Vaginal Administration of Contraceptives
by
 , , , and
, , , and
Esmat Jalalvandi
1,*, 
Hafez Jafari
2,
Christiani A. Amorim
3,
Denise Freitas Siqueira Petri
4,
Lei Nie
5,* and
and
Amin Shavandi
2,* 1
School of Engineering and Physical Sciences, Heriot-Watt University, Edinburgh EH14 4AS, UK
2
BioMatter Unit, École Polytechnique de Bruxelles, Université Libre de Bruxelles, Avenue F.D. Roosevelt, 50-CP 165/61, 1050 Brussels, Belgium
3
Pôle de Recherche en Gynécologie, Institut de Recherche Expérimentale et Clinique, Université Catholique de Louvain, 1200 Brussels, Belgium
4
Fundamental Chemistry Department, Institute of Chemistry, University of São Paulo, Av. Prof. Lineu Prestes 748, São Paulo 05508-000, Brazil
5
College of Life Sciences, Xinyang Normal University, Xinyang 464000, China
*
Authors to whom correspondence should be addressed.
Sci. Pharm. 2021, 89(1), 3; https://0-doi-org.brum.beds.ac.uk/10.3390/scipharm89010003
Submission received: 18 October 2020
/
Revised: 13 December 2020
/
Accepted: 15 December 2020
/
Published: 25 December 2020
Abstract
:While contraceptive drugs have enabled many people to decide when they want to have a baby, more than 100 million unintended pregnancies each year in the world may indicate the contraceptive requirement of many people has not been well addressed yet. The vagina is a well-established and practical route for the delivery of various pharmacological molecules, including contraceptives. This review aims to present an overview of different contraceptive methods focusing on the vaginal route of delivery for contraceptives, including current developments, discussing the potentials and limitations of the modern methods, designs, and how well each method performs for delivering the contraceptives and preventing pregnancy.
1. Introduction
Every year, approximately 213 million pregnancies occur, and as many as 99 million of these pregnancies are not intended [1]. Several contraceptives methods and strategies have been conducted to address unplanned pregnancies, as well as to minimize the side effects and to solve the possible important health problem. However, there are still some limitations, such as high cost and the need for professional skill for the placement of long-acting reversible contraceptives (LARC) [2]. In the case of oral administration, there is also the risk of side effects from high dosage estrogen and progestogen [3].
A great deal of research also has been done on identifying new contraceptive delivery systems to increase effectiveness by improving user compliance [4]. However, poor user adherence to pill regimens is responsible for the considerable difference between thenumber of women experiencing an unplanned pregnancy within the first year of use of oral contraceptives with perfect use (0.3%) and typical use (8%) [5].
Unlike the oral route, the vaginal counterpart avoids the gastrointestinal and hepatic first-pass effect. It lacks cell layers with metabolic enzymes, so drugs can directly reach the systemic circulation, and therefore lower doses are necessary, which in turn decreases the incidence of side effects. Moreover, due to continuous and stable drug release, this route improves patient compliance. Due to the presence of a dense network of blood vessels, the ability to bypass first-pass metabolism and a high permeability for drugs (especially low molecular weight drugs), the vaginal route is a convenient route for drug delivery [6,7].
Vaginal contraceptives, such as gels and rings, are also discreet and reversible. It can be part of a multipurpose prevention technology approach when combined with drugs for sexually transmitted disease (STD) prophylaxis [8]. Indeed, multipurpose prevention technology through the vaginal route has been thought to be a promising strategy to address reproductive and sexual health needs and can, therefore, be particularly beneficial for users and the health system [9].
This review aims to discuss available contraceptives as well as the ongoing research on the design of novel vaginal contraceptive systems.
2. Contraceptives
The contraceptive method is a product or medical procedure that inhibits reproduction from acts of sexual intercourse [10]. Access to safe and effective contraception is essential for supporting individual and public health and promotes the autonomy of women worldwide. Women can choose from a vast plethora of contraceptives based on convenience, cost, esthetic considerations, intercourse periodicity, method efficiency rate, ease of use, etc. Cultural and religious considerations can also influence a woman’s choice. When choosing a contraceptive method, women and their health care providers must consider the risks and benefits of the available options [11]. Currently, various non-vaginal contraceptive options are available, which will be discussed briefly in the following sections. Herein, the focus is on the local delivery of contraceptives to the vagina.
Non-Vaginal Contraceptives
Non-vaginal contraceptives include a wide range of methods, such as barrier and oral contraceptives, contraceptive patches and injections, implants, and intrauterine devices. Barrier contraceptives, including the diaphragm, cervical cap, sponge, female, and male condoms, are the earliest contraceptives aim to inhibit fertilization by blocking sperm and egg interaction (physically or chemically) [12].
Barrier contraceptives are well known, easy to use, and have about 80% success rate in preventing pregnancy when used correctly [13], and if used with a spermicide, they could be up to 96% effective [14]. In addition to their contraceptive efficacy, these methods have been investigated for their effectiveness in disease prevention (e.g., STDs) [15]. However, it is important to stress that an initial clinical examination is required for a diaphragm fitting and, one needs to master the correct insertion and removal technique for the best results. While rare, the use of a sponge and diaphragm has been reported to increase the risk of toxic shock syndrome, risk of urinary tract infections (UTIs), and latex allergy [16].
Oral administration is the most common form of contraceptives used by more than 140 million women worldwide [14,15]. Combined oral contraceptives comprise estrogen and progestin, which inhibit ovulation and change the cervical mucus that prevents sperm penetration.
All combined oral contraceptives are taken daily, and this may cause hormonal fluctuations and, consequently, poor compliance. Various side effects have been reported because of using oral contraceptives, including headache, nausea, breast tenderness, vaginal dryness, loss of libido, weight gain, irritability, and depression [17,18]. Some studies reported that the use of combined oral contraceptives is associated with an increased risk of breast cancer due to the carcinogenic nature of estrogen-progesterone contraceptives [19], cervical cancer [20], venous thromboembolism [21], and HIV [22,23]. Hence, due to the adverse effect of combined oral contraceptives, there is an immense need to focus on herbal analogs of these contraceptives, which can provide safe and effective contraception.
The combined hormonal transdermal contraceptive patch development goes back to the early 1990s. In 2002, Ortho EvraTM was approved by the FDA as the first contraceptive patch [24]. The patch releases norelgestromin (6 mg) and ethinyl estradiol (0.75 mg) to the systemic circulation in a week [25]. Contraceptive patches are more effective compared to non-hormonal barriers; their advantages are the ease of use and their low-cost. However, some serious side effects such as venous thromboembolism (VTE) due to the high levels of estrogen (>30 μg), lack of protection against sexually transmitted infections (STIs), and in some cases, skin irritation can limit contraceptive patch applications [21].
Furthermore, unlike the contraceptive patches, contraceptive injections and implants provide the possibility of birth control based on progestin only. A long-acting contraceptive is an injectable method, preventing pregnancy for 8–13 weeks by releasing progestin into the bloodstream. Depo-Provera®, Syana® Press (medroxyprogesterone acetate), and Noristerat® (norethisterone enanthate) are the most common contraceptive injections given in the UK. Common side effects of using injections include headache, cycle disturbance, amenorrhea, irregular bleeding, weight gain, and abdominal pain, as well as the disability to protect women against STDs [26,27]. Moreover, the long-term contraception effect (up to one year) is not suitable for women planning for pregnancy soon. Hence, there is an immense need to address the side effects and limitations of conventional contraception methods.
3. The Vaginal Route Delivery
Until the 1920s, the vagina was considered a site for the delivery of locally acting drugs only. However, this organ proved to be of great importance for systemic drug delivery, uterine targeting, or even vaccination [28,29] due to its large surface area, a dense network of blood vessels, and permeability to a wide range of compounds [30]. Topical delivery to the vaginal mucosa has many significant applications for preventing human immunodeficiency virus (HIV) and other STDs, mucosal vaccines, treatment of various sexually transmitted infections (STIs), and maintenance of reproductive health. Several drug classes have been administered through the vaginal mucosa, such as antimicrobials, labor inducers, spermicides, and sexual hormones [31,32]. Compared to the intestinal counterpart, vaginal mucosa permeability is higher with some substances such as water, 17-β-estradiol, arecoline, and arecaidine [33]. The permeation mechanism to most substances is simple diffusion, where the intracellular route preferentially absorbs hydrophobic substances. In contrast, hydrophilic drugs are preferentially absorbed by pores present in the vaginal mucosa by paracellular diffusion mechanism, with higher absorbability for low molecular weight lipophilic drugs compared to larger molecules or even hydrophilic drugs [34,35].
Nowadays, vaginal administration of different pharmacologically active molecules is a common practice, with a specific interest in managing local genital conditions, like infection, neoplastic lesions, or vaginal atrophy, or with contraceptive and labor-inducing/prevention purposes [36].
The vaginal route of administration has several advantages over conventional drug delivery methods, such as the ability to bypass hepatic first-passage, avoidance of gastrointestinal side effects, and reduction in hepatic side effects of steroids used in hormone replacement therapy or contraception [37,38]. Moreover, the vaginal route overcomes the inconvenience caused by pain, damage to the tissue, and possible infection by other parenteral routes. In addition, self-insertion and removal of the dosage form are possible [39]. Moreover, the vagina has a relatively high permeability to a wide range of molecular weight drugs that contributes to its pharmacokinetic advantages [40]. Nevertheless, the complexity of the vagina may limit the design and use of vaginal delivery formulations. It is also important to consider cyclic variations, cultural sensitivity, local irritation, and the influence of sexual intercourse [39].
From a drug delivery viewpoint, the vagina is a continually changing environment. It is a complex organ with multiple functions and physicochemical, physiological, histological, and anatomical parameters that change with age, menstrual cycle, pregnancy, and sexual arousal, all of which play a role in the efficiency and potential duration of vaginal contraceptive delivery [39]. In addition, the self-cleansing action of the vaginal tract will affect therapeutic outcome [41]. For example, several vaginal formulations (tablets, creams, gels, pessaries, and foams) have limited efficacy due to their lesser residence time on vaginal epithelium due to the self-cleansing action of the vagina. Mucoadhesive polymers such as polystyrene sulfonate, polycarbophil, hydroxypropyl cellulose, poly (acrylic acid), poly(ethylene glycol)-based block copolymers, and chitosan extend the contact with vaginal mucosa [42,43,44,45,46].
Furthermore, the vagina has natural biomechanical forces and fluid dynamics, which lead to a physiological removal mechanism that results in the limited absorption of drugs. The utilization of mucoadhesive formulations can prolong the permanence of the drug in the vaginal mucosa [38]. Therefore, the design of any vaginal drug delivery system must consider the anatomy and physiology of the vagina.
Vaginal Anatomy and Physiology
The human vagina is an S-shaped fibromuscular collapsed canal that extends from the lower part of the uterine cervix to the outer part of the vulva known as the labia minor. In adult women, it presents approximately 7–10 cm in length, more than 4 cm in width, and 150–200 μm in thickness [35]. The vagina lies at a 90° angle to the uterus and is held in place by endopelvic fascia and ligaments. The vaginal tube is composed of four different areas, which are related to the cervix: an anterior and two laterals shallow fornices and an ample posterior fornix. The anterior and posterior walls of the vagina join together to form two ridges of folds creating an H-shape appearance in cross-section [47].
Histologically, the vaginal wall is composed of three layers: tunica adventitia, muscular, and mucosa. The adventitia layer covers the muscular coat; its composition rich in collagen and elastic fibers contributes to the elasticity of the vagina. The muscular layer comprises smooth and elastic fibers in a spiral arrangement, which gives an incredible elasticity to this organ. The mucosa layer is divided into three sublayers (epithelium, lamina propria, and submucosa) and, due to changes in hormone level, its thickness changes at different stages of the menstrual cycle by about 200–300 μm. Hence, the menstrual cycle may influence drug absorption through the vaginal mucosa. It forms a series of transverse folds at the surface area of the vagina called “rugae”. This provides the vagina with a relatively large surface area [47]. While the vaginal epithelium is usually considered a mucosal surface, there are no glands in the vaginal mucosa, and it lacks the direct release of mucin. The vagina’s secretion is a mixture of cervical mucus, transudate from the vaginal mucosa, desquamated cellular debris, and leukocytes [48]. This mucus coating has several important physiological functions, playing an essential role in drug absorption or action. Throughout the menstrual cycle, viscoelastic properties, and the rate of production of vaginal mucus will change. During ovulation, cervical mucus is less viscoelastic, resulting in higher permeability of molecules [39].
The vagina’s pH with healthy, lactobacilli-dominated microbiota is acidic between about 3.5–4.0 [49]. This pH value is sustained by lactobacilli that convert glycogen from exfoliated epithelial cells into lactic acid. The vaginal tube has a pH gradient where the pH is lowest nearest the cervix. The pH changes with age, stages of the menstrual cycle, infections, and sexual arousal. For example, menstrual blood, cervical, and uterine secretions, yeast infection, and semen introduction to the vagina will act as alkaline agents and increase the vaginal pH [48,50] verm. The change in pH will affect the ionization and absorption of certain drugs, as well as the release profile of pH-sensitive drugs. Indeed, at normal vaginal pH, most weak bases drugs can be found in their ionized form due to their pKa value (8.5–10.5), while weak acids are mostly in un-ionized form because of their low pKa < 5.5. However, altering the pH of the vagina due to certain illnesses such as bacterial vaginosis and yeast infections, and even stress [51] can change the drug absorption profile [52]. Therefore, the basic physiology of the vagina must be considered when designing vaginal dosage formulations [53].
4. Vaginal Contraceptives
The vaginal route can be an optimal alternative for delivering hormonal contraceptives. It has lower drug interactions compared to the gastrointestinal tract, and so a lower dose of contraceptives is required to increase the bioavailability [55,56]. Additionally, compared to oral contraceptives, controlled-release products, such as vaginal rings, would increase effectiveness by improving user compliance.
4.1. Vaginal Rings
The contraceptive vaginal ring is an effective contraception with a low dose of hormones, self-administration, and high stability of drug diffusion. It does not require skilled providers and frequent high dosing than other common contraceptive methods [17,57].
Initial development of vaginal rings dates back to more than 50 years ago based on two known facts: the capacity of vaginal epithelium to absorb steroids and the capacity of elastomers to provide a sustained release of these hormones [58]. Distinct from oral contraceptives that require daily dosage, vaginal rings release a continuous dose of estrogen and progesterone into the bloodstream to inhibit ovulation. They are, therefore, more efficient and convenient. For this reason, several studies showed a high acceptance of the vaginal ring, and participants also highlighted how easy it is to use this contraceptive option [59,60,61]. The typical commercially available vaginal rings are shown in Table 1.
Various ring prototypes have been evaluated: progestin-only rings and combined progestin-estrogen rings, as well as different combinations of progestins and estrogens [62]. The most common vaginal ring, Nuvaring® (MSD, Oss, The Netherlands), is made of ethylene-vinyl acetate copolymer and magnesium stearate and releases both ethinyl estradiol and etonogestrel. Another common vaginal ring is Progering (Silesia; Santiago, Chile). Nuvaring releases both ethinyl estradiol and etonogestrel for one month, while Progering releases progesterone for three months and the ring should be removed and replaced after this period. Nuvaring and Progering are considered expensive products with low availability in low-income and middle-income countries. Indeed, high cost, short-term effectiveness, as well as storage condition (+4 °C) hindered their worldwide acceptability [63].
A recent FDA approved vaginal ring offers more prolonged protection against pregnancy [66]. AnnoveraTM is a reusable vaginal ring based on segesterone acetate/ethinyl estradiol combined hormonal contraceptives and can be used for one year of birth control [66]. Annovera is an opaque white ring made of silicone elastomer with a dimension of 56 mm in outside diameter and 8.4 mm in cross-sectional diameter containing two steroid-releasing channels. High effectiveness (97.5%) and patient acceptability (89% patient satisfaction) have been reported for the AnnoveraTM by Kaplan–Meier analysis [73]. A phase 3 clinical trial, including 2265 participants, showed that only 1.8% of the participants experienced unacceptable bleeding over the course of a year, which led to discontinuation of the Annovera ring [74].
Ornibel® (Exeltis, Madrid, Spain) is another recent contraceptive ring with the same size and external appearance as Nuvaring® (54 mm in outside diameter and 4 mm in cross-sectional diameter).
Ornibel® is made of a different polymeric composition, polyurethane core, and ethylene-vinyl acetate membrane containing 28% vinyl acetate, which allows the ring to show a gradual release of the hormone on the first day of use, particularly for ethinylestradiol. Moreover, there is no special storage condition needed for this ring [67].
Recently, a newly developed vaginal ring containing segesterone acetate and ethinyl estradiol with the sustainable daily release of 150 μg segesterone acetate and 15 μg ethinyl estradiol (for a year) has received FDA approval. The authors investigated the factors associated with non-adherence to instructions for using the contraceptive ring. The clinical trial (phase 3) demonstrated that two critical factors related to the non-adherence to instructions for using the ring are removing the ring for washing and for intercourse, which should be considered for the design of a contraceptive ring [75].
The development of vaginal rings releasing ulipristal acetate (UPA), which is a selective progesterone receptor modulator, has attracted a great deal of interest. The contraceptive effect of UPA is due to its ability to selectively bind to human PRs [76]. Currently, UPA is approved for use as an emergency contraception uterine leiomyoma treatment. Although a clinical trial with 39 women exhibited a high efficacy (two-thirds of the cycles) of UPA in ovulation inhabitation, the design of a vaginal ring with different dosages of UPA should be investigated to enhance its effectiveness as a promising contraceptive [77].
Recently, the development of vaginal rings as a multipurpose technology is growing fast due to the opportunity of addressing multiple sexual and reproductive health problems. Moreover, in addition to the contraception effect, vaginal rings can have anti-HIV activity by releasing microbicides [78]. It has been reported that a monthly vaginal ring releasing dapivirine could decrease the risk of HIV-1 infection higher adherence [79].
However, similar to oral contraceptives, the vaginal ring containing 20 μg ethinyl estradiol and 1 mg norethindrone acetate may cause transient nausea [80]. While vaginal rings can better control a woman’s cycles, some adverse effects may lead to higher discontinuation rates than combined oral contraceptives [81]. Indeed, studies reported some common side effects, such as headache, vaginitis, weight increase, vaginal discomfort, and acne [5], as well as rare reactions like vein thrombosis and strabismus [82,83].
4.2. Vaginal Spermicides as Non-Hormonal Contraceptives
Hormonal contraceptives and copper-based IUDs come with a series of side effects, and they do not offer any protection against STDs. Therefore, safe, effective, and convenient topical formulations with both microbicide and spermicidal activity are a global need to control the human population and spread STDs [84,85].
Spermicides are chemical agents that can be found in the format of gels, foam, film, or suppositories that immobilize the spermatozoa and can exert the contraceptive effect in the female genital tract by disrupting normal sperm activity by causing irreversible cell damage or death. An effective spermicidal agent must act rapidly to prevent the penetration of spermatozoa into the endocervical canal of the uterus and show a good cervical mucus bio diffusion [86]. It must be non-irritating and non-hostile to vaginal flora and penile mucosa, which must not have any adverse effect on the developing embryo or fetus and should also be less-toxic [87]. An ideal spermicide should preferably be free of detergent and surfactant molecules. Although many detergents have shown substantial microbicidal properties [88], some studies have suggested that detergent spermicides do not protect against STDs, including HIV [89,90]. Indeed, spermicides nonoxynol-9 (N-9) do not have a protective effect against HIV infection; besides, they can increase the risk of HIV transmission if used frequently. This may be due to the surfactant nature of these chemicals that irritate the epithelium membrane of the vagina and causes damage by repeated use, making the vagina more susceptible to STD infections. Stability and activity duration of spermicides, as well as their tissue reactivity, should be considered for the design of epidermal devices [91]. Based on their mode of action, spermicides are categorized as described below.
4.2.1. Bactericides/Surfactant
Membrane integrity and its composition are the fundamental characteristics of the sperm membrane. Changes in the fatty acid composition of membranes and the number of integral proteins account for the shift in fluidity that affects sperm’s function [92]. Bactericides often interact with components in the sperm membrane and immobilize the cell. For example, benzalkonium chloride (a cationic surfactant) and sodium docusate (an anionic detergent) is used as a vaginal spermicide [93]. Piperazine dicarboxamidine derivatives, quaternary ammonium chlorides, and octyl-phenoxy poly ethoxy ethanol are good bactericides with germicidal and spermicidal effects [87,94,95]. Many surfactant agents, such as nonoxynol-9 (N-9), can interact with the lipotropic membrane of spermatozoa. N-9 is a non-ionic spermicide approved by FDA and is the most commonly used spermicidal contraceptive in the UK and USA [14,96]. N-9 is the active ingredient of many contraceptive formulations, including foams, gels, creams, suppositories, and sponges [97]. In a study by Lee et al. [98], a mucoadhesive drug delivery system, gel, was developed using carbopol 934P for controlled delivery of N-9, while in another study, incorporation of N-9 into a silicon-based vaginal ring was proposed to investigate the potential use of this intravaginal ring to prevent STDs [99].
Although the primary function of N-9 is to prevent pregnancy, it is an effective barrier against STDs, including gonorrhea, chlamydia1 infection candidiasis, syphilis, genital herpes, trichomoniasis, and the acquired immunodeficiency syndrome [100,101,102]. However, because of the strong surfactant action of N-9, it often disrupts the vaginal mucosa [103] and targets other cells in the vagina, such as the cervicovaginal epithelia that are essential for maintaining a natural barrier to pathogen invasion, especially HIV [104,105]. Thus, N-9 causes an acute tissue inflammatory response, increasing the risk of STDs such as HIV [106,107].
Amphora, which was previously known as Acidform, is another spermicide with FDA approval as a vaginal lubricant that immobilizes and kills sperms by maintaining the acidity of the vagina (pH < 5, for hours) without any disadvantages. Moreover, the high adhesiveness of amphora to vaginal walls and the cervix paves the way for decreasing leakage, which results in preserving its activity for hours. It has been reported that amphora could be a promising alternative to N-9 as a contraceptive [108].
Another recent bactericide that has been investigated as a potential contraceptive is B07, a small molecule CCR5 antagonist-based HIV-1 entry inhibitor, which is used as an anti-HIV microbicide. A recent study demonstrated that B07 could exhibit a concentration- and time-dependent inhibitory effect against sperm motility and movement patterns tested on female rabbits. Although a slight irritation was reported for the B07, sound spermicidal effects against human sperm, and its anti-HIV properties make this bactericide a promising candidate for further investigation as a vaginal spermicide/microbicide [109].
G1-S4 or G2-S16 are another class of microbicides with anti-HIV-1 and HSV-2 activity where their potential contraceptive activity has been investigated. A study reported that a promising contraceptive from the combination of G1-S4 or G2-S16 platycodin D, which induced 100% immobilization of the sperm in 30 s without showing any toxicity and vaginal epithelium damage after 7 consecutive days (in vivo, mice) [110].
Other common detergent-type vaginal spermicide includes p-menthanyl-phenyl-polyoxyethylene (8,8) ether, or menfegol, which is available in a foaming tablet formulation and isooctyl-phenyl-polyoxyethylene-(9) ether, or octoxynol-9, which was removed from the US market due to failure in providing new studies required by FDA [111].
4.2.2. Sulfhydryl Binding Agents
Anaerobic energy metabolism, spermatozoa motility, and defense against reactive oxygen species, which are essential to the survival of both sperm and anaerobic microbes, such as Trichomonas vaginalis in the host, depending on the availability of free thiols. Thus, sulfhydryl binding agents (oxidants) are an option for the design of dual-purpose sperm immobilizing agents [112,113]. These agents interact with accessible thiols on sperm and T. vaginalis, resulting in lipid peroxidation, insufficient axonemal phosphorylations, and, consequently, loss of motility and viability. Sulfhydryl binding agents exert their damaging effect by oxidation, alkylation, or formation of mercaptides on the sperm membrane [92]. Mammalian spermatozoa, with a high content of polyunsaturated fatty acids in their membrane as well as low concentrations of scavenging enzymes in their cytoplasm, are particularly prone to oxidation damage [114]. Hydrogen peroxide, O-iodobenzoate, and hydroquinone are known to destroy the tertiary protein structure by converting the thiol group of cysteine to disulfide linkages. Phenyl mercuric acid is another mercaptide forming agent [87,115]. Thirty thiourea derivatives were synthesized in a study carried out by D’Cruz et al. In their chemical structures, one of the nitrogen atoms of the thiourea was attached either to a phenyl, heterocyclic or alicyclic moiety through an ethyl bridge and the other nitrogen atom was attached to a substituted pyridyl ring [116]. They reported that phenyl and cyclohexanyl-substituted thiourea derivatives show anti-HIV and spermicidal activities [116]. In another study by Dwivedi et al., various products of disulfide esters of dialkylaminocarbothioic acid were synthesized, and some exhibited active spermicidal effect [117].
4.2.3. Natural Products and Their Derivatives
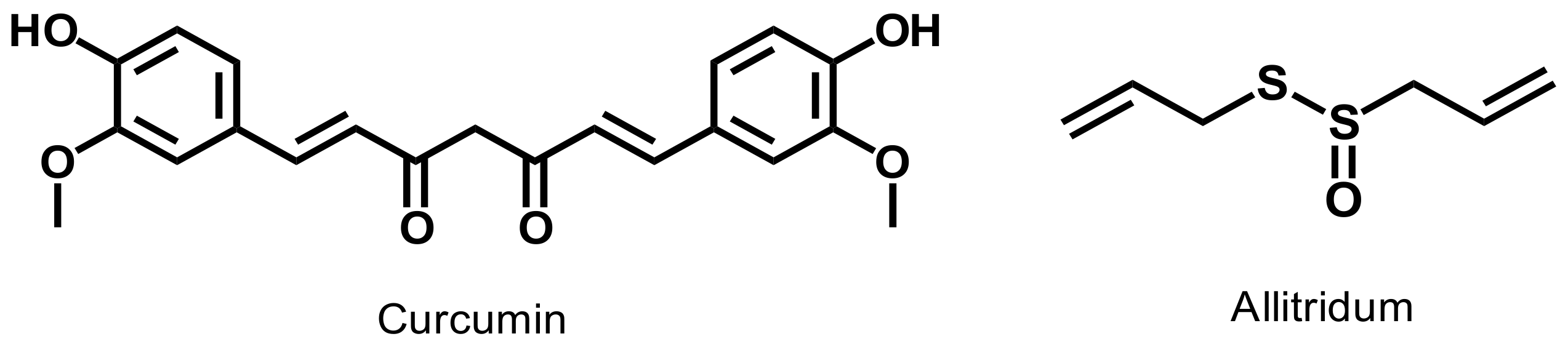
The spermicidal efficacy of many natural substances has been evaluated to develop new vaginal spermicides. For example, curcumin, a plant-derived diferuloylmethane compound, offers sperm-immobilizing effect, as well as anti-HIV property [118]. Allitridum, an active compound in garlic, was studied as an inhibitor to sperm mobility in vitro [119]. This study showed an evident spermicide effect of allitridum at the 7.5 mg/mL concentration. Various alkaloids, such as quinine, showed an inhibitory effect on spermatozoa cells, which was dose dependent. Figure 2 shows the chemical structures of curcumin and allitridum. Immotilin, a protein isolated from an earthworm, rapidly immobilizes and kills human spermatozoa without disturbing other cells [120]. Nisin, a cationic peptide, is produced by a group of Gram-positive bacteria that belongs to Lactococcus and Streptococcus species [121]. Nisin is known for its spermicidal and antibacterial activities [122]. Intravaginal administration of Nisin (200 μg) resulted in complete inhibition of sperm motility and, subsequently, fertilization prevention. The repetitive intravaginal application of Nisin at the dose of 200 μg for 14 continuous days did not cause any abnormalities in vaginal epithelial cells in rats. In addition, no histopathological irregularities in vaginal tissue or any change in blood and serum biochemical profiles were observed [88,122,123]. In addition to these natural products, microorganisms are also known to delay sperm motility either by agglutination or by secretion of extracellular substances. For instance, Staphylococcus aureus showed a spermicidal effect. In one study, Staphylococcus aureus was encapsulated in a carbopol based vaginal gel. The gel released about 80% of Staphylococcus aureus within 30 min that could completely restrain human spermatozoa within the 20 s, at a dose of 200 μg/mL [124]. It appears that Staphylococcus aureus contains a sperm-agglutinating factor that attaches to specific receptors on human spermatozoa and changes the morphology of spermatozoa, inducing agglutination [125]. Many other natural substances have been reported as a natural spermicide. For example, tartaric acid exhibited the highest spermicide effects among other components such as nonoxynol-9, benzalkonium chloride, and verapamil [85]. Furthermore, another study investigated the spermicide effects of different natural components, such as lemon juice, pineapple juice, and apple juice, in which lemon juice showed higher sperm immobilization exhibited [126]. Moreover, other natural compounds such as bivittoside D [127], saponins [128], tannins [129] have been investigated as spermicidal compounds.
4.2.4. Other Synthetic Products
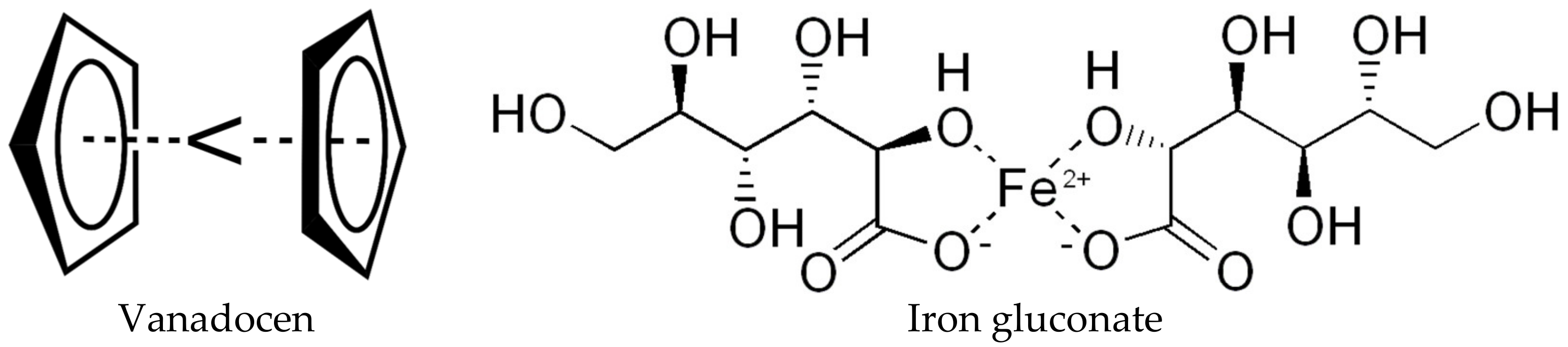
Bis(cyclopentadienyl) complexes of vanadium or vanadocenes (Figure 3) are a new class of contraceptive agents that quickly inhibit the mobility of human sperms [130,131]. The spermicidal activity of vanadocenes was reported to be 400-fold more than that of N-9, and unlike N-9, the sperm-immobilizing activity was not disruptive to the membrane at the ultrastructural level [132]. Vanadium can be found in both anionic and cationic forms with oxidation states from −1 to +5. Vanadium complexes with oxidation states +4 and +5 can catalyze the production of reactive oxygen species. These species can immobilize the spermatozoa at nanomolar to low micromolar concentrations [133,134].
Iron gluconate (Figure 3) is a synthetic reagent immobilizing the sperm tail and inducing lipid peroxidation. Reactive oxygen species produced during this process result in spermatozoa damage [135,136]. High levels of fatty acids present in human sperms make these cells susceptible to the free radical species upon exposure to iron gluconate. This encourages constant formation and decomposition of lipid peroxides and eventually causes structural damage, a decline in metabolic activity, and spermicidal effect [29,137]. Han et al. designed two different vaginal rings composed of acacia gum or non-biodegradable hydrogel of 2-hydroxyethyl methacrylate and sodium methacrylate. These vaginal rings were then infused with iron gluconate and an anti-HIV agent. The release profile of each reagent from each vaginal ring was examined, and the authors concluded that these vaginal rings have the potential application as non-hormonal contraceptive delivery systems [138]. Saxena et al. also investigated the possible use of a biodegradable hydrogel impregnated with iron gluconate as a non-hormonal contraception method [139]. They reported the hydrogel composed of dextran, copolymers of polylactide, and ε-caprolactone releases the iron gluconate over 16 days, and in vivo study on rabbits showed the effect of iron gluconate as an efficient spermicide reagent. Recently, a pH stimuli injectable hydrogel-based chitosan containing iron gluconate and doxorubicin hydrochloride (DOX) exhibited a promising result [29]. The hydrogel showed a fast release of iron gluconate and sustainable and controllable release of DOX from hydrogel due to the presence of pH stimuli bonds through Schiff based reaction with amine groups and aldehyde group [140].
Green et al. reported that enzymatically generated free iodine (I2) is an extremely efficient spermicidal agent [141]. Free I2 also showed microbicidal and virucidal activities at 2-5 ppm concentrations; thus, it can be useful as a dual-purpose contraceptive reagent with no irritating side effects on tissues [142]. In an oxidative environment (rich-reducing environment: vaginal and seminal fluids), alternate species, such as I3¯, or higher oxidation states of iodine such as IO¯, I2O2, and IO3¯, could form during the conversion of iodide into I2. These species could also be responsible for the spermicidal activity. Green et al. suggested encapsulating precursors for I2 formation in a vaginal delivery system (e.g., vaginal insert). The vaginal delivery device would release the precursor, and free I2 will form in situ. The pH of the vagina or semen fluid does not disturb the expression of I2-mediated oxidizing activity because free I2 is an effective oxidizing agent whether in the elemental form at low pH or upon conversion to hypoiodate at the more alkaline environment [141].
Jan et al. introduced a dual-purpose compound as a vaginal contraceptive capable of preventing STDs. The compound 5-bromo-6-methoxy-5,6-dihydro-3′-azidothymidine-5′-(p-bromophenyl methoxyalaninyl phosphate) was synthesized and proved to have an anti-HIV function at a lower concentration compared to N-9. In addition, the spermicidal activity of this novel agent was higher than that of N-9 when upon treatment of spermatozoa with this agent motility, the loss was complete within 30 min [143]. In a similar study, the spermicidal efficacy and potential against HIV of a bromo-methoxy substituted phenyl phosphate derivative of zidovudine were evaluated [144]. Unlike N-9, the spermicidal activity of this compound was not associated with damage to epithelial cells in the vaginal tract, and it exhibited an anti-HIV effect, hence, considered to be a unique active ingredient for vaginal contraceptive formulations [144]. Figure 4 illustrates the structure of these dual-purpose contraceptives.
Many more synthetic and natural compounds are being investigated as new spermicides and anti-STDs reagents. For example, recent extraction of Asiatic acid from Shorea robusta (tree) induced instantaneous immobilization of rat spermatozoa in vitro [145], whereas synthesis of 3,3-bis (5-methoxy-1H-indol-3-yl) indolin-2-one resulted in significant spermicidal activity [146]. All the mentioned spermicides can be exerted in various intravaginal delivery formulations including, jelly, hydrogel, creams, vaginal rings, and implants. Although these vaginal delivery systems containing spermicides may not be as effective as other contraceptive methods (e.g., hormonal contraceptive and copper-based IUD), they are still in the dawn of their development, and some appear to have great potential. It is important to note that currently, using spermicides as the only method of contraception has some weaknesses. Relatively high failure rate and risk of urinary tract infection in women who apply them regularly are some of the drawbacks. Many studies have been carried out on the potential application of spermicide as anti-STDs such as chlamydia, gonorrhea, or HIV. Some of these studies suggest an increased risk of these infections when using some effective spermicides (e.g., detergents such as N-9) since these types of spermicides irritate the vaginal epithelium and cause small tears that allow HIV and other infectious agents to enter [147].
5. Conclusions
Vagina, with a smooth and immobile surface with specific permeability properties, makes it a suitable route for placement and delivery of drugs such as contraceptives in a controlled manner compared to the traditional oral form. The present article provides a review of the several methods of vaginal delivery of contraceptives, which either are currently in the market or are in the design and development stage. We emphasized the challenges and potentials for the delivery of contraceptives through the vagina compared to the conventional route for the contraceptive administrations and summarizing the continuing interests toward the design and the development of new techniques, which are safe and affordable to most women and have no environmental impact. Further investigation of vaginal contraceptive methods with minimizing the side effect is required to fulfill woman’s needs that can be fitted into the real lives of the women who need them. Moreover, regarding the high demand for contraceptives worldwide, cost-effectiveness and availability of a contraceptive product should be considered.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Bearak, J.; Popinchalk, A.; Alkema, L.; Sedgh, G. Global, regional, and subregional trends in unintended pregnancy and its outcomes from 1990 to 2014: Estimates from a Bayesian hierarchical model. Lancet Glob. Health 2018, 6, e380–e389. [Google Scholar] [CrossRef] [Green Version]
- Polis, C.B.; Curtis, K.M.; Hannaford, P.C.; Phillips, S.J.; Chipato, T.; Kiarie, J.N.; Westreich, D.J.; Steyn, P.S. An updated systematic review of epidemiological evidence on hormonal contraceptive methods and HIV acquisition in women. Aids Lond. Engl. 2016, 30, 2665. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cervenka, I.; Mahamat-Saleh, Y.; Savoye, I.; Dartois, L.; Boutron-Ruault, M.; Fournier, A.; Kvaskoff, M. Oral contraceptive use and cutaneous melanoma risk: A French prospective cohort study. Int. J. Cancer 2018, 143, 2390–2399. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sitruk-Ware, R.; Nath, A.; Mishell, D.R., Jr. Contraception technology: Past, present and future. Contraception 2013, 87, 319–330. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gaffield, M.E.; Curtis, K.M.; Mohllajee, A.P.; Peterson, H.B. Medical eligibility criteria for new contraceptive methods: Combined hormonal patch, combined hormonal vaginal ring and the etonogestrel implant. Contraception 2006, 73, 134–144. [Google Scholar] [CrossRef]
- Sharifzadeh, G.; Hezaveh, H.; Muhamad, I.I.; Hashim, S.; Khairuddin, N. Montmorillonite-based polyacrylamide hydrogel rings for controlled vaginal drug delivery. Mater. Sci. Eng. C 2020, 110, 110609. [Google Scholar] [CrossRef]
- Hasanifard, M.; Ebrahimi-Hosseinzadeh, B.; Hatamian-Zarmi, A.; Rezayan, A.; Esmaeili, M. Development of thiolated chitosan nanoparticles based mucoadhesive vaginal drug delivery systems. Polym. Sci. Ser. A 2017, 59, 858–865. [Google Scholar] [CrossRef] [Green Version]
- Griffin, J.B.; Ridgeway, K.; Montgomery, E.; Torjesen, K.; Clark, R.; Peterson, J.; Baggaley, R.; van der Straten, A. Vaginal ring acceptability and related preferences among women in low- and middle-income countries: A systematic review and narrative synthesis. PLoS ONE 2019, 14, e0224898. [Google Scholar] [CrossRef]
- Lusti-Narasimhan, M.; Merialdi, M.; Holt, B. Multipurpose prevention technologies: Maximising positive synergies. Bjog: Int. J. Obstet. Gynaecol. 2014, 121, 251. [Google Scholar] [CrossRef]
- Hubacher, D.; Trussell, J. A definition of modern contraceptive methods. Contraception 2015, 92, 420–421. [Google Scholar] [CrossRef]
- Riley, H.E.M.; Steyn, P.S.; Achilles, S.L.; Bass, E.; Gray, A.L.; Polis, C.B.; Kiarie, J.N. Hormonal contraceptive methods and HIV: Research gaps and programmatic priorities. Contraception 2017, 96, 67–71. [Google Scholar] [CrossRef] [PubMed]
- Claure, I.; Anderson, D.; Klapperich, C.M.; Kuohung, W.; Wong, J.Y. Biomaterials and Contraception: Promises and Pitfalls. Ann. Biomed. Eng. 2020, 48, 2113–2131. [Google Scholar] [CrossRef] [PubMed]
- Narrigan, D. Women’s barrier contraceptive methods: Poised for change. J. Midwifery Women’s Health 2006, 51, 478–485. [Google Scholar] [CrossRef] [PubMed]
- Hassan, E.; Creatsas, G.; Gravanis, A.; Georgoulias, V.; Psychoyos, A. Anti-STD vaginal contraceptive sponges. Ann. N. Y. Acad. Sci. 1997, 816, 451–456. [Google Scholar] [CrossRef] [PubMed]
- Moench, T.R.; Chipato, T.; Padian, N.S. Preventing disease by protecting the cervix: The unexplored promise of internal vaginal barrier devices. Aids Lond. Engl. 2001, 15, 1595–1602. [Google Scholar] [CrossRef] [Green Version]
- Colquitt, C.W.; Martin, T.S. Contraceptive methods: A review of nonbarrier and barrier products. J. Pharm. Pract. 2017, 30, 130–135. [Google Scholar] [CrossRef]
- Caruso, S.; Agnello, C.; Intelisano, G.; Farina, M.; Di Mari, L.; Cianci, A. Sexual behavior of women taking low-dose oral contraceptive containing 15 microg ethinylestradiol/60 microg gestodene. Contraception 2004, 69, 237–240. [Google Scholar] [CrossRef]
- De Castro Coelho, F.; Barros, C. The Potential of Hormonal Contraception to Influence Female Sexuality. Int. J. Reprod. Med. 2019, 2019, 9701384. [Google Scholar] [CrossRef]
- Westhoff, C.L.; Pike, M.C. Hormonal contraception and breast cancer. Contraception 2018, 98, 171–173. [Google Scholar] [CrossRef]
- Smith, J.S.; Green, J.; de Gonzalez, A.B.; Appleby, P.; Peto, J.; Plummer, M.; Franceschi, S.; Beral, V. Cervical cancer and use of hormonal contraceptives: A systematic review. Lancet 2003, 361, 1159–1167. [Google Scholar] [CrossRef]
- Brynhildsen, J. Combined hormonal contraceptives: Prescribing patterns, compliance, and benefits versus risks. Ther. Adv. Drug Saf. 2014, 5, 201–213. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heffron, R.; Donnell, D.; Rees, H.; Celum, C.; Mugo, N.; Were, E.; de Bruyn, G.; Nakku-Joloba, E.; Ngure, K.; Kiarie, J.; et al. Use of hormonal contraceptives and risk of HIV-1 transmission: A prospective cohort study. Lancet Infect. Dis. 2012, 12, 19–26. [Google Scholar] [CrossRef] [Green Version]
- Gierisch, J.M.; Coeytaux, R.R.; Urrutia, R.P.; Havrilesky, L.J.; Moorman, P.G.; Lowery, W.J.; Dinan, M.; McBroom, A.J.; Hasselblad, V.; Sanders, G.D. Oral contraceptive use and risk of breast, cervical, colorectal, and endometrial cancers: A systematic review. Cancer Epidemiol. Prev. Biomark. 2013, 22, 1931–1943. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burkman, R.T. The transdermal contraceptive patch: A new approach to hormonal contraception. Int. J. Fertil. Womens Med. 2002, 47, 69–76. [Google Scholar] [PubMed]
- Feisullin, K.; Westhoff, C. Chapter 33-Contraception. In Principles of Gender-Specific Medicine, 2nd ed.; Legato, M.J., Ed.; Academic Press: San Diego, CA, USA, 2010; pp. 357–365. [Google Scholar]
- Jain, J.; Jakimiuk, A.J.; Bode, F.R.; Ross, D.; Kaunitz, A.M. Contraceptive efficacy and safety of DMPA-SC. Contraception 2004, 70, 269–275. [Google Scholar] [CrossRef] [PubMed]
- Noory, A.; Khabt Aboud, H.; Essam, N.; Rezaq, A. The side effect of noristerat injection in some biochemistry parameters in al-diwaniya city. Pak. J. Biotechnol. 2018, 15, 699–702. [Google Scholar]
- Major, I.; McConville, C. Vaginal drug delivery for the localised treatment of cervical cancer. Drug Deliv. Transl. Res. 2017, 7, 817–828. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jalalvandi, E.; Shavandi, A. In situ-forming and pH-responsive hydrogel based on chitosan for vaginal delivery of therapeutic agents. J. Mater. Sci. Mater. Med. 2018, 29, 158. [Google Scholar] [CrossRef]
- Pathak, Y.V. Surface Modification of Nanoparticles for Targeted Drug Delivery; Springer International Publishing: Cham, Switzerland, 2019. [Google Scholar]
- Mašek, J.; Mašková, E.; Lubasová, D.; Špánek, R.; Raška, M.; Turánek, J. Nanofibers in Mucosal Drug and Vaccine Delivery, Nanomaterials-Toxicity, Human Health and Environment; Clichici, S., Filip, A., do Nascimento, G.M., Eds.; IntechOpen: London, UK, 2018. [Google Scholar]
- Mirza, M.A.; Panda, A.K.; Asif, S.; Verma, D.; Talegaonkar, S.; Manzoor, N.; Khan, A.; Ahmed, F.J.; Dudeja, M.; Iqbal, Z. A vaginal drug delivery model. Drug Deliv. 2016, 23, 3123–3134. [Google Scholar] [CrossRef]
- Van der Bijl, P.; van Eyk, A.D. Comparative in vitro permeability of human vaginal, small intestinal and colonic mucosa. Int. J. Pharm. 2003, 261, 147–152. [Google Scholar] [CrossRef]
- Sassi, A.B.; McCullough, K.D.; Cost, M.R.; Hillier, S.L.; Rohan, L.C. Permeability of tritiated water through human cervical and vaginal tissue. J. Pharm. Sci. 2004, 93, 2009–2016. [Google Scholar] [CrossRef] [PubMed]
- Machado, R.M.; Palmeira-de-Oliveira, A.; Gaspar, C.; Martinez-de-Oliveira, J.; Palmeira-de-Oliveira, R. Studies and methodologies on vaginal drug permeation. Adv. Drug Deliv. Rev. 2015, 92, 14–26. [Google Scholar] [CrossRef] [PubMed]
- Das Neves, J.; Nunes, R.; Machado, A.; Sarmento, B. Polymer-based nanocarriers for vaginal drug delivery. Adv. Drug Deliv. Rev. 2015, 92, 53–70. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leyva-Gómez, G.; Piñón-Segundo, E.; Mendoza-Muñoz, N.; Zambrano-Zaragoza, M.L.; Mendoza-Elvira, S.; Quintanar-Guerrero, D. Approaches in Polymeric Nanoparticles for Vaginal Drug Delivery: A Review of the State of the Art. Int. J. Mol. Sci. 2018, 19, 1549. [Google Scholar] [CrossRef] [Green Version]
- Srikrishna, S.; Cardozo, L. The vagina as a route for drug delivery: A review. Int. Urogynecol. J. 2013, 24, 537–543. [Google Scholar] [CrossRef] [PubMed]
- Jitendra, P.K.; Bansal, S.; Banik, A. Noninvasive routes of proteins and peptides drug delivery. Indian J. Pharm. Sci. 2011, 73, 367–375. [Google Scholar] [CrossRef] [PubMed]
- Acarturk, F. Mucoadhesive vaginal drug delivery systems. Recent Pat. Drug Deliv. Formul. 2009, 3, 193–205. [Google Scholar] [CrossRef]
- Jøraholmen, M.W.; Basnet, P.; Tostrup, M.J.; Moueffaq, S.; Škalko-Basnet, N. Localized Therapy of Vaginal Infections and Inflammation: Liposomes-In-Hydrogel Delivery System for Polyphenols. Pharmaceutics 2019, 11, 53. [Google Scholar] [CrossRef] [Green Version]
- Kataria, K.; Sharma, A.; Garg, T.; Goyal, A.K.; Rath, G. Novel technology to improve drug loading in polymeric nanofibers. Drug Deliv. Lett. 2014, 4, 79–86. [Google Scholar] [CrossRef]
- Johal, H.S.; Garg, T.; Rath, G.; Goyal, A.K. Advanced topical drug delivery system for the management of vaginal candidiasis. Drug Deliv. 2016, 23, 550–563. [Google Scholar] [CrossRef]
- Zou, P.; Suo, J.; Nie, L.; Feng, S. Temperature-responsive biodegradable star-shaped block copolymers for vaginal gels. J. Mater. Chem. 2012, 22, 6316–6326. [Google Scholar] [CrossRef]
- Nie, L.; Zou, P.; Feng, S.; Suo, J. Temperature-sensitive star-shaped block copolymers hydrogels for an injection application: Phase transition behavior and biocompatibility. J. Mater. Sci. Mater. Med. 2013, 24, 689–700. [Google Scholar] [CrossRef] [PubMed]
- Nie, L.; Zou, P.; Dong, J.; Sun, M.; Ding, P.; Han, Y.; Ji, C.; Zhou, Q.; Yuan, H.; Suo, J. Injectable Vaginal Hydrogels as a Multi-Drug Carrier for Contraception. Appl. Sci. 2019, 9, 1638. [Google Scholar] [CrossRef] [Green Version]
- Krogstad, E.A.; Rathbone, M.J.; Woodrow, K.A. Vaginal Drug Delivery in Focal Controlled Drug Delivery; Domb, A.J., Khan, W., Eds.; Springer: New York, NY, USA, 2014; pp. 607–651. [Google Scholar]
- Vermani, K.; Garg, S. The scope and potential of vaginal drug delivery. Pharm. Sci. Technol. Today 2000, 3, 359–364. [Google Scholar] [CrossRef]
- Mirmonsef, P.; Gilbert, D.; Veazey, R.S.; Wang, J.; Kendrick, S.R.; Spear, G.T. A comparison of lower genital tract glycogen and lactic acid levels in women and macaques: Implications for HIV and SIV susceptibility. Aids Res. Hum. Retrovir. 2012, 28, 76–81. [Google Scholar] [CrossRef] [Green Version]
- Nakano, F.Y.; Leão, R.d.B.F.; Esteves, S.C. Insights into the role of cervical mucus and vaginal pH in unexplained infertility. MedicalExpress 2015, 2, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Amabebe, E.; Anumba, D.O. Psychosocial stress, cortisol levels, and maintenance of vaginal health. Front. Endocrinol. 2018, 9, 568. [Google Scholar] [CrossRef]
- Manallack, D.T. The p K a distribution of drugs: Application to drug discovery. Perspect. Med. Chem. 2007, 1, 1177391X0700100003. [Google Scholar] [CrossRef]
- Ensign, L.M.; Cone, R.; Hanes, J. Nanoparticle-based drug delivery to the vagina: A review. J. Control. Release Off. J. Control. Release Soc. 2014, 190, 500–514. [Google Scholar] [CrossRef] [Green Version]
- Jaraquemada, J.M.P.; Mónaco, R.G.; Barbosa, N.E.; Ferle, L.; Iriarte, H.; Conesa, H.A. Lower uterine blood supply: Extrauterine anastomotic system and its application in surgical devascularization techniques. Acta Obstet. Gynecol. Scand. 2007, 86, 228–234. [Google Scholar] [CrossRef]
- Faundes, A.; Brache, V.; Alvarez, F. Pros and cons of vaginal rings for contraceptive hormone delivery. Am. J. Drug Deliv. 2004, 2, 241–250. [Google Scholar] [CrossRef]
- Lopez, L.M.; Grimes, D.A.; Gallo, M.F.; Stockton, L.L.; Schulz, K.F. Skin patch and vaginal ring versus combined oral contraceptives for contraception. Cochrane Database Syst. Rev. 2013. [Google Scholar] [CrossRef] [PubMed]
- Sanders, S.A.; Graham, C.A.; Bass, J.L.; Bancroft, J. A prospective study of the effects of oral contraceptives on sexuality and well-being and their relationship to discontinuation. Contraception 2001, 64, 51–58. [Google Scholar] [CrossRef]
- Brache, V.; Faundes, A. Contraceptive vaginal rings: A review. Contraception 2010, 82, 418–427. [Google Scholar] [CrossRef] [PubMed]
- Novák, A.; de la Loge, C.; Abetz, L.; van der Meulen, E.A. The combined contraceptive vaginal ring, NuvaRing®: An international study of user acceptability. Contraception 2003, 67, 187–194. [Google Scholar] [CrossRef]
- Kestelyn, E.; Van Nuil, J.I.; Umulisa, M.M.; Umutoni, G.; Uwingabire, A.; Mwambarangwe, L.; Uwineza, M.; Agaba, S.; Crucitti, T.; van de Wijgert, J. High acceptability of a contraceptive vaginal ring among women in Kigali, Rwanda. PLoS ONE 2018, 13, e0199096. [Google Scholar] [CrossRef] [Green Version]
- Santibenchakul, S.; Jaisamrarn, U. Acceptability, tolerability, and satisfaction of a contraceptive vaginal ring (the NuvaRing) among Thai women. Asian Biomed. 2017, 10, 235–241. [Google Scholar]
- Brache, V.; Payan, L.J.; Faundes, A. Current status of contraceptive vaginal rings. Contraception 2013, 87, 264–272. [Google Scholar] [CrossRef]
- Temmerman, M. A new woman-controlled contraceptive vaginal ring: A global step forward. Lancet Glob. Health 2019, 7, e986–e987. [Google Scholar] [CrossRef] [Green Version]
- Roumen, F.J. Review of the combined contraceptive vaginal ring, NuvaRing®. Ther. Clin. Risk Manag. 2008, 4, 441. [Google Scholar] [CrossRef] [Green Version]
- Helbling, I.M.; Ibarra, J.C.; Luna, J.A. Evaluation and optimization of progesterone release from intravaginal rings using response surface methodology. J. Drug Deliv. Sci. Technol. 2015, 29, 218–225. [Google Scholar] [CrossRef]
- FDA. FDA Approves New Vaginal Ring for One Year of Birth Control. Available online: https://www.fda.gov/news-events/press-announcements/fda-approves-new-vaginal-ring-one-year-birth-control (accessed on 25 December 2020).
- Algorta, J.; Diaz, M.; de Benito, R.; Lefebvre, M.; Sicard, E.; Furtado, M.; Regidor, P.A.; Ronchi, C. Pharmacokinetic bioequivalence, safety and acceptability of Ornibel®, a new polymer composition contraceptive vaginal ring (etonogestrel/ethinylestradiol 11.00/3.474 mg) compared with Nuvaring®(etonogestrel/ethinylestradiol 11.7/2.7 mg). Eur. J. Contracept. Reprod Health Care 2017, 22, 429–438. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Santen, R. Vaginal administration of estradiol: Effects of dose, preparation and timing on plasma estradiol levels. Climacteric 2015, 18, 121–134. [Google Scholar] [CrossRef] [PubMed]
- Fraser, I.S.; Tiitinen, A.; Affandi, B.; Brache, V.; Croxatto, H.B.; Diaz, S.; Ginsburg, J.; Gu, S.; Holma, P.; Johansson, E.; et al. Norplant® Consensus Statement and Background Review 22The Consensus Statement follows the end of Appendix B. Contraception 1998, 57, 1–9. [Google Scholar] [CrossRef]
- Croxatt, H.B. Progestin implants for female contraception. Contraception 2002, 65, 15–19. [Google Scholar] [CrossRef]
- Coutinho, E.M. One year contraception with a single subdermal implant containing nomegestrol acetate (Uniplant). Contraception 1993, 47, 97–105. [Google Scholar] [CrossRef]
- Ernst, D. FDA Approves New Contraceptive Patch; Haymarket Media, Inc.: London, UK, 2020. [Google Scholar]
- Merkatz, R.B.; Plagianos, M.; Hoskin, E.; Cooney, M.; Hewett, P.C.; Mensch, B.S. Acceptability of the nestorone®/ethinyl estradiol contraceptive vaginal ring: Development of a model; implications for introduction. Contraception 2014, 90, 514–521. [Google Scholar] [CrossRef] [Green Version]
- Micks, E.A.; Jensen, J.T. A technology evaluation of Annovera: A segesterone acetate and ethinyl estradiol vaginal ring used to prevent pregnancy for up to one year. Expert Opin. Drug Deliv. 2020, 17, 1–10. [Google Scholar] [CrossRef]
- Stifani, B.M.; Plagianos, M.; Vieira, C.S.; Merkatz, R.B. Factors associated with nonadherence to instructions for using the Nestorone®/ethinyl estradiol contraceptive vaginal ring. Contraception 2018, 97, 415–421. [Google Scholar] [CrossRef]
- Larner, J.; Reel, J.; Blye, R. Circulating concentrations of the antiprogestins CDB-2914 and mifepristone in the female rhesus monkey following various routes of administration. Hum. Reprod. 2000, 15, 1100–1106. [Google Scholar] [CrossRef] [Green Version]
- Brache, V.; Sitruk-Ware, R.; Williams, A.; Blithe, D.; Croxatto, H.; Kumar, N.; Kumar, S.; Tsong, Y.-Y.; Sivin, I.; Nath, A. Effects of a novel estrogen-free, progesterone receptor modulator contraceptive vaginal ring on inhibition of ovulation, bleeding patterns and endometrium in normal women. Contraception 2012, 85, 480–488. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saxena, B.B.; Han, Y.A.; Fu, D.; Rathnam, P.; Singh, M.; Laurence, J.; Lerner, S. Sustained release of microbicides by newly engineered vaginal rings. Aids 2009, 23, 917–922. [Google Scholar] [CrossRef] [PubMed]
- Baeten, J.M.; Palanee-Phillips, T.; Brown, E.R.; Schwartz, K.; Soto-Torres, L.E.; Govender, V.; Mgodi, N.M.; Matovu Kiweewa, F.; Nair, G.; Mhlanga, F. Use of a vaginal ring containing dapivirine for HIV-1 prevention in women. N. Engl. J. Med. 2016, 375, 2121–2132. [Google Scholar] [CrossRef] [PubMed]
- Wieder, D.R.; Pattimakiel, L. Examining the efficacy, safety, and patient acceptability of the combined contraceptive vaginal ring (NuvaRing®). Int. J. Womens Health 2010, 2, 401. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roumen, F.J. The contraceptive vaginal ring compared with the combined oral contraceptive pill: A comprehensive review of randomized controlled trials. Contraception 2007, 75, 420–429. [Google Scholar] [CrossRef]
- Dieben, T.O.; Roumen, F.J.; Apter, D. Efficacy, cycle control, and user acceptability of a novel combined contraceptive vaginal ring. Obstet. Gynecol. 2002, 100, 585–593. [Google Scholar] [PubMed]
- Oddsson, K.; Leifels-Fischer, B.; de Melo, N.R.; Wiel-Masson, D.; Benedetto, C.; Verhoeven, C.H.; Dieben, T.O. Efficacy and safety of a contraceptive vaginal ring (NuvaRing) compared with a combined oral contraceptive: A 1-year randomized trial. Contraception 2005, 71, 176–182. [Google Scholar] [CrossRef]
- Patra, A.; Roy, A.K.; Gupta, G.; Maikhuri, J.P.; Kumar, M.; Shukla, P.K.; Jain, R.K.; Batra, S.; Singh, V. Discovery of substituted isoxazolecarbaldehydes as potent spermicides, acrosin inhibitors and mild anti-fungal agents. Hum. Reprod. 2005, 20, 2301–2308. [Google Scholar] [CrossRef] [Green Version]
- Maikhuri, J.P.; Dwivedi, A.K.; Dhar, J.D.; Setty, B.S.; Gupta, G. Mechanism of action of some acrylophenones, quinolines and dithiocarbamate as potent, non-detergent spermicidal agents. Contraception 2003, 67, 403–408. [Google Scholar] [CrossRef]
- Bernstein, G.S. Physiological aspects of vaginal contraception. Contraception 1974, 9, 333–345. [Google Scholar] [CrossRef]
- Singh, A.; Sharma, P.K.; Kumar, N.; Dudhe, R.; Dixit, S. Novel spermicidal agent—A review. Der Pharma Chem. 2010, 4, 278–297. [Google Scholar]
- Reddy, K.V.R.; Aranha, C.; Gupta, S.M.; Yedery, R.D. Evaluation of antimicrobial peptide nisin as a safe vaginal contraceptive agent in rabbits: In vitro and in vivo studies. Reproduction 2004, 128, 117–126. [Google Scholar] [CrossRef] [PubMed]
- Batar, I. State-of-the-art of non-hormonal methods of contraception: II. Chemical barrier contraceptives. Eur. J. Contracept. Reprod. Health Care Off. J. Eur. Soc. Contracept. 2010, 15, 89–95. [Google Scholar] [CrossRef] [PubMed]
- Tepper, N.K.; Krashin, J.W.; Curtis, K.M.; Cox, S.; Whiteman, M.K. Update to CDC’s US medical eligibility criteria for contraceptive use, 2016: Revised recommendations for the use of hormonal contraception among women at high risk for HIV infection. Mmwr. Morb. Mortal. Wkly. Rep. 2017, 66, 990. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schreiber, C.A.; Ratcliffe, S.J.; Sammel, M.D.; Whittaker, P.G. A self-assessment efficacy tool for spermicide contraceptive users. Am. J. Obstet. Gynecol. 2016, 214, 264.e261–264.e267. [Google Scholar] [CrossRef]
- Vignini, A.; Buldreghini, E.; Nanetti, L.; Amoroso, S.; Boscaro, M.; Ricciardo-Lamonica, G.; Mazzanti, L.; Balercia, G. Free thiols in human spermatozoa: Are Na+/K+-ATPase, Ca2+-ATPase activities involved in sperm motility through peroxynitrite formation? Reprod. Biomed. Online 2009, 18, 132–140. [Google Scholar] [CrossRef]
- Mendez, F.; Castro, A.; Ortega, A. Use effectiveness of a spermicidal suppository containing benzalkonium chloride. Contraception 1986, 34, 353–362. [Google Scholar]
- Xiao-Hui, D.; Qi, C.; Waller, D.P.; Kaminski, J.; Zaneveld, L.J.D. Comparison of the spermicidal activity and acute toxicity of nonoxynol-9 and agent 741[alkylphenoxy polyethoxy ethanol(10)]. Contraception 1986, 33, 1–5. [Google Scholar] [CrossRef]
- Livingston, G.M.; Thornburgh, D.B.; Longmore, J. Antiseptic Spermicidal Composition and Means for Its Application. U.S. Patent 8,518,434, 27 August 2013. [Google Scholar]
- D’Cruz, O.J.; Uckun, F.M. Gel-microemulsions as vaginal spermicides and intravaginal drug delivery vehicles. Contraception 2001, 64, 113–123. [Google Scholar] [CrossRef]
- Digenis, G.A.; Nosek, D.; Mohammadi, F.; Darwazeh, N.B.; Anwar, H.S.; Zavos, P.M. Novel vaginal controlled-delivery systems incorporating coprecipitates of nonoxynol-9. Pharm. Dev. Technol. 1999, 4, 421–430. [Google Scholar] [CrossRef]
- Lee, C.-H.; Chien, Y.W. Development and evaluation of a mucoadhesive drug delivery system for dual-controlled delivery of nonoxynol-9. J. Control. Release 1996, 39, 93–103. [Google Scholar] [CrossRef]
- Malcolm, K.; Woolfson, D.; Russell, J.; Andrews, C. In vitro release of nonoxynol-9 from silicone matrix intravaginal rings. J. Control. Release 2003, 91, 355–364. [Google Scholar] [CrossRef]
- Miari, V.F.; Ison, C.A. Is There a Role for Topical Antiseptics in the Treatment of Gonorrhoea? BMJ Publishing Group Ltd.: London, UK, 2017. [Google Scholar]
- Roddy, R.E.; Zekeng, L.; Ryan, K.A.; Tamoufé, U.; Tweedy, K.G. Effect of nonoxynol-9 gel on urogenital gonorrhea and chlamydial infection: A randomized controlled trial. JAMA 2002, 287, 1117–1122. [Google Scholar] [CrossRef] [Green Version]
- Wilkinson, D.; Ramjee, G.; Tholandi, M.; Rutherford, G.W. Nonoxynol-9 for preventing vaginal acquisition of sexually transmitted infections by women from men. Cochrane Database Syst. Rev. 2002. [Google Scholar] [CrossRef] [PubMed]
- Roberts, J.N.; Buck, C.B.; Thompson, C.D.; Kines, R.; Bernardo, M.; Choyke, P.L.; Lowy, D.R.; Schiller, J.T. Genital transmission of HPV in a mouse model is potentiated by nonoxynol-9 and inhibited by carrageenan. Nat. Med. 2007, 13, 857–861. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Florez, M.; Díaz, E.S.; Brito, I.; González, J.; Morales, P. N,N′–Dithiobisphthalimide, a disulfide aromatic compound, is a potent spermicide agent in humans. Syst. Biol. Reprod. Med. 2011, 57, 309–317. [Google Scholar] [CrossRef]
- Schill, W.B.; Wolff, H.H. Ultrastructure of human spermatozoa in the presence of the spermicide nonoxinol-9 and a vaginal contraceptive containing nonoxinol-9. Andrologia 1981, 13, 42–49. [Google Scholar] [CrossRef]
- Fichorova, R.N.; Tucker, L.D.; Anderson, D.J. The Molecular Basis of Nonoxynol-9-Induced Vaginal Inflammation and Its Possible Relevance to Human Immunodeficiency Virus Type 1 Transmission. J. Infect. Dis. 2001, 184, 418–428. [Google Scholar] [CrossRef] [Green Version]
- Pandey, R.R.; Srivastava, A.; Pachauri, S.D.; Khandelwal, K.; Naqvi, A.; Malasoni, R.; Kushwaha, B.; Kumar, L.; Maikhuri, J.P.; Pandey, G.; et al. Design and synthesis of gamma-butyrolactone derivatives as potential spermicidal agents. Bioorganic Med. Chem. Lett. 2014, 24, 3903–3906. [Google Scholar] [CrossRef]
- Nelson, A.L. An overview of properties of Amphora (Acidform) contraceptive vaginal gel. Expert Opin. Drug Saf. 2018, 17, 935–943. [Google Scholar] [CrossRef]
- Yang, M.; Zhi, R.; Lu, L.; Dong, M.; Wang, Y.; Tian, F.; Xia, M.; Hu, J.; Dai, Q.; Jiang, S. A CCR5 antagonist-based HIV entry inhibitor exhibited potent spermicidal activity: Potential application for contraception and prevention of HIV sexual transmission. Eur. J. Pharm. Sci. 2018, 117, 313–320. [Google Scholar] [CrossRef] [PubMed]
- Ceña-Diez, R.; Martin-Moreno, A.; de la Mata, F.J.; Gómez-Ramirez, R.; Muñoz, E.; Ardoy, M.; Muñoz-Fernández, M.Á. G1-S4 or G2-S16 carbosilane dendrimer in combination with Platycodin D as a promising vaginal microbicide candidate with contraceptive activity. Int. J. Nanomed. 2019, 14, 2371. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- D’Cruz, O.J.; Yiv, S.H.; Waurzyniak, B.; Uckun, F.M. Contraceptive efficacy and safety studies of a novel microemulsion-based lipophilic vaginal spermicide. Fertil. Steril. 2001, 75, 115–124. [Google Scholar] [CrossRef]
- Jangir, S.; Bala, V.; Lal, N.; Kumar, L.; Sarswat, A.; Kumar, L.; Kushwaha, B.; Singh, P.; Shukla, P.K.; Maikhuri, J.P.; et al. A unique dithiocarbamate chemistry during design & synthesis of novel sperm-immobilizing agents. Org. Biomol. Chem. 2014, 12, 3090–3099. [Google Scholar] [CrossRef] [PubMed]
- Jain, A.; Lal, N.; Kumar, L.; Verma, V.; Kumar, R.; Kumar, L.; Singh, V.; Mishra, R.K.; Sarswat, A.; Jain, S.K.; et al. Novel trichomonacidal spermicides. Antimicrob. Agents Chemother. 2011, 55, 4343–4351. [Google Scholar] [CrossRef] [Green Version]
- Agarwal, A.; Saleh, R.A.; Bedaiwy, M.A. Role of reactive oxygen species in the pathophysiology of human reproduction. Fertil. Steril. 2003, 79, 829–843. [Google Scholar] [CrossRef] [Green Version]
- Chaki, S.P.; Misro, M.M. Assessment of human sperm function after hydrogen peroxide exposure. development of a vaginal contraceptive. Contraception 2002, 66, 187–192. [Google Scholar] [CrossRef]
- D’Cruz, O.J.; Venkatachalam, T.K.; Uckun, F.M. Novel Thiourea Compounds as Dual-Function Anti-HIV and Spermicidal Agents. Fertil. Steril. 2000, 74, S72–S73. [Google Scholar] [CrossRef]
- Dwivedi, A.K.; Sharma, V.L.; Kumaria, N.; Kiran Kumar, S.T.V.S.; Srivastava, P.K.; Ansari, A.H.; Maikhuri, J.P.; Gupta, G.; Dhar, J.D.; Roy, R.; et al. Synthesis of disulfide esters of dialkylaminocarbothioic acid as potent, non-detergent spermicidal agents. Bioorganic Med. Chem. 2007, 15, 6642–6648. [Google Scholar] [CrossRef]
- Naz, R.K.; Lough, M.L.; Barthelmess, E.K. Curcumin: A novel non-steroidal contraceptive with antimicrobial properties. Front. Biosci. Elite Ed. 2016, 8, 113–128. [Google Scholar] [CrossRef]
- Ogbuewu, I.P.; Unamba-Oparah, I.C.; Odoemenam, V.U.; Etuk, I.F.; Okoli, I.C. The potentiality of medicinal plants as the source of new contraceptive principles in males. N. Am. J. Med. Sci. 2011, 3, 255. [Google Scholar] [CrossRef] [PubMed]
- Mukherjee, M.; Datta, M.; Biswas, S.; Pal, A.K.; Malakar, D.; Bhattacharyya, A.K.; Bhattacharya, S.; Kobayashi, H. Immotilin, a novel sperm immobilizing protein. Fertil. Steril. 2003, 79, 1673–1675. [Google Scholar] [CrossRef]
- Shin, J.M.; Gwak, J.W.; Kamarajan, P.; Fenno, J.C.; Rickard, A.H.; Kapila, Y.L. Biomedical applications of nisin. J. Appl. Microbiol. 2016, 120, 1449–1465. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sutyak, K.E.; Anderson, R.A.; Dover, S.E.; Feathergill, K.A.; Aroutcheva, A.A.; Faro, S.; Chikindas, M.L. Spermicidal Activity of the Safe Natural Antimicrobial Peptide Subtilosin. Infect. Dis. Obstet. Gynecol. 2008, 2008, 6. [Google Scholar] [CrossRef] [PubMed]
- Aranha, C.; Gupta, S.; Reddy, K.V. Contraceptive efficacy of antimicrobial peptide Nisin: In vitro and in vivo studies. Contraception 2004, 69, 333–338. [Google Scholar] [CrossRef] [PubMed]
- Gupta, S.; Kaur, I.P.; Prabha, V. Evaluation of antifertility effect of gel formulation containing sperm immobilizing factor: In vitro and in vivo studies. Eur. J. Pharm. Sci. Off. J. Eur. Fed. Pharm. Sci. 2016, 81, 67–74. [Google Scholar] [CrossRef]
- Kaur, S.; Prabha, V.; Sarwal, A. Receptor Mediated Agglutination of Human Spermatozoa by Spermagglutinating Factor Isolated From Staphylococcus aureus. J. Urol. 2010, 184, 2586–2590. [Google Scholar] [CrossRef]
- Suthutvoravut, S.; Kamyarat, O. Spermicidal effects of lemon juice and juices from other natural products. Agric. Nat. Resour. 2016, 50, 133–138. [Google Scholar] [CrossRef] [Green Version]
- Lakshmi, V.; Saxena, A.; Mishra, S.K.; Raghubir, R.; Srivastava, M.N.; Jain, R.K.; Maikhuri, J.P.; Gupta, G. Spermicidal Activity of Bivittoside D from Bohadschia vitiensis. Arch. Med. Res. 2008, 39, 631–638. [Google Scholar] [CrossRef]
- Saha, P.; Majumdar, S.; Pal, D.; Pal, B.C.; Kabir, S.N. Evaluation of spermicidal activity of MI-saponin A. Reprod. Sci. 2010, 17, 454–464. [Google Scholar] [CrossRef]
- Zhou, B.; Qiu, Z.; Liu, G.; Liu, C.; Zhang, J. Spermicidal and antigonococcal effects of tannins from pomegranate rind. J. Med. Plants Res. 2012, 6, 1334–1339. [Google Scholar] [CrossRef]
- D’Cruz, O.J.; Uckun, F.M. Vaginal contraceptive activity of a chelated vanadocene. Contraception 2005, 72, 146–156. [Google Scholar] [CrossRef] [PubMed]
- D’Cruz, O.J.; Dong, Y.; Uckun, F.M. Potent dual anti-HIV and spermicidal activities of novel oxovanadium(V) complexes with thiourea non-nucleoside inhibitors of HIV-1 reverse transcriptase. Biochem. Biophys. Res. Commun. 2003, 302, 253–264. [Google Scholar] [CrossRef]
- D’Cruz, O.J.; Ghosh, P.; Uckun, F.M. Spermicidal activity of metallocene complexes containing vanadium(IV) in humans. Biol. Reprod. 1998, 58, 1515–1526. [Google Scholar] [CrossRef]
- D’Cruz, O.J.; Vassilev, A.; Uckun, F.M. Evaluation of boar sperm as a model system to study the mechanism of spermicidal activity of vanadocenes. Biochem. Biophys. Res. Commun. 2000, 270, 826–830. [Google Scholar] [CrossRef]
- Less, G.B.; Ockwig, N.W.; Rasmussen, P.G.; Smith, G.D.; Keller, L.M.; Drach, J.C. Vanadium Complex of 2-(2′-Pyridyl)-4,5-dicyanoimidazole Showing Spermicidal and Cytotoxic Properties. Inorg. Chem. 2006, 45, 7105–7110. [Google Scholar] [CrossRef]
- Hong, C.Y.; Lee, M.F.; Lai, L.J.; Wang, C.P. Effect of lipid peroxidation on beating frequency of human sperm tail. Andrologia 1994, 26, 61–65. [Google Scholar] [CrossRef]
- Calamera, J.C.; Giovenco, P.; Quiros, M.C.; Brugo, S.; Dondero, F.; Nicholson, R.F. Effect of lipid peroxidation upon human spermatic adenosinetriphosphate (ATP). Relationship with motility, velocity and linearity of the spermatozoa. Andrologia 1989, 21, 48–54. [Google Scholar] [CrossRef]
- Aitken, R.J.; Harkiss, D.; Buckingham, D. Relationship between iron-catalysed lipid peroxidation potential and human sperm function. J. Reprod. Fertil. 1993, 98, 257–265. [Google Scholar] [CrossRef]
- Han, Y.A.; Singh, M.; Saxena, B.B. Development of vaginal rings for sustained release of nonhormonal contraceptives and anti-HIV agents. Contraception 2007, 76, 132–138. [Google Scholar] [CrossRef]
- Saxena, B.B.; Singh, M.; Gospin, R.M.; Chu, C.C.; Ledger, W.J. Efficacy of nonhormonal vaginal contraceptives from a hydrogel delivery system. Contraception 2004, 70, 213–219. [Google Scholar] [CrossRef] [PubMed]
- Jafari, H.; Bernaerts, K.V.; Dodi, G.; Shavandi, A. Chitooligosaccharides for wound healing biomaterials engineering. Mater. Sci. Eng. C 2020, 117, 111266. [Google Scholar] [CrossRef] [PubMed]
- Green, T.R.; Fellman, J.H.; Wolf, D.P. Human spermicidal activity of inorganic and organic oxidants. Fertil. Steril. 2001, 76, 157–162. [Google Scholar] [CrossRef]
- LeVeen, H.H.; LeVeen, R.F.; LeVeen, E.G. The mythology of povidone-iodine and the development of self-sterilizing plastics. Surg. Gynecol. Obstet. 1993, 176, 183–190. [Google Scholar]
- Jan, S.T.; Shih, M.J.; Venkatachalam, T.K.; D’Cruz, O.J.; Chen, C.L.; Uckun, F.M. Synthesis of dual function (5R,6R)- and (5S,6S)-5-bromo-6-methoxy-5,6-dihydro-AZT-5′-(para-bromophenyl methoxyalaninyl phosphate) as novel spermicidal and anti-HIV agents. Antivir. Chem. Chemother. 1999, 10, 39–46. [Google Scholar] [CrossRef]
- D’Cruz, O.J.; Zhu, Z.; Yiv, S.H.; Chen, C.-L.; Waurzyniak, B.; Uckun, F.M. WHI-05, a novel bromo-methoxy substituted phenyl phosphate derivative of zidovudine, is a dual-action spermicide with potent anti-HIV activity. Contraception 1999, 59, 319–331. [Google Scholar] [CrossRef]
- Bharitkar, Y.P.; Banerjee, M.; Kumar, S.; Paira, R.; Meda, R.; Kuotsu, K.; Mondal, N.B. Search for a potent microbicidal spermicide from the isolates of Shorea robusta resin. Contraception 2013, 88, 133–140. [Google Scholar] [CrossRef]
- Paira, P.; Hazra, A.; Kumar, S.; Paira, R.; Sahu, K.B.; Naskar, S.; Saha, P.; Mondal, S.; Maity, A.; Banerjee, S.; et al. Efficient synthesis of 3,3-diheteroaromatic oxindole analogues and their in vitro evaluation for spermicidal potential. Bioorganic Med. Chem. Lett. 2009, 19, 4786–4789. [Google Scholar] [CrossRef]
- Jones, R.E.; Lopez, K.H. Chapter 13-Contraception. In Human Reproductive Biology, 4th ed.; Jones, R.E., Lopez, K.H., Eds.; Academic Press: San Diego, CA, USA, 2014; pp. 245–269. [Google Scholar]
Figure 1.
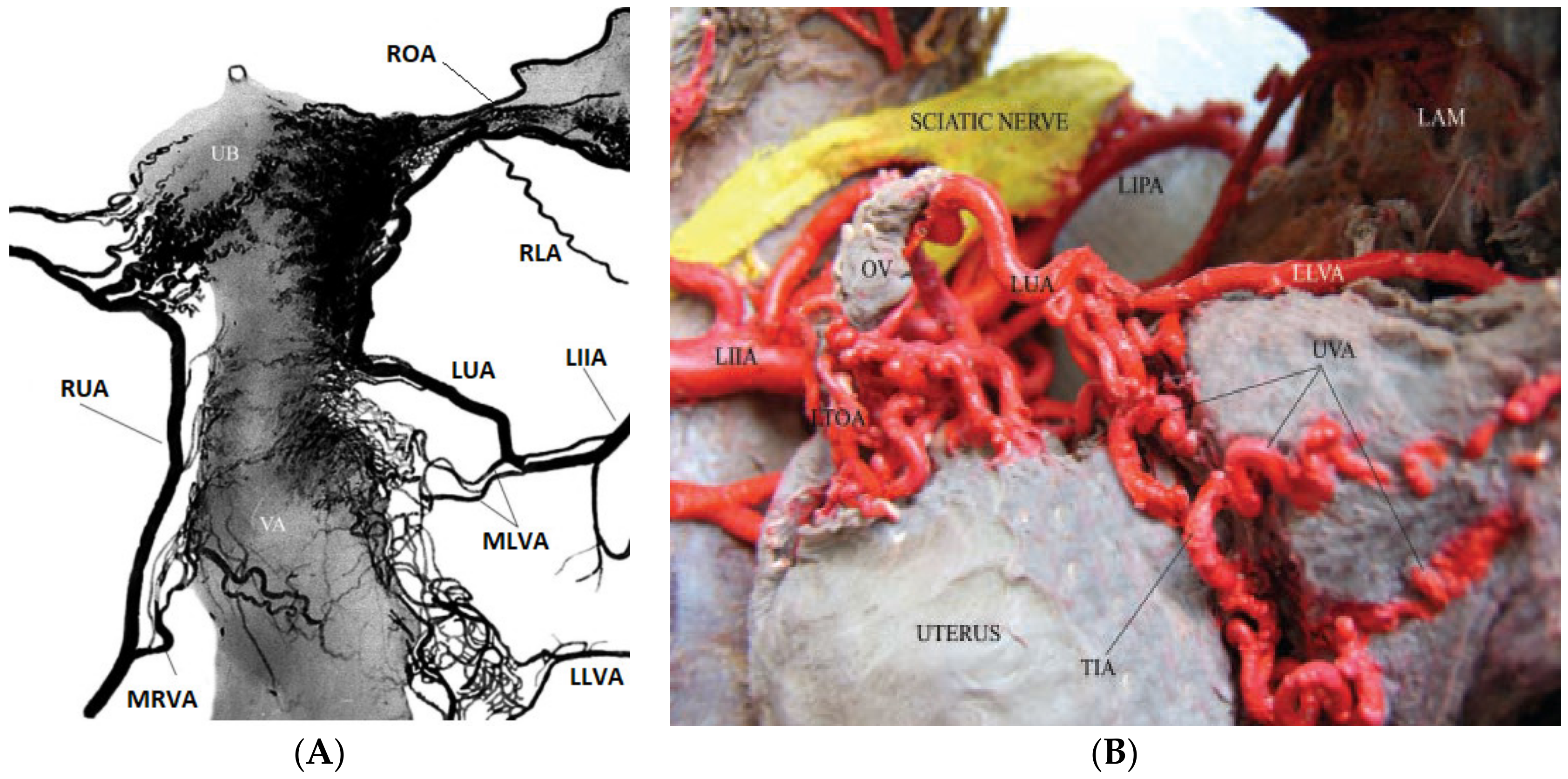
(A) Arteriography of the uterus, ovaries, fallopian tubes, and upper vaginal segment. With permission from Ref (Belou P. Atlas estereosco’pico de anatomı’a de las arterias del hombre. Tomo III 2da parte. En: Revisión anatómica del sistema arterial (Stereoscopic Atlas of Human Arterial Anatomy. Volume 3; 2nd Part in: Anatomic Revision of Arterial System). Buenos Aires: El Ateneo, 1934:98–119). LIIA, left internal iliac artery; LLVA, lower left vaginal artery; LUA, left uterine artery; MLVA, middle left vaginal artery; MRVA, middle right vaginal artery; RLA, round ligament artery; ROA, right ovarian artery; RUA, right uterine artery; UB, the uterine body; VA, vagina. (B) Cadaveric specimen. Upper and left view of the genital- urinary organs. In the middle sector of the illustration, a thick intrauterine anastomosis can be identified. Below, thick vaginal branches anastomosing with the uterine artery can be observed. LAM, levator ani muscle; LIIA, left internal iliac artery; LIPA, left internal pudendal artery; LLVA, lower left vaginal artery; LTOA, left tubo-ovarian artery; LUA, left uterine artery; OV, ovary; TIA, transmedial inter uterine anastomosis; UVA, uterovaginal anastomosis [54]. Figure license number: 4810031431586.
Figure 1.
(A) Arteriography of the uterus, ovaries, fallopian tubes, and upper vaginal segment. With permission from Ref (Belou P. Atlas estereosco’pico de anatomı’a de las arterias del hombre. Tomo III 2da parte. En: Revisión anatómica del sistema arterial (Stereoscopic Atlas of Human Arterial Anatomy. Volume 3; 2nd Part in: Anatomic Revision of Arterial System). Buenos Aires: El Ateneo, 1934:98–119). LIIA, left internal iliac artery; LLVA, lower left vaginal artery; LUA, left uterine artery; MLVA, middle left vaginal artery; MRVA, middle right vaginal artery; RLA, round ligament artery; ROA, right ovarian artery; RUA, right uterine artery; UB, the uterine body; VA, vagina. (B) Cadaveric specimen. Upper and left view of the genital- urinary organs. In the middle sector of the illustration, a thick intrauterine anastomosis can be identified. Below, thick vaginal branches anastomosing with the uterine artery can be observed. LAM, levator ani muscle; LIIA, left internal iliac artery; LIPA, left internal pudendal artery; LLVA, lower left vaginal artery; LTOA, left tubo-ovarian artery; LUA, left uterine artery; OV, ovary; TIA, transmedial inter uterine anastomosis; UVA, uterovaginal anastomosis [54]. Figure license number: 4810031431586.

Figure 2.
Chemical structures of curcumin and allitridum, natural substances evaluated for their spermicidal activities.
Figure 2.
Chemical structures of curcumin and allitridum, natural substances evaluated for their spermicidal activities.

Figure 3.
Chemical structure of two synthetic spermicide reagents, vanadocene and iron gluconate.

Figure 4.
Chemical structures of zidovudine derivatives as the potential spermicides and anti-HIV agents.
Figure 4.
Chemical structures of zidovudine derivatives as the potential spermicides and anti-HIV agents.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
Characteristics of commercially available vaginal formulations.
| Contraceptive | Product Name | Chemical Composition | Protect against STD | Hormones/Drug | Effectiveness Duration | Ref |
|---|---|---|---|---|---|---|
| Vaginal rings | Nuvaring® (MSD, Oss, the Netherlands) | Ethylene-vinyl acetate copolymer and magnesium stearate | No | Ethinyl estradiol and etonogestrel | One month | [64] |
| Progering (Silesia; Santiago, Chile) | Silicone | No | Progesterone | Three months | [65] | |
| AnnoveraTM | Silicone elastomer | No | Nestorone® and ethinyl estradiol | One year | [66] | |
| Ornibel® (Exeltis Healthcare, Spain) | polyurethane core, and ethylene-vinyl acetate membrane | No | Etonogestrel and ethinyl estradiol | Three weeks | [67] | |
| Femring® | Silicone | No | 17β-estradiol-3-acetate | Three months | [68] | |
| Implants | Norplant® | Six flexible closed capsules made of silicone rubber tubing | No | Progestin levonorgestrel | Five years | [69] |
| Implanon® | Ethylene-vinyl acetate copolymer | No | Etonogestrel | Five years | [70] | |
| Uniplant | Silicone rubber | Nomegestrol acetate | One year | [71] | ||
| Patch | Ortho EvraTM | Polyethylene, polyester | No | Norelgestromin /ethinyl estradiol | Three weeks | [25] |
| Twirla | Polyacrylate, polyisobutylene adhesive layer | No | Levonorgestrel/ethinyl estradiol | Every seven days | [72] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Jalalvandi, E.; Jafari, H.; Amorim, C.A.; Petri, D.F.S.; Nie, L.; Shavandi, A. Vaginal Administration of Contraceptives. Sci. Pharm. 2021, 89, 3. https://0-doi-org.brum.beds.ac.uk/10.3390/scipharm89010003
AMA Style
Jalalvandi E, Jafari H, Amorim CA, Petri DFS, Nie L, Shavandi A. Vaginal Administration of Contraceptives. Scientia Pharmaceutica. 2021; 89(1):3. https://0-doi-org.brum.beds.ac.uk/10.3390/scipharm89010003
Chicago/Turabian StyleJalalvandi, Esmat, Hafez Jafari, Christiani A. Amorim, Denise Freitas Siqueira Petri, Lei Nie, and Amin Shavandi. 2021. "Vaginal Administration of Contraceptives" Scientia Pharmaceutica 89, no. 1: 3. https://0-doi-org.brum.beds.ac.uk/10.3390/scipharm89010003