
Circulatory Shock among Hospitalized Patients for Salicylate Intoxication

 ,
,  , , ,
, , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source
2.2. Study Population
2.3. Data Collection
2.4. Statistical Analysis
3. Results
3.1. Incidence and Risk Factors for Circulatory Shock in Hospitalized Salicylate Intoxication Patients
3.2. The Association of Circulatory Shock with In-Hospital Treatments, Outcomes, and Resource Use
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pearlman, B.L.; Gambhir, R. Salicylate intoxication: A clinical review. Postgrad. Med. 2009, 121, 162–168. [Google Scholar] [CrossRef] [PubMed]
- Gummin, D.D.; Mowry, J.B.; Spyker, D.A.; Brooks, D.E.; Beuhler, M.C.; Rivers, L.J.; Hashem, H.A.; Ryan, M.L. 2018 Annual Report of the American Association of Poison Control Centers’ National Poison Data System (NPDS): 36th Annual Report. Clin. Toxicol. (Phila) 2019, 57, 1220–1413. [Google Scholar] [CrossRef] [PubMed]
- Palmer, B.F.; Clegg, D.J. Salicylate Toxicity. N. Engl. J. Med. 2020, 382, 2544–2555. [Google Scholar] [CrossRef] [PubMed]
- Walton, R.P.; Darby, T.D. Circulatory effects of salicylates. Circ. Res. 1958, 6, 155–158. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thongprayoon, C.; Petnak, T.; Kaewput, W.; Mao, M.A.; Kovvuru, K.; Kanduri, S.R.; Boonpheng, B.; Bathini, T.; Vallabhajosyula, S.; Pivovarova, A.I.; et al. Hospitalizations for Acute Salicylate Intoxication in the United States. J. Clin. Med. 2020, 9, 2638. [Google Scholar] [CrossRef] [PubMed]
- Bathini, T.; Thongprayoon, C.; Petnak, T.; Chewcharat, A.; Cheungpasitporn, W.; Boonpheng, B.; Chokesuwattanaskul, R.; Prasitlumkum, N.; Vallabhajosyula, S.; Kaewput, W. Circulatory Failure among Hospitalizations for Heatstroke in the United States. Medicines 2020, 7, 32. [Google Scholar] [CrossRef] [PubMed]
- Kaewput, W.; Thongprayoon, C.; Boonpheng, B.; Ungprasert, P.; Bathini, T.; Chewcharat, A.; Srivali, N.; Vallabhajosyula, S.; Cheungpasitporn, W. Inpatient Burden and Mortality of Goodpasture’s Syndrome in the United States: Nationwide Inpatient Sample 2003–2014. J. Clin. Med. 2020, 9, 455. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chalasani, N.; Roman, J.; Jurado, R.L. Systemic inflammatory response syndrome caused by chronic salicylate intoxication. South. Med. J. 1996, 89, 479–482. [Google Scholar] [CrossRef] [PubMed]
- Pei, Y.P.; Thompson, D.A. Severe salicylate intoxication mimicking septic shock. Am. J. Med. 1987, 82, 381–382. [Google Scholar] [CrossRef]
- Landry, D.W.; Oliver, J.A. The pathogenesis of vasodilatory shock. N. Engl. J. Med. 2001, 345, 588–595. [Google Scholar] [CrossRef] [PubMed]
- Marano, G.; Traversi, G.; Romagnoli, E.; Catalano, V.; Lotrionte, M.; Abbate, A.; Biondi-Zoccai, G.; Mazza, M. Cardiologic side effects of psychotropic drugs. J. Geriatr. Cardiol. 2011, 8, 243–253. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Temple, A.R. Acute and chronic effects of aspirin toxicity and their treatment. Arch. Intern. Med. 1981, 141, 364–369. [Google Scholar] [CrossRef] [PubMed]
- Greenblatt, D.J.; Abernethy, D.R.; Boxenbaum, H.G.; Matlis, R.; Ochs, H.R.; Harmatz, J.S.; Shader, R.I. Influence of age, gender, and obesity on salicylate kinetics following single doses of aspirin. Arthritis Rheum. 1986, 29, 971–980. [Google Scholar] [CrossRef] [PubMed]
- Chyka, P.A.; Erdman, A.R.; Christianson, G.; Wax, P.M.; Booze, L.L.; Manoguerra, A.S.; Caravati, E.M.; Nelson, L.S.; Olson, K.R.; Cobaugh, D.J.; et al. Salicylate poisoning: An evidence-based consensus guideline for out-of-hospital management. Clin. Toxicol. (Phila) 2007, 45, 95–131. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Total | Circulatory Shock | No Circulatory Shock | p-Value | |
|---|---|---|---|---|
| Clinical Characteristics | ||||
| N (%) | 13,805 | 484 | 13,321 | |
| Age (years), mean ± SD | 34.0 ± 18.7 | 47.6 ± 19.0 | 33.5 ± 18.5 | <0.001 |
| <20 | 3902 (28.3) | 42 (8.7) | 3860 (29.0) | <0.001 |
| 20–29 | 3228 (23.4) | 61 (12.6) | 3167 (23.8) | |
| 30–39 | 1951 (14.1) | 56 (11.6) | 1895 (14.2) | |
| ≥40 | 4710 (34.2) | 325 (67.1) | 4385 (33.0) | |
| Female | 8994 (65.0) | 344 (71.1) | 8650 (64.9) | 0.005 |
| Race | <0.001 | |||
| Caucasian | 7729 (56.0) | 319 (65.9) | 7410 (55.6) | |
| African American | 1391 (10.1) | 39 (8.0) | 1352 (10.1) | |
| Hispanic | 1311 (9.5) | 38 (7.9) | 1273 (9.6) | |
| Asian or Pacific Islander | 200 (1.4) | 4 (0.8) | 196 (1.5) | |
| Other | 3174 (23.0) | 84 (17.4) | 3090 (23.2) | |
| Year of hospitalization | <0.001 | |||
| 2003–2006 | 5011 (36.3) | 86 (17.8) | 4925 (37.0) | |
| 2007–2010 | 4434 (32.1) | 156 (32.2) | 4278 (32.1) | |
| 2011–2014 | 4360 (31.6) | 242 (50.0) | 4118 (30.9) | |
| Alcohol drinking | 2216 (16.1) | 73 (15.1) | 2143 (16.1) | 0.55 |
| Analgesics overdose | 967 (7.0) | 37 (7.6) | 930 (7.0) | 0.57 |
| Psychotropic agent overdose | 896 (6.5) | 48 (9.9) | 848 (6.4) | 0.002 |
| Obesity | 521 (3.8) | 15 (3.1) | 506 (3.8) | 0.43 |
| Anemia | 897 (6.5) | 98 (20.2) | 799 (6.0) | <0.001 |
| Diabetes Mellitus | 801 (5.8) | 49 (10.1) | 752 (5.6) | <0.001 |
| Hypertension | 2137 (15.5) | 129 (26.7) | 2008 (15.1) | <0.001 |
| Dyslipidemia | 749 (5.4) | 35 (7.2) | 714 (5.4) | 0.07 |
| Coronary artery disease | 512 (3.7) | 60 (12.4) | 452 (3.4) | <0.001 |
| Congestive heart failure | 239 (1.7) | 31 (6.4) | 208 (1.6) | <0.001 |
| Atrial flutter/fibrillation | 172 (1.2) | 20 (4.1) | 152 (1.1) | <0.001 |
| Chronic kidney disease | 218 (1.6) | 27 (5.6) | 191 (1.4) | <0.001 |
| Liver cirrhosis | 116 (0.8) | 5 (1.0) | 111 (0.8) | 0.61 |
| Volume depletion | 739 (5.4) | 67 (13.8) | 672 (5.0) | <0.001 |
| Rhabdomyolysis | 258 (1.9) | 33 (6.8) | 225 (1.7) | <0.001 |
| Seizure | 565 (4.1) | 45 (9.3) | 520 (3.9) | <0.001 |
| Gastrointestinal bleeding | 363 (2.6) | 38 (7.9) | 325 (2.4) | <0.001 |
| Sepsis | 126 (0.9) | 48 (9.9) | 78 (0.6) | <0.001 |
| Cardiac arrest | 95 (0.7) | 14 (2.9) | 81 (0.6) | <0.001 |
| Treatments | ||||
| Gastric lavage | 344 (2.5) | 18 (3.7) | 326 (2.4) | 0.08 |
| Noninvasive ventilation | 64 (0.5) | 7 (1.4) | 57 (0.4) | 0.007 |
| Invasive mechanical ventilation | 760 (5.5) | 153 (31.6) | 607 (4.6) | <0.001 |
| Blood component transfusion | 356 (2.6) | 68 (14.0) | 288 (2.2) | <0.001 |
| Renal replacement therapy | 811 (5.9) | 116 (24.0) | 695 (5.2) | <0.001 |
| Outcomes | ||||
| Renal failure | 1279 (9.3) | 157 (32.4) | 1122 (8.4) | <0.001 |
| Respiratory failure | 943 (6.8) | 168 (34.7) | 775 (5.8) | <0.001 |
| Liver failure | 110 (0.8) | 20 (4.1) | 90 (0.7) | <0.001 |
| Neurological failure | 689 (5.0) | 64 (13.2) | 625 (4.7) | <0.001 |
| Hematological failure | 303 (2.2) | 48 (9.9) | 255 (1.9) | <0.001 |
| In-hospital mortality | 132 (1.0) | 26 (5.4) | 106 (0.8) | <0.001 |
| Resource Utilization | ||||
| Length of hospital stay (days), mean ± SD | 2.6 ± 3.3 | 6.0 ± 7.3 | 2.4 ± 3.0 | <0.001 |
| Hospitalization cost (USD), mean ± SD | 18,128 ± 29,613 | 52,933 ± 83,537 | 16,856 ± 24,668 | <0.001 |
| Variables | Univariable Analysis | Multivariable Analysis | ||
|---|---|---|---|---|
| Crude Odds Ratio (95%CI) | p-Value | Adjusted Odds Ratio (95%CI) | p-Value | |
| Age (years) | ||||
| <20 | 1 (reference) | 1 (reference) | ||
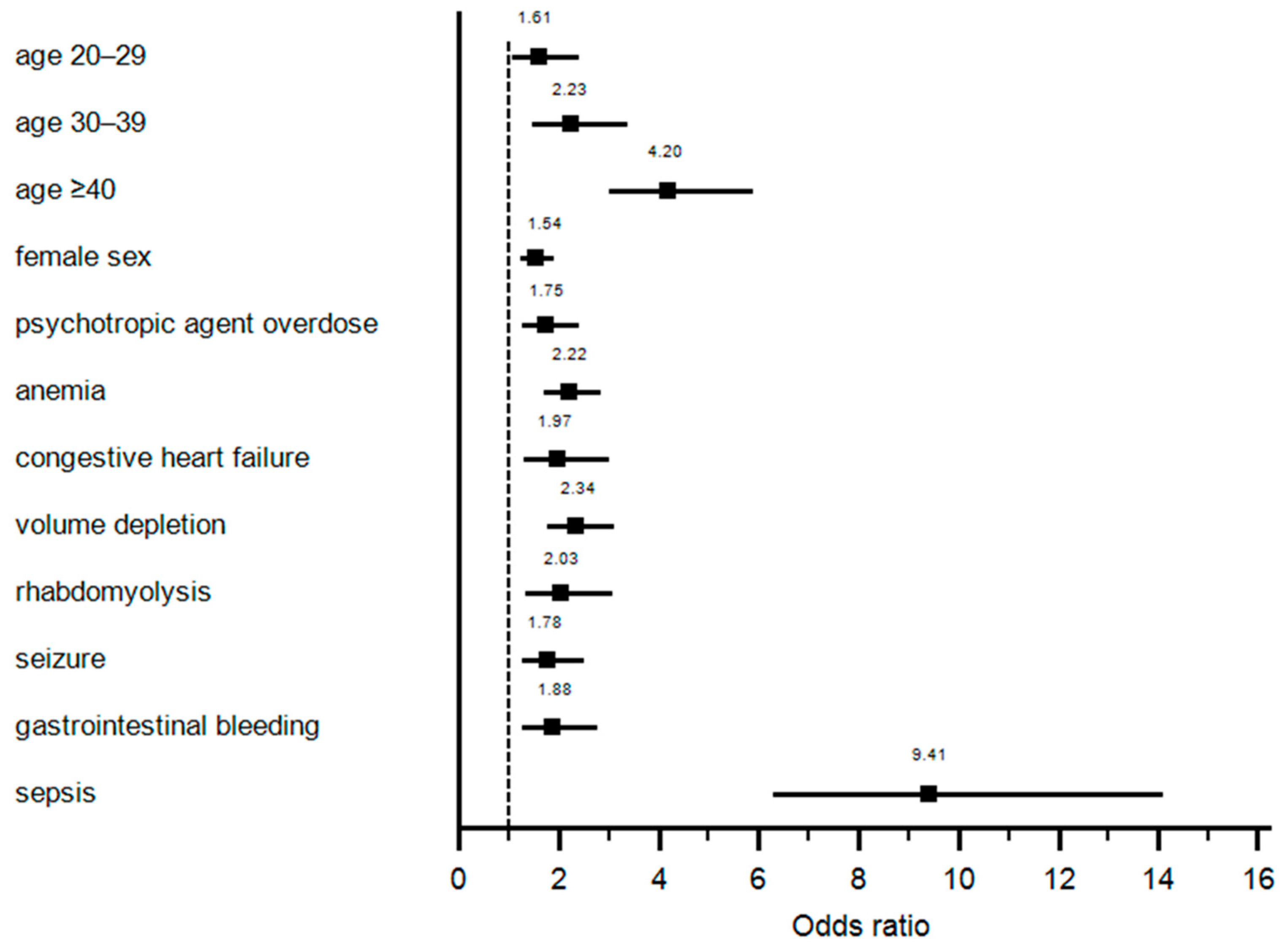
| 20–29 | 1.77 (1.19–2.63) | 0.005 | 1.61 (1.08–2.40) | 0.02 |
| 30–39 | 2.72 (1.81–4.07) | <0.001 | 2.23 (1.48–3.37) | <0.001 |
| ≥40 | 6.81 (4.93–9.42) | <0.001 | 4.20 (3.00–5.88) | <0.001 |
| Female | 1.33 (1.09–1.64) | 0.005 | 1.54 (1.25–1.92) | <0.001 |
| Race | ||||
| Caucasian | 1 (reference) | |||
| African American | 0.67 (0.48–0.94) | 0.02 | ||
| Hispanic | 0.69 (0.49–0.98) | 0.04 | ||
| Asian or Pacific Islander | 0.47 (0.18–1.28) | 0.14 | ||
| Other | 0.63 (0.50–0.81) | <0.001 | ||
| Year of data collection | ||||
| 2003–2006 | 1 (reference) | 1 (reference) | ||
| 2007–2010 | 2.09 (1.60–2.73) | <0.001 | 1.88 (1.43–2.47) | <0.001 |
| 2011–2014 | 3.37 (2.62–4.32) | <0.001 | 2.86 (2.21–3.70) | <0.001 |
| Alcoholic drinking | 0.93 (0.72–1.19) | 0.55 | ||
| Analgesics overdose | 1.10 (0.78–1.55) | 0.58 | ||
| Psychotropic agent overdose | 1.62 (1.19–2.20) | 0.002 | 1.75 (1.27–2.40) | 0.001 |
| Obesity | 0.81 (0.48–1.37) | 0.43 | ||
| Anemia | 3.98 (3.15–5.02) | <0.001 | 2.22 (1.72–2.86) | <0.001 |
| Diabetes Mellitus | 1.88 (1.39–2.55) | <0.001 | ||
| Hypertension | 2.05 (1.66–2.52) | <0.001 | ||
| Dyslipidemia | 1.38 (0.97–1.96) | 0.08 | ||
| Coronary artery disease | 4.03 (3.03–5.36) | <0.001 | ||
| Congestive heart failure | 4.31 (2.93–6.36) | <0.001 | 1.97 (1.29–3.01) | 0.002 |
| Atrial flutter/fibrillation | 3.73 (2.32–6.01) | <0.001 | ||
| Chronic kidney disease | 4.06 (2.69–6.14) | <0.001 | ||
| Liver cirrhosis | 1.24 (0.51–3.06) | 0.64 | ||
| Volume depletion | 3.02 (2.31–3.96) | <0.001 | 2.34 (1.76–3.11) | <0.001 |
| Rhabdomyolysis | 4.26 (2.92–6.21) | <0.001 | 2.03 (1.34–3.07) | 0.001 |
| Seizure | 2.52 (1.83–3.47) | <0.001 | 1.78 (1.27–2.50) | 0.001 |
| Gastrointestinal bleeding | 3.41 (2.40–4.83) | <0.001 | 1.88 (1.27–2.77) | 0.001 |
| Sepsis | 18.69 (12.89–27.12) | <0.001 | 9.41 (6.28–14.08) | <0.001 |
| Cardiac arrest | 4.87 (2.74–8.65) | <0.001 | ||
| Gastric lavage | 1.54 (0.95–2.50) | 0.08 | ||
| Variables | Univariable Analysis | Multivariable Analysis | ||
|---|---|---|---|---|
| Crude Odds Ratio (95%CI) | p-Value | Adjusted Odds Ratio * (95%CI) | p-Value | |
| Treatment | ||||
| Noninvasive ventilation | 3.42 (1.55–7.53) | 0.002 | 1.01 (0.41–2.49) | 0.98 |
| Invasive mechanical ventilation | 9.68 (7.86–11.92) | <0.001 | 5.01 (3.89–6.45) | <0.001 |
| Blood component transfusion | 7.40 (5.58–9.80) | <0.001 | 3.12 (2.19–4.44) | <0.001 |
| Renal replacement therapy | 5.73 (4.59–7.15) | <0.001 | 3.04 (2.37–3.90) | <0.001 |
| Complication and Outcome | ||||
| Renal failure | 5.22 (4.27–6.38) | <0.001 | 2.59 (2.04–3.28) | <0.001 |
| Respiratory failure | 8.61 (7.04–10.52) | <0.001 | 4.39 (3.45–5.59) | <0.001 |
| Liver failure | 6.34 (3.87–10.38) | <0.001 | 3.04 (1.73–5.35) | <0.001 |
| Neurological failure | 3.10 (2.35–4.08) | <0.001 | 1.75 (1.30–2.36) | <0.001 |
| Hematological failure | 5.64 (4.09–7.79) | <0.001 | 2.71 (1.89–3.88) | <0.001 |
| In-hospital mortality | 7.08 (4.56–10.98) | <0.001 | 3.43 (1.88–6.24) | <0.001 |
| Resource Utilization | Coefficient (95% CI) | p-Value | Adjusted Coefficient (95% CI) | p-Value |
| Length of hospital stay (days) | 3.5 (3.2–3.8) | <0.001 | 1.7 (1.4–2.0) | <0.001 |
| Hospitalization cost (USD) | 36,078 (33,449–38,706) | <0.001 | 18,801 (16,346–21,255) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Petnak, T.; Thongprayoon, C.; Kaewput, W.; Qureshi, F.; Boonpheng, B.; Vallabhajosyula, S.; Bathini, T.; Mao, M.A.; Lertjitbanjong, P.; Cheungpasitporn, W. Circulatory Shock among Hospitalized Patients for Salicylate Intoxication. Diseases 2021, 9, 7. https://0-doi-org.brum.beds.ac.uk/10.3390/diseases9010007
Petnak T, Thongprayoon C, Kaewput W, Qureshi F, Boonpheng B, Vallabhajosyula S, Bathini T, Mao MA, Lertjitbanjong P, Cheungpasitporn W. Circulatory Shock among Hospitalized Patients for Salicylate Intoxication. Diseases. 2021; 9(1):7. https://0-doi-org.brum.beds.ac.uk/10.3390/diseases9010007
Chicago/Turabian StylePetnak, Tananchai, Charat Thongprayoon, Wisit Kaewput, Fawad Qureshi, Boonphiphop Boonpheng, Saraschandra Vallabhajosyula, Tarun Bathini, Michael A. Mao, Ploypin Lertjitbanjong, and Wisit Cheungpasitporn. 2021. "Circulatory Shock among Hospitalized Patients for Salicylate Intoxication" Diseases 9, no. 1: 7. https://0-doi-org.brum.beds.ac.uk/10.3390/diseases9010007