Relationship between Bone Health Biomarkers and Cardiovascular Risk in a General Adult Population

Abstract
:1. Introduction
2. Material and Methods
2.1. Subjects and Cardiovascular Risk Scores
2.2. Laboratory Measurements
2.3. Statistical Analysis
3. Results
3.1. Characteristics of Subjects
3.2. Correlation between Bone Health Biomarkers
3.3. Correlation between Bone Health Biomarkers and CV Risk Factors
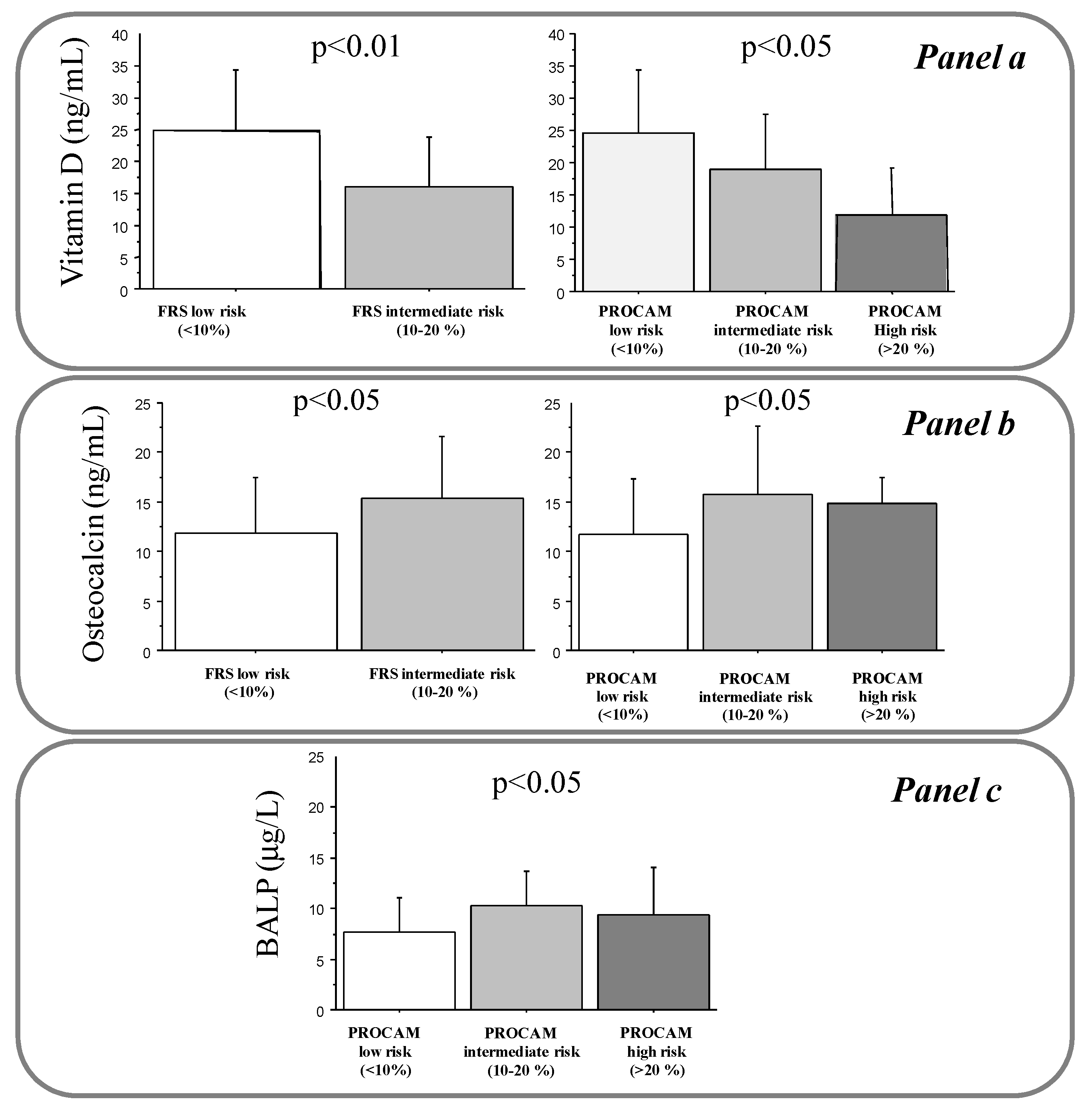
3.3.1. 25(OH)D
3.3.2. OC
3.3.3. BALP
3.3.4. CTx and P1NP
3.3.5. Logistic Analysis for FRS and PROCAM
4. Discussion
5. Conclusions
Author Contributions
Conflicts of Interest
References
- Vassalle, C.; Maffei, S.; Iervasi, G. Bone remodelling biomarkers: New actors on the old cardiovascular stage. In Biomarker Validation—Technological, Clinical and Commercial Aspects, KGaA; Wiley-VCH Verlag GmbH & Co.: Weinheim, Germany, 2015; Chapter 7; pp. 107–146. [Google Scholar]
- Magni, P.; Macchi, C.; Sirtori, C.R.; Corsi-Romanelli, M.M. Osteocalcin as a potential risk biomarker for cardiovascular and metabolic diseases. Clin. Chem. Lab. Med. 2016, 54, 1579–1587. [Google Scholar] [CrossRef] [PubMed]
- Bianchi, S.; Maffei, S.; Prontera, C.; Battaglia, D.; Vassalle, C. Preanalytical, analytical (DiaSorin LIAISON) and clinical variables potentially affecting the 25-OH Vitamin D estimation. Clin. Biochem. 2012, 45, 1652–1657. [Google Scholar] [CrossRef] [PubMed]
- Vassalle, C.; Pérez-López, F.R. The Importance of Some Analytical Aspects and Confounding Factors in Relation to Clinical Interpretation of Results. In Vitamin D: Daily Requirements, Dietary Sources and Symptoms of Deficiency; Nova Publisher: New York, NY, USA, 2013; Chapter 4; ISBN 978-1-62808-816-8. [Google Scholar]
- Iqbal, M.P.; Mehboobali, N.; Azam, I.; Tareen, A.K. Association of alkaline phosphatase with acute myocardial infarction in a population with high prevalence of hypovitaminosis D. Clin. Chim. Acta 2013, 425, 192–195. [Google Scholar] [CrossRef] [PubMed]
- Brøndum-Jacobsen, P.; Benn, M.; Jensen, G.B.; Nordestgaard, B.G. 25-Hydroxyvitamin d levels and risk of ischemic heart disease, myocardial infarction, and early death: Population-based study and meta-analyses of 18 and 17 studies. Arterioscler. Thromb. Vasc. Biol. 2012, 32, 2794–2802. [Google Scholar] [CrossRef] [PubMed]
- Tomson, J.; Emberson, J.; Hill, M.; Gordon, A.; Armitage, J.; Shipley, M.; Collins, R.; Clarke, R. Vitamin D and risk of death from vascular and non-vascular causes in the Whitehall study and meta-analyses of 12,000 deaths. Eur. Heart J. 2013, 34, 1365–1374. [Google Scholar] [CrossRef] [PubMed]
- D’Agostino, R.B.; Vasan, R.S.; Pencina, M.J.; Wolf, P.A.; Cobain, M.; Massaro, J.M.; Kannel, W.B. General cardiovascular risk profile for use in primary care: The Framingham Heart Study. Circulation 2008, 117, 743–753. [Google Scholar] [CrossRef] [PubMed]
- Assmann, G.; Cullen, P.; Schulte, H. Simple scoring scheme for calculating the risk of acute coronary events based on the 10-year follow-up of the prospective cardiovascular Münster (PROCAM) study. Circulation 2002, 105, 310–315. [Google Scholar] [CrossRef] [PubMed]
- Vassalle, C.; Pagani, F. Biomarkers of Bone Turnover: Potential, Challenges and Pitfalls from the Laboratory Point of view. Rheumatology (Sunnyvale) 2016, 6, 183. [Google Scholar] [CrossRef]
- Schnatz, P.F.; Manson, J.E. Vitamin D and cardiovascular disease: An appraisal of the evidence. Clin. Chem. 2014, 60, 600–609. [Google Scholar] [CrossRef] [PubMed]
- Leung, P.S. The Potential Protective Action of Vitamin D in Hepatic Insulin Resistance and Pancreatic Islet Dysfunction in Type 2 Diabetes Mellitus. Nutrients 2016, 8, 3. [Google Scholar] [CrossRef] [PubMed]
- Mozos, I.; Marginean, O. Links between Vitamin D Deficiency and Cardiovascular Diseases. Biomed. Res. Int. 2015, 2015, 109275. [Google Scholar] [CrossRef] [PubMed]
- Papandreou, D.; Hamid, Z.T. The Role of Vitamin D in Diabetes and Cardiovascular Disease: An Updated Review of the Literature. Dis Mark. 2015, 2015, 580474. [Google Scholar] [CrossRef] [PubMed]
- Jiménez-Osorio, A.S.; González-Reyes, S.; Pedraza-Chaverri, J. Natural Nrf2 activators in diabetes. Clin. Chim. Acta 2015, 448, 182–192. [Google Scholar] [CrossRef] [PubMed]
- Song, Y.; Wang, L.; Pittas, A.G.; Del Gobbo, L.C.; Zhang, C.; Manson, J.E.; Hu, F.B. Blood 25-hydroxy vitamin D levels and incident type 2 diabetes: A meta-analysis of prospective studies. Diabetes Care 2013, 36, 1422–1428. [Google Scholar] [CrossRef] [PubMed]
- Ferron, M.; Hinoi, E.; Karsenty, G.; Ducy, P. Osteocalcin differentially regulates beta cell and adipocyte gene expression and affects the development of metabolic diseases in wild-type mice. Proc. Natl. Acad. Sci. USA 2008, 105, 5266–5270. [Google Scholar] [CrossRef] [PubMed]
- Lee, N.K.; Sowa, H.; Hinoi, E.; Ferron, M.; Ahn, J.D.; Confavreux, C.; Dacquin, R.; Mee, P.J.; McKee, M.D.; Jung, D.Y.; et al. Endocrine regulation of energy metabolism by the skeleton. Cell 2007, 130, 456–469. [Google Scholar] [CrossRef] [PubMed]
- Montalcini, T.; Emanuele, V.; Ceravolo, R.; Gorgone, G.; Sesti, G.; Perticone, F.; Pujia, A. Relation of low bone mineral density and carotid atheroesclerosis in postmenopausal women. Am. J. Cardiol. 2004, 94, 266–269. [Google Scholar] [CrossRef] [PubMed]
- Luo, Y.; Ma, X.; Hao, Y.; Xiong, Q.; Xu, Y.; Pan, X.; Bao, Y.; Jia, W. Relationship between serum osteocalcin level and carotid intima-media thickness in a metabolically healthy Chinese population. Cardiovasc. Diabetol. 2015, 14, 82. [Google Scholar] [CrossRef] [PubMed]
- Yeap, B.B.; Chubb, S.A.; Flicker, L.; McCaul, K.A.; Ebeling, P.R.; Hankey, G.J.; Beilby, J.P.; Norman, P.E. Associations of total osteocalcin with all-cause and cardiovascular mortality in older men. Health Men Study Osteoporos. Int. 2012, 23, 599–606. [Google Scholar] [CrossRef] [PubMed]
- Lerchbaum, E.; Schwetz, V.; Pilz, S.; Grammer, T.B.; Look, M.; Boehm, B.O.; Obermayer-Pietsch, B.; März, W. Association of bone turnover markers with mortality in men referred to coronary angiography. Osteoporos. Int. 2013, 24, 1321–1332. [Google Scholar] [CrossRef] [PubMed]
- Unal, H.U.; Çelik, M.; Gökoğlan, Y.; Çetinkaya, H.; Gök, M.; Karaman, M.; Yilmaz, M.İ.; Eyileten, T.; Oğuz, Y. Mitral annular calcification and the serum osteocalcin level in patients with chronic kidney disease. Ren. Fail. 2014, 36, 1481–1485. [Google Scholar] [CrossRef] [PubMed]
- Flammer, A.J.; Gössl, M.; Widmer, R.J.; Reriani, M.; Lennon, R.; Loeffler, D.; Shonyo, S.; Simari, R.D.; Lerman, L.O.; Khosla, S.; et al. Osteocalcin positive CD133+/CD34−/KDR+ progenitor cells as an independent marker for unstable atherosclerosis. Eur. Heart J. 2012, 33, 2963–2969. [Google Scholar] [CrossRef] [PubMed]
- Gössl, M.; Mödder, U.I.; Atkinson, E.J.; Lerman, A.; Khosla, S. Osteocalcin expression by circulating endothelial progenitor cells in patients with coronary atherosclerosis. J. Am. Coll. Cardiol. 2008, 52, 1314–1325. [Google Scholar] [CrossRef] [PubMed]
- Manghat, P.; Souleimanova, I.; Cheung, J.; Wierzbicki, A.S.; Harrington, D.J.; Shearer, M.J.; Chowienczyk, P.; Fogelman, I.; Nerlander, M.; Goldsmith, D.; et al. Association of bone turnover markers and arterial stiffness in pre-dialysis chronic kidney disease (CKD). Bone 2011, 48, 1127–1132. [Google Scholar] [CrossRef] [PubMed]
- Ertugrul, D.T.; Yavuz, B.; Cil, H.; Ata, N.; Akin, K.O.; Kucukazman, M.; Yalcin, A.A.; Dal, K.; Yavuz, B.B.; Tutal, E. STATIN-D study: Comparison of the influences of rosuvastatin and fluvastatin treatment on the levels of 25 hydroxyvitamin D. Cardiovasc. Ther. 2011, 29, 146–152. [Google Scholar] [CrossRef] [PubMed]
- Pater, A.; Sypniewska, G.; Pilecki, O. Biochemical markers of bone cell activity in children with type 1 diabetes mellitus. J. Pediatr. Endocrinol. MeTable 2010, 23, 81–86. [Google Scholar] [CrossRef]
- Achemlal, L.; Tellal, S.; Rkiouak, F.; Nouijai, A.; Bezza, A.; Derouiche, M.; Ghafir, D.; El Maghraoui, A. Bone metabolism in male patients with type 2 diabetes. Clin. Rheumatol. 2005, 24, 493–496. [Google Scholar] [CrossRef] [PubMed]
- Ricci, T.A.; Chowdhury, H.A.; Heymsfield, S.B.; Stahl, T.; Pierson, R.N.; Shapses, S.A. Calcium supplementation suppresses bone turnover during weight reduction in postmenopausal women. J. Bone Miner. Res. 1998, 13, 1045–1050. [Google Scholar] [CrossRef] [PubMed]
- Ricci, T.A.; Heymsfield, S.B.; Pierson, R.N.; Stahl, T.; Chowdhury, H.A.; Shapses, S.A. Moderate energy restriction increases bone resorption in obese postmenopausal women. Am. J. Clin. Nutr. 2001, 73, 347–352. [Google Scholar] [PubMed]
- Shapses, S.A.; Von Thun, N.L.; Heymsfield, S.B.; Ricci, T.A.; Ospina, M.; Pierson, R.N.; Stahl, T. Bone turnover and density in obese premenopausal women during moderate weight loss and calcium supplementation. J. Bone Miner. Res. 2001, 16, 1329–1336. [Google Scholar] [CrossRef] [PubMed]
- Giusti, V.; Gasteyger, C.; Suter, M.; Heraief, E.; Gaillard, R.C.; Burckhardt, P. Gastric banding induces negative bone remodelling in the absence of secondary hyperparathyroidism: Potential role of serum C telopeptides for follow-up. Int. J. Obes. (Lond.) 2005, 29, 1429–1435. [Google Scholar] [CrossRef] [PubMed]
- Hinton, P.S.; LeCheminant, J.D.; Smith, B.K.; Rector, R.S.; Donnelly, J.E. Weight loss-induced alterations in serum markers of bone turnover persist during weight maintenance in obese men and women. J. Am. Coll. Nutr. 2009, 28, 565–573. [Google Scholar] [CrossRef] [PubMed]
- Yeap, B.B.; Alfonso, H.; Chubb, S.A.; Byrnes, E.; Beilby, J.P.; Ebeling, P.R.; Allan, C.A.; Schultz, C.; Hankey, G.J.; Golledge, J.; et al. Proportion of Undercarboxylated Osteocalcin and Serum P1NP Predict Incidence of Myocardial Infarction in Older Men. J. Clin. Endocrinol. Metable. 2015, 100, 3934–3942. [Google Scholar] [CrossRef] [PubMed]
- Sheppard, C. How large should my sample be? Some quick guides to sample size and the power of tests. Mar. Pollut. Bull. 1999, 38, 439–447. [Google Scholar] [CrossRef]


{kind=link}
| Parameters | Values |
|---|---|
| n | 103 |
| Age (years) | 56 ± 12 |
| Males, n (%) | 21 (20) |
| Hypertension, n (%) | 30 (29) |
| Diabetes, n (%) | 10 (10) |
| Dyslipidemia, n (%) | 48 (47) |
| Current smokers, n (%) | 19 (19) |
| Obesity, n (%) | 11 (11) |
| Body Mass Index (Kg/m2) | 24.8 ± 4.6 |
| Total cholesterol (mg/dL) | 207 ± 36 |
| HDL cholesterol (mg/dL) | 62 ± 16 |
| Triglycerides (mg/dL), median (min-max) | 89 (39–299) |
| LDL cholesterol (mg/dL) | 125 ± 30 |
| Glycemia (mg/dL), median (min-max) | 88 (73–161) |
| Insulin (mUI/mL) *, median (min-max) | 4 (1–18) |
| Systolic blood pressure (mmHg) | 125 ± 18 |
| Diastolic blood pressure (mmHg) | 75 ± 9 |
| C-reactive protein (mg/dL), median (min-max) | 0.14 (0.02–3.1) |
| 25-hydroxyvitamin D (ng/mL) | 23 ± 10 |
| Osteocalcin (ng/mL), median (min-max) | 11 (5–32) |
| Bone alkaline phosphatase (mg/L) | 8 ± 3.6 |
| Amino-terminal propeptide (mg/L) | 32.4 ± 15.5 |
| C-terminal telopeptide (ng/mL), median (min-max) | 0.2 (0.1–0.8) |
| OC | BALP | P1NP | CTx | |
|---|---|---|---|---|
| 25(OH)D | r = −0.3 p < 0.01 | r = −0.27 p < 0.01 | r = −0.1 p = ns | r = −0.15 p = ns |
| OC | r = 0.66 p < 0.001 | r = 0.53 p < 0.001 | r = 0.54 p < 0.001 | |
| BALP | r = 0.45 p < 0.001 | r = 0.45 p < 0.001 | ||
| P1NP | r = 0.82 p < 0.001 |
| Age | BMI | Glycemia | Insulin * | Total Cholesterol | HDL | TG | LDL | CRP | SBP | DBP | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Years | Kg/m2 | mg/dL | mUI/mL | mg/dL | mg/dL | mg/dL | mg/dL | mg/dL | mmHg | mmHg | |
| VitD (ng/mL) | r = −0.47, p < 0.001 | r = − 0.17, ns | r = −0.32, p <0.01 | r = −0.07, ns | r = 0.02, ns | r = 0.2, ns | r = −0.16, ns | r = 0.01, ns | r = 0.13, ns | r = 0.1, ns | r = 0.03, ns |
| OC (ng/mL) | r = 0.37, p < 0.001 | r = 0.02, ns | r = 0.18, ns | r = 0.32, p <0.01 | r = 0.1, ns | r = −0.15, ns | r = 0.1, ns | r = 0.05, ns | r = 0.04, ns | r = 0.06, ns | r = 0.03, ns |
| BALP (mg/L) | r = 0.3, p < 0.01 | r = 0.002, ns | r = 0.18, ns | r = 0.26, p <0.05 | r = 0.13, ns | r = −0.13, ns | r = 0.02, ns | r = 0.17, ns | r = 0.07, ns | r = 0.18, ns | r = 0.1, ns |
| P1NP (mg/L) | r = 0.05, ns | r = 0.002, ns | r = −0.13, ns | r = −0.12, ns | r = 0.12, ns | r = 0.02, ns | r = 0.07, ns | r = 0.13, ns | r = 0.05, ns | r = −0.12, ns | r = 0.02, ns |
| CTx (ng/mL) | r = 0.1, ns | r = 0.01, ns | r = 0.03, ns | r = 0.08, ns | r = 0.2, ns | r = 0.01, ns | r = 0.03, ns | r = 0.17, ns | r = 0.1,ns | r = 0.01, ns | r = 0.09, ns |
| Males | Diabetes | Hypertension | Dyslipidemia | Smoking Habit | Obesity | DST | |
|---|---|---|---|---|---|---|---|
| VitD (ng/mL) | -* | -** | -** | -** | ns | ns | ns |
| OC (ng/mL) | +* | ns | ns | ns | ns | -* | -* |
| BALP (mg/L) | ns | ns | ns | +* | ns | ns | ns |
| P1NP (mg/L) | ns | ns | ns | ns | ns | ns | -** |
| CTx (ng/mL) | ns | ns | ns | ns | ns | ns | -* |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vassalle, C.; Sabatino, L.; Cecco, P.D.; Maltinti, M.; Ndreu, R.; Maffei, S.; Pingitore, A. Relationship between Bone Health Biomarkers and Cardiovascular Risk in a General Adult Population. Diseases 2017, 5, 24. https://0-doi-org.brum.beds.ac.uk/10.3390/diseases5040024
Vassalle C, Sabatino L, Cecco PD, Maltinti M, Ndreu R, Maffei S, Pingitore A. Relationship between Bone Health Biomarkers and Cardiovascular Risk in a General Adult Population. Diseases. 2017; 5(4):24. https://0-doi-org.brum.beds.ac.uk/10.3390/diseases5040024
Chicago/Turabian StyleVassalle, Cristina, Laura Sabatino, Pietro Di Cecco, Maristella Maltinti, Rudina Ndreu, Silvia Maffei, and Alessandro Pingitore. 2017. "Relationship between Bone Health Biomarkers and Cardiovascular Risk in a General Adult Population" Diseases 5, no. 4: 24. https://0-doi-org.brum.beds.ac.uk/10.3390/diseases5040024