
Identification of Potential Distinguishing Markers for the Use of Cannabis-Based Medicines or Street Cannabis in Serum Samples

Abstract
:1. Introduction
2. Results and Discussion
2.1. Demographics and Therapy of Study Population
2.2. Quantitative Study Sample Analysis
2.2.1. Sativex®
2.2.2. Sativex® and Medical Cannabis
2.2.3. Medical Cannabis
2.2.4. Dronabinol and Street Cannabis
2.2.5. Dronabinol
2.2.6. Dr. Nice Rebound CBD Capsules
2.3. Comparison to Forensic Serum Samples and Identification of Potential Distinguishing Markers
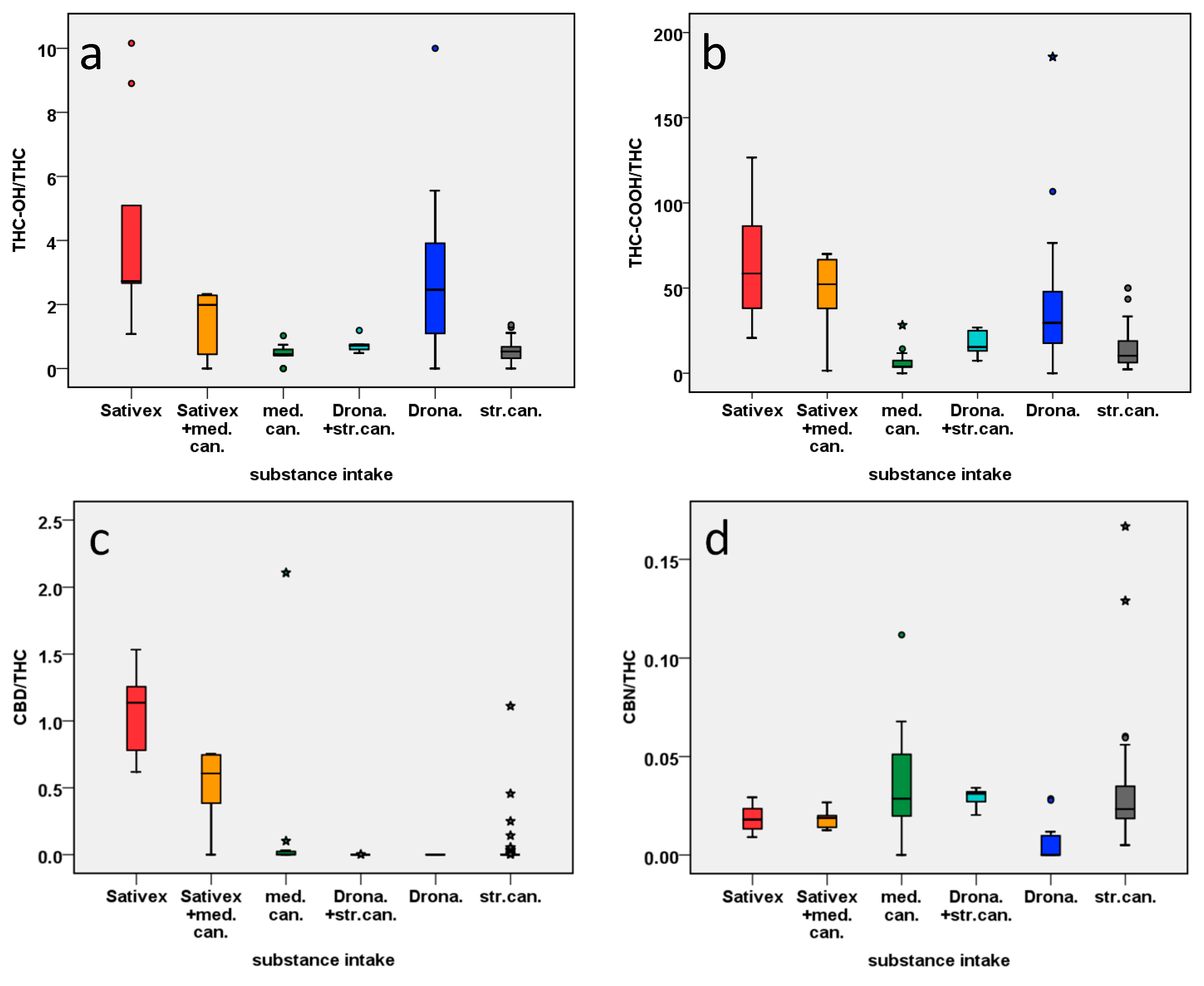
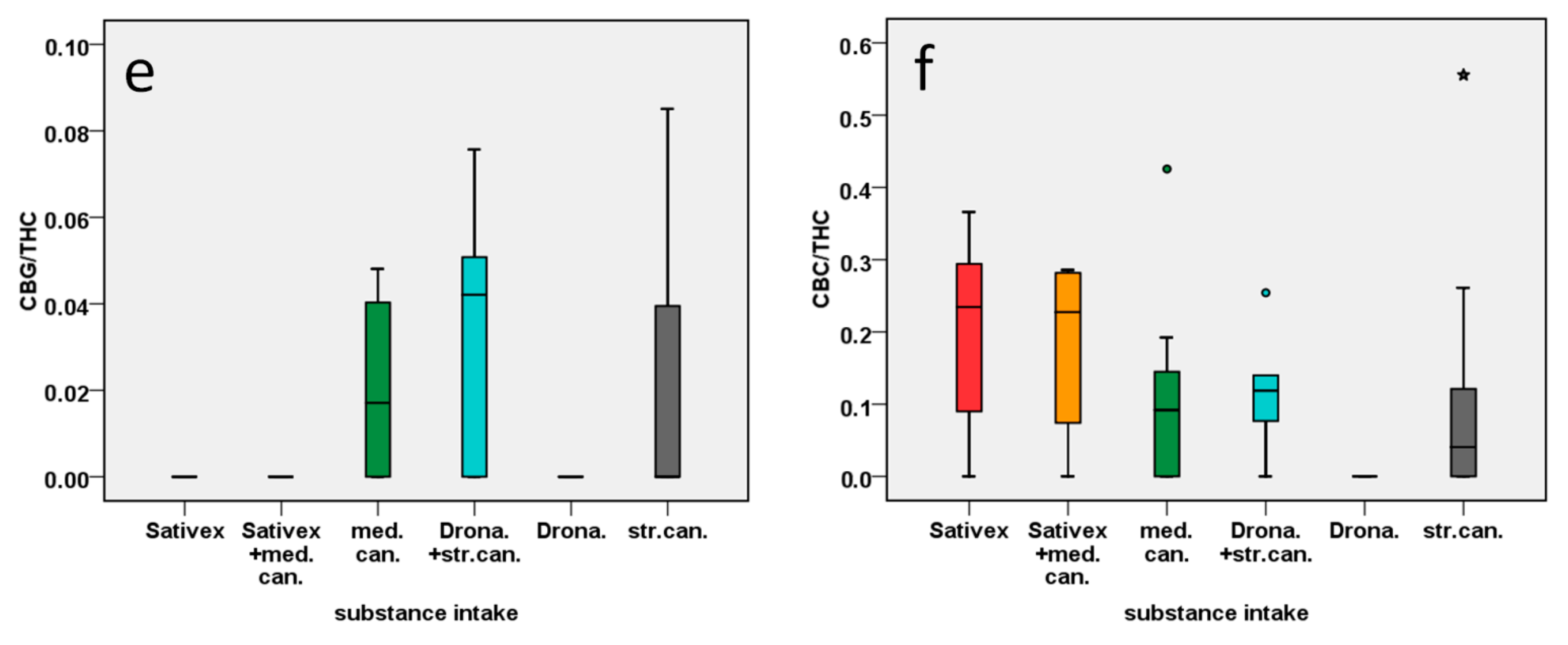
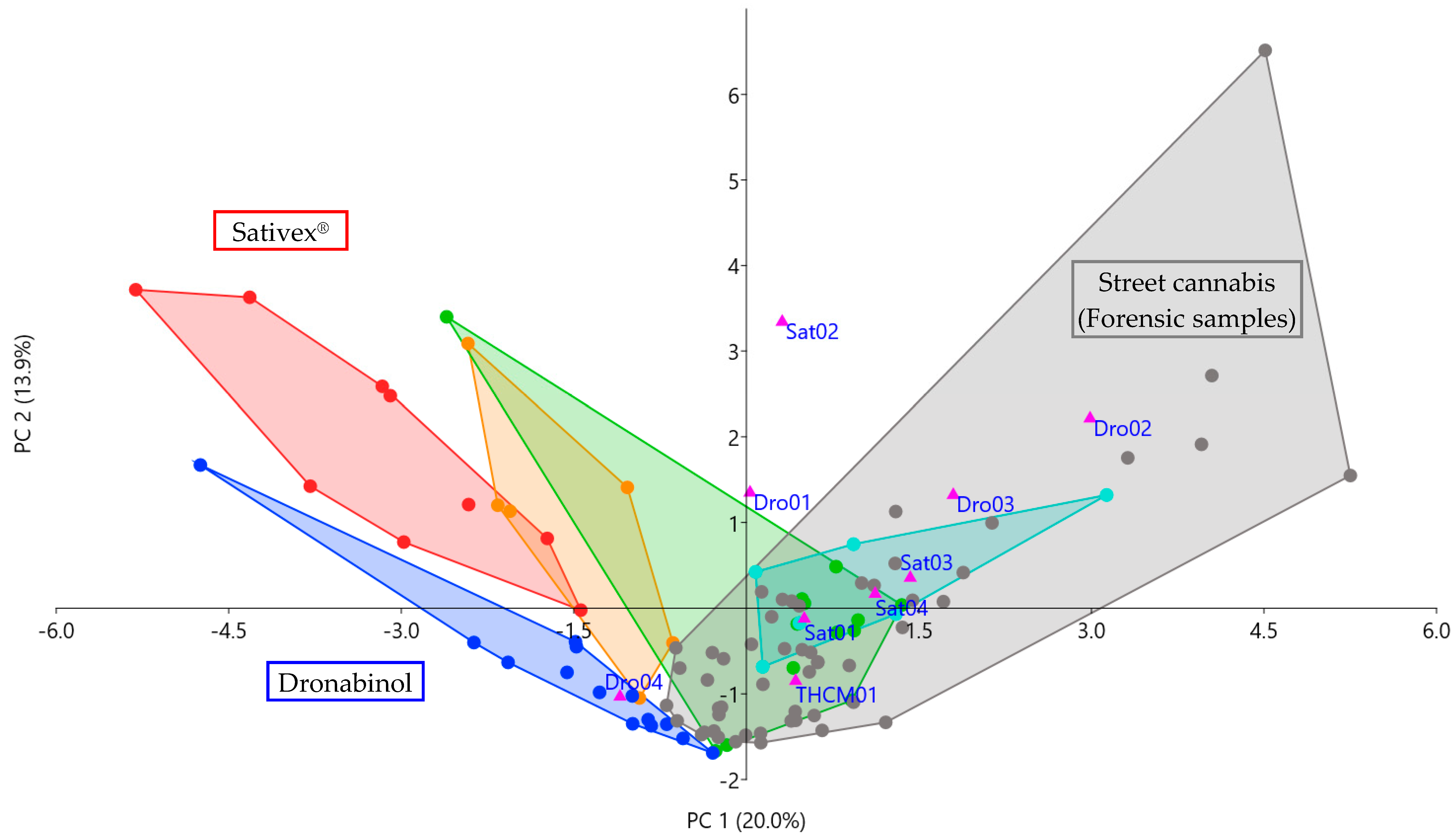
2.3.1. Statistical Analysis via Principal Component Analysis and Kruskal–Wallis Test
2.3.2. Sativex® vs. Cannabis or Combination of Sativex® and Cannabis
2.3.3. Dronabinol vs. Cannabis or Combination of Dronabinol and Cannabis
2.3.4. Medical Cannabis vs. Street Cannabis
2.4. Application to Forensic Case Samples
2.5. Limitations
3. Materials and Methods
3.1. Study Participants
3.2. Study Design
3.3. Chemicals and Reagents
3.4. Sample Preparation
3.5. LC-MS/MS Analysis
3.6. Data Analysis
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- United Nations Office on Drugs and Crime. World Drug Report 2019; United Nations: Vienna, Austria, 2019; ISBN 978-92-1-148314-7. [Google Scholar]
- United Nations Office on Drugs and Crime. World Drug Report 2020; United Nations: Vienna, Austria, 2020; ISBN 978-92-1-148345-1. [Google Scholar]
- Ramaekers, J.G.; Kauert, G.; Theunissen, E.L.; Toennes, S.W.; Moeller, M.R. Neurocognitive performance during acute THC intoxication in heavy and occasional cannabis users. J. Psychopharmacol. 2009, 23, 266–277. [Google Scholar] [CrossRef] [PubMed]
- European Monitoring Centre for Drugs and Drug Addiction. Driving under the Influence of Drugs, Alcohol and Medicines in Europe—Findings from the DRUID Project; Publications Office of the European Union: Luxembourg, 2012. [Google Scholar]
- European Monitoring Centre for Drugs and Drug Addiction. Medical Use of Cannabis and Cannabinoids: Questions and Answers for Policymaking; Publications Office of the European Union: Luxembourg, 2018. [Google Scholar]
- Russo, E.B. Taming THC: Potential cannabis synergy and phytocannabinoid-terpenoid entourage effects. Br. J. Pharmacol. 2011, 163, 1344–1364. [Google Scholar] [CrossRef] [PubMed]
- Almirall Hermal GmbH. Fachinformation Sativex Spray zur Anwendung in der Mundhöhle. Available online: https://www.cannabis-med.org/german/sativex.pdf (accessed on 23 November 2020).
- Cannabis Ärzte. Medizinische Cannabissorten. Available online: https://www.cannabis-aerzte.de/medizinische-cannabissorten/ (accessed on 18 February 2021).
- Gegenfurtner, H. Sonderbeilage zur GKV-Arzneimittel-Schnellinformation für Deutschland: Bruttoumsätze und Verordnungen von Cannabinoidhaltigen Fertigarzneimitteln und Zubereitungen von Januar bis Juni. 2018. Available online: https://www.gkv-gamsi.de/media/dokumente/quartalsberichte/2018/q2_18/Bundesbericht_GAmSi_201806_konsolidiert_Sonderbeilage_Cannabis.pdf (accessed on 23 November 2020).
- Sahle, M. Sonderbeilage zur GKV-Arzneimittel-Schnellinformation für Deutschland: Bruttoumsätze und Verordnungen von Cannabinoidhaltigen Fertigarzneimitteln und Zubereitungen von Januar bis Juni. 2020. Available online: https://www.gkv-gamsi.de/media/dokumente/quartalsberichte/2020/q2_22/Bundesbericht_GAmSi_202006_konsolidiert_Sonderbeilage_Cannabis.pdf (accessed on 23 November 2020).
- Radünz, L.; Westphal, F.; Maser, E.; Rochholz, G. THCVA-A—A new additional marker for illegal cannabis consumption. Forensic Sci. Int. 2012, 215, 171–174. [Google Scholar] [CrossRef] [PubMed]
- Raikos, N.; Schmid, H.; Nussbaumer, S.; Ambach, L.; Lanz, S.; Längin, A.; König, S.; Roth, N.; Auwärter, V.; Weinmann, W. Determination of Δ9-tetrahydrocannabinolic acid A (Δ9-THCA-A) in whole blood and plasma by LC-MS/MS and application in authentic samples from drivers suspected of driving under the influence of cannabis. Forensic Sci. Int. 2014, 243, 130–136. [Google Scholar] [CrossRef] [PubMed]
- Scheunemann, A.; Elsner, K.; Germerott, T.; Hess, C.; Zörntlein, S.; Röhrich, J. Extensive phytocannabinoid profiles of seized cannabis and cannabis-based medicines—Identification of potential distinguishing markers. Forensic Sci. Int. 2021, 322, 110773. [Google Scholar] [CrossRef] [PubMed]
- Meijer, E.D. The Chemical Phenotypes (Chemotypes) of Cannabis. In Handbook of Cannabis; Pertwee, R., Ed.; Oxford University Press: Oxford, UK, 2014; pp. 89–110. ISBN 9780199662685. [Google Scholar]
- Hazekamp, A.; Fischedick, J.T. Cannabis—From cultivar to chemovar. Drug Test. Anal. 2012, 4, 660–667. [Google Scholar] [CrossRef] [PubMed]
- Scheunemann, A.; Elsner, K.; Germerott, T.; Hess, C.; Röhrich, J. Simultaneous quantification of 18 different phytocanna-binoids in serum using a highly sensitive liquid chromatography-tandem mass spectrometry (LC-MS/MS) method. J. Chromatogr. B Analyt. Technol. Biomed. Life Sci. 2021, 1173, 122685. [Google Scholar] [CrossRef] [PubMed]
- MR NICE SEEDBANK. Dr. Nice Rebound—GMP (x30)—DrNice Website. Available online: https://drnice.nl/product/dr-nice-rebound-box-set/ (accessed on 18 February 2021).
- Kaiser, H.F.; Rice, J. Little Jiffy, Mark IV. Educ. Psychol. Meas. 1974, 34, 111–117. [Google Scholar] [CrossRef]
- Cleff, T. Deskriptive Statistik und Explorative Datenanalyse; Gabler Verlag: Wiesbaden, Germany, 2015; ISBN 978-3-8349-4747-5. [Google Scholar]
- Walther, B. Kruskal-Wallis-Test in SPSS Rechnen. Available online: https://www.bjoernwalther.com/kruskal-wallis-test-in-spss-rechnen/ (accessed on 1 February 2021).
- Feise, R.J. Do multiple outcome measures require p-value adjustment? BMC Med. Res. Methodol. 2002, 2, 8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nadulski, T.; Sporkert, F.; Schnelle, M.; Stadelmann, A.M.; Roser, P.; Schefter, T.; Pragst, F. Simultaneous and sensitive analysis of THC, 11-OH-THC, THC-COOH, CBD, and CBN by GC-MS in plasma after oral application of small doses of THC and cannabis extract. J. Anal. Toxicol. 2005, 29, 782–789. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karschner, E.L.; Darwin, W.D.; Goodwin, R.S.; Wright, S.; Huestis, M.A. Plasma cannabinoid pharmacokinetics following controlled oral delta9-tetrahydrocannabinol and oromucosal cannabis extract administration. Clin. Chem. 2011, 57, 66–75. [Google Scholar] [CrossRef] [PubMed]
- Guy, G.W.; Robson, P.J. A Phase I, Double Blind, Three-Way Crossover Study to Assess the Pharmacokinetic Profile of Cannabis Based Medicine Extract (CBME) Administered Sublingually in Variant Cannabinoid Ratios in Normal Healthy Male Volunteers (GWPK0215). J. Cannabis Ther. 2004, 3, 121–152. [Google Scholar] [CrossRef]
- Lee, D.; Karschner, E.L.; Milman, G.; Barnes, A.J.; Goodwin, R.S.; Huestis, M.A. Can oral fluid cannabinoid testing monitor medication compliance and/or cannabis smoking during oral THC and oromucosal Sativex administration? Drug Alcohol Depend. 2013, 130, 68–76. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- European Monitoring Centre for Drugs and Drug Addiction. European Drug Report 2019: Trends and Developments. Available online: https://www.emcdda.europa.eu/system/files/publications/11364/20191724_TDAT19001ENN_PDF.pdf (accessed on 23 November 2020).
- Fischedick, J.T.; Hazekamp, A.; Erkelens, T.; Choi, Y.H.; Verpoorte, R. Metabolic fingerprinting of Cannabis sativa L., cannabinoids and terpenoids for chemotaxonomic and drug standardization purposes. Phytochemistry 2010, 71, 2058–2073. [Google Scholar] [CrossRef] [PubMed]
- Jung, B. Medizinalhanf: Welche Rolle Spielt das Terpenprofil? Available online: https://www.deutsche-apotheker-zeitung.de/news/artikel/2019/05/23/medizinalhanf-welche-rolle-spielt-das-terpenprofil/chapter:all (accessed on 21 September 2020).
- Röhrich, J.; Zörntlein, S.; Becker, J.; Urban, R. Detection of Delta9-tetrahydrocannabinol and amphetamine-type stimulants in oral fluid using the Rapid Stat point-of-collection drug-testing device. J. Anal. Toxicol. 2010, 34, 155–161. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hammer, Ø.; Harper, D.A.T.; Ryan, P.D. PAST: Paleontological Statistics Software Package for Education and Data Analysis. Palaeontol. Electron. 2001, 4, 9–17. [Google Scholar]
- Hammer, Ø. et al. (1999–2021). PAST (Paleontological Statistics) [Software]. Available online: https://www.nhm.uio.no/english/research/infrastructure/past/index.html (accessed on 10 May 2021).
- Ringnér, M. What is principal component analysis? Nat. Biotechnol. 2008, 26, 303–304. [Google Scholar] [CrossRef] [PubMed]
- Abdi, H.; Williams, L.J. Principal component analysis. WIREs Comp. Stat. 2010, 2, 433–459. [Google Scholar] [CrossRef]
- Kessler, W. Hauptkomponentenanalyse. In Multivariate Datenanalyse; Kessler, W., Ed.; Wiley-VCH Verlag GmbH & Co. KGaA: Weinheim, Germany, 2006; pp. 21–88. ISBN 9783527610037. [Google Scholar]
- Kessler, W. Einführung in die multivariate Datenanalyse. In Multivariate Datenanalyse; Kessler, W., Ed.; Wiley-VCH Verlag GmbH & Co. KGaA: Weinheim, Germany, 2006; pp. 1–20. ISBN 9783527610037. [Google Scholar]
- Kessler, W. Kalibrieren, Validieren, Vorhersagen. In Multivariate Datenanalyse; Kessler, W., Ed.; Wiley-VCH Verlag GmbH & Co. KGaA: Weinheim, Germany, 2006; pp. 153–181. ISBN 9783527610037. [Google Scholar]
- Hammer, Ø. PAST Version 4.03 Reference Manual. Available online: https://www.nhm.uio.no/english/research/infrastructure/past/downloads/past4manual.pdf (accessed on 29 September 2020).
- Cohen, J. The Significance of a Product Moment rs. In Statistical Power Analysis for the Behavioral Sciences; Cohen, J., Ed.; Elsevier Science: Burlington, NJ, USA, 2013; pp. 75–107. ISBN 9780121790608. [Google Scholar]
- Holm, S. A Simple Sequentially Rejective Multiple Test Procedure. Scand. J. Stat. 1979, 6, 65–70. [Google Scholar]
- Hemmerich, W.A. Rechner zur Adjustierung des α-Niveaus|StatistikGuru.de. Available online: https://statistikguru.de/rechner/adjustierung-des-alphaniveaus.html (accessed on 1 February 2021).
- Latour, A. Medizinische Cannabissorten in Apotheken. Available online: https://www.leafly.de/cannabissorten-in-apotheken/ (accessed on 25 March 2021).
- Bedrocan—Beyond Pioneering. Cannabis Products by Bedrocan—For Patients and Medicine Development. Available online: https://bedrocan.com/products-services/ (accessed on 25 March 2021).
- Bionorica ethics. Dronabinol—Informationen zur Herstellung des Rezepturarzneimittels in der Apotheke: Information für Fachkreise. Available online: https://www.bionorica-ethics.de/Resources/Herstellbroschuere_Stand_012019.PDF (accessed on 25 March 2021).





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sample | Substance Intake | Time between Last Intake and Blood Draw | THC | THC-OH | THC-COOH | THCAA | CBD | CBDA | CBN | CBNA | CBG | CBGA | CBC | CBCA | CBL | CBLA | THCV | THCVA | CBDV | CBDVA |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| S01-01 | Sativex | 2 h 25 min | 0.34 | 0.89 | 26 | (0.016) * | 0.36 | nd | 0.0085 | nd | nd | nd | (0.14) | nd | nd | nd | nd | (0.023) | nd | nd |
| S01-02 | Sativex | 18 h 20 min | 0.22 | 0.62 | 19 | (0.012) | 0.25 | nd | (0.0032) | nd | nd | nd | nd | nd | nd | nd | nd | (0.019) | nd | nd |
| S01-03 | Sativex | 7 h 15 min | (0.15) | (0.36) | 19 | (0.0055) | 0.23 | nd | (0.0016) | nd | nd | nd | nd | nd | nd | nd | nd | (0.021) | nd | nd |
| S02-01 | Sativex | 9 h | 1.1 | 1.2 | 23 | 0.028 | 0.75 | (0.0020) | 0.020 | nd | nd | nd | (0.11) | nd | nd | nd | nd | (0.023) | nd | nd |
| S02-02 | Sativex | 16 h 15 min | 1.3 | 4.5 | 54 | 0.047 | 1.0 | (0.0028) | 0.030 | nd | nd | nd | 0.29 | nd | nd | nd | nd | (0.021) | nd | nd |
| S03-01 | Sativex | 50 min | 0.82 | 7.3 | 48 | 0.056 | 1.0 | 0.010 | 0.024 | nd | nd | nd | 0.28 | nd | nd | nd | nd | (0.015) | nd | nd |
| S03-02 | Sativex | 33 min | 0.63 | 6.4 | 72 | 0.032 | 0.77 | 0.0054 | 0.016 | nd | nd | nd | (0.16) | nd | nd | nd | nd | (0.017) | nd | nd |
| S03-03 | Sativex | 1 h 24 min | 4.6 | 12 | 100 | 0.084 | 2.8 | 0.041 | 0.044 | nd | nd | nd | 0.82 | (0.030) | nd | nd | nd | (0.019) | nd | nd |
| S03-04 | Sativex | 1 h 5 min | 4.4 | 22 | 170 | 0.034 | 6.1 | 0.042 | 0.040 | (0.0066) | nd | (0.011) | 1.1 | 0.032 | nd | nd | nd | (0.024) | nd | nd |
| S04-01 | Sativex+ Bedrocan | 10 h 44 min (Sativex) | 1.4 | 0.63 | 2.1 | nd | 0.52 | 0.013 | 0.017 | nd | nd | nd | (0.10) | (0.011) | nd | nd | nd | (0.024) | nd | nd |
| S05-01 | Sativex+ Bedrocan | 13 h 35 min (Sativex) | (0.10) | nd | 6.8 | (0.0062) | nd | nd | (0.0022) | nd | nd | nd | nd | nd | nd | nd | nd | (0.034) | nd | nd |
| S05-02 | Sativex+ Bedrocan | 2 h 15 min (Sativex) | 0.43 | 1.0 | 22 | (0.017) | 0.26 | 0.0042 | (0.0078) | nd | nd | nd | (0.10) | nd | nd | nd | nd | (0.032) | nd | nd |
| S05-03 | Sativex+ Bedrocan | 1 h 45 min (Sativex) | 0.45 | 0.88 | 30 | 0.040 | 0.34 | 0.024 | 0.012 | nd | nd | nd | (0.12) | nd | nd | nd | nd | 0.047 | nd | nd |
| S05-04 | Sativex+ Bedrocan | 3 h 30 min (Sativex) | 1.1 | 2.4 | 56 | 0.036 | 0.64 | 0.0071 | 0.020 | nd | nd | nd | 0.28 | (0.015) | nd | nd | nd | 1.8 | nd | nd |
| S05-05 | Sativex+ Bedrocan | 2 h 10 min (Sativex) | 0.71 | 1.4 | 27 | 0.040 | 0.53 | (0.0034) | 0.010 | nd | nd | nd | (0.18) | nd | nd | nd | nd | (0.029) | nd | nd |
| S06-01 | Bediol | 3 h 56 min | 0.94 | 0.72 | 7.2 | (0.013) | 2.0 | 0.0054 | 0.048 | nd | nd | nd | 0.45 | nd | nd | nd | nd | 0.18 | nd | nd |
| S07-01 | Bedrocan | 1 h 10 min | 49 | 22 | 170 | 9.3 | 0.18 | 0.0088 | 0.97 | 0.022 | 2.4 | 1.1 | 4.5 | 0.58 | nd | 0.022 | 0.36 | 3.2 | nd | nd |
| S07-02 | Bedrocan | 1 h 30 min | 32 | 17 | 170 | 3.7 | (0.071) | (0.0031) | 0.48 | (0.013) | 1.5 | 0.54 | 3.0 | 0.21 | nd | (0.0096) | 0.23 | 2.7 | nd | nd |
| S07-03 | Bedrocan | 2 h 30 min | 43 | 26 | 150 | 1.9 | (0.080) | (0.0035) | 0.92 | 0.030 | 1.7 | 0.74 | 4.2 | 0.36 | nd | 0.014 | 0.25 | 0.91 | nd | nd |
| S07-04 | Bedrocan | 1 h 10 min | 48 | 21 | 180 | 1.6 | (0.045) | 0.0053 | 0.84 | 0.026 | 2.1 | 0.34 | 4.4 | 0.12 | nd | (0.0071) | (0.17) | 1.5 | nd | nd |
| S08-01 | Bedrolite+ Pedanios | 10 h 10 min (Pedanios 22/1) | nd | nd | nd | nd | nd | nd | nd | nd | nd | nd | nd | nd | nd | nd | nd | (0.013) | nd | nd |
| S08-02 | Bedrolite+ Bedrocan | 9 h (Bedrolite) | nd | nd | nd | (0.011) | nd | nd | nd | (0.011) | nd | nd | nd | nd | nd | nd | nd | (0.017) | nd | nd |
| S08-03 | Bedrolite+ Bedrocan | 2 h 30 min (Bedrolite) | nd | nd | nd | (0.0094) | nd | nd | nd | nd | nd | nd | nd | nd | nd | nd | nd | (0.013) | nd | nd |
| S08-04 | Bedrolite+ Bedrocan | 2 h 30 min (Bedrocan) | (0.084) | nd | nd | (0.0049) | nd | nd | nd | nd | nd | nd | nd | nd | nd | nd | nd | nd | nd | nd |
| S09-01 | Bedrocan | 15 h 26 min | 0.39 | 0.42 | 11 | (0.0093) | (0.036) | 0.0063 | 0.018 | nd | nd | 0.022 | nd | nd | nd | nd | nd | 0.37 | nd | nd |
| S09-02 | Bedrocan | 10 h 55 min | 0.42 | (0.27) | 6.4 | 0.047 | nd | (0.0020) | 0.012 | nd | nd | 0.024 | nd | nd | nd | nd | nd | 0.23 | nd | nd |
| S09-03 | Bedrocan | 1 d 14 h 50 min | (0.17) | nd | 2.2 | (0.019) | nd | nd | 0.019 | nd | nd | nd | nd | nd | nd | nd | nd | 0.27 | nd | nd |
| S10-01 | Bedrobinol | 4 h 50 min | 0.20 | nd | nd | (0.012) | nd | nd | (0.0036) | nd | nd | nd | nd | nd | nd | nd | nd | (0.0087) | nd | nd |
| S10-02 | Bedrobinol | 3 h 20 min | 3.7 | 1.5 | 14 | 0.88 | (0.087) | nd | 0.25 | nd | 0.090 | 0.033 | 0.64 | (0.029) | nd | nd | nd | 0.21 | nd | nd |
| S10-03 | Bedrobinol | 1 h 55 min | 4.7 | 2.0 | 20 | 1.3 | (0.076) | nd | 0.18 | nd | (0.079) | 0.054 | 0.85 | 0.055 | nd | nd | nd | 0.56 | nd | nd |
| S10-04 | Bedrobinol | 5 d 14 h 40 min | 2.1 | 1.1 | 8.4 | 0.45 | (0.073) | nd | 0.12 | nd | (0.046) | (0.011) | 0.27 | (0.023) | nd | nd | nd | 0.28 | nd | nd |
| S11-01 | Dronabinol+ Street cannabis | 6 h 34 min (Dronabinol) | 0.84 | 1.0 | 21 | (0.016) | nd | nd | 0.027 | nd | nd | (0.0082) | (0.15) | nd | nd | (0.0021) | nd | 0.29 | nd | nd |
| S11-02 | Dronabinol+ Street cannabis | 8 h 19 min (Dronabinol) | 1.4 | 1.0 | 21 | 0.17 | nd | nd | 0.029 | (0.0049) | (0.057) | 0.024 | (0.18) | (0.013) | nd | nd | nd | 2.3 | nd | nd |
| S11-03 | Dronabinol+ Street cannabis | approx. 4,5 d (Dronabinol) | 0.41 | (0.26) | 2.5 | 0.11 | nd | nd | 0.014 | (0.0045) | nd | (0.012) | nd | (0.011) | nd | (0.0024) | nd | 0.31 | nd | nd |
| S11-04 | Dronabinol+ Street cannabis | 12 h 50 min (Joint) | 1.2 | 0.69 | 19 | 0.11 | nd | nd | 0.032 | nd | (0.056) | (0.015) | 0.27 | (0.010) | nd | (0.0023) | nd | 0.40 | nd | nd |
| S12-01 | Dronabinol+ Street cannabis | 3 h (Dronabinol) | 11 | 5.3 | 290 | 0.66 | nd | nd | 0.35 | nd | 0.83 | 0.14 | 1.3 | (0.025) | nd | nd | nd | 0.78 | nd | nd |
| S12-02 | Dronabinol+ Street cannabis | 2 h 47 min (Dronabinol) | 16 | 12 | 210 | 0.78 | (0.044) | nd | 0.47 | 0.020 | 0.66 | 0.11 | 1.2 | 0.032 | nd | nd | nd | 1.7 | nd | nd |
| S13-01 | Dronabinol | 7 h 20 min | 0.48 | 1.9 | 23 | (0.0005) | nd | nd | nd | nd | nd | (0.0091) | nd | nd | nd | nd | nd | nd | nd | nd |
| S14-01 | Dronabinol | 1 h 20 min | 0.82 | 0.93 | 16 | (0.0004) | nd | nd | (0.0076) | nd | nd | nd | nd | nd | nd | nd | nd | 0.18 | nd | nd |
| S15-01 | Dronabinol | 1 h 40 min | (0.17) | 0.53 | 13 | nd | nd | nd | nd | nd | nd | nd | nd | nd | nd | nd | nd | nd | nd | nd |
| S15-02 | Dronabinol | 3 h 20 min | 1.0 | 2.0 | 29 | nd | nd | nd | (0.0024) | nd | nd | (0.0085) | nd | nd | nd | nd | nd | nd | nd | nd |
| S16-01 | Dronabinol | 23 h 40 min | (0.15) | (0.20) | 2.4 | (0.0025) | nd | nd | nd | nd | nd | nd | nd | nd | nd | nd | nd | nd | nd | nd |
| S16-02 | Dronabinol | 24 h 30 min | (0.048) | nd | 2.4 | nd | nd | nd | nd | nd | nd | nd | nd | nd | nd | nd | nd | nd | nd | nd |
| S16-03 | Dronabinol | 3 h 17 min | 0.23 | 0.65 | 6.6 | (0.017) | nd | nd | nd | nd | nd | nd | nd | nd | nd | nd | nd | nd | nd | nd |
| S17-01 | Dronabinol | 6 h 20 min | 0.25 | (0.27) | 6.3 | (0.015) | nd | nd | nd | nd | nd | nd | nd | nd | nd | nd | nd | nd | nd | nd |
| S17-02 | Dronabinol | 6 h 45 min | (0.067) | 0.71 | 13 | (0.017) | nd | nd | (0.0022) | nd | nd | nd | nd | nd | nd | nd | nd | nd | nd | nd |
| S17-03 | Dronabinol | 15 h 6 min | nd | nd | nd | nd | nd | nd | nd | nd | nd | nd | nd | nd | nd | nd | nd | nd | nd | nd |
| S17-04 | Dronabinol | 15 h 30 min | nd | nd | (1.0) | (0.0021) | nd | nd | nd | nd | nd | nd | nd | nd | nd | nd | nd | nd | nd | nd |
| S17-05 | Dronabinol | 15 h 25 min | nd | nd | nd | nd | nd | nd | nd | nd | nd | nd | nd | nd | nd | nd | nd | nd | nd | nd |
| S18-01 | Dronabinol | 2 h 5 min | (0.12) | nd | nd | (0.0044) | nd | nd | nd | nd | nd | nd | nd | nd | nd | nd | nd | nd | nd | nd |
| S19-01 | Dronabinol | 1h | (0.18) | 1.0 | 2.8 | 0.031 | nd | nd | (0.0053) | nd | nd | nd | nd | nd | nd | nd | nd | nd | nd | nd |
| S19-02 | Dronabinol | Missing data | nd | nd | (1.6) | (0.012) | nd | nd | nd | nd | nd | nd | nd | nd | nd | nd | nd | nd | nd | nd |
| S20-01 | Dronabinol | 1 to 1,5 h | (0.17) | nd | 3.4 | nd | nd | nd | (0.0021) | nd | nd | nd | nd | nd | nd | nd | nd | nd | nd | nd |
| S21-01 | Dronabinol | 3 h 24 min | 0.69 | 2.7 | 28 | (0.0080) | nd | nd | (0.0046) | (0.0054) | nd | nd | nd | nd | nd | nd | nd | nd | nd | nd |
| S22-01 | Dronabinol | 13 h 54 min | (0.15) | 0.46 | 16 | nd | nd | nd | nd | nd | nd | nd | nd | nd | nd | nd | nd | (0.032) | nd | nd |
| S23-01 | CBD capsules | 14 h 15 min | nd | nd | nd | 0.10 | 0.24 | 0.37 | (0.0043) | (0.0062) | nd | 0.48 | nd | 0.18 | nd | (0.0041) | nd | 0.42 | nd | 0.018 |
| Pairwise Comparison | (χ2 = 36.0, p = 0.000) | (χ2 = 40.2, p = 0.000) | (χ2 = 23.1, p = 0.000) | (χ2 = 51.3, p = 0.000) | (χ2 = 36.5, p = 0.000) | (χ2 = 30.3, p = 0.000) | (χ2 = 38.6, p = 0.000) | (χ2 = 21.6, p = 0.0010) | (χ2 = 23.2, p = 0.000) | (χ2 = 26.1, p = 0.000) | (χ2 = 14.3, p = 0.014) | (χ2 = 1.76, p = 0.88) | (χ2 = 14.5, p = 0.013) | (χ2 = 9.44, p = 0.093) | (χ2 = 36.8, p = 0.000) | (χ2 = 0.873, p = 0.97) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Sativex vs. Street Cannabis | z = 4.82 p = 0 (0) | z = 4.17 p = 0 (0) | z = −2.79 p = 0.0050 (0.070) | z = 5.68 p = 0 (0) | z = 3.49 p = 0 (0) | z = −3.63 p = 0 (0) | z = −2.48 p = 0.013 (0.13) | z = −2.53 p = 0.011 (0.090) | z = 2.61 p = 0.0090 (0.090) | z = −3.22 p = 0.0010 (0.013) | ||||||
| Sativex vs. Medical Cannabis | z = 4.35 p = 0 (0) | z = 4.95 p = 0 (0) | z = −1.84 p = 0.067 (0.67) | z = 3.01 p = 0.0030 (0.027) | z = −1.88 p = 0.060 (0.60) | z = −2.36 p = 0.018 (0.16) | z = −2.70 p = 0.0070 (0.084) | z = −1.83 p = 0.067 (0.64) | z = −1.79 p = 0.074 (0.67) | |||||||
| Sativex vs. Sativex + Medical Cannabis | z = 1.85 p = 0.064 (0.64) | |||||||||||||||
| Dronabinol vs. Street Cannabis | z = 3.60 p = 0 (0) | z = 3.29 p = 0.0010 (0.011) | z = −4.09 p = 0 (0) | z = −4.74 p = 0 (0) | z = −4.32 p = 0 (0) | z = −2.98 p = 0.0030 (0.042) | z = −2.62 p = 0.0090 (0.090) | z = −2.91 p = 0.0040 (0.048) | z =−3.02 p = 0.0030 (0.045) | z = −5.20 p = 0 (0) | ||||||
| Dronabinol vs. Medical Cannabis | z = −3.20 p = 0.0010 (0.012) | z = -4.23 p = 0 (0) | z = 2.65 p = 0.0080 (0.10) | z = 3.05 p = 0.0020 (0.020) | z = 2.90 p = 0.0040 (0.036) | z = 4.15 p = 0 (0) | z = 2.66 p = 0.0080 (0.096) | z = 2.70 p = 0.0070 (0.084) | z = 2.92 p = 0.0040 (0.048) | z = 2.55 p = 0.011 (0.14) | z = 2.06 p = 0.039 (0.43) | z = 3.05 p = 0.0020 (0.024) | ||||
| Dronabinol vs. Dronabinol + Street Cannabis | z = 1.96 p = 0.050 (0.58) | z = 3.79 p = 0 (0) | z = 1.78 p = 0.075 (0.83) | z = 3.10 p = 0.0020 (0.030) | z = 3.06 p = 0.0020 (0.030) | z = 3.03 p = 0.0020 (0.026) | z = 2.99 p = 0.0030 (0.045) | z = 3.16 p = 0.0020 (0.030) | z = 4.10 p = 0 (0) | |||||||
| Street Cannabis vs. Medical Cannabis | z = −2.10 p = 0.036 (0.29) | z = 2.39 p = 0.017 (0.12) | z = 2.58 p = 0.010 (0.080) | z = −3.64 p = 0 (0) |
| Sample | Substance Intake | THC | THC-OH | THC-COOH | THCAA | CBD | CBDA | CBN | CBNA | CBG | CBGA | CBC | CBCA | CBL | CBLA | THCV | THCVA | CBDV | CBDVA |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Sat01 | Sativex | 2.9 | 1.3 | 40 | 0.14 | 0.39 | 0.0043 | 0.12 | nd | 0.11 | (0.015) * | 0.42 | nd | nd | nd | (0.048) | 0.34 | nd | nd |
| Sat02 | Sativex | 6.5 | 3.3 | 130 | 1.7 | 1.5 | 0.61 | 0.16 | 0.022 | 0.22 | 0.054 | 0.84 | 0.099 | nd | nd | (0.026) | 0.92 | nd | nd |
| Sat03 | Sativex | 3.8 | 2.7 | 53 | 1.2 | 0.16 | 0.014 | 0.18 | 0.018 | 0.16 | 0.047 | 0.46 | (0.024) | nd | nd | (0.080) | 0.60 | nd | nd |
| Sat04 | Sativex | 12 | 4.4 | 56 | 0.27 | 1.4 | (0.0022) | 2.0 | 0.050 | 0.46 | 0.027 | 1.8 | (0.014) | nd | nd | (0.18) | 0.36 | nd | nd |
| Dro01 | Dronabinol | 0.96 | 0.4 | 30 | 0.050 | 0.31 | nd | 0.12 | (0.011) | (0.048) | nd | 0.36 | nd | nd | nd | nd | 0.29 | nd | nd |
| Dro02 | Dronabinol | 1.3 | (0.3) | 23 | 0.046 | nd | nd | 0.053 | nd | 0.12 | nd | 0.26 | 0.16 | nd | nd | nd | 0.26 | nd | nd |
| Dro03 | Dronabinol | 5.9 | 2.4 | 100 | 2.6 | (0.063) | nd | 0.19 | 0.022 | 0.35 | 0.19 | 1.7 | 0.039 | nd | nd | (0.067) | 2.9 | nd | nd |
| Dro04 | Dronabinol | (0.19) | (0.3) | 8.6 | (0.016) | nd | nd | (0.0015) | nd | nd | nd | nd | nd | nd | nd | nd | (0.031) | nd | nd |
| THCM01 | THC medicine | 2.1 | 0.5 | 9.8 | 0.12 | (0.086) | nd | 0.045 | (0.014) | 0.078 | nd | (0.19) | (0.0091) | nd | nd | nd | 0.87 | nd | nd |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Scheunemann, A.; Elsner, K.; Germerott, T.; Groppa, S.; Hess, C.; Miederer, I.; Poplawski, A.; Röhrich, J. Identification of Potential Distinguishing Markers for the Use of Cannabis-Based Medicines or Street Cannabis in Serum Samples. Metabolites 2021, 11, 316. https://0-doi-org.brum.beds.ac.uk/10.3390/metabo11050316
Scheunemann A, Elsner K, Germerott T, Groppa S, Hess C, Miederer I, Poplawski A, Röhrich J. Identification of Potential Distinguishing Markers for the Use of Cannabis-Based Medicines or Street Cannabis in Serum Samples. Metabolites. 2021; 11(5):316. https://0-doi-org.brum.beds.ac.uk/10.3390/metabo11050316
Chicago/Turabian StyleScheunemann, Anne, Katrin Elsner, Tanja Germerott, Sergiu Groppa, Cornelius Hess, Isabelle Miederer, Alicia Poplawski, and Jörg Röhrich. 2021. "Identification of Potential Distinguishing Markers for the Use of Cannabis-Based Medicines or Street Cannabis in Serum Samples" Metabolites 11, no. 5: 316. https://0-doi-org.brum.beds.ac.uk/10.3390/metabo11050316