Histoplasma and Cytomegalovirus Coinfection of the Gastrointestinal Tract in a Patient with AIDS: A Case Report and Review of the Literature



Abstract
:1. Introduction
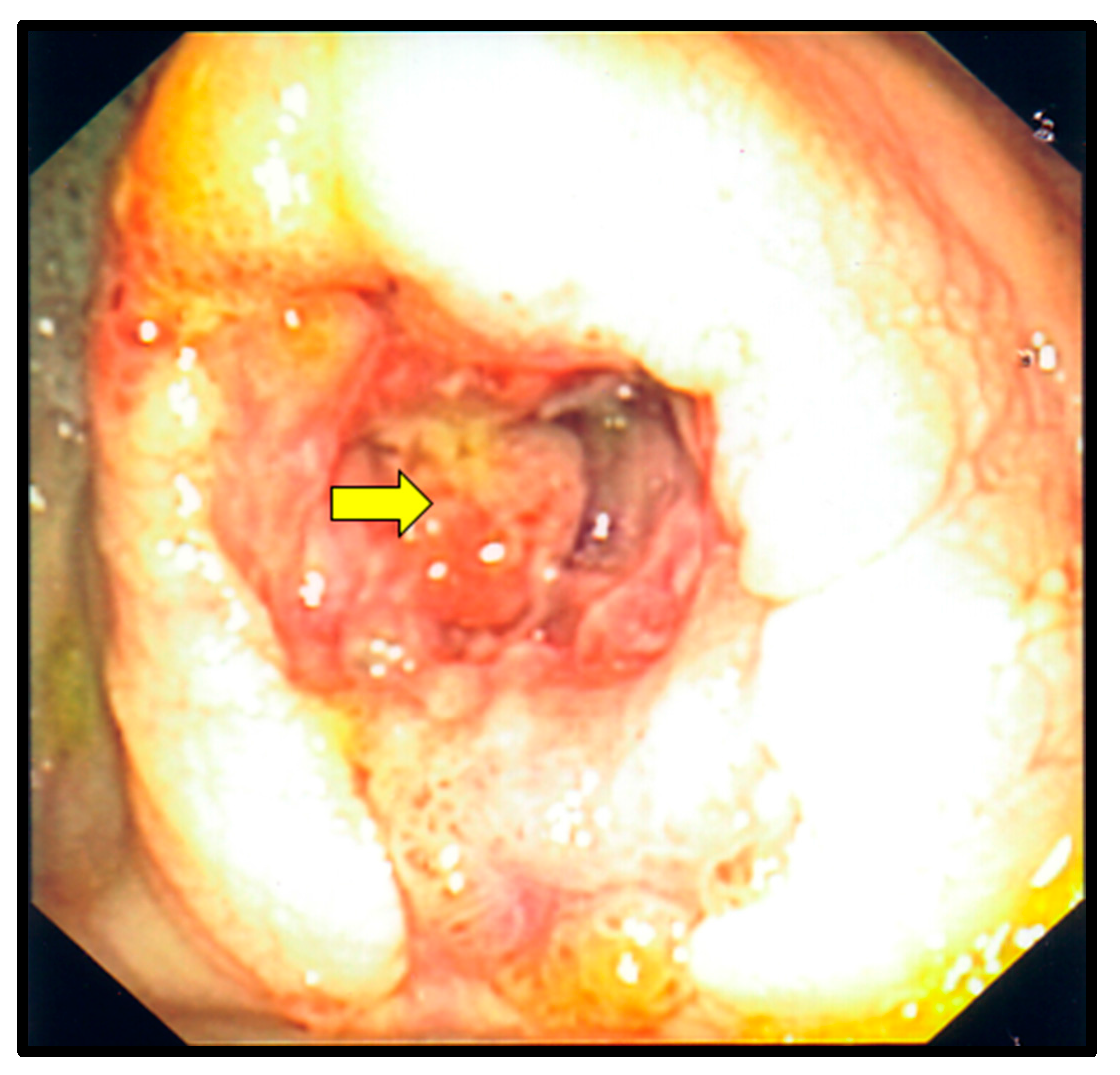
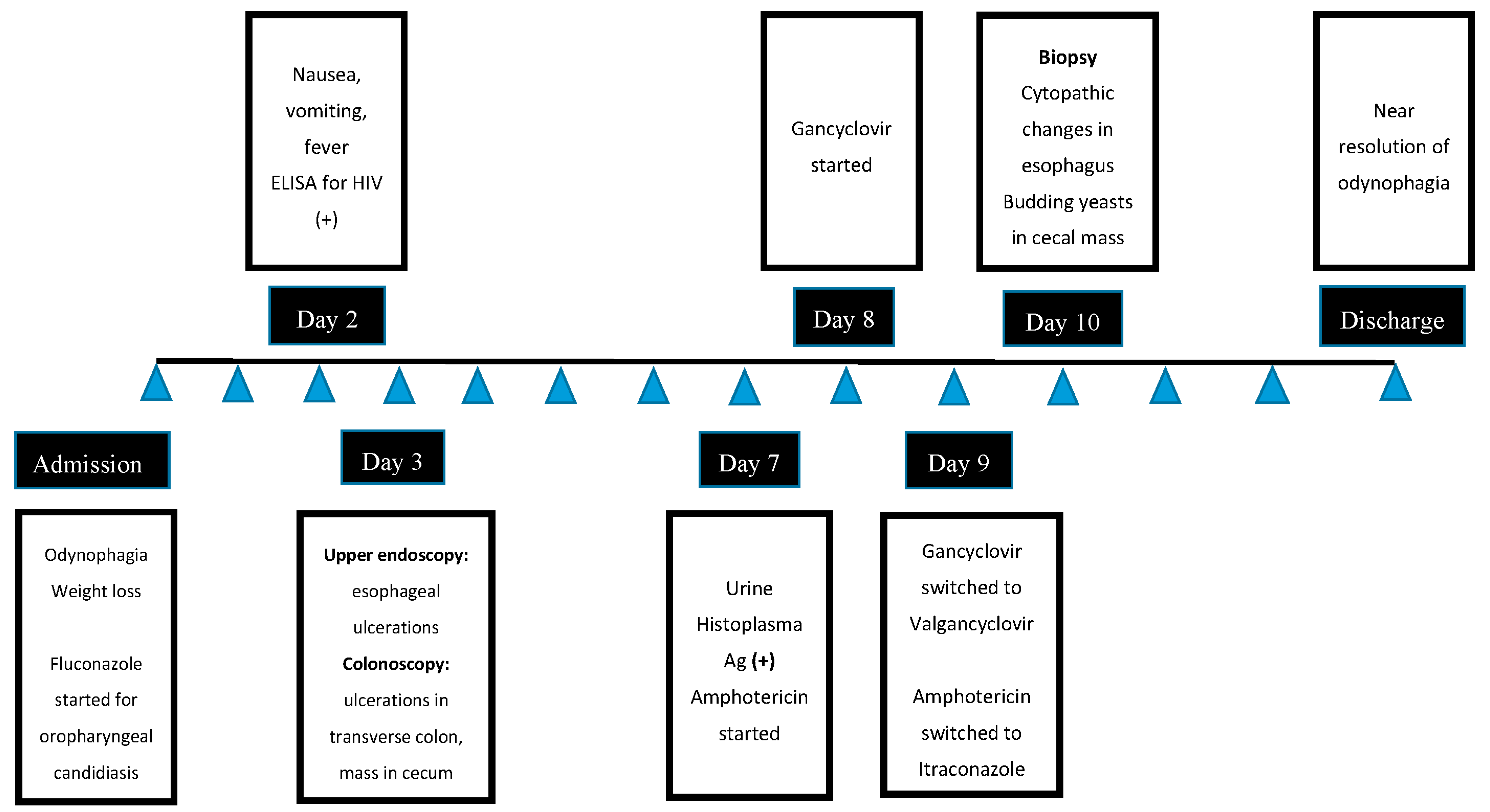
2. Case Description
3. Discussion
4. Conclusions
Conflicts of Interest
Human/Animal Rights
Informed Consent
References
- Boaitey, Y.A.; Nkrumah, B.; Idriss, A.; Tay, S.C. Gastrointestinal and urinary tract pathogenic infections among HIV seropositive patients at the Komfo Anokye Teaching Hospital in Ghana. BMC Res. Notes 2012, 5, 454. [Google Scholar] [CrossRef] [PubMed]
- Assi, M.; McKinsey, D.S.; Driks, M.R.; O’Connor, M.C.; Bonacini, M.; Graham, B.; Manian, F. Gastrointestinal histoplasmosis in the acquired immunodeficiency syndrome: Report of 18 cases and literature review. Diagn. Microbiol. Infect. Dis. 2006, 55, 195–201. [Google Scholar] [CrossRef] [PubMed]
- Wheat, L.J.; Connolly-Stringfield, P.A.; Baker, R.L.; Curfman, M.F.; Eads, M.E.; Israel, K.S.; Norris, S.A.; Webb, D.H.; Zeckel, M.L. Disseminated histoplasmosis in the acquired immune deficiency syndrome: clinical findings, diagnosis and treatment, and review of the literature. Medicine 1990, 69, 361–374. [Google Scholar] [CrossRef] [PubMed]
- Gallant, J.E.; Moore, R.D.; Richman, D.D.; Keruly, J.; Chaisson, R.E. Incidence and natural history of cytomegalovirus disease in patients with advanced human immunodeficiency virus disease treated with zidovudine. The Zidovudine Epidemiology Study Group. J. Infect. Dis. 1992, 166, 1223–1227. [Google Scholar] [CrossRef] [PubMed]
- Suh, K.N.; Anekthananon, T.; Mariuz, P.R. Gastrointestinal histoplasmosis in patients with AIDS: Case report and review. Clin. Infect. Dis. 2001, 32, 483–491. [Google Scholar] [CrossRef] [PubMed]
- Salzberger, B.; Hartmann, P.; Hanses, F.; Uyanik, B.; Cornely, O.A.; Wöhrmann, A.; Fätkenheuer, G. Incidence and prognosis of CMV disease in HIV-infected patients before and after introduction of combination antiretroviral therapy. Infect. 2005, 33, 345–349. [Google Scholar] [CrossRef] [PubMed]
- Huppmann, A.R.; Orenstein, J.M. Opportunistic disorders of the gastrointestinal tract in the age of highly active antiretroviral therapy. Hum. Pathol. 2010, 41, 1777–1787. [Google Scholar] [CrossRef] [PubMed]
- Orenstein, J.M.; Dieterich, D.T. The histopathology of 103 consecutive colonoscopy biopsies from 82 symptomatic patients with acquired immunodeficiency syndrome: Original and look-back diagnoses. Arch. Pathol. Lab. Med. 2001, 125, 1042–1046. [Google Scholar] [PubMed]
- Jones, A.C.; Migliorati, C.A.; Baughman, R.A. The simultaneous occurrence of oral herpes simplex virus, cytomegalovirus, and histoplasmosis in an HIV-infected patient. Oral Surg. Oral Med. Oral Pathol. 1992, 74, 334–339. [Google Scholar] [CrossRef]
- Fan, X.; Scott, L.; Qiu, S.; Raju, G.S.; Shabot, M. Colonic coinfection of histoplasma and cytomegalovirus mimicking carcinoma in a patient with HIV/AIDS. Gastrointest. Endosc. 2008, 67, 977–978. [Google Scholar] [CrossRef] [PubMed]
- Khara, H.; Mysior, J.; Metwally, M.; Provost, J.; Bakr, M.; Adelmann, C.; Riback, H.; Sammarco, F. Disseminated histoplasmosis and CMV colitides coinfection in AIDS. Am. J. Gastroenterol. 2013, 108 (Supp. 1), S413. [Google Scholar]
- Bruno, M.A.; Parodi, M.; Olmedo, I.; Picón Molina, H.; Palencia, R.; Doniquian, A. Massive gastrointestinal bleeding in AIDS patients secondary to histoplasma and cytomegalovirus infection. Int. J. Surg. Case Rep. 2016, 25, 128–131. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient | Report | Age | Sex | Symptoms | CD4 Count (Cells/uL) | Affected GI * Area by Histoplasma | Affected GI Area by CMV | Type of GI Lesions | Extraintestinal Organs Involved | Outcome |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Jones et al (1992) [2] | 51 | M | Painful oral ulcerations | Unknown | Oral mucosa | Oral mucosa, stomach | Ulcerations | Lungs, adrenal glands, spleen a | Died |
| 2 | Fan X et al. (2008) [3] | 45 | M | Abdominal pain, weight loss, fever | 17 | Ascending colon | Ascending colon | Mass | None | Unknown |
| 3 | Khara H et al. (2013) [4] | 41 | M | Diarrhea, weight loss, fever | 31 | Descending colon | Descending colon | Ulcerations | None | Survived |
| 4 | Bruno MA et al. (2016) [5] | 40 | M | Odynophagia, cough, night sweats, dyspnea, GI bleeding | 8 | Ileum | Ileum | Mass | Lungs b | Survived |
| 5 | Present report | 31 | M | Odynophagia, weight loss | 20 | Cecum, transverse colon | Esophagus, transverse colon | Mass, ulcerations | None | Survived |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gonzales Zamora, J.A.; Espinoza, L.A. Histoplasma and Cytomegalovirus Coinfection of the Gastrointestinal Tract in a Patient with AIDS: A Case Report and Review of the Literature. Diseases 2017, 5, 30. https://0-doi-org.brum.beds.ac.uk/10.3390/diseases5040030
Gonzales Zamora JA, Espinoza LA. Histoplasma and Cytomegalovirus Coinfection of the Gastrointestinal Tract in a Patient with AIDS: A Case Report and Review of the Literature. Diseases. 2017; 5(4):30. https://0-doi-org.brum.beds.ac.uk/10.3390/diseases5040030
Chicago/Turabian StyleGonzales Zamora, Jose Armando, and Luis Alberto Espinoza. 2017. "Histoplasma and Cytomegalovirus Coinfection of the Gastrointestinal Tract in a Patient with AIDS: A Case Report and Review of the Literature" Diseases 5, no. 4: 30. https://0-doi-org.brum.beds.ac.uk/10.3390/diseases5040030