The Vascular Factor Plays the Main Role in the Cause of Pain in Men with Chronic Prostatitis and Chronic Pelvic Pain Syndrome: The Results of Clinical Trial on Thermobalancing Therapy


{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Methods and Results
2.1. Study Design
2.2. Participants
2.3. Evaluation
2.4. Statistical Analysis
2.5. DATD
3. Results
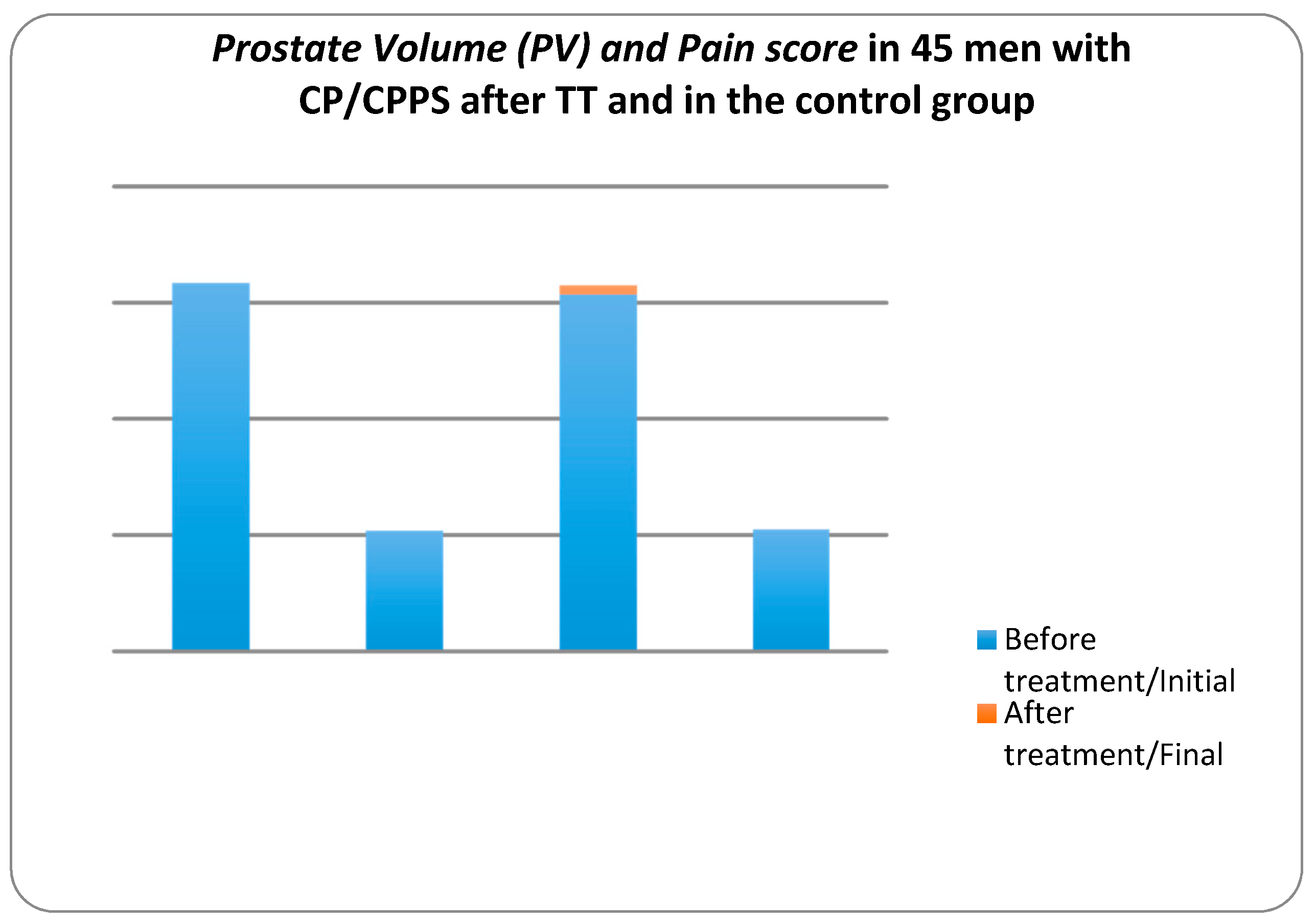
3.1. Prostate Volume and Pain Score
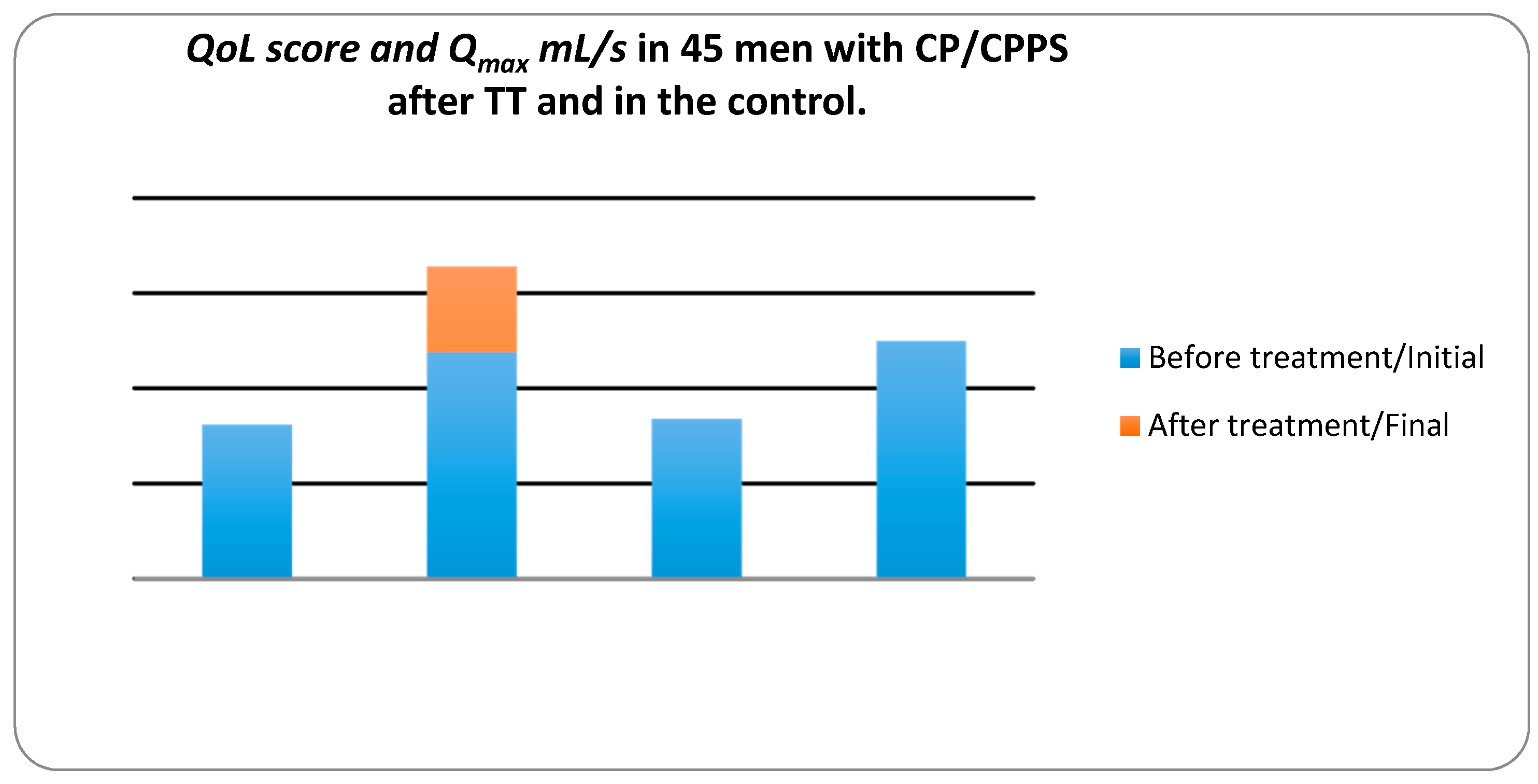
3.2. Quality of Life and Maximum Urinary Flow Rate
4. Discussions
4.1. Outcomes
4.2. Quality of Life
4.3. Prostate Volume
4.4. Etiology
4.5. Prevalence
5. Conclusions
Acknowledgments
Conflicts of Interest
References
- Nickel, J.C.; Freedland, S.J.; Castro-Santamaria, R.; Moreira, D.M. Chronic Prostate Inflammation Predicts Symptom Progression in Chronic Prostatitis/Chronic Pelvic Pain (CP/CPPS) Patients. J. Urol. 2017, 198, 122–128. [Google Scholar] [CrossRef] [PubMed]
- Arora, H.C.; Eng, C.; Shoskes, D.A. Gut microbiome and chronic prostatitis/chronic pelvic pain syndrome. Ann. Trans. Med. 2017, 5. [Google Scholar] [CrossRef] [PubMed]
- Benelli, A.; Hossain, H.; Pilatz, A.; Weidner, W. Prostatitis and its Management. Eur. Urol. Suppl. 2016. [Google Scholar] [CrossRef]
- Krsmanovic, A.; Tripp, D.A.; Nickel, J.C.; Shoskes, D.A.; Pontari, M.; Litwin, M.S.; McNaughton-Collins, M.F. Psychosocial mechanisms of the pain and quality of life relationship for chronic prostatitis/chronic pelvic pain syndrome (CP/CPPS). Can. Urol. Assoc. J. 2014, 8, 403–408. [Google Scholar] [CrossRef] [PubMed]
- Tripp, D.A.; Nickel, J.C.; Wang, Y.; Litwin, M.S.; McNaughton-Collins, M.; Landis, J.R.; Alexander, R.B.; Schaeffer, A.J.; O’Leary, M.P.; Pontari, M.A.; et al. Catastrophizing and pain-contingent rest predict patient adjustment in men with chronic prostatitis/chronic pelvic pain syndrome. J. Pain 2006, 7, 697–708. [Google Scholar] [CrossRef] [PubMed]
- Nickel, J.C.; Tripp, D.A.; Chuai, S.; Litwin, M.S.; McNaughton-Collins, M.; Landis, J.R.; Alexander, R.B.; Schaeffer, A.J.; O’Leary, M.P.; Pontari, M.A.; et al. Psychosocial variables affect the quality of life of men diagnosed with chronic prostatitis/chronic pelvic pain syndrome. BJU Int. 2007, 101, 59–64. [Google Scholar] [CrossRef] [PubMed]
- Hedelin, H.; Jonsson, K. Chronic abacterial prostatitis and cold exposure: An explorative study. Scand. J. Urol. Nephrol. 2007, 41, 430–435. [Google Scholar] [CrossRef] [PubMed]
- Bartkowski-Abbate, L.; Ariail, A.; Wood, A. Healing in Urology, Adjunct Modalities for Physical Therapy; World Scientific Publishing Co., Pte. Ltd: Singapore, 2016; Chapter 8; pp. 165–167. [Google Scholar]
- Vance, C.G.; Rakel, B.A.; Dailey, D.L.; Sluka, K.A. Skin impedance is not a factor in transcutaneous electrical nerve stimulation effectiveness. J. Pain Res. 2015, 8, 571–580. [Google Scholar] [CrossRef] [PubMed]
- Allen, S.; Aghajanyan, I. Effect of thermobalancing therapy on chronic prostatitis and chronic pelvic pain syndrome. J. Clin. Urol. 2016, 1–8. [Google Scholar] [CrossRef]
- Baldwin, A.L. A brief history of capillaries and some examples of their apparently strange behaviour. Clin. Exp. Pharmacol. Physiol. 2000, 27, 821–825. [Google Scholar] [CrossRef] [PubMed]
- Hansen-Smith, F.M. Capillary network patterning during angiogenesis. Clin. Exp. Pharmacol. Physiol. 2000, 27, 830–835. [Google Scholar] [CrossRef] [PubMed]
- Allen, S.; Adjani, A. Therapeutic Device and Method, United States Patent and Trademark Office. U.S. Patent 9,408,744 B2, 9 August 2016. Available online: https://www.google.com/patents/US9408744 (accessed on 23 September 2017).
- Allen, S.; Aghajanyan, I.G. Benign Prostatic Hyperplasia Treatment with New Physiotherapeutic Device. Urol. J. 2015, 12, 2371–2376. [Google Scholar] [PubMed]
- Allen, S.; Aghajanyan, I.G. Thermobalancing conservative treatment for moderate-to-low-degree lower urinary tract symptoms (LUTS) secondary to prostate enlargement. Cogent Med. 2016, 3, 1195067. [Google Scholar] [CrossRef]
- Chung, S.D.; Lin, H.C. Association between chronic prostatitis/chronic pelvic pain syndrome and anxiety disorder: A population-based study. PLoS ONE 2013, 8, e64630. [Google Scholar] [CrossRef] [PubMed]
- Lamph, S. Regulation of medical devices outside the European Union. J. R. Soc. Med. 2012, 105, 186–188. [Google Scholar] [CrossRef] [PubMed]
- Allen, S. The Origin of Chronic Diseases Can Be in Capillary Pathology: An Evidence from Clinical Trials on Thermobalancing Treatment of Prostate Reveals. Achiev. Life Sci. 2016, 10, 197–202. [Google Scholar] [CrossRef]
- Mehik, A.; Leskinen, M.J.; Hellström, P. Mechanisms of pain in chronic pelvic pain syndrome: Influence of prostatic inflammation. World J. Urol. 2003, 21–22, 90–94. [Google Scholar] [CrossRef] [PubMed]
- Turner, J.A.; Hauge, S.; VonKorff, M.; Saunders, K.; Lowe, M.; Berger, R. Primary care and urology patients with male pelvic pain syndrome: Symptoms and quality of life. J. Urol. 2002, 167, 1768–1773. [Google Scholar] [CrossRef]
- Ku, J.A.H.; Kwak, C.; Oh, S.-J.; Lee, E.; Lee, S.E.; Paick, J.-S. Influence of pain and urinary symptoms on quality of life in young men with chronic prostatitis-like symptoms. Int. J. Urol. 2004, 11, 489–493. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Zheng, T.; Tu, X.A.; Chen, X.; Wang, Z.; Chen, S.; Yang, Q.; Wan, Z.; Han, D.; Xiao, H.; et al. Erectile Dysfunction in Chronic Prostatitis/Chronic Pelvic Pain Syndrome: Outcomes from a Multi-Center Study and Risk Factor Analysis in a Single Center. PLoS ONE 2016, 11, e0153054. [Google Scholar] [CrossRef]
- McNaughton Collins, M.; Pontari, M.A.; O’leary, M.P.; Calhoun, E.A.; Santanna, J.; Landis, J.R.; Kusek, J.W.; Litwin, M.S. Quality of life is impaired in men with chronic prostatitis: Results from the NIH Cohort Study. J. Gen. Intern. Med. 2001, 16, 656–662. [Google Scholar] [CrossRef] [PubMed]
- Kwon, J.K.; Chang, I.H. Pain, Catastrophizing, and Depression in Chronic Prostatitis/Chronic Pelvic Pain Syndrome. Int. Neurourol. J. 2013, 17, 48–58. [Google Scholar] [CrossRef] [PubMed]
- Aghajanyan, I.G.; Allen, S. Positive Response to Thermobalancing Therapy Enabled by Therapeutic Device in Men with Non-Malignant Prostate Diseases: BPH and Chronic Prostatitis. Diseases 2016, 4, 18. [Google Scholar] [CrossRef] [PubMed]
- Nickel, J.C. Recommendations for the evaluation of patients with prostatitis. World J. Urol. 2003, 21, 75–81. [Google Scholar] [CrossRef] [PubMed]
- Shukla-Dave, A.; Hricak, H.; Eberhardt, S.C.; Olgac, S.; Muruganandham, M.; Scardino, P.T.; Reuter, V.E.; Koutcher, J.A.; Zakian, K.L. Chronic Prostatitis: MR Imaging and 1H MR Spectroscopic Imaging Findings—Initial Observations. Radiology 2004, 231, 717–724. [Google Scholar] [CrossRef] [PubMed]
- Franiel, T.; Lüdemann, L.; Rudolph, B.; Rehbein, H.; Staack, A.; Taupitz, M.; Prochnow, D.; Beyersdorff, D. Evaluation of normal prostate tissue, chronic prostatitis, and prostate cancer by quantitative perfusion analysis using a dynamic contrast-enhanced inversion-prepared dual-contrast gradient echo sequence. Investig. Radiol. 2008, 43, 481–487. [Google Scholar] [CrossRef] [PubMed]
- Sah, V.K.; Wang, L.; Min, X.; Fen, Z.; Rizal, R.; Li, L.; Deng, M.; Liu, J.; Li, H. Multiparametric MR imaging in diagnosis of chronic prostatitis and its differentiation from prostate cancer. Radiol. Infect. Dis. 2015, 1, 70–77. [Google Scholar] [CrossRef]
- Murphy, A.B.; Macejko, A.; Taylor, A.; Nadler, R.B. Chronic Prostatitis, Management Strategies. Drugs 2009, 69, 71–84. [Google Scholar] [CrossRef] [PubMed]
- Allen, S.; Aghajanyan, I.G. New independent thermobalancing treatment with therapeutic device for internal diseases: Chronic prostatitis and chronic pelvic pain syndrome. Nephrourol. Mon. 2017, e44694. [Google Scholar] [CrossRef]
- Cho, I.C.; Min, S.K. Proposed new pathophysiology of chronic prostatitis/chronic pelvic pain syndrome. Urogenit. Tract Infect. 2015, 10, 92–101. [Google Scholar] [CrossRef]
- Cho, I.R.; Keener, T.S.; Nghiem, H.V.; Winter, T.; Krieger, J.N. Prostate blood flow characteristics in the chronic prostatitis/pelvic pain syndrome. J. Urol. 2000, 163, 1130–1133. [Google Scholar] [CrossRef]
- Kogan, M.I.; Belousov, I.I.; Bolotskov, A.S. Arterial blood flow in the prostate in the syndrome of chronic pelvic pain/chronic prostatitis. Urologiia 2011, 3, 22–28. [Google Scholar]
- Shoskes, D.A.; Prots, D.; Karns, J.; Horhn, J.; Shoskes, A.S. Greater endothelial dysfunction and arterial stiffness in men with chronic prostatitis/chronic pelvic pain syndrome—A possible link to cardiovascular disease. J. Urol. 2011, 186, 907–910. [Google Scholar] [CrossRef] [PubMed]
- Allen, S.; Aghajanyan, I.G. Efficacy of Thermobalancing therapy for chronic prostatitis/chronic pelvic pain syndrome, confirmed by clinical study, may suggest ethology and pathophysiology of this disease. Can. Urol. Assoc. J. 2017, 11. [Google Scholar] [CrossRef] [PubMed]
- Allen, S.; Aghajanyan, I.G. Use of thermobalancing therapy in ageing male with benign prostatic hyperplasia with a focus on etiology and pathophysiology. Aging Male 2016, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Chung, S.-D.; Lin, H.-C. Association between Chronic Prostatitis/Chronic Pelvic Pain Syndrome and Anxiety Disorder: A Population-Based Study. PLoS ONE 2013, 8, e64630. [Google Scholar] [CrossRef] [PubMed]
- Magistro, G.; Wagenlehner, F.M.; Grabe, M.; Weidner, W.; Stief, C.G.; Nickel, J.C. Contemporary management of chronic prostatitis/chronic pelvic pain syndrome. Eur. Urol. 2016, 69, 286–297. [Google Scholar] [CrossRef] [PubMed]
- Bajpayee, P.; Kumar, K.; Sharma, S.; Maurya, N.; Kumar, P.; Singh, R.; Lal, C. Prostatitis: Prevalence, health impact and quality improvement strategies. Acta Poloniae Pharm. 2012, 69, 571–579. [Google Scholar] [PubMed]
- Tran, C.N.; Shoskes, D.A. Sexual dysfunction in chronic prostatitis/chronic pelvic pain syndrome. World J. Urol. 2013, 31, 741–746. [Google Scholar] [CrossRef] [PubMed]
- Fu, W.; Zhou, Z.; Liu, S.; Li, Q.; Yao, J.; Li, W.; Yan, J. The Effect of Chronic Prostatitis/Chronic Pelvic Pain Syndrome (CP/CPPS) on Semen Parameters in Human Males: A Systematic Review and Meta-Analysis. PLoS ONE 2014, 9, e94991. [Google Scholar] [CrossRef] [PubMed]



© 2017 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Allen, S. The Vascular Factor Plays the Main Role in the Cause of Pain in Men with Chronic Prostatitis and Chronic Pelvic Pain Syndrome: The Results of Clinical Trial on Thermobalancing Therapy. Diseases 2017, 5, 25. https://0-doi-org.brum.beds.ac.uk/10.3390/diseases5040025
Allen S. The Vascular Factor Plays the Main Role in the Cause of Pain in Men with Chronic Prostatitis and Chronic Pelvic Pain Syndrome: The Results of Clinical Trial on Thermobalancing Therapy. Diseases. 2017; 5(4):25. https://0-doi-org.brum.beds.ac.uk/10.3390/diseases5040025
Chicago/Turabian StyleAllen, Simon. 2017. "The Vascular Factor Plays the Main Role in the Cause of Pain in Men with Chronic Prostatitis and Chronic Pelvic Pain Syndrome: The Results of Clinical Trial on Thermobalancing Therapy" Diseases 5, no. 4: 25. https://0-doi-org.brum.beds.ac.uk/10.3390/diseases5040025