An Examination of People’s Privacy Concerns, Perceptions of Social Benefits, and Acceptance of COVID-19 Mitigation Measures That Harness Location Information: A Comparative Study of the U.S. and South Korea


Abstract
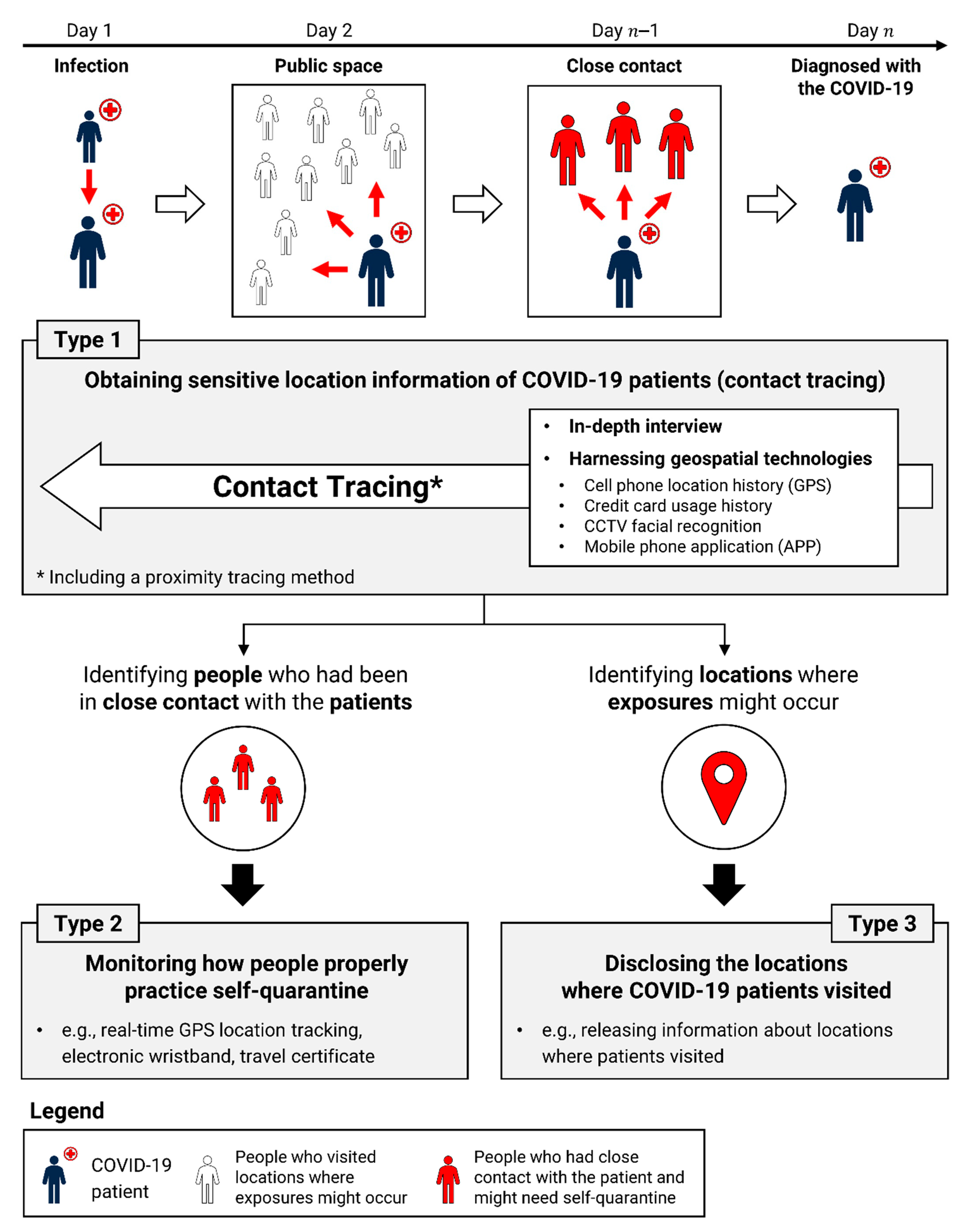
:1. Introduction
2. Data and Methods
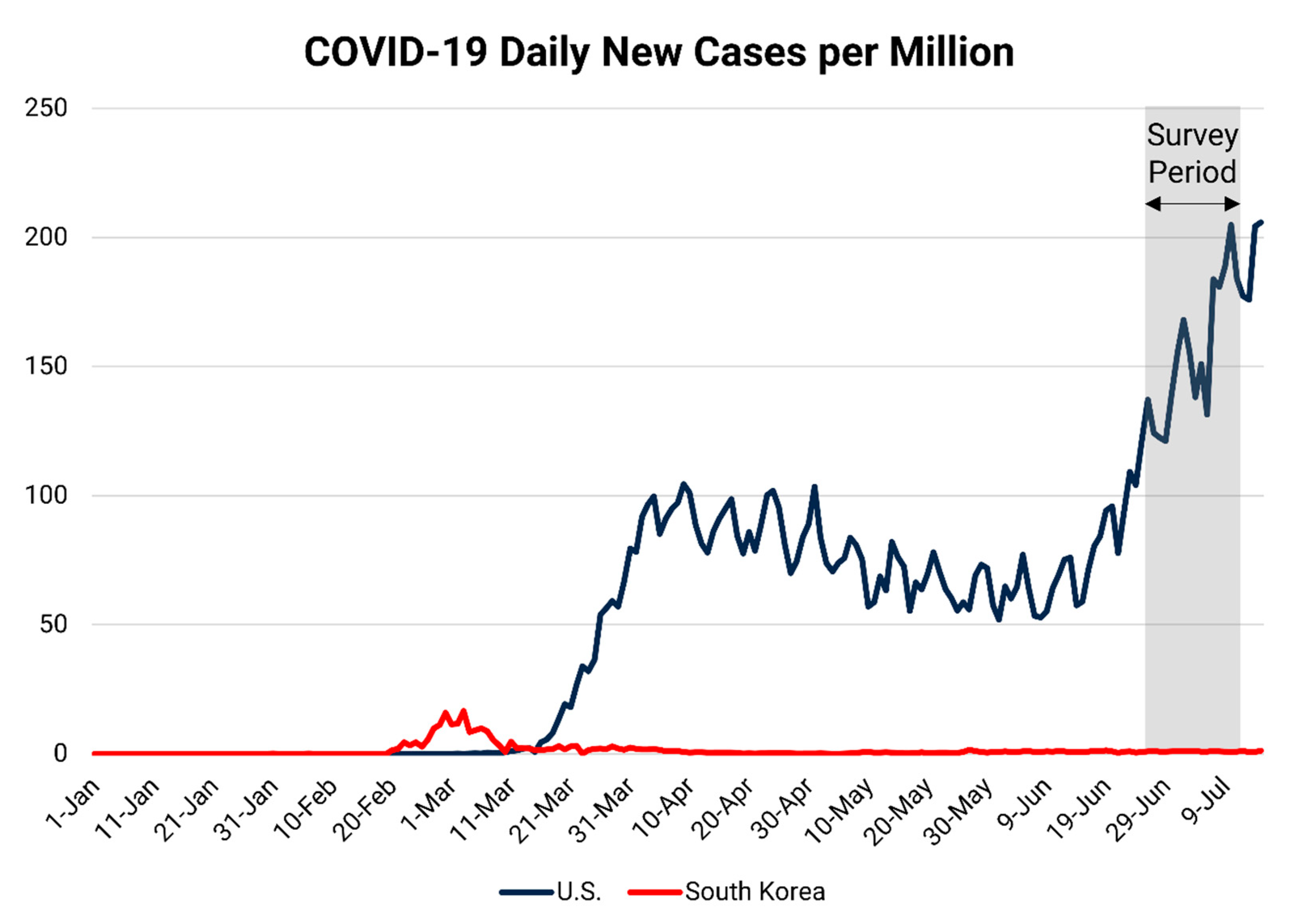
2.1. Data Collection
2.2. Survey Questionnaire
3. Results
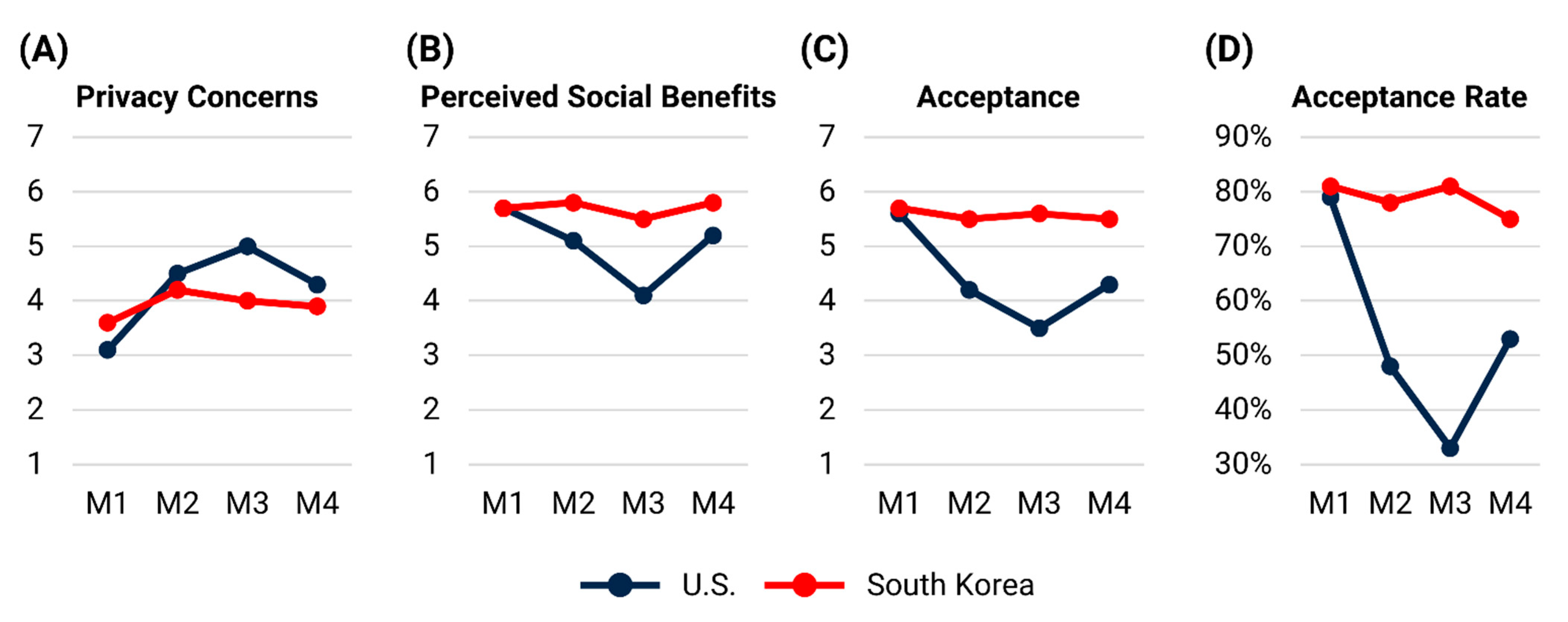
3.1. Privacy Concerns, Perceptions of Social Benefits, and Acceptance of COVID-19 Contact Tracing Methods (M1–4)
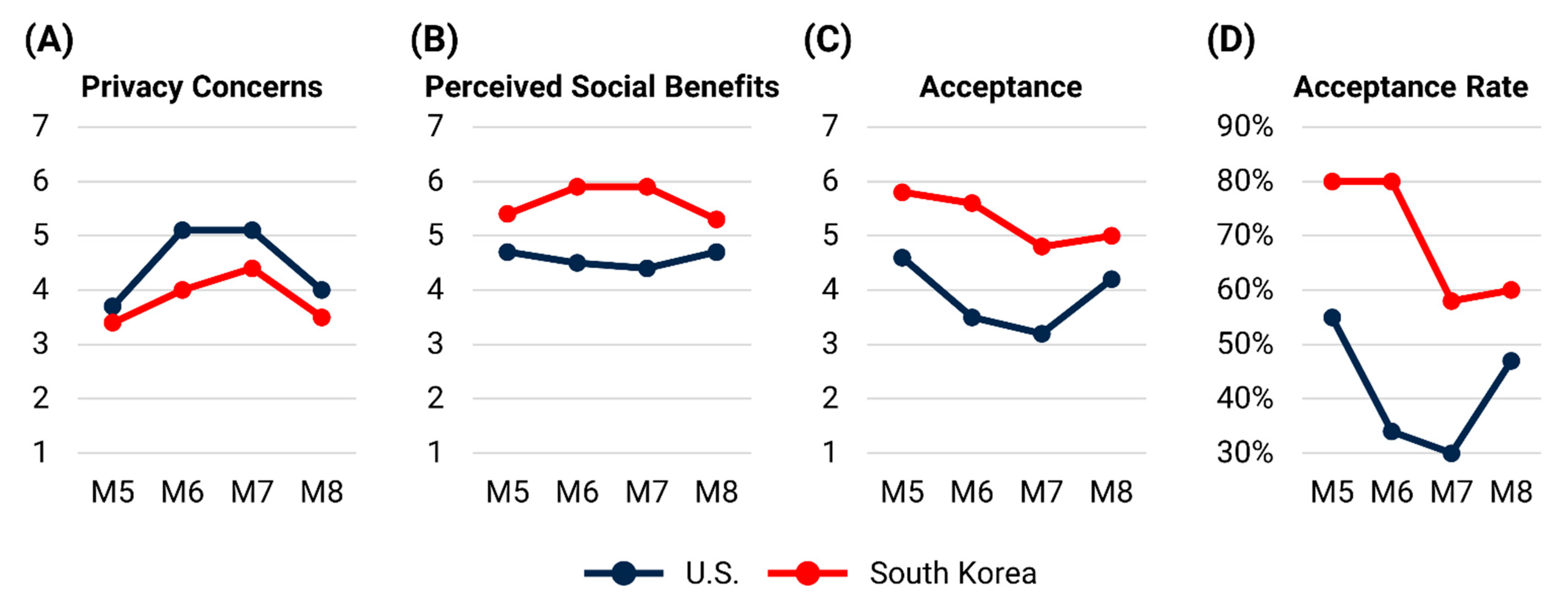
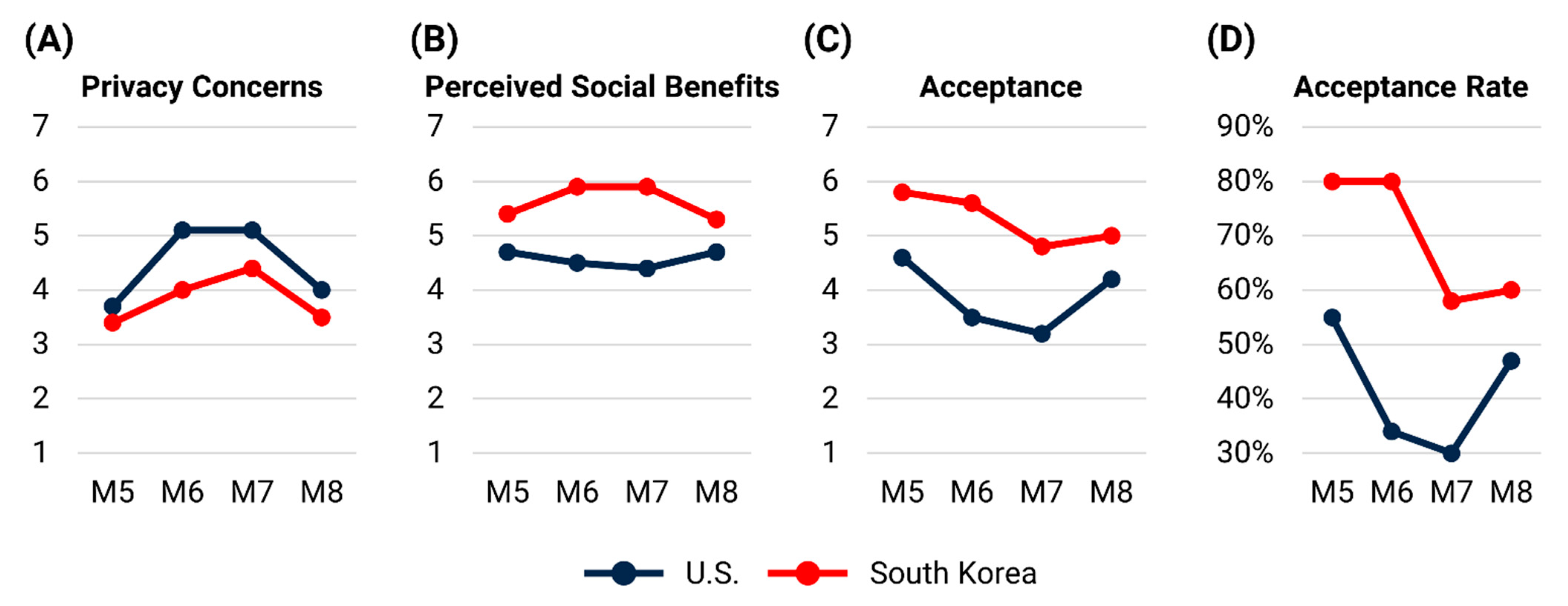
3.2. Privacy Concerns, Perceptions of Social Benefits, and Acceptance of Self-Quarantine Monitoring Methods (M5–8)
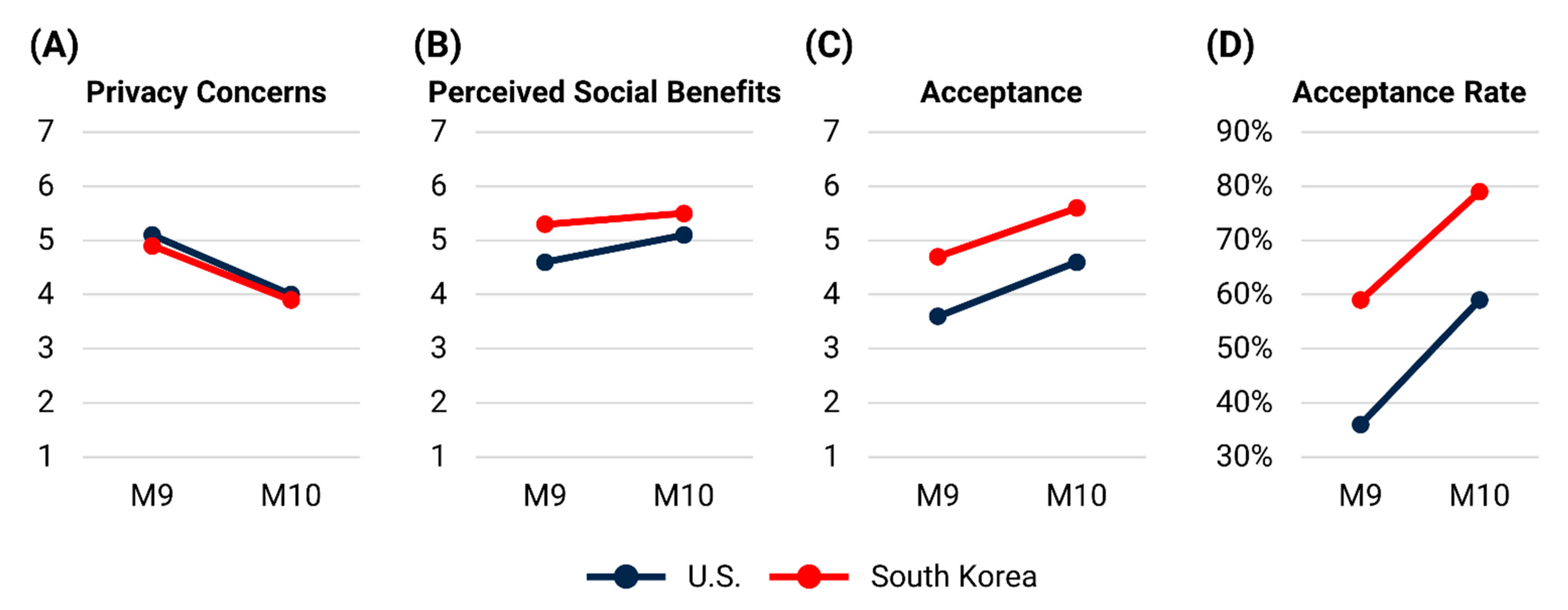
3.3. Privacy Concerns, Perceptions of Social Benefits, and Acceptance of Location Disclosure Methods (M9–10)
3.4. Acceptance with Respect to Sociodemographic Characteristics
4. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Method | Type | Instructions |
|---|---|---|
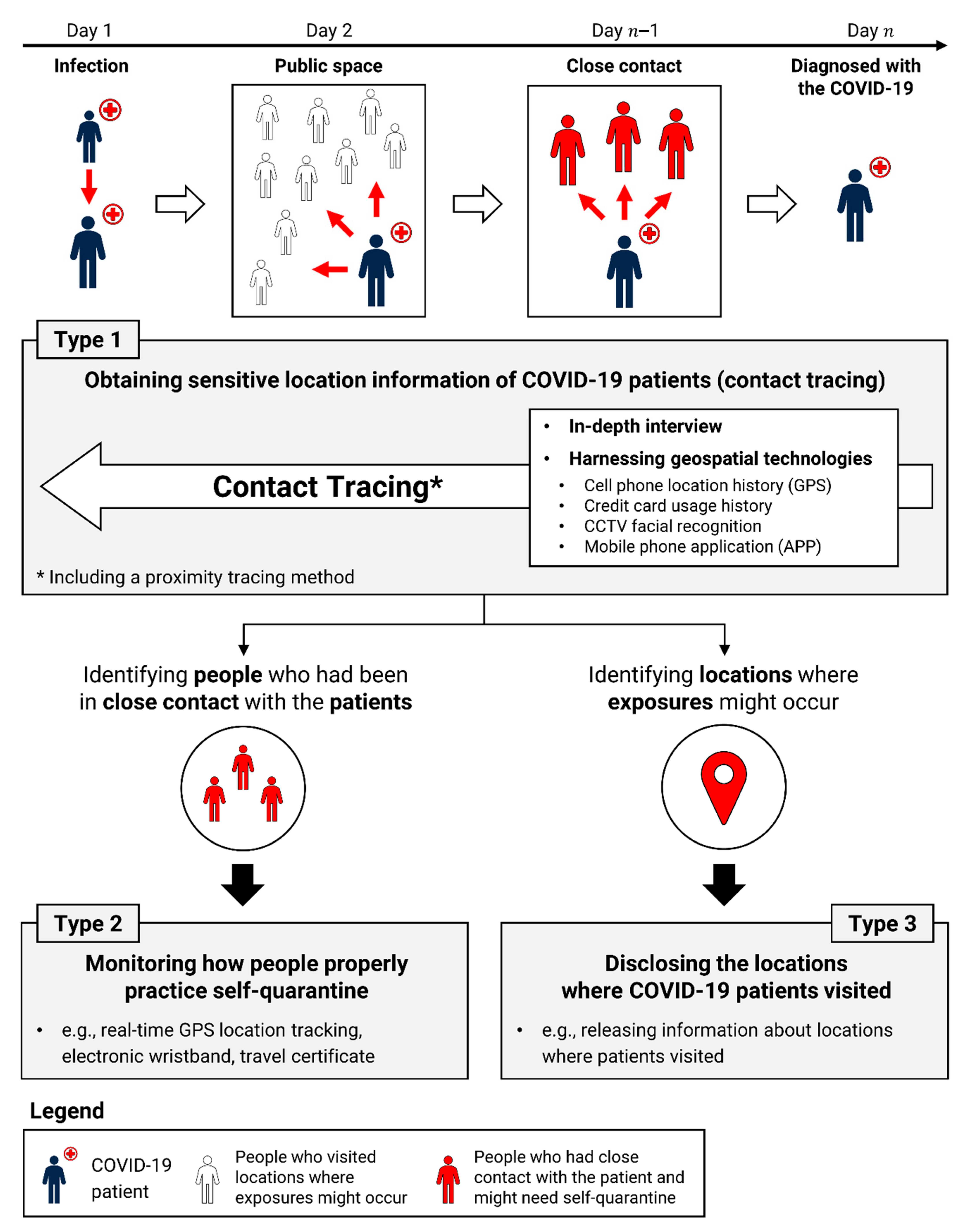
| M1 | Contact Tracing | Assume that you are diagnosed with COVID-19. Government agencies (e.g., public health authorities) conduct an in-depth interview with you to identify locations of your major activities in the past few days. The obtained information is only shared by public health authorities and other relevant government agencies and is NOT open or available to the public. |
| M2 | Assume that you are diagnosed with COVID-19. Government agencies (e.g., public health authorities) obtain the location information in your mobile phone location history (e.g., based on cell-tower or GPS signals) to identify the locations of your main activities in the past few days. The obtained information is only shared by public health authorities and other relevant government agencies and is NOT open or available to the public. | |
| M3 | Assume that you are diagnosed with COVID-19. Government agencies (e.g., public health authorities) obtain the location information from your debit/credit card transaction history to identify the locations of your main activities in the past few days. The obtained information is only shared by public health authorities and other relevant government agencies and is NOT open or available to the public. | |
| M4 | Government agencies (e.g., public health authorities) launch a mobile phone application that records the anonymized ID of other application users who are in close contact (physical proximity) with you by using Bluetooth technology. The application does NOT collect your actual location (e.g., longitude and latitude). It also does NOT send real-time close-contact information to government agencies. Assume that government agencies request you (and other citizens as well) to install the application. Additionally, assume that you are diagnosed with COVID-19. In this case, your records of close contacts will be shared with government agencies so that the agencies can alert people who were in close contact with you. Please be advised that the government agencies do NOT share your identity (e.g., name) with other application users. | |
| M5 | Self-Quarantine Monitoring | Assume that you are required to self-quarantine at your home. Government agencies (e.g., public health authorities) monitor your location (i.e., whether you indeed are staying at your home) by calling you at a random time on some of the days of your self-quarantine period. |
| M6 | Assume that you are required to self-quarantine at your home. Government agencies (e.g., public health authorities) monitor your real-time location (i.e., whether you indeed are staying at your home) by using the real-time location obtained from your mobile phone’s wireless and GPS signals. | |
| M7 | Assume that you are required to self-quarantine at your home. Government agencies (e.g., public health authorities) monitor your real-time location (i.e., whether you indeed are staying at your home) by requesting you to wear an electronic wristband that sends your real-time location information to the government agencies. Note that you should keep wearing your electronic wristband during the self-quarantine period. | |
| M8 | Assume that government agencies (e.g., public health authorities) request you to install a mobile phone application that carries your travel certificate. Your travel certificate is valid only when you are NOT required to self-quarantine. However, if you are required to self-quarantine, your travel certificate becomes invalid. Specifically, you must display your valid travel certificate to the government agencies or other responsible agencies when using public transit or visiting public spaces (e.g., libraries, markets, etc.). Note that the travel certificate does NOT collect your real-time location data. | |
| M9 | Location Disclosure | Assume that you are diagnosed with COVID-19. Government agencies (e.g., public health authorities) disclose to the public the time and locations (e.g., street address) where COVID-19 patients (including you) have visited in the past few days as well as the patients’ information on age and gender. However, the locations disclosed do NOT include patients’ home addresses. |
| M10 | Assume that you are diagnosed with COVID-19. Government agencies (e.g., public health authorities) disclose to the public the time and locations (e.g., street address) where COVID-19 patients (including you) have visited in the past few days. However, the locations disclosed do NOT include patients’ home addresses. Additionally, patients’ age and gender information are NOT disclosed. |
| Methods | Country | Privacy Concerns | ||||||
|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | ||
| M1 | U.S. | 32% | 14% | 12% | 19% | 10% | 5% | 7% |
| South Korea | 18% | 16% | 14% | 13% | 21% | 12% | 6% | |
| M2 | U.S. | 12% | 9% | 12% | 15% | 19% | 10% | 24% |
| South Korea | 11% | 14% | 13% | 10% | 26% | 13% | 13% | |
| M3 | U.S. | 10% | 5% | 9% | 13% | 18% | 15% | 32% |
| South Korea | 15% | 14% | 9% | 15% | 17% | 19% | 9% | |
| M4 | U.S. | 11% | 13% | 13% | 15% | 15% | 9% | 24% |
| South Korea | 14% | 15% | 12% | 19% | 15% | 11% | 14% | |
| M5 | U.S. | 25% | 9% | 12% | 20% | 13% | 7% | 15% |
| South Korea | 23% | 16% | 16% | 14% | 12% | 11% | 8% | |
| M6 | U.S. | 7% | 6% | 7% | 12% | 19% | 13% | 35% |
| South Korea | 17% | 10% | 15% | 11% | 20% | 14% | 13% | |
| M7 | U.S. | 10% | 4% | 7% | 13% | 19% | 8% | 39% |
| South Korea | 14% | 8% | 14% | 14% | 10% | 20% | 19% | |
| M8 | U.S. | 20% | 12% | 11% | 14% | 14% | 9% | 21% |
| South Korea | 19% | 19% | 18% | 17% | 8% | 9% | 10% | |
| M9 | U.S. | 7% | 2% | 11% | 10% | 23% | 14% | 32% |
| South Korea | 8% | 8% | 5% | 13% | 18% | 22% | 25% | |
| M10 | U.S. | 14% | 11% | 18% | 16% | 20% | 6% | 15% |
| South Korea | 16% | 10% | 14% | 19% | 19% | 12% | 8% | |
| Methods | Country | Perceived Social Benefits | ||||||
|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | ||
| M1 | U.S. | 5% | 4% | 2% | 8% | 13% | 17% | 51% |
| South Korea | 2% | 3% | 1% | 9% | 22% | 31% | 33% | |
| M2 | U.S. | 9% | 5% | 6% | 11% | 16% | 20% | 32% |
| South Korea | 1% | 3% | 5% | 6% | 15% | 32% | 38% | |
| M3 | U.S. | 15% | 10% | 13% | 12% | 23% | 9% | 18% |
| South Korea | 1% | 3% | 3% | 17% | 14% | 31% | 31% | |
| M4 | U.S. | 6% | 4% | 5% | 16% | 16% | 19% | 33% |
| South Korea | 0% | 2% | 3% | 10% | 21% | 31% | 33% | |
| M5 | U.S. | 12% | 7% | 8% | 14% | 18% | 16% | 26% |
| South Korea | 1% | 5% | 7% | 11% | 19% | 28% | 29% | |
| M6 | U.S. | 13% | 10% | 5% | 19% | 15% | 18% | 21% |
| South Korea | 1% | 1% | 6% | 8% | 10% | 37% | 37% | |
| M7 | U.S. | 18% | 3% | 7% | 17% | 21% | 15% | 20% |
| South Korea | 1% | 0% | 4% | 11% | 14% | 31% | 39% | |
| M8 | U.S. | 12% | 5% | 6% | 18% | 20% | 15% | 23% |
| South Korea | 0% | 3% | 10% | 19% | 19% | 20% | 28% | |
| M9 | U.S. | 11% | 7% | 10% | 14% | 23% | 13% | 22% |
| South Korea | 2% | 3% | 7% | 16% | 21% | 25% | 25% | |
| M10 | U.S. | 7% | 4% | 6% | 13% | 22% | 18% | 30% |
| South Korea | 0% | 2% | 3% | 14% | 27% | 26% | 27% | |
| Methods | Country | Acceptance | ||||||
|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | ||
| M1 | U.S. | 5% | 1% | 4% | 11% | 19% | 20% | 40% |
| South Korea | 1% | 1% | 4% | 13% | 19% | 27% | 36% | |
| M2 | U.S. | 16% | 7% | 16% | 13% | 15% | 17% | 16% |
| South Korea | 1% | 3% | 6% | 13% | 22% | 25% | 31% | |
| M3 | U.S. | 26% | 10% | 20% | 12% | 11% | 8% | 14% |
| South Korea | 1% | 2% | 5% | 11% | 26% | 19% | 36% | |
| M4 | U.S. | 18% | 6% | 7% | 16% | 23% | 14% | 16% |
| South Korea | 2% | 3% | 4% | 16% | 18% | 26% | 31% | |
| M5 | U.S. | 16% | 4% | 7% | 18% | 13% | 17% | 25% |
| South Korea | 0% | 1% | 9% | 10% | 8% | 31% | 42% | |
| M6 | U.S. | 27% | 10% | 16% | 13% | 11% | 10% | 13% |
| South Korea | 0% | 7% | 8% | 6% | 14% | 26% | 40% | |
| M7 | U.S. | 32% | 12% | 15% | 11% | 17% | 4% | 9% |
| South Korea | 6% | 10% | 12% | 14% | 13% | 19% | 26% | |
| M8 | U.S. | 21% | 5% | 10% | 17% | 14% | 14% | 19% |
| South Korea | 3% | 3% | 10% | 23% | 16% | 17% | 27% | |
| M9 | U.S. | 22% | 12% | 13% | 17% | 17% | 7% | 12% |
| South Korea | 6% | 8% | 14% | 14% | 21% | 15% | 23% | |
| M10 | U.S. | 11% | 7% | 10% | 13% | 22% | 14% | 23% |
| South Korea | 1% | 3% | 5% | 12% | 21% | 23% | 35% | |
References
- Anderson, R.M.; Heesterbeek, H.; Klinkenberg, D.; Hollingsworth, T.D. How Will Country-Based Mitigation Measures Influence the Course of the COVID-19 Epidemic? Lancet 2020, 395, 931–934. [Google Scholar] [CrossRef]
- Bedford, J.; Enria, D.; Giesecke, J.; Heymann, D.L.; Ihekweazu, C.; Kobinger, G.; Lane, H.C.; Memish, Z.; Oh, M.-D.; Sall, A.A.; et al. WHO Strategic and Technical Advisory Group for Infectious Hazards. COVID-19: Towards Controlling of a Pandemic. Lancet 2020, 395, 1015–1018. [Google Scholar] [CrossRef]
- COVID-19 Map-Johns Hopkins Coronavirus Resource Center. Available online: https://0-coronavirus-jhu-edu.brum.beds.ac.uk/map.html (accessed on 20 September 2020).
- Ekong, I.; Chukwu, E.; Chukwu, M. COVID-19 Mobile Positioning Data Contact Tracing and Patient Privacy Regulations: Exploratory Search of Global Response Strategies and the Use of Digital Tools in Nigeria. JMIR MHealth UHealth 2020, 8, e19139. [Google Scholar] [CrossRef] [PubMed]
- Oliver, N.; Lepri, B.; Sterly, H.; Lambiotte, R.; Deletaille, S.; De Nadai, M.; Letouzé, E.; Salah, A.A.; Benjamins, R.; Cattuto, C.; et al. Mobile Phone Data for Informing Public Health Actions across the COVID-19 Pandemic Life Cycle. Sci. Adv. 2020, 6, eabc0764. [Google Scholar] [CrossRef]
- Kamel Boulos, M.N.; Geraghty, E.M. Geographical Tracking and Mapping of Coronavirus Disease COVID-19/Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Epidemic and Associated Events around the World: How 21st Century GIS Technologies Are Supporting the Global Fight against Outbreaks and Epidemics. Int. J. Health Geogr. 2020, 19, 8. [Google Scholar] [PubMed] [Green Version]
- Buckee, C.O.; Balsari, S.; Chan, J.; Crosas, M.; Dominici, F.; Gasser, U.; Grad, Y.H.; Grenfell, B.; Halloran, M.E.; Kraemer, M.U.G.; et al. Aggregated Mobility Data Could Help Fight COVID-19. Science 2020, 368, 145–146. [Google Scholar] [PubMed] [Green Version]
- Kang, J.-Y.; Michels, A.; Lyu, F.; Wang, S.; Agbodo, N.; Freeman, V.L.; Wang, S. Rapidly Measuring Spatial Accessibility of COVID-19 Healthcare Resources: A Case Study of Illinois, USA. Int. J. Health Geogr. 2020, 19, 36. [Google Scholar] [CrossRef]
- Smith, C.D.; Mennis, J. Incorporating Geographic Information Science and Technology in Response to the COVID-19 Pandemic. Prev. Chronic Dis. 2020, 17, E58. [Google Scholar] [CrossRef]
- Yang, C.; Sha, D.; Liu, Q.; Li, Y.; Lan, H.; Guan, W.W.; Hu, T.; Li, Z.; Zhang, Z.; Thompson, J.H.; et al. Taking the Pulse of COVID-19: A Spatiotemporal Perspective. Int. J. Digit. Earth 2020, 13, 1186–1211. [Google Scholar] [CrossRef]
- Eames, K.T.D.; Keeling, M.J. Contact Tracing and Disease Control. Proc. Biol. Sci. 2003, 270, 2565–2571. [Google Scholar] [CrossRef] [Green Version]
- A National Plan to Enable Comprehensive COVID-19 Case Finding and Contact Tracing in the US. Available online: https://www.centerforhealthsecurity.org/our-work/pubs_archive/pubs-pdfs/2020/200410-national-plan-to-contact-tracing.pdf (accessed on 20 September 2020).
- Sonn, J.W.; Kang, M.; Choi, Y. Smart City Technologies for Pandemic Control without Lockdown. Int. J. Urban Sci. 2020, 24, 149–151. [Google Scholar] [CrossRef]
- Ferretti, L.; Wymant, C.; Kendall, M.; Zhao, L.; Nurtay, A.; Abeler-Dörner, L.; Parker, M.; Bonsall, D.; Fraser, C. Quantifying SARS-CoV-2 Transmission Suggests Epidemic Control with Digital Contact Tracing. Science 2020, 368, eabb6936. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kwan, M.-P.; Casas, I.; Schmitz, B. Protection of Geoprivacy and Accuracy of Spatial Information: How Effective Are Geographical Masks? Cartogr. Int. J. Geogr. Inf. Geovis. 2004, 39, 15–28. [Google Scholar] [CrossRef]
- Hawryluck, L.; Gold, W.L.; Robinson, S.; Pogorski, S.; Galea, S.; Styra, R. SARS Control and Psychological Effects of Quarantine, Toronto, Canada. Emerg. Infect. Dis. 2004, 10, 1206–1212. [Google Scholar] [CrossRef] [PubMed]
- Mandavilli, A. SARS Epidemic Unmasks Age-Old Quarantine Conundrum. Nat. Med. 2003, 9, 487. [Google Scholar] [CrossRef]
- Mann, B. Some States to Out-of-Towners: If You Come Visit, Plan to Quarantine for 2 Weeks; NPR: Washington, DC, USA, 2020. [Google Scholar]
- Kitchin, R. Civil Liberties or Public Health, or Civil Liberties and Public Health? Using Surveillance Technologies to Tackle the Spread of COVID-19. Space Polity 2020, 1–20. [Google Scholar] [CrossRef]
- Lin, L.; Hou, Z. Combat COVID-19 with Artificial Intelligence and Big Data. J. Travel Med. 2020, 27. [Google Scholar] [CrossRef]
- Sharma, T.; Bashir, M. Use of Apps in the COVID-19 Response and the Loss of Privacy Protection. Nat. Med. 2020, 26, 1165–1167. [Google Scholar] [CrossRef]
- Sang-Hun, C.; Krolik, A.; Zhong, R.; Singer, N. Major Security Flaws Found in South Korea Quarantine App; The New York Times: New York, NY, USA, 2020. [Google Scholar]
- Her, M. How Is COVID-19 Affecting South Korea? What Is Our Current Strategy? Disaster Med. Public Health Prep. 2020, 14, 684–686. [Google Scholar] [CrossRef] [Green Version]
- Moon, M.J. Fighting COVID-19 with Agility, Transparency, and Participation: Wicked Policy Problems and New Governance Challenges. Public Adm. Rev. 2020, 80, 651–656. [Google Scholar] [CrossRef]
- Brownstein, J.S.; Cassa, C.A.; Mandl, K.D. No Place to Hide--Reverse Identification of Patients from Published Maps. N. Engl. J. Med. 2006, 355, 1741–1742. [Google Scholar] [CrossRef] [PubMed]
- Gutmann, M.; Witkowski, K.; Colyer, C.; O’Rourke, J.M.; McNally, J. Providing Spatial Data for Secondary Analysis: Issues and Current Practices Relating to Confidentiality. Popul. Res. Policy Rev. 2008, 27, 639–665. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, J.; Kwan, M.-P.; Levenstein, M.C.; Richardson, D.B. How Do People Perceive the Disclosure Risk of Maps? Examining the Perceived Disclosure Risk of Maps and Its Implications for Geoprivacy Protection. Cartogr. Geogr. Inf. Sci. 2021, 48, 2–20. [Google Scholar] [CrossRef]
- Kang, J.-Y.; Aldstadt, J.; Vandewalle, R.; Yin, D.; Wang, S. A CyberGIS Approach to Spatiotemporally Explicit Uncertainty and Global Sensitivity Analysis for Agent-Based Modeling of Vector-Borne Disease Transmission. Ann. Am. Assoc. Geogr. 2020, 110, 1855–1873. [Google Scholar] [CrossRef]
- Kamel Boulos, M.N.; Peng, G.; VoPham, T. An Overview of GeoAI Applications in Health and Healthcare. Int. J. Health Geogr. 2019, 18, 7. [Google Scholar] [CrossRef] [PubMed]
- Eby, L.T.; Dobbins, G.H. Collectivistic Orientation in Teams: An Individual and Group-Level Analysis. J. Organ. Behav. 1997, 18, 275–295. [Google Scholar] [CrossRef]
- Han, S.-P.; Shavitt, S. Persuasion and Culture: Advertising Appeals in Individualistic and Collectivistic Societies. J. Exp. Soc. Psychol. 1994, 30, 326–350. [Google Scholar] [CrossRef]
- Park, S.; Choi, G.J.; Ko, H. Information Technology-Based Tracing Strategy in Response to COVID-19 in South Korea-Privacy Controversies. JAMA 2020, 323, 2129–2130. [Google Scholar] [CrossRef] [Green Version]
- Sonn, J.W.; Lee, J.K. The Smart City as Time-Space Cartographer in COVID-19 Control: The South Korean Strategy and Democratic Control of Surveillance Technology. Eurasian Geogr. Econ. 2020, 1–11. [Google Scholar] [CrossRef]
- Coronavirus Pandemic (COVID-19). Available online: https://ourworldindata.org/coronavirus-data (accessed on 19 December 2020).
- Babbie, E. The Practice of Social Research, 12th ed.; Wadsworth Publishing: Belmont, CA, USA, 2010. [Google Scholar]
- Forgasz, H.; Tan, H.; Leder, G.; McLeod, A. Enhancing Survey Participation: Facebook Advertisements for Recruitment in Educational Research. Int. J. Res. Method Educ. 2018, 41, 257–270. [Google Scholar] [CrossRef]
- Privitera, G.J. Statistics for the Behavioral Sciences, 3rd ed.; SAGE Publications: Thousand Oaks, CA, USA, 2017. [Google Scholar]
- Triandis, H.C.; Gelfand, M.J. Converging Measurement of Horizontal and Vertical Individualism and Collectivism. J. Pers. Soc. Psychol. 1998, 74, 118–128. [Google Scholar] [CrossRef]
- Simmons-Duffin, S. As States Reopen, Do They Have the Workforce They Need to Stop Coronavirus Outbreaks? NPR: Washington, DC, USA, 2020. [Google Scholar]
- Timberg, C.; Harwell, D. Most Americans Are Not Willing or Able to Use an App Tracking Coronavirus Infections. That’s a Problem for Big Tech’s Plan to Slow the Pandemic; Washington Post: Washington, DC, USA, 2020. [Google Scholar]
- Servick, K. COVID-19 Contact Tracing Apps Are Coming to a Phone near You. How Will We Know Whether They Work? Science 2020. [Google Scholar] [CrossRef]
- Safer Illinois App. Available online: https://covid19.illinois.edu/health-and-support/safer-illinois-app/ (accessed on 19 December 2020).
- Public Survey Results. Available online: https://www.4th-ir.go.kr/pressRelease/detail/1131?category=report (accessed on 14 November 2020). (In Korean).
- Li, Y. Theories in Online Information Privacy Research: A Critical Review and an Integrated Framework. Decis. Support Syst. 2012, 54, 471–481. [Google Scholar] [CrossRef]
- Zhao, L.; Lu, Y.; Gupta, S. Disclosure Intention of Location-Related Information in Location-Based Social Network Services. Int. J. Electron. Commer. 2012, 16, 53–90. [Google Scholar] [CrossRef]
- Bellman, S.; Johnson, E.J.; Kobrin, S.J.; Lohse, G.L. International Differences in Information Privacy Concerns: A Global Survey of Consumers. Inf. Soc. 2004, 20, 313–324. [Google Scholar] [CrossRef]
- Cho, H.; Rivera-Sánchez, M.; Lim, S.S. A Multinational Study on Online Privacy: Global Concerns and Local Responses. New Media Soc. 2009, 11, 395–416. [Google Scholar]
- Milberg, S.J.; Smith, H.J.; Burke, S.J. Information Privacy: Corporate Management and National Regulation. Organ. Sci. 2000, 11, 35–57. [Google Scholar] [CrossRef]
- American Association of Geographers. Ethical Research in the Age of COVID-19: A Participatory Forum. Available online: http://news.aag.org/2020/11/ethical-research-in-the-age-of-covid-19-a-participatory-forum/ (accessed on 19 December 2020).
- American Association of Geographers. Summer Series on Questions of Geoethics and Human Rights highlighted by COVID-19 Conditions. Available online: http://news.aag.org/2020/06/summer-series-on-questions-of-geo-ethics-and-human-rights-highlighted-by-covid-19-conditions/ (accessed on 19 December 2020).
- American Geographical Society. EthicalGEO–Exploring the Ethics of Geospatial Data and Technology. Available online: https://ethicalgeo.org/ (accessed on 19 December 2020).
- Liang, H.; Shen, F.; Fu, K.-W. Privacy Protection and Self-Disclosure across Societies: A Study of Global Twitter Users. New Media Soc. 2017, 19, 1476–1497. [Google Scholar] [CrossRef]
- Trepte, S.; Reinecke, L.; Ellison, N.B.; Quiring, O.; Yao, M.Z.; Ziegele, M. A Cross-Cultural Perspective on the Privacy Calculus. Soc. Media Soc. 2017, 3, 205630511668803. [Google Scholar] [CrossRef] [Green Version]
- Bansal, G.; Zahedi, F. “mariam”; Gefen, D. The Impact of Personal Dispositions on Information Sensitivity, Privacy Concern and Trust in Disclosing Health Information Online. Decis. Support Syst. 2010, 49, 138–150. [Google Scholar] [CrossRef]
- Maiorana, A.; Steward, W.T.; Koester, K.A.; Pearson, C.; Shade, S.B.; Chakravarty, D.; Myers, J.J. Trust, Confidentiality, and the Acceptability of Sharing HIV-Related Patient Data: Lessons Learned from a Mixed Methods Study about Health Information Exchanges. Implement. Sci. 2012, 7, 34. [Google Scholar] [CrossRef] [PubMed] [Green Version]




| U.S. | South Korea | ||||
|---|---|---|---|---|---|
| Sample (n = 188) | National Population 1 | Sample (n = 118) | National Population 2 | ||
| Gender | Female | 70% | 51% | 42% | 50% |
| Age | 18–24 | 26% | 12% | 30% | 14% |
| 25–44 | 57% | 34% | 49% | 33% | |
| 45+ | 17% | 53% | 19% | 53% | |
| Race | White alone | 55% | 74% | N/A 3 | N/A 3 |
| Higher Education | 88% | 32% 4 | 73% | 33% 4 | |
| Student | 31% | N/A | 41% | N/A | |
| Method | Type | Description | Execution | |
|---|---|---|---|---|
| U.S. | South Korea | |||
| M1 | Contact Tracing | Obtaining location information by conducting conventional interviews | O | O |
| M2 | Obtaining location information from patients’ mobile phones (e.g., GPS trajectories) | △ | O | |
| M3 | Obtaining location information from patients’ credit card history | X | O | |
| M4 | Bluetooth-based proximity tracing method | △ | X | |
| M5 | Self-Quarantine Monitoring | Monitoring people’s self-quarantine by calling them at random times of day | △ | O |
| M6 | Monitoring people’s self-quarantine by obtaining their real-time locations from their mobile phones (e.g., signal) | X | O | |
| M7 | Monitoring people’s self-quarantine by requiring them to wear an e-wristband that reported their real-time locations to public health officers | X | ☐ | |
| M8 | People were required to carry a valid travel certificate (i.e., not in self-quarantine) when using public places | X | X | |
| M9 | Location Disclosure | Publicly disclosing the locations of major activities of COVID-19 patients with their ages and genders | X | O |
| M10 | Publicly disclosing the locations of major activities of COVID-19 patients (not disclosing age and gender) | X | O | |
| Methods | U.S. | South Korea | ||||
|---|---|---|---|---|---|---|
| Privacy Concerns | Perceived Social Benefits | Acceptance | Privacy Concerns | Perceived Social Benefits | Acceptance | |
| M1 | 3.1 (1.9) | 5.7 (1.7) | 5.6 (1.6) | 3.6 (1.9) | 5.7 (1.3) | 5.7 (1.3) |
| M2 | 4.5 (2.0) | 5.1 (1.9) | 4.2 (2.0) | 4.2 (1.9) | 5.8 (1.4) | 5.5 (1.4) |
| M3 | 5.0 (2.0) | 4.1 (2.0) | 3.5 (2.1) | 4.0 (2.0) | 5.5 (1.4) | 5.6 (1.4) |
| M4 | 4.3 (2.1) | 5.2 (1.8) | 4.3 (2.0) | 3.9 (1.9) | 5.8 (1.2) | 5.5 (1.5) |
| Methods | Privacy Concerns | Perceived Social Benefits | Acceptance | |||
|---|---|---|---|---|---|---|
| p-Value | |r| | p-Value | |r| | p-Value | |r| | |
| M1 | 0.007 ** | 0.155 | 0.077 | 0.101 | 0.944 | 0.004 |
| M2 | 0.188 | 0.076 | 0.006 ** | 0.158 | 0.000 *** | 0.314 |
| M3 | 0.000 *** | 0.242 | 0.000 *** | 0.340 | 0.000 *** | 0.476 |
| M4 | 0.123 | 0.088 | 0.031 * | 0.123 | 0.000 *** | 0.294 |
| Methods | U.S. | South Korea | ||
|---|---|---|---|---|
| Acceptance | Disapproval | Acceptance | Disapproval | |
| M1 | 79% | 10% | 82% | 6% |
| M2 | 48% | 39% | 78% | 10% |
| M3 | 33% | 56% | 81% | 8% |
| M4 | 53% | 31% | 75% | 9% |
| Methods | U.S. | South Korea | ||||
|---|---|---|---|---|---|---|
| Privacy Concerns | Perceived Social Benefits | Acceptance | Privacy Concerns | Perceived Social Benefits | Acceptance | |
| M5 | 3.7 (2.1) | 4.7 (2.0) | 4.6 (2.1) | 3.4 (1.9) | 5.4 (1.5) | 5.8 (1.4) |
| M6 | 5.1 (1.9) | 4.5 (2.0) | 3.5 (2.1) | 4.0 (2.0) | 5.9 (1.3) | 5.6 (1.6) |
| M7 | 5.1 (2.0) | 4.4 (2.1) | 3.2 (2.0) | 4.4 (2.1) | 5.9 (1.2) | 4.8 (1.9) |
| M8 | 4.0 (2.2) | 4.7 (2.0) | 4.2 (2.1) | 3.5 (1.9) | 5.3 (1.5) | 5.0 (1.7) |
| Methods | Privacy Concerns | Perceived Social Benefits | Acceptance | |||
|---|---|---|---|---|---|---|
| p-Value | |r| | p-Value | |r| | p-Value | |r| | |
| M5 | 0.280 | 0.062 | 0.005 ** | 0.159 | 0.000 *** | 0.285 |
| M6 | 0.000 *** | 0.270 | 0.000 *** | 0.333 | 0.000 *** | 0.472 |
| M7 | 0.002 ** | 0.181 | 0.000 *** | 0.350 | 0.000 *** | 0.377 |
| M8 | 0.036 * | 0.120 | 0.030 * | 0.125 | 0.001 ** | 0.194 |
| Methods | U.S. | South Korea | ||
|---|---|---|---|---|
| Acceptance | Disapproval | Acceptance | Disapproval | |
| M5 | 55% | 27% | 81% | 10% |
| M6 | 34% | 53% | 80% | 15% |
| M7 | 30% | 59% | 58% | 28% |
| M8 | 47% | 36% | 60% | 16% |
| Methods | U.S. | South Korea | ||||
|---|---|---|---|---|---|---|
| Privacy Concerns | Perceived Social Benefits | Acceptance | Privacy Concerns | Perceived Social Benefits | Acceptance | |
| M9 | 5.1 (1.8) | 4.6 (1.9) | 3.6 (2.0) | 4.9 (1.9) | 5.3 (1.5) | 4.7 (1.8) |
| M10 | 4.0 (1.9) | 5.1 (1.8) | 4.6 (1.9) | 3.9 (1.9) | 5.5 (1.2) | 5.6 (1.4) |
| Methods | Privacy Concerns | Perceived Social Benefits | Acceptance | |||
|---|---|---|---|---|---|---|
| p-Value | |r| | p-Value | |r| | p-Value | |r| | |
| M9 | 0.384 | 0.050 | 0.004 ** | 0.163 | 0.000 *** | 0.264 |
| M10 | 0.693 | 0.023 | 0.167 | 0.079 | 0.000 *** | 0.235 |
| Methods | U.S. | South Korea | ||
|---|---|---|---|---|
| Acceptance | Disapproval | Acceptance | Disapproval | |
| M9 | 36% | 47% | 59% | 28% |
| M10 | 59% | 28% | 79% | 9% |
| Variables | Coefficient | |
|---|---|---|
| Female | 0.149 (0.116) | |
| Age | Age1 (18–24) | −0.032 (0.145) |
| Age2 (45+) | 0.122 (0.154) | |
| Employment Status | Student | 0.017 (0.226) |
| Employed | −0.048 (0.217) | |
| High education | 0.189 (0.154) | |
| USA | −1.043 *** (0.123) | |
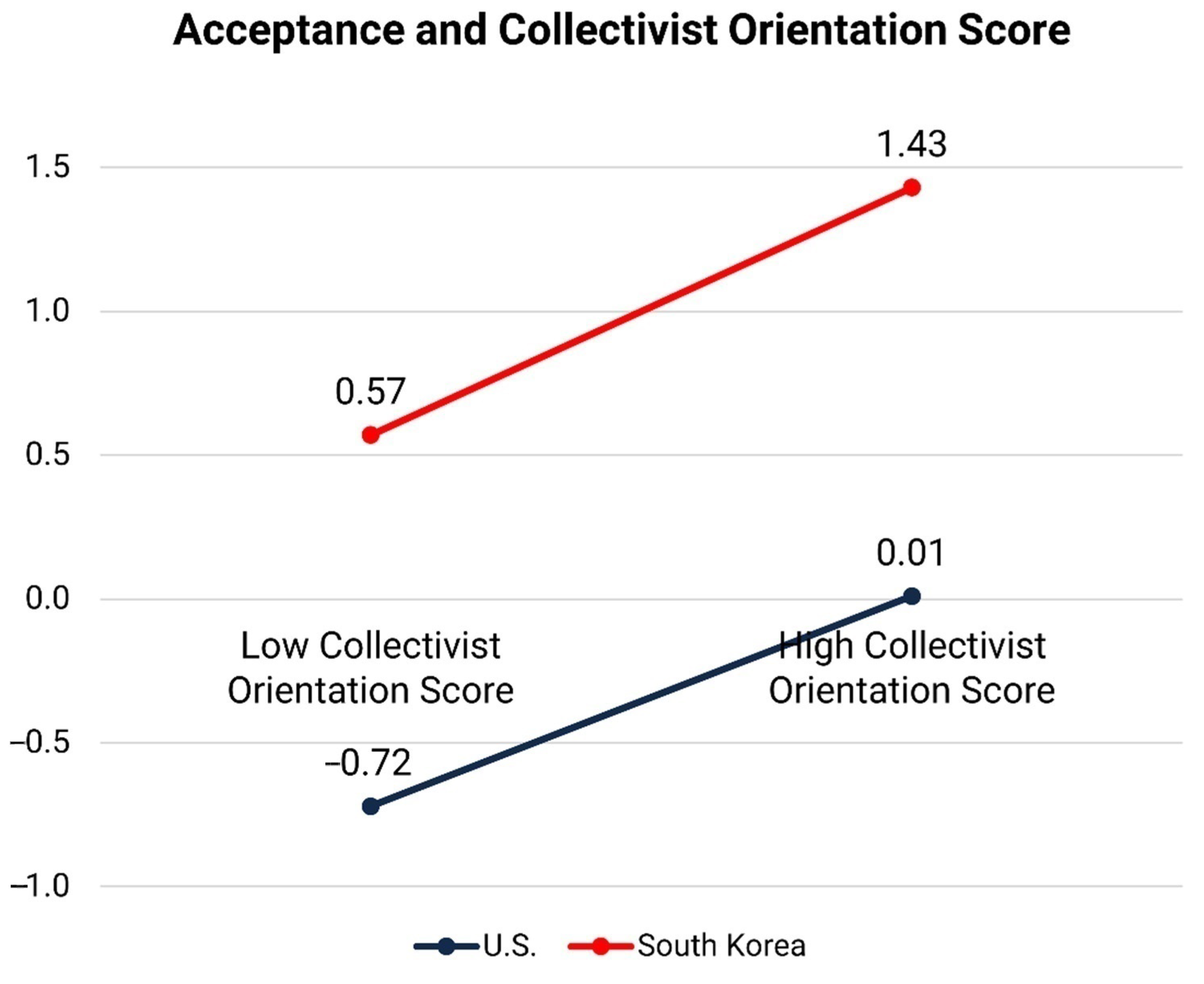
| Collectivist orientation score | 0.177 ** (0.059) | |
| Intercept | 0.399 (0.274) | |
| R2 | 0.225 | |
| 0.202 | ||
| Cohen’s f2 | 0.290 | |
| Variables | Model 3 (Privacy Concerns) | Model 4 (Perceived Social Benefits) | |
|---|---|---|---|
| Female | 0.162 (0.128) | 0.113 (0.123) | |
| Age | Age1 (18–24) | −0.093 (0.161) | 0.115 (0.154) |
| Age2 (45+) | −0.156 (0.171) | 0.071 (0.164) | |
| Employment Status | Student | −0.001 (0.250) | 0.073 (0.240) |
| Employed | 0.163 (0.241) | 0.111 (0.231) | |
| Higher education | −0.281 (0.170) | 0.413 * (0.163) | |
| USA | 0.302 * (0.136) | −0.749 *** (0.130) | |
| Collectivist orientation score | −0.129 * (0.065) | 0.138 * (0.063) | |
| Intercept | −0.087 (0.304) | −0.085 (0.291) | |
| R2 | 0.052 | 0.132 | |
| 0.024 | 0.106 | ||
| Cohen’s f2 | 0.055 | 0.152 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, J.; Kwan, M.-P. An Examination of People’s Privacy Concerns, Perceptions of Social Benefits, and Acceptance of COVID-19 Mitigation Measures That Harness Location Information: A Comparative Study of the U.S. and South Korea. ISPRS Int. J. Geo-Inf. 2021, 10, 25. https://0-doi-org.brum.beds.ac.uk/10.3390/ijgi10010025
Kim J, Kwan M-P. An Examination of People’s Privacy Concerns, Perceptions of Social Benefits, and Acceptance of COVID-19 Mitigation Measures That Harness Location Information: A Comparative Study of the U.S. and South Korea. ISPRS International Journal of Geo-Information. 2021; 10(1):25. https://0-doi-org.brum.beds.ac.uk/10.3390/ijgi10010025
Chicago/Turabian StyleKim, Junghwan, and Mei-Po Kwan. 2021. "An Examination of People’s Privacy Concerns, Perceptions of Social Benefits, and Acceptance of COVID-19 Mitigation Measures That Harness Location Information: A Comparative Study of the U.S. and South Korea" ISPRS International Journal of Geo-Information 10, no. 1: 25. https://0-doi-org.brum.beds.ac.uk/10.3390/ijgi10010025