
Retinal Vessel Density Changes on Optical Coherence Tomography Angiography and Predictive Factors in Normal-Tension Glaucoma Treated with Topical Beta-Blocker


Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. OCTA Measurements
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Augusto, A.B.; Luca, B.; Alessandro, B.; Keith, B. European Glaucoma Society Terminology and Guidelines for Glaucoma, 4th Edition. Br. J. Ophthalmol. 2017, 101, 130–195. [Google Scholar] [CrossRef] [Green Version]
- Kaiser, H.J.; Schoetzau, A.; Stumpfig, D.; Flammer, J. Blood-flow velocities of the extraocular vessels in patients with high-tension and normal-tension primary open-angle glaucoma. Am. J. Ophthalmol. 1997, 123, 320–327. [Google Scholar] [CrossRef]
- Flammer, J.; Konieczka, K.; Flammer, A.J. The primary vascular dysregulation syndrome: Implications for eye diseases. EPMA J. 2013, 4, 14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsai, J.C. Influencing ocular blood flow in glaucoma patients: The cardiovascular system and healthy lifestyle choices. Can. J. Ophthalmol. 2008, 43, 347–350. [Google Scholar] [CrossRef] [PubMed]
- Triolo, G.; Rabiolo, A. Optical coherence tomography and optical coherence tomography angiography in glaucoma: Diagnosis, progression, and correlation with functional tests. Ther. Adv. Ophthalmol. 2020, 12, 2515841419899822. [Google Scholar] [CrossRef] [PubMed]
- Bekkers, A.; Borren, N.; Ederveen, V.; Fokkinga, E.; Andrade De Jesus, D.; Sanchez Brea, L.; Klein, S.; van Walsum, T.; Barbosa-Breda, J.; Stalmans, I. Microvascular damage assessed by optical coherence tomography angiography for glaucoma diagnosis: A systematic review of the most discriminative regions. Acta Ophthalmol. 2020, 98, 537–558. [Google Scholar] [CrossRef] [Green Version]
- Van Melkebeke, L.; Barbosa-Breda, J.; Huygens, M.; Stalmans, I. Optical Coherence Tomography Angiography in Glaucoma: A Review. Ophthalmic Res. 2018, 60, 139–151. [Google Scholar] [CrossRef]
- Renard, P.; Kovalski, J.L.; Cochereau, I.; Jaulerry, S.; Williamson, W.; Elena, P.P.; Lablache Combier, M.; Allaire, C.; Siou-Mermet, R. Comparison of carteolol plasmatic levels after repeated instillations of long-acting and regular formulations of carteolol 2% in glaucoma patients. Graefes Arch. Clin. Exp. Ophthalmol. 2005, 243, 1221–1227. [Google Scholar] [CrossRef]
- Chihara, E.; Dimitrova, G.; Chihara, T. Increase in the OCT angiographic peripapillary vessel density by ROCK inhibitor ripasudil instillation: A comparison with brimonidine. Graefes Arch. Clin. Exp. Ophthalmol. 2018, 256, 1257–1264. [Google Scholar] [CrossRef] [Green Version]
- Venugopal, J.P.; Rao, H.L.; Weinreb, R.N.; Dasari, S.; Riyazuddin, M.; Pradhan, Z.S.; Puttaiah, N.K.; Devi, S.; Mansouri, K.; Webers, C.A.B. Repeatability and comparability of peripapillary vessel density measurements of high-density and non-high-density optical coherence tomography angiography scans in normal and glaucoma eyes. Br. J. Ophthalmol. 2019, 103, 949–954. [Google Scholar] [CrossRef]
- Venugopal, J.P.; Rao, H.L.; Weinreb, R.N.; Pradhan, Z.S.; Dasari, S.; Riyazuddin, M.; Puttiah, N.K.; Rao, D.A.S.; Devi, S.; Mansouri, K.; et al. Repeatability of vessel density measurements of optical coherence tomography angiography in normal and glaucoma eyes. Br. J. Ophthalmol. 2018, 102, 352–357. [Google Scholar] [CrossRef]
- Jaillon, P. Relevance of intrinsic sympathomimetic activity for beta blockers. Am. J. Cardiol. 1990, 66, 21C–23C. [Google Scholar] [CrossRef]
- Ireland, M.A.; Littler, W.A. The effects of oral accbutolol and propranolol on forearm blood flow in hypertensive patients. Br. J. Clin. Pharmacol. 1981, 12, 363–368. [Google Scholar] [CrossRef] [Green Version]
- Langlois, M.; Bremont, B.; Rousselle, D.; Gaudy, F. Structural analysis by the comparative molecular field analysis method of the affinity of beta-adrenoreceptor blocking agents for 5-HT1A and 5-HT1B receptors. Eur. J. Pharmacol. 1993, 244, 77–87. [Google Scholar] [CrossRef]
- De Vries, P.; Sanchez-Lopez, A.; Centurion, D.; Heiligers, J.P.; Saxena, P.R.; Villalon, C.M. The canine external carotid vasoconstrictor 5-HT1 receptor: Blockade by 5-HT1B (SB224289), but not by 5-HT1D (BRL15572) receptor antagonists. Eur. J. Pharmacol. 1998, 362, 69–72. [Google Scholar] [CrossRef]
- Montanari, P.; Marangoni, P.; Oldani, A.; Ratiglia, R.; Raiteri, M.; Berardinelli, L. Color Doppler imaging study in patients with primary open-angle glaucoma treated with timolol 0.5% and carteolol 2. Eur. J. Ophthalmol. 2001, 11, 240–244. [Google Scholar] [CrossRef] [PubMed]
- Kawai, M.; Nagaoka, T.; Takahashi, A.; Sato, E.; Yoshida, A. Effects of topical carteolol on retinal arterial blood flow in primary open-angle glaucoma patients. Jpn. J. Ophthalmol. 2012, 56, 458–463. [Google Scholar] [CrossRef] [PubMed]
- Cruickshank, J.M. The clinical importance of cardioselectivity and lipophilicity in beta blockers. Am. Heart J. 1980, 100, 160–178. [Google Scholar] [CrossRef]
- Ferrari-Dileo, G. Beta 1 and beta 2 adrenergic binding sites in bovine retina and retinal blood vessels. Investig. Ophthalmol. Vis. Sci. 1988, 29, 695–699. [Google Scholar]
- Denis, P.; Elena, P.P. Retinal vascular beta-adrenergic receptors in man. Ophtalmologie 1989, 3, 62–64. [Google Scholar]
- Feihl, F.; Liaudet, L.; Levy, B.I.; Waeber, B. Hypertension and microvascular remodelling. Cardiovasc. Res. 2008, 78, 274–285. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| n = 80 | Mean | SD | SEM |
|---|---|---|---|
| Age (yrs) | 59.7 | 11.4 | 1.28 |
| CCT (um) | 536.1 | 39.5 | 4.40 |
| Axial length (mm) | 25 | 1.6 | 0.18 |
| VA(logMAR) | 0.27 | 0.27 | 0.03 |
| IOP(mmHg) | 15.2 | 2.5 | 0.27 |
| MD (dB) | −4.8 | 4.5 | 0.50 |
| PSD (dB) | 5.6 | 3.8 | 0.43 |
| Univariate | Multivariate | |||||
|---|---|---|---|---|---|---|
| B | (95% CI) | p Value | B | (95% CI) | p Value | |
| Age | −0.718 | (−1.254, −0.182) | 0.009 | −0.644 | (−1.253, −0.036) | 0.038 |
| CCT | −0.159 | (−0.354, 0.037) | 0.111 | −0.109 | (−0.293, 0.075) | 0.247 |
| Axial length | 0.345 | (−4.221, 4.911) | 0.882 | -- | ||
| VA | −7.999 | (−33.166, 17.169) | 0.533 | -- | ||
| IOP | −0.827 | (−3.590, 1.935) | 0.557 | -- | ||
| IOP change percentage | 0.211 | (−0.103, 0.526) | 0.188 | 0.111 | (−0.216, 0.438) | 0.507 |
| MD | 0.358 | (−0.886, 1.602) | 0.573 | -- | ||
| PSD | 1.122 | (−0.492, 2.737) | 0.173 | 0.77 | (−0.661, 2.201) | 0.292 |
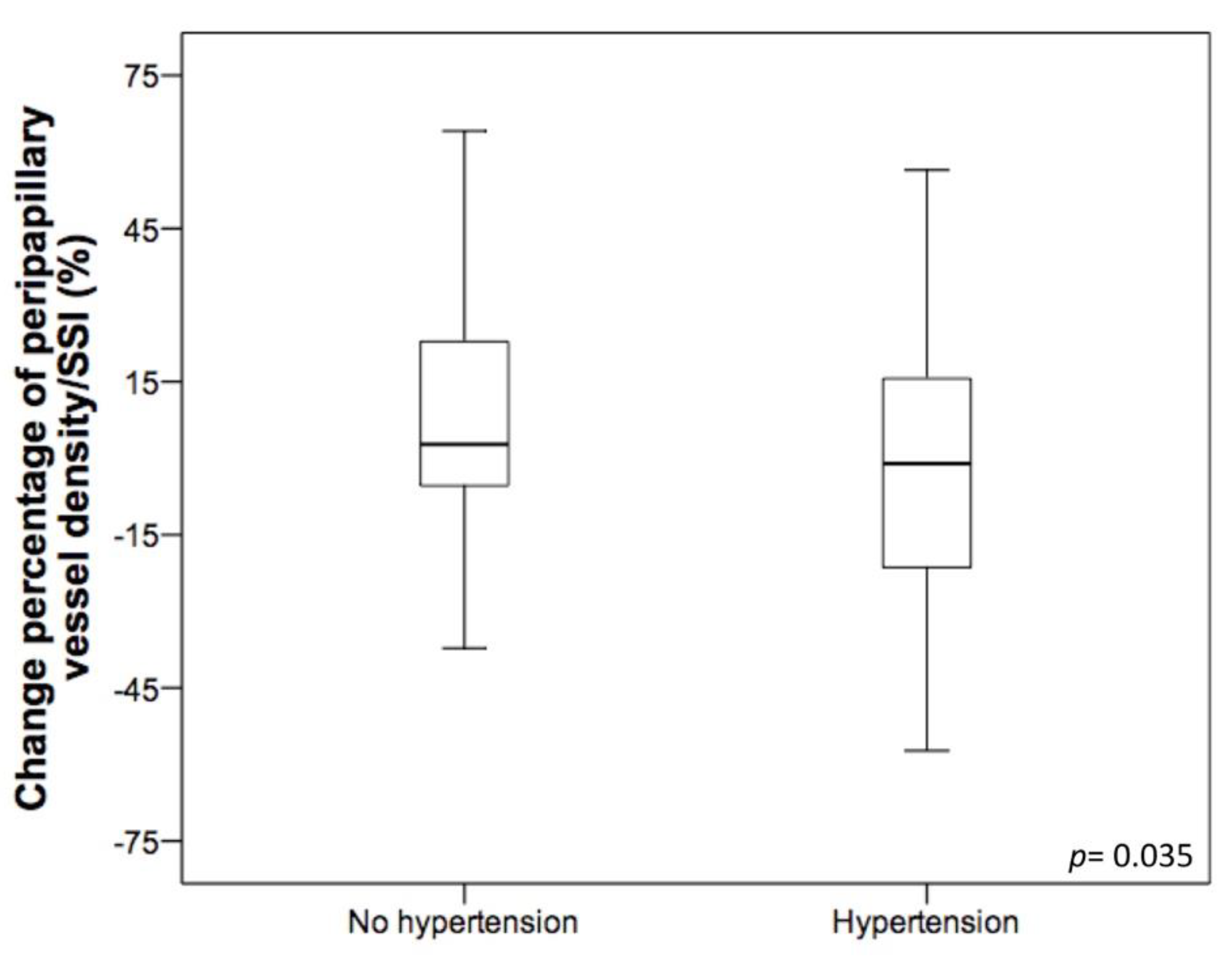
| Hypertension | −14.415 | (−27.816, −1.014) | 0.035 | −12.483 | (−24.569, −0.397) | 0.043 |
| Gender | 0.336 | (−12.923, 13.596) | 0.96 | -- | ||
| Univariate | Multivariate | |||||
|---|---|---|---|---|---|---|
| B | (95% CI) | p Value | B | (95% CI) | p Value | |
| Peripapillary VD/SSI | −69.06 | (−94.11, −44.00) | <0.001 | −64.94 | (−89.72, −40.17) | <0.001 |
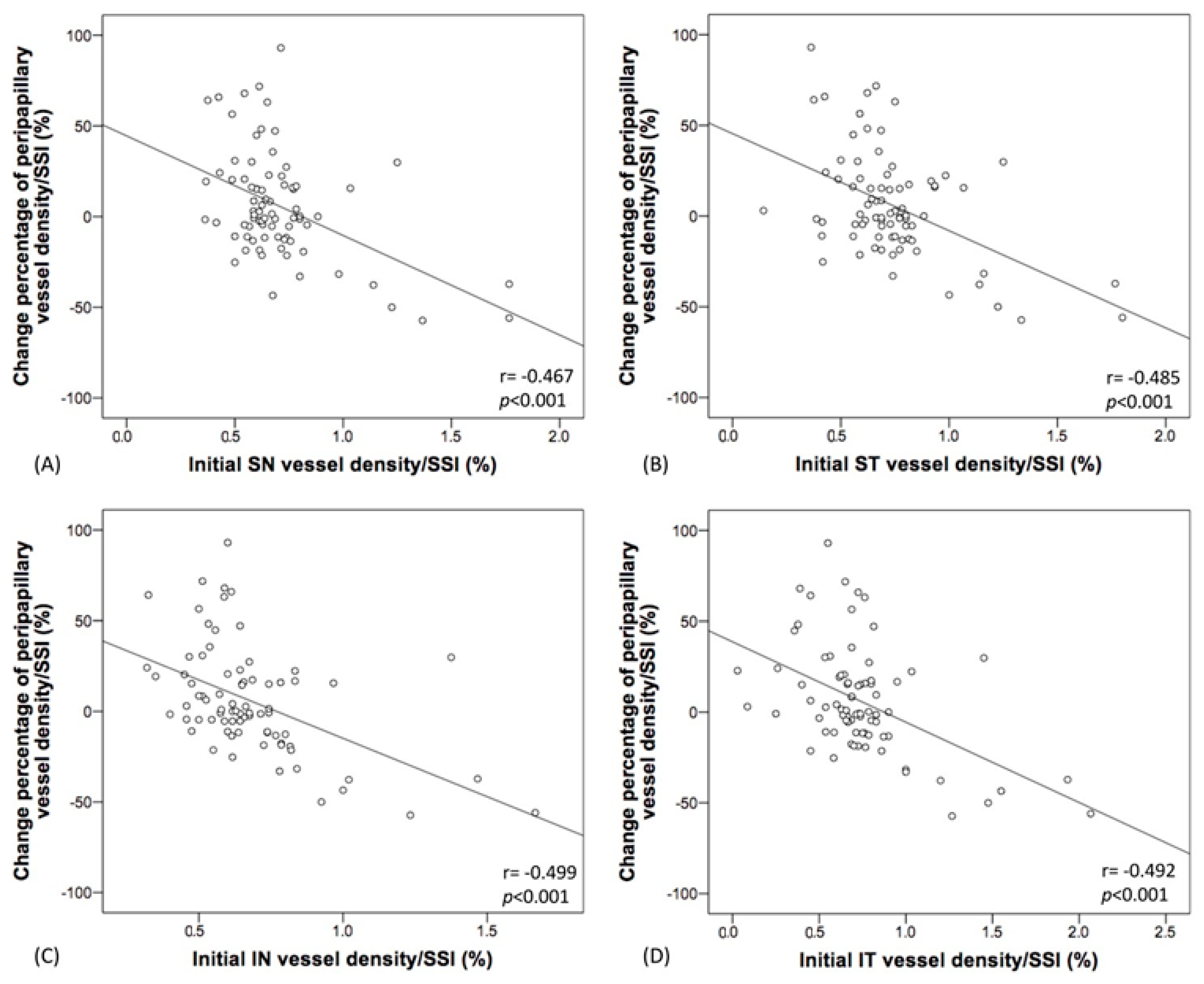
| SN peripapillary VD/SSI | −54.66 | (−78.38, −35.95) | <0.001 | −52.45 | (−68.97, −35.93) | <0.001 |
| ST peripapillary VD/SSI | −53.81 | (−72.19, −35.43) | <0.001 | −51.95 | (−68.97, −33.94) | <0.001 |
| T peripapillary VD/SSI | −58.84 | (−85.21, −32.47) | <0.001 | −53.4 | (−80.96, −25.85) | <0.001 |
| IT peripapillary VD/SSI | −43.34 | (−54.22, −32.67) | <0.001 | −42.62 | (−55.32, −29.92) | <0.001 |
| IN peripapillary VD/SSI | −66.07 | (−90.95, −41.19) | <0.001 | −62.91 | (−86.85, −38.94) | <0.001 |
| N peripapillary VD/SSI | −56.17 | (−75.57, −36.77) | <0.001 | −52.52 | (−73.03, −32.01) | <0.001 |
| Superficial macula VD/SSI | −69.34 | (−97.03, −41.66) | <0.001 | −66.88 | (−95.66, −38.10) | <0.001 |
| Deep macula VD/SSI | −48.93 | (−80.31, −17.55) | 0.002 | −45.14 | (−76.54, −13.75) | 0.005 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, Y.-H.; Huang, S.-M.; Chuang, L.-H.; Chen, L.-C. Retinal Vessel Density Changes on Optical Coherence Tomography Angiography and Predictive Factors in Normal-Tension Glaucoma Treated with Topical Beta-Blocker. Sci. Pharm. 2021, 89, 40. https://0-doi-org.brum.beds.ac.uk/10.3390/scipharm89030040
Lin Y-H, Huang S-M, Chuang L-H, Chen L-C. Retinal Vessel Density Changes on Optical Coherence Tomography Angiography and Predictive Factors in Normal-Tension Glaucoma Treated with Topical Beta-Blocker. Scientia Pharmaceutica. 2021; 89(3):40. https://0-doi-org.brum.beds.ac.uk/10.3390/scipharm89030040
Chicago/Turabian StyleLin, Yun-Hsuan, Shih-Ming Huang, Lan-Hsin Chuang, and Lung-Chien Chen. 2021. "Retinal Vessel Density Changes on Optical Coherence Tomography Angiography and Predictive Factors in Normal-Tension Glaucoma Treated with Topical Beta-Blocker" Scientia Pharmaceutica 89, no. 3: 40. https://0-doi-org.brum.beds.ac.uk/10.3390/scipharm89030040