
Vitamin D, Bone Metabolism, and Fracture Risk in Polycystic Ovary Syndrome
by
 , , and
, , and
Flavia Di Bari
1, 
Antonino Catalano
1,*,
Federica Bellone
1,
Gabriella Martino
1 and
Salvatore Benvenga
1,2,3 1
Department of Clinical and Experimental Medicine, University of Messina, Messina, Viale Gazzi, 98125 Messina, Italy
2
Master Program on Childhood, Adolescent and Women’s Endocrine Health, University of Messina, Viale Gazzi, 98125 Messina, Italy
3
Interdepartmental Program of Molecular & Clinical Endocrinology and Women’s Endocrine Health, University Hospital, A.O.U. Policlinico G. Martino, Viale Gazzi, 98125 Messina, Italy
*
Author to whom correspondence should be addressed.
Metabolites 2021, 11(2), 116; https://0-doi-org.brum.beds.ac.uk/10.3390/metabo11020116
Submission received: 31 December 2020
/
Revised: 15 February 2021
/
Accepted: 16 February 2021
/
Published: 18 February 2021
(This article belongs to the Special Issue Vitamin D and Bone Metabolism)
{kind=link}
Abstract
:Polycystic ovary syndrome (PCOS) is the most common endocrine disorder among premenopausal women. PCOS may have reproductive, metabolic, cardiovascular, and psychological implications. Vitamin D deficit is often encountered in PCOS women and may contribute to the pathophysiology of this disorder. As of the key role of vitamin D in bone and mineral metabolism, and because the vitamin D status appears to be closely linked with the PCOS manifestations including insulin resistance, obesity, ovulatory and menstrual irregularities, oxidative stress and PTH elevation, hypovitaminosis D may directly and indirectly via the different facets of PCOS impair bone health in these women. Although limited data are available on life-long fracture risk in women with PCOS, the importance of preserving bone health in youth and adults to prevent osteoporosis and related fractures is also recognized in PCOS women. Evidence of the association between vitamin D and the clinical hallmarks of PCOS are summarized and discussed. Vitamin D arises as a cornerstone in women with PCOS and contributes to the pathophysiological link between PCOS and bone metabolism.
1. Introduction
Polycystic ovary syndrome (PCOS) is a heterogeneous endocrine disorder affecting up to 20% of premenopausal women, possibly making this syndrome the most common endocrine and metabolic disorder in women of reproductive age. PCOS was first described in 1935 by Stein and Leventhal as the combination of hirsutism (a condition of male pattern terminal hair growth in women), amenorrhea, chronic anovulation and infertility, obesity, and enlarged cystic ovaries [1,2,3]. PCOS is defined in accordance with the Rotterdam criteria (at least two of the following criteria: (1) irregular/no ovulation; (2) clinical/biochemical hyperandrogenemia, and (3) polycystic ovaries [1] or the National Institutes of Health (NIH) criteria (oligo-anovulation and biochemical and/or clinical signs of hyperandrogenism in the absence of other endocrinopathies) or the Androgen Excess and PCOS Society (AE-PCOS) criteria (mandatory presence of hyperandrogenism associated with ovarian dysfunction, defined by oligo-anovulation and/ or ultrasound PCO) [4]. The polycystic appearance of the ovaries frequently found in patients suffering from PCOS is caused by the accumulation of ovarian follicles in different stages of maturation or atresia. The etiology of PCOS remains largely unknown, although it can be considered a complex multigene condition influenced by epigenetic and lifestyle factors [1]. Vitamin D deficiency is defined as 25(OH)D serum levels < 20 ng/mL, while vitamin D insufficiency as serum levels of 21–29 ng/mL [5]. Not adequate vitamin D levels are very common worldwide, not only in the elderly population but also in young people [5]. About 67–85% of women with PCOS show vitamin D deficiency [6]. A poor vitamin D status has been associated with the salient features of PCOS including insulin resistance (IR), ovulatory and menstrual irregularities, decreased pregnancy rate, hirsutism, hyperandrogenism, obesity, and elevated cardiovascular disease [6,7]. Therefore, vitamin D might not only participate in the pathophysiology of PCOS but might also indirectly contribute to lower bone mineral density (BMD) in this particular situation [7]. A poor vitamin D status has been consistently associated with an increased risk of fragility fractures in several clinical settings [8,9,10].
2. Vitamin D Metabolism and Vitamin D Role in Female Reproduction
Vitamin D exists in two forms: ergocalciferol (D2) and cholecalciferol (D3). Vitamin D3 is mainly produced by the skin cells upon exposure to sun rays [11]. A small proportion (about 10–20%) is introduced with food [11]. Then, cholecalciferol is hydroxylated in the liver in 25-hydroxyvitamin D or calcifediol [25(OH)D], the circulating form of the vitamin, whose serum levels are indicative of vitamin D status. In the kidney, 25-hydroxyvitamin D is converted into 1,25-dihydroxy vitamin D or calcitriol [1,25(OH)D] [12]. Calcitriol is the active form of the hormone and its primary function is to regulate calcium/phosphorus metabolism and bone mineralization by osteoclast action [13]. However, vitamin D acts in other tissues such as parathyroid glands, immune cells, pancreas and placenta, uterus, ovaries, and testes via binding to the nuclear vitamin D receptor (VDR) [14,15,16]. VDR is a DNA binding transcription factor, forming a heterodimer with a retinoid X receptor (RXR) [14]. Ramagopalan et al. reported approximately 230 genes in more than 30 different tissues responsive to vitamin D stimulation [16]. Thus, vitamin D has been implicated in a wide range of extra-skeletal effects and diseases, including reproductive dysfunctions and polycystic ovary syndrome (PCOS) [6,17,18,19,20,21,22,23,24,25,26,27,28]. Physiologically, VDR is expressed in reproductive tissues of the cycling mice and pregnant mice, including placenta and decidua [29]. Furthermore, VDR knockout mice have impaired folliculogenesis and hypergonadotropic hypogonadism [30]. In humans, in vitro exposure of ovarian cells to vitamin D increases 3β-HSD mRNA levels and production of progesterone, estrogen, and estrone [13,31,32,33]. Vitamin D stimulates the differentiation and the development of human granulosa cells (GC) and influences follicular maturation by a direct effect on the anti-Mullerian hormone (AMH) gene [13]. AMH, which is considered a marker of the ovarian reserve, is usually produced by the GC of preantral/antral ovarian follicles [34]. Women with PCOS have abnormally increased serum and intrafollicular AMH levels, due to a rise in the number of arrested small antral follicles, besides AMH hypersecretion by the granulosa cells themselves [35]. A study on 54 women undergoing in vitro fertilization described a two-fold increase in AMHR-II expression in GC of women with insufficient follicular fluid 25(OH)D (<30 ng/mL) compared with women having normal follicular fluid vitamin D levels (>30 ng/mL) [31]. It is conceivable that vitamin D alters AMH signaling and steroidogenesis in human cumulus GC [31]. Moreover, a relationship exists between vitamin D and follicle-stimulating hormone (FSH) receptor (FSHR), so vitamin D regulates follicular sensitivity to FSH [5]. Probably, vitamin D regulates both AMHR-II and FSHR gene expression [13]. Although conflicting, these findings suggest that vitamin D influences AMH gene expression and probably, it could neutralize the inhibitory effect of AMH on GC differentiation and follicular growth by inhibiting AMHR-II expression and downstream signaling [33]. A positive correlation between AMH and BMD has been recently found in premenopausal women with suspected ovarian insufficiency [36]. Although this review does not attempt to discuss the pleiotropic effects of vitamin D on female reproduction, these results highlight the crucial role of vitamin D in human biology; it also suggests modifications of bone metabolism in PCOS women via an indirect effect of vitamin D through several hormone changes [15,37]. In other terms, while vitamin D is primarily essential for musculoskeletal health, accumulating data are suggesting that vitamin D may be important for fertility, but also pregnancy outcomes and lactation [38,39]. Thus, by conditioning endocrine PCOS women milieu, vitamin D may secondarily interfere with bone metabolism.
3. Vitamin D and PCOS
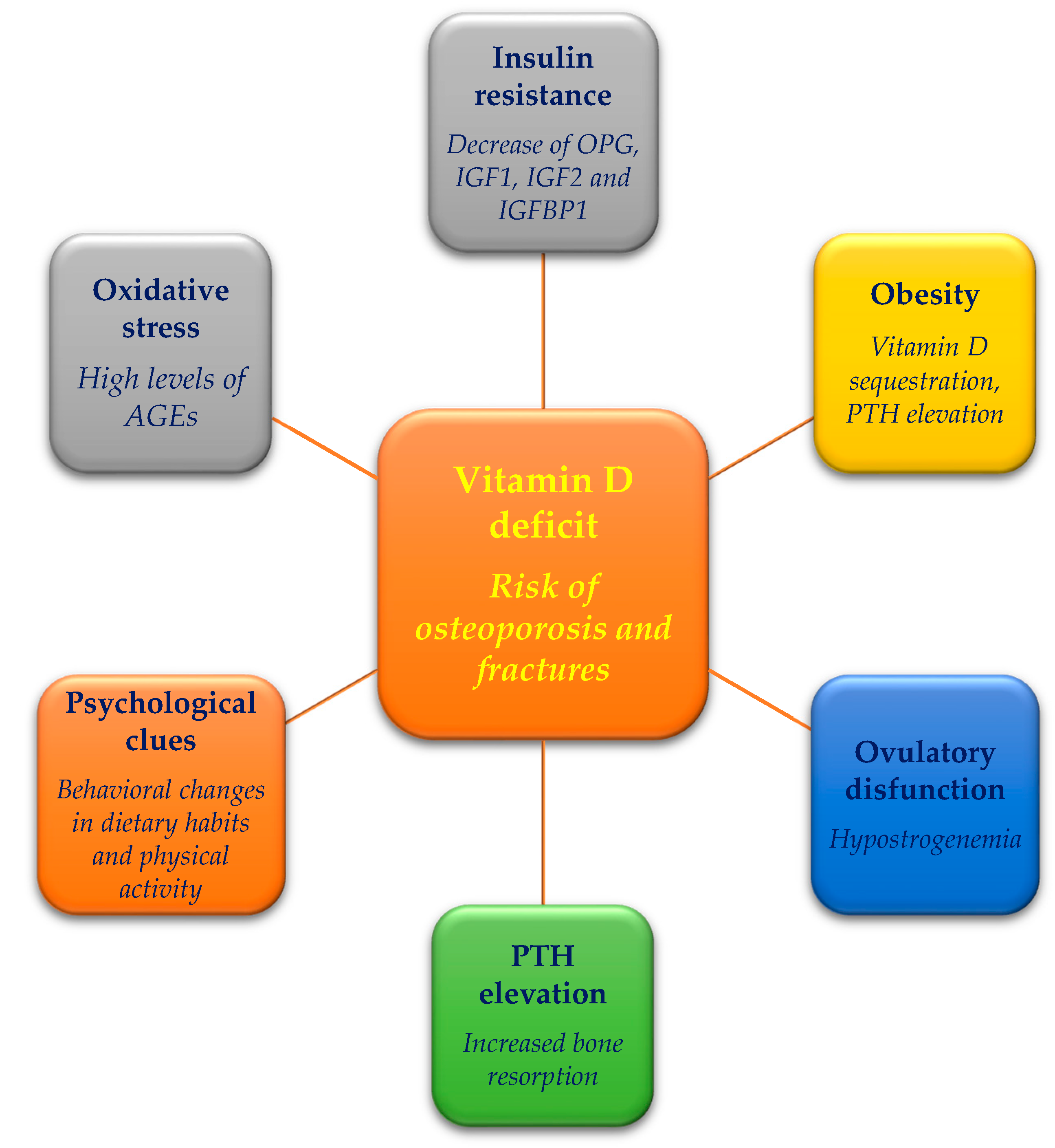
As mentioned above, a poor vitamin D status is described in women with PCOS. Several studies reported an involvement of the vitamin D pathway in the development of PCOS and its symptoms, comprising hirsutism, ovulatory dysfunction, IR, and cardiovascular diseases [40,41]. Upon comparing PCOS with non-PCOS women, serum levels of vitamin D levels were reported to be either lower [42,43,44] or statistically similar [45] in PCOS compared with non-PCOS women. Interestingly, interventional studies revealed that vitamin D supplementation might improve menstrual irregularity and follicular development in PCOS women [13]. Additionally, some PCOS clinical features associated with vitamin D, as highlighted in Figure 1, have been previously associated with the risk of osteoporosis and fractures in the general population [46,47]; thus, it is reasonable they could contribute to bone fragility even in PCOS.
3.1. VDR Polymorphism
The binding of the heterodimer VDR-RXR with vitamin-D-responsive elements (VDRE) activates gene transcription, and it has been described that VDR polymorphisms influence the production of its correspondent mRNA, but the exact mechanism is unclear [48]. Several studies described that the gene polymorphism of VDR is associated with a low concentration of 25(OH)D and with the pathogenesis of PCOS metabolic and endocrine features [49]. However, most studies were conducted in Asian countries, and evidence from other geographical areas are needed [48]. VDR polymorphism could regulate the insulin secretor capacity through changes in the quantity of the corresponding gene product [48]. VDR Tru 9I, Bsm1, TaqI, Apa-I, Cdx2, and Fok1 are the most studied polymorphic variants [13,50]. Particularly, Al-Daghri et al. reported a relationship between the VDR Bsm1 variant and the reduced risk of vitamin D deficiency [50]. VDR Apa-I and Bsm1 polymorphisms appear to be associate with an increased risk of PCOS, while TaqI and Cdx2 could be related to severity and susceptibility of PCOS, including strong symptoms such as higher IR, fasting insulin, testosterone levels, body mass index (BMI) and lower vitamin D levels [50]. Furthermore, Cdx2 and FokI variants could be associated with testosterone levels and infertility, respectively [51]. Polymorphisms of vitamin VDR have been also proposed as genetic determinants of bone quality, skeletal geometry, and bone turnover markers [52,53]. Overall, significant correlations between VDR ApaI, VDR FokI, and osteoporosis susceptibility have been found [52,53,54]. A recent meta-analysis has also suggested VDR BsmI genotype is associated with an increased risk of postmenopausal osteoporosis in Caucasians but not in Asians, highlighting possible ethnic differences [54]. Even though results are still conflicting and the molecular mechanisms by which these polymorphisms influence receptor activity remain in part to be investigated, an additional important issue is represented by their potential pharmacogenomic and pharmacogenetic implications [55].
3.2. Insulin Resistance and Vitamin D
PCOS is characterized by IR and metabolic dysfunctions and low levels of 25(OH)D levels are negatively associated with IR, BMI, non-HDL cholesterol, blood pressure, leptin levels, androgen levels, but positively with HDL cholesterol [27,56,57,58,59,60,61]. IR is associated with an increased risk for dysglycemia, type 2 diabetes mellitus, metabolic syndrome, and cardiovascular disease [14,62]. Women with PCOS and vitamin D deficiency have a greater prevalence of impaired glucose tolerance compared with PCOS women with no vitamin D deficiency [6]. Vitamin D appears to regulate the glyco-insulin homeostasis via different mechanisms: (1) stimulating insulin release through the expression of VDR in the pancreatic β-cells; (2) increasing responsiveness of GLUT (glucose transport) to insulin through the binding of the 1,25(OH)D–VDR complex to the VDRE of the insulin receptor at the tissue level; (3) suppressing of the release of proinflammatory cytokines that are believed to mediate IR; (4) regulating of intra and extracellular calcium levels, which are essential for insulin-mediated actions [62,63,64,65]. At the bone tissue level, insulin physiologically increases osteoblast proliferation and collagen formation and inhibits parathyroid hormone (PTH) action; conversely, the state of hyperinsulinism leads to a decrease of osteoprotegerin (OPG) as well as insulin-like growth factors 1 and 2 and insulin-like growth factor-binding protein 1, increasing bone reabsorption [66,67]. The decrease in OPG/RANKL ratio can result in an increased expression of Tcirg1 in osteoclast, which encodes for a proton pump and contributes to the acidification of the resorption lacunae. The acidic pH can decarboxylate and activate osteocalcin. The undercarboxylated form of osteocalcin, on the other hand, has been shown to facilitate pancreatic β-cell proliferation and insulin secretion [68]. The treatment with both vitamin D and calcium appears to reduce IR and serum androgen levels in vitamin D-deficient PCOS women with consequent improvement of hirsutism and menses regularity [69,70,71]. In a recent review, supplementation of vitamin D < 4000 IU/d or administration of vitamin D as a co-supplement improved insulin sensitivity reducing the fasting glucose concentration (about 6.3% with supplementation with vitamin D and other micronutrients), the mean fasting insulin levels (about 22% in some trials) and HOMA-IR [72]. However, Menichini and Facchinetti, after reviewing the effects of vitamin D supplementation in women with PCOS, showed better outcomes after the supplementation of high dose (4000 IU), compared with low-dose (1000 IU) of vitamin D or placebo, for a period of at least 12 weeks [73]. In addition, a recent meta-analysis, including 10 randomized controlled trials, has shown a significant reduction of fasting glucose levels but no significant effect on fasting insulin concentration and HOMA-IR, in vitamin D-deficient PCOS women [74]. Overall, vitamin D supplementation appears to have beneficial effects on IR and dysglycemia and could as well modulate bone metabolism [66,67,75,76,77].
3.3. Hyperandrogenemia and Vitamin D
The low serum levels of FSH and the increased serum levels of luteinizing hormone characterizing PCOS, stimulate the androgen synthesis and the subsequent development of IR [31]. IR leads to the enhanced ovarian secretion of androgens and consequently reduction of sex hormone-binding globulin (SHBG) production [61], low SHBG concentrations determining elevated free serum testosterone levels [78]. Furthermore, hyperandrogenemia is a principal causal factor of the metabolic dysfunctions observed in PCOS [79]. Indeed, hyperandrogenemia is often accountable for impaired insulin sensitivity and it influences the distribution of adipose tissue with the development of insulin-signaling abnormalities and IR, abnormal visceral adiposity, and adipose tissue dysfunction, thus determining a vicious circle [79]. Androgen receptors are expressed by osteoblasts, osteoclasts, and osteocytes in both men and women, suggesting a direct action of androgen on these bone cells [80]. However, androgens could affect bone metabolism indirectly, e.g., via the inhibition of bone resorption by downregulating interleukin-6 (IL-6) and prostaglandin E (PGE) synthesis, or via the inhibition of PTH release by increasing intestinal calcium absorption and preventing its excretion and by increasing vitamin D3 production. Androgen receptors in bone are upregulated not only by androgens, but also by estrogens, glucocorticoids, and 1,25(OH)D; however, serum levels of estrogens and 1,25(OH)D are reduced in patients affected form PCOS [81]. This aspect of PCOS may adversely affect the regulation of BMD by androgens, although BMD is almost always positively associated with testosterone levels. It is also known that vitamin D deficiency is associated with abnormalities in serum DHEAS, testosterone, SHBG, and free androgen index (FAI) [6]. For instance, some studies on PCOS women have reported inverse associations between serum 25(OH)D levels and testosterone, DHEAS and FAI and SHBG [44,58,82], and lower 25(OH)D levels have been detected in hirsute PCOS women in comparison with BMI-matched controls [15]. Vitamin D supplementation has significantly decreased serum total testosterone, serum free-testosterone, and DHEAS, even if it has been ineffective in improving other androgenic markers, such as SHBG [83,84,85]. Vitamin D supplementation has been shown to improve features of PCOS-related metabolic syndrome [86,87]. Menichini and Facchinetti reported that vitamin D supplementation at high doses (4000 IU/d) for at least 12 weeks, can improve serum levels of SHBG, FAI, and total testosterone [73]. In a randomized clinical study, vitamin D supplementation at 50,000 IU/week for 12 weeks in 30 over-weight PCOS-women decreased hirsutism score, FAI, and increased SHBG and 25(OH)D levels, with significant changes in ovaries ultrasonography and menstrual cycle regularity [88]. However, randomized placebo-controlled trials are needed to confirm the beneficial effect of vitamin D on hyperandrogenemia and to determine the dose and the duration of vitamin D treatment required to improve the androgenic profile [83].
3.4. Oxidative Stress and Vitamin D
A relationship exists between vitamin D deficiency and oxidative stress in the pathogenesis of PCOS [89]. Merhi and colleagues reported high levels of advanced glycation end-products (AGEs), produced endogenously by a combination of oxidation and glycation or absorbed exogenously from modern heat-processed diets in women with PCOS [90]. Both AGEs and their anti-inflammatory soluble receptors, sRAGE, have a role in the metabolic and reproductive features of PCOS [90]. AGEs accumulate in granulosa and techa cell layers of PCOS women with consequent worsening of follicular growth [91,92]. sRAGE levels in follicular fluid are reduced in PCOS women [93]. It has been observed that vitamin D supplementation in PCOS women may improve the steroidogenesis and enzymatic antioxidant activity in the human GC [94] and it may attenuate the actions of AGEs [95,96]. AGEs play a role in age-related bone loss [97,98]. AGEs provoke bone cell impairment and alter bone biomechanical properties. Pentosidine (PENT), a well-characterized AGE, is even considered a predictor of bone fracture [97]. It has been reported AGEs interfere with osteoblast maturation, leading to morphological cell modifications, function failure, and inhibition of the calcification process. In vitro, coadministration of vitamin D and vitamin K2 prevented the AGEs related inhibition of ALP secretion and up-regulated collagen gene expression. In contrast, in the absence of vitamin D and vitamin K2, intracellular collagen and osteocalcin levels were decreased and the RANKL/OPG ratio was increased after PENT exposure [99]. These pieces of evidence suggest a favorable vitamin D status may promote bone strength also via contrasting AGEs impact on bone metabolism.
3.5. Parathyroid Hormone (PTH) and Vitamin D in PCOS
Vitamin D and calcium metabolism are linked with obesity in PCOS women [41,45]. Probably, the obesity-related deficiency of vitamin D is attributable to a more sedentary lifestyle that leads to less sun exposure and consequently reduced cutaneous vitamin D production and/or vitamin D sequestration in subcutaneous adipose tissue [100]. Due to vitamin D deficiency, obese individuals have higher serum PTH levels [101]. Furthermore, PTH itself could favor obesity by increasing intracellular calcium concentrations, which in turn seems to promote triglycerides accumulation and inhibit lipolysis [102]. PTH concentration is increased in PCOS women compared with BMI-matched controls and in obese PCOS women compared with normal-weight PCOS women [45,103]. Studies have also revealed a direct correlation between PTH concentration and serum levels of testosterone, independently of BMI [45], and an inverse association between vitamin D concentration and androgen levels [104]. Adrenal androgen excess in PCOS is associated with increased inactivation of cortisol, which in turn leads to elevated levels of TNFα and IL-1β potentially resulting in chronic inflammatory bone disease and bone loss [105]. PTH is also supposed to directly stimulate the adrenal cortex through interaction with PTH receptor 1 [106]. It is possible there is a direct relationship between PTH and PCOS and that the beneficial effects of vitamin D supplementation on hyperandrogenemia are mediated, at least in part, by the vitamin D action on insulin sensitivity [45]. Overall, the increased circulating PTH levels, because of low 25(OH)D levels in PCOS, may drive bone loss by promoting bone resorption [105,107].
3.6. Fracture Risk in PCOS
Few studies have addressed bone health and fracture risk in women with PCOS (Table S1). The largest register-based cohort study considered a total of 19,199 women (age 12–60 years) in Denmark and found a decreased fracture risk [adjusted hazard ratio (aHR) = 0.76, 95% CI = 0.71–0.80 for all fractures; 0.82, 95% CI = 0.74–0.92 for major osteoporotic fractures] [108]. Conversely, an observational population-based study of 11,106 women (age 15–80 years) with PCOS in Taiwan reported an increased incidence of any fractures in comparison with non-PCOS women [aHR= 1.23, 95% CI = 1.13–1.33]; particularly, the aHR of osteoporotic fractures was 1.33, 95% IC = 1.15–1.54; that of spine fractures was 1.36, 95% IC = 1.11–1.66 and that of forearm fractures was 1.39, 95% IC = 1.07–1.80 [109]. Of note, the Denmark study [108] included women with hirsutism in addition to women with PCOS, which may have contributed to the heterogeneity of the study findings. Also, differences between European and Asian patients with PCOS may exist, as Chinese women with PCOS have a higher prevalence of polycystic ovarian morphology, less severe hyperandrogenism, and lower prevalence of impaired glucose tolerance and IR compared with Caucasian women [109]. However, these two studies did not analyze the potential role of confounders including body weight or BMI, lifestyle factors, and physical activity that could be involved in the peak of bone mass and the pathophysiology of bone loss later in life [110]. Yang et al reported PCOS women had a significantly higher incidence of osteoporotic fractures, spine fractures, and forearm fractures in comparison with matched healthy controls, but the similar incidence in femur or hip, humerus, wrist, and non-osteoporotic fractures [108]. Inconsistent results were reported also for BMD measurements in PCOS women. BMD is a major determinant of bone strength, but fragility fractures can occur also in women with normal or slightly reduced BMD as observed in the general population [109]. In PCOS women, some studies reported lower BMD values [111,112,113,114,115], while others reported no difference in BMD in comparison with healthy controls [116,117,118,119,120,121,122,123,124,125,126,127,128], probably due to differences in selection criteria and age of participants. A systematic review and meta-analysis showed that, in comparison with controls, women with PCOS and BMI < 27 kg/m², but not women with PCOS with BMI ≥ 27 kg/m², have decreased spinal and femur BMD, suggesting a role for adiposity in contributing to bone parameters [66]. Women with PCOS show also impaired bone metabolism as highlighted by studies that analyzed surrogate markers of bone turnover; namely carboxy-terminal collagen type 1 telopeptide, which is a bone resorption marker, and procollagen type 1 N-terminal propeptide and osteocalcin, which are bone formation markers [109,117,121,129,130,131,132,133]. Overall, PCOS women were reported to have decreased serum levels of bone formation markers that could negatively impact BMD and ultimately enhance the risk of fractures [60].
3.7. Vitamin D and Clinical Psychological Features in PCOS
PCOS women have been documented to be at risk for psychological distress. In a cross-sectional analysis based on the Australian Longitudinal Study of Women’s Health (ALWSH), comparing women with (n = 478) and without (n = 8134) a self-reported diagnosis of PCOS, women with PCOS showed a higher prevalence of depression, anxiety symptoms and greater score for perceived stress [132]. A number of studies have associated low 25(OH)D levels with poor mental health, depression, and anxiety [133,134,135,136,137,138,139]. Using the validated Hospital Anxiety and Depression Score questionnaire, Moran et al reported a positive association between depression and weight, BMI, waist circumference, and highly sensitive C-reactive protein (hsCRP) in women with PCOS [140]. Additionally, in a sensitivity analysis including Caucasian women who had no history of psychiatric illness or current use of vitamin supplements or psychiatric medication, a significant negative association between 25(OH)D and depression score was observed. At a multiple regression analysis, the 25(OH)D concentration was the only significant predictor of CRP and depression, so that for each 1.0 nmol/L decrease in serum levels of 25(OH)D, there was an increase by 0.041 mg/L in serum levels of CRP and an increase by 0.063 points in depression score [133]. The correlation between 25(OH)D and depression in PCOS reflects what is observed in the general population. It may depend on behavioral modifications, including changes in dietary habits and physical activity leading to weight gain or changes in sun exposure. Depression may seriously affect bone health and increase the risk of fragility fractures [141,142]. High levels of serum PTH, also due to poor vitamin D status, have been observed in major depression, with these high levels contributing to bone loss [143]. However, PCOS was not per se an independent predictor of depression, but it was the only independent predictor of anxiety [140]. Anxiety has been recently proven to predict low BMD and increased fracture risk in middle-aged women [142,144]. Both depression and anxiety have been related to low vitamin D concentrations [145,146]. In this context, quality of life, which is also influenced by psychological features, is lower in women with poor 25(OH)D, underlining the role of vitamin D as a marker of both physical and mental health [147,148].
4. Conclusions
Vitamin D is a hormone with pleiotropic and multiple functions. Beyond bone metabolism, it influences the reproductive axis and plays a role in the pathogenesis of PCOS. Indeed: (1) PCOS women showed a relative vitamin D deficiency (in 67–85% of cases); (2) Several VDR polymorphisms are linked with PCOS and its severity phenotypes; (3) An association exists between low vitamin D levels and each of obesity, hyperandrogenism, IR, and other metabolic dysfunctions that are PCOS-related; (4) Bone health can be influenced by several facets of PCOS possibly resulting in an increased risk of fracture over time; (5) Hypovitaminosis D is directly and indirectly linked to poor bone health in PCOS; (6) Supplementation of vitamin D-deficient PCOS women with vitamin D may improve different aspects of this disorder including menstrual regularity, fertility, BMI, lipidic profile, IR, cardiovascular risk and probably bone health. For all its beneficial properties, cheapness, and safety, vitamin D supplementation could be inserted into the therapeutic options of PCOS women, in addition to insulin-sensitizing agents and antioxidants, regardless of BMI. However, further trials are needed to clarify the role and all the possible effects of vitamin D on PCOS parameters, comprising bone health and the life-long fracture risk.
Supplementary Materials
The following are available online at https://0-www-mdpi-com.brum.beds.ac.uk/2218-1989/11/2/116/s1, Table S1: Main studies focused on bone health in polycystic ovary syndrome.
Author Contributions
Conceptualization: A.C. and S.B.; methodology F.D.B., A.C., F.B., G.M. and S.B.; writing—original draft preparation: F.D.B. and A.C., equally contributed; writing—review and editing: F.D.B., A.C. and S.B.; supervision: S.B. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Escobar-Morreale, H.F. Polycystic ovary syndrome: Definition, aetiology, diagnosis and treatment. Nat. Rev. Endocrinol. 2018, 14, 270–284. [Google Scholar] [CrossRef] [PubMed]
- Azziz, R.; Adashi, E.Y. Stein and Leventhal: 80 years on. Am. J. Obstet. Gynecol. 2016, 214, 247.e1–247.e11. [Google Scholar] [CrossRef] [PubMed]
- Azziz, R. Polycystic ovary syndrome: What’s in a name? J. Clin. Endocrinol. Metab. 2014, 99, 1142–1145. [Google Scholar] [CrossRef] [PubMed]
- Belenkaia, L.V.; Lazareva, L.M.; Walker, W.; Lizneva, D.V.; Suturina, L.V. Criteria, phenotypes and prevalence of polycystic ovary syndrome. Minerva Ginecol. 2019, 71, 211–223. [Google Scholar] [CrossRef]
- Holick, M.F.; Binkley, N.C.; Bischoff-Ferrari, H.A.; Gordon, C.M.; Hanley, D.A.; Heaney, R.P.; Murad, M.H.; Weaver, C.M. Evaluation, treatment, and prevention of vitamin D deficiency: An Endocrine Society clinical practice guideline. J. Clin. Endocrinol. Metab. 2011, 96, 1911–1930. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- He, C.; Lin, Z.; Robb, S.W.; Ezeamama, A.E. Serum Vitamin D Levels and Polycystic Ovary syndrome: A Systematic Review and Meta-Analysis. Nutrients 2015, 7, 4555–4577. [Google Scholar] [CrossRef] [Green Version]
- Glintborg, D.; Andersen, M. MANAGEMENT OF ENDOCRINE DISEASE: Morbidity in polycystic ovary syndrome. Eur. J. Endocrinol. 2017, 176, R53–R65. [Google Scholar] [CrossRef] [Green Version]
- Bischoff-Ferrari, H.A.; Willett, W.C.; Orav, E.J.; Lips, P.; Meunier, P.J.; Lyons, R.A.; Flicker, L.; Wark, J.; Jackson, R.D.; Cauley, J.A.; et al. A pooled analysis of vitamin D dose requirements for fracture prevention. N. Engl. J. Med. 2012, 367, 40–49. [Google Scholar] [CrossRef] [Green Version]
- Ferrari, S.; Bianchi, M.L.; Eisman, J.A.; Foldes, A.J.; Adami, S.; Wahl, D.A.; Stepan, J.J.; de Vernejoul, M.C.; Kaufman, J.M.; IOF Committee of Scientific Advisors Working Group on Osteoporosis Pathophysiology. Osteoporosis in young adults: Pathophysiology, diagnosis, and management. Osteoporos. Int. J. Establ. Result Coop. Eur. Found. Osteoporos. Natl. Osteoporos. Found. USA 2012, 23, 2735–2748. [Google Scholar] [CrossRef] [Green Version]
- Atteritano, M.; Mirarchi, L.; Venanzi-Rullo, E.; Santoro, D.; Iaria, C.; Catalano, A.; Lasco, A.; Arcoraci, V.; Lo Gullo, A.; Bitto, A.; et al. Vitamin D Status and the Relationship with Bone Fragility Fractures in HIV-Infected Patients: A Case Control Study. Int. J. Mol. Sci. 2018, 19, 119. [Google Scholar] [CrossRef] [Green Version]
- Bouillon, R.; Carmeliet, G.; Daci, E.; Segaert, S.; Verstuyf, A. Vitamin D metabolism and action. Osteoporos. Int. 1998, 8 (Suppl. 2), S13. [Google Scholar] [CrossRef]
- Mu, Y.; Cheng, D.; Yin, T.L.; Yang, J. Vitamin D and Polycystic Ovary Syndrome: A Narrative Review. Reprod. Sci. 2020. [Google Scholar] [CrossRef] [PubMed]
- Irani, M.; Merhi, Z. Role of vitamin D in ovarian physiology and its implication in reproduction: A systematic review. Fertil. Steril. 2014, 102, 460–468.e3. [Google Scholar] [CrossRef] [PubMed]
- Thomson, R.L.; Spedding, S.; Buckley, J. D Vitamin D in the aetiology and management of polycystic ovary syndrome. Clin. Endocrinol. 2012, 77, 343–350. [Google Scholar] [CrossRef] [PubMed]
- Muscogiuri, G.; Mitri, J.; Mathieu, C.; Badenhoop, K.; Tamer, G.; Orio, F.; Mezza, T.; Vieth, R.; Colao, A.; Pittas, A. Mechanisms in endocrinology: Vitamin D as a potential contributor in endocrine health and disease. Eur. J. Endocrinol. 2014, 171, R101–R110. [Google Scholar] [CrossRef] [Green Version]
- Ramagopalan, S.V.; Heger, A.; Berlanga, A.J.; Maugeri, N.J.; Lincoln, M.R.; Burell, A.; Handunnetthi, L.; Handel, A.E.; Disanto, G.; Orton, S.M.; et al. A chip-seq defined genome-wide map of vitamin d receptor binding: Associations with disease and evolution. Genome. Res. 2010, 20, 1352–1360. [Google Scholar] [CrossRef] [Green Version]
- Wacker, M.; Holick, M.F. Vitamin D—Effects on skeletal and extraskeletal health and the need for supplementation. Nutrients 2013, 5, 111–148. [Google Scholar] [CrossRef] [Green Version]
- Li, X.; Liu, Y.; Zheng, Y.; Wang, P.; Zhang, Y. The Effect of Vitamin D Supplementation on Glycemic Control in Type 2 Diabetes Patients: A Systematic Review and Meta-Analysis. Nutrients 2018, 10, 375. [Google Scholar] [CrossRef] [Green Version]
- Carnevale, V.; Inglese, M.; Annese, M.A.; De Matthaeis, A.; Santini, S.A.; Frusciante, V.; Fontana, A.; Copetti, M.; Pellegrini, F.; D’Amico, G. Vitamin D and parameters of calcium homeostasis in inpatients with and without Type 2 diabetes mellitus. J. Endocrinol. Investig. 2012, 35, 853–858. [Google Scholar] [CrossRef]
- Medrano, M.; Carrillo-Cruz, E.; Montero, I.; Perez-Simon, J.A. Vitamin D: Effect on Haematopoiesis and Immune System and Clinical Applications. Int. J. Mol. Sci. 2018, 19, 2663. [Google Scholar] [CrossRef] [Green Version]
- Gembillo, G.; Cernaro, V.; Siligato, R.; Curreri, F.; Catalano, A.; Santoro, D. Protective Role of Vitamin D in Renal Tubulopathies. Metabolites 2020, 10, 115. [Google Scholar] [CrossRef] [Green Version]
- Lasco, A.; Catalano, A.; Benvenga, S. Improvement of primary dysmenorrhea caused by a single oral dose of vitamin D: Results of a randomized, double-blind, placebo-controlled study. Arch. Intern. Med. 2012, 172, 366–367. [Google Scholar] [CrossRef] [Green Version]
- Vojdeman, F.J.; Madsen, C.M.; Frederiksen, K.; Durup, D.; Olsen, A.; Hansen, L.; Heegaard, A.M.; Lind, B.; Tjønneland, A.; Jørgensen, H.L.; et al. Vitamin D levels and cancer incidence in 217,244 individuals from primary health care in Denmark. Int. J. Cancer 2019, 145, 338–346. [Google Scholar] [CrossRef] [Green Version]
- Saponaro, F.; Marcocci, C.; Zucchi, R. Vitamin D status and cardiovascular outcome. J. Endocrinol. Investig. 2019, 42, 1285–1290. [Google Scholar] [CrossRef] [PubMed]
- Catalano, A.; Morabito, N.; Atteritano, M.; Basile, G.; Cucinotta, D.; Lasco, A. Vitamin D reduces musculoskeletal pain after infusion of zoledronic acid for postmenopausal osteoporosis. Calcif. Tissue Int. 2012, 90, 279–285. [Google Scholar] [CrossRef]
- Oteri, G.; Cicciù, M.; Peditto, M.; Catalano, A.; Loddo, S.; Pisano, M.; Lasco, A. Does Vitamin D3 Have an Impact on Clinical and Biochemical Parameters Related to Third Molar Surgery. J. Craniofacial Surg. 2016, 27, 469–476. [Google Scholar] [CrossRef]
- Catalano, A.; Morabito, N.; Basile, G.; Cucinotta, D.; Lasco, A. Calcifediol improves lipid profile in osteopenicatorvastatin-treated postmenopausal women. Eur. J. Clin. Investig. 2015, 45, 144–149. [Google Scholar] [CrossRef]
- Panfili, F.M.; Roversi, M.; D’Argenio, P.; Rossi, P.; Cappa, M.; Fintini, D. Possible role of vitamin D in Covid-19 infection in pediatric population. J. Endocrinol. Investig. 2020, 1–9, Advance online publication. [Google Scholar] [CrossRef]
- Zarnani, A.H.; Shahbazi, M.; Salek-Moghaddam, A.; Zareie, M.; Tavakoli, M.; Ghasemi, J.; Rezania, S.; Moravej, A.; Torkabadi, E.; Rabbani, H.; et al. Vitamin D3 receptor is expressed in the endometrium of cycling mice throughout the estrous cycle. Fertil. Steril. 2010, 93, 2738–2743. [Google Scholar] [CrossRef] [PubMed]
- Yoshizawa, T.; Handa, Y.; Uematsu, Y.; Takeda, K.; Sekine, K.; Yoshihara, Y.; Kawakami, T.; Arioka, K.; Sato, H.; Uchiyama, Y.; et al. Mice lacking the vitamin D receptor exhibit impaired bone formation, uterine hypoplasia and growth retardation after weaning. Nat. Genet. 1997, 16, 391–396. [Google Scholar] [CrossRef] [PubMed]
- Merhi, Z.; Doswell, A.; Krebs, K.; Cipolla, M. Vitamin D alters genes involved in follicular development and steroidogenesis in human cumulus granulosa cells. J. Clin. Endocrinol. Metab. 2014, 99, E1137–E1145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parikh, G.; Varadinova, M.; Suwandhi, P.; Araki, T.; Rosenwaks, Z.; Poretsky, L.; Seto-Young, D. Vitamin D regulates steroidogenesis and insulin-like growth factor binding protein-1 (IGFBP-1) production in human ovarian cells. Horm. Metab. Res. 2010, 42, 754–757. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moridi, I.; Chen, A.; Tal, O.; Reshef, T. The Association between Vitamin D and Anti-Müllerian Hormone: A Systematic Review and Meta-Analysis. Nutrients 2020, 12, 1567. [Google Scholar] [CrossRef]
- Malloy, P.J.; Peng, L.; Wang, J.; Feldman, D. Interaction of the vitamin D receptor with a vitamin D response element in the Mullerian-inhibiting substance (MIS) promoter: Regulation of MIS expression by calcitriol in prostate cancer cells. Endocrinology 2009, 150, 1580–1587. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pellatt, L.; Rice, S.; Dilaver, N.; Heshri, A.; Galea, R.; Brincat, M.; Brown, K.; Simpson, E.R.; Mason, H. D Anti-müllerian hormone reduces follicle sensitivity to follicle-stimulating hormone in human granulosa cells. Fertil. Steril. 2011, 96, 1246–1251.e1. [Google Scholar] [CrossRef] [PubMed]
- Yan, Y.; Chen, W.; Wang, J.; Huang, J.; Lv, J.; Zhao, H.; Guo, L. Serum anti-Müllerian hormone levels are associated with low bone mineral density in premenopausal women. Biomarkers 2020, 1–8, Advance online publication. [Google Scholar] [CrossRef]
- Chen, Y.; Zhi, X. Roles of Vitamin D in Reproductive Systems and Assisted Reproductive Technology. Endocrinology 2020, 161, bqaa023. [Google Scholar] [CrossRef]
- Bouillon, R.; Marcocci, C.; Carmeliet, G.; Bikle, D.; White, J.H.; Dawson-Hughes, B.; Lips, P.; Munns, C.F.; Lazaretti-Castro, M.; Giustina, A.; et al. Skeletal and Extraskeletal Actions of Vitamin D: Current Evidence and Outstanding Questions. Endocr. Rev. 2019, 40, 1109–1151. [Google Scholar] [CrossRef] [Green Version]
- Pilz, S.; Zittermann, A.; Obeid, R.; Hahn, A.; Pludowski, P.; Trummer, C.; Lerchbaum, E.; Pérez-López, F.R.; Karras, S.N.; März, W. The Role of Vitamin D in Fertility and during Pregnancy and Lactation: A Review of Clinical Data. Int. J. Environ. Res. Public Health 2018, 15, 2241. [Google Scholar] [CrossRef] [Green Version]
- Azhar, A.; Abid, F.; Rehman, R. Polycystic Ovary Syndrome, Subfertility and Vitamin D Deficiency. J. Coll. Physicians. Surg. Pak. 2020, 30, 545–546. [Google Scholar]
- Qazi, I.; Qazi, A.; Ijaz, F.; Jawed, S.; Aftab, R.; Qazi, S. Relationship of obesity with insulin resistance in polycystic ovarian syndrome. Pak. J. Physiol. 2018, 14, 46–49. [Google Scholar]
- Wang, L.; Lv, S.; Li, F.; Yu, X.; Bai, E.; Yang, X. Vitamin D Deficiency Is Associated With Metabolic Risk Factors in Women With Polycystic Ovary Syndrome: A Cross-Sectional Study in Shaanxi China. Front. Endocrinol. 2020, 11, 171. [Google Scholar] [CrossRef]
- Wehr, E.; Trummer, O.; Giuliani, A.; Gruber, H.J.; Pieber, T.R.; Obermayer-Pietsch, B. Vitamin D-associated polymorphisms are related to insulin resistance and vitamin D deficiency in polycystic ovary syndrome. Eur. J. Endocrinol. 2011, 164, 741–749. [Google Scholar] [CrossRef] [Green Version]
- Li, H.W.R.; Brereton, R.E.; Anderson, R.A.; Wallace, A.M.; Ho, C.K.M. Vitamin D deficiency is common and associated with metabolic risk factors in patients with polycystic ovary syndrome. Metabolism 2011, 60, 1475–1481. [Google Scholar] [CrossRef] [PubMed]
- Panidis, D.; Balaris, C.; Farmakiotis, D.; Rousso, D.; Kourtis, A.; Balaris, V.; Katsikis, I.; Zournatzi, V.; Diamanti-Kandarakis, E. Serum parathyroid hormone concentrations are increased in women with polycystic ovary syndrome. Clin. Chem. 2005, 51, 1691–1697. [Google Scholar] [CrossRef]
- Kanis, J.A.; Cooper, C.; Rizzoli, R.; Abrahamsen, B.; Al-Daghri, N.M.; Brandi, M.L.; Cannata-Andia, J.; Cortet, B.; Dimai, H.P.; Ferrari, S.; et al. European Society for Clinical and Economic Aspects of Osteoporosis, Osteoarthritis and Musculoskeletal Diseases (ESCEO) Identification and management of patients at increased risk of osteoporotic fracture: Outcomes of an ESCEO expert consensus meeting. Osteoporos. Int. A J. Establ. Result Coop. Eur. Found. Osteoporos. Natl. Osteoporos. Found. USA 2017, 28, 2023–2034. [Google Scholar] [CrossRef] [Green Version]
- Liu, J.; Curtis, E.M.; Cooper, C.; Harvey, N.C. State of the art in osteoporosis risk assessment and treatment. J. Endocrinol. Investig. 2019, 42, 1149–1164. [Google Scholar] [CrossRef] [Green Version]
- Reis, G.V.; Gontijo, N.A.; Rodrigues, K.F.; Alves, M.T.; Ferreira, C.N.; Gomes, K.B. Vitamin D receptor polymorphisms and the polycystic ovary syndrome: A systematic review. J. Obstet. Gynaecol. Res. 2017, 43, 436–446. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Colonese, F.; Laganà, A.S.; Colonese, E.; Sofo, V.; Salmeri, F.M.; Granese, R.; Triolo, O. The pleiotropic effects of vitamin D in gynaecological and obstetric diseases: An overview on a hot topic. Biomed. Res. Int. 2015, 2015, 986281. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Daghri, N.M.; Al-Attas, O.S.; Alkharfy, K.M.; Khan, N.; Mohammed, A.K.; Vinodson, B.; Ansari, M.G.A.; Alenad, A.; Alokail, M.S. Association of VDR-gene variants with factors related to the metabolic syndrome, type 2 diabetes and vitamin D deficiency. Gene 2014, 542, 129–133. [Google Scholar] [CrossRef] [PubMed]
- Dasgupta, S.; Dutta, J.; Annamaneni, S.; Kudugunti, N.; Battini, M.R. Association of vitamin D receptor gene polymorphisms with polycystic ovary syndrome among Indian women. Indian J. Med. Res. 2015, 142, 276–285. [Google Scholar] [PubMed] [Green Version]
- Massart, F.; Marcucci, G.; Brandi, M.L. Pharmacogenetics of bone treatments: The VDR and ERalpha gene story. Pharmacogenomics 2008, 9, 733–746. [Google Scholar] [CrossRef] [PubMed]
- Gaudio, A.; Morabito, N.; Catalano, A.; Rapisarda, R.; Xourafa, A.; Lasco, A. Pathogenesis of Thalassemia Major-associated Osteoporosis: A Review with Insights from Clinical Experience. J. Clin. Res. Pediatric Endocrinol. 2019, 11, 110–117. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Yin, X.; Wang, J.; Xu, D.; Wang, Y.; Yang, J.; Tao, Y.; Zhang, S.; Feng, X.; Yan, C. Associations between VDR Gene Polymorphisms and Osteoporosis Risk and Bone Mineral Density in Postmenopausal Women: A systematic review and Meta-Analysis. Sci. Rep. 2018, 8, 981. [Google Scholar] [CrossRef] [Green Version]
- Gennari, L.; Merlotti, D.; De Paola, V.; Martini, G.; Nuti, R. Update on the pharmacogenetics of the vitamin D receptor and osteoporosis. Pharmacogenomics 2009, 10, 417–433. [Google Scholar] [CrossRef] [PubMed]
- Jager, J.; Gremeaux, T.; Cormont, M.; Le Marchand-Brustel, Y.; Tanti, J.F. Interleukin-1beta-induced insulin resistance in adipocytes through down-regulation of insulin receptor substrate-1 expression. Endocrinology 2007, 148, 241–251. [Google Scholar] [CrossRef]
- Hahn, S.; Haselhorst, U.; Tan, S.; Quadbeck, B.; Schmidt, M.; Roesler, S.; Kimmig, R.; Mann, K.; Janssen, O.E. Low serum 25-hydroxyvitamin D concentrations are associated with insulin resistance and obesity in women with polycystic ovary syndrome. Exp. Clin. Endocrinol. Diabetes 2006, 114, 577–583. [Google Scholar] [CrossRef]
- Wehr, E.; Pilz, S.; Schweighofer, N.; Giuliani, A.; Kopera, D.; Pieber, T.R.; Obermayer-Pietsch, B. Association of hypovitaminosis D with metabolic disturbances in polycystic ovary syndrome. Eur. J. Endocrinol. 2009, 161, 575–582. [Google Scholar] [CrossRef] [Green Version]
- Muscogiuri, G.; Policola, C.; Prioletta, A.; Sorice, G.; Mezza, T.; Lassandro, A.; Della Casa, S.; Pontecorvi, A.; Giaccari, A. Low levels of 25(OH)D and insulin-resistance: 2 unrelated features or a cause–effect in PCOS? Clin. Nutr. 2012, 31, 47–480. [Google Scholar] [CrossRef]
- Voulgaris, N.; Papanastasiou, L.; Piaditis, G.; Angelousi, A.; Kaltsas, G.; Mastorakos, G.; Kassi, E. Vitamin D and aspects of female fertility. Hormones 2017, 16, 5–21. [Google Scholar]
- Plymate, S.R.; Matej, L.A.; Jones, R.E.; Friedl, K.E. Inhibition of sex hormone-binding globulin production in the human hepatoma (Hep G2) cell line by insulin and prolactin. J. Clin. Endocrinol. Metab. 1988, 67, 460–464. [Google Scholar] [CrossRef]
- Bargiota, A.; Diamanti-Kandarakis, E. The effects of old, new and emerging medicines on metabolic aberrations in PCOS. Ther. Adv. Endocrinol. Metab. 2012, 3, 27–47. [Google Scholar] [CrossRef]
- Alvarez, J.A.; Ashraf, A. Role of vitamin D in insulin secretion and insulin sensitivity for glucose homeostasis. Int. J. Endocrinol. 2012, 351385, 1–19. [Google Scholar] [CrossRef] [Green Version]
- Krul-Poel, Y.H.M.; Snackey, C.; Louwers, Y.; Lips, P.; Lambalk, C.B.; Laven, J.S.E.; Simsek, S. The role of vitamin D in metabolic disturbances in polycystic ovary syndrome: A systematic review. Eur. J. Endocrinol. 2013, 169, 853–865. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Teegarden, D.; Donkin, S.S. Vitamin D: Emerging new roles in insulin sensitivity. Nutr. Res. Rev. 2009, 22, 82–92. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Piovezan, J.M.; Premaor, M.O.; Comim, F.V. Negative impact of polycystic ovary syndrome on bone health: A systematic review and meta-analysis. Hum. Reprod. Update 2019, 25, 633–645. [Google Scholar] [CrossRef] [PubMed]
- Russo, G.T.; Giandalia, A.; Romeo, E.L.; Nunziata, M.; Muscianisi, M.; Ruffo, M.C.; Catalano, A.; Cucinotta, D. Fracture Risk in Type 2 Diabetes: Current Perspectives and Gender Differences. Int. J. Endocrinol. 2016, 2016, 1615735. [Google Scholar] [CrossRef] [Green Version]
- Clemens, T.L.; Karsenty, G. The osteoblast: An insulin target cell controlling glucose homeostasis. J. Bone Miner. Res. Off. J. Am. Soc. Bone Miner. Res. 2011, 26, 677–680. [Google Scholar] [CrossRef]
- Shojaeian, Z.; Sadeghi, R.; Roudsari, R.L. Calcium and vitamin D supplementation effects on metabolic factors, menstrual cycles and follicular responses in women with polycystic ovary syndrome: A systematic review and meta-analysis. Casp. J. Int. Med. 2019, 10, 359–369. [Google Scholar]
- Firouzabadi, R.D.; Aflatoonian, A.; Modarresi, S.; Sekhavat, L.; MohammadTaheri, S. Therapeutic effects of calcium & vitamin D supplementation in women with PCOS. Complement Ther. Clin. Pract. 2012, 18, 85–88. [Google Scholar] [PubMed]
- Pal, L.; Berry, A.; Coraluzzi, L.; Kustan, E.; Danton, C.; Shaw, J.; Taylor, H. Therapeutic implications of vitamin D and calcium in overweight women with polycystic ovary syndrome. Gynecol. Endocrinol. 2012, 8, 965–968. [Google Scholar] [CrossRef]
- Łagowska, K.; Bajerska, J.; Jamka, M. The role of vitamin D oral supplementation in insulin resistance in women with polycystic ovary syndrome: A systematic review and meta-analysis of randomized controlled trials. Nutrients 2018, 2, 10–11. [Google Scholar]
- Menichini, D.; Facchinetti, F. Effects of vitamin D supplementation in women with polycystic ovary syndrome: A review. Gynecol. Endocrinol. 2020, 36, 1–5. [Google Scholar] [CrossRef]
- Wang, L.; Wen, X.; Lv, S.; Tian, S.; Jiang, Y.; Yang, X. Effects of vitamin D supplementation on metabolic parameters of women with polycystic ovary syndrome: A meta-analysis of randomized controlled trials. Gynecol. Endocrinol. 2020, 10, 1–10. [Google Scholar] [CrossRef]
- Selimoglu, H.; Duran, C.; Kiyici, S.; Ersoy, C.; Guclu, M.; Ozkaya, G.; Tuncel, E.; Erturk, E.; Imamoglu, S. The effect of vitamin D replacement therapy on insulin resistance and androgen levels in women with polycystic ovary syndrome. J. Endocrinol. Invest. 2010, 33, 234–238. [Google Scholar] [CrossRef] [PubMed]
- Aversa, A.; La Vignera, S.; Rago, R.; Gambineri, A.; Nappi, R.E.; Calogero, A.E.; Ferlin, A. Fundamental Concepts and Novel Aspects of Polycystic Ovarian Syndrome: Expert Consensus Resolutions. Front. Endocrinol. 2020, 11, 516. [Google Scholar] [CrossRef]
- Cândido, F.G.; Bressan, J. Vitamin D: Link between osteoporosis, obesity, and diabetes? Int. J. Mol. Sci. 2014, 15, 6569–6591. [Google Scholar] [CrossRef] [Green Version]
- Teede, H.; Deeks, A.; Moran, L. Polycystic ovary syndrome: A complex condition with psychological, reproductive and metabolic manifestations that impacts on health across the lifespan. BMC Med. 2010, 8, 41. [Google Scholar] [CrossRef] [Green Version]
- Diamanti-Kandarakis, E.; Papalou, O.; Kandaraki, E.A. The Role of Androgen Excess on Insulin Sensitivity in Women. Front. Horm. Res. 2019, 53, 50–64. [Google Scholar] [PubMed]
- Abu, E.O.; Horner, A.; Kusec, V.; Triffitt, J.T.; Compston, J.E. The localization of androgen receptors in human bone. J. Clin. Endocrinol. Metab. 1997, 82, 3493–3497. [Google Scholar] [CrossRef] [PubMed]
- Krishnan, A.; Muthusami, S. Hormonal alterations in PCOS and its influence on bone metabolism. J. Endocrinol. 2017, 232, R99–R113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Velija-Asimi, Z. Evaluation of the association of vitamin D deficiency with gonadotropins and sex hormone in obese and non-obese women with polycystic ovary syndrome. Med. Glas. 2014, 11, 170–176. [Google Scholar]
- Azadi-Yazdi, M.; Nadjarzade, A.; Khosravi-Boroujeni, H.; Salehi-Abargouei, A. The effect of vitamin D supplementation on the androgenic profile in patients with polycystic ovary syndrome: A systematic review and meta-analysis of clinical trials. Horm. Metab. Res. 2017, 49, 174–179. [Google Scholar] [CrossRef] [Green Version]
- Miao, C.Y.; Fang, X.J.; Chen, Y.; Zhang, Q. Effect of vitamin D supplementation on polycystic ovary syndrome: A meta-analysis. Exp. Ther. Med. 2020, 19, 2641–2649. [Google Scholar] [CrossRef] [Green Version]
- Razavi, M.; Jamilian, M.; Karamali, M.; Bahmani, F.; Aghadavod, E.; Asemi, Z. The effects of vitamin d-k-calcium co-supplementation on endocrine, inflammation, and oxidative stress biomarkers in vitamin d-deficient women with polycystic ovary syndrome: A randomized, double-blind, placebo-controlled trial. Horm. Metab. Res. 2016, 48, 446–451. [Google Scholar] [PubMed]
- Mahalingaiah, S.; Diamanti-Kandarakis, E. Targets to treat metabolic syndrome in polycystic ovary syndrome. Expert Opin. Ther. Target 2015, 19, 1561–1574. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Williams, A.; Babu, J.R.; Wadsworth, D.D.; Burnett, D.; Geetha, T. The Effects of Vitamin D on Metabolic Profiles in Women with Polycystic Ovary Syndrome: A Systematic Review. Horm. Metab. Res. 2020, 52, 485–491. [Google Scholar] [PubMed]
- Al-Bayyari, N.; Al-Domi, H.; Zayed, F.; Hailat, R.; Eaton, A. Androgens and hirsutism score of overweight women with polycystic ovary syndrome improved after vitamin D treatment: A randomized placebo controlled clinical trial. Clin. Nutr. 2020, S0261-5614(20)30496. [Google Scholar] [CrossRef]
- Shi, H.; Wang, T.; Wang, Q.; Lin, L.; Zhao, Z.; Wang, Z.; Hu, Y. Relationship between vitamin D levels and oxidative stress indicators and related inflammatory factors in patients with polycystic ovary syndrome. Minerva Med. 2020. [Google Scholar] [CrossRef]
- Merhi, Z.; Kandaraki, E.A.; Diamanti-Kandarakis, E. Implications and Future Perspectives of AGEs in PCOS Pathophysiology. Trends Endocrinol. Metab. 2019, 30, 150–162. [Google Scholar] [CrossRef]
- Diamanti-Kandarakis, E.; Piperi, C.; Patsouris, E.; Korkolopoulou, P.; Panidis, D.; Pawelczyk, L.; Papavassiliou, A.G.; Duleba, A.J. Immunohistochemical localization of advanced glycation end-products (AGEs) and their receptor (RAGE) in polycystic and normal ovaries. Histochem. Cell Biol. 2007, 127, 581–589. [Google Scholar] [CrossRef]
- Diamanti-Kandarakis, E.; Katsikis, I.; Piperi, C.; Kandaraki, E.; Piouka, A.; Papavassiliou, A.G.; Panidis, D. Increased serum advanced glycation end-products is a distinct finding in lean women with polycystic ovary syndrome (PCOS). Clin. Endocrinol. 2008, 69, 634–641. [Google Scholar] [CrossRef]
- Garg, D.; Grazi, R.; Lambert-Messerlian, G.M.; Merhi, Z. Correlation between follicular fluid levels of sRAGE and vitamin D in women with PCOS. J. Assist. Reprod. Genet. 2017, 34, 1507–1513. [Google Scholar] [CrossRef] [PubMed]
- Masjedi, F.; Keshtgar, S.; Zal, F.; Talaei-Khozani, T.; Sameti, S.; Fallahi, S.; Kazeroni, M. Effects of vitamin D on steroidogenesis, reactive oxygen species production, and enzymatic antioxidant defense in human granulosa cells of normal and polycystic ovaries. J. Steroid. Biochem. Mol. Biol. 2020, 197, 105521. [Google Scholar] [CrossRef]
- Merhi, Z.; Fadiel, A.; Buyuk, E.; Naftolin, F.; Cipolla, M. Vitamin D attenuates the adverse effect of advanced glycation end products on human granulosa cells: Implications for women with PCOS. Fertil. Steril. 2015, 104, e106. [Google Scholar] [CrossRef]
- Merhi, Z.; Wang, S.; Cipolla, M.J. Special research presentation: Vitamin D reverses the adverse effects of advanced glycation end products on granulosa cells. Fertil. Steril. 2016, 106, e76. [Google Scholar] [CrossRef]
- Eller-Vainicher, C.; Cairoli, E.; Grassi, G.; Grassi, F.; Catalano, A.; Merlotti, D.; Falchetti, A.; Gaudio, A.; Chiodini, I.; Gennari, L. Pathophysiology and Management of Type 2 Diabetes Mellitus Bone Fragility. J. Diabetes Res. 2020, 2020, 7608964. [Google Scholar] [CrossRef] [PubMed]
- Corrado, A.; Cici, D.; Rotondo, C.; Maruotti, N.; Cantatore, F.P. Molecular Basis of Bone Aging. Int. J. Mol. Sci. 2020, 21, 3679. [Google Scholar] [CrossRef] [PubMed]
- Sanguineti, R.; Monacelli, F.; Parodi, A.; Furfaro, A.L.; Borghi, R.; Pacini, D.; Pronzato, M.A.; Odetti, P.; Molfetta, L.; Traverso, N. Vitamins D3 and K2 may partially counterbalance the detrimental effects of pentosidine in ex vivo human osteoblasts. J. Biol. Regul. Homeost. Agents 2016, 30, 713–726. [Google Scholar]
- Parikh, S.J.; Edelman, M.; Uwaifo, G.I.; Freedman, R.J.; Semega-Janneh, M.; Reynolds, J.; Yanovski, J. A The relationship between obesity and serum 1,25-dihydroxy-vitamin D concentrations in healthy adults. J. Clin. Endocrinol. Metab. 2004, 89, 1196–1199. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hamoui, N.; Anthone, G.; Crookes, P.F. Calcium metabolism in the morbidly obese. Obes. Surg. 2004, 14, 9–12. [Google Scholar] [CrossRef]
- McCarthy, M.F.; Thomas, C.A. PTH excess may promote weight gain by impeding catecholamine-induced lipolysis-implications for the impact of calcium, vitamin D, and alcohol on body weight. Med. Hypotheses 2004, 61, 535–542. [Google Scholar] [CrossRef]
- Thys-Jacobs, S.; Donovan, D.; Papadopoulos, A.; Sarrel, P.; Bilezikian, J.P. Vitamin D and calcium dysregulation in the polycystic ovarian syndrome. Steroids 1999, 6, 430–435. [Google Scholar] [CrossRef]
- Davis, E.M.; Peck, K.D.; Hansen, K.R.; Neas, B.R.; Craig, L.B. Associations between vitamin D levels and polycystic ovary syndrome phenotypes. Minerva Endocrinol. 2019, 44, 176–184. [Google Scholar] [CrossRef] [PubMed]
- Raisz, L.G. Pathogenesis of osteoporosis: Concepts, conflicts, and prospects. J. Clin. Invest. 2005, 115, 3318–3325. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lasco, A.; Catalano, A.; Morabito, N.; Gaudio, A.; Basile, G.; Trifiletti, A.; Atteritano, M. Adrenal effects of teriparatide in the treatment of severe postmenopausal osteoporosis. Osteoporos. Int. 2011, 22, 299–303. [Google Scholar] [CrossRef] [PubMed]
- Radetti, G.; Franceschi, R.; Adami, S.; Longhi, S.; Rossini, M.; Gatti, D. Higher circulating parathormone is associated with smaller and weaker bones in obese children. Calcif. Tissue Int. 2014, 95, 1–7. [Google Scholar] [CrossRef]
- Rubin, K.H.; Glintborg, D.; Nybo, M.; Andersen, M.; Abrahamsen, B. Fracture Risk Is Decreased in Women with Polycystic Ovary Syndrome: A Register-Based and Population-Based Cohort Study. J. Bone Miner. Res. Off. J. Am. Soc. Bone Miner. Res. 2016, 31, 709–717. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, H.Y.; Lee, H.S.; Huang, W.T.; Chen, M.J.; Chen, S.C.; Hsu, Y.H. Increased risk of fractures in patients with polycystic ovary syndrome: A nationwide population-based retrospective cohort study. J. Bone Miner. Metab. 2018, 36, 741–748. [Google Scholar] [CrossRef]
- Siris, E.S.; Chen, Y.T.; Abbott, T.A.; Barrett-Connor, E.; Miller, P.D.; Wehren, L.E.; Berger, M.L. Bone mineral density thresholds for pharmacological intervention to prevent fractures. Arch. Intern. Med. 2004, 164, 1108–1112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yüksel, O.; Dökmetaş, H.S.; Topcu, S.; Erselcan, T.; Sencan, M. Relationship between bone mineral density and insulin resistance in polycystic ovary syndrome. J. Bone Miner. Metab. 2001, 19, 257–262. [Google Scholar] [CrossRef] [PubMed]
- Katulski, K.; Slawek, S.; Czyzyk, A.; Podfigurna-Stopa, A.; Paczkowska, K.; Ignaszak, N.; Podkowa, N.; Meczekalski, B. Bone mineral density in women with polycystic ovary syndrome. J. Endocrinol. Investig. 2014, 37, 1219–1224. [Google Scholar] [CrossRef] [Green Version]
- Kalyan, S.; Patel, M.S.; Kingwell, E.; Côté, H.; Liu, D.; Prior, J.C. Competing Factors Link to Bone Health in Polycystic Ovary Syndrome: Chronic Low-Grade Inflammation Takes a Toll. Sci. Rep. 2017, 7, 3432. [Google Scholar] [CrossRef]
- Karadağ, C.; Yoldemir, T.; Gogas Yavuz, D. Determinants of low bone mineral density in premenopausal polycystic ovary syndrome patients. Gynecol. Endocrinol. 2017, 33, 234–237. [Google Scholar] [CrossRef]
- Attlee, A.; Nusralla, A.; Eqbal, R.; Said, H.; Hashim, M.; Obaid, R.S. Polycystic ovary syndrome in university students: Occurrence and associated factors. Int. J. Fertil. Steril. 2014, 8, 261–266. [Google Scholar]
- Kirchengast, S.; Huber, J. Body composition characteristics and body fat distribution in lean women with polycystic ovary syndrome. Hum. Reprod. 2001, 16, 1255–1260. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adami, S.; Zamberlan, N.; Castello, R.; Tosi, F.; Gatti, D.; Moghetti, P. Effect of hyperandrogenism and menstrual cycle abnormalities on bone mass and bone turnover in young women. Clin. Endocrinol. 1998, 48, 169–173. [Google Scholar] [CrossRef]
- Noyan, V.; Yucel, A.; Sagsoz, N. The association of bone mineral density with insulin resistance in patients with polycystic ovary syndrome. Eur. J. Obstet. Gynecol. Reprod. Biol. 2004, 115, 200–205. [Google Scholar] [CrossRef]
- Good, C.; Tulchinsky, M.; Mauger, D.; Demers, L.M.; Legro, R.S. Bone mineral density and body composition in lean women with polycystic ovary syndrome. Fertil. Steril. 1999, 72, 21–25. [Google Scholar] [CrossRef]
- Glintborg, D.; Hermann, A.P.; Rasmussen, L.M.; Andersen, M. Plasma osteoprotegerin is associated with testosterone levels but unaffected by pioglitazone treatment in patients with polycystic ovary syndrome. J. Endocrinol. Investig. 2013, 36, 460–465. [Google Scholar] [CrossRef]
- Gao, S.; Cheng, Y.; Zhao, L.; Chen, Y.; Liu, Y. The relationships of irisin with bone mineral density and body composition in PCOS patients. Diabetes/Metab. Res. Rev. 2016, 32, 421–428. [Google Scholar] [CrossRef]
- McBreairty, L.E.; Zello, G.A.; Gordon, J.J.; Serrao, S.B.; Pierson, R.A.; Chizen, D.R.; Chilibeck, P.D. Women With Polycystic Ovary Syndrome Have Comparable Hip Bone Geometry to Age-Matched Control Women. J. Clin. Densitom. Off. J. Int. Soc. Clin. Densitom. 2018, 21, 54–60. [Google Scholar] [CrossRef]
- Schmidt, J.; Dahlgren, E.; Brännström, M.; Landin-Wilhelmsen, K. Body composition, bone mineral density and fractures in late postmenopausal women with polycystic ovary syndrome—A long-term follow-up study. Clin. Endocrinol. 2012, 77, 207–214. [Google Scholar] [CrossRef] [PubMed]
- Albaik, M.; Khan, J.A.; Ardawi, M. Vitamin D status in Polycystic Ovarian Women: Case-Control Study. IOF Regionals Singapore 6th Asia-Pacific Osteoporosis Meeting. Osteoporos. Int. 2016, 27 (Suppl. 3), S709–S787. [Google Scholar]
- Berberoglu, Z.; Aktas, A.; Fidan, Y.; Yazici, A.C.; Aral, Y. Association of plasma GDF-9 or GDF-15 levels with bone parameters in polycystic ovary syndrome. J. Bone Miner. Metab. 2015, 33, 101–108. [Google Scholar] [CrossRef] [PubMed]
- Kassanos, D.; Trakakis, E.; Baltas, C.S.; Papakonstantinou, O.; Simeonidis, G.; Salamalekis, G.; Grammatikakis, I.; Basios, G.; Labos, G.; Skarantavos, G.; et al. Augmentation of cortical bone mineral density in women with polycystic ovary syndrome: A peripheral quantitative computed tomography (pQCT) study. Hum. Reprod. 2010, 25, 2107–2114. [Google Scholar] [CrossRef] [PubMed]
- Carmina, E.; Guastella, E.; Longo, R.A.; Rini, G.B.; Lobo, R.A. Correlates of increased lean muscle mass in women with polycystic ovary syndrome. Eur. J. Endocrinol. 2009, 161, 583–589. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Glintborg, D.; Andersen, M.; Hagen, C.; Heickendorff, L.; Hermann, A.P. Association of pioglitazone treatment with decreased bone mineral density in obese premenopausal patients with polycystic ovary syndrome: A randomized, placebo-controlled trial. J. Clin. Endocrinol. Metab. 2008, 93, 1696–1701. [Google Scholar] [CrossRef]
- Diamanti-Kandarakis, E.; Livadas, S.; Katsikis, I.; Piperi, C.; Mantziou, A.; Papavassiliou, A.G.; Panidis, D. Serum concentrations of carboxylated osteocalcin are increased and associated with several components of the polycystic ovarian syndrome. J. Bone Miner. Metab. 2011, 29, 201–206. [Google Scholar] [CrossRef] [PubMed]
- Lingaiah, S.; Morin-Papunen, L.; Piltonen, T.; Puurunen, J.; Sundström-Poromaa, I.; Stener-Victorin, E.; Bloigu, R.; Risteli, J.; Tapanainen, J.S. Bone markers in polycystic ovary syndrome: A multicentre study. Clin. Endocrinol. 2017, 87, 673–679. [Google Scholar] [CrossRef] [PubMed]
- Pepene, C.E. Serum under-carboxylated osteocalcin levels in women with polycystic ovary syndrome: Weight-dependent relationships with endocrine and metabolic traits. J. Ovarian Res. 2013, 6, 4. [Google Scholar] [CrossRef] [Green Version]
- Damone, A.L.; Joham, A.E.; Loxton, D.; Earnest, A.; Teede, H.J.; Moran, L.J. Depression, anxiety and perceived stress in women with and without PCOS: A community-based study. Psychol. Med. 2019, 49, 1510–1520. [Google Scholar] [CrossRef] [PubMed]
- Lerner, P.P.; Sharony, L.; Miodownik, C. Association between mental disorders, cognitive disturbances and vitamin D serum level: Current state. Clin. Nutr. ESPEN 2018, 23, 89–102. [Google Scholar] [CrossRef] [PubMed]
- Llewellyn, D.J.; Lang, I.A.; Langa, K.M.; Muniz-Terrera, G.; Phillips, C.L.; Cherubini, A.; Ferrucci, L.; Melzer, D. Vitamin D and risk of cognitive decline in elderly persons. Arch. Intern. Med. 2010, 170, 1135–1141. [Google Scholar] [CrossRef] [PubMed]
- Bigman, G. Vitamin D metabolites, D3 and D2, and their independent associations with depression symptoms among adults in the United States. Nutr. Neurosci. 2020, 1–9, Advance online publication. [Google Scholar] [CrossRef]
- Köhnke, C.; Herrmann, M.; Berger, K. Associations of major depressive disorder and related clinical characteristics with 25-hydroxyvitamin D levels in middle-aged adults. Nutr. Neurosci. 2020, 1–10, Advance online publication. [Google Scholar] [CrossRef]
- Camargo, A.; Dalmagro, A.P.; Platt, N.; Rosado, A.F.; Neis, V.B.; Zeni, A.L.B.; Kaster, M.P.; Rodrigues, A.L.S. Cholecalciferol abolishes depressive-like behavior and hippocampal glucocorticoid receptor impairment induced by chronic corticosterone administration in mice. Pharmacol. Biochem. Behav. 2020, 196, 172971. [Google Scholar] [CrossRef]
- Bakhtiari-Dovvombaygi, H.; Izadi, S.; Zare Moghaddam, M.; Hashemzehi, M.; Hosseini, M.; Azhdari-Zarmehri, H.; Dinpanah, H.; Beheshti, F. Beneficial effects of vitamin D on anxiety and depression-like behaviors induced by unpredictable chronic mild stress by suppression of brain oxidative stress and neuroinflammation in rats. Naunyn-Schmiedeberg’s Arch. Pharmacol. 2020. Advance online publication. [Google Scholar] [CrossRef]
- Cheng, Y.C.; Huang, Y.C.; Huang, W.L. The effect of vitamin D supplement on negative emotions: A systematic review and meta-analysis. Depress. Anxiety 2020, 37, 549–564. [Google Scholar] [CrossRef]
- Moran, L.J.; Teede, H.J.; Vincent, A.J. Vitamin D is independently associated with depression in overweight women with and without PCOS. Gynecol. Endocrinol. Off. J. Int. Soc. Gynecol. Endocrinol. 2015, 31, 179–182. [Google Scholar] [CrossRef]
- Eskandari, F.; Martinez, P.E.; Torvik, S.; Phillips, T.M.; Sternberg, E.M.; Mistry, S.; Ronsaville, D.; Wesley, R.; Toomey, C.; Sebring, N.G.; et al. Premenopausal, Osteoporosis Women, Alendronate, Depression (POWER) Study Group Low bone mass in premenopausal women with depression. Arch. Intern. Med. 2007, 167, 2329–2336. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Catalano, A.; Martino, G.; Bellone, F.; Gaudio, A.; Lasco, C.; Langher, V.; Lasco, A.; Morabito, N. Anxiety levels predict fracture risk in postmenopausal women assessed for osteoporosis. Menopause 2018, 25, 1110–1115. [Google Scholar] [CrossRef]
- Atteritano, M.; Lasco, A.; Mazzaferro, S.; Macrì, I.; Catalano, A.; Santangelo, A.; Bagnato, G.; Bagnato, G.; Frisina, N. Bone mineral density, quantitative ultrasound parameters and bone metabolism in postmenopausal women with depression. Intern. Emerg. Med. 2013, 8, 485–491. [Google Scholar] [CrossRef] [PubMed]
- Hong-Jhe, C.; Chin-Yuan, K.; Ming-Shium, T.; Fu-Wei, W.; Ru-Yih, C.; Kuang-Chieh, H.; Hsiang-Ju, P.; Ming-Yueh, C.; Pan-Ming, C.; Chih-Chuan, P. The incidence and risk of osteoporosis in patients with anxiety disorder: A Population-based retrospective cohort study. Medicine 2016, 95, e4912. [Google Scholar] [CrossRef] [PubMed]
- Ju, S.Y.; Lee, Y.J.; Jeong, S.N. Serum 25-hydroxyvitamin D levels and the risk of depression: A systematic review and meta-analysis. J. Nutr. Health Aging 2013, 17, 447–455. [Google Scholar] [CrossRef]
- Martino, G.; Catalano, A.; Bellone, F.; Sardella, A.; Lasco, C.; Caprì, T.; Langher, V.; Caputo, A.; Fabio, R.A.; Morabito, N. Vitamin D status is associated with anxiety levels in postmenopausal women evaluated for osteoporosis. Mediterr. J. Clin. Psychol. 2018, 6. [Google Scholar] [CrossRef]
- Martino, G.; Catalano, A.; Bellone, F.; Langher, V.; Lasco, C.; Penna, A.; Nicocia, G.; Morabito, N. Quality of life in postmenopausal women: Which role for vitamin D? Mediterr. J. Clin. Psychol. 2018, 6. [Google Scholar] [CrossRef]
- Martino, G.; Catalano, A.; Bellone, F.; Russo, G.T.; Vicario, C.M.; Lasco, A.; Quattropani, M.C.; Morabito, N. As Time Goes by: Anxiety Negatively Affects the Perceived Quality of Life in Patients With Type 2 Diabetes of Long Duration. Front. Psychol. 2019, 10, 1779. [Google Scholar] [CrossRef] [Green Version]
Figure 1.
Hypovitaminosis D is associated with several facets of polycystic ovary syndrome, which per se are also related to fracture risk.
Figure 1.
Hypovitaminosis D is associated with several facets of polycystic ovary syndrome, which per se are also related to fracture risk.

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Di Bari, F.; Catalano, A.; Bellone, F.; Martino, G.; Benvenga, S. Vitamin D, Bone Metabolism, and Fracture Risk in Polycystic Ovary Syndrome. Metabolites 2021, 11, 116. https://0-doi-org.brum.beds.ac.uk/10.3390/metabo11020116
AMA Style
Di Bari F, Catalano A, Bellone F, Martino G, Benvenga S. Vitamin D, Bone Metabolism, and Fracture Risk in Polycystic Ovary Syndrome. Metabolites. 2021; 11(2):116. https://0-doi-org.brum.beds.ac.uk/10.3390/metabo11020116
Chicago/Turabian StyleDi Bari, Flavia, Antonino Catalano, Federica Bellone, Gabriella Martino, and Salvatore Benvenga. 2021. "Vitamin D, Bone Metabolism, and Fracture Risk in Polycystic Ovary Syndrome" Metabolites 11, no. 2: 116. https://0-doi-org.brum.beds.ac.uk/10.3390/metabo11020116
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.