
Investigating the Effects of Dehydrated Human Amnion-Chorion Membrane on Periodontal Healing


Abstract
:1. Introduction
2. Materials and Methods
2.1. dHACM
2.2. Animals
2.3. Surgical Procedures
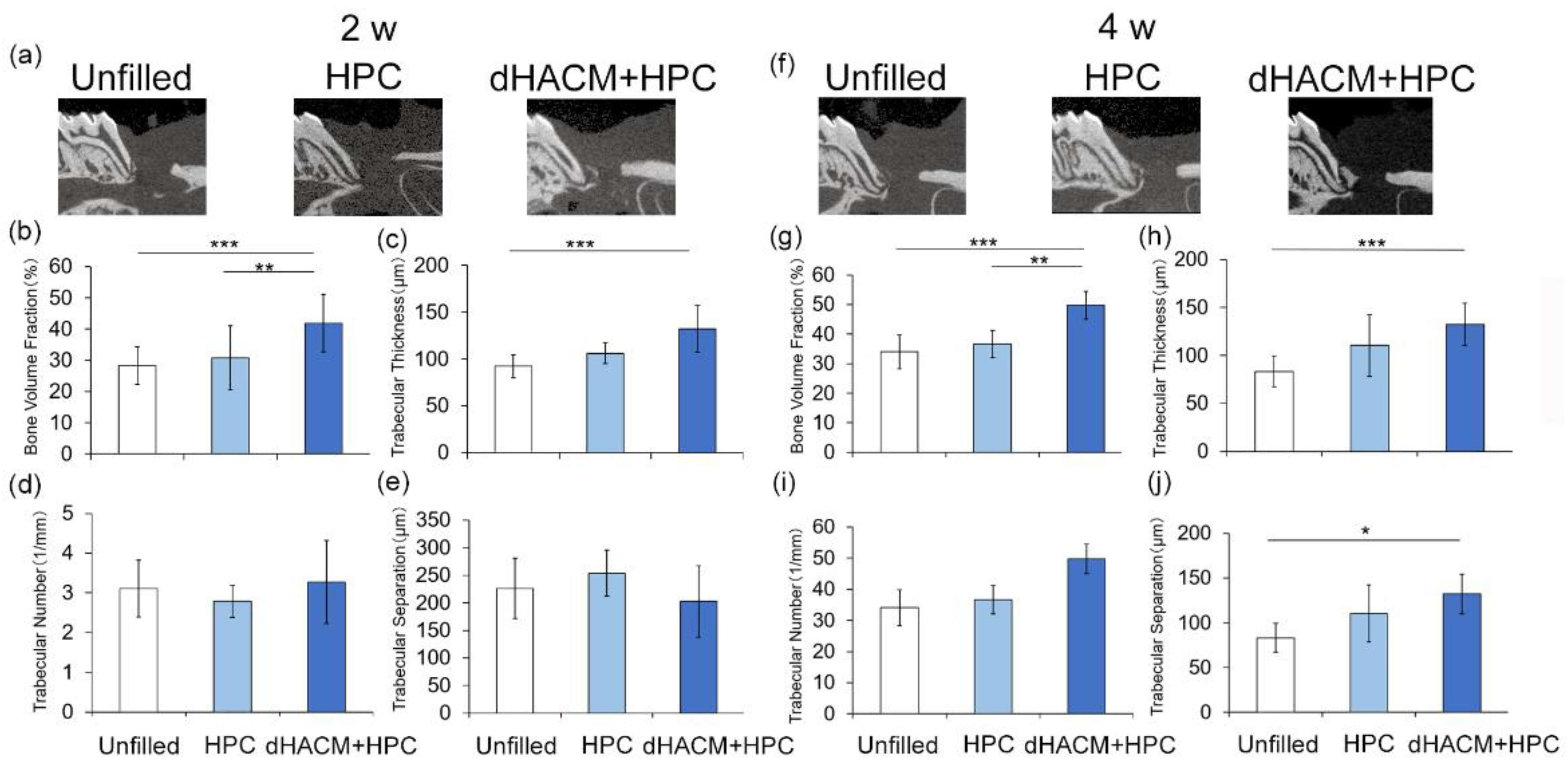
2.4. Microcomputed Tomography Analysis
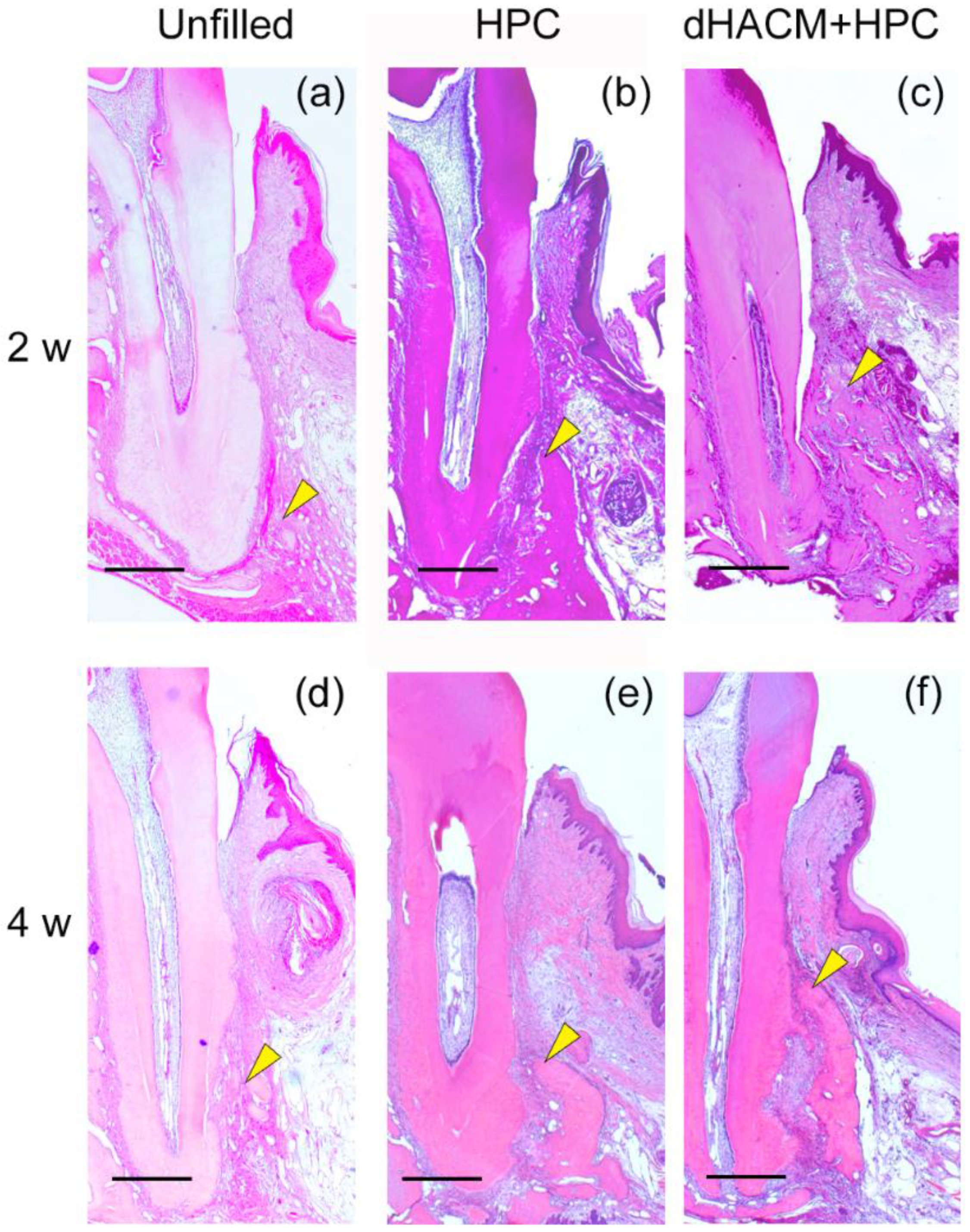
2.5. Histological Processing
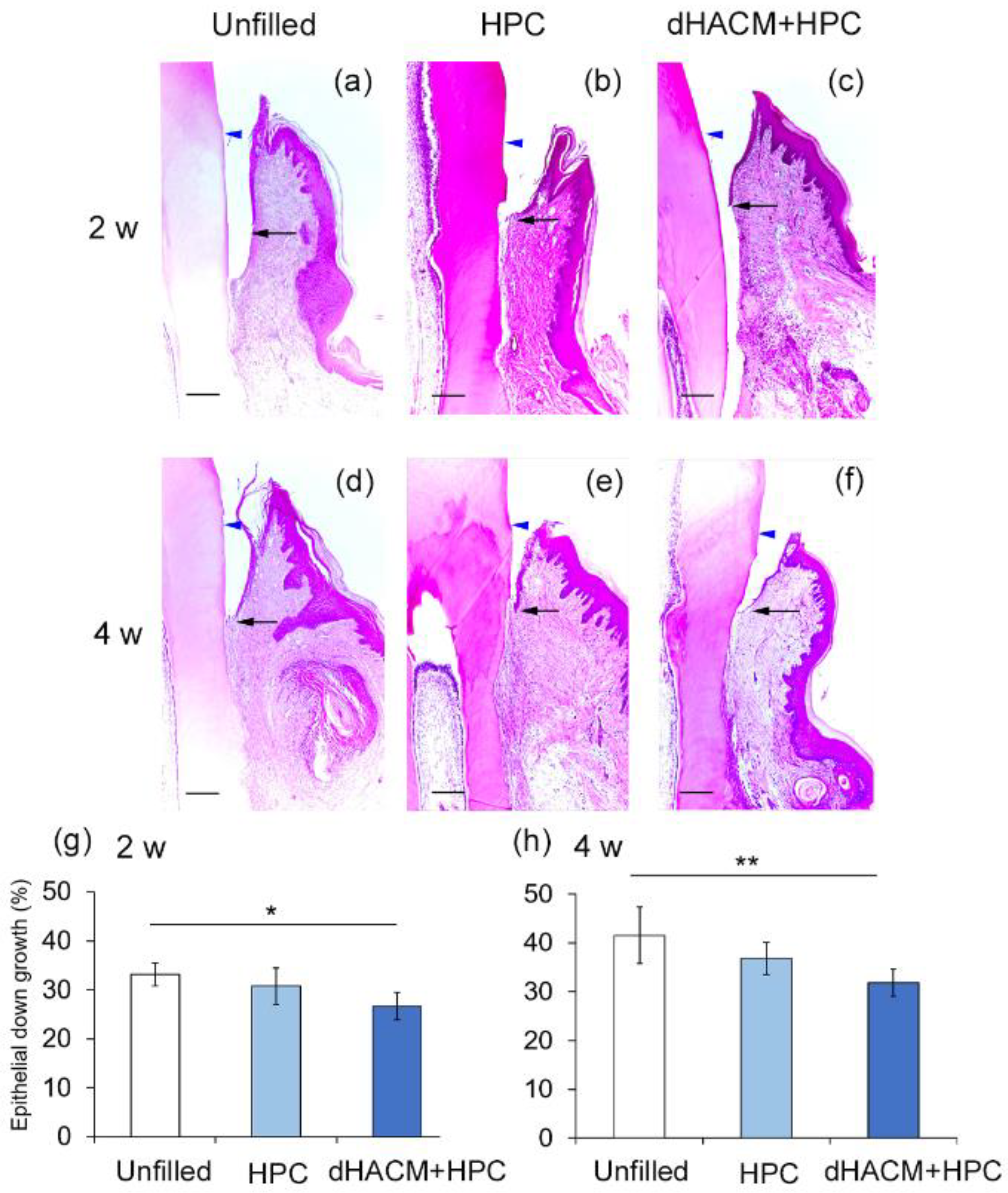
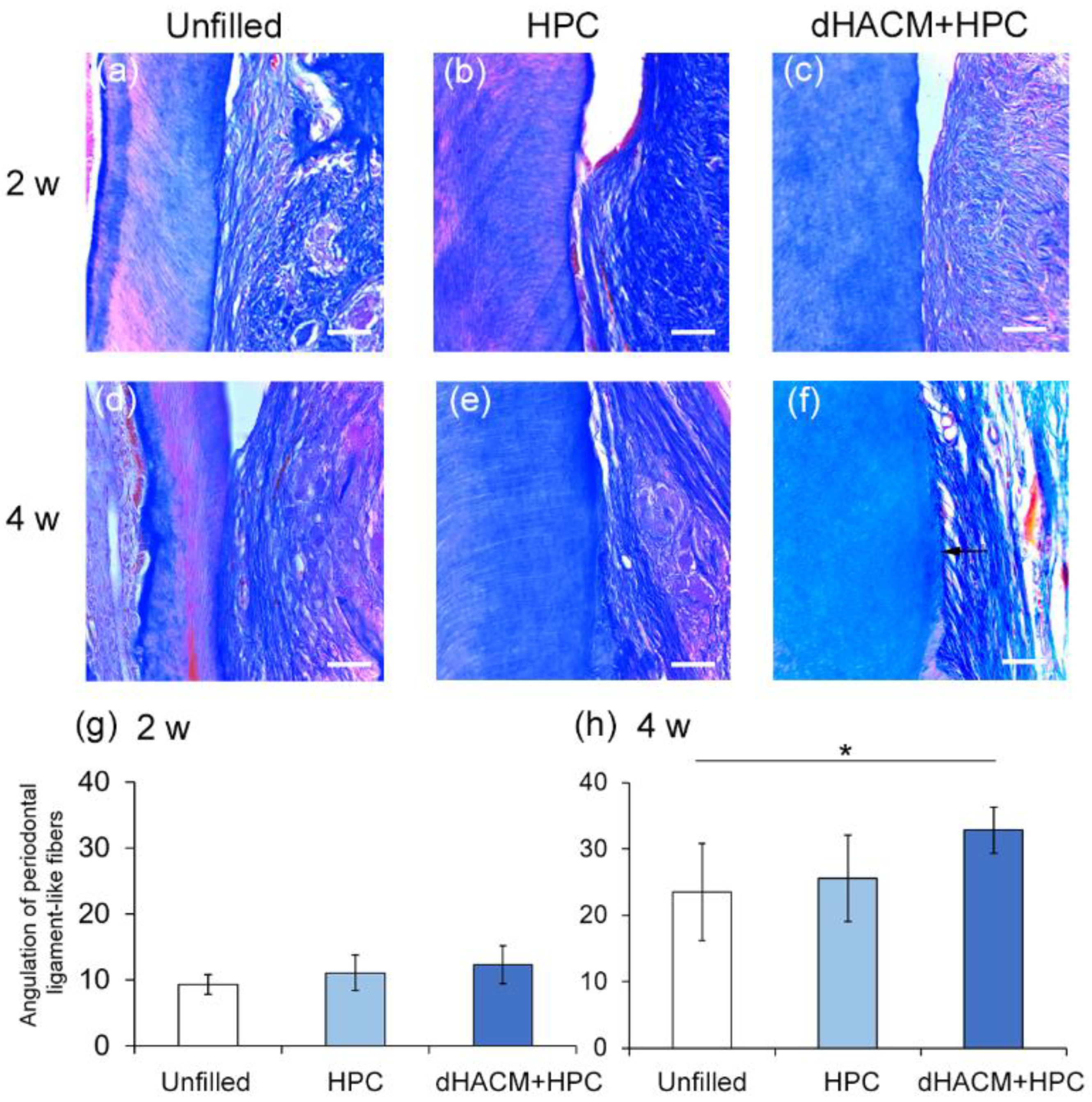
2.6. Histomorphometric Analysis
2.7. Immunohistochemistry
2.8. Preparation of dHACM Extract
2.9. Isolation of Rat Periodontal Ligamint-Derived Cells (rPDLCs) and Culturing Method
2.10. Cell Viability/Proliferation and Wound Healing Assays
2.11. Statistical Analysis
3. Results
3.1. Micro-CT Analysis of Defect Healing
3.2. Histological Observations
3.3. Histomorphometric Analysis
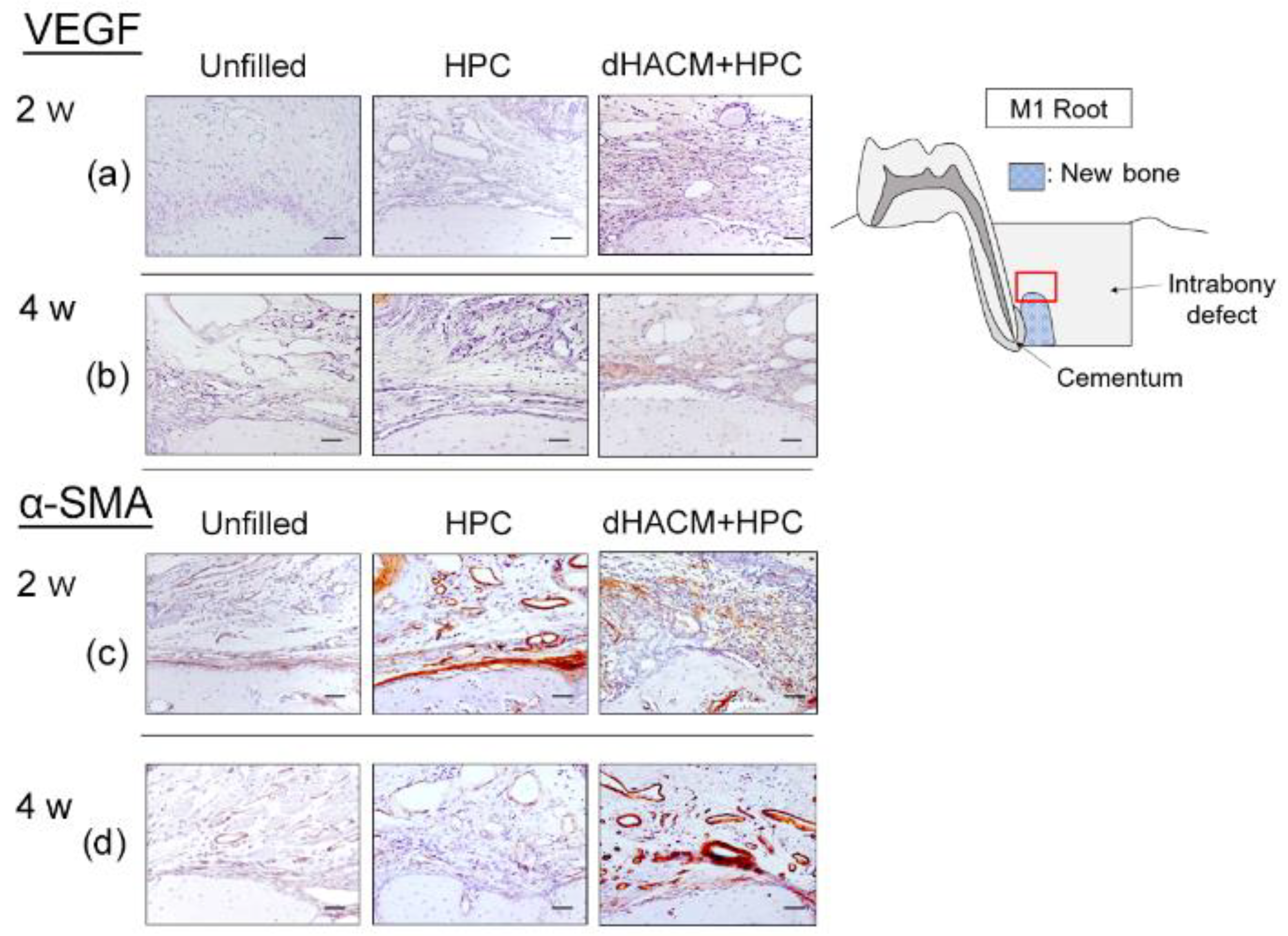
3.4. Immunohistochemical Analysis
3.5. The Concentration of VEGF and FGF-2 in the dHACM Extract
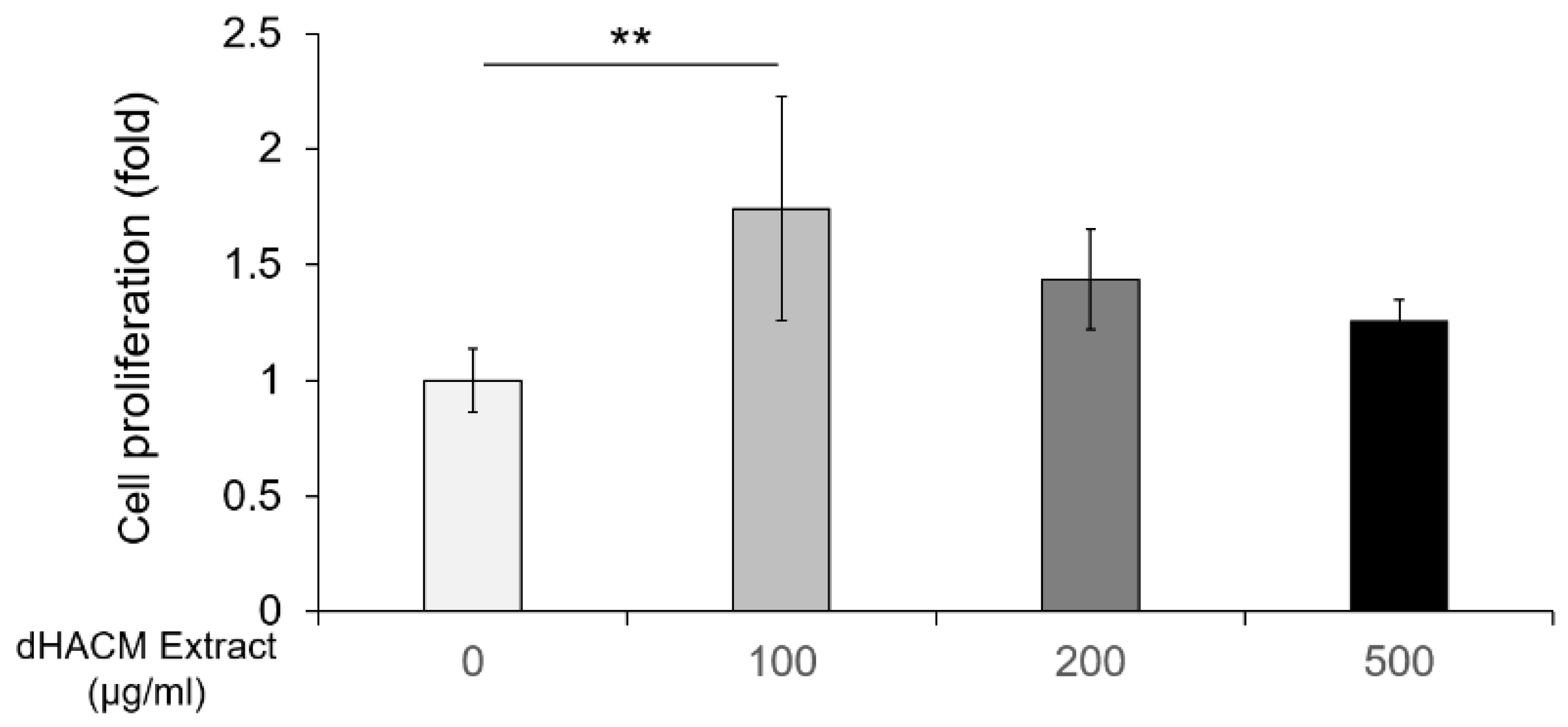
3.6. The Effect of dHACM Extract on Cell Proliferation
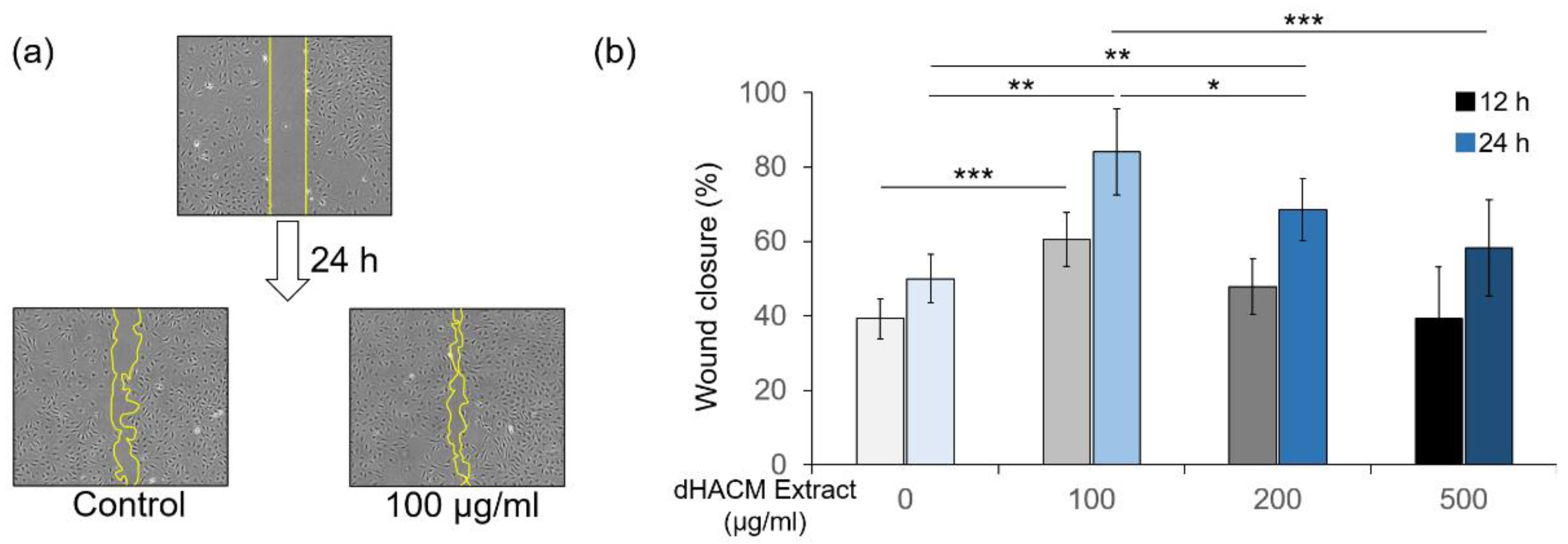
3.7. The Effect of dHACM Extract on Cell Migration
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ramseier, C.A.; Rasperini, G.; Batia, S.; Giannobile, W.V. Advanced reconstructive technologies for periodontal tissue repair. Periodontology 2000 2021, 59, 185–202. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rios, H.F.; Lin, Z.; Oh, B.; Park, C.H.; Giannobile, W.V. Cell- and gene-based therapeutic strategies for periodontal regenerative medicine. J. Periodontol. 2011, 82, 1223–1237. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, F.M.; Zhang, J.; Zhang, M.; An, Y.; Chen, F.; Wu, Z.F. A review on endogenous regenerative technology in periodontal regenerative medicine. Biomaterials 2010, 31, 7892–7927. [Google Scholar] [CrossRef] [PubMed]
- Parolini, O.; Alviano, F.; Bagnara, G.P.; Bilic, G.; Bühring, H.J.; Evangelista, M.; Hennerbichler, S.; Liu, B.; Magatti, M.; Mao, N.; et al. Concise review: Isolation and characterization of cells from human term placenta: Outcome of the first international workshop on placenta derived stem cells. Stem Cells 2008, 26, 300–311. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sawhney, C.P. Amniotic membrane as a biological dressing in the management of burns. Burns 1989, 15, 339–342. [Google Scholar] [CrossRef]
- Zelen, C.; Serena, T.E.; Denoziere, G.; Fetterolf, D.E. A prospective randomized comparative parallel study of amniotic membrane wound graft in the management of diabetic foot ulcers. Int. Wound J. 2013, 10, 502–507. [Google Scholar] [CrossRef]
- Russo, A.; Bonci, P.; Bonci, P. The effects of different preservation processes on the total protein and growth factor content in a new biological product developed from human amniotic membrane. Cell Tissue Bank 2012, 13, 353–361. [Google Scholar] [CrossRef]
- Koizumi, N.J.; Inatomi, T.J.; Sotozono, C.J.; Fullwood, N.J.; Quantock, A.J.; Kinoshita, S. Growth factor mRNA and protein in preserved human amniotic membrane. Curr. Eye Res. 2000, 20, 173–177. [Google Scholar] [CrossRef]
- Lopez-Valladares, M.J.; Rodriguez-Ares, M.T.; Tourino, R.; Gude, F.; Silva, T.M.; Couceiro, J. Donor age and gestational age influence on growth factor levels in human amniotic membrane. Acta Opththalmol. 2010, 88, e211–e216. [Google Scholar] [CrossRef]
- Sheikh, E.S.; Sheikh, E.S.; Fetterolf, D.E. Use of dehydrated human amniotic membrane allografts to promote healing in patients with refractory non healing wounds. Int. Wound J. 2014, 11, 711–717. [Google Scholar] [CrossRef]
- Parry, S.; Strauss, J.F. Premature rupture of the fetal membranes. N. Engl. J. Med. 1998, 338, 663–670. [Google Scholar] [CrossRef] [PubMed]
- Koob, T.J.; Lim, J.J.; Massee, M.; Zabek, N.; Rennert, R.; Gurtner, G.; Li, W.W. Angiogenic properties of dehydrated human amnion/chorion allografts: Therapeutic potential for soft tissue repair and regeneration. Vasc. Cell 2014, 1, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hassan, M.; Prakasam, S.; Bain, C.; Ghoneima, A.; Liu, S.S. A randomized split-mouth clinical trial on effectiveness of amnion-chorion membranes in alveolar ridge preservation: A clinical, radiologic, and morphometric study. Int. J. Oral Maxillofac. Implant. 2017, 32, 1389–1398. [Google Scholar] [CrossRef] [PubMed]
- Bhide, V.M.; Tenenbaum, H.C. Horizontal guided bone regeneration using a dehydrated amnion/chorion membrane: A case report. Int. J. Periodontics Restor. Dent. 2021, 41, 375–381. [Google Scholar] [CrossRef] [PubMed]
- Holtzclaw, D.J.; Toscano, N.J. Amnion–chorion allograft barrier used for guided tissue regeneration treatment of periodontal intrabony defects: A retrospective observational report. Clin. Adv. Periodontics 2013, 3, 131–137. [Google Scholar] [CrossRef]
- Hamada, Y.; Yeh, Y.T.; Blanchard, S.B. Amnion-chorion allograft barrier used on root surface for regenerative procedures: Case report. Clin. Adv. Periodontics 2020, 10, 195–199. [Google Scholar] [CrossRef]
- Oortgiesen, D.A.; Plachokova, A.S.; Geenen, C.; Meijer, G.J.; Walboomers, X.F.; Van den Beucken, J.J.; Jansen, J.A. Alkaline phosphatase immobilization onto Bio-Gide® and Bio-Oss® for periodontal and bone regeneration. J. Clin. Periodontol. 2012, 39, 546–555. [Google Scholar] [CrossRef]
- Takeuchi, T.; Bizenjima, T.; Ishii, Y.; Imamura, K.; Suzuki, E.; Seshima, F.; Saito, A. Enhanced healing of surgical periodontal defects in rats following application of a self-assembling peptide nanofibre hydrogel. J. Clin. Periodontol. 2016, 43, 279–288. [Google Scholar] [CrossRef]
- Bizenjima, T.; Seshima, F.; Ishizuka, Y.; Takeuchi, T.; Kinumatsu, T.; Saito, A. Fibroblast growth factor-2 promotes healing of surgically created periodontal defects in rats with early, streptozotocin-induced diabetes via increasing cell proliferation and regulating angiogenesis. J. Clin. Periodontol. 2015, 42, 62–71. [Google Scholar] [CrossRef]
- Park, C.H.; Rios, H.F.; Jin, Q.; Sugai, J.V.; Padial-Molina, M.; Taut, A.D.; Flanagan, C.L.; Hollister, S.J.; Giannobile, W.V. Tissue engineering bone-ligament complexes using fiber-guiding scaffolds. Biomaterials 2012, 33, 137–145. [Google Scholar] [CrossRef] [Green Version]
- Lucarini, G.; Zizzi, A.; Aspriello, S.D.; Ferrante, L.; Tosco, E.; Muzio, L.L.; Foglini, P.; Mattioli-Belmonte, M.; Primio, R.D.; Piemontese, M. Involvement of vascular endothelial growth factor, CD44 and CD133 in periodontal disease and diabetes: An immunohistochemical study. J. Clin. Periodontol. 2009, 36, 3–10. [Google Scholar] [CrossRef] [PubMed]
- Matsui, M.; Tabata, Y. Enhanced angiogenesis by multiple release of platelet-rich plasma contents and basic fibroblast growth factor from gelatin hydrogels. Acta Biomater. 2012, 8, 1792–1801. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Inoue, T.; Deporter, D.A.; Melcher, A.H. Induction of chondrogenesis in muscle, skin, bone marrow, and periodontal ligament by demineralized dentin and bone matrix in vivo and in vitro. J. Dent. Res. 1986, 65, 12–22. [Google Scholar] [CrossRef] [PubMed]
- Imamura, K.; Kokubu, E.; Kita, D.; Ota, K.; Ishihara, K.; Saito, A. Cigarette smoke condensate modulates migration of human gingival epithelial cells and their interactions with Porphyromonas gingivalis. J. Periodontal. Res. 2015, 50, 411–421. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosen, P.S.; Froum, S.J.; Cohen, D.W. Consecutive Case Series Using a Composite Allograft Containing Mesenchymal Cells with an Amnion-Chorion Barrier to Treat Mandibular Class III/IV Furcations. Int. J. Periodontics Restor. Dent. 2015, 35, 453–460. [Google Scholar] [CrossRef] [Green Version]
- Nyman, S. Bone regeneration using the principle of guided tissue regeneration. J. Clin. Periodontol. 1991, 18, 494–498. [Google Scholar] [CrossRef]
- Yanagita, M.; Kojima, Y.; Kubota, M.; Mori, K.; Yamashita, M.; Yamada, S.; Kitamura, M.; Murakami, S. Cooperative effects of FGF-2 and VEGF-A in periodontal ligament cells. J. Dent. Res. 2014, 93, 89–95. [Google Scholar] [CrossRef] [Green Version]
- Dvorak, H.; Brown, L.; Detmar, M.; Dvorak, A. Vascular permeability factor/vascular endothelial growth factor: Microvascular permeability and angiogenesis. Am. J. Pathol. 1995, 146, 1029–1039. [Google Scholar]
- Nissen, N.; Polverini, P.; Koch, A.; Volin, M.; Gamelli, R.; DiPietro, L. Vascular endothelial growth factor mediates angiogenic activity during the proliferative phase of wound healing. Am. J. Pathol. 1998, 152, 1445–1452. [Google Scholar]
- Murakami, T.; Matsugami, D.; Yoshida, W.; Imamura, K.; Bizenjima, T.; Seshima, F.; Saito, A. Healing of experimental periodontal defects following treatment with fibroblast growth factor-2 and deproteinized bovine bone mineral. Biomolecules 2021, 11, 805. [Google Scholar] [CrossRef]
- Armulik, A.; Genove, G.; Betsholtz, C. Pericytes: Developmental, physiological, and pathological perspectives, problems, and promises. Dev. Cell 2011, 21, 193–215. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seo, B.M.; Miura, M.; Gronthos, S.; Bartold, P.M.; Batouli, S.; Brahim, J.; Young, M.; Robey, P.G.; Wang, C.Y.; Shi, S. Investigation of multipotent postnatal stem cells from human periodontal ligament. Lancet 2004, 364, 149–155. [Google Scholar] [CrossRef]
- Cho, M.I.; Garant, P.R. Development and general structure of the periodontium. Periodontol. 2000 2000, 24, 9–27. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | Unfilled | HPC | dHACM+HPC | |
|---|---|---|---|---|
| VEGF | 2 W | 7.7 ± 1.6 | 10.5 ± 3.2 | 17.4 ± 3.1 a |
| 4 W | 10.3 ± 1.0 | 14.3 ± 2.5 | 17.9 ± 2.6 a | |
| α-SMA | 2 W | 9.7 ± 3.6 | 11.3 ± 3.0 | 12.0 ± 4.6 |
| 4 W | 11.8 ± 3.1 | 11.7 ± 4.5 | 20.7 ± 4.9 a,b | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Imamura, K.; Hamada, Y.; Yoshida, W.; Murakami, T.; Nakane-Koyachi, S.; Yoshikawa, K.; Saito, A. Investigating the Effects of Dehydrated Human Amnion-Chorion Membrane on Periodontal Healing. Biomolecules 2022, 12, 857. https://0-doi-org.brum.beds.ac.uk/10.3390/biom12060857
Imamura K, Hamada Y, Yoshida W, Murakami T, Nakane-Koyachi S, Yoshikawa K, Saito A. Investigating the Effects of Dehydrated Human Amnion-Chorion Membrane on Periodontal Healing. Biomolecules. 2022; 12(6):857. https://0-doi-org.brum.beds.ac.uk/10.3390/biom12060857
Chicago/Turabian StyleImamura, Kentaro, Yusuke Hamada, Wataru Yoshida, Tasuku Murakami, Saki Nakane-Koyachi, Kouki Yoshikawa, and Atsushi Saito. 2022. "Investigating the Effects of Dehydrated Human Amnion-Chorion Membrane on Periodontal Healing" Biomolecules 12, no. 6: 857. https://0-doi-org.brum.beds.ac.uk/10.3390/biom12060857