
Incidence and Characteristics of Kidney Stones in Patients on Ketogenic Diet: A Systematic Review and Meta-Analysis

 , , , , ,
, , , , , 
Abstract
:1. Introduction
2. Materials and Methods
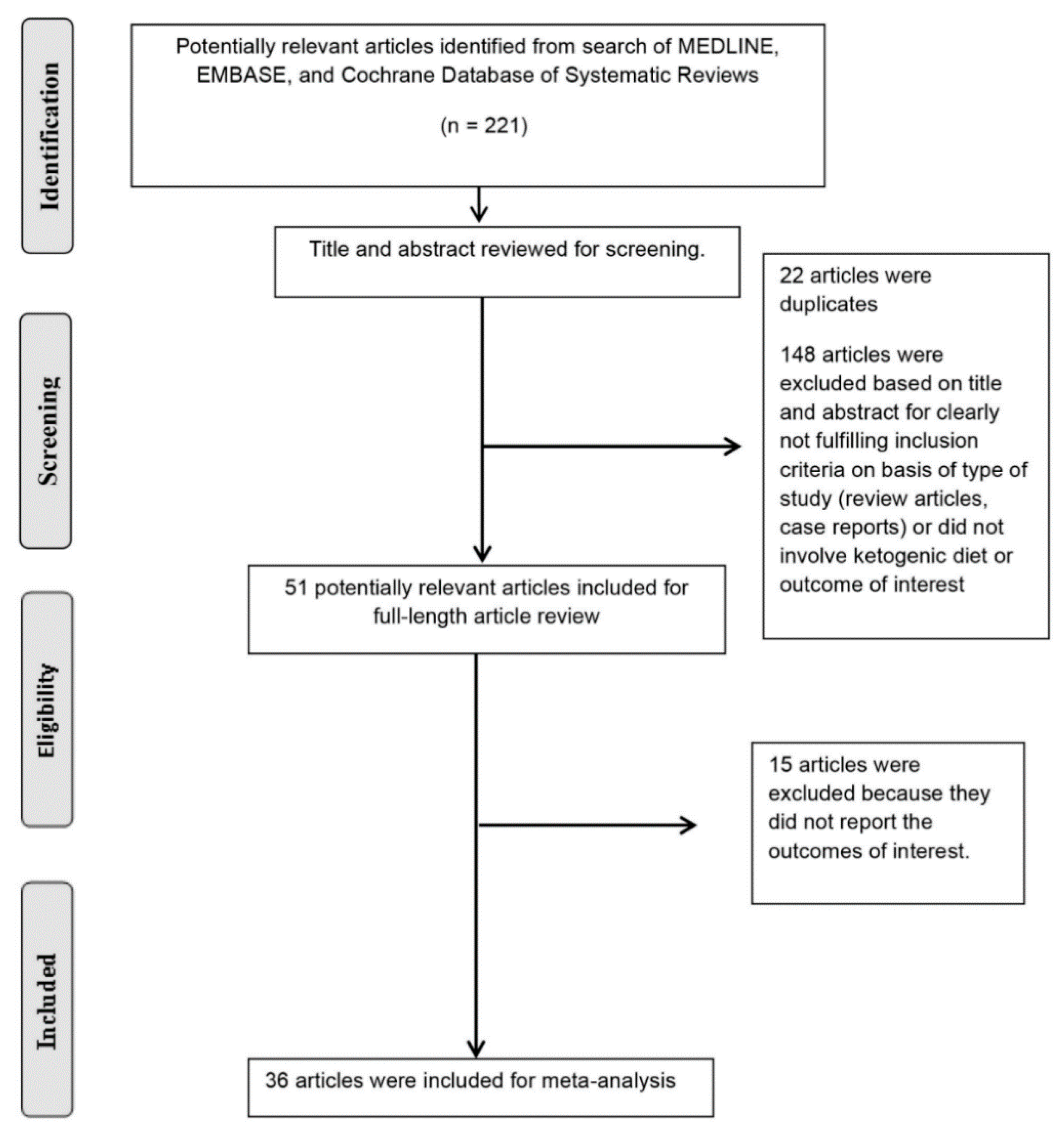
2.1. Search Strategies
2.2. Study Selection
2.3. Data Extraction
2.4. Data Synthesis and Statistical Analysis
3. Results
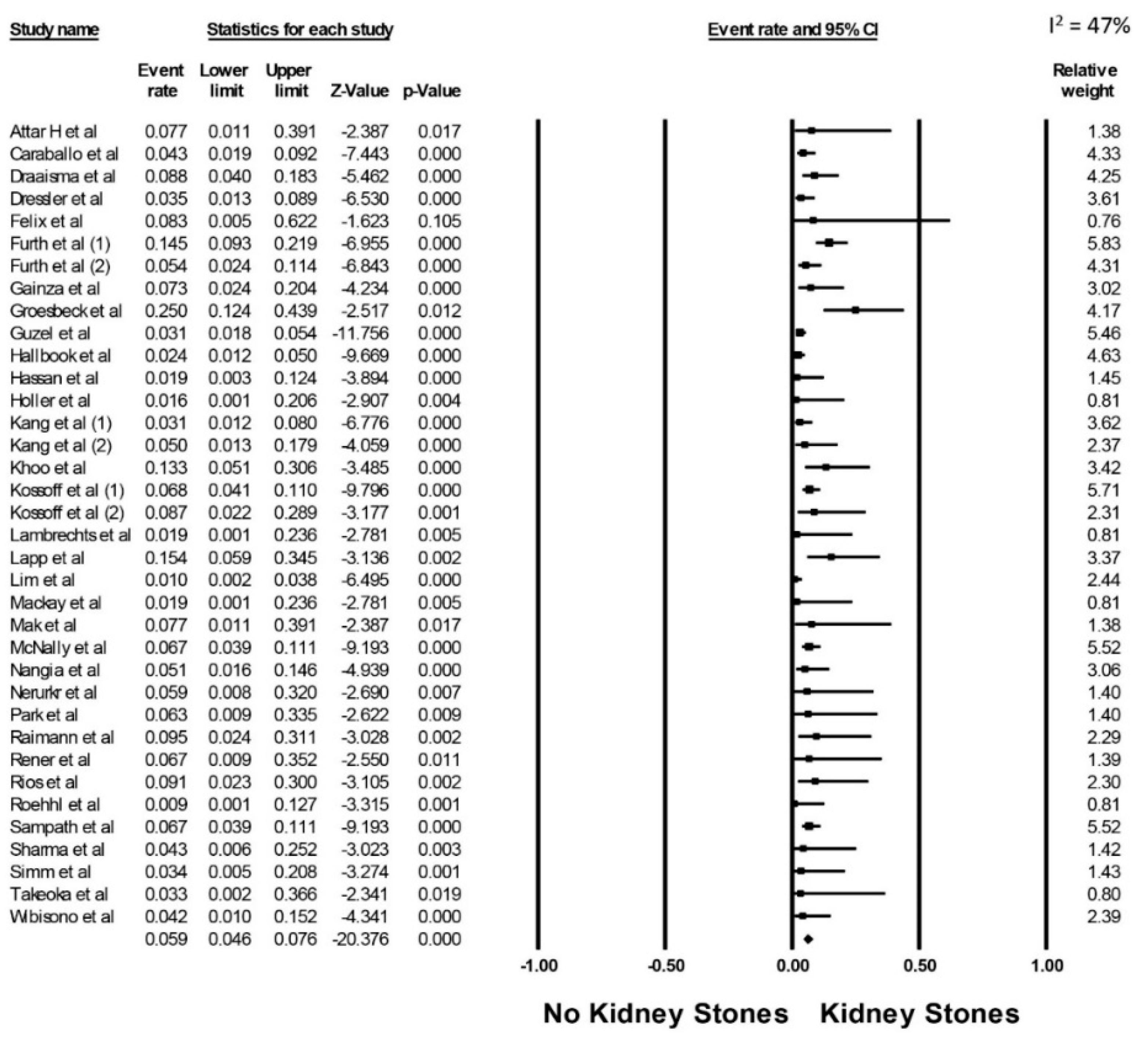
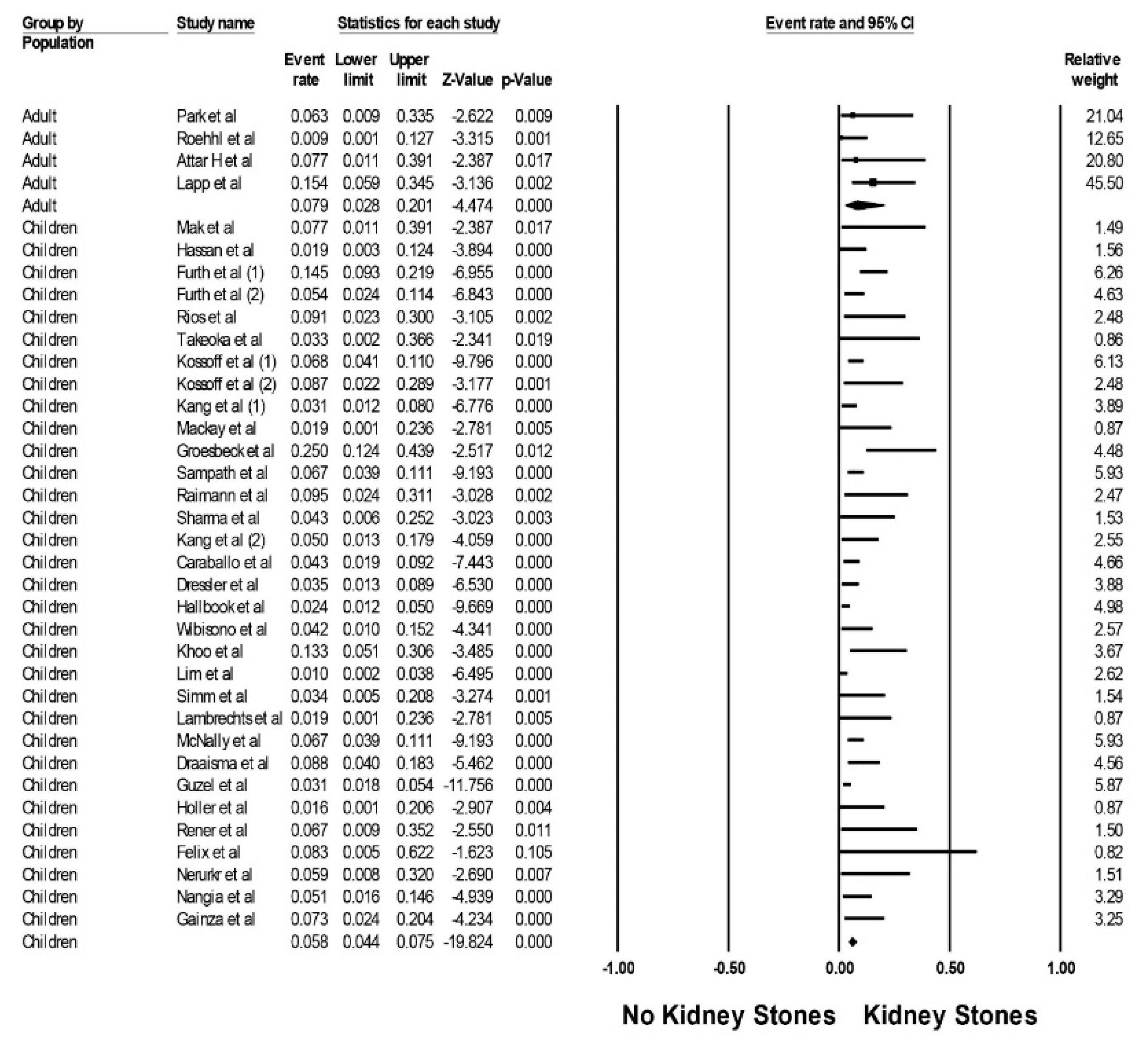
3.1. Incidence of Kidney Stones among Patients on Ketogenic Diets
3.2. Type of Kidney Stones among Patients on Ketogenic Diet
3.3. Evaluation for Publication Bias
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Paoli, A.; Cenci, L.; Grimaldi, K. Effect of ketogenic mediterranean diet with phytoextracts and low carbohydrates/high-protein meals on weight, cardiovascular risk factors, body composition and diet compliance in Italian council employees. Nutr. J. 2011, 10, 112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hawkes, C.P.; Roy, S.M.; Dekelbab, B.; Frazier, B.; Grover, M.; Haidet, J.; Listman, J.; Madsen, S.; Roan, M.; Rodd, C.; et al. Hypercalcemia in Children Using the Ketogenic Diet: A Multicenter Study. J. Clin. Endocrinol. Metab. 2021, 106, e485–e495. [Google Scholar] [CrossRef] [PubMed]
- Sinha, S.R.; Kossoff, E.H. The Ketogenic Diet. Neurology 2005, 11, 161–170. [Google Scholar] [CrossRef] [PubMed]
- Stafstrom, C.E.; Spencer, S. The ketogenic diet: A therapy in search of an explanation. Neurology 2000, 54, 282. [Google Scholar] [CrossRef] [PubMed]
- Hartman, A.L.; Stafstrom, C.E. Harnessing the power of metabolism for seizure prevention: Focus on dietary treatments. Epilepsy Behav. 2013, 26, 266–272. [Google Scholar] [CrossRef] [Green Version]
- Nylen, K.; Likhodii, S.; Burnham, W.M. The ketogenic diet: Proposed mechanisms of action. Neurotherapeutics 2009, 6, 402–405. [Google Scholar] [CrossRef] [Green Version]
- Klesges, R.C.; Ward, K.D.; Shelton, M.L.; Applegate, W.B.; Cantler, E.D.; Palmieri, G.M.A.; Harmon, K.; Davis, J. Changes in Bone Mineral Content in Male Athletes. JAMA 1996, 276, 226–230. [Google Scholar] [CrossRef]
- Wheless, J.W. History of the ketogenic diet. Epilepsia 2008, 49, 3–5. [Google Scholar] [CrossRef]
- Kossoff, E.H.; Zupec-Kania, B.A.; Amark, P.E.; Ballaban-Gil, K.R.; Bergqvist, A.G.C.; Blackford, R.; Buchhalter, J.R.; Caraballo, R.H.; Cross, J.H.; Dahlin, M.G.; et al. Optimal clinical management of children receiving the ketogenic diet: Recommendations of the International Ketogenic Diet Study Group. Epilepsia 2009, 50, 304–317. [Google Scholar] [CrossRef] [PubMed]
- Kossoff, E.H.; Zupec-Kania, B.A.; Rho, J.M. Ketogenic Diets: An Update for Child Neurologists. J. Child Neurol. 2009, 24, 979–988. [Google Scholar] [CrossRef]
- Davidson, T.; Hargrave, S.; Swithers, S.; Sample, C.; Fu, X.; Kinzig, K.; Zheng, W. Inter-relationships among diet, obesity and hippocampal-dependent cognitive function. Neuroscience 2013, 253, 110–122. [Google Scholar] [CrossRef] [PubMed]
- Freedland, S.J.; Mavropoulos, J.; Wang, A.; Darshan, M.; Demark-Wahnefried, W.; Aronson, W.J.; Cohen, P.; Hwang, D.; Peterson, B.; Fields, T.; et al. Carbohydrate restriction, prostate cancer growth, and the insulin-like growth factor axis. Prostate 2008, 68, 11–19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Klepper, J.; Leiendecker, B. GLUT1 deficiency syndrome—2007 update. Dev. Med. Child Neurol. 2007, 49, 707–716. [Google Scholar] [CrossRef] [PubMed]
- Wexler, I.D.; Hemalatha, S.G.; McConnell, J.; Buist, N.; Dahl, H.-H.M.; Berry, S.A.; Cederbaum, S.D.; Patel, M.S.; Kerr, D.S. Outcome of pyruvate dehydrogenase deficiency treated with ketogenic diets: Studies in patients with identical mutations. Neurology 1997, 49, 1655–1661. [Google Scholar] [CrossRef] [PubMed]
- Meira, I.D.; Romão, T.T.; Prado, H.J.P.D.; Krüger, L.T.; Pires, M.E.P.; Da Conceição, P.O. Ketogenic Diet and Epilepsy: What We Know So Far. Front. Neurosci. 2019, 13, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Freeman, J.M.; Kelly, M.T.; Freeman, J.B. The Epilepsy Diet Treatment: An Introduction to the Ketogenic Diet; Demos Vermande: New York, NY, USA, 1996. [Google Scholar]
- Liu, Y.M.; Wang, H.S. Medium-chain triglyceride ketogenic diet, an effective treatment for drug-resistant epilepsy and a comparison with other ketogenic diets. Biomed. J. 2013, 36, 9–15. [Google Scholar] [CrossRef]
- Tanchoco, C.C.; Cruz, A.J.; Rogaccion, J.M.; Casem, R.S.; Rodriguez, M.P.; Orense, C.L.; Hermosura, L.C. Diet supplemented with MCT oil in the management of childhood diarrhea. Asia Pac. J. Clin. Nutr. 2007, 16, 286–292. [Google Scholar]
- Ballaban-Gil, K.; Callahan, C.; O’Dell, C.; Pappo, M.; Moshe, S.; Shinnar, S. Complications of the Ketogenic Diet. Epilepsia 1998, 39, 744–748. [Google Scholar] [CrossRef]
- Bach, A.C.; Babayan, V.K. Medium-chain triglycerides: An update. Am. J. Clin. Nutr. 1982, 36, 950–962. [Google Scholar] [CrossRef]
- Chesney, D.; Brouhard, B.H.; Wyllie, E.; Powaski, K. Biochemical abnormalities of the ketogenic diet in children. Clin. Pediatr. 1999, 38, 107–109. [Google Scholar] [CrossRef]
- Bertoli, S.; Trentani, C.; Ferraris, C.; De Giorgis, V.; Veggiotti, P.; Tagliabue, A. Long-term effects of a ketogenic diet on body composition and bone mineralization in GLUT-1 deficiency syndrome: A case series. Nutrition 2014, 30, 726–728. [Google Scholar] [CrossRef] [PubMed]
- Bergqvist, A.C.; Schall, J.I.; Stallings, V.A. Vitamin D Status in Children with Intractable Epilepsy, and Impact of the Ketogenic Diet. Epilepsia 2007, 48, 66–71. [Google Scholar] [CrossRef] [PubMed]
- Bergqvist, A.G.C.; Schall, J.; Stallings, V.; Zemel, B.S. Progressive bone mineral content loss in children with intractable epilepsy treated with the ketogenic diet. Am. J. Clin. Nutr. 2008, 88, 1678–1684. [Google Scholar] [CrossRef] [Green Version]
- Choi, J.N.; Song, J.E.; Shin, J.I.; Kim, H.D.; Kim, M.J.; Lee, J.S. Renal stone associated with the ketogenic diet in a 5-year old girl with intractable epilepsy. Yonsei Med. J. 2010, 51, 457–459. [Google Scholar] [CrossRef] [Green Version]
- Kielb, S.; Koo, H.P.; Bloom, D.A.; Faerber, G.J. Nephrolithiasis associated with the ketogenic diet. J. Urol. 2000, 164, 464–466. [Google Scholar] [CrossRef]
- Rule, A.D.; Bergstralh, E.J.; Melton, L.J.; Li, X.; Weaver, A.L.; Lieske, J.C. Kidney Stones and the Risk for Chronic Kidney Disease. Clin. J. Am. Soc. Nephrol. 2009, 4, 804–811. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- El-Zoghby, Z.M.; Lieske, J.C.; Foley, R.N.; Bergstralh, E.J.; Li, X.; Melton, L.J.; Krambeck, A.E.; Rule, A.D. Urolithiasis and the Risk of ESRD. Clin. J. Am. Soc. Nephrol. 2012, 7, 1409–1415. [Google Scholar] [CrossRef] [Green Version]
- Thongprayoon, C.; Hansrivijit, P.; Kovvuru, K.; Kanduri, S.R.; Torres-Ortiz, A.; Acharya, P.; Gonzalez-Suarez, M.L.; Kaewput, W.; Bathini, T.; Cheungpasitporn, W. Diagnostics, Risk Factors, Treatment and Outcomes of Acute Kidney Injury in a New Paradigm. J. Clin. Med. 2020, 9, 1104. [Google Scholar] [CrossRef] [Green Version]
- Paul, E.; Conant, K.D.; Dunne, I.E.; Pfeifer, H.H.; Lyczkowski, D.A.; Linshaw, M.A.; Thiele, E.A. Urolithiasis on the ketogenic diet with concurrent topiramate or zonisamide therapy. Epilepsy Res. 2010, 90, 151–156. [Google Scholar] [CrossRef] [Green Version]
- Kang, H.C.; Kim, Y.J.; Kim, N.W.; Kim, H.D. Efficacy and Safety of the Ketogenic Diet for Intractable Childhood Epilepsy: Korean Multicentric Experience. Epilepsia 2005, 46, 272–279. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Easterbrook, P.; Gopalan, R.; Berlin, J.; Matthews, D. Publication bias in clinical research. Lancet 1991, 337, 867–872. [Google Scholar] [CrossRef]
- Holler, A.; Albrecht, U.; Baumgartner Sigl, S.; Zoggeler, T.; Ramoser, G.; Bernar, B.; Karall, D.; Scholl-Burgi, S. Successful implementation of classical ketogenic dietary therapy in a patient with Niemann-Pick disease type C. Mol. Genet. Metab. Rep. 2021, 27, 100723. [Google Scholar] [CrossRef] [PubMed]
- Rener-Primec, Z.; Trojar, A.; Rogač, M.; Neubauer, D. P15.2 Ketogenic diet in infants and toddlers: Efficacy and tolerability in 15 consecutive children. Eur. J. Paediatr. Neurol. 2011, 15, S92. [Google Scholar] [CrossRef]
- Attar, H.; Rolfe, S.; Marsey, M.; Rogers, L. Results of the modified atkins diet in patients with recurrent glioma: Retrospective review. Neurology 2016, 86, 16S. [Google Scholar]
- Felix, G.; Kossoff, E.; Baron, B.; Getzoff, E.; Krekel, C.; Scheimann, A. Preliminary experience of the modified atkins diet for children with prader-willi syndrome. J. Pediatr. Gastroenterol. Nutr. 2017, 65, S191–S192. [Google Scholar] [CrossRef]
- Lapp, K.; Sandok, E.; Timmler, T. Modified atkins/ketogenic diet in adults with epilepsy in a rural community-based clinical practice. Epilepsy Curr. 2012, 12. [Google Scholar]
- Nerurkar, L.; Buttle, J.; Symonds, J.; Zuberi, S.M.; Brunklaus, A. The ketogenic diet in drug-resistant epilepsy of early childhood (<3 years): Indications, tolerability and outcomes. Dev. Med. Child Neurol. 2019, 61, 45. [Google Scholar] [CrossRef] [Green Version]
- Nangia, S.; Blackford, R.; Nordli, D.R.; Berg, A.T. Ketogenic diet: Extending the boundaries of its use. Epilepsy Curr. 2012, 12. [Google Scholar]
- Gainza, M.; Michoulas, A.; Connolly, M.B.; Zanotta, F.; Simonson, C.; Huh, L.; Selby, K.; Farrell, K. Complications of prolonged treatment with the ketogenic diet in treatment resistant epilepsy. Epilepsia 2013, 54, 348–349. [Google Scholar] [CrossRef]
- Mak, S.C.; Chi, C.S.; Wan, C.J. Clinical experience of ketogenic diet on children with refractory epilepsy. Acta Paediatr. Sin. 1999, 40, 97–100. [Google Scholar]
- Furth, S.L.; Casey, J.C.; Pyzik, P.L.; Neu, A.M.; Docimo, S.G.; Vining, E.P.G.; Freeman, J.M.; Fivush, B.A. Risk factors for urolithiasis in children on the ketogenic diet. Pediatr. Nephrol. 2000, 15, 125–128. [Google Scholar] [CrossRef]
- Ríos, V.G.; Panico, L.R.; Demartini, M.G.; Carniello, M.A. Complications of treatment of epilepsy by a ketogenic diet. Rev. Neurol. 2001, 33, 909–915. [Google Scholar] [PubMed]
- Sharma, S.; Gulati, S.; Kalra, V.; Agarwala, A.; Kabra, M. Seizure control and biochemical profile on the ketogenic diet in young children with refractory epilepsy—Indian experience. Seizure 2009, 18, 446–449. [Google Scholar] [CrossRef] [Green Version]
- Kang, H.C.; Chung, D.E.; Kim, D.W.; Kim, H.D. Early- and Late-onset Complications of the Ketogenic Diet for Intractable Epilepsy. Epilepsia 2004, 45, 1116–1123. [Google Scholar] [CrossRef]
- Wibisono, C.; Rowe, N.; Beavis, E.; Kepreotes, H.; Mackie, F.E.; Lawson, J.A.; Cardamone, M. Ten-Year Single-Center Experience of the Ketogenic Diet: Factors Influencing Efficacy, Tolerability, and Compliance. J. Pediatr. 2015, 166, 1030–1036.e1. [Google Scholar] [CrossRef]
- Simm, P.J.; Bicknell-Royle, J.; Lawrie, J.; Nation, J.; Draffin, K.; Stewart, K.G.; Cameron, F.J.; Scheffer, I.E.; Mackay, M.T. The effect of the ketogenic diet on the developing skeleton. Epilepsy Res. 2017, 136, 62–66. [Google Scholar] [CrossRef]
- Guzel, O.; Uysal, U.; Arslan, N. Efficacy and tolerability of olive oil-based ketogenic diet in children with drug-resistant epilepsy: A single center experience from Turkey. Eur. J. Paediatr. Neurol. 2019, 23, 143–151. [Google Scholar] [CrossRef] [Green Version]
- Hassan, A.M.; Keene, D.L.; Whiting, S.; Jacob, P.J.; Champagne, J.R.; Humphreys, P. Ketogenic diet in the treatment of refractory epilepsy in childhood. Pediatr. Neurol. 1999, 21, 548–552. [Google Scholar] [CrossRef]
- Takeoka, M.; Riviello, J.J.; Pfeifer, H.; Thiele, E.A. Concomitant treatment with topiramate and ketogenic diet in pediatric epilepsy. Epilepsia 2002, 43, 1072–1075. [Google Scholar] [CrossRef] [Green Version]
- Kossoff, E.H.; Pyzik, P.L.; Furth, S.L.; Hladky, H.D.; Freeman, J.M.; Vining, E.P.G. Kidney Stones, Carbonic Anhydrase Inhibitors, and the Ketogenic Diet. Epilepsia 2002, 43, 1168–1171. [Google Scholar] [CrossRef] [PubMed]
- Kossoff, E.H.; Pyzik, P.L.; McGrogan, J.R.; Rubenstein, J.E. The impact of early versus late anticonvulsant reduction after ketogenic diet initiation. Epilepsy Behav. 2004, 5, 499–502. [Google Scholar] [CrossRef] [PubMed]
- Kossoff, E.H.; Pyzik, P.L.; McGrogan, J.R.; Vining, E.P.G.; Freeman, J.M. Efficacy of the Ketogenic Diet for Infantile Spasms. Pediatrics 2002, 109, 780–783. [Google Scholar] [CrossRef] [PubMed]
- Kang, H.-C.; Kim, H.D. Diet therapy in refractory pediatric epilepsy: Increased efficacy and tolerability. Epileptic Disord. 2006, 8, 309–316. [Google Scholar] [PubMed]
- Mackay, M.T.; Nation, J.; Humphrey, M.; Harvey, A.S.; Bicknell-Royle, J. The ketogenic diet in refractory childhood epilepsy. J. Paediatr. Child Health 2005, 41, 353–357. [Google Scholar] [CrossRef]
- Groesbeck, D.K.; Bluml, R.M.; Kossoff, E.H. Long-term use of the ketogenic diet in the treatment of epilepsy. Dev. Med. Child Neurol. 2006, 48, 978–981. [Google Scholar] [CrossRef] [PubMed]
- Sampath, A.; Kossoff, E.H.; Furth, S.L.; Pyzik, P.L.; Vining, E.P.G. Kidney Stones and the Ketogenic Diet: Risk Factors and Prevention. J. Child Neurol. 2007, 22, 375–378. [Google Scholar] [CrossRef]
- Raimann, T.X.; Marín, B.V.; Burón, K.V.; Devilat, B.M.; Ugalde, F.A. Ketogenic diet in refractory epilepsy: Efficacy, evolution and long-term complications. Rev. Chil. Pediatr. 2007, 78, 477–481. [Google Scholar]
- Caraballo, R.; Vaccarezza, M.; Cersósimo, R.; Rios, V.; Soraru, A.; Arroyo, H.; Agosta, G.; Escobal, N.; Demartini, M.; Maxit, C.; et al. Long-term follow-up of the ketogenic diet for refractory epilepsy: Multicenter Argentinean experience in 216 pediatric patients. Seizure 2011, 20, 640–645. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dressler, A.; Trimmel-Schwahofer, P.; Reithofer, E.; Gröppel, G.; Mühlebner, A.; Samueli, S.; Grabner, V.; Abraham, K.; Benninger, F.; Feucht, M. The ketogenic diet in infants—Advantages of early use. Epilepsy Res. 2015, 116, 53–58. [Google Scholar] [CrossRef] [PubMed]
- Hallböök, T.; Sjölander, A.; Åmark, P.; Miranda, M.; Bjurulf, B.; Dahlin, M. Effectiveness of the ketogenic diet used to treat resistant childhood epilepsy in Scandinavia. Eur. J. Paediatr. Neurol. 2015, 19, 29–36. [Google Scholar] [CrossRef] [PubMed]
- Khoo, T.B.; Tukimin, S.M.B.; Syed Zainal Abidin, S.M.B.; Lai, J.J.; Yusoof, N.A.B. Long-term outcome and tolerability of ketogenic diet treatment for refractory epilepsies in children—A tertiary centre Malaysian experience. Neurol. Asia 2016, 21, 17–21. [Google Scholar]
- Lim, Z.; Wong, K.; Olson, H.E.; Bergin, A.M.; Downs, J.; Leonard, H. Use of the ketogenic diet to manage refractory epilepsy in CDKL5 disorder: Experience of >100 patients. Epilepsia 2017, 58, 1415–1422. [Google Scholar] [CrossRef] [Green Version]
- McNally, M.A.; Pyzik, P.L.; Rubenstein, J.E.; Hamdy, R.F.; Kossoff, E.H. Empiric use of potassium citrate reduces kidney-stone incidence with the ketogenic diet. Pediatrics 2009, 124, e300–e304. [Google Scholar] [CrossRef] [Green Version]
- Park, E.G.; Lee, J.; Lee, J. The ketogenic diet for super-refractory status epilepticus patients in intensive care units. Brain Dev. 2019, 41, 420–427. [Google Scholar] [CrossRef]
- Draaisma, J.M.; Hampsink, B.M.; Janssen, M.; Van Houdt, N.B.; Linders, E.T.; Willemsen, M.A. The Ketogenic Diet and Its Effect on Bone Mineral Density: A Retrospective Observational Cohort Study. Neuropediatrics 2019, 50, 353–358. [Google Scholar] [CrossRef] [Green Version]
- Roehl, K.; Falco-Walter, J.; Ouyang, B.; Balabanov, A. Modified ketogenic diets in adults with refractory epilepsy: Efficacious improvements in seizure frequency, seizure severity, and quality of life. Epilepsy Behav. 2019, 93, 113–118. [Google Scholar] [CrossRef]
- Lambrechts, D.A.J.E.; De Kinderen, R.J.A.; Vles, J.S.H.; De Louw, A.J.A.; Aldenkamp, A.P.; Majoie, M. A randomized controlled trial of the ketogenic diet in refractory childhood epilepsy. Acta Neurol. Scand. 2016, 135, 231–239. [Google Scholar] [CrossRef] [Green Version]
- Curhan, G.C. Epidemiology of Stone Disease. Urol. Clin. N. Am. 2007, 34, 287–293. [Google Scholar] [CrossRef] [Green Version]
- Bushinsky, D.A.; Coe, F.L.; Moe, O.W. Nephrolithiasis. Brenner Rector’s Kidney 2012, 9, 1455–1507. [Google Scholar] [CrossRef]
- Dunn-Geier, J.; Ho, H.H.; Auersperg, E.; Doyle, D.; Eaves, L.; Orrbine, E.; Whiting, S. Effect of secretin on children with autism: A randomized controlled trial. Dev. Med. Child Neurol. 2007, 42, 796–802. [Google Scholar] [CrossRef]
- Chow, K.; Dixon, J.; Gilpin, S.; Kavanagh, J.P.; Rao, P.N. Citrate inhibits growth of residual fragments in an in vitro model of calcium oxalate renal stones. Kidney Int. 2004, 65, 1724–1730. [Google Scholar] [CrossRef] [Green Version]
- Rudman, D.; Kunter, M.H.; Redd, S.C.; Waters, W.C.; Gerron, G.G.; Bleier, J. Hypocitraturia in Calcium Nephrolithiasis. J. Clin. Endocrinol. Metab. 1982, 55, 1052–1057. [Google Scholar] [CrossRef]
- Pak, C.Y. Etiology and Treatment of Urolithiasis. Am. J. Kidney Dis. 1991, 18, 624–637. [Google Scholar] [CrossRef]
- Pak, C.Y.; Poindexter, J.R.; Adams-Huet, B.; Pearle, M.S. Predictive value of kidney stone composition in the detection of metabolic abnormalities. Am. J. Med. 2003, 115, 26–32. [Google Scholar] [CrossRef]
- Curhan, G.; Taylor, E. 24-h uric acid excretion and the risk of kidney stones. Kidney Int. 2008, 73, 489–496. [Google Scholar] [CrossRef] [Green Version]
- Ngo, T.C.; Assimos, D.G. Uric Acid Nephrolithiasis: Recent Progress and Future Directions. Rev. Urol. 2007, 9, 17–27. [Google Scholar]
- Okamoto, N.; Aruga, S.; Matsuzaki, S.; Takahashi, S.; Matsushita, K.; Kitamura, T. Associations between renal sodium-citrate cotransporter (hNaDC-1) gene polymorphism and urinary citrate excretion in recurrent renal calcium stone formers and normal controls. Int. J. Urol. 2007, 14, 344–349. [Google Scholar] [CrossRef]
- Nicar, M.J.; Skurla, C.; Sakhaee, K.; Pak, C.Y. Low urinary citrate excretion in nephrolithiasis. Urology 1983, 21, 8–14. [Google Scholar] [CrossRef]
- Siener, R.; Hesse, A. The effect of a vegetarian and different omnivorous diets on urinary risk factors for uric acid stone formation. Eur. J. Nutr. 2003, 42, 332–337. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, N.; Arkilo, D.; Farooq, O.; Gillogly, C.; Kavak, K.S.; Weinstock, A. Ketogenic diet: Predictors of seizure control. SAGE Open Med. 2017, 5. [Google Scholar] [CrossRef]
- Wirrell, E.C.; Darwish, H.Z.; Williams-Dyjur, C.; Blackman, M.; Lange, V. Is a Fast Necessary When Initiating the Ketogenic Diet? J. Child Neurol. 2002, 17, 179–182. [Google Scholar] [CrossRef] [PubMed]
- Zupec-Kania, B.A.; Spellman, E. An Overview of the Ketogenic Diet for Pediatric Epilepsy. Nutr. Clin. Pract. 2008, 23, 589–596. [Google Scholar] [CrossRef] [PubMed]
- DeVivo, D.C.; Haymond, M.W.; Leckie, M.P.; Bussmann, Y.L.; McDougal, J.D.B.; Pagliara, A.S. The Clinical and Biochemical Implications of Pyruvate Carboxylase Deficiency. J. Clin. Endocrinol. Metab. 1977, 45, 1281–1296. [Google Scholar] [CrossRef]
- Rendina, D.; De Filippo, G.; Iannuzzo, G.; Abate, V.; Strazzullo, P.; Falchetti, A. Idiopathic Osteoporosis and Nephrolithiasis: Two Sides of the Same Coin? Int. J. Mol. Sci. 2020, 21, 8183. [Google Scholar] [CrossRef]
- Merlotti, D.; Cosso, R.; Eller-Vainicher, C.; Vescini, F.; Chiodini, I.; Gennari, L.; Falchetti, A. Energy Metabolism and Ketogenic Diets: What about the Skeletal Health? A Narrative Review and a Prospective Vision for Planning Clinical Trials on This Issue. Int. J. Mol. Sci. 2021, 22, 435. [Google Scholar] [CrossRef]
- Aronica, L.; Volek, J.; Poff, A.; D’Agostino, D.P. Genetic variants for personalised management of very low carbohydrate ketogenic diets. BMJ Nutr. Prev. Health 2020, 3, 363–373. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Reference | Description of Ketogenic Diet | Total Number of Patients on Ketogenic Diet | Mean Age of Included Patients | Mean Duration of KGD | No. of Patients with Kidney Stones | % of Patients with Kidney Stones | 24 h Urine Study |
|---|---|---|---|---|---|---|---|
| Holler A. et al. [36] | Classical KD (16), Modified Atkins diet (MAD) (14) | 31 | Median 5.5, mean 5.5 (0.1–15.7 Y) | N/A | 0 | 0 | Hypercalciuria in 12/22 |
| Rener et al. [37] | 2.5:1 to 45/3/20201 | 15 | <3 Y | Average 13 M (4–16 M) | 1 | 6.60% | N/A |
| Attar H. et al. [38] | Modified Atkins diet | 13 | 23–72 Y | Range 1–21 M | 1 | 7.69% | N/A |
| Felix et al. [39] | Modified Atkins diet | 5 | 6–12 Y | 4 M | 0 | 0 | 1 had hypercalciuria |
| Lapp et al. [40] | KGD in 7 and Modified Atkins diet in 19 | 26 | >18 Y | N/A | 4 | 15% | N/A |
| Nerurkar et al. [41] | KGD | 17 | <3 Y | N/A | 1 | 5.88% | N/A |
| Nangia et al. [42] | KGD | 59 | 4.5 Y (range 0.2–22 Y) | Mean 2 Y (range 0–5.5 Y) | 3 | 5% | N/A |
| Gainza et al. [43] | KGD | 41 | 4.7 Y (range 1–13 Y) | Mean 5.79 Y (3–10.6) | 3 | 7.10% | Hypercalciuria in 11 (26.2%) |
| Mak et al. [44] | KGD (MCT oil diet) | 13 | 7.3 Y | N/A | 1 | 7.70% | Increase Ca/Cr ratio in 1 patient |
| Furth et al. [45] | N/A | 112 | 5 Y | N/A | 6 | 5.30% | Elevated Ca/Cr ratio |
| Rios et al. [46] | 4:1 (1.5:1–4.5:1) KGD | 22 | Range 1–19 Y (min age 18 M) | 25 M (1–54 M) | 2 | 9.09% | N/A |
| Sharma et al. [47] | 3:1 KGD in <18 M, 4:1 KGD in >18 M | 23 | (range 6 M–5 Y) | N/A | 1 | 3.70% | Elevated Ca/Cr ratio |
| Kang et al. [48] | 3:1 KGD | 40 | Median ± IQR- 15 ± 13.0 (range 6–60 M) | N/A | 2 | 5.00% | N/A |
| Wibisono et al. [49] | Classic KGD, MCT diet, Modified Atkins diet | 48 | 3.8 Y (range 2.3–7 Y) | Range 1–14 Y | 2 | 4.00% | N/A |
| Simm et al. [50] | 4:1 to 2:1 KGD | 29 | 6.4 Y (range 3.3–17.8 Y) | Mean 2.1 Y (range 0.5–6.5 Y) | 1 | N/A | N/A |
| Guzel et al. [51] | Olive oil-based KGD | 389 | Median 4.0 (2–7)Y | 12 M | 12 | 3% | N/A |
| Hassan et al. [52] | Classic 4:1 KGD (49 of 52 pts), rest with modified diet supplemented by MCT oil | 52 | 5 Y, 6 M ± 3 Y, 4 M | N/A | 1 | 1.90% | Increased calcium oxide in urine |
| Takeoka et al. [53] | 3:1 to 4.1 KGD + Topiramate | 14 | Mean age 4.7 Y | N/A | 0 | 0% | N/A |
| Kossoff et al. [54] | KGD (older children on 4:1 diet and younger on 3:1) without carbonic anhydrase inhibitors | 221 | 5.1 Y (SD 4.5, range 16.5 Y) | N/A | 15 | 6.70% | N/A |
| Kossoff et al. [55] | KGD (older children on 4:1 diet and younger on 3:1) with topiramate or zonisamide | 80 | 4.8 Y (SD 2.4, range 6.5 Y) | N/A | 5 | 6.30% | N/A |
| Kossoff et al. [56] | 4:1 KGD in 9, 3.5:1 in 1 and 3:1 in 13 | 23 | 1.1 Y (range 0.5–24 M) | N/A | 2 | 8.60% | N/A |
| Kang et al. [57] | 4:1 KGD | 129 | 64.9 (±59.3) M | 12.0 (±10.1) M | 4 | 3.10% | N/A |
| Mackay et al. [58] | N/A | 26 | Median age 6.1 Y (range 2.3–13.2) | N/A | 0 | 0% | Increased urine calcium in 8% |
| Groesbeck et al. [59] | 4:1 KGD in 19, 3:1 KGD in 9 | 28 | 3 Y 9 M (range 6 M–13 Y 6 M) | 7 Y 9 M | 7 | 25% | Increase Ca Cr ratio in 14 pts |
| Sampath et al. [60] | 3:1 (56%) or 4:1 KGD | 195 | Median 3 Y (0.5–15 Y) | Median 12 M (range 1–72 M) | 13 | 7% | N/A |
| Raimann et al. [61] | 4:1 in 16, 3.5:1 in 3 and 3:1 in 2 + Calcium and MV supplement | 21 | 6.2 Y (range 6 M–17 Y) | 15 pt completed 1 Y of KGD 2.6 Y (1–6.3 Y) | 2 | 10% | Hypercalciuria in both stone formers |
| Caraballo et al. [62] | N/A | 140 | 5 Y (range 1–18 Y | 3.5 Y (range 1–20 Y) | 6 | 4.28% | N/A |
| Dressler et al. [63] | 4:1 in 36, 3:1 in 53, 3.5:1 in 6, 2.5:1 in 17, 2:1 in 3 | 115 | 2.86 ± 3.1 (min 0.0–max 16.8) | N/A | 4 | 3.40% | N/A |
| Hallbook et al. [64] | N/A | 290 | 5.3 (0.6–18.6) | 2 Y | 7 | N/A | N/A |
| Khoo et al. [65] | 4:1 in 12, 3:1 in 11, 2:1 in 3, MAD in 4 | 30 | 6.8 Y (8 M to 17 Y) | 8 M (range 7 days to 6 Y) | 4 | 13% | N/A |
| Lim et al. [66] | N/A | 204 | 4.8 Y (range 0.3–33.9 Y) | Median 17 M (95% CI 9–24 M) | 2 | 0.98% | N/A |
| McNally et al. [67] | 3:1 or 4;1 KGD | 195 (KGD + hypercalciuria so polycitra K given) | 4.3 Y in reactive group | 15.6 (13.1) | 13 | 6.70% | N/A |
| Park et al. [68] | N/A | 16 | Age range (0.1–40 Y) | N/A | 1 | 6.25% | N/A |
| Draaisma et al. [69] | Classic KGD (67.6%), MCT diet (2.9%), MAD (19.1%) or LGIT (7.4%), other (1.5%) | 68 | 5.7 ± 4.3 Y | 25.6 ± 24.8 M | 6 | 8.80% | N/A |
| Roehhl et al. [70] | Modified KGD | 55 | Mean 38 Y (range 17–70 Y) | N/A | 0 | 0% | N/A |
| Lambrechts et al. [71] | MCT diet and Classic KGD | 26 | 7 Y | 0 | 0 | N/A | N/A |
| Author | Different Types of Ketogenic Diet | Side Effects/Complication of Ketogenic Diet besides Renal Stones |
|---|---|---|
| Holler A. et al. [36] | Classical KGD and MAD | Constipation, increased bromine level (3.2%) |
| Rener et al. [37] | KGD 2.5:1 to 4:1 | Vomiting |
| Attar H. et al. [38] | MAD | NR |
| Felix et al. [39] | MAD | Weight loss, hyperlipidemia |
| Lapp et al. [40] | KGD, MAD | Gallstones (3.8%), hyperlipidemia (3.8%) |
| Nerurkar et al. [41] | KGD not specified | Constipation (57%) |
| Nangia et al. [42] | KGD 3:1 to 4:1 | Constipation (39%), acidosis (21%), nausea/emesis (14%), increased seizures (7%). |
| Gainza et al. [43] | KGD not specified | Osteopenia (38.1%), severe metabolic acidosis (9.5%), recurrent pneumonia (21.4%), neutropenia (0.5%), fatty liver (0.1%), easy bruising (4.8%) |
| Mak et al. [44] | KGD—Protein + carb (<19%) of caloric requirements MCT 60–70% of caloric requirements | Weight loss (46%), diarrhea (38%), bad temper (7.6%), abdominal cramps (15%), nausea (15%), bad body smell (7.6%) |
| Furth et al. [45] | NR | |
| Rios et al. [46] | KGD 4:1 (1.5:1 to 4.5:1) | Nausea and vomiting (26.3%), hypercholesterolemia (64.7%), anorexia (31.8%), constipation (40.9%), symptomatic acidosis (9.09%), carnitine deficiency (9.09%) |
| Sharma et al. [47] | Classical KGD 3:1 or 4:1 | Vomiting (75%), asymptomatic hypocalcemia, Constipation (75%), weight loss, hypoalbuminemia |
| Kang et al. [48] | Classical KGD 4:1 | Dehydration, GI discomfort, hyperlipidemia, hyperuricemia, symptomatic hypoglycemia, lipoid aspiration pneumonia, hypoproteinemia, hypomagnesemia, repeated hyponatremia |
| Wibisono et al. [49] | Classical KGD, MCT, MAD | Constipation, hypertriglyceridemia, hypercholesterolemia, diarrhea, lethargy, iron deficiency, GERD, vomiting, hypoglycemia |
| Simm et al. [50] | KGD 2:1 to 4:1 | Osteopenia, fracture |
| Guzel et al. [51] | KGD 2.5:1 and 4:1 | Hyperlipidemia (50.8%), selenium deficiency (26.9%), constipation (26.2%), sleep disturbances (20%), hyperuricemia (3%), hepatic effects (2.6%), hypoproteinemia (2.6%), hypoglycemia(1.5%) |
| Hassan et al. [52] | Classic 4:1 KGD or MCT diet | Constipation (85%), gall bladder stone (1.9%), hyponatremia (1.9%) |
| Takeoka et al. [53] | KGD not specified | Nausea/vomiting (7%), irritability (7%), lethargy (21%), sedation (14%) |
| Kossoff et al. [54] | KGD 3:1 to 4:1 | NR |
| Kossoff et al. [55] | KGD 3:1 to 4:1 | Sedation (27%), rash, irritability |
| Kossoff et al. [56] | KGD 3:1 to 4:1 | Severe GERD (13%), hip dislocation (0.4%) |
| Kang et al. [57] | Dehydration, GI discomfort, hyperlipidemia, hyperuricemia, hypoglycemia | |
| Mackay et al. [58] | Classical KGD 3:1 to 4.2:1 | Asymptomatic hypoglycemia (24%), poor linear growth (20%), hyperlipidemia (16%), vomiting (12%), hypocarnitinemia (8%), hypercalciuria (8%), constipation (8%), osteopenia (4%), pancreatitis (4%), Diarrhea (4%) |
| Groesbeck et al. [59] | 60.7% on classical KDT 7% MAD, 32% other KGD | Fractures (21.4%), hyperlipidemia (7%), constipation (53%) |
| Sampath et al. [60] | KGD 3:1 (56%) or 4:1 | NR |
| Raimann et al. [61] | KGD 4:1 (3 pts 3.5:1 2 pts 3:1) | Hypercholesterolemia 64% (at 12 months) 15% (at 18 months), growth retardation |
| Caraballo et al. [62] | KGD | GI side effects (30.5%), hyperlipidemia (9.7%), weight gain (2.3%), hypocarnitinemia (3.7%), hypercalciuria (6.9%), hypoglycemia (5.5%), dehydration (6.4%) |
| Dressler et al. [63] | KGD 3:1, 4:1 or 2.5:1 | Carnitine deficiency (13%), growth deficit (5.2%), weight gain (1.7%), hypertriglyceridemia (29.5%), hypercholesterolemia (10.4%) |
| Hallbook et al. [64] | KGD 3:1 or 4:1 ratio | Hyperlipidemia (6%), bone fractures (0.9%) |
| Khoo et al. [65] | Classical KGD (81.2%), MAD (18.75%) | Constipation (43%), hunger (23%), excessive weight gain or loss (20%), vomiting (10%), hyperuricemia (30%), hypocalcemia (20%) |
| Lim et al. [66] | NR | GI side effects (nausea, vomiting, and constipation), Inadequate weight gain or significant weight loss, ketoacidosis, hepatotoxicity, renal dysfunction, sinus tachycardia, osteoporosis |
| McNally et al. [67] | KGD unspecified | NR |
| Park et al. [68] | KGD 4:1 (87.5%), KGD 3:1 (12.5%) | Regurgitation, constipation, aspiration, hypertriglyceridemia, hypoproteinemia, nausea, vomiting |
| Draaisma et al. [69] | Classic KGD (67.6%), MCT diet (2.9%) MAD (19.1%), LGID (7.4%), others (1.5%) | Decrease in BMD 0.22 Z-score/year |
| Roehhl et al. [70] | Modified ketogenic diet 15 gm carb vs. 50 gm carb diet | Constipation (9%) |
| Lambrechts et al. [71] | KGD | GI side effects (30%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Acharya, P.; Acharya, C.; Thongprayoon, C.; Hansrivijit, P.; Kanduri, S.R.; Kovvuru, K.; Medaura, J.; Vaitla, P.; Garcia Anton, D.F.; Mekraksakit, P.; et al. Incidence and Characteristics of Kidney Stones in Patients on Ketogenic Diet: A Systematic Review and Meta-Analysis. Diseases 2021, 9, 39. https://0-doi-org.brum.beds.ac.uk/10.3390/diseases9020039
Acharya P, Acharya C, Thongprayoon C, Hansrivijit P, Kanduri SR, Kovvuru K, Medaura J, Vaitla P, Garcia Anton DF, Mekraksakit P, et al. Incidence and Characteristics of Kidney Stones in Patients on Ketogenic Diet: A Systematic Review and Meta-Analysis. Diseases. 2021; 9(2):39. https://0-doi-org.brum.beds.ac.uk/10.3390/diseases9020039
Chicago/Turabian StyleAcharya, Prakrati, Chirag Acharya, Charat Thongprayoon, Panupong Hansrivijit, Swetha R. Kanduri, Karthik Kovvuru, Juan Medaura, Pradeep Vaitla, Desiree F. Garcia Anton, Poemlarp Mekraksakit, and et al. 2021. "Incidence and Characteristics of Kidney Stones in Patients on Ketogenic Diet: A Systematic Review and Meta-Analysis" Diseases 9, no. 2: 39. https://0-doi-org.brum.beds.ac.uk/10.3390/diseases9020039