.; Maria Heikkinen, A.; Meurman, J.H.; Sorsa, T.; et al. The relationship between oral diseases and infectious complications in patients under dialysis. Oral Dis. 2020, 26, 1045–1052. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.T.; Shih, C.J.; Ou, S.M.; Hung, S.C.; Lin, C.H.; Tarng, D.C. Periodontal Disease and Risks of Kidney Function Decline and Mortality in Older People: A community-based cohort study. Am. J. Kidney Dis. 2015, 66, 223–230. [Google Scholar]
- Rodrigues Gomes, S.S.; Barretobezerra, A.C.; Maia Prado, A.C. Salivary biomarkers, vital signs and behaviour of pre-school children during their first dental visit. Eur. J. Paediatr. Dent. 2013, 14, 279–283. [Google Scholar]
- Kshirsagar, A.V.; Grubbs, V. Periodontal disease and CKD-associated morbidity: Is there now enough evidence to move from observation to intervention? Am. J. Kidney Dis. 2015, 66, 181–183. [Google Scholar]
- Caton, J.G.; Armitage, G.; Berglundh, T.; Chapple, I.L.; Jepsen, S.; Kornman, K.S.; Mealey, B.L.; Papapanou, P.N.; Sanz, M.; Tonetti, M.S.; et al. A new classification scheme for periodontal and peri-implant diseases and conditions—Introduction and key changes from the 1999 classification. J. Periodontol. 2018, 89 (Suppl. 1), S1–S8. [Google Scholar] [CrossRef]
- García, E.; Padilla, A.; Romo, S.; Ramírez, M. Oral mucosa symptoms, signs and lesions, in end stage renal disease and non-end stage renal disease diabetic patients. Med. Oral Patol. Oral Cir. Bucal. 2006, 11, 467–473. [Google Scholar]
- Becherucci, F.; Roperto, R.M.; Materassi, M.; Romagnani, P. Chronic kidney disease in children. Clin. Kidney J. 2016, 9, 583–591. [Google Scholar] [CrossRef]
- Coelho, J.M.F.; Miranda, S.S.; da Cruz, S.S.; Dos Santos, D.N.; Trindade, S.C.; Cerqueira, E.D.M.; Passos-Soares, J.D.S.; Costa, M.D.C.N.; Figueiredo, A.C.M.; Hintz, A.M.; et al. Common mental disorder is associated with periodontitis. J. Periodontal Res. 2020, 55, 221–228. [Google Scholar] [CrossRef]
- Cavelti-Weder, C.; Babians-Brunner, A.; Keller, C.; Stahel, M.A.; Kurz-Levin, M.; Zayed, H.; Solinger, A.M.; Mandrup-Poulsen, T.; Dinarello, C.A.; Donath, M.Y.; et al. Effects of Gevokizumab on Glycemia and infalmatory Markers in Type 2 Diabetes. Diabetes Care 2012, 35, 1654–1662. [Google Scholar] [CrossRef]
- Zhao, G.; Dharmadhikari, G.; Maedler, K.; Meyer-Hermann, M. Possible Role of Interleukin-1 b in Type 2 Diabetes Onset and Implications for Anti-inflammatory Therapy Strategies. PLoS Comput. Biol. 2014, 10, e1003798. [Google Scholar] [CrossRef] [PubMed]
- Dioguardi, M.; Caloro, G.A.; Troiano, G.; Giannatempo, G.; Laino, L.; Petruzzi, M.; Lo Muzio, L. Oral manifestations in chronic uremia patients. Ren. Fail. 2015, 38, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Romandini, M.; Cordaro, M.; Laforí, A.; Romandini, P.; Baima, G. Periodontitis and platelet count: A new potential link with cardiovascular and other systemic inflammatory diseases. J. Clin. Periodontol. 2018, 45, 1299–1310. [Google Scholar] [CrossRef] [PubMed]
- Arai, Y.; Kanda, E.; Iimori, S.; Naito, S. Low white blood cell count is independently associated with chronic kidney disease progression in the elderly: The CKD-ROUTE study. Clin. Exp. Nephrol. 2018, 22, 291–298. [Google Scholar] [CrossRef] [PubMed]
- Gupta, M.; Gupta, M. Oral conditions in renal disorders and treatment considerations—A review for pediatric dentist. Saudi Dent. J. 2015, 27, 113–119. [Google Scholar] [CrossRef] [PubMed]
- Rudick, C.P.; Miyamoto, T.; Lang, M.S.; Agrawal, D.K. Triggering receptor expressed on myeloid cells in the pathogenesis of periodontitis: Potential novel treatment strategies. Expert Rev. Clin. Immunol. 2017, 13, 1189–1197. [Google Scholar] [CrossRef]
- Opal, S.M.; Depalo, V.A. Anti-Inflammatory Cytokines. Chest 2000, 117, 1162–1172. [Google Scholar] [CrossRef]
- Jamieson, L.; Skilton, M.; Maple-Brown, L.; Kapellas, K.; Askie, L.; Hughes, J.; Arrow, P.; Cherian, S.; Fernandes, D.; Pawar, B.; et al. Periodontal disease and chronic kidney disease among Aboriginal adults; An RCT. BMC Nephrol. 2015, 16, 181. [Google Scholar] [CrossRef]
- Iwagami, M.; Mansfield, K.E.; Hayes, J.F.; Walters, K.; Osborn, D.P.; Smeeth, L.; Nitsch, D.; Tomlinson, L.A. Severe mental illness and chronic kidney disease: A cross-sectional study in the United Kingdom. Clin. Epidemiol. 2018, 10, 421–429. [Google Scholar] [CrossRef]
- Zhao, D.; Khawaja, A.T.; Jin, L.; Li, K.Y.; Tonetti, M.; Pelekos, G. The directional and non-directional associations of periodontitis with chronic kidney disease: A systematic review and meta-analysis of observational studies. J. Periodontal Res. 2018, 53, 682–704. [Google Scholar] [CrossRef]
- Fitzpatrick, A.; Mohammadi, F.; Jesudason, S. Managing pregnancy in chronic kidney disease: Improving outcomes for mother and baby. Int. J. Women’s Health 2016, 8, 273–285. [Google Scholar]
- Deschamps-Lenhardt, S.; Martin-Cabezas, R.; Hannedouche, T.; Huck, O. Association between periodontitis and chronic kidney disease: Systematic review and meta-analysis. Oral Dis. 2019, 25, 385–402. [Google Scholar] [CrossRef] [PubMed]
- Sharma, P.; Dietrich, T.; Ferro, C.J.; Cockwell, P.; Chapple, I.L.C. Association between periodontitis and mortality in stages 3–5 chronic kidney disease: NHANES III and linked mortality study. J. Clin. Periodontol. 2016, 43, 104–113. [Google Scholar] [CrossRef] [PubMed]
- Machowska, A.; Carrero, J.J.; Lindholm, B.; Stenvinkel, P. Therapeutics targeting persistent inflammation in chronic kidney disease. Transl. Res. 2016, 167, 204–213. [Google Scholar] [CrossRef]
- Grubbs, V.; Garcia, F.; Jue, B.L.; Vittinghoff, E.; Ryder, M.; Lovett, D.; Carrillo, J.; Offenbacher, S.; Ganz, P.; Bibbins-Domingo, K.; et al. The Kidney and Periodontal Disease (KAPD) study: A pilot randomized controlled trial testing the effect of non-surgical periodontal therapy on chronic kidney disease. Contemp. Clin. Trials 2017, 53, 143–150. [Google Scholar] [CrossRef]
- Kaneko, N.; Kurata, M.; Yamamoto, T.; Morikawa, S.; Masumoto, J. The role of interleukin-1 in general pathology. Inflamm. Regen. 2019, 39, 1–16. [Google Scholar] [CrossRef]
- Dinarello, C.A. Interleukin-1 in the pathogenesis and treatment of inflammatory diseases. Blood 2011, 117, 3720–3732. [Google Scholar] [CrossRef]
- Farivar, S.; Hassani, M.; Shiari, R. Interleukin-1 as a key factor in the development of inflammatory diseases. Arch. Pediatr. Infect. Dis. 2014, 2, 1–5. [Google Scholar] [CrossRef]
- Zakiyanov, O.; Kalousová, M.; Zima, T.; Tesař, V. Matrix metalloproteinases in renal diseases: A critical appraisal. Kidney Blood Press Res. 2019, 44, 298–330. [Google Scholar] [CrossRef]
- Dai, X.; Zeng, Z.; Fu, C.; Zhang, S.; Cai, Y.; Chen, Z. Diagnostic value of neutrophil gelatinase-associated lipocalin, cystatin C, and soluble triggering receptor expressed on myeloid cells-1 in critically ill patients with sepsis-associated acute kidney injury. Crit. Care 2015, 19, 1–10. [Google Scholar] [CrossRef]
- Tammaro, A.; Derive, M.; Gibot, S.; Leemans, J.C.; Florquin, S.; Dessing, M.C. TREM-1 and its potential ligands in non-infectious diseases: From biology to clinical perspectives. Pharmacol. Ther. 2017, 177, 81–95. [Google Scholar] [CrossRef] [PubMed]
- Raivisto, T.; Heikkinen, A.M.; Silbereisen, A.; Kovanen, L.; Ruokonen, H.; Tervahartiala, T.; Haukka, J.; Sorsa, T.; Bostanci, N. Regulation of Salivary Peptidoglycan Recognition Protein1in Adolescents. JDR Clin. Transl. Res. 2019, 20, 1–10. [Google Scholar]
- Cheng, R.; Wu, Z.; Li, M.; Shao, M.; Hu, T. Interleukin-1β is a potential therapeutic target for periodontitis: A narrative review. Int. J. Oral Sci. 2020, 12, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Basu, R.K.; Donaworth, E.; Siroky, B.; Devarajan, P.; Wong, H.R. Loss of matrix metalloproteinase-8 is associated with worsened recovery after ischemic kidney injury. Ren. Fail. 2015, 37, 469–475. [Google Scholar] [CrossRef] [PubMed]
- Cruz, M.C.; Andrade, C.; Urrutia, M.; Draibe, S.; Nogueira-Martins, L.A.; Sesso, R.D.C.C. Quality of life in patients with chronic kidney disease. Clinics 2011, 66, 991–995. [Google Scholar] [CrossRef]
- Ismail, F.B.; Ismail, G.; Dumitriu, A.S.; Baston, C.; Berbecar, V.; Jurubita, R.; Andronesi, A.; Dumitriu, H.T.; Sinescu, I. Identification of subgingival periodontal pathogens and association with the severity of periodontitis in patients with chronic kidney diseases: A cross-sectional study. Biomed. Res. Int. 2015, 2015, 370314. [Google Scholar] [CrossRef]


{kind=link}
| MEDLINE (PubMed) | Embase | Web of Science | |
|---|---|---|---|
| #1 | P—Patients with chronic kidney disease and periodontitis | ||
| “Chronic Kidney Disease” [MeSH Terms] AND Periodontitis [MeSH Terms] OR “periodontal disease” [All Terms] | “Chronic Kidney Disease” AND Periodontitis OR “periodontal disease” | “Chronic Kidney Disease” AND Periodontitis OR “periodontal disease” | |
| #2 | I—Analysis of saliva biomarkers | ||
| …AND “Inflammatory biomarkers” [MeSH Terms] OR “Salivary biomarkers” [All Terms] | …AND “Inflammatory biomarkers” OR “Salivary biomarkers” | …AND “Inflammatory biomarkers” OR “Salivary biomarkers” | |
| #3 | C—Analysis of blood biomarkers | ||
| #4 | O—Exhibit similar outcomes | ||
| Search Combination | (#1 AND #2) No combination was done with #3 and #4. Using the #3 we would be repeating the terms of #1 and #2, and the combination using keywords related to outcome #4 would limit even more the search and eliminate some relevant studies. | ||
| Filters | Humans, 11 years | ||
| Inclusion and Exclusion Criteria | |
|---|---|
| Inclusion | Exclusion |
| Clinical Study | Systematic review/Meta-analysis |
| Clinical Trial | Review |
| Clinical Trial Protocol | No biomarkers analyzed |
| Clinical Trial, Phase I | Blood biomarkers |
| Clinical Trial, Phase II | Crevicular fluid biomarkers |
| Clinical Trial, Phase III | Patients without CKD |
| Clinical Trial, Phase IV | Patient without periodontitis/ peri-implantitis |
| Research study | Urinary biomarkers |
| Randomized Controlled Trial | Animal study |
| Controlled Clinical Trial | |
| Published in the last 10 years | |
| Humans | |
| Any language | |
| Author/Year | Reason for Exclusion |
|---|---|
| Maciejczyk et al., 2018 | Patients with periodontitis were excluded |
| Joseph et al., 2011 | No CKD patients |
| Kovalciková et al., 2019 | |
| Marinoski et al., 2019 | |
| Schmalz et al., 2017 | |
| Schmalz et al., 2016 | |
| Grubbs et al., 2015 | |
| Caglayan et al., 2015 | |
| Oyetola et al., 2015 | No biomarkers were analyzed |
| Zhao et al., 2014 | |
| Doscas et al., 2018 | |
| Sharma et al., 2014 | |
| Garneata et al., 2014 | |
| Ibrahim et al., 2020 | |
| Iwasaki et al., 2019 | |
| Lertpimonchai et al., 2019 | No biomarker association |
| Machowska et al., 2016 | |
| Opatrná et al., 2015 | Review |
| Hickey et al., 2020 | |
| Demoersman et al., 2018 | No clear data for CKD patients |
| Rodrigues et al., 2016 | |
| Pallos et al., 2015 | No direct relation with periodontitis |
| Luo et al., 2013 | |
| Nylund et al., 2015 | Data was updated in 2017, Nylund et al., 2017 |
| Nylund et al., 2017 | Data was updated in 2020, Arenius et al., 2020 |
| Trivedi et al., 2018 | Trial still recruiting patients |
| Grubbs et al., 2017 | Planning of trial phase, no results |
| Jamieson et al., 2015 | |
| Sharma et al., 2016 | Urinary samples were used instead of blood or salivary samples |
| Yoshihara et al., 2016 | Same results as Yoshihara et al., 2016, with the addition of genotype analysis |
| Study | Patient | Health | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Author/Year | Study Design | Mean Period (Months) | N | Age (Years) | Gender (Female %) | Periodontal Condition | CKD | Diabetes (%) | Smoking (%) | |
| Mean | Range | |||||||||
| Blood collection | ||||||||||
| Cotic et al., 2017 [34] | RCT | NS | 111 | NS | 26–90 | 38.74 | 64.6% had a CPITN > 3 | HD | 34.2 | 15.3 |
| Hou et al., 2017 [37] | OB | 4 | 135 | 50.8 | 50.8 ± 13.3 | 41.91 | 51.50% gingivitis/periodontitis | HD | 36 | 55.7 (of 51.50) |
| Veisa et al., 2017 [38] | CSS | 31 | 101 | 52.5 | 52.5 ± 14.3 | 56.44 | 75.2% periodontitis | HD | 5.94 | 13.86 |
| Garneata et al., 2014 [35] | CSS | NS | 238 | 57.0 | NS | 39.91 | 75.63% periodontitis | HD | 10.92 | 60.92 |
| Ksiazek et al., 2019 [33] | CSS | 96 | 442 | 63 | 63 ± 16.3 | 48.9 | 40.72% periodontitis | ESRD | NS | NS |
| Perozini et al., 2017 [36] | CSS | 16 | 102 | 54.74 | 54.74 ± 13.01 | Early stage 75.0; Predialysis 50.0; Hemodialysis 41.7 | 100% Periodontitis | 44 CKD 1-2; 30 CKD 3-4; 28 CKD; 5 (HDG) | Early stage: 40.0; Predialysis: 30.0; Hemodialysis: 16.7 | NS |
| Rodrigues et al., 2014 [39] | CSS | 6 | 96 | 39.8 | 39.8 ± 13.2 | 53.13 | 59.4% periodontitis | HD | NS | NS |
| Chen et al., 2015 [44] | CS | 120 | 100,263 | NS | >65 | 49.1 | 13.7% periodontitis | eGFR (mL/min/1.73 m2) 68.76 ± 17.6 | 13.9 | 8.7 |
| Grubss et al., 2019 [40] | RCT | 12 | 51 | 59 | 34–73 | 32.3 | 100% Periodontitis | 71% CKD 3 and 29% CKD 4 | 47.0 | 10.0 |
| Yoshihara et al., 2016 [41] | CSS | NS | 332 | NS | 55–74 | 100 | Periodontitis (NS) | CKD (NS) | NS | No |
| Ausavarungnituna et al., 2016 [42] | CSS | 12 | 129 | NS | 30–86 | 24 | Periodontitis (NS) | 27% severe CKD, 37% moderate CKD and 36% mild CKD | NS | NS |
| Saliva collection | ||||||||||
| Arenius et al., 2020 [43] | OB | 180 | 117 | NS | 23–83 | 29.1 | PIBI = 6 (median) TDI = 3 (median) | 100% CKD stage 4 and 5 (dialysis) | NS | NS |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tavares, L.T.R.; Saavedra-Silva, M.; López-Marcos, J.F.; Veiga, N.J.; Castilho, R.d.M.; Fernandes, G.V.d.O. Blood and Salivary Inflammatory Biomarkers Profile in Patients with Chronic Kidney Disease and Periodontal Disease: A Systematic Review. Diseases 2022, 10, 12. https://0-doi-org.brum.beds.ac.uk/10.3390/diseases10010012
Tavares LTR, Saavedra-Silva M, López-Marcos JF, Veiga NJ, Castilho RdM, Fernandes GVdO. Blood and Salivary Inflammatory Biomarkers Profile in Patients with Chronic Kidney Disease and Periodontal Disease: A Systematic Review. Diseases. 2022; 10(1):12. https://0-doi-org.brum.beds.ac.uk/10.3390/diseases10010012
Chicago/Turabian StyleTavares, Lisandra Taísa Reginaldo, Mariana Saavedra-Silva, Joaquín Francisco López-Marcos, Nélio Jorge Veiga, Rogerio de Moraes Castilho, and Gustavo Vicentis de Oliveira Fernandes. 2022. "Blood and Salivary Inflammatory Biomarkers Profile in Patients with Chronic Kidney Disease and Periodontal Disease: A Systematic Review" Diseases 10, no. 1: 12. https://0-doi-org.brum.beds.ac.uk/10.3390/diseases10010012