
Hematological, Micro-Rheological, and Metabolic Changes Modulated by Local Ischemic Pre- and Post-Conditioning in Rat Limb Ischemia-Reperfusion

 , and
, and
Abstract
:1. Introduction
2. Results
2.1. Hematological Parameters
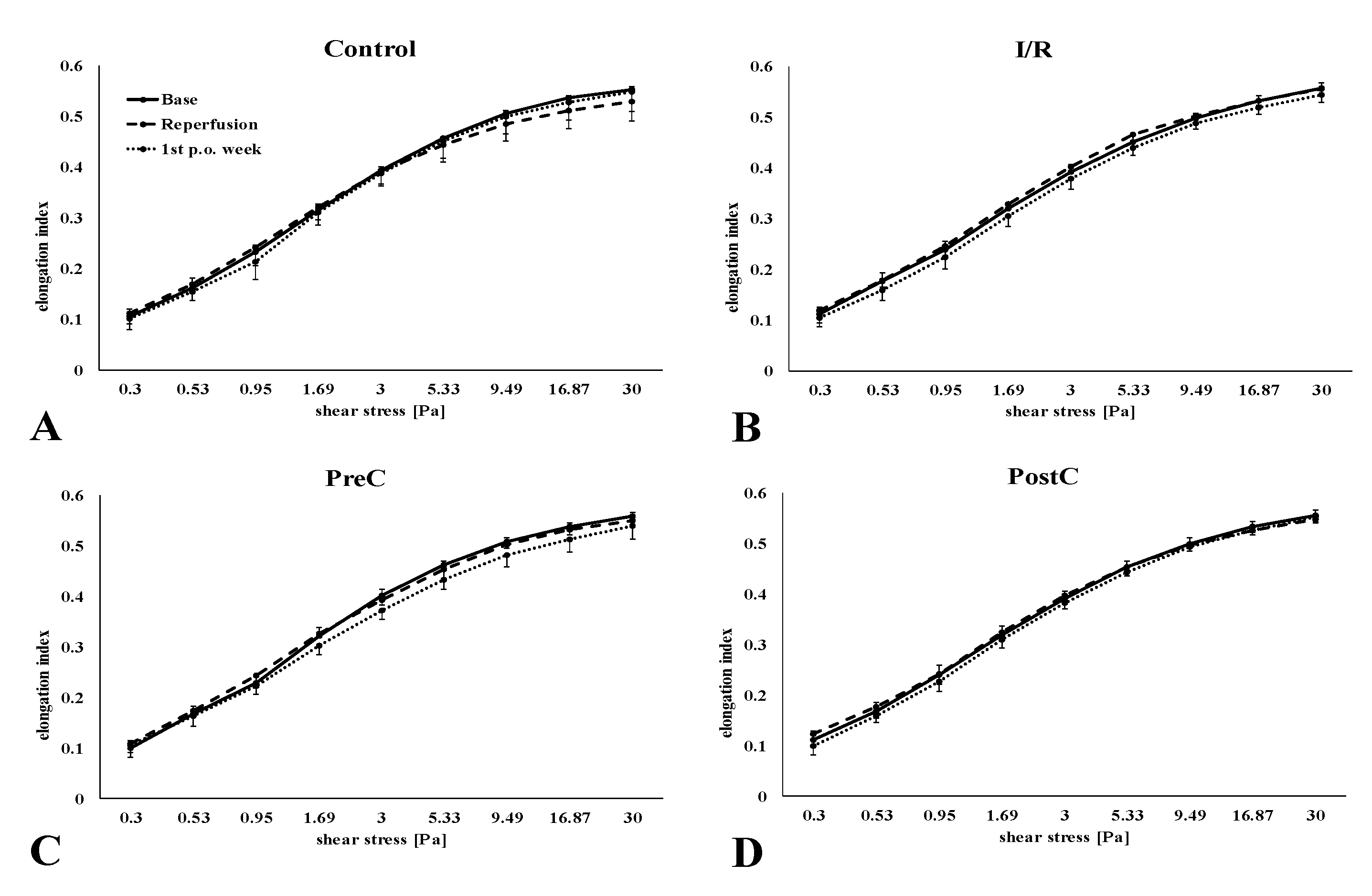
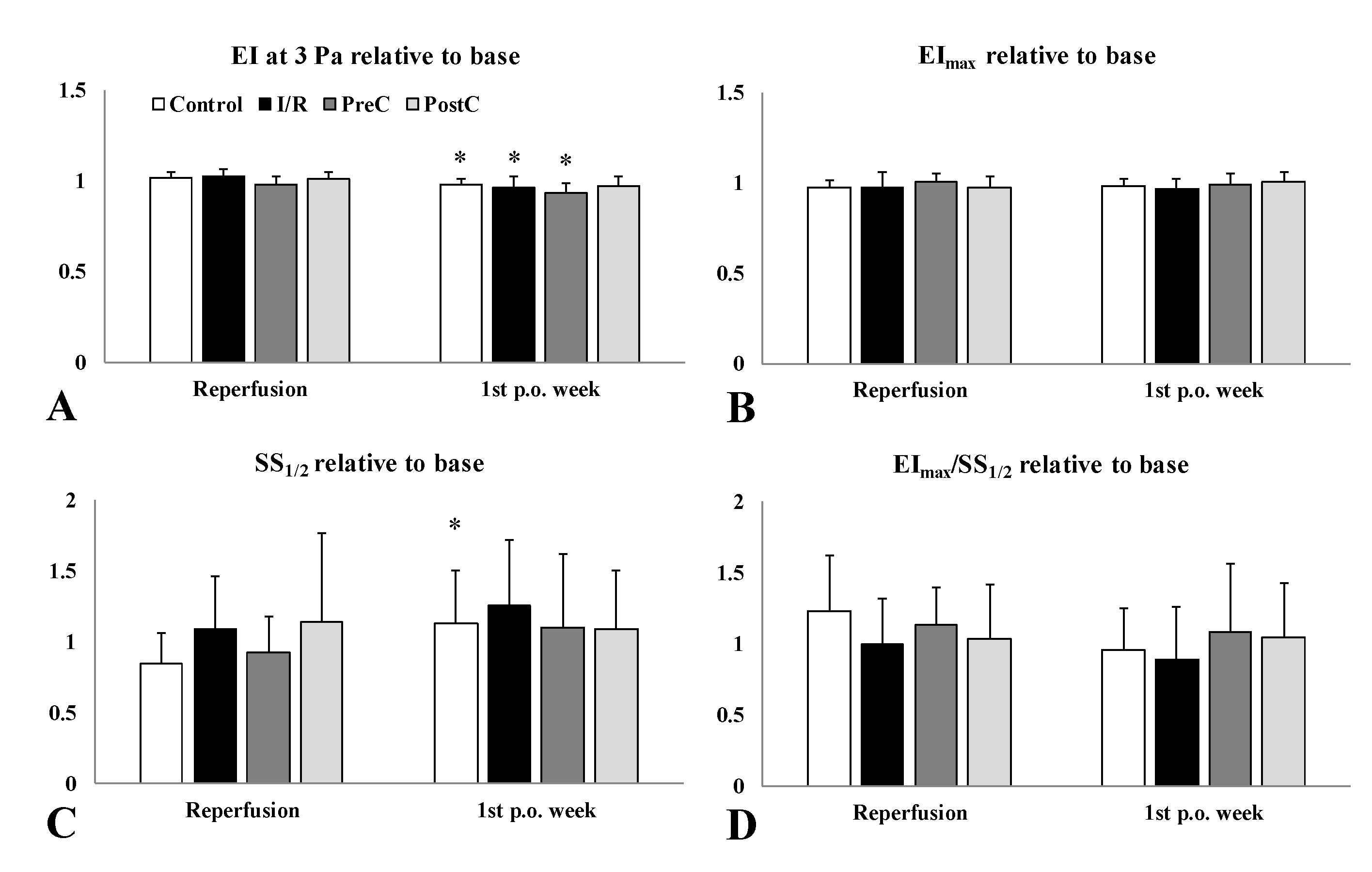
2.2. Red Blood Cell Deformability
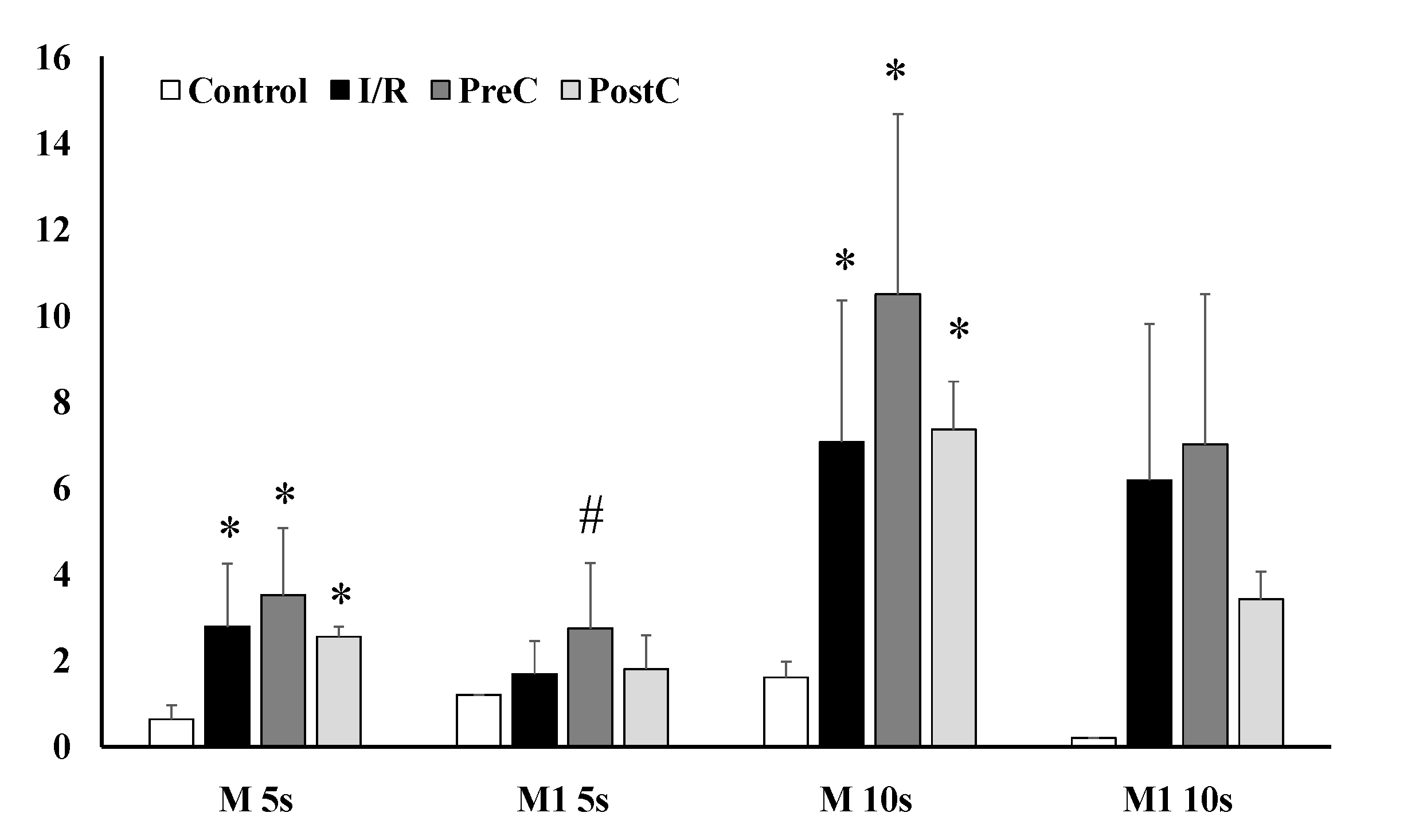
2.3. Red Blood Cell Aggregation
2.4. Blood Gases, Acid-Base Parameters, Electrolytes, and Metabolites
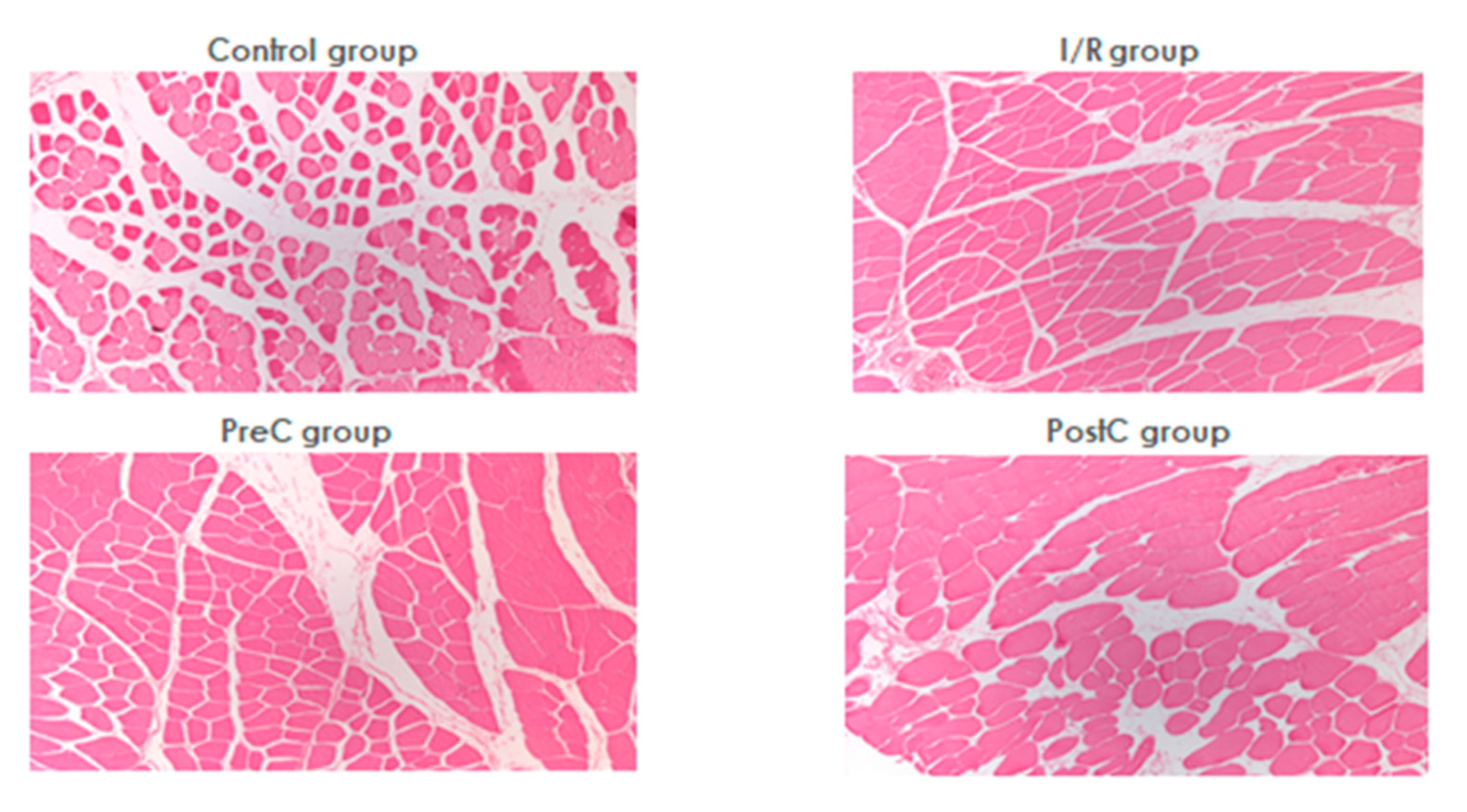
2.5. Histology
3. Discussion
4. Materials and Methods
4.1. Experimental Animals
4.2. Operative Techniques and Sampling Protocol
- I.
- Control (C) group (n = 8, 320.4 ± 9 g): besides the common carotid artery cannulation, no other intervention was performed;
- II.
- Ischemia-reperfusion (I/R) group (n = 7, 376.4 ± 42.4 g): unilateral hind limb ischemia was induced by tourniquet application around the thigh, below the right inguinal region. After 120-min ischemia the tourniquet was completely released to allow full reperfusion;
- III.
- Pre-conditioned (PreC) group (n = 8, 388.6 ± 39.1 g): three cycles of 10-min ischemia and reperfusion (by tightening then releasing the tourniquet, alternately) was applied before the prolonged ischemia, as described in the I/R group;
- IV.
- Post-conditioned (PostC) group (n = 7, 386.7 ± 46 g): the same three cycles of ischemia-reperfusion were introduced at the onset of the reperfusion, after 120-min ischemia as described in the I/R group.
4.3. Laboratory Methods
4.4. Histology
4.5. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Santistevan, J.R. Acute limb ischemia: An emergency medicine approach. Emerg. Med. Clin. N. Am. 2017, 35, 889–909. [Google Scholar] [CrossRef]
- Olinic, D.M.; Stanek, A.; Tataru, D.A.; Homorodean, C.; Olinic, M. Acute limb ischemia: An update on diagnosis and management. J. Clin. Med. 2019, 8, 1215. [Google Scholar] [CrossRef] [Green Version]
- Naito, H.; Nojima, T.; Fujisaki, N.; Tsukahara, K.; Yamamoto, H.; Yamada, T.; Aokage, T.; Yumoto, T.; Osako, T.; Nakao, A. Therapeutic strategies for ischemia reperfusion injury in emergency medicine. Acute Med. Surg. 2020, 7, e501. [Google Scholar] [CrossRef] [Green Version]
- Natarajan, B.; Patel, P.; Mukherjee, A. Acute lower limb ischemia-etiology, pathology, and management. Int. J. Angiol. 2020, 29, 168–174. [Google Scholar] [CrossRef]
- Walker, A.C.; Johnson, N.J. Critical care of the post-cardiac arrest patient. Cardiol. Clin. 2018, 36, 419–428. [Google Scholar] [CrossRef]
- De Groot, H.; Rauen, U. Ischemia-reperfusion injury: Processes in pathogenetic networks: A review. Transplant. Proc. 2007, 39, 481–484. [Google Scholar] [CrossRef]
- Mustoe, T. Understanding chronic wounds: A unifying hypothesis on their pathogenesis and implications for therapy. Am. J. Surg. 2004, 187, 65S–70S. [Google Scholar] [CrossRef]
- Eckert, P.; Schnackerz, K. Ischemic tolerance of human skeletal muscle. Ann. Plast. Surg. 1991, 26, 77–84. [Google Scholar] [CrossRef]
- Blaisdell, F.W. The pathophysiology of skeletal muscle ischemia and the reperfusion syndrome: A review. Cardiovasc. Surg. 2002, 10, 620–630. [Google Scholar] [CrossRef]
- Eltzschig, H.; Eckle, T. Ischemia and reperfusion—From mechanism to translation. Nat. Med. 2011, 17, 1391–1401. [Google Scholar] [CrossRef] [Green Version]
- Gillani, S.; Cao, J.; Suzuki, T.; Hak, D.J. The effect of ischemia reperfusion injury on skeletal muscle. Injury 2012, 43, 670–675. [Google Scholar] [CrossRef] [PubMed]
- Okamoto, F.; Allen, B.S.; Buckberg, G.D.; Bugyi, H.; Leaf, J. Reperfusion conditions: Importance of ensuring gentle versus sudden reperfusion during relief of coronary occlusion. J. Thorac. Cardiovasc. Surg. 1986, 92, 613–620. [Google Scholar] [CrossRef]
- Murry, C.E.; Jennings, R.B.; Reimer, K.A. Preconditioning with ischemia: A delay of lethal cell injury in ischemic myocardium. Circulation 1986, 74, 1124–1136. [Google Scholar] [CrossRef] [Green Version]
- Pasupathy, S.; Homer-Vanniasinkam, S. Surgical implications of ischemic preconditioning. Arch. Surg. 2005, 140, 405–409. [Google Scholar] [CrossRef] [Green Version]
- Ulus, A.T.; Yavas, S.; Sapmaz, A.; Sakaoğullari, Z.; Simsek, E.; Ersoz, S.; Koksoy, C. Effect of conditioning on visceral organs during indirect ischemia/reperfusion injury. Ann. Vasc. Surg. 2014, 28, 437–444. [Google Scholar] [CrossRef]
- Przyklenk, K.; Bauer, B.; Ovize, M.; Kloner, R.A.; Whittaker, P. Regional ischemic ‘preconditioning’ protects remote virgin myocardium from subsequent sustained coronary occlusion. Circulation 1993, 87, 893–899. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.; Liu, X.R.; Yan, F.; Min, L.Q.; Ji, X.M.; Luo, Y.M. Protective effects of remote ischemic preconditioning in rat hindlimb on ischemia- reperfusion injury. Neural Regen. Res. 2012, 7, 583–587. [Google Scholar]
- Zhao, Z.Q.; Corvera, J.S.; Halkos, M.E.; Kerendi, F.; Wang, N.P.; Guyton, R.A.; Vinten-Johansen, J. Inhibition of myocardial injury by ischemic postconditioning during reperfusion: Comparison with ischemic preconditioning. Am. J. Physiol. Heart Circ. Physiol. 2003, 285, H579–H588. [Google Scholar] [CrossRef]
- Kayar, E.; Mat, F.; Meiselman, H.J.; Baskurt, O.K. Red blood cell rheological alterations in a rat model of ischemia-reperfusion injury. Biorheology 2001, 38, 405–414. [Google Scholar]
- Baskurt, O.K. Mechanisms of blood rheology alterations. In Handbook of Hemorheology and Hemodynamics; Baskurt, O.K., Hardeman, M.R., Rampling, M.W., Meiselman, H.J., Eds.; IOS Press: Amsterdam, The Netherlands, 2007; pp. 170–190. [Google Scholar]
- Nemeth, N.; Peto, K.; Magyar, Z.; Klarik, Z.; Varga, G.; Oltean, M.; Mantas, A.; Czigany, Z.; Tolba, R.H. Hemorheological and microcirculatory factors in liver ischemia-reperfusion injury—An update on pathophysiology, molecular mechanisms and protective strategies. Int. J. Mol. Sci. 2021, 22, 1864. [Google Scholar] [CrossRef]
- McAllister, S.E.; Ashrafpour, H.; Cahoon, N.; Huang, N.; Moses, M.A.; Neligan, P.C.; Forrest, C.R.; Lipa, J.E.; Pang, C.Y. Postconditioning for salvage of ischemic skeletal muscle from reperfusion injury: Efficacy and mechanism. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2008, 295, R681–R689. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, J.W.; Kang, J.W.; Jeon, W.J.; Na, H.S. Postconditioning protects skeletal muscle from ischemia-reperfusion injury. Microsurgery 2010, 30, 223–229. [Google Scholar] [CrossRef]
- Lintz, J.A.; Dalio, M.B.; Joviliano, E.E.; Piccinato, C.E. Ischemic pre and postconditioning in skeletal muscle injury produced by ischemia and reperfusion in rats. Acta Cir. Bras. 2013, 28, 441–446. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Magyar, Z.; Mester, A.; Nadubinszky, G.; Varga, G.; Ghanem, S.; Somogyi, V.; Tanczos, B.; Deak, A.; Bidiga, L.; Oltean, M.; et al. Beneficial effects of remote organ ischemic preconditioning on micro-rheological parameters during liver ischemia-reperfusion in the rat. Clin. Hemorheol. Microcirc. 2018, 70, 181–190. [Google Scholar] [CrossRef]
- Varga, G.; Ghanem, S.; Szabo, B.; Nagy, K.; Pal, N.; Tanczos, B.; Somogyi, V.; Barath, B.; Deak, A.; Peto, K.; et al. Renal ischemia-reperfusion-induced metabolic and micro-rheological alterations and their modulation by remote organ ischemic preconditioning protocols in the rat. Clin. Hemorheol. Microcirc. 2019, 71, 225–236. [Google Scholar] [CrossRef] [PubMed]
- Nemeth, N.; Szokoly, M.; Acs, G.; Brath, E.; Lesznyak, T.; Furk, I.; Miko, I. Systemic and regional hemorheological consequences of warm and cold hind limb ischemia-reperfusion in a canine model. Clin. Hemorheol. Microcirc. 2004, 30, 133–145. [Google Scholar]
- Nemeth, N.; Lesznyak, T.; Szokoly, M.; Furka, I.; Miko, I. Allopurinol prevents erythrocyte deformability impairing but not the hematological alterations after limb ischemia-reperfusion in rats. J. Investig. Surg. 2006, 19, 47–56. [Google Scholar] [CrossRef]
- Nemeth, N.; Kiss, F.; Hever, T.; Brath, E.; Sajtos, E.; Furka, I.; Miko, I. Hemorheological consequences of hind limb ischemia-reperfusion differs in normal and gonadectomized male and female rats. Clin. Hemorheol. Microcirc. 2012, 50, 197–211. [Google Scholar] [CrossRef] [Green Version]
- Rosero, O.; Nemeth, K.; Turoczi, Z.; Fulop, A.; Garbaisz, D.; Gyorffy, A.; Szuak, A.; Dorogi, B.; Kiss, M.; Nemeskeri, A.; et al. Collateral circulation of the rat lower limb and its significance in ischemia–reperfusion studies. Surg. Today 2014, 44, 2345–2353. [Google Scholar] [CrossRef]
- Nemeth, N.; Deak, A.; Szentkereszty, Z.; Peto, K. Effects and influencing factors on hemorheological variables taken into consideration in surgical pathophysiology research. Clin. Hemorheol. Microcirc. 2018, 69, 133–140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kocman, E.A.; Ozatik, O.; Sahin, A.; Guney, T.; Kose, A.A.; Dag, I.; Alatas, O.; Cetin, C. Effects of ischemic preconditioning protocols on skeletal muscle ischemia-reperfusion injury. J. Surg. Res. 2015, 193, 942–952. [Google Scholar] [CrossRef] [PubMed]
- Johnson, R.M. pH effects on red blood cell deformability. Blood Cells. 1985, 11, 317–321. [Google Scholar] [PubMed]
- Koppensteiner, R. Blood rheology in emergency medicine. Semin. Thromb. Hemost. 1996, 22, 89–91. [Google Scholar] [CrossRef]
- Reinhart, W.H.; Gaudenz, R.; Walter, R. Acidosis induced by lactate, pyruvate, or HCl increases blood viscosity. Crit. Care 2002, 17, 38–42. [Google Scholar] [CrossRef] [PubMed]
- Cicha, I.; Suzuki, Y.; Tateishi, N.; Maeda, N. Changes of RBC aggregation in oxygenation-deoxygenation: pH dependency and cell morphology. Am. J. Physiol. Heart Circ. Physiol. 2003, 284, H2335–H2342. [Google Scholar] [CrossRef]
- Uyuklu, M.; Meiselman, H.J.; Baskurt, O.K. Effect of hemoglobin oxygenation level on red blood cell deformability and aggregation parameters. Clin. Hemorheol. Microcirc. 2009, 41, 179–188. [Google Scholar] [CrossRef]
- Lipowsky, H.H. Microvascular rheology and hemodynamics. Microcirculation 2005, 12, 5–15. [Google Scholar] [CrossRef]
- Pries, A.R.; Secomb, T.W. Blood flow in microvascular networks. In Handbook of Physiology, Microcirculation, 2nd ed.; Tuma, R.F., Duran, W.N., Ley, K., Eds.; Elsevier Academic Press: Amsterdam, The Netherlands, 2008; pp. 3–36. [Google Scholar]
- Chandran, K.B.; Rittgers, S.E.; Yoganathan, A.P. Rheology of blood and vascular mechanics. In Biofluid Mechanics; Chandran, K.B., Rittgers, S.E., Yoganathan, A.P., Eds.; CRC Press: Boca Raton, FL, USA, 2012; pp. 109–154. [Google Scholar]
- Baskurt, O.K. In vivo correlates of altered blood rheology. Biorheology 2008, 45, 629–638. [Google Scholar] [CrossRef]
- Schoen, M.; Rotter, R.; Gierer, P.; Gradl, G.; Strauss, U.; Jonas, L.; Mittlmeier, T.; Vollmar, B. Ischemic preconditioning prevents skeletal muscle tissue injury, but not nerve lesion upon tourniquet-induced ischemia. J. Trauma 2007, 63, 788–797. [Google Scholar] [CrossRef]
- Turchanyi, B.; Korei, C.; Somogyi, V.; Kiss, F.; Peto, K.; Nemeth, N. Beneficial postoperative micro-rheological effects of intraoperative administration of diclophenac or ischemic preconditioning in patients with lower extremity operations—Preliminary data. Clin. Hemorheol. Microcirc. 2021; Epub ahead of print. [Google Scholar] [CrossRef]
- Hardeman, M.; Goedhart, P.; Shin, S. Methods in hemorheology. In Handbook of Hemorheology and Hemodynamics; Baskurt, O.K., Hardeman, M.R., Rampling, M.W., Meiselman., H.J., Eds.; IOS Press: Amsterdam, The Netherlands, 2007; pp. 242–266. [Google Scholar]
- Baskurt, O.K.; Boynard, M.; Cokelet, G.C.; Connes, P.; Cooke, B.M.; Forconi, S.; Liao, F.; Hardeman, M.R.; Jung, F.; Meiselman, H.J.; et al. International Expert Panel for Standardization of Hemorheological Methods. New guidelines for hemorheological laboratory techniques. Clin. Hemorheol. Microcirc. 2009, 42, 75–97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baskurt, O.K.; Hardeman, M.R.; Uyuklu, M.; Ulker, P.; Cengiz, M.; Nemeth, N.; Shin, S.; Alexy, T.; Meiselman, H.J. Parameterization of red blood cell elongation index—Shear stress curves obtained by ektacytometry. Scand. J. Clin. Lab. Investig. 2009, 69, 777–788. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Group | Base | Reperfusion | 1st p.o. Week |
|---|---|---|---|---|
| WBC [G/L] | Control | 9.36 ± 1.85 | 8.62 ± 2.35 | 10.4 ± 3.59 |
| I/R | 8.05 ± 1.23 | 10.77 ± 4.23 * | 10.17 ± 4.47 | |
| PreC | 7.08 ± 1.11 | 10.67 ± 2.53 * | 11.2 ± 4.15 * | |
| PostC | 7.51 ± 1.57 | 8.77 ± 3.67 | 10.65 ± 3.1 * | |
| RBC [T/L] | Control | 7.78 ± 0.47 | 7.49 ± 0.41 | 7.44 ± 0.37 |
| I/R | 8.38 ± 0.64 | 7.69 ± 0.71 * | 7.09 ± 0.28 * | |
| PreC | 8.35 ± 0.39 | 7.65 ± 0.56 * | 6.93 ± 1.37 * | |
| PostC | 8.18 ± 0.73 | 7.69 ± 0.77 | 7.09 ± 0.43 * | |
| Hgb [g/dL] | Control | 15.23 ± 0.74 | 14.89 ± 0.67 | 14.52 ± 0.83 * |
| I/R | 15.61 ± 0.82 | 14.75 ± 0.76 * | 13.41 ± 0.51 * | |
| PreC | 15.18 ± 0.41 | 14.14 ± 0.79 * | 12.84 ± 2.56 * | |
| PostC | 15.16 ± 0.68 | 14.25 ± 0.84 * | 13.25 ± 0.78 * # | |
| Hct [%] | Control | 46.68 ± 2.45 | 45.23 ± 2.43 | 43.6 ± 2.07 * |
| I/R | 47.4 ± 3.07 | 44.6 ± 3.49 | 40.39 ± 1.31 * # | |
| PreC | 46.7 ± 1.41 | 43.81 ± 2.99 | 38.96 ± 7.56 * | |
| PostC | 45.93 ± 2.87 | 44.13 ± 3.16 | 40.21 ± 2.09 * # | |
| Plt [G/L] | Control | 741.2 ± 62.1 | 626.8 ± 99.5 * | 833.6 ± 40.9 * |
| I/R | 810.1 ± 72.9 | 747.6 ± 80.5 * # | 958.5 ± 100.1 * # | |
| PreC | 726.3 ± 82.7 | 638.3 ± 63 * | 873.1 ± 315.4 * | |
| PostC | 712.6 ± 67.2 | 625.7 ± 57.2 * | 1000 ± 44.5 * # |
| Variable | Group | Base | Reperfusion | 1st p.o. Week |
|---|---|---|---|---|
| EI at 3 Pa | Control | 0.393 ± 0.007 | 0.392 ± 0.024 | 0.387 ± 0.01 |
| I/R | 0.392 ± 0.013 | 0.402 ± 0.009 | 0.378 ± 0.02 * | |
| PreC | 0.400 ± 0.012 | 0.392 ± 0.012 | 0.371 ± 0.018 | |
| PostC | 0.391 ± 0.013 | 0.397 ± 0.01 | 0.382 ± 0.012 | |
| EImax | Control | 0.582 ± 0.015 | 0.553 ± 0.049 | 0.571 ± 0.017 |
| I/R | 0.601 ± 0.02 | 0.587 ± 0.022 | 0.581 ± 0.032 | |
| PreC | 0.585 ± 0.019 | 0.589 ± 0.024 | 0.588 ± 0.046 | |
| PostC | 0.595 ± 0.028 | 0.576 ± 0.023 | 0.593 ± 0.022 | |
| SS1/2 [Pa] | Control | 1.44 ± 0.25 | 1.2 ± 0.42 | 1.53 ± 0.3 |
| I/R | 1.23 ± 0.33 | 1.26 ± 0.25 | 1.45 ± 0.27 | |
| PreC | 1.36 ± 0.25 | 1.21 ± 0.23 | 1.33 ± 0.52 | |
| PostC | 1.28 ± 0.46 | 1.32 ± 0.36 | 1.34 ± 0.25 | |
| EImax/SS1/2 [Pa−1] | Control | 0.419 ± 0.092 | 0.52 ± 0.19 | 0.387 ± 0.087 |
| I/R | 0.524 ± 0.156 | 0.488 ± 0.136 | 0.418 ± 0.112 | |
| PreC | 0.454 ± 0.143 | 0.499 ± 0.096 | 0.553 ± 0.365 | |
| PostC | 0.487 ± 0.223 | 0.473 ± 0.165 | 0.458 ± 0.103 |
| Variable | Group | Base | Reperfusion | 1st p.o. Week |
|---|---|---|---|---|
| pO2 [mmHg] | Control | 68.87 ± 13.26 | 65.73 ± 11.05 | 55.2 ± 6.93 |
| I/R | 60.14 ± 6.61 | 61.37 ± 8.49 | 55.06 ± 9.22 | |
| PreC | 65.05 ± 5.75 | 69.47 ± 15.27 | 51.78 ± 11.8 | |
| PostC | 59.65 ± 9.27 | 68.08 ± 6.57 | 57.1 ± 16.21 | |
| pCO2 [mmHg] | Control | 41.3 ± 9.04 | 43.55 ± 5.54 | 52.62 ± 11.23 |
| I/R | 50.45 ± 6.57 | 49.94 ± 17.77 | 49.4 ± 4.72 | |
| PreC | 47.64 ± 6.78 | 48.01 ± 11.17 | 42.42 ± 4.95 | |
| PostC | 47.78 ± 6.62 | 47.68 ± 12.2 | 45.12 ± 5.86 | |
| pH | Control | 7.41 ± 0.03 | 7.37 ± 0.03 | 7.36 ± 0.06 |
| I/R | 7.36 ± 0.04 | 7.33 ± 0.11 | 7.38 ± 0.04 | |
| PreC | 7.38 ± 0.07 | 7.31 ± 0.07 | 7.41 ± 0.04 | |
| PostC | 7.35 ± 0.03 | 7.32 ± 0.08 | 7.39 ± 0.02 | |
| Na+ [mmol/L] | Control | 142.12 ± 3.35 | 141.83 ± 2.13 | 143.6 ± 2.61 |
| I/R | 141 ± 2.31 | 140.28 ± 5.4 | 142 ± 2.34 | |
| PreC | 142.28 ± 2.69 | 140.28 ± 4.46 | 141.71 ± 2.56 | |
| PostC | 142.42 ± 3.2 | 140.14 ± 2.47 | 143.85 ± 2.41 | |
| K+ [mmol/L] | Control | 4.72 ± 0.32 | 5.45 ± 0.56 * | 4.82 ± 0.29 |
| I/R | 4.32 ± 0.28 | 5.92 ± 0.57 * | 4.04 ± 0.38 # | |
| PreC | 4.25 ± 0.25 | 5.58 ± 0.86 * | 4.61 ± 0.5 | |
| PostC | 4.24 ± 0.25 | 6.05 ± 0.62 * | 4.17 ± 0.29 # | |
| Ca2+ [mmol/L] | Control | 1.36 ± 0.04 | 1.38 ± 0.11 | 1.28 ± 0.19 |
| I/R | 1.35 ± 0.04 | 1.39 ± 0.04 | 1.23 ± 0.31 | |
| PreC | 1.34 ± 0.06 | 1.39 ± 0.06 | 1.27 ± 0.17 | |
| PostC | 1.39 ± 0.05 | 1.39 ± 0.03 | 1.32 ± 0.09 | |
| Cl− [mmol/L] | Control | 104.25 ± 1.67 | 108.16 ± 3.18 | 104.6 ± 1.34 |
| I/R | 103.14 ± 2.11 | 105.85 ± 2.19 | 102.6 ± 1.67 | |
| PreC | 103.14 ± 2.03 | 104.85 ± 2.79 | 104 ± 1.52 | |
| PostC | 104 ± 2.31 | 106.28 ± 1.6 | 103.85 ± 2.19 | |
| glucose [mmol/L] | Control | 19.62 ± 3.54 | 17.11 ± 3.47 | 17.94 ± 3.08 |
| I/R | 17.98 ± 2.09 | 19.6 ± 4.27 | 12.34 ± 2.21 * # | |
| PreC | 17.22 ± 2.19 | 22.48 ± 7.61 | 11.8 ± 2.61 * # | |
| PostC | 16.5 ± 1.09 | 22.64 ± 4.77 * # | 13.12 ± 2.45 * # | |
| lactate [mmol/L] | Control | 1.171 ± 0.34 | 1.52 ± 0.61 | 1.02 ± 0.32 |
| I/R | 1.61 ± 0.73 | 1.36 ± 0.34 | 2.31 ± 0.91 # | |
| PreC | 1.78 ± 0.87 | 1.72 ± 0.85 | 3.11 ± 1.89 # | |
| PostC | 1.82 ± 0.99 | 1.28 ± 0.31 | 3.39 ± 2.2 # | |
| creatinine [µmol/L] | Control | 31 ± 4.37 | 43.83 ± 10 | 36.2 ± 3.89 |
| I/R | 35.33 ± 5.68 | 47.85 ± 8.47 | 37.2 ± 5.26 | |
| PreC | 32.42 ± 3.59 | 68.42 ± 31.28 * | 52.85 ± 25.51 | |
| PostC | 43.85 ± 8.45 | 83 ± 43.77 * # + | 35.71 ± 6.15 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Korei, C.; Szabo, B.; Varga, A.; Barath, B.; Deak, A.; Vanyolos, E.; Hargitai, Z.; Kovacs, I.; Nemeth, N.; Peto, K. Hematological, Micro-Rheological, and Metabolic Changes Modulated by Local Ischemic Pre- and Post-Conditioning in Rat Limb Ischemia-Reperfusion. Metabolites 2021, 11, 776. https://0-doi-org.brum.beds.ac.uk/10.3390/metabo11110776
Korei C, Szabo B, Varga A, Barath B, Deak A, Vanyolos E, Hargitai Z, Kovacs I, Nemeth N, Peto K. Hematological, Micro-Rheological, and Metabolic Changes Modulated by Local Ischemic Pre- and Post-Conditioning in Rat Limb Ischemia-Reperfusion. Metabolites. 2021; 11(11):776. https://0-doi-org.brum.beds.ac.uk/10.3390/metabo11110776
Chicago/Turabian StyleKorei, Csaba, Balazs Szabo, Adam Varga, Barbara Barath, Adam Deak, Erzsebet Vanyolos, Zoltan Hargitai, Ilona Kovacs, Norbert Nemeth, and Katalin Peto. 2021. "Hematological, Micro-Rheological, and Metabolic Changes Modulated by Local Ischemic Pre- and Post-Conditioning in Rat Limb Ischemia-Reperfusion" Metabolites 11, no. 11: 776. https://0-doi-org.brum.beds.ac.uk/10.3390/metabo11110776