
Short- and Long-Term Effects of Rehabilitation after Perimesencephalic Subarachnoid Hemorrhage

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Diagnostic Work-Up and SF-36 Questionnaire
2.2. Trial Registration
2.3. Rehabilitation
3. Results
3.1. Patient Collective
3.2. Short-Term Outcome after 6 Months
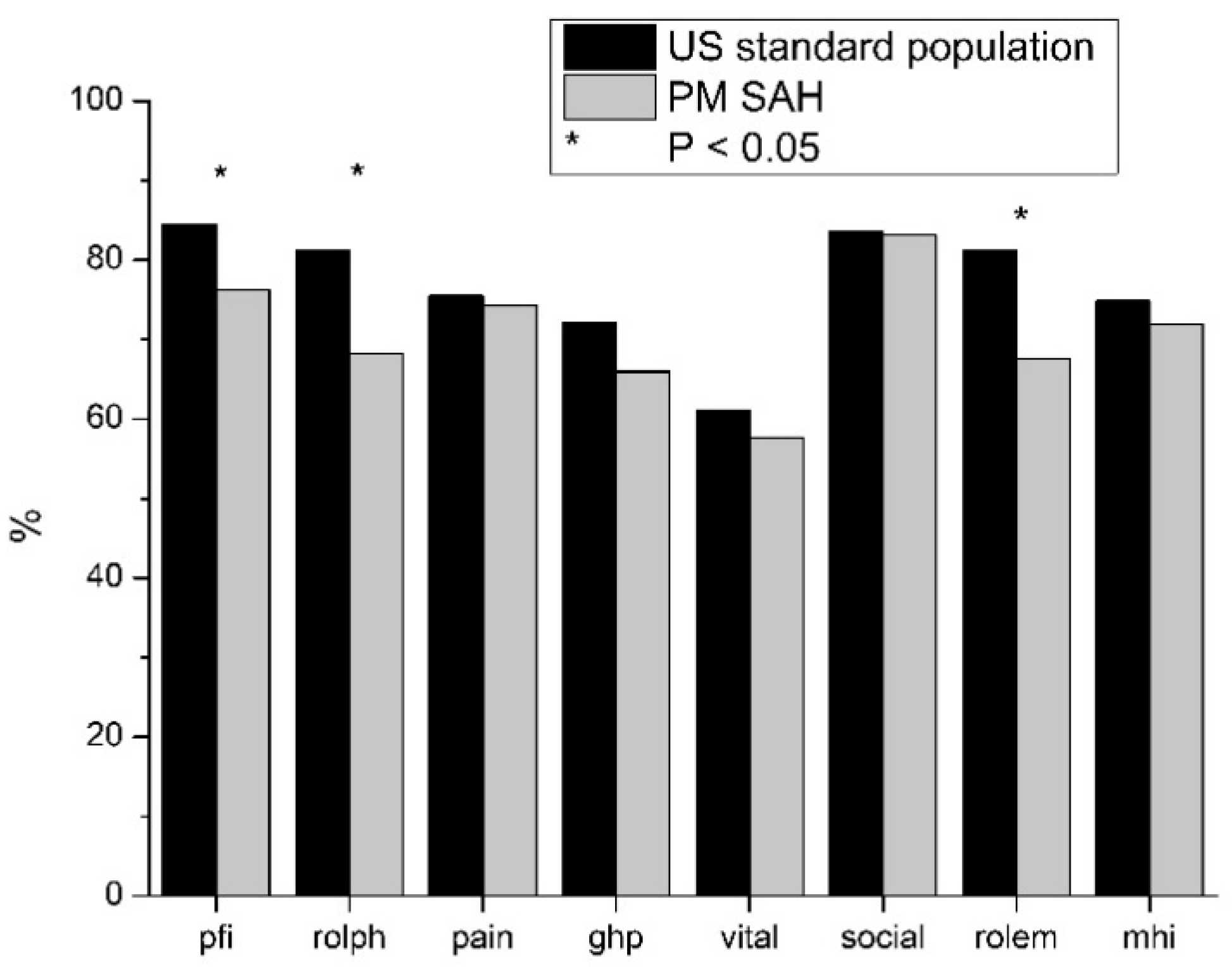
3.3. Long-Term Outcome of PM SAH and Comparison with Standard Population
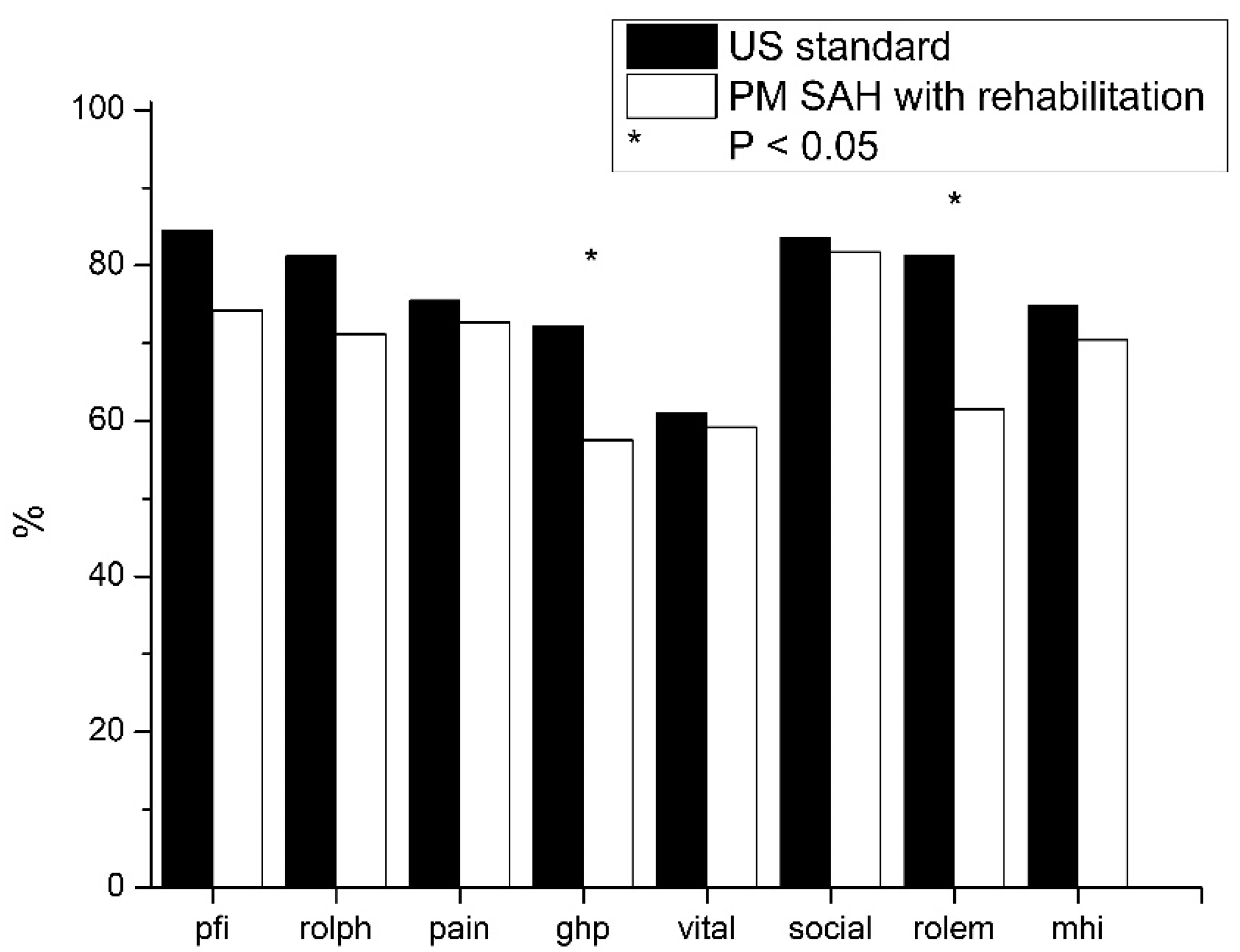
3.4. Long-Term Outcome of PM SAH Patients with Subsequent Rehabilitation
4. Discussion
4.1. Outcome at Discharge until 6 Months Short-Term Follow-Up
4.2. PM SAH at Long-Term Follow-Up
4.3. Limitations and Generalizability
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
Disclosure Statement
References
- Lucke-Wold, B.P.; Logsdon, A.F.; Manoranjan, B.; Turner, R.C.; McConnell, E.; Vates, G.E.; Huber, J.D.; Rosen, C.L.; Simard, J.M. Aneurysmal Subarachnoid Hemorrhage and Neuroinflammation: A Comprehensive Review. Int. J. Mol. Sci. 2016, 17, 497. [Google Scholar] [CrossRef] [PubMed]
- Konczalla, J.; Kashefiolasl, S.; Brawanski, N.; Senft, C.; Seifert, V.; Platz, J. Increasing numbers of nonaneurysmal subarachnoid hemorrhage in the last 15 years: Antithrombotic medication as reason and prognostic factor? J. Neurosurg. 2016, 124, 1731–1737. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- The European Registers of Stroke (EROS) Investigators. Incidence of Stroke in Europe at the Beginning of the 21st Century. Stroke 2009, 40, 1557–1563. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Gijn, J.; Rinkel, G.J.E. Subarachnoid haemorrhage: Diagnosis, causes and management. Brain 2001, 124, 249–278. [Google Scholar] [CrossRef] [PubMed]
- Konczalla, J.; Kashefiolasl, S.; Brawanski, N.; Lescher, S.; Senft, C.; Platz, J.; Seifert, V. Cerebral vasospasm and delayed cerebral infarctions in 225 patients with non-aneurysmal subarachnoid hemorrhage: The underestimated risk of Fisher 3 blood distribution. J. NeuroInterv. Surg. 2016, 8, 1247–1252. [Google Scholar] [CrossRef] [PubMed]
- Konczalla, J.; Schuss, P.; Platz, J.; Vatter, H.; Seifert, V.; Güresir, E. Clinical outcome and prognostic factors of patients with angiogram-negative and non-perimesencephalic subarachnoid hemorrhage: Benign prognosis like perimesencephalic SAH or same risk as aneurysmal SAH? Neurosurg. Rev. 2014, 38, 121–127. [Google Scholar] [CrossRef] [PubMed]
- Fisher, C.M.; Kistler, J.P.; Davis, J.M. Relation of Cerebral Vasospasm to Subarachnoid Hemorrhage Visualized by Computerized Tomographic Scanning. Neurosurgery 1980, 6, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Beseoglu, K.; Pannes, S.; Steiger, H.J.; Hänggi, D. Long-term outcome and quality of life after nonaneurysmal subarachnoid hemorrhage. Acta Neurochir. 2009, 152, 409–416. [Google Scholar] [CrossRef] [PubMed]
- Konczalla, J.; Schmitz, J.; Kashefiolasl, S.; Senft, C.; Platz, J.; Seifert, V. Non-aneurysmal non-perimesencephalic subarachnoid Hemorrhage: Effect of rehabilitation at short-term and in a prospective study of long-term follow-up. Top. Stroke Rehab. 2016, 23, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Konczalla, J.; Schmitz, J.; Kashefiolasl, S.; Senft, C.; Seifert, V.; Platz, J. Non-aneurysmal subarachnoid hemorrhage in 173 patients: A prospective study of long-term outcome. Eur. J. Neurol. 2015, 22, 1329–1336. [Google Scholar] [CrossRef] [PubMed]
- Kashefiolasl, S.; Brawanski, N.; Platz, J.; Bruder, M.; Senft, C.; Marquardt, G.; Seifert, V.; Tritt, S.; Konczalla, J. MRI-detection rate and incidence of lumbar bleeding sources in 190 patients with non-aneurysmal SAH. PLoS ONE 2017, 12, e0174734. [Google Scholar] [CrossRef] [PubMed]
- Steiner, T.; Juvela, S.; Unterberg, A.; Jung, C.; Forsting, M.; Rinkel, G. European Stroke Organization Guidelines for the Management of Intracranial Aneurysms and Subarachnoid Haemorrhage. Cerebrovasc. Dis. 2013, 35, 93–112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rinkel, G.J.; Wijdicks, E.F.; Vermeulen, M.; Ramos, L.M.; Tanghe, H.L.; Hasan, D.; Meiners, L.C.; van Gijn, J. Nonaneurysmal perimesencephalic subarachnoid hemorrhage: CT and MR patterns that differ from aneurysmal rupture. Am. J. Neuroradiol. 1991, 12, 829–834. [Google Scholar] [PubMed]
- Rankin, J. Cerebral Vascular Accidents in Patients over the Age of 60: II. Prognosis. Scott. Med. J. 1957, 2, 200–215. [Google Scholar] [CrossRef] [PubMed]
- Ware, J.E.; Kosinski, M.; Keller, S.D. SF-36 Physical and Mental Health Summary Scales: A User’s Manual; Health Institute, New England Medical Center: Boston, MA, USA, 1994. [Google Scholar]
- Ware, J.E.; Gandek, B.; Kosinki, M.; Aaronson, N.K.; Apolone, G.; Brazier, J.; Bullinger, M.; Kaasa, S.; Leplege, A.; Priesto, L.; et al. The equivalence of SF-36 summa-ry health scores estimated using standard and coun-try-specific algorithms in 10 countries: Results from the IQOLA project. J. Clin. Epidemiol. 1998, 51, 1167–1170. [Google Scholar] [CrossRef]
- Ildan, F.; Tuna, M.; Erman, T.; Göçer, A.I.; Çetinalp, E. Prognosis and prognostic factors in nonaneurysmal perimesencephalic hemorrhage: A follow-up study in 29 patients. Surg. Neurol. 2002, 57, 160–165. [Google Scholar] [CrossRef]
- Konczalla, J.; Platz, J.; Schuss, P.; Vatter, H.; Seifert, V.; Güresir, E. Non-aneurysmal non-traumatic subarachnoid hemorrhage: Patient characteristics, clinical outcome and prognostic factors based on a single-center experience in 125 patients. BMC Neurol. 2014, 14, 140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kielbergerová, L.; Mayer, O.; Vaněk, J.; Bruthans, J.; Wohlfahrt, P.; Cífková, R. Quality of Life Predictors in Chronic Stable Post-Stroke Patients and Prognostic Value of SF-36 Score as a Mortality Surrogate. Transl. Stroke Res. 2015, 6, 375–383. [Google Scholar] [CrossRef] [PubMed]
- Viswanathan, V.; Lucke-Wold, B.; Jones, C.; Aiello, G.; Li, Y.; Ayala, A.; Fox, W.C.; Maciel, C.B.; Busl, K.M. Change in opioid and analgesic use for headaches after aneurysmal subarachnoid hemorrhage over time. Neurochirurigie 2021, 67, 427–432. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Item | Abbreviation | |
|---|---|---|
| Pyhsical | Physical functioning | pfi |
| Role limitations due to physical health problems | rolph | |
| Physical pain | pain | |
| General health problems | ghp | |
| Psychological | Vitality | vital |
| Social functioning | social | |
| Role limitations due to emotional problems | rolem | |
| General mental health | mhi |
| Characteristics | All PM SAH | Without Subsequent Rehabilitation | With Subsequent Rehabilitation | p (with vs. without Rehabilitation) |
|---|---|---|---|---|
| No. of patients | 37 (100%) | 24 (65%) | 13 (35%) | NS |
| mean age ± SD | 55.1 ± 9.6 | 53.7 ± 10.8 | 57.8 ± 6.2 | NS |
| Outcome at discharge (mean mRS ± SD) | 1.56 ± 0.64 | 1.36 ± 0.74 | 1.7 ± 0.5 | NS |
| short-term outcome (mean mRS ± SD) | 0.6 ± 0.59 | 0.54 ± 0.59 | 0.8 ± 0.6 | NS |
| Improvement from discharge to short-term outcome (6 months) | 0.69 | 0.82 | 0.9 | NS |
| p (mRS discharge vs. mRS 6 months FU) | NS | NS | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schmitz, J.; Kashefiolasl, S.; Brawanski, N.; Dinc, N.; Gessler, F.; Senft, C.; Tritt, S.; Seifert, V.; Konczalla, J. Short- and Long-Term Effects of Rehabilitation after Perimesencephalic Subarachnoid Hemorrhage. Diseases 2021, 9, 69. https://0-doi-org.brum.beds.ac.uk/10.3390/diseases9040069
Schmitz J, Kashefiolasl S, Brawanski N, Dinc N, Gessler F, Senft C, Tritt S, Seifert V, Konczalla J. Short- and Long-Term Effects of Rehabilitation after Perimesencephalic Subarachnoid Hemorrhage. Diseases. 2021; 9(4):69. https://0-doi-org.brum.beds.ac.uk/10.3390/diseases9040069
Chicago/Turabian StyleSchmitz, Jens, Sepide Kashefiolasl, Nina Brawanski, Nazife Dinc, Florian Gessler, Christian Senft, Stephanie Tritt, Volker Seifert, and Jürgen Konczalla. 2021. "Short- and Long-Term Effects of Rehabilitation after Perimesencephalic Subarachnoid Hemorrhage" Diseases 9, no. 4: 69. https://0-doi-org.brum.beds.ac.uk/10.3390/diseases9040069