
Impact of Venoarterial Extracorporeal Membrane Oxygenation on Alkaline Phosphatase Metabolism after Cardiac Surgery

 ,
,  , ,
, ,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Laboratory Data
2.3. Follow-Up
2.4. Statistical Analysis
3. Results
3.1. Patient Population and Cut-Off Values
3.2. Preoperative Characteristics
3.3. Procedural Data
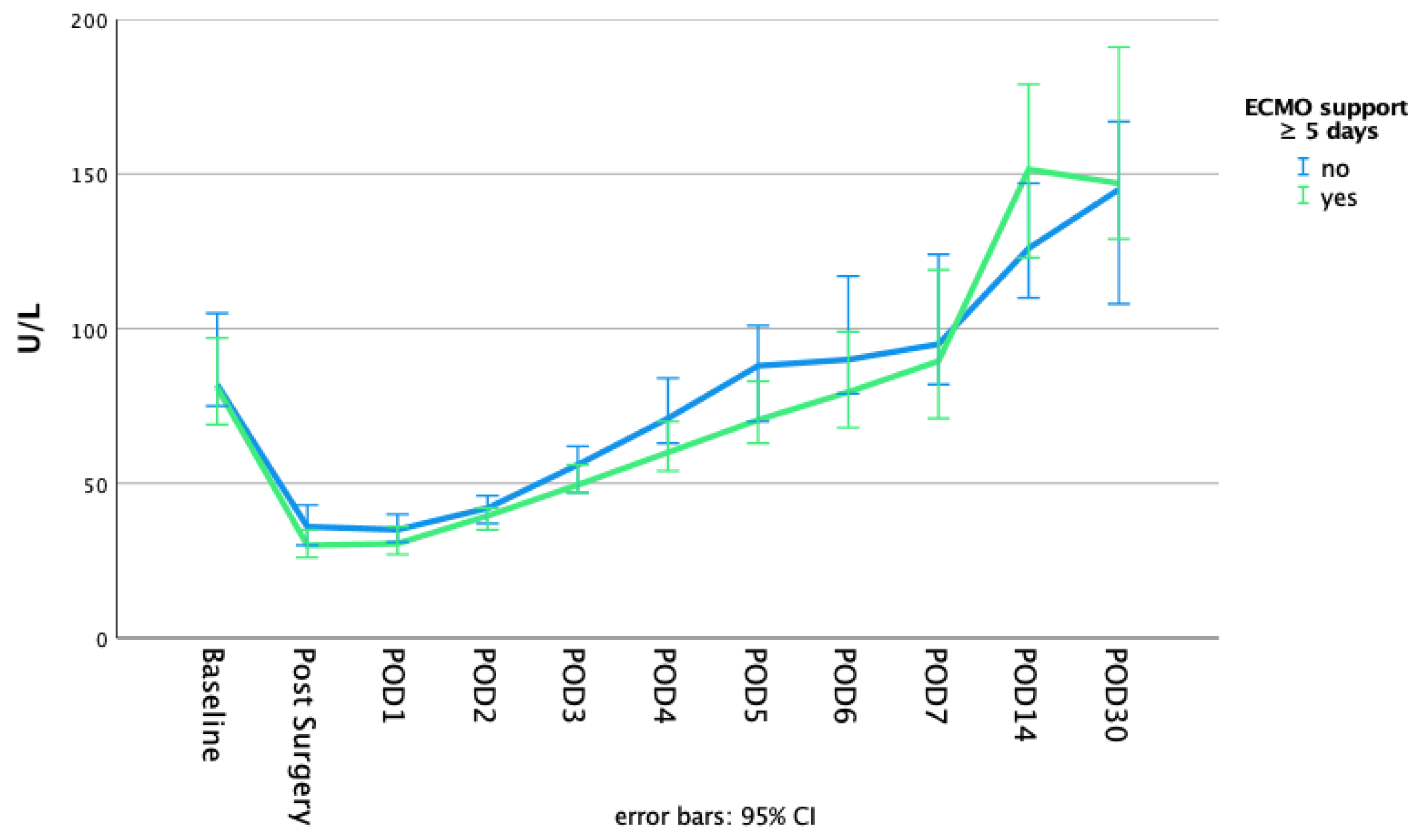
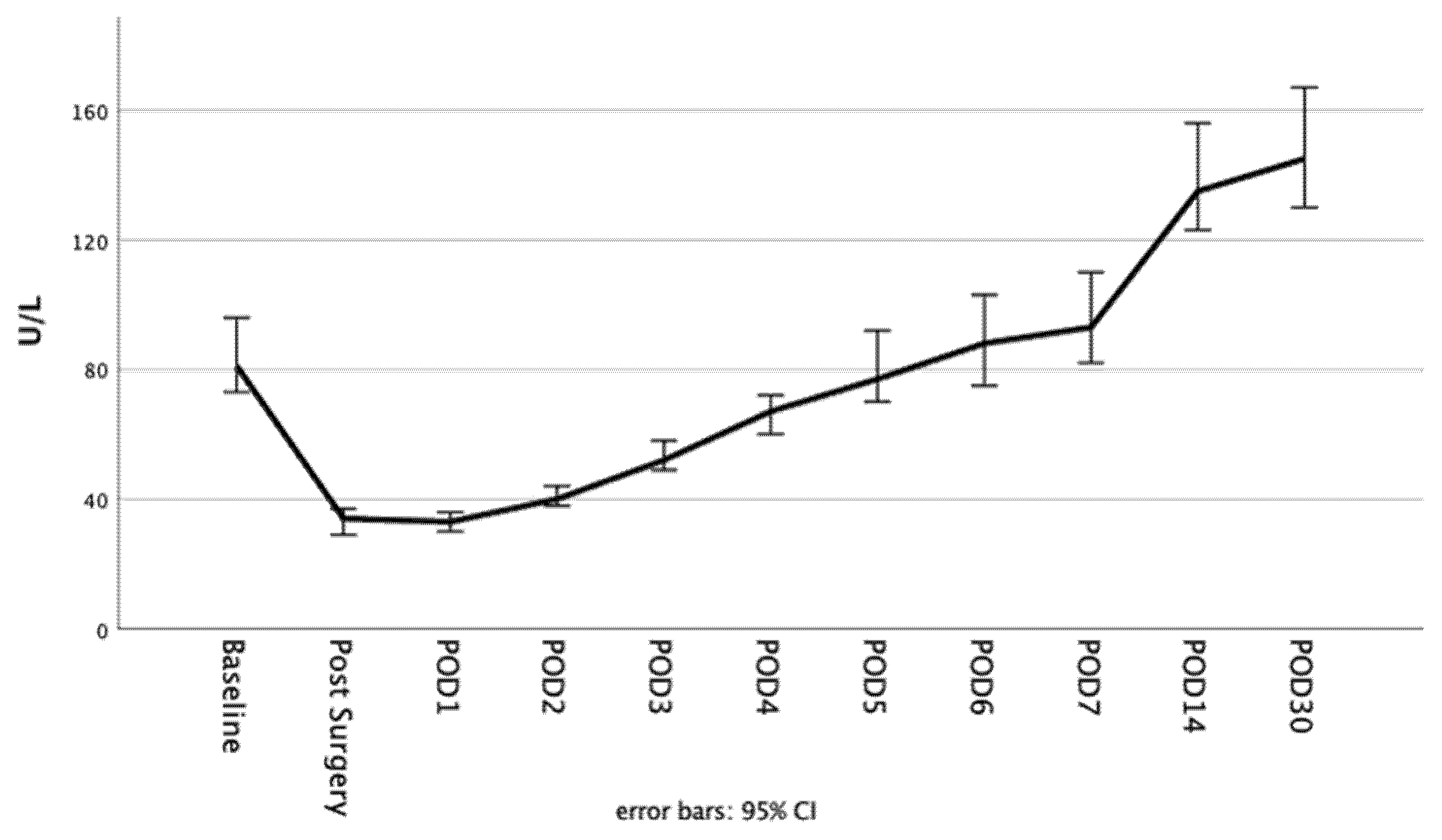
3.4. Alkaline Phosphatase
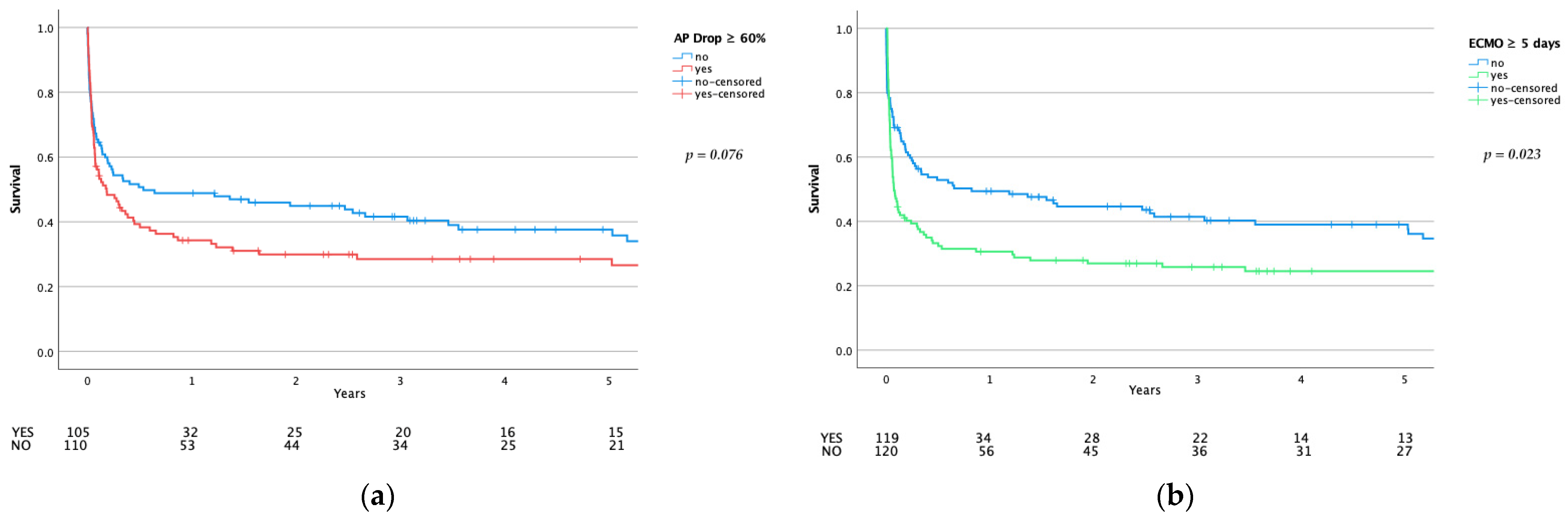
3.5. Adverse Events and Mortality
4. Discussion
5. Conclusions
6. Limitations
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Al-Fares, A.; Pettenuzzo, T.; Del Sorbo, L. Extracorporeal life support and systemic inflammation. Intensiv. Care Med. Exp. 2019, 7, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Giacinto, O.; Satriano, U.; Nenna, A.; Spadaccio, C.; Lusini, M.; Mastroianni, C.; Nappi, F.; Chello, M. Inflammatory Response and Endothelial Dysfunction Following Cardiopulmonary Bypass: Pathophysiology and Pharmacological Targets. Recent Pat. Inflamm. Allergy Drug Discov. 2019, 13, 158–173. [Google Scholar] [CrossRef]
- Squiccimarro, E.; Labriola, C.; Malvindi, P.G.; Margari, V.; Guida, P.; Visicchio, G.; Kounakis, G.; Favale, A.; Dambruoso, P.; Mastrototaro, G.; et al. Prevalence and Clinical Impact of Systemic Inflammatory Reaction After Cardiac Surgery. J. Cardiothorac. Vasc. Anesth. 2019, 33, 1682–1690. [Google Scholar] [CrossRef]
- Peters, E.; Heemskerk, S.; Masereeuw, R.; Pickkers, P. Alkaline Phosphatase: A Possible Treatment for Sepsis-Associated Acute Kidney Injury in Critically Ill Patients. Am. J. Kidney Dis. 2014, 63, 1038–1048. [Google Scholar] [CrossRef] [Green Version]
- Montesinos, M.C.; Takedachi, M.; Thompson, L.F.; Wilder, T.F.; Fernandez, P.; Cronstein, B.N. The antiinflammatory mechanism of methotrexate depends on extracellular conversion of adenine nucleotides to adenosine by ec-to-5′-nucleotidase: Findings in a study of ecto-5′-nucleotidase gene-deficient mice. Arthritis Rheum. 2007, 56, 1440–1445. [Google Scholar] [CrossRef] [PubMed]
- Neuhof, C.; Wendling, J.; Dapper, F.; Bauer, J.; Zickmann, B.; Jochum, M.; Tillmanns, H.; Neuhof, H. Endotoxemia and cytokine generation in cardiac surgery in relation to flow mode and duration of cardiopulmonary bypass. Shock 2001, 16, 39–43. [Google Scholar] [CrossRef] [PubMed]
- Riddington, D.W.; Venkatesh, B.; Boivin, C.M.; Bonser, R.S.; Elliott, T.S.; Marshall, T.; Mountford, P.J.; Bion, J.F. Intestinal permeability, gastric intramucosal pH, and systemic endotoxemia in patients undergoing cardiopulmonary bypass. JAMA 1996, 275, 1007–1012. [Google Scholar] [CrossRef]
- Paparella, D.; Yau, T.; Young, E. Cardiopulmonary bypass induced inflammation: Pathophysiology and treatment. An update. Eur. J. Cardiothorac. Surg. 2002, 21, 232–244. [Google Scholar] [CrossRef] [Green Version]
- Johnsen, B.; Kaschubowski, K.E.; Nader, S.; Schneider, E.; Nicola, J.-A.; Fliegert, R.; Wolf, I.M.A.; Guse, A.H.; Nikolaev, V.O.; Koch-Nolte, F.; et al. P2X7-mediated ATP secretion is accompanied by depletion of cytosolic ATP. Purinergic Signal. 2019, 15, 155–166. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fawley, J.; Gourlay, D.M. Intestinal alkaline phosphatase: A summary of its role in clinical disease. J. Surg. Res. 2016, 202, 225–234. [Google Scholar] [CrossRef] [Green Version]
- Siller, A.F.; Whyte, M.P. Alkaline Phosphatase: Discovery and Naming of Our Favorite Enzyme. J. Bone Miner. Res. 2018, 33, 362–364. [Google Scholar] [CrossRef] [Green Version]
- Poelstra, K.; Bakker, W.W.; Klok, P.A.; Kamps, J.A.; Hardonk, M.J.; Meijer, D.K. Dephosphorylation of endotoxin by alkaline phosphatase in vivo. Am. J. Pathol. 1997, 151, 1163–1169. [Google Scholar]
- Koyama, I.; Matsunaga, T.; Harada, T.; Hokari, S.; Komoda, T. Alkaline phosphatases reduce toxicity of lipopolysaccharides in vivo and in vitro through dephosphorylation. Clin. Biochem. 2002, 35, 455–461. [Google Scholar] [CrossRef]
- Schaefer, A.-K.; Hutschala, D.; Andreas, M.; Bernardi, M.H.; Brands, R.; Shabanian, S.; Laufer, G.; Wiedemann, D. Decrease in serum alkaline phosphatase and prognostic relevance in adult cardiopulmonary bypass. Interact. Cardiovasc. Thorac. Surg. 2020, 31, 383–390. [Google Scholar] [CrossRef]
- Davidson, J.; Tong, S.; Hauck, A.; Lawson, D.S.; Jaggers, J.; Kaufman, J.; Da Cruz, E. Alkaline phosphatase activity after cardiothoracic surgery in infants and correlation with post-operative support and inflammation: A prospective cohort study. Crit. Care 2012, 16, R160. [Google Scholar] [CrossRef] [Green Version]
- Davidson, J.A.; Urban, T.T.; Tong, S.; Maddux, A.; Hill, G.; Frank, B.S.; Watson, J.D.; Jaggers, J.; Simões, E.A.F.; Wischmeyer, P. Alkaline Phosphatase Activity and Endotoxemia after Infant Cardiothoracic Surgery. Shock 2019, 51, 328–336. [Google Scholar] [CrossRef]
- Lorusso, R.; Raffa, G.M.; Alenizy, K.; Sluijpers, N.; Makhoul, M.; Brodie, D.; McMullan, M.; Wang, I.-W.; Meani, P.; MacLaren, G.; et al. Structured review of post-cardiotomy extracorporeal membrane oxygenation: Part 1—Adult patients. J. Hearth Lung Transplant. 2019, 38, 1125–1143. [Google Scholar] [CrossRef] [PubMed]
- Singh, G.; Hudson, D.; Shaw, A. Medical Optimization and Liberation of Adult Patients from VA-ECMO. Can. J. Cardiol. 2020, 36, 280–290. [Google Scholar] [CrossRef] [PubMed]
- Distelmaier, K.; Wiedemann, D.; Binder, C.; Haberl, T.; Zimpfer, D.; Heinz, G.; Koinig, H.; Felli, A.; Steinlechner, B.; Niessner, A.; et al. Duration of extracorporeal membrane oxygenation support and survival in cardiovascular surgery patients. J. Thorac. Cardiovasc. Surg. 2018, 155, 2471–2476. [Google Scholar] [CrossRef]
- Kats, S.; Brands, R.; Hamad, M.A.S.; Seinen, W.; Scharnhorst, V.; Wulkan, R.W.; Schoenberger, J.P.; Van Oeveren, W. Prophylactic Treatment with Alkaline Phosphatase in Cardiac Surgery Induces Endogenous Alkaline Phosphatase Release. Int. J. Artif. Organs 2012, 35, 144–151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gallagher, K.M.; Harrison, E.M.; Ross, A.J.; Wigmore, S.J.; Hughes, J.; O’Neill, S. Recent early clinical drug development for acute kidney injury. Expert Opin. Investig. Drugs 2016, 26, 141–154. [Google Scholar] [CrossRef]
- Bauerle, J.D.; Grenz, A.; Kim, J.-H.; Lee, H.T.; Eltzschig, H.K. Adenosine Generation and Signaling during Acute Kidney Injury. J. Am. Soc. Nephrol. 2011, 22, 14–20. [Google Scholar] [CrossRef] [PubMed]
- Davidson, J.A.; Urban, T.T.; Baird, C.; Tong, S.; Woodruff, A.; Twite, M.; Jaggers, J.; Simões, E.A.F.; Wischmeyer, P. Alkaline Phosphatase in Infant Cardiopulmonary Bypass: Kinetics and Relationship to Organ Injury and Major Cardiovascular Events. J. Pediatr. 2017, 190, 49–55.e2. [Google Scholar] [CrossRef] [PubMed]
- Corredor, C.; Thomson, R.; Al-Subaie, N. Long-Term Consequences of Acute Kidney Injury After Cardiac Surgery: A Systematic Review and Meta-Analysis. J. Cardiothorac. Vasc. Anesth. 2016, 30, 69–75. [Google Scholar] [CrossRef]
- Hausenloy, D.J.; Yellon, D.M. The therapeutic potential of ischemic conditioning: An update. Nat. Rev. Cardiol. 2011, 8, 619–629. [Google Scholar] [CrossRef] [PubMed]
- Shen, Y.; Liu, X.; Shi, J.; Wu, X. Involvement of Nrf2 in myocardial ischemia and reperfusion injury. Int. J. Biol. Macromol. 2019, 125, 496–502. [Google Scholar] [CrossRef]
- Sahin, I.; Karabulut, A.; Gungor, B.; Avci, I.I.; Okuyan, E.; Kizkapan, F.; Yildiz, S.S.; Can, M.M.; Dinckal, M. Correlation between the serum alkaline phosphatase level and the severity of coronary artery disease. Coron. Artery Dis. 2014, 25, 349–352. [Google Scholar] [CrossRef]
- Presbitero, A.; Mancini, E.; Brands, R.; Krzhizhanovskaya, V.V.; Sloot, P.M.A. Supplemented Alkaline Phosphatase Supports the Immune Response in Patients Undergoing Cardiac Surgery: Clinical and Computational Evidence. Front. Immunol. 2018, 9, 2342. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Busse, L.W. Novel therapies for acute kidney injury. Kidney Int. Rep. 2017, 2, 785–799. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Baseline Specifics | Overall n = 239 | ECMO < 5 Days n = 120 | ECMO ≥ 5 Days n = 119 | p-Value ª | AP Drop < 60% n = 110 | AP Drop ≥ 60% n = 105 | p-Value ª |
|---|---|---|---|---|---|---|---|
| age | 68 (75, 58) | 69 (77, 61) | 67 (74, 57) | 0.228 | 64 (72, 55) | 70 (75, 62) | 0.001 * |
| female | 92 (38.5) | 42 (35.0) | 50 (42.0) | 0.265 | 45 (40.9) | 42 (40.0) | 0.892 |
| BMI | 27.1 (30.8, 24.2) | 26.7 (30.8, 24.5) | 27.2 (30.4, 23.9) | 0.884 | 27.7 (30.8, 24.9) | 26.0 (30.4, 23.6) | 0.045 * |
| hypertension | 174 (73.7) | 93 (78.8) | 81 (68.6) | 0.076 | 72 (66.7) | 85 (81.7) | 0.012 * |
| IDDM | 22 (9.4) | 9 (7.8) | 13 (10.9) | 0.405 | 12 (11.0) | 9 (8.6) | 0.580 |
| preoperative dialysis | 20 (8.4) | 9 (7.5) | 11 (9.2) | 0.626 | 8 (7.3) | 8 (7.6) | 0.923 |
| CVA | 46 (19.2) | 21 (17.5) | 25 (21.0) | 0.492 | 22 (20.0) | 20 (19.0) | 0.860 |
| CAD | 148 (61.9) | 79 (65.8) | 69 (58.0) | 0.211 | 61 (55.5) | 71 (67.6) | 0.067 |
| PCI | 39 (16.3) | 23 (19.2) | 16 (13.4) | 0.231 | 17 (15.5) | 17 (16.2) | 0.882 |
| CABG | 28 (11.7) | 18 (15.0) | 10 (8.4) | 0.113 | 10 (9.1) | 11 (10.5) | 0.732 |
| MI | 85 (35.6) | 46 (38.3) | 39 (32.8) | 0.369 | 40 (36.4) | 37 (35.2) | 0.863 |
| CPR | 19 (7.9) | 7 (5.8) | 12 (10.1) | 0.225 | 10 (9.1) | 8 (7.6) | 0.697 |
| NYHA III + IV | 188 (79.7) | 88 (75.2) | 100 (84.0) | 0.092 | 85 (80.0) | 84 (80.8) | 0.615 |
| LVEF | 45 (60, 30) | 45 (60, 30) | 45 (60, 25) | 0.453 | 45 (60, 30) | 45 (60, 29) | 0.788 |
| Surgical Specifics | Overall n = 239 | ECMO < 5 Days n = 120 | ECMO ≥ 5 Days n = 119 | p-Value ª | AP Drop < 60% n = 110 | AP Drop ≥ 60% n = 105 | p-Value ª |
|---|---|---|---|---|---|---|---|
| EuroScore II | 18.2 (34.5, 7.5) | 16.1 (36.5, 4.8) | 18.9 (32.7, 8.7) | 0.320 | 16.0 (35.6, 5.6) | 18.6 (32.2, 8.9) | 0.333 |
| critical preoperative state | 104 (43.5) | 53 (44.2) | 51 (42.9) | 0.838 | 53 (48.2) | 40 (38.1) | 0.136 |
| h/o cardiac surgery | 73 (30.5) | 34 (28.3) | 39 (32.8) | 0.456 | 31 (28.2) | 30 (28.6) | 0.949 |
| active endocarditis | 32 (13.4) | 19 (15.8) | 13 (10.9) | 0.265 | 16 (14.5) | 12 (11.4) | 0.497 |
| elective operation | 109 (45.6) | 54 (45.0) | 55 (46.2) | 0.850 | 46 (41.8) | 53 (50.5) | 0.203 |
| urgent operation | 58 (24.3) | 26 (21.7) | 32 (26.9) | 0.346 | 28 (25.5) | 25 (23.8) | 0.780 |
| emergency operation | 68 (28.5) | 38 (31.7) | 30 (25.2) | 0.269 | 34 (30.9) | 25 (23.8) | 0.244 |
| salvage operation | 4 (1.7) | 2 (1.7) | 2 (1.7) | 1.000 º | 2 (1.8) | 2 (1.9) | 1.000 º |
| surgery time | 8.5 (10.4, 6.8) | 8.5 (10.3, 6.4) | 8.5 (10.7, 7.2) | 0.341 | 8.1 (9.9, 6.0) | 9.3 (12.1, 7.5) | 0.000 * |
| CPB | 258 (347, 185) | 251 (337, 178) | 276 (373, 196) | 0.087 | 244 (326, 177) | 299 (411, 200) | 0.003 * |
| ACC | 128 (181, 81) | 122 (174, 78) | 132 (194, 85) | 0.322 | 120 (169, 73) | 137 (215, 87) | 0.026 * |
| VA-ECMO duration | 4.9 (8.1, 3.1) | 3.1 (3.9, 2.2) | 8.1 (11.7, 5.9) | 0.000 * | 4.7 (6.7, 2.9) | 5.3 (9.1, 3.5) | 0.048 * |
| Outcome | Overall n = 239 | ECMO < 5 Days n = 120 | ECMO ≥ 5 Days n = 119 | p-Value ª | AP Drop < 60% n = 110 | AP Drop ≥ 60% n = 105 | p-Value ª |
|---|---|---|---|---|---|---|---|
| any stroke | 42 (17.6) | 14 (11.7) | 28 (23.5) | 0.016 * | 20 (18.2) | 17 (16.2) | 0.699 |
| any bleeding complication | 125 (52.3) | 53 (44.2) | 72 (60.5) | 0.011 * | 44 (40.0) | 63 (60.0) | 0.003 * |
| need for any renal replacement therapy | 123 (51.5) | 50 (41.7) | 73 (61.3) | 0.002 * | 45 (40.9) | 65 (61.9) | 0.002 * |
| days until first extubation/decannulation | 13 (22, 7) | 9 (15, 4) | 15 (26, 10) | 0.000 * | 12 (20, 7) | 14 (26, 7) | 0.108 |
| need for tracheotomy | 62 (25.9) | 29 (24.2) | 33 (27.7) | 0.530 | 23 (20.9) | 37 (35.2) | 0.019 * |
| Mortality … | |||||||
| … on ECMO support | 69 (28.9) | 24 (20.0) | 45 (37.8) | 0.002 * | 28 (25.5) | 30 (28.6) | 0.607 |
| … within 30 days | 97 (40.6) | 37 (30.8) | 60 (50.4) | 0.002 * | 36 (32.7) | 45 (42.9) | 0.125 |
| … before extubation/decannulation | 103 (43.3) | 35 (29.4) | 68 (57.1) | 0.000 * | 39 (35.5) | 48 (46.2) | 0.111 |
| … post weaning | 102 (42.9) | 37 (31.1) | 65 (54.6) | 0.000 * | 39 (35.5) | 47 (45.2) | 0.146 |
| … on ICU ward | 113 (47.3) | 42 (35.0) | 71 (59.7) | 0.000 * | 42 (38.2) | 54 (51.4) | 0.051 |
| … in hospital | 121 (50.6) | 49 (40.8) | 72 (60.5) | 0.002 * | 47 (42.7) | 57 (54.3) | 0.090 |
| … 1 year | 142 (60.4) | 60 (51.3) | 82 (69.5) | 0.004 * | 56 (51.4) | 68 (66.0) | 0.031* |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Poschner, T.; Schaefer, A.-K.; Hutschala, D.; Goliasch, G.; Riebandt, J.; Distelmaier, K.; Bernardi, M.H.; Andreas, M.; Brands, R.; Aref, T.; et al. Impact of Venoarterial Extracorporeal Membrane Oxygenation on Alkaline Phosphatase Metabolism after Cardiac Surgery. Biomolecules 2021, 11, 748. https://0-doi-org.brum.beds.ac.uk/10.3390/biom11050748
Poschner T, Schaefer A-K, Hutschala D, Goliasch G, Riebandt J, Distelmaier K, Bernardi MH, Andreas M, Brands R, Aref T, et al. Impact of Venoarterial Extracorporeal Membrane Oxygenation on Alkaline Phosphatase Metabolism after Cardiac Surgery. Biomolecules. 2021; 11(5):748. https://0-doi-org.brum.beds.ac.uk/10.3390/biom11050748
Chicago/Turabian StylePoschner, Thomas, Anne-Kristin Schaefer, Doris Hutschala, Georg Goliasch, Julia Riebandt, Klaus Distelmaier, Martin H. Bernardi, Martin Andreas, Ruud Brands, Tandis Aref, and et al. 2021. "Impact of Venoarterial Extracorporeal Membrane Oxygenation on Alkaline Phosphatase Metabolism after Cardiac Surgery" Biomolecules 11, no. 5: 748. https://0-doi-org.brum.beds.ac.uk/10.3390/biom11050748