
Compatibility of Different Formulations in Pentravan® and Pentravan® Plus for Transdermal Drug Delivery


1
Fagron BV, Fascinatio Boulevard 350, 3065 WB Rotterdam, The Netherlands
2
Fagron US, 2400 Pilot Knob Rd. #200, St. Paul, MN 55120, USA
*
Author to whom correspondence should be addressed.
Sci. Pharm. 2021, 89(4), 51; https://0-doi-org.brum.beds.ac.uk/10.3390/scipharm89040051
Submission received: 25 October 2021
/
Revised: 18 November 2021
/
Accepted: 22 November 2021
/
Published: 23 November 2021
(This article belongs to the Special Issue Feature Papers in Scientia Pharmaceutica)
Abstract
:The potential therapeutic benefit of transdermal delivery systems for some active pharmaceutical ingredients (APIs) has been well-established for decades within the scientific community. However, together with the clinical efficacy, there is the need for an evaluation of the stability of such APIs in bases with known transdermal capabilities, which is necessary to provide the compounding pharmacist with confidence when providing transdermal products. In this study, the stability of danazol, metformin HCl, and resveratrol as individual ingredients, as well as metformin HCl, resveratrol, and Vitamin D3 in combinations at bracketed high and low concentrations, were evaluated over a period of 6 months, using a ready-to-use transdermal vehicle for compounding pharmacies (Pentravan® or Pentravan® Plus). The five formulations tested (F1: Danazol 50 mg/g + MiodesinTM 85 mg/g in Pentravan®, F2: Metformin HCl 200 mg/g in Pentravan®, F3: Resveratrol 200 mg/g in Pentravan®, F4: Metformin HCl 100 mg/g + Resveratrol 100 mg/g + Vitamin D3 5000 IU in Pentravan®, and F5: Metformin HCl 200 mg/g + Resveratrol 200 mg/g + Vitamin D3 5000 IU in Pentravan® Plus) presented a beyond-use date of at least 6 months, presenting high convenience for the compounding pharmacies.
1. Introduction
The pharmaceutical market is seeing an increased need for drugs available for transdermal delivery. Since the first transdermal patch was approved in the US by the FDA in 1979, not only has the number of transdermal drugs significantly increased but the rate at which transdermal drugs are approved has also more than tripled in recent years [1,2]. Despite this increase, there are still a significant number of drugs that could meet the criteria for transdermal delivery but remain commercially available via limited routes—most commonly, the oral route. There is a need for evidence to support the transdermal delivery of active pharmaceutical ingredients (APIs) to offer therapeutic alternatives for APIs that meet one or more of the below criteria [1,2]:
- undergoes extensive gut metabolism;
- undergoes extensive first-pass (hepatic) metabolism;
- associated with increased adverse effects when given orally;
- may exert benefits from localized elevated concentrations.
Additionally, there are a number of factors likened to API that need to be taken into consideration when one wishes to develop a transdermal dosage form, as the physicochemical properties of APIs determine their route and degree of absorption. These include, but are not limited to, pKa, molecule size, molecule stability, possibility of binding to epidermal components found along the way, and the oil/water partition coefficient. It is known, for example, that drugs in their nonionic forms have a greater capacity for permeation than those in dissociated forms. From this statement, it is clear that a lipophilic—more than a hydrophilic—character is necessary, although amphipathic molecules are good candidates to be promptly permeated. Another condition that directly affects absorption is the system’s thermodynamic potential. The greater the difference in concentration between the vehicle and the skin, the higher the potential and, hence, the greater the drive into the skin. Additionally, the pH of the formulation also interferes with the permeability. This is because, depending on its value, the ionization of weak acids and bases may occur, which is not desirable, since neutral substances are easier to permeate. In addition to the pH of the formulation, the skin pH (~6 in adults) also interferes with the degree of ionization of the compound, both of which should be taken into account. Finally, the factors related to patients are also important, as the skin is a tissue that is extremely rich in enzymes, which can metabolize drugs during their courses, as they catalyze both phase I and phase II reactions. This can be strategically considered in order to add a prodrug to the formulation so that it only becomes pharmacologically active when it crosses the skin. On the other hand, unforeseen reactions may occur that may inactivate it or change its intended action [3,4,5].
In this work, we focused on some of the APIs that meet the abovementioned criteria. Metformin HCl is a commonly prescribed drug for the management of type II diabetes and is often considered as a first-line treatment for this condition. It is an example of a drug that, when used orally, can cause significant gastrointestinal adverse effects, including nausea and diarrhea [6]. In addition to its utility for the systemic management of conditions such as diabetes, metformin HCl may also benefit from the local administration of specific types of cicatricial alopecia [7]. The transdermal penetration of metformin HCl has already been demonstrated in Pentravan, but in order to offer a complete transdermal solution, the stability must also be evaluated [8].
Danazol is a synthetic steroid used in the management of conditions such as endometriosis [9]. It is another example of a drug that may benefit from transdermal use, as it undergoes extensive first-pass metabolism, and as a result, it demonstrates poor oral bioavailability [10]. Resveratrol is a case of a substance with two isomeric forms, one of which undergoes significant and extensive metabolism. Trans-resveratrol undergoes significant degradation in acidic environments, which may contribute to its reduced oral bioavailability [11]. For both of these APIs, an alternative route of administration, such as transdermal application, would bypass the first-pass and gut metabolism, potentially offering increased bioavailability. In addition to its systemic use, resveratrol may also have utility topically for a variety of cutaneous disorders, such as inflammation and aging skin, and may even have antiproliferative activity [12]. Delivery through the outer layers of the skin will ensure it gets to the site of action in pharmaceutically relevant levels and provides an alternative to systemic use via the oral route.
Vitamin D3 (cholecalciferol) may also benefit from transdermal administration. When taken orally, systemic bioavailability is subject to significant variability, especially with patients suffering from fat malabsorption conditions [13]. Topical vitamin D3, similarly to resveratrol, may also play a role in the localized management of inflammatory skin conditions such as psoriasis [14].
Given the potential therapeutic benefits of a transdermal delivery system for each of these APIs, an evaluation of the stability in bases with known transdermal capabilities is necessary to provide the compounding pharmacist with confidence when providing therapeutic alternatives to patients for whom an oral route cannot be tolerated, for patients who need APIs that are associated with significant oral metabolism, or for patients that necessitate high local concentrations for the management of cutaneous conditions [15,16].
In this study, the stability of danazol, metformin HCl, and resveratrol as individual ingredients, as well as metformin HCl, resveratrol, and Vitamin D3 in combinations at bracketed high and low concentrations, has been evaluated over a period of 6 months, using a ready-to-use transdermal vehicle for compounding pharmacies (Pentravan® or Pentravan® Plus; Fagron, St. Paul, MN, USA).
2. Materials and Methods
2.1. Preparation of Active Pharmaceutical Ingredient Cream Samples
- The creams were prepared using the following general protocol with the formulations from Table 1. All the ingredients were provided by Fagron (St. Paul, MN, USA)
- The required quantity of each ingredient for the total amount to be prepared was calculated.
- Each ingredient was accurately weighed in a containment hood.
- The APIs and vehicle were placed into FagronLabTM mixing jars (FagronLabTM, Glinde, Germany) and stirred manually to initially combine the ingredients.
- The jar was placed in a FagronLabTM Mixing Pro (FagronLabTM, Glinde, Germany) and spun on the normal setting.
- The product was then transferred to an FagronLab™ TRM Ointment Mill (FagronLabTM, St. Paul, MN, USA) twice: first, on setting 3, and then, on setting 1.
- The product was then manually mixed an additional time.
- Finally, the creams were transferred to appropriately sized clean containers and labeled.
- The creams were then immediately assayed at T = 0 and stored at room temperature (20–25 °C) for the duration of the study.
2.2. Stability Study
The API samples were assayed by high-performance liquid chromatography (HPLC) at predetermined timepoints to verify the stability of the API in the vehicles. Aliquots for quantification (variable for each API) were withdrawn and diluted in order to obtain work solutions in the concentrations described in Table 1. Sampling times were: initial (T = 0), 1 month (T = 1), 2 months (T = 2), 3 months (T = 3), 4 months (T = 4), 5 months (T = 5), and 6 months (T = 6).
All creams were assayed independently, and at each timepoint, a system suitability check was performed using 5 standards run; the analyses were considered valid if the relative standard deviation (RSD) of each suitability check was lower than 2%. The evaluation parameter for the stability was the API assay with respect to T = 0 using the HPLC method (results given as percentage ± standard deviation). This normalization to force T = 0 to have a 100% result in the assay was performed to adequately see the possible decreases in contents of the APIs and to evaluate their suitability for use (for the products to be considered stable/compatible, the relative assay should lie within 90–110%, according to what international pharmacopeias suggest for finished products, such as the United States Pharmacopeia, British Pharmacopoeia, and European Pharmacopoeia) [17,18].
2.3. Chromatographic Conditions
All analyses were performed by HPLC using the conditions described in Table 2. The APIs contents were calculated by direct comparisons of their areas with the standard ones. All samples were diluted to the work concentration with the mobile phase and then filtered through a 0.45-mm filter membrane and degassed using an ultrasonic apparatus for 30 min immediately before use. The standards were also diluted in the mobile phase. All columns were from Phenomenex (Torrance, CA, USA) and were connected with a precolumn with the same packing (4.0 × 3.0 mm, 5 mm) from the same manufacturer. All volumetric glassware and analytical balances used were calibrated.
3. Results
At each sampling time, the visual appearance of the creams was also evaluated to verify their homogeneity and physical stability (data not shown). Throughout the whole study, no phenomena such as creaming, sedimentation, flocculation, coalescence, or phase separation were observed when the drug content was within the specifications.
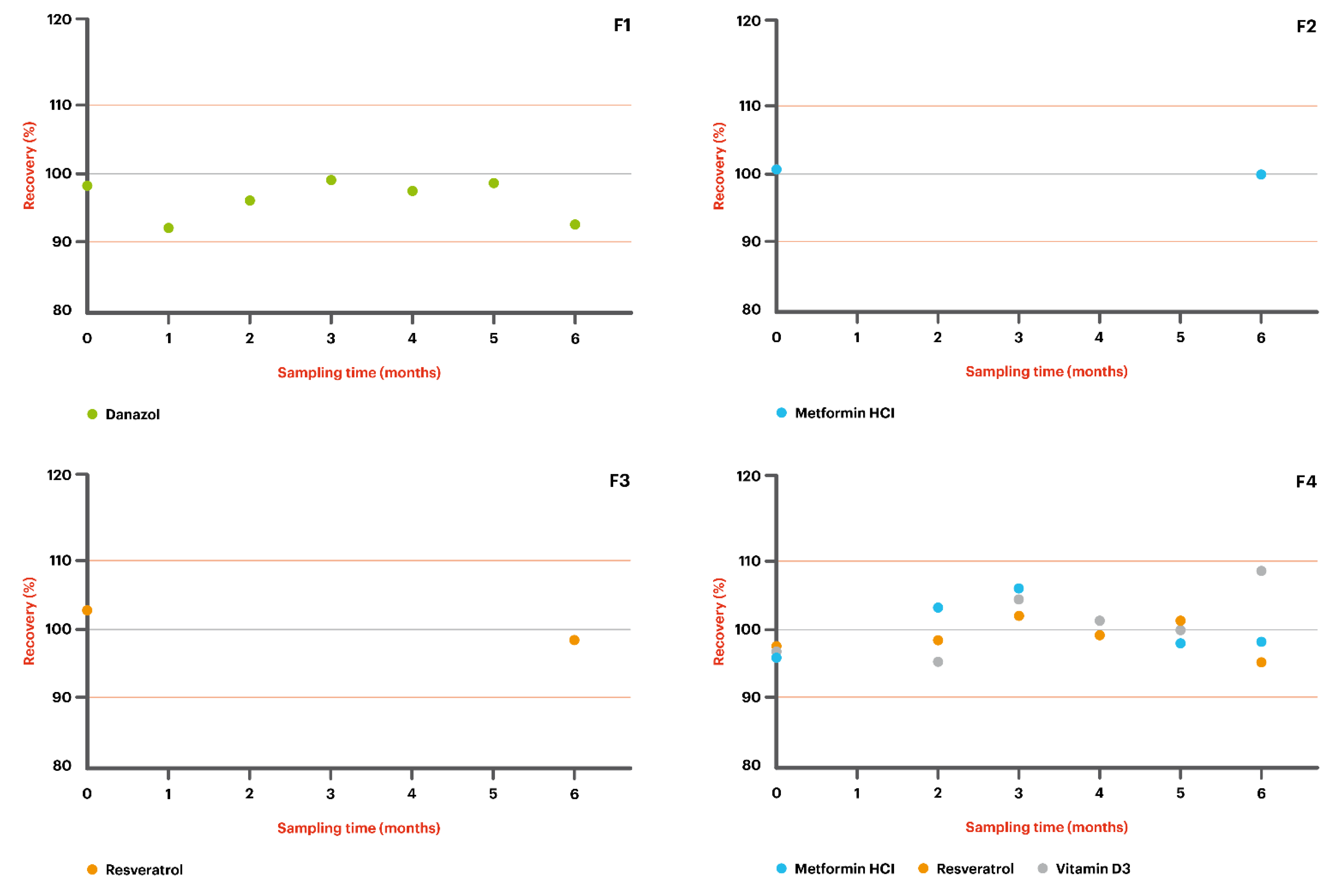
The chemical stability results are shown in Table 3 and Figure 1, expressed as the assay (in %). For the creams to be considered stable, the relative assay should lie within 90–110%.
In our study, a beyond-use date (BUD) of 6 months was observed for the formulations stored at room temperature. In the absence of stability information for a specific formulation, USP <795> (Pharmaceutical compounding—nonsterile preparations) can be used as a guideline, which advises a beyond-use date of no more than 30 days [19]. The long BUD of 180 days presented in this study offers an increased convenience for both the compounding pharmacist and the patient.
The lower and upper limits were set as 90% and 100% of the labeled concentrations, respectively. The system suitability was checked for all analyses, with a relative standard deviation lower than 2%.
4. Conclusions
We tested five formulations using Pentravan® or Pentravan® Plus:
- F1: Danazol 50 mg/g + MiodesinTM 85 mg/g in Pentravan®;
- F2: Metformin HCl 200 mg/g in Pentravan®;
- F3: Resveratrol 200 mg/g in Pentravan®;
- F4: Metformin HCl 100 mg/g + Resveratrol 100 mg/g + Vitamin D3 5000 IU in Pentravan®;
- F5: Metformin HCl 200 mg/g + Resveratrol 200 mg/g + Vitamin D3 5000 IU in Pentravan® Plus.
All the formulations presented a beyond-use date of at least 6 months. Thus, this study showed that the APIs were all compatible for 6 months with Pentravan® or Pentravan® Plus in the conditions described, reinforcing that both vehicles are compatible with a wide range of APIs from diverse pharmacological classes. These results validate APIs for use at various dosages in transdermal creams for drug administration, which confirms that both Pentravan® and Pentravan® Plus are an adequate choice for use by compounders.
Author Contributions
Conceptualization and methodology, C.Z. and S.T.; writing—original draft preparation and writing—review and editing, H.P., C.Z. and S.T. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Conflicts of Interest
The authors work for Fagron. The funders had no role in the design of the study; in the collection, analyses, or interpretation of the data; in the writing of the manuscript; or in the decision to publish the results.
References
- Prausnitz, M.R.; Langer, R. Transdermal drug delivery. Nat. Biotechnol. 2008, 26, 1261–1268. [Google Scholar] [CrossRef] [PubMed]
- Prausnitz, M.R.; Mitragotri, S.; Langer, R. Current status and future potential of transdermal drug delivery. Nat. Rev. Drug Discov. 2004, 3, 115–124. [Google Scholar] [CrossRef] [PubMed]
- Alkilani, A.; McCrudden, M.T.; Donnelly, R. Transdermal Drug Delivery: Innovative Pharmaceutical Developments Based on Disruption of the Barrier Properties of the Stratum Corneum. Pharmaceutics 2015, 7, 438–470. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paudel, K.S.; Milewski, M.; Swadley, C.L.; Brogden, N.K.; Ghosh, P.; Stinchcomb, A.L. Challenges and opportunities in dermal/transdermal delivery. Ther. Deliv. 2010, 1, 109–131. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ramadon, D.; McCrudden, M.T.C.; Courtenay, A.J.; Donnelly, R.F. Enhancement strategies for transdermal drug delivery systems: Current trends and applications. Drug Deliv. Transl. Res. 2021, 1–34. [Google Scholar] [CrossRef]
- Klepser, T.B.; Kelly, M.W. Metformin hydrochloride: An antihyperglycemic agent. Am. J. Heal. Pharm. 1997, 54, 893–903. [Google Scholar] [CrossRef]
- Araoye, E.F.; Thomas, J.A.L.; Aguh, C.U.; Dallas, M. CASE REPORT Hair regrowth in 2 patients with recalcitrant central centrifugal cicatricial alopecia after use of topical metformin. JAAD Case Rep. 2020, 6, 106–108. [Google Scholar] [CrossRef] [PubMed]
- Polonini, H.; Cândido, P.J.L.; Andrade, J.L.; Loures, S.; Raposo, N.R.; Brandão, M.A.F.; de Oliveira Ferreira, A. Transdermal Delivery of Metformin Hydrochloride from a Semisolid Vehicle. Int. J. Pharm. Compd. 2019, 23, 65–69. [Google Scholar] [PubMed]
- Carlyle, D.; Khader, T.; Lam, D.; Vadivelu, N.; Shiwlochan, D.; Yonghee, C. Endometriosis Pain Management: A Review. Curr. Pain Headache Rep. 2020, 24, 49. [Google Scholar] [CrossRef] [PubMed]
- Devalapally, H.; Silchenko, S.; Zhou, F.; McDade, J.; Goloverda, G.; Owen, A.; Hidalgo, I.J. Evaluation of a Nanoemulsion Formulation Strategy for Oral Bioavailability Enhancement of Danazol in Rats and Dogs. J. Pharm. Sci. 2013, 102, 3808–3815. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berretta, M.; Bignucolo, A.; Di Francia, R.; Comello, F.; Facchini, G.; Ceccarelli, M.; Iaffaioli, R.V.; Quagliariello, V.; Maurea, N. Resveratrol in Cancer Patients: From Bench to Bedside. Int. J. Mol. Sci. 2020, 21, 2945. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wen, S.; Zhang, J.; Yang, B.; Elias, P.M.; Man, M.-Q. Role of Resveratrol in Regulating Cutaneous Functions. Evid. Based Complement. Altern. Med. 2020, 2020, 2416837. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alsaqr, A.; Rasoully, M.; Musteata, F.M. Investigating transdermal delivery of vitamin D3. AAPS PharmSciTech 2015, 16, 963–972. [Google Scholar] [CrossRef] [PubMed]
- Umar, M.; Sastry, K.S.; Al Ali, F.; Al-Khulaifi, M.; Wang, E.; Chouchane, A.I. Vitamin D and the Pathophysiology of Inflammatory Skin Diseases. Skin Pharmacol. Physiol. 2018, 31, 74–86. [Google Scholar] [CrossRef] [PubMed]
- Lehman, P.A.; Raney, S.G. In vitro percutaneous absorption of ketoprofen and testosterone: Comparison of pluronic lecithin organogel vs. pentravan cream. Int. J. Pharm. Compd. 2012, 16, 248–252. [Google Scholar] [PubMed]
- Polonini, H.C.; Brandão, M.A.; Ferreira, A.O.; Ramos, C.; Raposo, N.R. Evaluation of percutaneous absorption performance for human female sexual steroids into pentravan cream. Int. J. Pharm. Compd. 2014, 18, 332–340. [Google Scholar] [PubMed]
- United States Pharmacopeial Convention. USP 40-NF 35 The United States Pharmacopeia and National Formulary; United States Pharmacopeial Convention, Inc.: Rockville, MD, USA, 2017. [Google Scholar]
- Council of Europe. Uniformity of dosage units. In European Pharmacopoeia 10.0; Council of Europe: Strasbourg, France, 2019; pp. 398–400. [Google Scholar]
- United States Pharmacopeia. <795> Pharmaceutical Compounding–Nonsterile Preparations. In United States Pharmacopeia; United States Pharmacopeial Convention, Inc.: Rockville, MD, USA, 2020. [Google Scholar]
Figure 1.
Stability of the selected APIs in Pentravan® or Pentravan® Plus. Red lines represent the lower and upper limits, corresponding to 90% and 110% of the labeled concentrations.
Figure 1.
Stability of the selected APIs in Pentravan® or Pentravan® Plus. Red lines represent the lower and upper limits, corresponding to 90% and 110% of the labeled concentrations.



{kind=link}
{kind=link}
Table 1.
The active pharmaceutical ingredients studied and their formulations.
| API | F1 | F2 | F3 | F4 | F5 | Pharmaceutical Action |
|---|---|---|---|---|---|---|
| Danazol | 50 mg | - | - | - | - | Androgen; treatment of endometriosis, fibrocystic breast disease, hereditary angioedema, and other conditions. |
| MiodesinTM | 85 mg | - | - | - | - | Natural anti-inflammatory; treatment of endometriosis; uterine leiomyomas; adenomyosis; inflammaging (chronic inflammation, in ageing, cardiovascular disease, and frailty. joint health); and other conditions. |
| Metformin HCl | - | 200 mg | - | 100 mg | 200 mg | Biguanide; treatment of diabetes mellitus. |
| Resveratrol | - | - | 200 mg | 100 mg | 200 mg | Polyphenolic phytoalexin; antioxidant. |
| Vitamin D3 | - | - | - | 5000 IU | 5000 IU | Vitamin; treatment and prevention of bone disorders and low levels of calcium or phosphate. |
| Pentravan® | q.s. 1 g | q.s. 1 g | q.s. 1 g | q.s. 1 g | - | Ready-to-use transdermal vehicle. |
| Pentravan® Plus | - | - | - | - | q.s. 1 g | Ready-to-use transdermal vehicle. |
F1 = danazol 50 mg/g + MiodesinTM 85 mg/g, F2 = metformin HCl 200 mg/g, F3 = resveratrol 200 mg/g, F4 = metformin HCl 100 mg/g + resveratrol 100 mg/g + vitamin D3 5000 IU/g, and F5 = metformin HCl 200 mg/g + resveratrol 200 mg/g + vitamin D3 5000 IU/g.
Table 2.
Chromatographic conditions used in the compatibility study.
| Active Pharmaceutical Ingredient | Mobile Phase Composition | Work Concentration (μg/mL)/Injection Volume (µL) | Column | Flux (mL/min) | Ultraviolet Detection Wavelength (nm) |
|---|---|---|---|---|---|
| F1 | 60 mL acetonitrile + 40 mL water | 400/5.0 | C18, 150 × 4.6 mm | 1.5 | 290 |
| F2 | 450 mL water + 0.25 g HeptaneSO3Na + 0.25 g NaCl + 0.6 g NaH2PO4 + 14 µL H3PO4 + 50 mL acetonitrile | 1000/3.0 | C18, 150 × 4.6 mm, at 30 °C | 2.0 | 245 |
| F3 | 400 mL 50 mM KH2PO4 + 100 mL acetonitrile | 2000/4.0 | C18, 300 × 4.6 mm | 2.0 | 350 |
| F4/F5 * | 90 mL methanol + 10 mL isopropyl alcohol | 200/10.0 | C18, 250 × 4.6 mm | 2.0 | 269 |
F1 = danazol 50 mg/g + MiodesinTM 85 mg/g, F2 = metformin HCl 200 mg/g, F3 = resveratrol 200 mg/g, F4 = metformin HCl 100 mg/g + resveratrol 100 mg/g + vitamin D3 5000 IU/g, and F5 = metformin HCl 200 mg/g + resveratrol 200 mg/g + vitamin D3 5000 IU/g. * For F4/F5, the APIs were quantified separately. For metformin HCl and resveratrol, the methods used were the same as for F2 and F3, respectively.
Table 3.
Stability of the active pharmaceutical ingredients in Pentravan® or Pentravan® Plus.
| Elapsed Time (Days) | % Assay (Room Temperature, 20–25 °C) |
|---|---|
| Danazol 50 mg/g—compounded in combination with Miodesin 85mg/g in Pentravan® | |
| T = 0 | 98.5 |
| T = 32 | 92.7 |
| T = 62 | 96.6 |
| T = 90 | 99.4 |
| T = 120 | 97.7 |
| T = 153 | 98.8 |
| T = 183 | 93.0 |
| Metformin HCl 200 mg/g—in Pentravan® | |
| T = 0 | 100.5 |
| T = 176 | 100.1 |
| Resveratrol 200 mg/g—in Pentravan® | |
| T = 0 | 102.8 |
| T = 178 | 98.7 |
| Metformin HCl 100 mg/g—compounded in combination with Resveratrol 100mg/g and Vitamin D3 5000 IU in Pentravan® | |
| T = 0 | 95.8 |
| T = 63 | 103.1 |
| T = 89 | 105.7 |
| T = 118 | 99.4 |
| T = 154 | 97.9 |
| T = 183 | 98.1 |
| Resveratrol 100mg/g—compounded in combination with Metformin HCl 100 mg/g and Vitamin D3 5000 IU in Pentravan® | |
| T = 0 | 97.4 |
| T = 63 | 98.4 |
| T = 89 | 102.0 |
| T = 118 | 99.4 |
| T = 154 | 101.0 |
| T = 183 | 95.5 |
| Vitamin D3 5000 IU—compounded in combination with Metformin HCl 100 mg/g and Resveratrol 100mg/g in Pentravan® | |
| T = 0 | 96.7 |
| T = 63 | 95.3 |
| T = 89 | 104.5 |
| T = 118 | 101.1 |
| T = 154 | 99.9 |
| T = 183 | 108.4 |
| Metformin HCl 200 mg/g—compounded in combination with Resveratrol 200 mg/g and Vitamin D3 5000 IU in Pentravan® Plus | |
| T = 0 | 93.7 |
| T = 63 | 99.9 |
| T = 89 | 103.0 |
| T = 125 | 103.6 |
| T = 154 | 100.1 |
| T = 187 | 98.9 |
| Resveratrol 200 mg/g—compounded in combination with Metformin HCl 200 mg/g and Vitamin D3 5000 IU in Pentravan® Plus | |
| T = 0 | 95.3 |
| T = 63 | 95.8 |
| T = 89 | 101.8 |
| T = 125 | 100.5 |
| T = 154 | 100.6 |
| T = 187 | 93.1 |
| Vitamin D3 5000 IU—compounded in combination with Metformin HCl 200 mg/g and Resveratrol 200 mg/g in Pentravan® Plus | |
| T = 0 | 94.6 |
| T = 63 | 92.7 |
| T = 89 | 102.8 |
| T = 125 | 98.2 |
| T = 154 | 99.8 |
| T = 187 | 97.3 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Polonini, H.; Taylor, S.; Zander, C. Compatibility of Different Formulations in Pentravan® and Pentravan® Plus for Transdermal Drug Delivery. Sci. Pharm. 2021, 89, 51. https://0-doi-org.brum.beds.ac.uk/10.3390/scipharm89040051
AMA Style
Polonini H, Taylor S, Zander C. Compatibility of Different Formulations in Pentravan® and Pentravan® Plus for Transdermal Drug Delivery. Scientia Pharmaceutica. 2021; 89(4):51. https://0-doi-org.brum.beds.ac.uk/10.3390/scipharm89040051
Chicago/Turabian StylePolonini, Hudson, Sarah Taylor, and Clark Zander. 2021. "Compatibility of Different Formulations in Pentravan® and Pentravan® Plus for Transdermal Drug Delivery" Scientia Pharmaceutica 89, no. 4: 51. https://0-doi-org.brum.beds.ac.uk/10.3390/scipharm89040051