
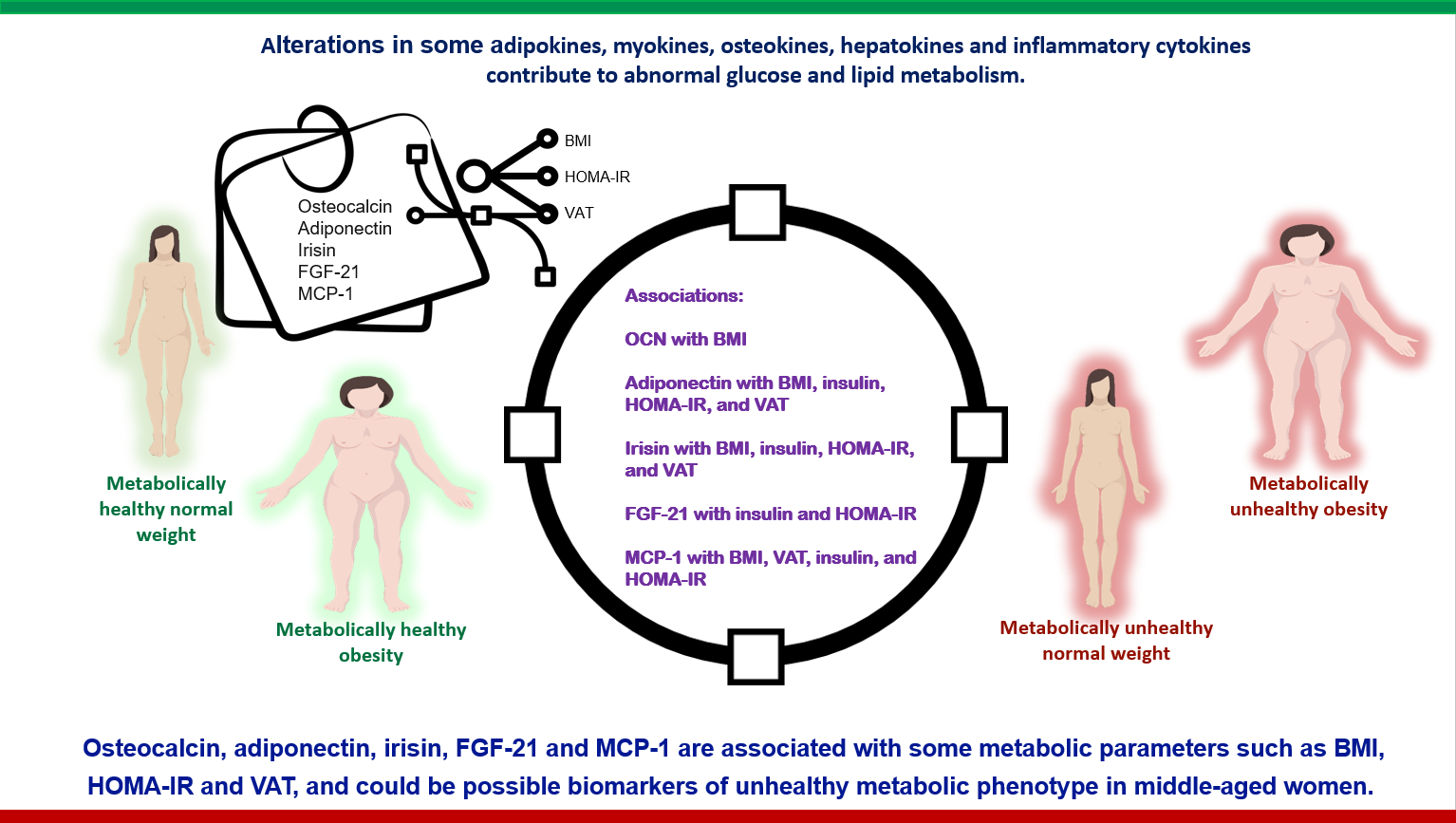
Pattern of Adiponectin, Osteocalcin, Irisin, FGF-21, and MCP-1 According to the Body Size Phenotype: Could They Be Markers of Metabolic Health in Mexican-Mestizo Middle-Aged Women?

 , , , ,
, , , , 
Abstract
:
1. Introduction
2. Results
2.1. Clinical and Biochemical Characteristics of Participants
2.2. Differences in Adiponectin, OCN, Irisin, FGF-21 and MCP-1 According to the Body Size Phenotype in Middle-Aged Women
2.2.1. MHNW vs. MUNW Phenotype
2.2.2. MHNW vs. MHO Phenotype
2.2.3. MHNW vs. MUO Phenotype
2.2.4. MUNW vs. MUO Phenotype
2.2.5. MHO vs. MUO Phenotype
2.3. Associations of Adiponectin, OCN, Irisin, FGF-21 and MCP-1, BMI, VAT, Insulin and HOMA-IR
2.4. Adiponectin, OCN, Irisin, FGF-21 and MCP-1 According to Menopausal Status
2.5. Factors Associated with a Metabolic Phenotype
3. Discussion
4. Materials and Methods
4.1. Study Design and Patients
4.2. Clinical Evaluation
4.2.1. Anthropometry
4.2.2. Clinical Characteristics and Definitions
4.3. Phenotypes
4.4. Biochemical Evaluation
4.5. Statistical Analysis
4.6. Ethics
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| BMI | body mass index |
| CRP | C-reactive protein |
| CV | coefficients of variation |
| CVD | cardiovascular disease |
| FFA | free fatty acid |
| FGF-21 | fibroblast growth factor-21 |
| FNDC5 | fibronectin type III domain-containing 5 |
| HDL-C | high density cholesterol |
| HOMA-IR | homeostasis model assessment of insulin resistance |
| IL-1β | interleukin-1β |
| IL-6 | interleukin-6 |
| IQR | interquartile range |
| LDL-C | low density cholesterol |
| MCP-1 | monocyte chemoattractant protein-1 |
| MHNW | metabolically healthy normal weight |
| MHO | metabolically healthy obesity |
| MUNW | metabolically unhealthy normal weight |
| MUO | metabolically unhealthy obesity |
| OCN | osteocalcin |
| TC | total cholesterol |
| TNF-α | tumor necrosis alpha |
| ucOCN | undercarboxylated osteocalcin |
| VAT | visceral adipose tissue |
References
- Shi, J.; Fan, J.; Su, Q.; Yang, Z. Cytokines and Abnormal Glucose and Lipid Metabolism. Front. Endocrinol. 2019, 10, 703. [Google Scholar] [CrossRef] [PubMed]
- Raschke, S.; Eckel, J. Adipo-myokines: Two sides of the same coin-mediators of inflammation and mediators of exercise. Mediat. Inflamm. 2013, 2013, 320724. [Google Scholar] [CrossRef] [PubMed]
- Kirk, B.; Feehan, J.; Lombardi, G.; Duque, G. Muscle, Bone, and Fat Crosstalk: The Biological Role of Myokines, Osteokines, and Adipokines. Curr. Osteoporos Rep. 2020, 18, 388–400. [Google Scholar] [CrossRef] [PubMed]
- Dirckx, N.; Moorer, M.C.; Clemens, T.L.; Riddle, R.C. The role of osteoblasts in energy homeostasis. Nat. Rev. Endocrinol. 2019, 15, 651–665. [Google Scholar] [CrossRef] [PubMed]
- Landecho, M.F.; Tuero, C.; Valentí, V.; Bilbao, I.; de la Higuera, M.; Frühbeck, G. Relevance of Leptin and Other Adipokines in Obesity-Associated Cardiovascular Risk. Nutrients 2019, 11, 2664. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakamura, K.; Fuster, J.J.; Walsh, K. Adipokines: A link between obesity and cardiovascular disease. J. Cardiol. 2014, 63, 250–259. [Google Scholar] [CrossRef] [Green Version]
- Basurto, L.; Gregory, M.A.; Hernández, S.B.; Sánchez-Huerta, L.; Martínez, A.D.; Manuel-Apolinar, L.; Avelar, F.J.; Alonso, L.A.M.; Sánchez-Arenas, R. Monocyte chemoattractant protein-1 (MCP-1) and fibroblast growth factor-21 (FGF-21) as biomarkers of subclinical atherosclerosis in women. Exp. Gerontol. 2019, 124, 110624. [Google Scholar] [CrossRef] [PubMed]
- Basurto-Acevedo, L.; Saucedo-García, R.; Vázquez-Martínez, A.; Cruz-García, M.; Valle-Hernández, M.M.; Rosales-Cruz, E.; Sánchez-Arenas, R. Relación entre la actividad ósea y el metabolismo en el adulto mayor [Relationship between bone remodeling and metabolism in the elderly]. Rev. Med. Inst. Mex Seguro Soc. 2018, 56 (Suppl. S1), S6–S11. [Google Scholar]
- Blüher, M. Metabolically Healthy Obesity. Endocr. Rev. 2020, 41, 405–420. [Google Scholar] [CrossRef] [Green Version]
- Schulze, M.B. Metabolic health in normal-weight and obese individuals. Diabetologia 2019, 62, 558–566. [Google Scholar] [CrossRef] [Green Version]
- Neeland, I.J.; Poirier, P.; Després, J.P. Cardiovascular and Metabolic Heterogeneity of Obesity: Clinical Challenges and Implications for Management. Circulation 2018, 137, 1391–1406. [Google Scholar] [CrossRef]
- Ferreira, F.G.; Juvanhol, L.L.; da Silva, D.C.G.; Longo, G.Z. Visceral adiposity index is a better predictor of unhealthy metabolic phenotype than traditional adiposity measures: Results from a population-based study. Public Health Nutr. 2019, 22, 1545–1554. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gao, M.; Lv, J.; Yu, C.; Guo, Y.; Bian, Z.; Yang, R.; Du, H.; Yang, L.; Chen, Y.; Li, Z.; et al. China Kadoorie Biobank (CKB) Collaborative Group. Metabolically healthy obesity, transition to unhealthy metabolic status, and vascular disease in Chinese adults: A cohort study. PLoS Med. 2020, 17, e1003351. [Google Scholar] [CrossRef] [PubMed]
- Hwang, Y.C.; Hayashi, T.; Fujimoto, W.Y.; Kahn, S.E.; Leonetti, D.L.; McNeely, M.J.; Boyko, E.J. Visceral abdominal fat accumulation predicts the conversion of metabolically healthy obese subjects to an unhealthy phenotype. Int. J. Obes. 2015, 39, 1365–1370. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Foresta, C.; Strapazzon, G.; De Toni, L.; Gianesello, L.; Calcagno, A.; Pilon, C.; Plebani, M.; Vettor, R. Evidence for osteocalcin production by adipose tissue and its role in human metabolism. J. Clin. Endocrinol. Metab. 2010, 95, 3502–3506. [Google Scholar] [CrossRef] [Green Version]
- Liu, X.; Liu, Y.; Mathers, J.; Cameron, M.; Levinger, I.; Yeap, B.B.; Lewis, J.R.; Brock, K.E.; Brennan-Speranza, T.C. Osteocalcin and measures of adiposity: A systematic review and meta-analysis of observational studies. Arch. Osteoporos. 2020, 15, 145. [Google Scholar] [CrossRef] [PubMed]
- Kord-Varkaneh, H.; Djafarian, K.; Khorshidi, M.; Shab-Bidar, S. Association between serum osteocalcin and body mass index: A systematic review and meta-analysis. Endocrine 2017, 58, 24–32. [Google Scholar] [CrossRef] [PubMed]
- García-Martín, A.; Cortés-Berdonces, M.; Luque-Fernández, I.; Rozas-Moreno, P.; Quesada-Charneco, M.; Muñoz-Torres, M. Osteocalcin as a marker of metabolic risk in healthy postmenopausal women. Menopause 2011, 18, 537–541. [Google Scholar] [CrossRef] [PubMed]
- Aguilar-Salinas, C.A.; García, E.G.; Robles, L.; Riaño, D.; Ruiz-Gomez, D.G.; García-Ulloa, A.C.; Melgarejo, M.A.; Zamora, M.; Guillen-Pineda, L.E.; Mehta, R.; et al. High adiponectin concentrations are associated with the metabolically healthy obese phenotype. J. Clin. Endocrinol. Metab. 2008, 93, 4075–4079. [Google Scholar] [CrossRef]
- Liu, Z.; Liang, S.; Que, S.; Zhou, L.; Zheng, S.; Mardinoglu, A. Meta-Analysis of Adiponectin as a Biomarker for the Detection of Metabolic Syndrome. Front. Physiol. 2018, 9, 1238. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perakakis, N.; Triantafyllou, G.A.; Fernández-Real, J.M.; Huh, J.Y.; Park, K.H.; Seufert, J.; Mantzoros, C.S. Physiology and role of irisin in glucose homeostasis. Nat. Rev. Endocrinol. 2017, 13, 324–337. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leung, W.K.C.; Yu, A.P.; Lai, C.W.K.; Siu, P.M. Association of Markers of Proinflammatory Phenotype and Beige Adipogenesis with Metabolic Syndrome in Chinese Centrally Obese Adults. J. Diabetes Res. 2018, 2018, 8956509. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jia, J.; Yu, F.; Wei, W.P.; Yang, P.; Zhang, R.; Sheng, Y.; Shi, Y.Q. Relationship between circulating irisin levels and overweight/obesity: A meta-analysis. World J. Clin. Cases 2019, 7, 1444–1455. [Google Scholar] [CrossRef] [PubMed]
- Zhou, K.; Qiao, X.; Cai, Y.; Li, A.; Shan, D. Lower circulating irisin in middle-aged and older adults with osteoporosis: A systematic review and meta-analysis. Menopause 2019, 26, 1302–1310. [Google Scholar] [CrossRef] [PubMed]
- Hale, C.; Chen, M.M.; Stanislaus, S.; Chinookoswong, N.; Hager, T.; Wang, M.; Véniant, M.M.; Xu, J. Lack of overt FGF21 resistance in two mouse models of obesity and insulin resistance. Endocrinology 2012, 153, 69–80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fisher, F.M.; Chui, P.C.; Antonellis, P.J.; Bina, H.A.; Kharitonenkov, A.; Flier, J.S.; Maratos-Flier, E. Obesity is a fibroblast growth factor 21 (FGF21)-resistant state. Diabetes 2010, 59, 2781–2789. [Google Scholar] [CrossRef] [Green Version]
- Jimenez, V.; Jambrina, C.; Casana, E.; Sacristan, V.; Muñoz, S.; Darriba, S.; Rodó, J.; Mallol, C.; Garcia, M.; León, X.; et al. FGF21 gene therapy as treatment for obesity and insulin resistance. EMBO Mol. Med. 2018, 10, e8791. [Google Scholar] [CrossRef]
- Westerbacka, J.; Cornér, A.; Kolak, M.; Makkonen, J.; Turpeinen, U.; Hamsten, A.; Fisher, R.M.; Yki-Järvinen, H. Insulin regulation of MCP-1 in human adipose tissue of obese and lean women. Am. J. Physiol. Endocrinol. Metab. 2008, 294, E841–E845. [Google Scholar] [CrossRef]
- Kim, C.S.; Park, H.S.; Kawada, T.; Kim, J.H.; Lim, D.; Hubbard, N.E.; Kwon, B.S.; Erickson, K.L.; Yu, R. Circulating levels of MCP-1 and IL-8 are elevated in human obese subjects and associated with obesity-related parameters. Int. J. Obes. 2006, 30, 1347–1355. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, T.H.; Jeon, W.S.; Han, K.J.; Lee, S.Y.; Kim, N.H.; Chae, H.B.; Jang, C.M.; Yoo, K.M.; Park, H.J.; Lee, M.K.; et al. Comparison of Serum Adipocytokine Levels according to Metabolic Health and Obesity Status. Endocrinol. Metab. 2015, 30, 185–194. [Google Scholar] [CrossRef]
- Wang, B.; Zhuang, R.; Luo, X.; Yin, L.; Pang, C.; Feng, T.; You, H.; Zhai, Y.; Ren, Y.; Zhang, L.; et al. Prevalence of Metabolically Healthy Obese and Metabolically Obese but Normal Weight in Adults Worldwide: A Meta-Analysis. Horm. Metab. Res. 2015, 47, 839–845. [Google Scholar] [CrossRef] [PubMed]
- Gomez-Huelgas, R.; Narankiewicz, D.; Villalobos, A.; Wärnberg, J.; Mancera-Romero, J.; Cuesta, A.L.; Tinahones, F.J.; Bernal-Lopez, M.R. Prevalence of metabolically discordant phenotypes in a Mediterranean population–The IMAP study. Endocr. Pract. 2013, 19, 758–768. [Google Scholar] [CrossRef] [PubMed]
- Shamah-Levy, T.; Vielma-Orozco, E.; Heredia-Hernández, O.; Romero-Martínez, M.; Mojica-Cuevas, J.; Cuevas-Nasu, L.; Santaella-Castell, J.A.; Rivera-Dommarco, J. Encuesta Nacional de Salud y Nutrición 2018–19: Resultados Nacionales; Instituto Nacional de Salud Pública: Cuernavaca, Mexico, 2020. [Google Scholar]
- Karelis, A.D.; Brochu, M.; Rabasa-Lhoret, R. Can we identify metabolically healthy but obese individuals (MHO)? Diabetes Metab. 2004, 30, 569–572. [Google Scholar] [CrossRef]
- Matthews, D.R.; Hosker, J.P.; Rudenski, A.S.; Naylor, B.A.; Treacher, D.F.; Turner, R.C. Homeostasis model assessment: Insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 1985, 28, 412–419. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
| Characteristics | Results |
|---|---|
| Age; (years) | 52.2 ± 5.8 |
| Postmenopausal; % (n=) | 67.9 (180) |
| BMI; (kg/m2) | 28.8 ± 4.9 |
| Phenotype; % (n=) | MHNW: 6 (16) MUNW: 57 (151) MHO: 1.9 (5) MUO: 35.1 (93) |
| VAT; (cm2) | 127 (98–167) |
| Osteocalcin; (ng/mL) | 5.2 (3.5–7.7) |
| Adiponectin; (µg/mL) | 11.7 (7.8–16.0) |
| Irisin; (ng/mL) | 495.4 (267.9–713.2) |
| FGF-21; (pg/mL) | 205.0 (73.8–353.0) |
| MCP-1; (pg/mL) | 21.7 (8.1–37.4) |
| Glucose; (mg/dL) | 85 (77–95) |
| Insulin; (mIU/L) | 17 (13–24) |
| HOMA-IR | 3.5 (2.6–5.3) |
| Total cholesterol; (mg/dL) | 225.5 (200.5–267.75) |
| LDL-C; (mg/dL) | 141.8 (118.4–170.6) |
| HDL-C; (mg/dL) | 53.5 (45–63) |
| Triglycerides; (mg/dL) | 142 (111–198) |
| MHNW (n = 16) | MUNW (n = 151) | MHO (n = 5) | MUO (n = 93) | MHNW vs. MUNW p Value | MHNW vs. MHO p Value | MHNW vs. MUO p Value | MUNW vs. MUO p Value | MHO vs. MUO p Value | |
|---|---|---|---|---|---|---|---|---|---|
| Age (years) | 51.4 ± 7.1 | 52.7 ± 5.7 | 53 ± 5.3 | 51.6 ± 5.6 | 0.380 | 0.375 | 0.875 | 0.14 | 0.26 |
| VAT; (cm2) | 91.5 (68–123) | 105 (87–125) | 195.6 (155–215) | 201 (153–227) | 0.112 | 0.080 | 0.0001 * | 0.0001 * | 0.001 * |
| Osteocalcin; (ng/mL) | 3.4 (2.5–5.5) | 5.8 (3.7–8.4) | 5.2 (3.8–6.8) | 4.7 (3.4–7.0) | 0.011 * | 0.011 * | 0.157 | 0.001 * | 0.761 |
| Adiponectin; (µg/mL) | 16.1 (11.2–21.7) | 12.5 (7.9–16.0) | 14.6 (9.8–29.1) | 10.1 (7.6–13.3) | 0.002 * | 0.002 * | 0.0001 * | 0.03 * | 0.155 |
| Irisin; (ng/mL) | 464 (186–559) | 348.8 (201.4–660) | 649 (270–868) | 676 (503–787) | 0.909 | 0.413 | 0.0001 * | 0.0001 * | 0.942 |
| FGF-21; (pg/mL) | 370 (315–851) | 201 (70–335) | 195 (194–197) | 162 (21.8–229) | 0.067 | 0.024 * | 0.004 * | 0.30 | 0.279 |
| MCP-1; (pg/mL) | 15.9 (4.3–43.5) | 15.8 (7.7–34.2) | 25.1 (18.5–46.5) | 38.6 (32.7–52.8) | 0.620 | 0.756 | 0.291 | 0.0001 * | 0.627 |
| Glucose; (mg/dL) | 74 (64–85) | 83 (77–91) | 77 (74–91) | 89 (79.5–98.5) | 0.003 * | 0.004 * | 0.0001 * | 0.007 * | 0.121 |
| Insulin; (mIU/L) | 12.1 (10–13.2) | 15.8 (12.6–20.5) | 22.5 (12.4–34.4) | 22.5 (17.9–30.2) | 0.0001 * | 0.0001 * | 0.0001 * | 0.0001 * | 0.62 |
| HOMA-IR | 2.14 (1.5–2.6) | 3.2 (2.4–4.7) | 4.2 (2.2–7.9) | 4.9 (3.7–7.4) | 0.0001 * | 0.0001 * | 0.0001 * | 0.0001 * | 0.342 |
| Total cholesterol; (mg/dL) | 186 (175–190) | 230 (211–275) | 165 (124.5–178.5) | 229 (203–262) | 0.0001 * | 0.0001 * | 0.0001 * | 0.237 | 0.001 * |
| LDL-C; (mg/dL) | 95 (87–107) | 145 (124–178) | 62.6 (54.2–92.6) | 147 (124–179) | 0.0001 * | 0.0001 * | 0.0001 * | 0.65 | 0.001 * |
| HDL-C; (mg/dL) | 67 (54–72) | 55 (45–63) | 63.0 (47.5–71.0) | 49 (41–59) | 0.002 * | 0.002 * | 0.0001 * | 0.01 * | 0.09 * |
| Triglycerides; (mg/dL) | 109 (80–125) | 145 (109–198) | 121 (88.5–138) | 154 (121–209) | 0.003 * | 0.003 * | 0.0001 * | 0.20 | 0.056 * |
| MHNW vs. MUNW OR (95%CI) | MHNW vs. MHO OR (95%CI) | MHNW vs. MUO OR (95%CI) | MUNW vs. MUO OR (95%CI) | |
|---|---|---|---|---|
| Osteocalcin; (ng/mL) | 1.4 (1.06–1.81) | 1.4 (1.07–1.84) | NS | NS |
| Adiponectin; (µg/mL) | 0.9 (0.84–0.96) | 0.9 (0.84–0.96) | NS | NS |
| Irisin; (ng/mL) | NS | NS | 1.01 (1.001–1.01) | 1.007 (1.003–1.011) |
| MCP-1; (pg/mL) | NS | NS | NS | 1.044 (1.008–1.083) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Balcázar-Hernandez, L.; Basurto, L.; Manuel-Apolinar, L.; Vega-García, S.; Basurto-Acevedo, N.; Martínez-Murillo, C.; Sánchez-Arenas, R. Pattern of Adiponectin, Osteocalcin, Irisin, FGF-21, and MCP-1 According to the Body Size Phenotype: Could They Be Markers of Metabolic Health in Mexican-Mestizo Middle-Aged Women? Metabolites 2021, 11, 771. https://0-doi-org.brum.beds.ac.uk/10.3390/metabo11110771
Balcázar-Hernandez L, Basurto L, Manuel-Apolinar L, Vega-García S, Basurto-Acevedo N, Martínez-Murillo C, Sánchez-Arenas R. Pattern of Adiponectin, Osteocalcin, Irisin, FGF-21, and MCP-1 According to the Body Size Phenotype: Could They Be Markers of Metabolic Health in Mexican-Mestizo Middle-Aged Women? Metabolites. 2021; 11(11):771. https://0-doi-org.brum.beds.ac.uk/10.3390/metabo11110771
Chicago/Turabian StyleBalcázar-Hernandez, Lourdes, Lourdes Basurto, Leticia Manuel-Apolinar, Sara Vega-García, Norma Basurto-Acevedo, Carlos Martínez-Murillo, and Rosalinda Sánchez-Arenas. 2021. "Pattern of Adiponectin, Osteocalcin, Irisin, FGF-21, and MCP-1 According to the Body Size Phenotype: Could They Be Markers of Metabolic Health in Mexican-Mestizo Middle-Aged Women?" Metabolites 11, no. 11: 771. https://0-doi-org.brum.beds.ac.uk/10.3390/metabo11110771