Newly Reported Studies on the Increase in Gastrointestinal Symptom Prevalence with COVID-19 Infection: A Comprehensive Systematic Review and Meta-Analysis

 , ,
, ,  and
and
Abstract
:1. Introduction
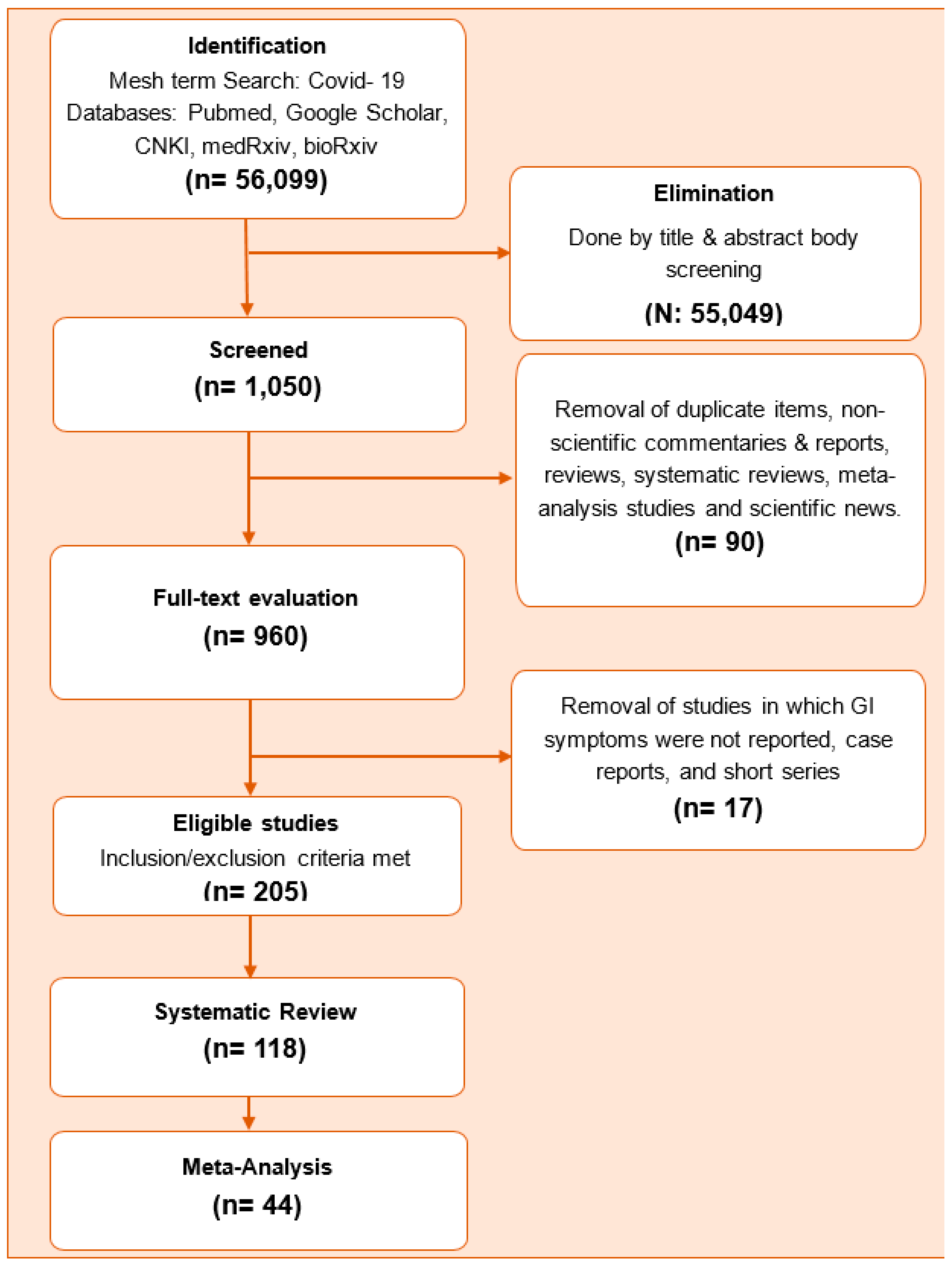
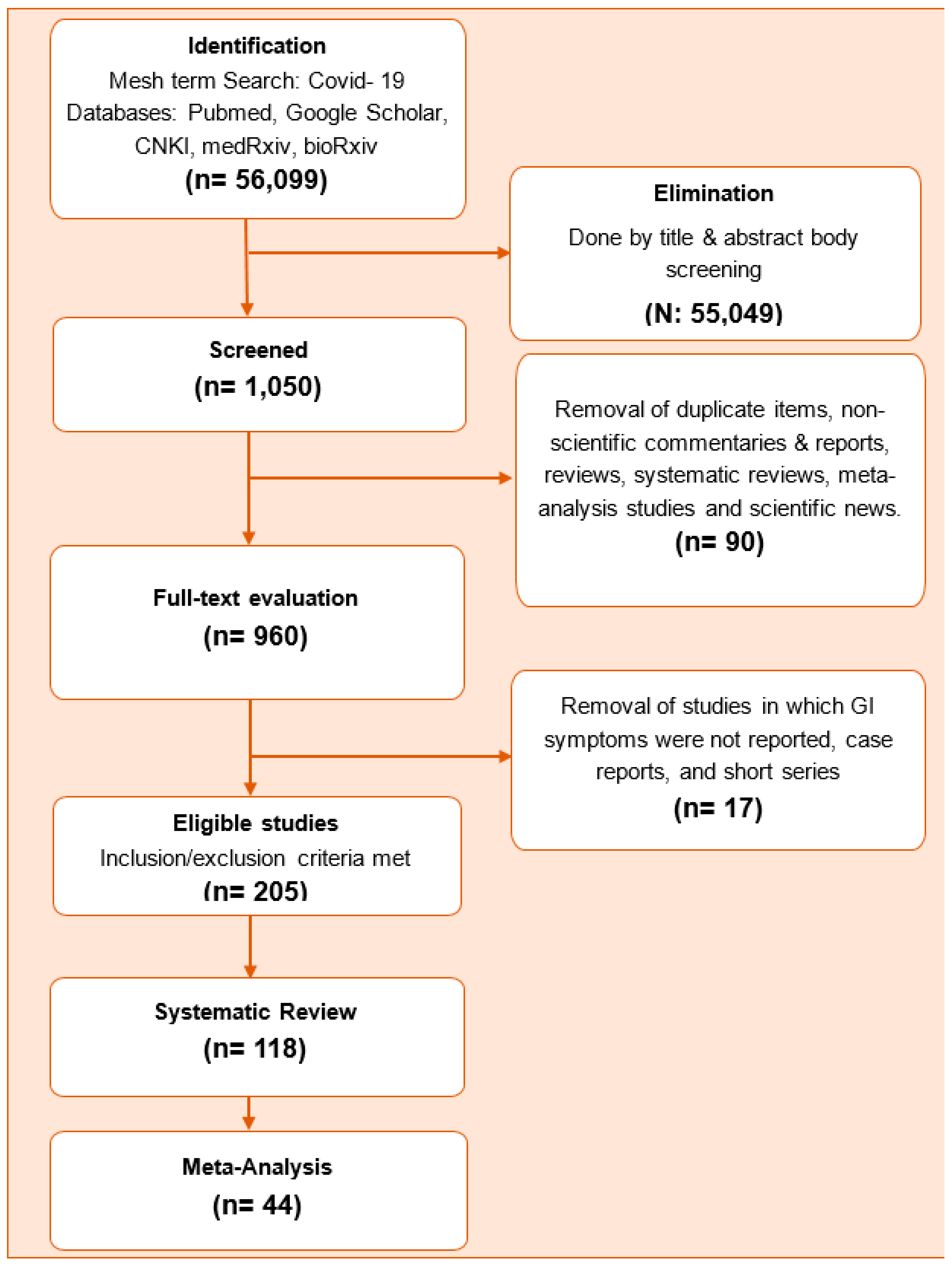
2. Methods
- (1)
- Term 1: COVID-19(supplementary concept).
- (2)
- Term 2: Severe acute respiratory syndrome Coronavirus 2 (supplementary concept).
- (1)
- Any study including data of “COVID-19 documented patients” which was defined as patients with relevant clinical manifestations and radiologic findings of COVID-19 infection, plus PCR and/or antigen test for COVID-19 infection positivity.
- (2)
- Any study reporting respiratory and GI symptoms of “documented COVID-19 infection” (as defined above) was included.
- (3)
- Authors that clearly reported the absence of GI symptoms were also included in this study.
- (1)
- If the index study included non-documented or suspected COVID-19 infection data.
- (2)
- If the presence or absence of GI symptoms was not reported.
- (3)
- Non-scientific commentaries and reports, reviews, meta-analysis studies, and scientific news.
- Authors’ names;
- Title of the manuscript;
- Study language: no language restriction was done;
- Place of study: where the study population’s data were collected and not where they were published;
- Study date: beginning and end period of study period;
- Number of patients included: study population;
- Age (mean or median (± 1 SD or IQR); range);
- Age related type of the study: we separated the studies according to age groups since age data were significantly heterogeneous;
- Pediatric studies: 0–14 years;
- Mixed studies: studies including both children and adults, adult studies of 15 years or higher;
- Male: number and percentage of male subjects included in the study
3. Statistical Analysis
4. Results
5. Discussion
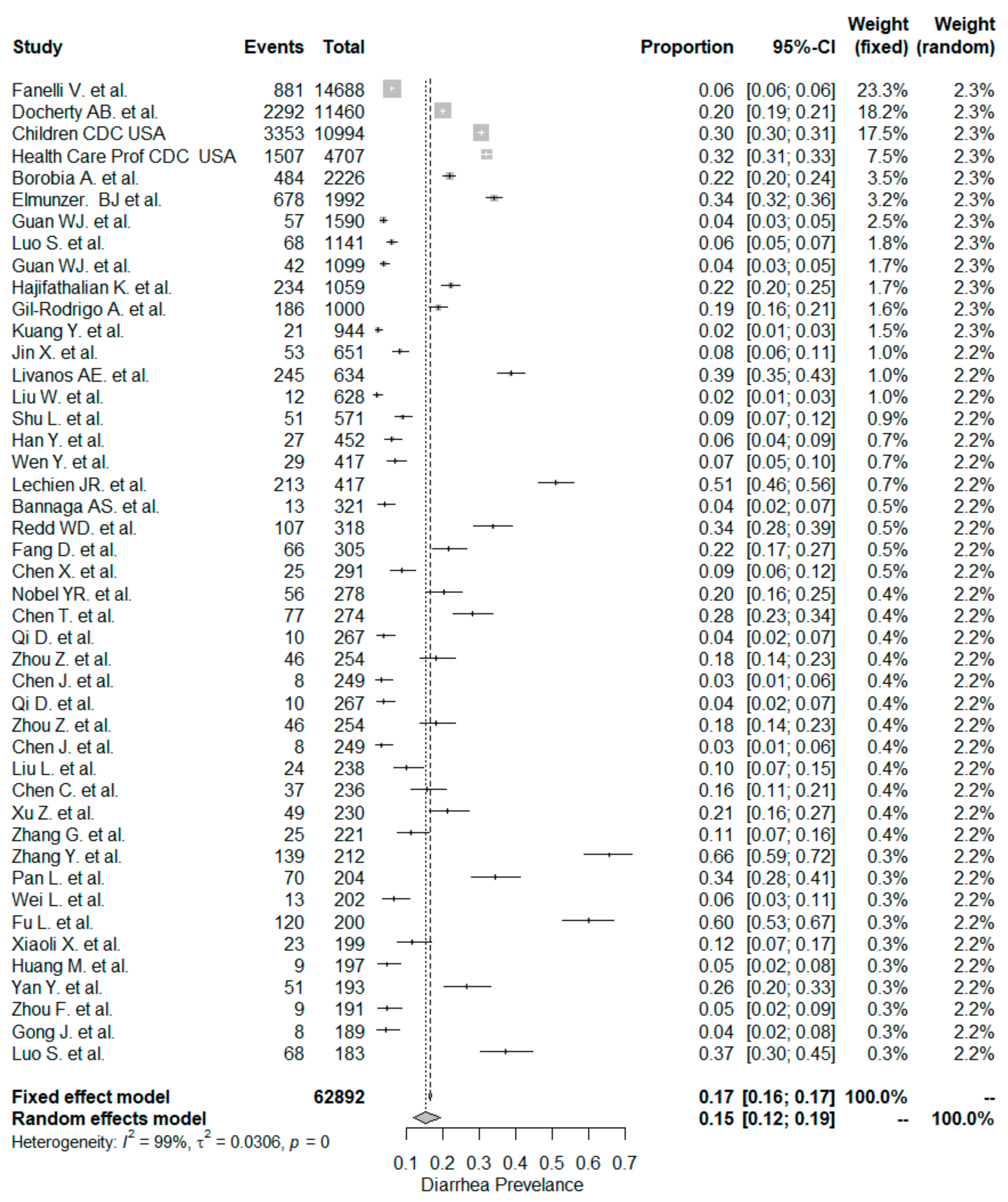
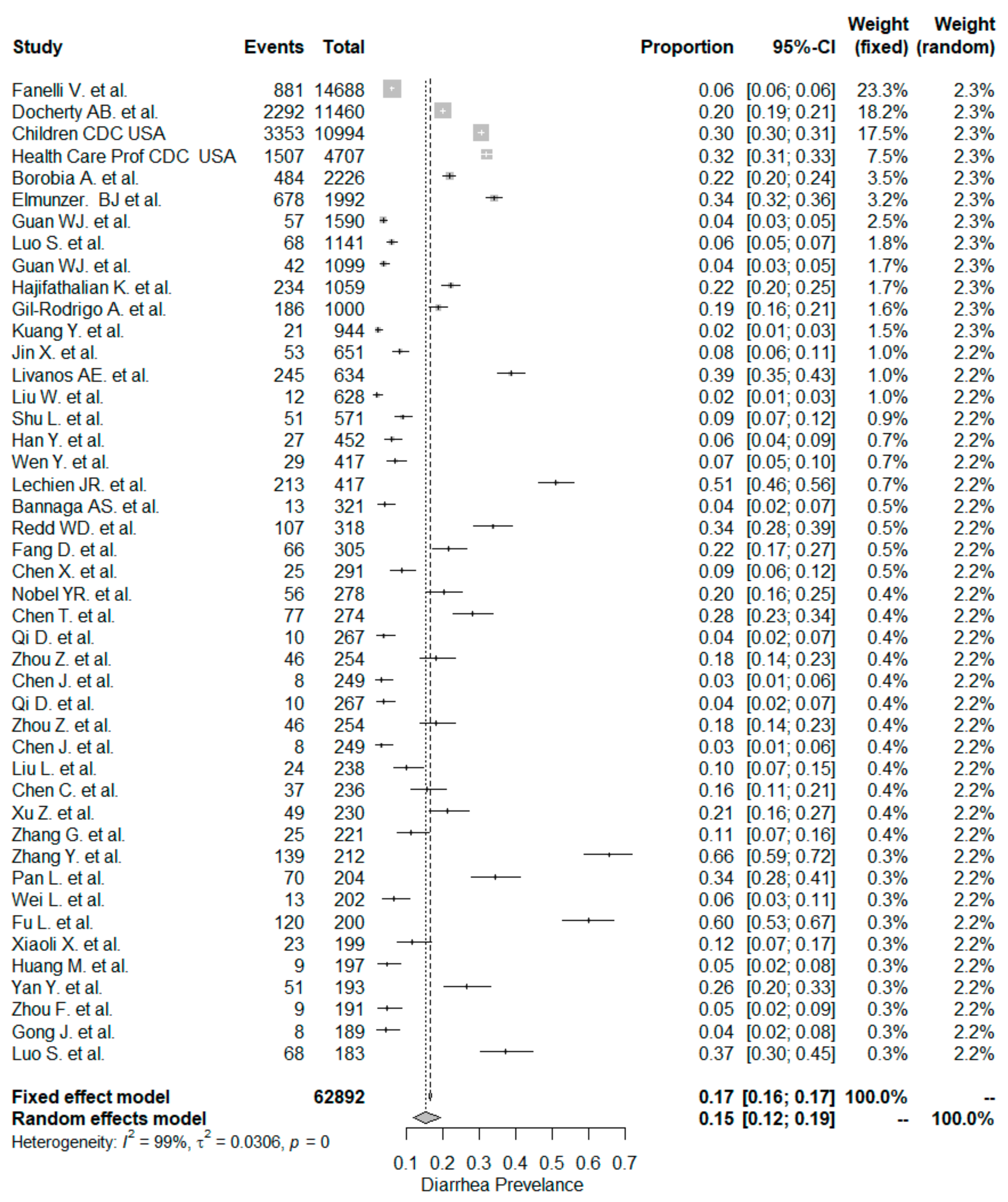
5.1. Diarrhea
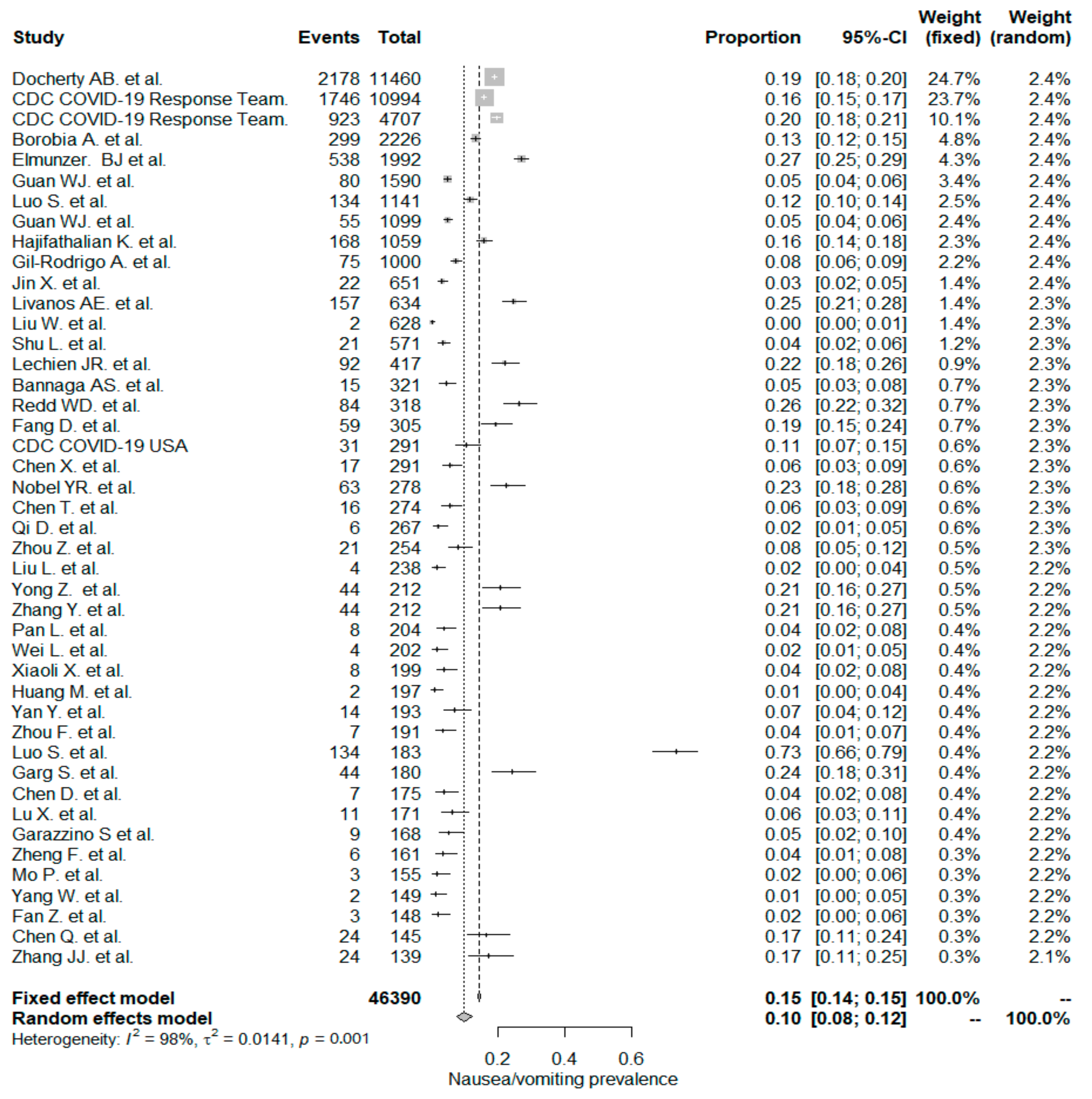
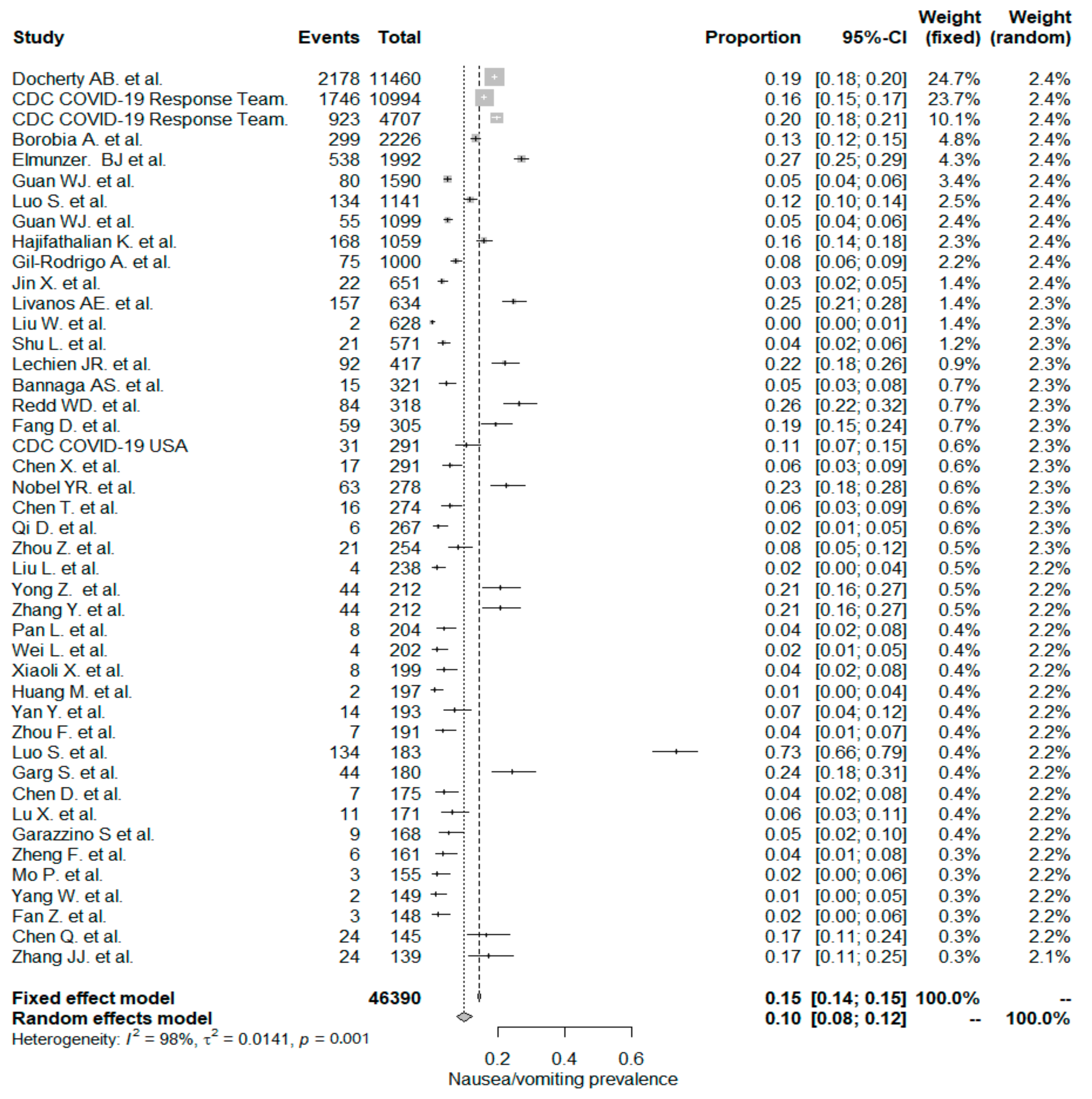
5.2. Nausea/Vomiting
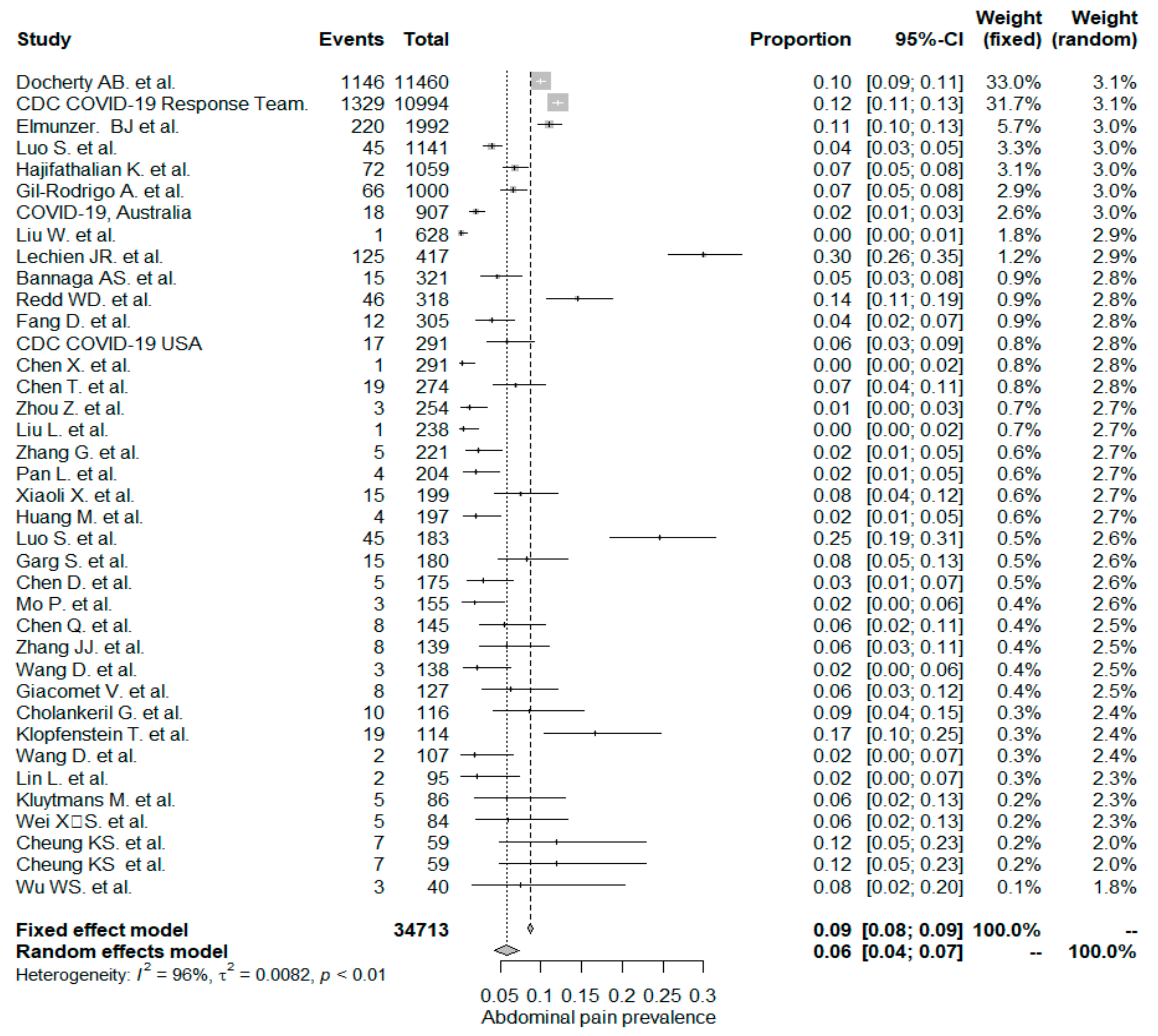
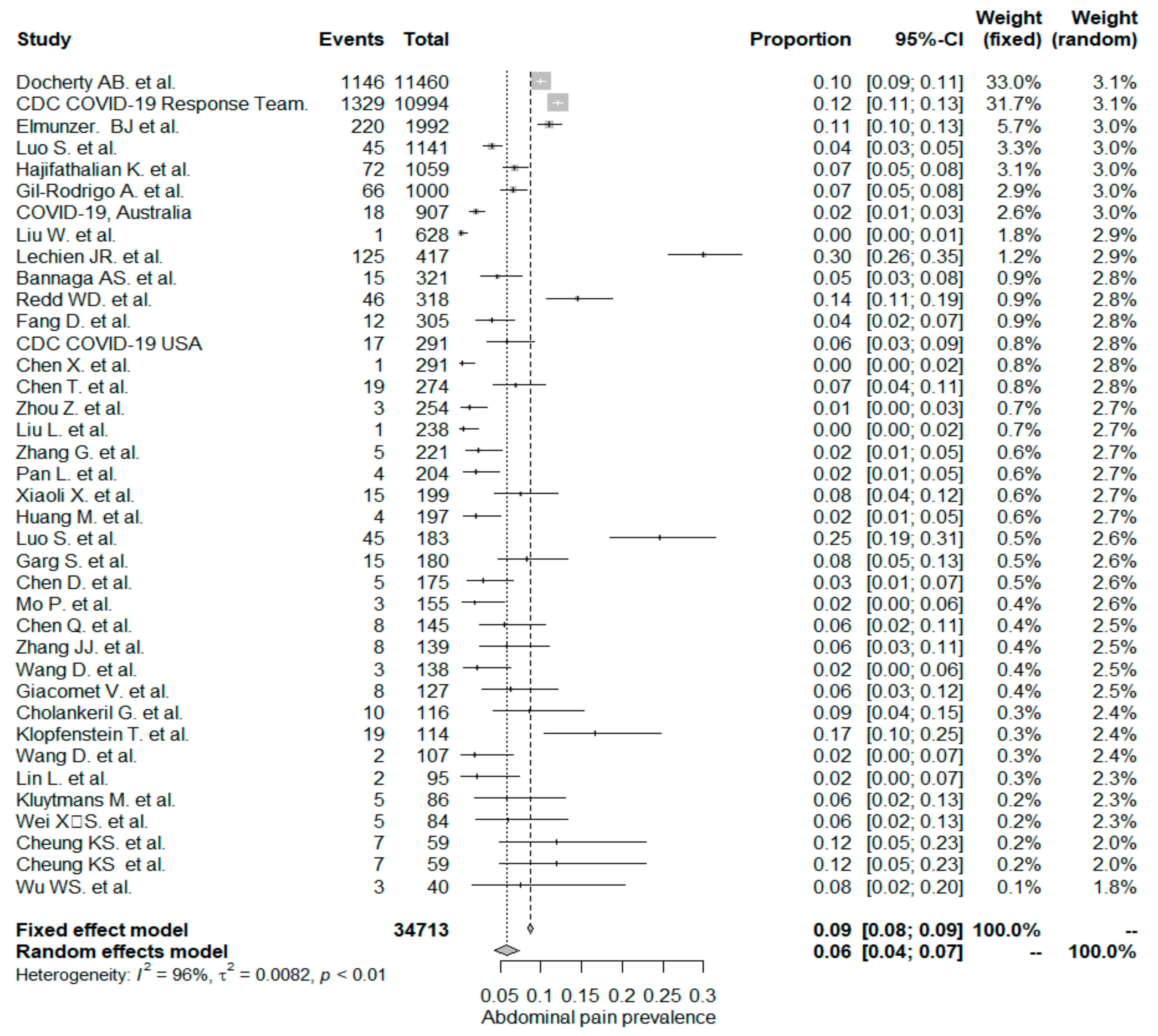
5.3. Abdominal Pain/Discomfort
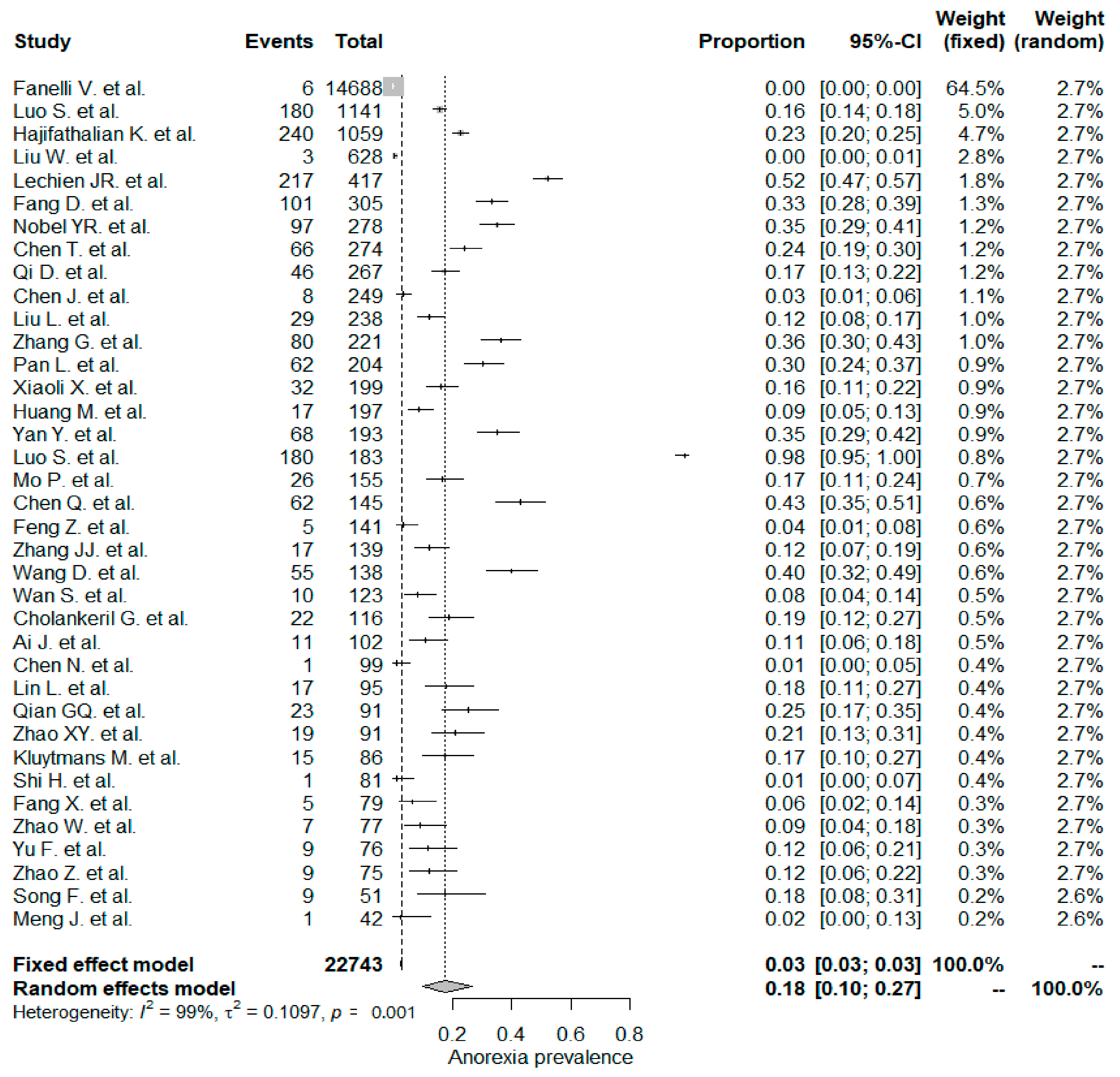
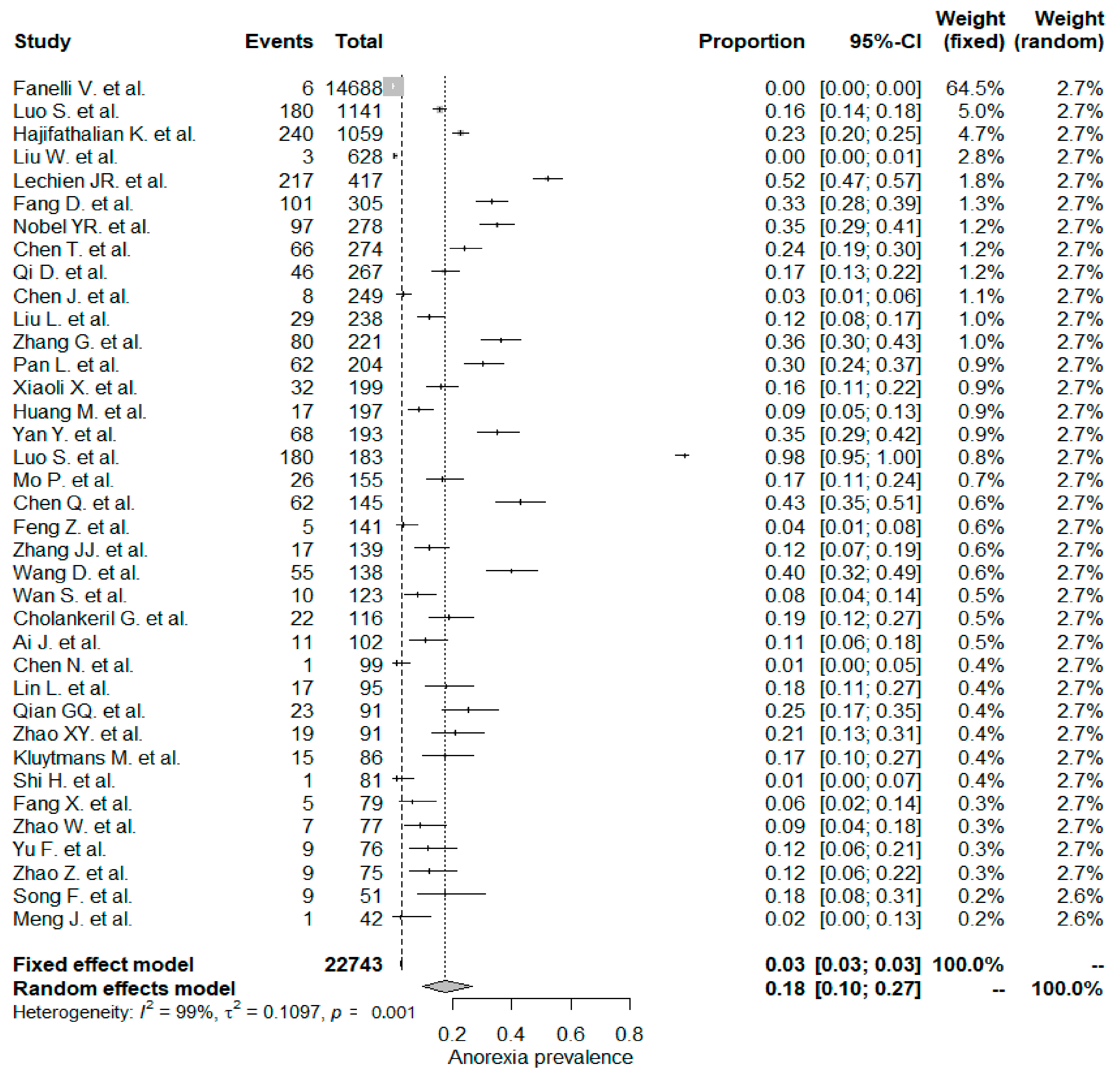
5.4. Anorexia
5.5. Limitations
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Guan, W.J.; Ni, Z.Y.; Hu, Y.; Liang, W.H.; Ou, C.Q.; He, J.X.; Liu, L.; Shan, H.; Lei, C.L.; Hui, D.S.C.; et al. Clinical Characteristics of Coronavirus Disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef] [PubMed]
- Andersen, K.G.; Rambaut, A.; Lipkin, W.I.; Holmes, E.C.; Garry, R.F. The proximal origin of SARS-CoV-2. Nat. Med. 2020, 26, 450–452. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO. COVID-19 Update (25 September 2020). Wkly. Epidemiol. Rec. 2020, 95, 461–476. [Google Scholar]
- Xiao, F.; Tang, M.; Zheng, X.; Liu, Y.; Li, X.; Shan, H. Evidence for Gastrointestinal Infection of SARS-CoV-2. Gastroenterology 2020, 158, 1831–1833. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, M.; Kleine-Weber, H.; Krüger, N.; Müller, M.; Drosten, C.; Pöhlmann, S. The novel coronavirus 2019 (2019-nCoV) uses the SARS-coronavirus receptor ACE2 and the cellular protease TMPRSS2 for entry into target cells. bioRxiv 2020. [Google Scholar] [CrossRef] [Green Version]
- WHO. WHO issues consensus document on the epidemiology of SARS. Wkly Epidemiol. Rec. Relev. Épidémiol. Hebd. 2003, 78, 373–375. [Google Scholar]
- Gu, J.; Han, B.; Wang, J. COVID-19: Gastrointestinal Manifestations and Potential Fecal-Oral Transmission. Gastroenterology 2020, 158, 1518–1519. [Google Scholar] [CrossRef]
- National Health Commission of the People’s Republic of China. Diagnosis and Treatment Plan for Pneumonia Infected by New Coronavirus (TrialSixthEdition)[EB/OL]. Available online: http://www.nhc.gov.cn (accessed on 2 August 2020).
- Docherty, A.B.; Green, C.A. Featuresof 16, 749 hospitalised UK patients with COVID-19 using the ISARIC WHO Clinical Characterization Protocol. MedRvix 2020. [Google Scholar] [CrossRef]
- Fanelli, V.; Fiorentino, M.; Cantaluppi, V.; Gesualdo, L.; Stallone, G.; Ronco, C.; Castellano, G. Acute kidney injury in SARS-CoV-2 infected patients. Crit. Care 2020, 24, 155. [Google Scholar] [CrossRef] [Green Version]
- CDC COVID-19 Response Team. Coronavirus Disease 2019 in Children-UnitedStates, February12-April2, 2020. Mmwr. Morb. Mortal. Wkly Rep. 2020, 69, 422–426. [Google Scholar] [CrossRef]
- CDC COVID-19 Response Team. Characteristics of Health Care Personnel with COVID-19-UnitedStates, February12-April9, 2020. Mmwr. Morb. Mortal. Wkly Rep. 2020, 69, 477–481. [Google Scholar] [CrossRef] [Green Version]
- Casas-Rojo, J.M.; Antón-Santos, J.M.; Millán-Núñez-Cortés, J.; Lumbreras-Bermejo, C.; Ramos-Rincón, J.M.; Roy-Vallejo, E.; Artero-Mora, A.; Arnalich-Fernández, F.; García-Bruñén, J.M.; Vargas-Núñez, J.A.; et al. Clinical characteristics of patients hospitalized with COVID-19 in Spain: Results from the SEMI-COVID-19 Registry. Rev. Clin. Esp. 2020, 10, 1016. [Google Scholar] [CrossRef]
- Borobia, A.M.; Carcas, A.J.; Arnalich, F.; Álvarez-Sala, R.; Monserrat-Villatoro, J.; Quintana, M.; Figueira, J.C.; Torres Santos-Olmo, R.M.; García-Rodríguez, J.; Martín-Vega, A.; et al. A Cohort of Patients with COVID-19 in a Major Teaching Hospital in Europe. J. Clin. Med. 2020, 9, 1733. [Google Scholar] [CrossRef] [PubMed]
- Elmunzer, B.J.; Spitzer, R.L.; Foster, L.D.; Merchant, A.A.; Howard, E.F.; Patel, V.A.; West, M.K.; Qayad, E.; Nustas, R.; Zakaria, A.; et al. Digestive Manifestations in Patients Hospitalized with COVID-19. MedRxiv 2020. [Google Scholar] [CrossRef] [PubMed]
- Guan, W.J.; Liang, W.H.; Zhao, Y.; Liang, H.R.; Chen, Z.S.; Li, Y.M.; Liu, X.Q.; Chen, R.C.; Tang, C.L.; Wang, T.; et al. Comorbidity and its impact on 1590 patients with COVID-19 in China: A nationwide analysis. Eur. Respir. J. 2020, 55, 547–557. [Google Scholar] [CrossRef] [Green Version]
- Luo, S.; Zhang, X.; Xu, H. Don’t Overlook Digestive Symptoms in Patients With 2019 Novel Coronavirus Disease (COVID-19). Clin. Gastroenterol. Hepatol. 2020, 18, 1636–1637. [Google Scholar] [CrossRef]
- Cheng, J.L.; Huang, C.; Zhang, G.J.; Liu, D.W.; Li, P.; Lu, C.Y.; Li, J. Epidemiological characteristics of novel coronavirus pneumonia in Henan. Zhonghua Jie He He Hu Xi Za Zhi 2020, 43, 327–331. [Google Scholar] [CrossRef]
- Hajifathalian, K.; Krisko, T.; Mehta, A.; Kumar, S.; Schwartz, R.; Fortune, B.; Sharaiha, R.Z. Gastrointestinal and Hepatic Manifestations of 2019 Novel Coronavirus Disease in a Large Cohort of Infected Patients From New York: Clinical Implications. Gastroenterology 2020, 159, 1137–1140. [Google Scholar] [CrossRef]
- Gil-Rodrigo, A.; Miro, O.; Pinera, P.; Burillo-Putze, G.; Jimenez, S.; Martin, A.; Martin-Sanchez, F.J.; Jacob, J.; Guardiola, J.M.; Garcia-Lamberechts, E.J.; et al. Analysis of clinical characteristics and outcomes in patients with COVID-19 based on a series of 1000 patients treated in Spanish emergency departments. Emergencias 2020, 32, 233–241. [Google Scholar]
- Kuang, Y.; Zhang, H.; Zhou, R.; Lin, S.; Lin, M.; Wang, J.; Pang, P.; Ma, L.; Ji, W. Epidemiological and clinical characteristics of 944 cases of 2019 novel Coronavirus infection of non-COVID-19 exporting city, Zhejiang, China. Available online: https://ssrn.com/abstract=3543604 (accessed on 20 February 2020).
- COVID-19 National Incident Room Surveillance Team. COVID-19, Australia: Epidemiology Report 13 (Reporting week to 23: 59 AEST 26 April 2020). Commun. Dis. Intell. (2018) 2020, 44, 1–27. [Google Scholar]
- Jin, X.; Xu, K.; Jiang, P.; Lian, J.; Hao, S.; Yao, H.; Jia, H.; Zhang, Y.; Zheng, L.; Zheng, N. Virus strain from a mild COVID-19 patient in Hangzhou represents a new trend in SARS-CoV-2 evolution potentially related to Furin cleavage site. Emerg. Microbes Infect. 2020, 9, 1474–1488. [Google Scholar] [CrossRef] [PubMed]
- Jin, X.; Lian, J.-S.; Hu, J.-H.; Gao, J.; Zheng, L.; Zhang, Y.-M.; Hao, S.-R.; Jia, H.-Y.; Cai, H.; Zhang, X.-L. Epidemiological, clinical and virological characteristics of 74 cases of coronavirus-infected disease 2019 (COVID-19) with gastrointestinal symptoms. Gut 2020, 69, 1002–1009. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Livanos, A.E.; Jha, D.; Cossarini, F.; Gonzalez-Reiche, A.S.; Tokuyama, M.; Aydillo, T.; Parigi, T.L.; Ramos, I.; Dunleavy, K.; Lee, B. Gastrointestinal involvement attenuates COVID-19 severity and mortality. MedRxiv 2020. [Google Scholar] [CrossRef]
- Liu, W.; Wang, F.; Li, G.; Wei, Y.; Li, X.; He, L.; Yue, H.; Zhang, F.; Hu, Q.; Chu, J. Analysis of 2019 Novel Coronavirus Infection and Clinical Characteristics of Outpatients: An Epidemiological Study from the Fever Clinic in Wuhan, China. Available online: https://papers.ssrn.com/sol3/papers.cfm?abstract_id=3539646 (accessed on 20 February 2020).
- Shu, L.; Wang, X.; Li, M.; Chen, X.; Shi, L.; Wu, M.; Deng, K.; Wei, J.; Wang, X.; Cao, Y. Clinical Characteristics of 545 Cases Confirmed COVID-19 in Wuhan Stadium Cabin Hospital. Available online: https://papers.ssrn.com/sol3/papers.cfm?abstract_id=3552844 (accessed on 20 February 2020).
- Han, Y.; Liu, Y.; Zhou, L.; Chen, E.; Liu, P.; Pan, X.; Lu, Y. Epidemiological Assessment of Imported Coronavirus Disease 2019 (COVID-19) Cases in the Most Affected City Outside of Hubei Province, Wenzhou, China. Jama Netw. Open 2020, 3, e206785. [Google Scholar] [CrossRef] [PubMed]
- Wen, Y.; Wei, L.; Li, Y.; Tang, X.; Feng, S.; Leung, K.; Wu, X.; Pan, X.-F.; Chen, C.; Xia, J. Epidemiological and clinical characteristics of COVID-19 in Shenzhen, the largest migrant city of China. MedRvix 2020. [Google Scholar] [CrossRef]
- Lechien, J.R.; Chiesa-Estomba, C.M.; De Siati, D.R.; Horoi, M.; Le Bon, S.D.; Rodriguez, A.; Dequanter, D.; Blecic, S.; El Afia, F.; Distinguin, L. Olfactory and gustatory dysfunctions as a clinical presentation of mild-to-moderate forms of the coronavirus disease (COVID-19): A multicenter European study. Eur. Arch. Oto-Rhino-Laryngol. 2020, 277, 2251–2261. [Google Scholar] [CrossRef]
- Bannaga, A.S.; Tabuso, M.; Farrugia, A.; Chandrapalan, S.; Somal, K.; Lim, V.K.; Mohamed, S.; Nia, G.J.; Mannath, J.; Wong, J.L. C-reactive protein and albumin association with mortality of hospitalised SARS-CoV-2 patients: A tertiary hospital experience. Clin. Med. 2020, 20, 463–467. [Google Scholar] [CrossRef]
- Reddm, W.D.; Zhou, J.C.; Hathorn, K.E.; McCarty, T.R.; Bazarbashi, A.N.; Thompson, C.C.; Shen, L.; Chan, W.W. Prevalence and characteristics of gastrointestinal symptoms in patients with severe acute respiratory syndrome coronavirus 2 infection in the United States: A multicenter cohort study. Gastroenterology 2020, 159, 765–767. [Google Scholar] [CrossRef]
- Fang, D.; Ma, J.; Guan, J.; Wang, M.; Song, Y.; Tian, D. Manifestations of digestive system in hospitalized patients with novel coronavirus pneumonia in Wuhan, China: A single-center, descriptive study. Chin. J. Dig. 2020, 40, 110–115. [Google Scholar]
- Chen, X.; Zheng, F.; Qing, Y.; Ding, S.; Yang, D.; Lei, C.; Yin, Z.; Zhou, X.; Jiang, D.; Zuo, Q. Epidemiological and clinical features of 291 cases with coronavirus disease 2019 in areas adjacent to Hubei, China: A double-center observational study. MedRvix 2020. [Google Scholar] [CrossRef] [Green Version]
- Covid, C.; COVID, C.; COVID, C.; Bialek, S.; Gierke, R.; Hughes, M.; McNamara, L.A.; Pilishvili, T.; Skoff, T. Coronavirus Disease 2019 in Children—United States, 12 February–2 April 2020. Morb. Mortal. Wkly. Rep. 2020, 69, 422. [Google Scholar]
- Nobel, Y.; Phipps, M.; Zucker, J. Gastrointestinal Symptoms and COVID-19: Case-Control Study from the United States. Gastroenterology 2020, 159, 373–375. [Google Scholar] [CrossRef] [PubMed]
- Chen, T.; Wu, D.; Chen, H.; Yan, W.; Yang, D.; Chen, G.; Ma, K.; Xu, D.; Yu, H.; Wang, H. Clinical characteristics of 113 deceased patients with coronavirus disease 2019: Retrospective study. Bmj 2020, 368, 1–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qi, D.; Yan, X.; Tang, X.; Peng, J.; Yu, Q.; Feng, L.; Yuan, G.; Zhang, A.; Chen, Y.; Yuan, J. Epidemiological and clinical features of 2019-nCoV acute respiratory disease cases in Chongqing municipality, China: A retrospective, descriptive, multiple-center study. MedRxiv 2020. [Google Scholar] [CrossRef] [Green Version]
- Zhou, Z.; Zhao, N.; Shu, Y.; Han, S.; Chen, B.; Shu, X. Effect of Gastrointestinal Symptoms in Patients With COVID-19. Gastroenterology 2020, 158, 2294. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Qi, T.; Liu, L.; Ling, Y.; Qian, Z.; Li, T.; Li, F.; Xu, Q.; Zhang, Y.; Xu, S. Clinical progression of patients with COVID-19 in Shanghai, China. J. Infect. 2020, 80, 1–6. [Google Scholar] [CrossRef]
- Liu, L.; Liu, W.; Zheng, Y.; Jiang, X.; Kou, G.; Ding, J.; Wang, Q.; Huang, Q.; Ding, Y.; Ni, W. A preliminary study on serological assay for severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) in 238 admitted hospital patients. Microbes Infect. 2020, 22, 206–211. [Google Scholar] [CrossRef]
- Chen, C.; Huang, J.; Cheng, Z.; Wu, J.; Chen, S.; Zhang, Y.; Chen, B.; Lu, M.; Luo, Y.; Zhang, J. Favipiravir versus arbidol for COVID-19: A randomized clinical trial. MedRxiv 2020. [Google Scholar] [CrossRef] [Green Version]
- Wan, Y.; Li, J.; Shen, L.; Zou, Y.; Hou, L.; Zhu, L.; Faden, H.S.; Tang, Z.; Shi, M.; Jiao, N. Enteric involvement in hospitalised patients with COVID-19 outside Wuhan. Lancet Gastroenterol. Hepatol. 2020, 5, 534–535. [Google Scholar] [CrossRef]
- Zhang, G.; Hu, C.; Luo, L.; Fang, F.; Chen, Y.; Li, J.; Peng, Z.; Pan, H. Clinical features and short-term outcomes of 221 patients with COVID-19 in Wuhan, China. J. Clin. Virol. 2020, 127, 104364. [Google Scholar] [CrossRef]
- Zhang, Y. Gastrointestinal tract symptoms in coronavirus disease 2019: Analysis of clinical symptoms in adult patients. MedRxiv 2020. [Google Scholar] [CrossRef]
- Pan, L.; Mu, M.; Yang, P.; Sun, Y.; Wang, R.; Yan, J.; Li, P.; Hu, B.; Wang, J.; Hu, C. Clinical characteristics of COVID-19 patients with digestive symptoms in Hubei, China: A descriptive, cross-sectional, multicenter study. Am. J. Gastroenterol. 2020, 115, 766–773. [Google Scholar] [CrossRef] [PubMed]
- Wei, L.; JIN, D.; Zhang, J.; Wang, B.; Sun, M.; Li, X.; Zhang, Y.; Lian, F.; Tong, X. Clinical Findings of 100 Mild Cases of COVID-19 in Wuhan: A Descriptive Study. Available online: https://papers.ssrn.com/sol3/papers.cfm?abstract_id=3551332 (accessed on 20 February 2020).
- Fu, L.; Fei, J.; Xiang, H.-X.; Xiang, Y.; Tan, Z.-X.; Li, M.-D.; Liu, F.-F.; Liu, H.-Y.; Zheng, L.; Li, Y. Influence factors of death risk among COVID-19 patients in Wuhan, China: A hospital-based case-cohort study. MedRxiv 2020. [Google Scholar] [CrossRef] [Green Version]
- Xiong, X.; Wong, K.K.-Y.; Chi, S.; Zhou, A.; Tang, J.; Zhou, L.; Chung, P.H.-y.; Chua, G.; Tung, K.T.; Wong, I.C. Are COVID-19 infected children with gastrointestinal symptoms different from those without symptoms? A comparative study of the clinical characteristics and epidemiological trend of 244 pediatric cases from Wuhan. MedRxiv 2020. [Google Scholar] [CrossRef]
- Huang, M.; Zhan, F.; Wang, J.; Yi, Q.; Zhu, F.; Yang, H.; Xiang, Q.; Xiang, J.; Fan, S.; Zhang, X. Epidemiological and Clinical Features of 197 Patients Infected with 2019 Novel Coronavirus in Chongqing, China: A Single Center Descriptive Study. Available online: https://papers.ssrn.com/sol3/papers.cfm?abstract_id=3539687 (accessed on 20 February 2020).
- Yan, Y.; Yang, Y.; Wang, F.; Ren, H.; Zhang, S.; Shi, X.; Yu, X.; Dong, K. Clinical characteristics and outcomes of patients with severe covid-19 with diabetes. Bmj Open Diabetes Res. Care 2020, 8, e001343. [Google Scholar] [CrossRef] [PubMed]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Gong, J.; Ou, J.; Qiu, X.; Jie, Y.; Chen, Y.; Yuan, L.; Cao, J.; Tan, M.; Xu, W.; Zheng, F. A tool to early predict severe 2019-novel coronavirus pneumonia (COVID-19): A multicenter study using the risk nomogram in Wuhan and Guangdong, China. MedRxiv 2020. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. COVID-NET: COVID-19 associated hospitalization surveillance network. Access: April 2020, 8, 6. [Google Scholar]
- Li, X.; Hu, C.; Su, F.; Dai, J. Hypokalemia and clinical implications in patients with coronavirus disease 2019 (COVID-19). MedRxiv 2020. [Google Scholar] [CrossRef]
- Lu, X.; Zhang, L.; Du, H.; Zhang, J.; Li, Y.Y.; Qu, J.; Zhang, W.; Wang, Y.; Bao, S.; Li, Y. SARS-CoV-2 infection in children. N. Engl. J. Med. 2020, 382, 1663–1665. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garazzino, S.; Montagnani, C.; Donà, D.; Meini, A.; Felici, E.; Vergine, G.; Bernardi, S.; Giacchero, R.; Vecchio, A.L.; Marchisio, P. Multicentre Italian study of SARS-CoV-2 infection in children and adolescents, preliminary data as at 10 April 2020. Eurosurveillance 2020, 25, 2000600. [Google Scholar] [CrossRef] [PubMed]
- Zheng, F.; Tang, W.; Li, H.; Huang, Y.; Xie, Y.; Zhou, Z. Clinical characteristics of 161 cases of corona virus disease 2019 (COVID-19) in Changsha. Eur. Rev. Med. Pharm. Sci. 2020, 24, 3404–3410. [Google Scholar]
- Mo, P.; Xing, Y.; Xiao, Y.; Deng, L.; Zhao, Q.; Wang, H.; Xiong, Y.; Cheng, Z.; Gao, S.; Liang, K. Clinical characteristics of refractory COVID-19 pneumonia in Wuhan, China. Clin. Infect. Dis. 2020. Online ahead of print. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, W.; Cao, Q.; Qin, L.; Wang, X.; Cheng, Z.; Pan, A.; Dai, J.; Sun, Q.; Zhao, F.; Qu, J. Clinical characteristics and imaging manifestations of the 2019 novel coronavirus disease (COVID-19): A multi-center study in Wenzhou city, Zhejiang, China. J. Infect. 2020, 80, 388–393. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fan, Z.; Chen, L.; Li, J.; Cheng, X.; Yang, J.; Tian, C.; Zhang, Y.; Huang, S.; Liu, Z.; Cheng, J. Clinical features of COVID-19-related liver damage. Clin. Gastroenterol. Hepatol. 2020, 18, 1561–1566. [Google Scholar] [CrossRef] [PubMed]
- Chen, Q.; Zheng, Z.; Zhang, C.; Zhang, X.; Wu, H.; Wang, J.; Wang, S.; Zheng, C. Clinical characteristics of 145 patients with corona virus disease 2019 (COVID-19) in Taizhou, Zhejiang, China. Infection 2020, 48, 543–551. [Google Scholar] [CrossRef] [PubMed]
- Feng, Z.; Yu, Q.; Yao, S.; Luo, L.; Duan, J.; Yan, Z.; Yang, M.; Tan, H.; Ma, M.; Li, T. Early prediction of disease progression in 2019 novel coronavirus pneumonia patients outside Wuhan with CT and clinical characteristics. MedRxiv 2020. [Google Scholar] [CrossRef]
- Zhang, J.-j.; Dong, X.; Cao, Y.-y.; Yuan, Y.-d.; Yang, Y.-b.; Yan, Y.-q.; Akdis, C.A.; Gao, Y.-d. Clinical characteristics of 140 patients infected with SARS-CoV-2 in Wuhan, China. Allergy 2020, 75, 1730–1741. [Google Scholar] [CrossRef]
- Wang, D.; Hu, B.; Hu, C.; Zhu, F.; Liu, X.; Zhang, J.; Wang, B.; Xiang, H.; Cheng, Z.; Xiong, Y. Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus–infected pneumonia in Wuhan, China. Jama 2020, 323, 1061–1069. [Google Scholar] [CrossRef]
- Liu, K.; Fang, Y.-Y.; Deng, Y.; Liu, W.; Wang, M.-F.; Ma, J.-P.; Xiao, W.; Wang, Y.-N.; Zhong, M.-H.; Li, C.-H. Clinical characteristics of novel coronavirus cases in tertiary hospitals in Hubei Province. Chin. Med. J. 2020, 133, 1025–1031. [Google Scholar] [CrossRef]
- Li, X.; Zeng, W.; Li, X.; Chen, H.; Shi, L.; Li, X.; Xiang, H.; Cao, Y.; Chen, H.; Liu, C. CT imaging changes of corona virus disease 2019 (COVID-19): A multi-center study in Southwest China. J. Transl. Med. 2020, 18, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giacomet, V.; Barcellini, L.; Stracuzzi, M.; Longoni, E.; Folgori, L.; Leone, A.; Zuccotti, G.V. Gastrointestinal Symptoms in Severe COVID-19 Children. Pediatric Infect. Dis. J. 2020, 39, e317–e320. [Google Scholar] [CrossRef] [PubMed]
- Bai, T.; Tu, S.; Wei, Y.; Xiao, L.; Jin, Y.; Zhang, L.; Song, J.; Liu, W.; Zhu, Q.; Yang, L. Clinical and Laboratory Factors Predicting the Prognosis of Patients with COVID-19: An Analysis of 127 Patients in Wuhan, China. Available online: https://papers.ssrn.com/sol3/papers.cfm?abstract_id=3546118 (accessed on 20 February 2020).
- Wan, S.; Yi, Q.; Fan, S.; Lv, J.; Zhang, X.; Guo, L.; Lang, C.; Xiao, Q.; Xiao, K.; Yi, Z. Relationships among lymphocyte subsets, cytokines, and the pulmonary inflammation index in coronavirus (COVID-19) infected patients. Br. J. Haematol. 2020, 189, 428–437. [Google Scholar] [CrossRef] [PubMed]
- Cholankeril, G.; Podboy, A.; Aivaliotis, V.I.; Tarlow, B.; Pham, E.A.; Spencer, S.P.; Kim, D.; Hsing, A.; Ahmed, A. High Prevalence of Concurrent Gastrointestinal Manifestations in Patients With Severe Acute Respiratory Syndrome Coronavirus 2: Early Experience From California. Gastroenterology 2020, 159, 775–777. [Google Scholar] [CrossRef] [PubMed]
- Ma, Y.-L.; Xia, S.-Y.; Wang, M.; Zhang, S.-M.; WH, D.; Chen, Q. Clinical features of children with SARS-CoV-2 infection: An analysis of 115 cases. Zhongguo Dang Dai Er Ke Za Zhi= Chin. J. Contemp. Pediatrics 2020, 22, 290–293. [Google Scholar]
- Wang, K.; Kang, S.; Tian, R.; Zhang, X.; Wang, Y. Imaging manifestations and diagnostic value of chest CT of corona virus disease 2019 (COVID-19) in the Xiaogan area. Clin. Radiol. 2020, 75, 341–347. [Google Scholar] [CrossRef] [Green Version]
- Klopfenstein, T.; N’driJuliette Kadiane-Oussou, P.; Royer, Y.; Toko, L.; Gendrin, V.; Zayet, S. Diarrhea: An under estimated symptom in Corona virus disease 2019. Clin. Res. Hepatol. Gastroenterol. 2020, 44, 282–283. [Google Scholar] [CrossRef]
- Peng, Y.; Meng, K.; Guan, H.; Leng, L.; Zhu, R.; Wang, B.; He, M.; Cheng, L.; Huang, K.; Zeng, Q. Clinical characteristics and outcomes of 112 cardiovascular disease patients infected by 2019 -n CoV. Zhonghua Xin Xue Guan Bing Za Zhi 2020, 48, E004. [Google Scholar]
- Liu, Y.; Sun, W.; Li, J.; Chen, L.; Wang, Y.; Zhang, L.; Yu, L. Clinical features and progression of acute respiratory distress syndrome in corona virus disease 2019. MedRxiv 2020. [Google Scholar] [CrossRef]
- Han, R.; Huang, L.; Jiang, H.; Dong, J.; Peng, H.; Zhang, D. Early clinical and CT manifestations of corona virus disease 2019 (COVID-19)pneumonia. Am. J. Roentgenol. 2020, 215, 338–343. [Google Scholar] [CrossRef]
- Wang, D.; Yin, Y.; Hu, C.; Liu, X.; Zhang, X.; Zhou, S.; Jian, M.; Xu, H.; Prowle, J.; Hu, B. Clinical course and outcome of 107 patients infected with the novel corona virus, SARS-CoV-2, discharged from two hospitals in Wuhan, China. Crit. Care 2020, 24, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.-Y.; Wang, L.-W.; Chen, Y.-Y.; Shen, X.-K.; Wang, Q.; Yan, Y.-Q.; Yu, Y.; Wu, Q.; Wang, X.; Zhong, Y.-H. A multi centre study of 2019 novel corona virus disease outcomes of cancer patients in Wuhan, China. MedRxiv 2020. [Google Scholar] [CrossRef]
- Tabata, S.; Imai, K.; Kawano, S.; Ikeda, M.; Kodama, T.; Miyoshi, K.; Obinata, H.; Mimura, S.; Kodera, T.; Kitagaki, M. The clinical characteristics of COVID-19: A retrospective analysis of 104 patients from the outbreak on board the Diamond Princess cruiseship in Japan. MedRxiv 2020. [Google Scholar] [CrossRef]
- Ai, J.; Chen, J.; Wang, Y.; Liu, X.; Fan, W.; Qu, G.; Zhang, M.; Pei, S.P.; Tang, B.; Yuan, S. The cross-sectional study of hospitalized corona virus disease 2019 patients in Xiangyang, Hubei province. MedRxiv 2020. [Google Scholar] [CrossRef] [Green Version]
- Zhao, W.; Zhong, Z.; Xie, X.; Yu, Q.; Liu, J. Relation between chest CT findings and clinical conditions of corona virus disease (COVID-19) pneumonia: A multi center study. Am. J. Roentgenol. 2020, 214, 1072–1077. [Google Scholar] [CrossRef]
- Chen, N.; Zhou, M.; Dong, X.; Qu, J.; Gong, F.; Han, Y.; Qiu, Y.; Wang, J.; Liu, Y.; Wei, Y. Epidemiological and clinical characteristics of 99 cases of 2019 novel corona virus pneumonia in Wuhan, China: A descriptive study. Lancet 2020, 395, 507–513. [Google Scholar] [CrossRef] [Green Version]
- Lin, L.; Jiang, X.; Zhang, Z.; Huang, S.; Zhang, Z.; Fang, Z.; Gu, Z.; Gao, L.; Shi, H.; Mai, L. Gastrointestinal symptoms of 95 cases with SARS-CoV-2 infection. Gut 2020, 69, 997–1001. [Google Scholar] [CrossRef]
- Yu, X.; Sun, S.; Shi, Y.; Wang, H.; Zhao, R.; Sheng, J. SARS-CoV-2 viral load in sputum correlates with risk of COVID-19 progression. Crit. Care 2020, 24, 1–4. [Google Scholar] [CrossRef] [Green Version]
- Qian, G.-Q.; Yang, N.-B.; Ding, F.; Ma, A.H.Y.; Wang, Z.-Y.; Shen, Y.-F.; Shi, C.-W.; Lian, X.; Chu, J.-G.; Chen, L. Epidemiologic and Clinical Characteristics of 91 Hospitalized Patients with COVID-19 in Zhejiang, China: A retrospective, multi-centre case series. Qjm: Int. J. Med. 2020, 113, 474–481. [Google Scholar] [CrossRef] [Green Version]
- Zhao, X.-Y.; Xu, X.-X.; Yin, H.-S.; Hu, Q.-M.; Xiong, T.; Tang, Y.-Y.; Yang, A.-Y.; Yu, B.-P.; Huang, Z.-P. Clinical characteristics of patients with 2019 corona virus disease in a non-Wuhan area of Hubei Province, China: A retrospective study. Bmc Infect. Dis. 2020, 20, 1–8. [Google Scholar] [CrossRef]
- Xu, X.; Yu, C.; Qu, J.; Zhang, L.; Jiang, S.; Huang, D.; Chen, B.; Zhang, Z.; Guan, W.; Ling, Z. Imaging and clinical features of patients with 2019 novel corona virus SARS-CoV-2. Eur. J. Nucl. Med. Mol. Imaging 2020, 47, 1275–1280. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, Z.; Hu, J.; Zhang, Z.; Jiang, S.; Wang, T.; Shi, Z.; Zhang, Z. Caution: Clinical Characteristics of COVID-19 Patients Are Changing at Admission. Available online: https://papers.ssrn.com/sol3/papers.cfm?abstract_id=3546044 (accessed on 20 February 2020).
- Xu, W.; Qu, S.; Xing, M.; Zhang, M.; Lu, G.; Liao, Z.; Griffin, K.; Wang, J.; Zen, K.; Yao, B. Epidemiologic Features and Clinical Findings of COVID-19 Infected Patients in Suzhou. Available online: https://papers.ssrn.com/sol3/papers.cfm?abstract_id=3551352 (accessed on 20 February 2020).
- Kluytmans, M.; Buiting, A.; Pas, S.; Bentvelsen, R.; vanden Bijllaardt, W.; van Oudheusden, A.; van Rijen, M.; Verweij, J.; Koopmans, M.; Kluytmans, J. SARS-CoV-2 infection in 86 healthcare workers in two Dutch hospitals in March 2020. MedRxiv 2020. [Google Scholar] [CrossRef] [Green Version]
- Wei, X.-S.; Wang, X.; Niu, Y.-R.; Ye, L.-L.; Peng, W.-B.; Wang, Z.-H.; Yang, W.-B.; Yang, B.-H.; Zhang, J.-C.; Ma, W.-L. Diarrhea is associated with prolonged symptoms and viral carriage in COVID-19. Clin. Gastroenterol. Hepatol. 2020, 18, 1753–1759. [Google Scholar] [CrossRef] [PubMed]
- Li, K.; Wu, J.; Wu, F.; Guo, D.; Chen, L.; Fang, Z.; Li, C. The clinical and chest CT features associated with severe and critical COVID-19 pneumonia. Investig. Radiol. 2020, 55, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Shi, H.; Han, X.; Jiang, N.; Cao, Y.; Alwalid, O.; Gu, J.; Fan, Y.; Zheng, C. Radiological findings from 81 patients with COVID-1 9 pneumonia in Wuhan, China: A descriptive study. Lancet Infect. Dis. 2020, 20, 425–434. [Google Scholar] [CrossRef]
- Cai, Q.; Yang, M.; Liu, D.; Chen, J.; Shu, D.; Xia, J.; Liao, X.; Gu, Y.; Cai, Q.; Yang, Y. Experimental treatment with favipiravir for COVID-19: An open-label control study. Engineering 2020, Article in press. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.; Liu, J.; Zhao, X.; Liu, C.; Wang, W.; Wang, D.; Xu, W.; Zhang, C.; Yu, J.; Jiang, B. Clinical characteristics of imported cases of COVID-19 in Jiangs uprovince: A multicenter descriptive study. Clin Infect Dis 2020, 10, 1–7. [Google Scholar]
- Wu, J.; Wu, X.; Zeng, W.; Guo, D.; Fang, Z.; Chen, L.; Huang, H.; Li, C. Chest CT findings in patients with corona virus disease 2019 and its relationship with clinical features. Investig. Radiol. 2020, 55, 257. [Google Scholar] [CrossRef]
- Fang, X.; Mei, Q.; Yang, T.; Zhang, L.; Yang, Y.; Wang, Y. Clinical characteristics and treatment strategies of 79 patients with COVID-19. Chin. Pharmacol. Bull. 2020, 36, 11–18. [Google Scholar]
- Zhao, W.; Yu, S.; Zha, X.; Wang, N.; Pang, Q.; Li, T.; Li, A. Clinical characteristics and durations of hospitalized patients with COVID-19 in Beijing: A retrospective cohortstudy. MedRxiv 2020. [Google Scholar] [CrossRef] [Green Version]
- Yu, F.; Yan, L.; Wang, N.; Yang, S.; Wang, L.; Tang, Y.; Gao, G.; Wang, S.; Ma, C.; Xie, R. Quantitative detection and viral load analysis of SARS-CoV-2 in infected patients. Clin. Infect. Dis. 2020, 71, 793–798. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, Z.; Xie, J.; Yin, M.; Yang, Y.; He, H.; Jin, T.; Li, W.; Zhu, X.; Xu, J.; Zhao, C. Clinical and laboratory profiles of 75 hospitalized patients with novel corona virus disease 2019 in Hefei, China. MedRxiv 2020. [Google Scholar] [CrossRef]
- Wu, Y.; Guo, C.; Tang, L.; Hong, Z.; Zhou, J.; Dong, X.; Yin, H.; Xiao, Q.; Tang, Y.; Qu, X. Prolonged presence of SARS-CoV-2 viral RNA in faecal samples. Lancet Gastroenterol. Hepatol. 2020, 5, 434–435. [Google Scholar] [CrossRef]
- Tang, X.; Du, R.; Wang, R.; Cao, T.; Guan, L.; Yang, C.; Zhu, Q.; Hu, M.; Li, X.; Li, Y. Comparison of hospitalized patients with acute respiratory distress syndrome caused by Covid-19 and H1N1. Chest 2020, 158, 195–205. [Google Scholar] [CrossRef] [PubMed]
- Zhou, S.; Wang, Y.; Zhu, T.; Xia, L. CT features of corona virus disease 2019 (COVID-19) pneumonia in 62 patients in Wuhan, China. Am. J. Roentgenol. 2020, 214, 1287–1294. [Google Scholar] [CrossRef] [PubMed]
- Xu, X.-W.; Wu, X.-X.; Jiang, X.-G.; Xu, K.-J.; Ying, L.-J.; Ma, C.-L.; Li, S.-B.; Wang, H.-Y.; Zhang, S.; Gao, H.-N. Clinical findings in a group of patients infected with the 2019 novel corona virus (SARS-Cov-2) outside of Wuhan, China: Retrospective case series. Bmj 2020, 368, 606–613. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miao, C.; Zhuang, J.; Jin, M.; Xiong, H.; Huang, P.; Zhao, Q.; Miao, L.; Du, J.; Yang, X.; Huang, P. A comparative multi-centre study on the clinical and imaging features of comfirmed and uncomfirmed patients with COVID-19. MedRxiv 2020. [Google Scholar] [CrossRef] [Green Version]
- Cheung, K.S.; Hung, I.F.; Chan, P.P.; Lung, K.; Tso, E.; Liu, R.; Ng, Y.; Chu, M.Y.; Chung, T.W.; Tam, A.R. Gastrointestinal manifestations of SARS-CoV-2 infection and virus load in fecal samples from the Hong Kong cohort and systematic review and meta-analysis. Gastroenterology 2020, 159, 81–95. [Google Scholar] [CrossRef]
- Grein, J.; Ohmagari, N.; Shin, D.; Diaz, G.; Asperges, E.; Castagna, A.; Feldt, T.; Green, G.; Green, M.L.; Lescure, F.-X. Compassionate use of remdesivir for patients with severe Covid-19. New Engl. J. Med. 2020, 382, 2327–2336. [Google Scholar] [CrossRef] [PubMed]
- Fu, H.; Xu, H.; Zhang, N.; Xu, H.; Li, Z.; Chen, H.; Xu, R.; Sun, R.; Wen, L.; Xie, L. Association between Clinical, Laboratory and CT Characteristics and RT-PCR Results in the Follow-up of COVID-19 patients. MedRxiv 2020. [Google Scholar] [CrossRef]
- Yang, X.; Yu, Y.; Xu, J.; Shu, H.; Liu, H.; Wu, Y.; Zhang, L.; Yu, Z.; Fang, M.; Yu, T. Clinical course and outcomes of critically ill patients with SARS-CoV-2 pneumonia in Wuhan, China: A single-centered, retrospective, observational study. Lancet Respir. Med. 2020, 8, 475–481. [Google Scholar] [CrossRef] [Green Version]
- Song, F.; Shi, N.; Shan, F.; Zhang, Z.; Shen, J.; Lu, H.; Ling, Y.; Jiang, Y.; Shi, Y. Emerging 2019 novel coronavirus (2019-nCoV) pneumonia. Radiology 2020, 295, 210–217. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, T.; Chen, C.; Zhu, Z.; Cui, M.; Chen, C.; Dai, H.; Xue, Y. Clinical features and dynamics of viral load in imported and non-imported patients with COVID-19. Int. J. Infect. Dis. 2020, 94, 68–71. [Google Scholar] [CrossRef] [PubMed]
- Dreher, M.; Kersten, A.; Bickenbach, J.; Balfanz, P.; Hartmann, B.; Cornelissen, C.; Daher, A.; Stöhr, R.; Kleines, M.; Lemmen, S. Charakteristik von 50 hospitalisierten COVID-19-Patienten mit un dohne ARDS. Dtsch Arztebl Int 2020, 117, 271–278. [Google Scholar]
- Xu, Y.-H.; Dong, J.-H.; An, W.-M.; Lv, X.-Y.; Yin, X.-P.; Zhang, J.-Z.; Dong, L.; Ma, X.; Zhang, H.-J.; Gao, B.-L. Clinical and computed tomographic imaging features of novel corona virus pneumonia caused by SARS-CoV-2. J. Infect. 2020, 80, 394–400. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Colaneri, M.; Sacchi, P.; Zuccaro, V.; Biscarini, S.; Sachs, M.; Roda, S.; Pieri, T.C.; Valsecchi, P.; Piralla, A.; Seminari, E. Clinical characteristics of corona virus disease (COVID-19) early findings from a teaching hospital in Pavia, North Italy, 21 to 28 February 2020. Eurosurveillance 2020, 25, 2000460. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jin, J.-M.; Bai, P.; He, W.; Wu, F.; Liu, X.-F.; Han, D.-M.; Liu, S.; Yang, J.-K. Gender differences in patients with COVID-19: Focus on severity and mortality. Front. Public Health 2020, 8, 152. [Google Scholar] [CrossRef]
- Xiong, Y.; Sun, D.; Liu, Y.; Fan, Y.; Zhao, L.; Li, X.; Zhu, W. Clinical and high-resolution CT features of the COVID-19 infection: Comparison of the initial and follow-upchanges. Investig. Radiol. 2020, 55, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Meng, J.; Xiao, G.; Zhang, J.; He, X.; Ou, M.; Bi, J.; Yang, R.; Di, W.; Wang, Z.; Li, Z. Renin-angiotensin system inhibitors improve the clinical outcomes of COVID-19 patients with hypertension. Emerg. Microbes Infect. 2020, 9, 757–760. [Google Scholar] [CrossRef]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X. Clinical features of patients infected with 2019 novel corona virus in Wuhan, China. Lancet. 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Rodríguez-Lago, I.; delaPiscina, P.R.; Elorza, A.; Merino, O.; deZárate, J.O.; Cabriada, J.L. Characteristics and prognosis of patients with inflammatory bowel disease during the SARS-CoV-2 pandemic in the Basque Country (Spain). Gastroenterology 2020, 159, 781–783. [Google Scholar] [CrossRef] [PubMed]
- Wu, W.; Li, Y.; Wei, Z.; Zhou, P.; Lyu, L.; Zhang, G.; Zhao, Y.; He, H.; Li, X.; Gao, L. Investigation and analysis on characteristics of a cluster of COVID-19 associated with exposure in a department store in Tianjin. Zhonghua Liu Xing Bing Xue Za Zhi = Zhonghua Liuxingbingxue Zazhi 2020, 41, 489–493. [Google Scholar] [PubMed]
- Yao, N.; Wang, S.; Lian, J.; Sun, Y.; Zhang, G.; Kang, W.; Kang, W. Clinical characteristics and influencing factors of patients with novel corona virus pneumonia combined with liver injury in Shaanxi region. Zhonghua Gan Zang Bing Za Zhi = Zhonghua Ganzangbing Zazhi = Chin. J. Hepatol. 2020, 28, E003. [Google Scholar]
- Holshue, M.L.; DeBolt, C.; Lindquist, S.; Lofy, K.H.; Wiesman, J.; Bruce, H.; Spitters, C.; Ericson, K.; Wilkerson, S.; Tural, A. First case of 2019 novel corona virus in the United States. New Engl. J. Med. 2020, 382, 929–936. [Google Scholar] [CrossRef] [PubMed]
- Bezerra, J.; Pochapin, M.; El-Serag, H.; Vargo, J. COVID-19 Clinical Insights for Our Community of Gastroenterologists and Gastroenterology Care Providers. 2020. Available online: https://gastro.org/press-releases/joint-gi-society-message-covid-19 (accessed on 20 February 2020).
- Borgesdo Nascimento, I.J.; Cacic, N.; Abdulazeem, H.M.; vonGroote, T.C.; Jayarajah, U.; Weerasekara, I.; Esfahani, M.A.; Civile, V.T.; Marusic, A.; Jeroncic, A. Novel corona virus infection (COVID-19) in humans: A scoping review and meta-analysis. J. Clin. Med. 2020, 9, 941. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hall, A.B.; Tolonen, A.C.; Xavier, R.J. Human genetic variation and the gut microbiome in disease. Nat. Rev. Genet. 2017, 18, 690–699. [Google Scholar] [CrossRef]
- Zhang, D.; Li, S.; Wang, N.; Tan, H.Y.; Zhang, Z.; Feng, Y. The Cross-Talk Between Gut Microbiota and Lungs in Common Lung Diseases. Front Microbiol 2020, 11, 301. [Google Scholar] [CrossRef] [PubMed]
- Keely, S.; Talley, N.J.; Hansbro, P.M. Pulmonary-intestinal cross-talk in mucosal inflammatory disease. Mucosal Immunol 2012, 5, 7–18. [Google Scholar] [CrossRef] [Green Version]
- Dumas, A.; Bernard, L.; Poquet, Y.; Lugo-Villarino, G.; Neyrolles, O. The role of the lung microbiota and the gut-lung axis in respiratory infectious diseases. Cell Microbiol. 2018, 20, e12966. [Google Scholar] [CrossRef] [Green Version]
- Groves, H.T.; Higham, S.L.; Moffatt, M.F.; Cox, M.J.; Tregoning, J.S. Respiratory Viral Infection Alters the Gut Microbiota by Inducing Inappetence. mBio 2020, 11, 1–17. [Google Scholar] [CrossRef] [Green Version]
- Mosca, A.; Leclerc, M.; Hugot, J.P. Gut Microbiota Diversity and Human Diseases: Should We Reintroduce Key Predators in Our Ecosystem? Front. Microbiol. 2016, 7, 455. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sultan, S.; Altayar, O.; Siddique, S.M.; Davitkov, P.; Feuerstein, J.D.; Lim, J.K.; Falck-Ytter, Y.; El-Serag, H.B. AGA Institute Rapid Review of the GI and Liver Manifestations of COVID-19, Meta-Analysis of International Data, and Recommendations for the Consultative Management of Patients with COVID-19. Gastroenterology 2020, 159, 320–334. [Google Scholar] [CrossRef] [PubMed]
- Mao, R.; Qiu, Y.; He, J.-S.; Tan, J.-Y.; Li, X.-H.; Liang, J.; Shen, J.; Zhu, L.-R.; Chen, Y.; Iacucci, M. Manifestations and prognosis of gastrointestinal and liver involvement in patients with COVID-19: A systematic review and meta-analysis. Lancet Gastroenterol. Hepatol. 2020, 5, 667–678. [Google Scholar] [CrossRef]
- To, K.K.-W.; Hung, I.F.-N.; Ip, J.D.; Chu, A.W.-H.; Chan, W.-M.; Tam, A.R.; Fong, C.H.-Y.; Yuan, S.; Tsoi, H.-W.; Ng, A.C.-K. COVID-19 re-infection by a phylogenetically distinct SARS-coronavirus-2 strain confirmed by whole genome sequencing. Clin. Infect. Dis. 2020. [Google Scholar] [CrossRef]
- Edridge, A.W.; Kaczorowska, J.M.; Hoste, A.C.; Bakker, M.; Klein, M.; Jebbink, M.F.; Matser, A.; Kinsella, C.; Rueda, P.; Prins, M. Human corona virus reinfection dynamics: Lessons for SARS-CoV-2. MedRxiv 2020. [Google Scholar] [CrossRef]
- Shu, Z.; Zhou, Y.; Chang, K.; Liu, J.; Min, X.; Zhang, Q.; Sun, J.; Xiong, Y.; Zou, Q.; Zheng, Q. Clinical features and the traditional Chinese medicine therapeutic characteristics of 293 COVID-19 in patient cases. Front. Med. 2020. [Google Scholar] [CrossRef]
- Palayew, A.; Norgaard, O.; Safreed-Harmon, K.; Andersen, T.H.; Rasmussen, L.N.; Lazarus, J.V. Pandemic publishing poses a new COVID-19 challenge. Nat. Hum. Behav. 2020, 4, 666–669. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Authors | Study Type | Setting | Age Group | Place of Study | Number of Patients Included | Male Patients, n (%) | Severe Disease, n (%) | Diarrhea, n (%) | Nausea, n (%) | Abdominal Pain, n (%) | Anorexia, n (%) |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Docherty AB. et al. [9] | RCS | Mixed | Mixed | UK | 16,749 | 7715 (46, 06) | 5528 (33) | 2292 (13, 68) | 2178 (13) | 1146 (6, 84) | n.a. |
| Fanelli V. et al. [10] | RCS | IP | Mixed | Italy | 14,688 | 9253 (63) | 14,688 (100) | 881 (6) | n.a. | n.a. | 6 (0, 04) |
| CDC USA [11] | RCS | Mixed | adult | USA | 10,994 | 5827 (53) | 495 (4, 5) | 3353 (30, 5) | 1746 (15, 88) | 1329 (12, 09) | n.a. |
| CDC USA [12] | RCS | Mixed | adult | USA | 6760 | 2464 (36, 45) | 184 (2, 72) | 1507 (22, 29) | 923 (13, 65) | n.a. | n.a. |
| Rojo JMC. et al. [13] | RCS | IP | adult | Spain | 6424 | 3651 (56, 83) | 2025 (31, 52) | n.a. | n.a. | n.a. | n.a. |
| Borobia A. et al. [14] | RCS | IP | adult | Spain | 2226 | 1074 (48, 25) | 460 (20, 66) | 484 (21, 74) | 299 (13, 43) | n.a. | n.a. |
| Elmunzer. BJ et al. [15] | RCS | IP | adult | USA and Canada | 1992 | 1128 (56, 63) | 646 (32, 43) | 678 (34, 04) | 538 (27, 01) | 220 (11, 04) | n.a. |
| Guan WJ. et al. [16] | RCS | Mixed | adult | China | 1590 | 904 (56, 86) | 99 (6, 23) | 57 (3, 58) | 80 (5, 03) | n.a. | n.a. |
| Luo S. et al. [17] | CS | IP | adult | China | 1141 | n.a. | n.a. | 68 (5, 96) | 134 (11, 74) | 45 (3, 94) | 180 (15, 78) |
| Guan WJ. et al. [1] | RCS | Mixed | adult | China | 1099 | 637 (57, 96) | 173 (15, 74) | 42 (3, 82) | 55 (5) | n.a. | n.a. |
| Cheng JL. et al. [18] | CSS | IP | Mixed | China | 1079 | 573 (53, 1) | 72 (6, 67) | n.a. | n.a. | n.a. | n.a. |
| Hajifathalian K. et al. [19] | RCS | Mixed | adult | USA | 1059 | 614 (57, 98) | n.a. | 234 (22, 1) | 168 (15, 86) | 72 (6, 8) | 240 (22, 66) |
| Gil-Rodrigo A. et al. [20] | RCS | Mixed | adult | Spain | 1000 | 562 (56, 2) | 119 (11, 9) | 186 (18, 6) | 75 (7, 5) | 66 (6, 6) | n.a. |
| Kuang Y. et al. [21] | CSS | n.a. | adult | China | 944 | 476 (50, 42) | n.a. | 21 (2, 22) | n.a. | n.a. | n.a. |
| COVID-19, Australia [22] | ER | Mixed | Mixed | Australia | 907 | 454 (50, 06) | 17 (1, 87) | n.a. | n.a. | 18 (1, 98) | n.a. |
| Jin X. et al. [23] | CSS | IP | adult | China | 788 | 407 (51, 65) | 78 (9, 9) | n.a. | n.a. | n.a. | n.a. |
| Jin X. et al. [24] | CCS | IP | adult | China | 651 | 331 (50, 84) | 205 (31, 49) | 53 (8, 14) | 22 (3, 38) | n.a. | n.a. |
| Livanos AE. et al. [25] | RCS | Mixed | adult | USA | 634 | 369 (58, 2) | 158 (24, 92) | 245 (38, 64) | 157 (24, 76) | n.a. | n.a. |
| Liu W. et al. [26] | CS | OP | adult | China | 628 | 296 (47, 13) | 75 (11, 94) | 12 (1, 91) | 2 (0, 32) | 0 (0) | 3 (0, 48) |
| Shu L. et al. [27] | RCS | IP | adult | China | 571 | 278 (48, 69) | 38 (6, 65) | 51 (8, 93) | 21 (3, 68) | n.a. | n.a. |
| Han Y. et al. [28] | RCS | Mixed | adult | China | 452 | 254 (56, 19) | n.a. | 27 (5, 97) | n.a. | n.a. | n.a. |
| Wen Y. et al. [29] | CSS | Mixed | adult | China | 417 | 197 (47, 24) | 36 (8, 63) | 29 (6, 95) | n.a. | n.a. | n.a. |
| Lechien JR. et al. [30] | RCS | Mixed | adult | Europe | 417 | 154 (36, 93) | 0 (0) | 213 (51, 08) | 92 (22, 06) | 125 (29, 98) | 217 (52, 04) |
| Bannaga AS. et al. [31] | RCS | IP | adult | UK | 321 | 189 (58, 88) | 44 (13, 71) | 13 (4, 05) | 15 (4, 67) | 15 (4, 67) | n.a. |
| Redd WD. et al. [32] | RCS | IP | adult | USA | 318 | 174 (54, 72) | n.a. | 107 (33, 65) | 84 (26, 42) | 46 (14, 47) | 110 (34.8) |
| Fang D. et al. [33] | RCS | IP | adult | China | 305 | 146 (47, 87) | 46 (15, 08) | 66 (21, 64) | 59 (19, 34) | 12 (3, 93) | 101 (33, 11) |
| Chen X. et al. [34] | RCS | Mixed | Mixed | China | 291 | 145 (49, 83) | 50 (17, 18) | 25 (8, 59) | 17 (5, 84) | 1 (0, 34) | n.a. |
| CDC USA [35] | RCS | Mixed | pediatric | USA | 291 | 166 (57, 04) | 4 (1, 37) | 37 (12, 71) | 31 (10, 65) | 17 (5, 84) | n.a. |
| Nobel YR. et al. [36] | RCS | OP | adult | USA | 278 | 145 (52, 16) | n.a. | 56 (20, 14) | 63 (22, 66) | n.a. | 97 (34, 89) |
| Chen T. et al. [37] | RCS | IP | adult | China | 274 | 171 (62, 41) | 113 (41, 24) | 77 (28, 1) | 16 (5, 84) | 19 (6, 93) | 66 (24, 09) |
| Qi D. et al. [38] | RCS | IP | adult | China | 267 | 149 (55, 81) | n.a. | 10 (3, 75) | 6 (2, 25) | n.a. | 46 (17, 23) |
| Zhou Z. et al. [39] | RCS | IP | adult | China | 254 | 115 (45, 28) | 16 (6, 3) | 46 (18, 11) | 21 (8, 27) | 3 (1, 18) | n.a. |
| Chen J. et al. [40] | RCS | IP | adult | China | 249 | 126 (50, 6) | 22 (8, 84) | 8 (3, 21) | n.a. | n.a. | 8 (3, 21) |
| Liu L. et al. [41] | RCS | Mixed | adult | China | 238 | 138 (57, 98) | n.a. | 24 (10, 08) | 4 (1, 68) | 1 (0, 42) | 29 (12, 18) |
| Chen C. et al. [42] | RCS | IP | adult | China | 236 | 110 (46, 61) | 27 (11, 44) | 37 (15, 68) | n.a. | n.a. | n.a. |
| Wan Y. et al. [43] | RCS | IP | Mixed | China | 230 | 129 (56, 09) | 61 (26, 52) | 49 (21, 3) | n.a. | n.a. | n.a. |
| Yong Z.et al. [44] | RCS | Mixed | adult | China | 212 | 85 (40, 09) | n.a. | 93 (43, 87) | 44 (20, 75) | n.a. | n.a. |
| Zhang Y. et al. [45] | CSS | IP | adult | China | 212 | 85 (40, 09) | n.a. | 139 (65, 57) | 44 (20, 75) | n.a. | n.a. |
| Pan L. et al. [46] | CSS | IP | adult | China | 204 | 107 (52, 45) | 37 (18, 14) | 70 (34, 31) | 8 (3, 92) | 4 (1, 96) | 62 (30, 39) |
| Wei L. et al. [47] | RCS | Mixed | adult | China | 202 | 116 (57, 43) | 23 (11, 39) | 13 (6, 44) | 4 (1, 98) | n.a. | n.a. |
| Fu L. et al. [48] | RCS | IP | adult | China | 200 | 99 (49, 5) | 109 (54, 5) | 120 (60) | n.a. | n.a. | n.a. |
| Xiaoli X. et al. [49] | RCS | Mixed | pediatric | China | 193 | 120 (62, 18) | 120 (62, 18) | 23 (11, 92) | 8 (4, 15) | 15 (7, 77) | 32 (16, 58) |
| Huang M. et al. [50] | RCS | IP | Mixed | China | 197 | 109 (55, 33) | 55 (27, 92) | 9 (4, 57) | 2 (1, 02) | 4 (2, 03) | 17 (8, 63) |
| Yan Y. et al. [51] | RCS | IP | adult | China | 193 | 114 (59, 07) | 108 (55, 96) | 51 (26, 42) | 14 (7, 25) | n.a. | 68 (35, 23) |
| Zhou F. et al. [52] | RCS | IP | adult | China | 191 | 119 (62, 3) | 53 (27, 75) | 9 (4, 71) | 7 (3, 66) | n.a. | n.a. |
| Gong J. et al. [53] | RCS | IP | adult | China | 189 | 88 (46, 56) | 28 (14, 81) | 8 (4, 23) | n.a. | n.a. | n.a. |
| CDC MMWR USA [54] | RCS | Mixed | Mixed | USA | 180 | 97 (53, 89) | n.a. | 48 (26, 67) | 44 (24, 44) | 15 (8, 33) | n.a. |
| Chen D. et al. [55] | RCS | IP | adult | China | 175 | 83 (47, 43) | 40 (22, 86) | 34 (19, 43) | 7 (4) | 5 (2, 86) | n.a. |
| Lu X. et al. [56] | RCS | Mixed | pediatric | China | 171 | 104 (60, 82) | 3 (1, 75) | 15 (8, 77) | 11 (6, 43) | n.a. | n.a. |
| Garazzino S et al. [57] | RCS | Mixed | pediatric | Italy | 168 | 94 (55, 95) | 16 (9, 52) | 22 (13, 1) | 9 (5, 36) | n.a. | n.a. |
| Zheng F. et al. [58] | CS | Mixed | adult | China | 161 | 80 (49, 69) | 30 (18, 63) | 17 (10, 56) | 6 (3, 73) | n.a. | n.a. |
| Mo P. et al. [59] | CS | IP | adult | China | 155 | 86 (55, 48) | 37 (23, 87) | 7 (4, 52) | 3 (1, 94) | 3 (1, 94) | 26 (31.7)(n.a.) |
| Yang W. et al. [60] | CS | IP | adult | China | 149 | 81 (54, 36) | 14 (9, 4) | 11 (7, 38) | 2 (1, 34) | n.a. | n.a. |
| Fan Z. et al. [61] | RCS | IP | adult | China | 148 | 73 (49, 32) | 10 (6, 76) | 6 (4, 05) | 3 (2, 03) | n.a. | n.a. |
| Chen Q. et al. [62] | RCS | IP | adult | China | 145 | 79 (54, 48) | 43 (29, 66) | 39 (26, 9) | 24 (16, 55) | 8 (5, 52) | 62 (42, 76) |
| Feng Z. et al. [63] | RCS | IP | adult | China | 141 | 72 (51, 06) | 15 (10, 64) | 6 (4, 26) | n.a. | n.a. | 5 (3, 55) |
| Zhang JJ. et al. [64] | CSS | IP | adult | China | 140 | 71 (50, 71) | 58 (41, 43) | 18 (12, 86) | 24 (17, 14) | 8 (5, 71) | 17 (12, 14) |
| Wang D. et al. [65] | CS | IP | adult | China | 138 | 75 (54, 35) | 36 (26, 09) | 14 (10, 14) | 14 (10, 14) | 3 (2, 17) | 55 (39, 86) |
| Liu K. et al. [66] | RCS | IP | adult | China | 137 | 61 (44, 53) | n.a. | 11 (8, 03) | n.a. | n.a. | n.a. |
| Li X. et al. [67] | RCS | IP | adult | China | 131 | 63 (48, 09) | n.a. | 1 (0, 76) | n.a. | n.a. | n.a. |
| Giacomet V. et al. [68] | RCS | IP | pediatric | Italy | 127 | 83 (65, 35) | 20 (15, 75) | 28 (22, 05) | 12 (9, 45) | 8 (6, 3) | n.a. |
| Bai T. et al. [69] | CSS | IP | adult | China | 127 | 80 (62, 99) | 36 (28, 35) | 5 (3, 94) | 3 (2, 36) | n.a. | n.a. |
| Wan S. et al. [70] | RCS | IP | adult | China | 123 | 55 (44, 72) | 21 (17, 07) | n.a. | n.a. | n.a. | 10 (8, 13) |
| Cholankeril G. et al. [71] | RCS | IP | adult | USA | 116 | 62 (53, 45) | 9 (7, 76) | 12 (10, 34) | 5 (4, 31) | 10 (8, 62) | 22 (18, 97) |
| Ma YL. et al. [72] | RCS | Mixed | pediatric | China | 115 | 73 (63, 48) | 3 (2, 61) | n.a. | n.a. | n.a. | n.a. |
| Wang K. et al. [73] | RCS | IP | adult | China | 114 | 58 (50, 88) | n.a. | 3 (2, 63) | n.a. | n.a. | n.a. |
| Klopfenstein T. et al. [74] | RCS | Mixed | adult | France | 114 | 58 (50, 88) | n.a. | 55 (48, 25) | 25 (21, 93) | 19 (16, 67) | n.a. |
| Peng YD. et al. [75] | RCS | Mixed | adult | China | 112 | 53 (47, 32) | 16 (14, 29) | 15 (13, 39) | n.a. | n.a. | n.a. |
| Liu Y. et al. [76] | RCS | IP | adult | China | 109 | 59 (54, 13) | 53 (48, 62) | 12 (11, 01) | n.a. | n.a. | n.a. |
| Han R. et al. [77] | CSS | IP | adult | China | 108 | 38 (35, 19) | n.a. | 15 (13, 89) | n.a. | n.a. | n.a. |
| Wang D. et al. [78] | RCS | IP | adult | China | 107 | 57 (53, 27) | 20 (18, 69) | 7 (6, 54) | 6 (5, 61) | 2 (1, 87) | n.a. |
| Zhang H. et al. [79] | RCS | IP | adult | China | 107 | 60 (56, 07) | 56 (52, 34) | 15 (14, 02) | n.a. | n.a. | n.a. |
| Tabata S. et al. [80] | RCS | Mixed | adult | Japan | 104 | 54 (51, 92) | 28 (26, 92) | 9 (8, 65) | n.a. | n.a. | n.a. |
| Ai J. et al. [81] | RCS | IP | adult | China | 102 | 52 (50, 98) | 8 (7, 84) | 15 (14, 71) | 9 (8, 82) | n.a. | 11 (10, 78) |
| Zhao W. et al. [82] | RCS | IP | adult | China | 101 | 56 (55, 45) | 14 (13, 86) | 15 (14, 85) | 2 (1, 98) | n.a. | n.a. |
| Chen N. et al. [83] | CS | IP | adult | China | 99 | 67 (67, 68) | 17 (17, 17) | n.a. | 2 (2, 02) | n.a. | 1 (1, 01) |
| Lin L. et al. [84] | RCS | IP | adult | China | 95 | 45 (47, 37) | 20 (21, 05) | 23 (24, 21) | 21 (22, 11) | 2 (2, 11) | 17 (17, 89) |
| Yu X. et al. [85] | RCS | 0 | adult | China | 92 | 57 (61, 96) | 41 (44, 57) | 7 (7, 61) | 4 (4, 35) | n.a. | n.a. |
| Qian GQ. et al. [86] | RCS | IP | adult | China | 91 | 37 (40, 66) | 9 (9, 89) | 21 (23, 08) | 11 (12, 09) | n.a. | 23 (25, 27) |
| Zhao XY. et al. [87] | RCS | IP | adult | China | 91 | 49 (53, 85) | 30 (33) | 14 (15, 38) | 19 (20, 88) | n.a. | 19 (20, 88) |
| Xu X. et al. [88] | RCS | IP | adult | China | 90 | 39 (43, 33) | n.a. | 5 (5, 56) | 5 (5, 56) | n.a. | n.a. |
| Chen S. et al. [89] | CSS | IP | Mixed | China | 89 | 30 (33, 71) | n.a. | 5 (5, 62) | 2 (2, 25) | n.a. | n.a. |
| Xu W. et al. [90] | CSS | IP | Mixed | china | 87 | 46 (52, 87) | 40 (45, 98) | n.a. | n.a. | n.a. | n.a. |
| Kluytmans M. et al. [91] | RCS | Mixed | adult | Germany | 86 | 15 (17, 44) | n.a. | 16 (18, 6) | 15 (17, 44) | 5 (5, 81) | 15 (17, 44) |
| Wei X-S. et al. [92] | CS | IP | adult | China | 84 | 28 (33, 33) | n.a. | n.a. | 16 (19, 05) | 5 (5, 95) | n.a. |
| Li K. et al. [93] | RCS | IP | adult | China | 83 | 44 (53, 01) | 25 (30, 12) | 7 (8, 43) | n.a. | n.a. | n.a. |
| Shi H. et al. [94] | CS | IP | adult | China | 81 | 42 (51, 85) | n.a. | 3 (3, 7) | 4 (4, 94) | n.a. | 1 (1, 23) |
| Cai Q. et al. [95] | CSS | IP | adult | China | 80 | 35 (43, 75) | n.a. | 1 (1, 25) | n.a. | n.a. | n.a. |
| Wu J. et al. [96] | RCS | IP | adult | China | 80 | 42 (52, 5) | n.a. | 7 (8, 75) | n.a. | n.a. | n.a. |
| Wu J. et al. [97] | CSS | IP | adult | China | 80 | 39 (48, 75) | 3 (3, 75) | 1 (1, 25) | 1 (1, 25) | n.a. | n.a. |
| Fang X. et al. [98] | RCS | Mixed | adult | China | 79 | 45 (56, 96) | 24 (30, 38) | 4 (5, 06) | n.a. | n.a. | 5 (6, 33) |
| Zhao W. et al. [99] | RCS | IP | Mixed | China | 77 | 34 (44, 16) | 20 (25, 97) | 1 (1, 3) | 6 (7, 79) | n.a. | 7 (9, 09) |
| Yu F. et al. [100] | RCS | IP | adult | China | 76 | 38 (50) | 17 (22, 37) | 3 (3, 95) | 4 (5, 26) | n.a. | 9 (11, 84) |
| Zhao Z. et al. [101] | CS | IP | adult | China | 75 | 42 (56) | n.a. | 7 (9, 33) | n.a. | n.a. | 9 (12) |
| Wu Y. et al. [102] | RCS | Mixed | adult | China | 74 | 39 (52, 7) | 18 (24, 32) | n.a. | n.a. | n.a. | n.a. |
| Xiao F. et al. [4] | RCS | IP | Mixed | China | 73 | 41 (56, 16) | 4 (5, 48) | 26 (35, 62) | n.a. | n.a. | n.a. |
| Tang X. et al. [103] | CCS | IP | adult | China | 73 | 45 (61, 64) | 73 (100) | n.a. | n.a. | n.a. | n.a. |
| Zhou S. et al. [104] | RCS | IP | adult | China | 62 | 39 (62, 9) | n.a. | 9 (14, 52) | n.a. | n.a. | n.a. |
| Xu XW. et al. [105] | RCS | IP | adult | China | 62 | 35 (56, 45) | 1 (1, 61) | 3 (4, 84) | n.a. | n.a. | n.a. |
| Miao C. et al. [106] | CSS | IP | adult | China | 62 | 32 (51, 61) | 4 (6, 45) | 7 (11, 29) | n.a. | n.a. | n.a. |
| Cheung KS. et al. [107] | RCS | Mixed | adult | China | 59 | 27 (45, 76) | n.a. | 13 (22, 03) | 1 (1, 69) | 7 (11, 86) | n.a. |
| Grein J. et al. [108] | RCS | IP | adult | USA, Europa and Japan | 53 | 40 (75, 47) | 34 (64, 15) | 5 (9, 43) | n.a. | n.a. | n.a. |
| Fu H. et al. [109] | RCS | IP | adult | China | 52 | 28 (53, 85) | 10 (19, 23) | 7 (13, 46) | 1 (1, 92) | n.a. | n.a. |
| Yang X. et al. [110] | RCS | IP | adult | China | 52 | 35 (67, 31) | 52 (100) | n.a. | 2 (3, 85) | n.a. | n.a. |
| Song F. et al. [111] | CSS | IP | adult | China | 51 | 25 (49, 02) | 4 (7, 84) | 5 (9, 8) | 3 (5, 88) | n.a. | 9 (17, 65) |
| Xu T. et al. [112] | RCS | IP | adult | China | 51 | 25 (49, 02) | n.a. | n.a. | n.a. | n.a. | n.a. |
| Dreher M. et al. [113] | RCS | IP | Mixed | Germany | 50 | 33 (66) | 24 (48) | 8 (16) | 2 (4) | n.a. | n.a. |
| Xu YH. et al. [114] | CSS | IP | Mixed | China | 50 | 29 (58) | 13 (26) | n.a. | n.a. | n.a. | n.a. |
| Colaneri M. et al. [115] | RCS | Mixed | Mixed | Italy | 44 | 28 (63, 64) | 17 (38, 64) | 3 (6, 82) | n.a. | n.a. | n.a. |
| Jin J-M. et al. [116] | CS | IP | adult | China | 43 | 22 (51, 16) | 30 (69, 77) | 7 (16, 28) | n.a. | n.a. | n.a. |
| Xiong Y. et al. [117] | RCS | IP | adult | China | 42 | 25 (59, 52) | n.a. | 10 (23, 81) | n.a. | n.a. | n.a. |
| Meng J. et al. [118] | RCS | IP | adult | China | 42 | 24 (57, 14) | 16 (38, 1) | 3 (7, 14) | 2 (4, 76) | n.a. | 1 (2, 38) |
| Huang C. et al. [119] | RCS | IP | adult | China | 41 | 30 (73, 17) | 13 (31, 71) | 1 (2, 44) | n.a. | n.a. | n.a. |
| Rodriguez-Lago I. et al. [120] | RCS | IP | adult | Spain | 40 | 24 (60) | 2 (5) | 9 (22, 5) | n.a. | n.a. | n.a. |
| Wu WS. et al. [121] | RCS | Mixed | Mixed | China | 40 | 13 (32, 5) | 17 (42, 5) | 6 (15) | 3 (7, 5) | 3 (7, 5) | n.a. |
| Yao N. et al. [122] | CSS | Mixed | adult | China | 40 | 25 (62, 5) | 6 (15) | 7 (17, 5) | 7 (17, 5) | n.a. | n.a. |
| Overall | Chinese | Non-Chinese | |||||
|---|---|---|---|---|---|---|---|
| Prevalence (95% CI) | n/Patients | Prevalence (95% CI) | n/Patients | Prevalence(95% CI) | n/Patients | p * | |
| Diarrhea | 0.15 (0.12, 0.19) | 44/62,892 | 0.12 (0.17, 0.32) | 31/12,798 | 0.24 (0.09, 0.16) | 13/50,094 | <0.001 |
| Nausea/vomiting | 0.10 (0.08, 0.12) | 44/46,390 | 0.07 (0.04, 0.10) | 29/10,345 | 0.17 (0.14, 0.19) | 15/36,045 | <0.001 |
| Abdominal pain | 0.06 (0.04, 0.07) | 38/34,713 | 0.04 (0.02, 0.05) | 22/5272 | 0.09 (0.07, 0.11) | 16/29,441 | <0.001 |
| Anorexia | 0.18 (0.10, 0.27) | 37/22,743 | 0.21 (0.02, 0.51) | 31/6099 | 0.17 (0.11, 0.24) | 6/16,644 | 0.783 |
| Severe | 0.18 (0.07, 0.31) | 44/75,086 | 0.17 (0.13, 0.22) | 30/11,515 | 0.17 (0.02, 0.45) | 14/63,571 | 0.978 |
| Any GI symptom | 0.21 (0.16, 0.27) | 50/71,593 | 0.19 (0.13, 0.26) | 33/13,808 | 0.24 (0.15, 0.35) | 17/57,785 | 0.370 |
| Fever | 0.73 (0.70, 0.76) | 45/74,543 | 0.75 (0.69, 0.81) | 30/12,309 | 0.69 (0.65, 0.73) | 15/62,234 | 0.088 |
| Respiratory | 0.60 (0.56, 0.64) | 43/74,115 | 0.55 (0.48, 0.62) | 29/12,120 | 0.70 (0.67, 0.73) | 14/61,995 | <0.001 |
| Overall | Inpatient | Mix | |||||
|---|---|---|---|---|---|---|---|
| Prevalence (95% CI) | n/Patients | Prevalence(95% CI) | n/Patients | Prevalence (95% CI) | n/Patients | p * | |
| Diarrhea** | 0.15 (0.12, 0.19) | 44/62,892 | 0.14 (0.10, 0.19) | 24/25,508 | 0.16 (0.11, 0.21) | 18/36,655 | 0.795 |
| Nausea/vomiting | 0.10 (0.08, 0.12) | 44/46,390 | 0.12 (0.09, 0.15) | 22/10,228 | 0.08 (0.05, 0.11) | 22/36,162 | 0.096 |
| Abdominal pain | 0.06 (0.04, 0.07) | 38/34,713 | 0.04 (0.03, 0.06) | 20/6508 | 0.07 (0.05, 0.10) | 18/28,205 | 0.032 |
| Anorexia | 0.18 (0.10, 0.27) | 37/22,743 | 0.15 (0.08, 0.24) | 28/19,576 | 0.27 (0.09, 0.50) | 9/3167 | 0.260 |
| Severe ** | 0.18 (0.07, 0.31) | 44/75,086 | 0.26 (0.08, 0.49) | 24/32,013 | 0.09 (0.04, 0.16) | 20/43,073 | 0.111 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Akin, H.; Kurt, R.; Tufan, F.; Swi, A.; Ozaras, R.; Tahan, V.; Hammoud, G. Newly Reported Studies on the Increase in Gastrointestinal Symptom Prevalence with COVID-19 Infection: A Comprehensive Systematic Review and Meta-Analysis. Diseases 2020, 8, 41. https://0-doi-org.brum.beds.ac.uk/10.3390/diseases8040041
Akin H, Kurt R, Tufan F, Swi A, Ozaras R, Tahan V, Hammoud G. Newly Reported Studies on the Increase in Gastrointestinal Symptom Prevalence with COVID-19 Infection: A Comprehensive Systematic Review and Meta-Analysis. Diseases. 2020; 8(4):41. https://0-doi-org.brum.beds.ac.uk/10.3390/diseases8040041
Chicago/Turabian StyleAkin, Hakan, Ramazan Kurt, Fatih Tufan, Ahmed Swi, Resat Ozaras, Veysel Tahan, and Ghassan Hammoud. 2020. "Newly Reported Studies on the Increase in Gastrointestinal Symptom Prevalence with COVID-19 Infection: A Comprehensive Systematic Review and Meta-Analysis" Diseases 8, no. 4: 41. https://0-doi-org.brum.beds.ac.uk/10.3390/diseases8040041