
COVID-19 Infection and Mortality: Association with PM2.5 Concentration and Population Density—An Exploratory Study

 , , , ,
, , , ,  , and
, and
Abstract
:1. Introduction
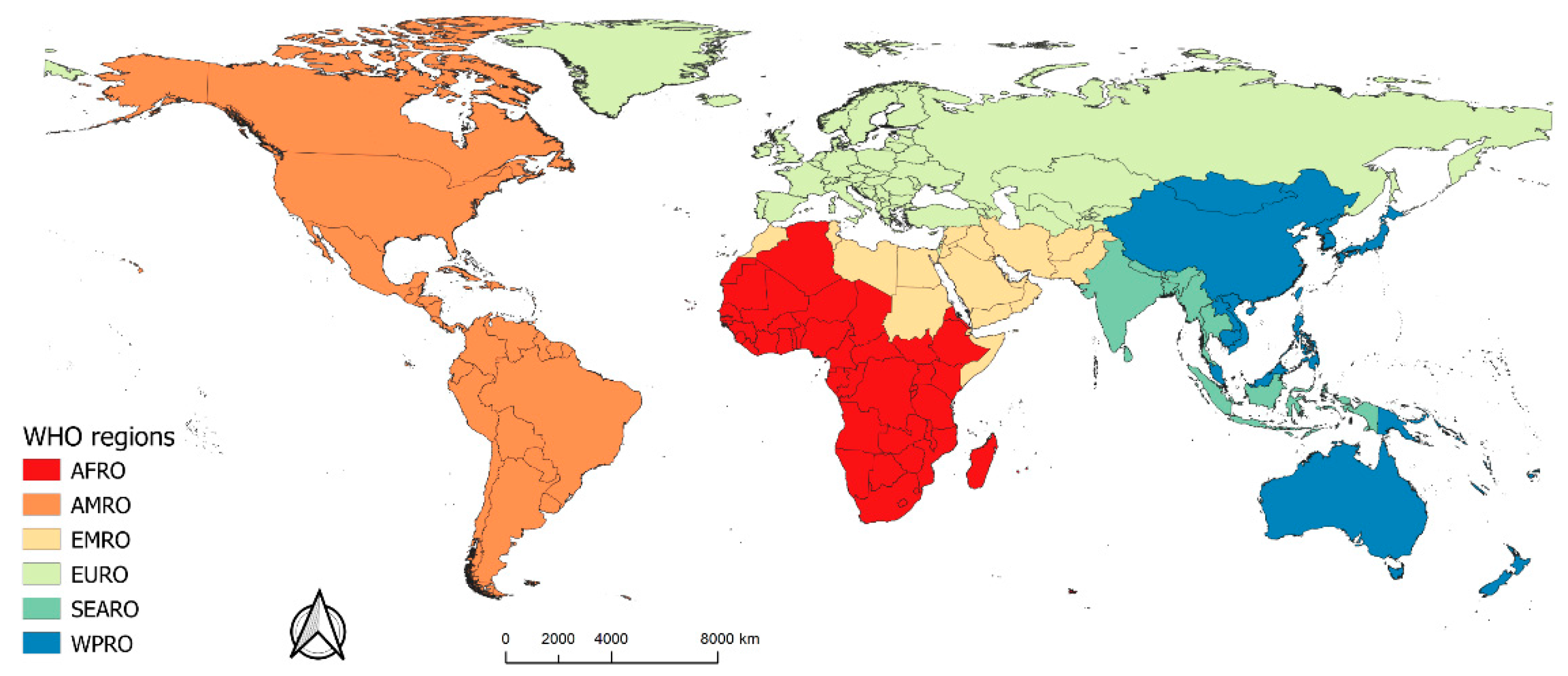
2. Study Area and Data Collection
3. Methodology
3.1. Spearman Rank Correlation
3.2. Multivariate Linear Regression Based on Moran Eigenvector Spatial Filtering for COVID-19
3.3. Geographically Weighted Regression Model
3.4. Bivariate Local Spatial Association
4. Results
4.1. Global Correlation between COVID-19 and Impact Factors
4.2. Relationship between COVID-19 and Both Population Density and PM2.5 Concentrations
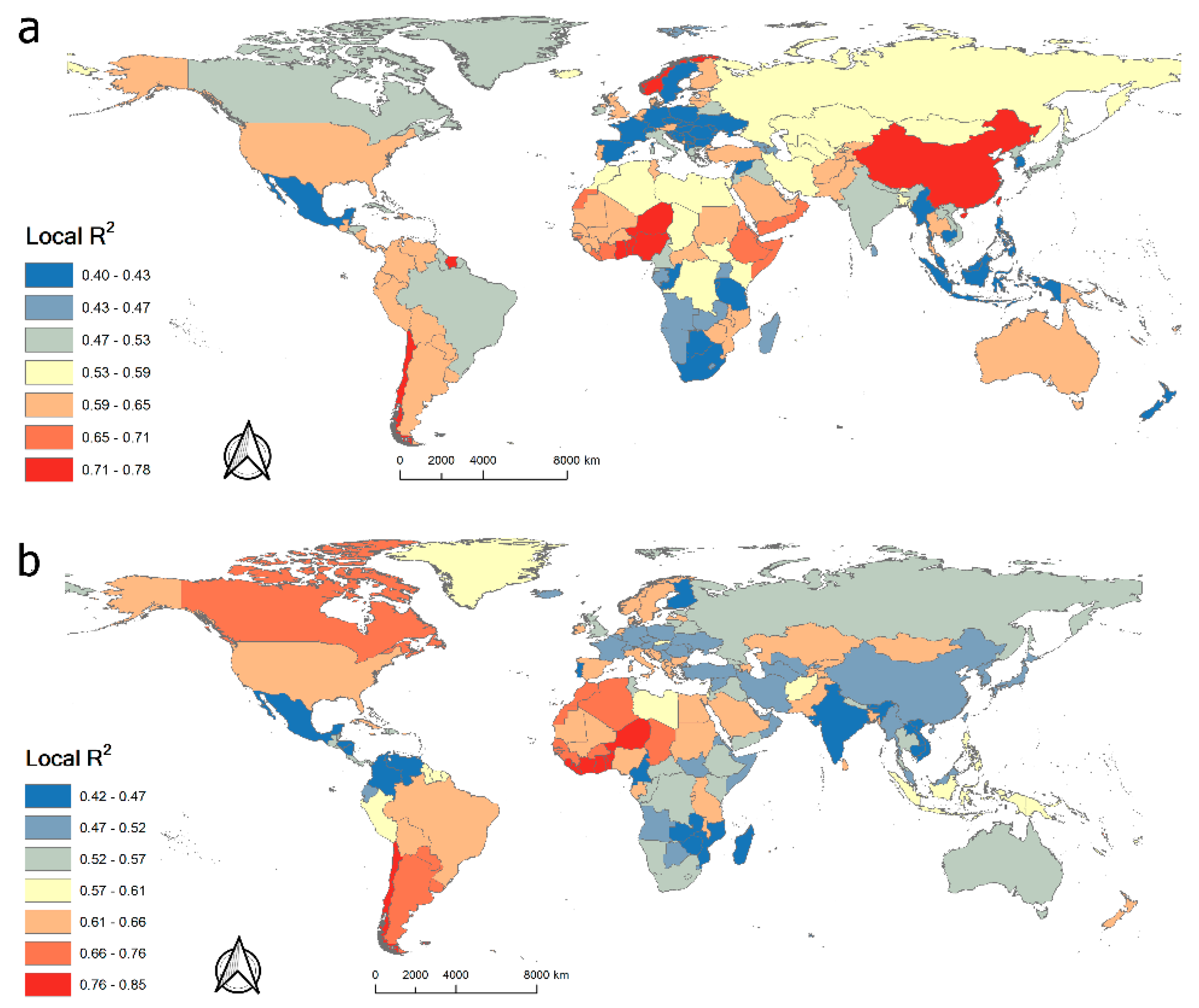
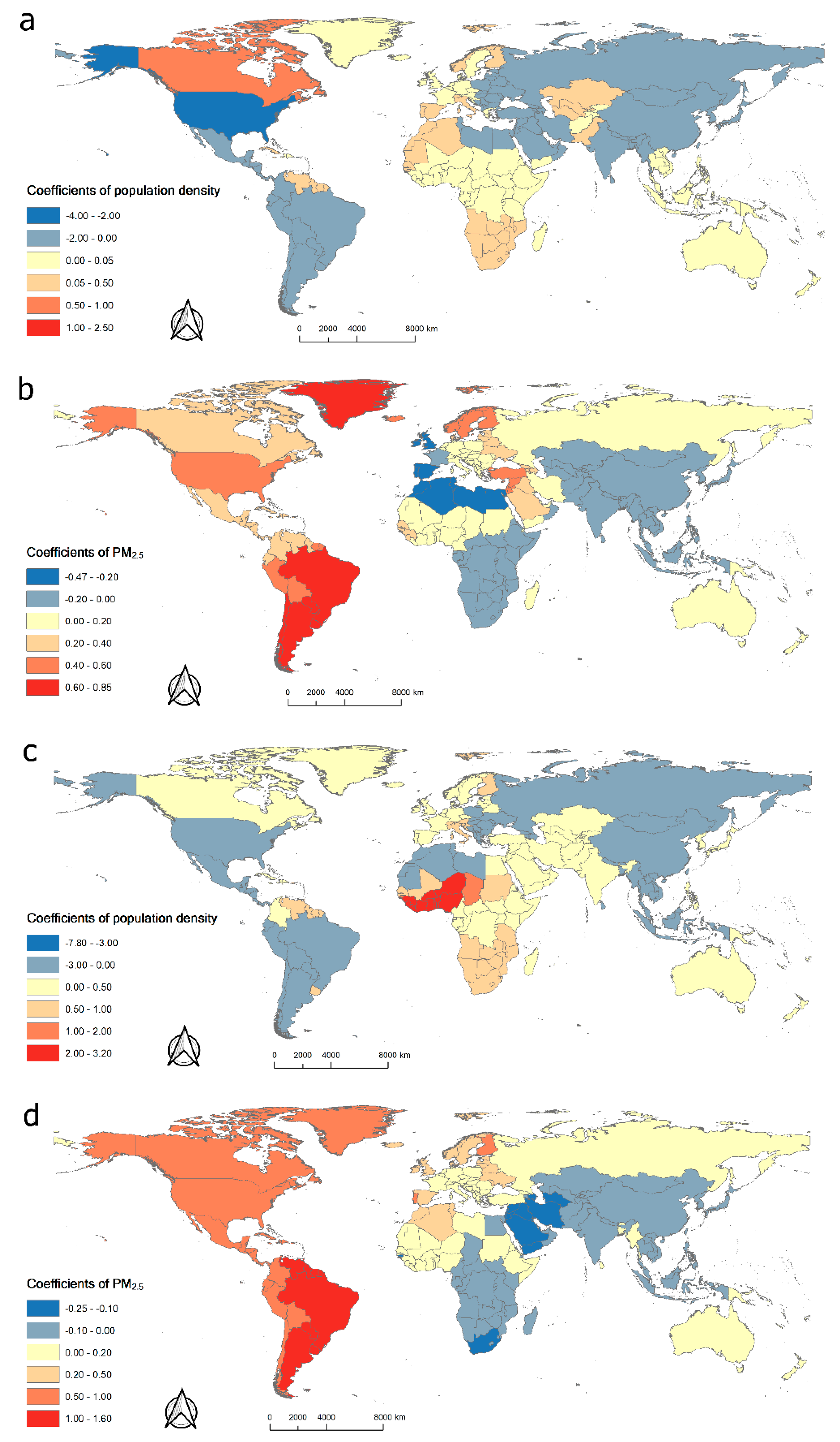
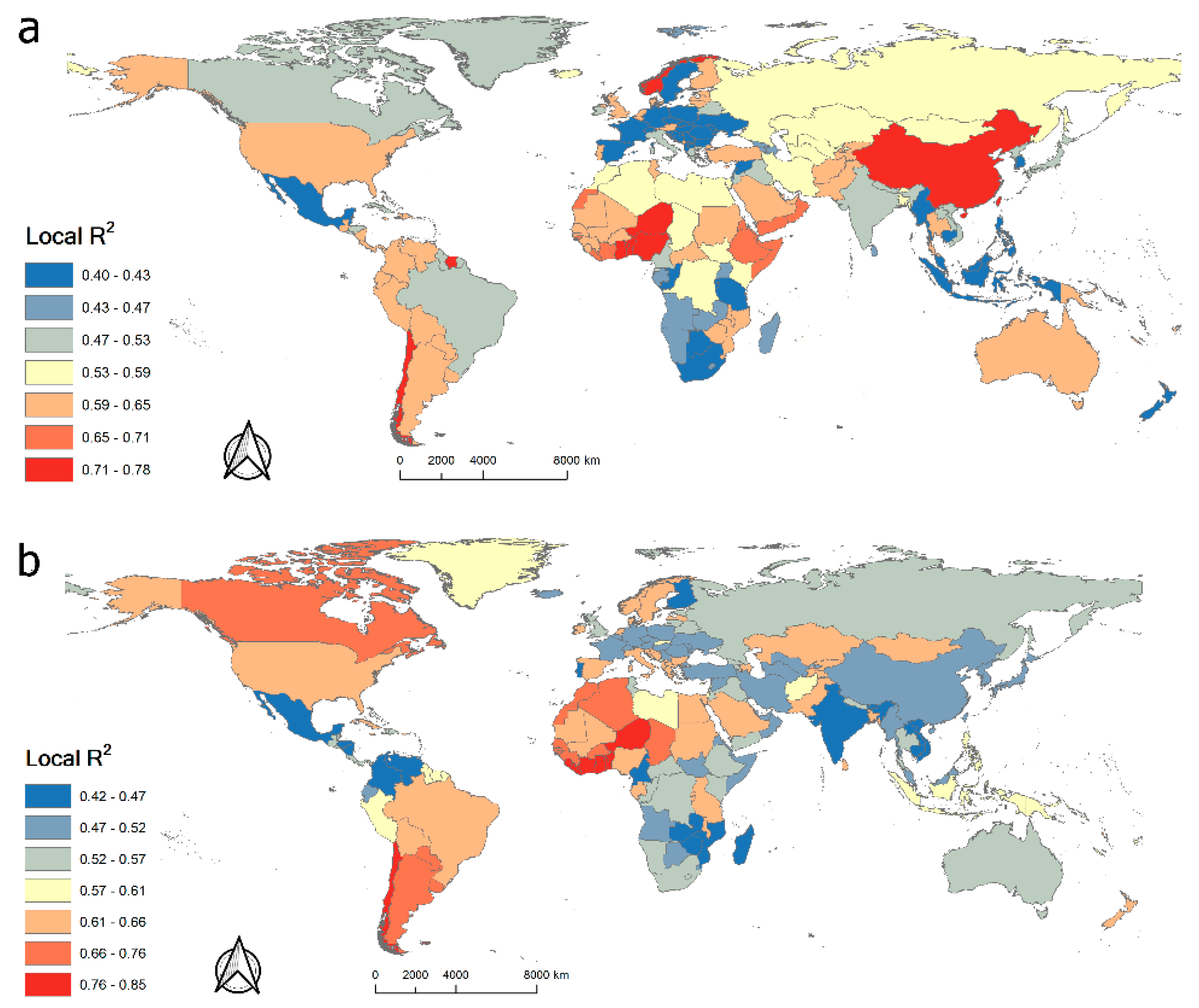
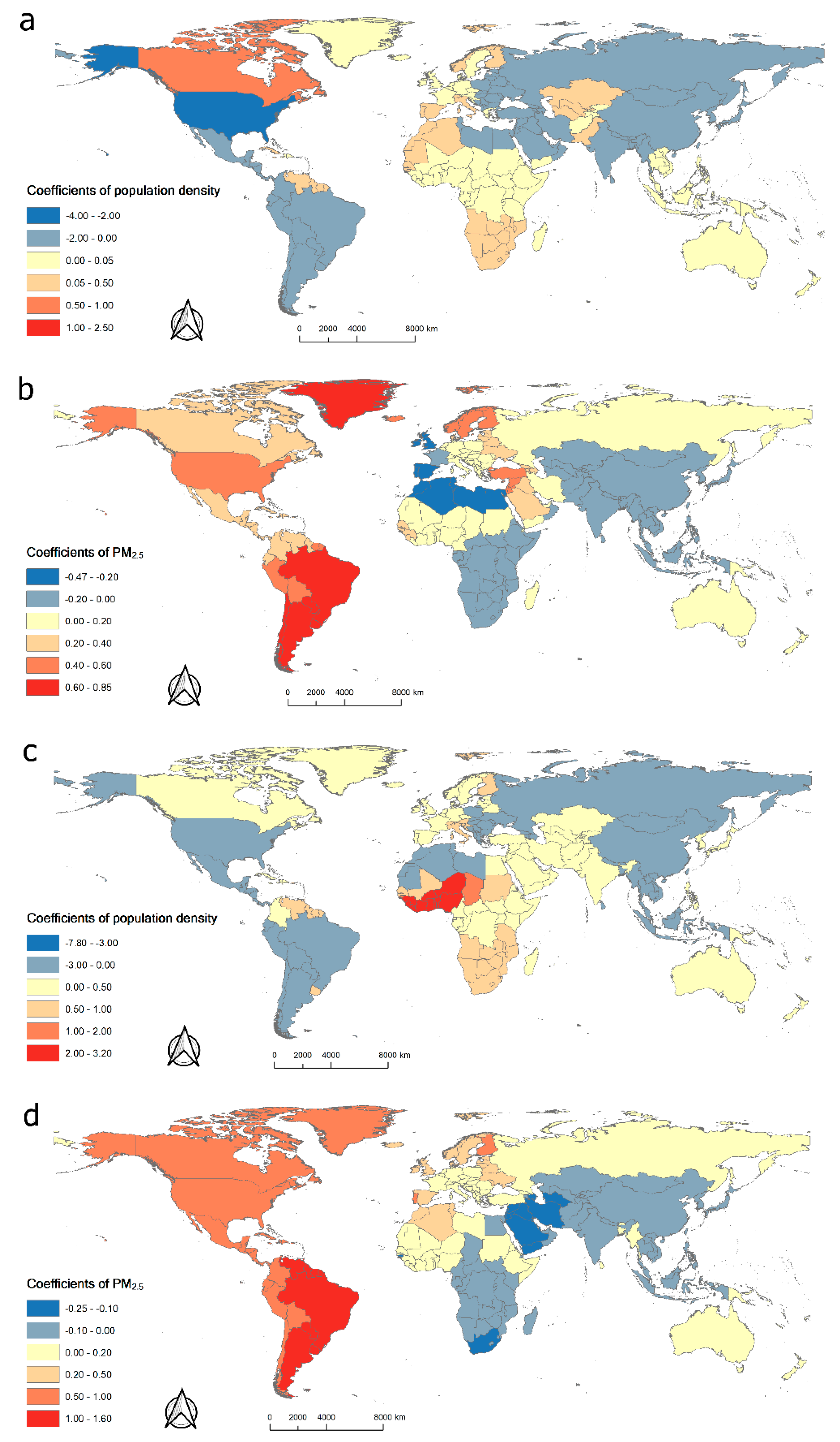
4.3. Spatial Regression Results Based on GWR
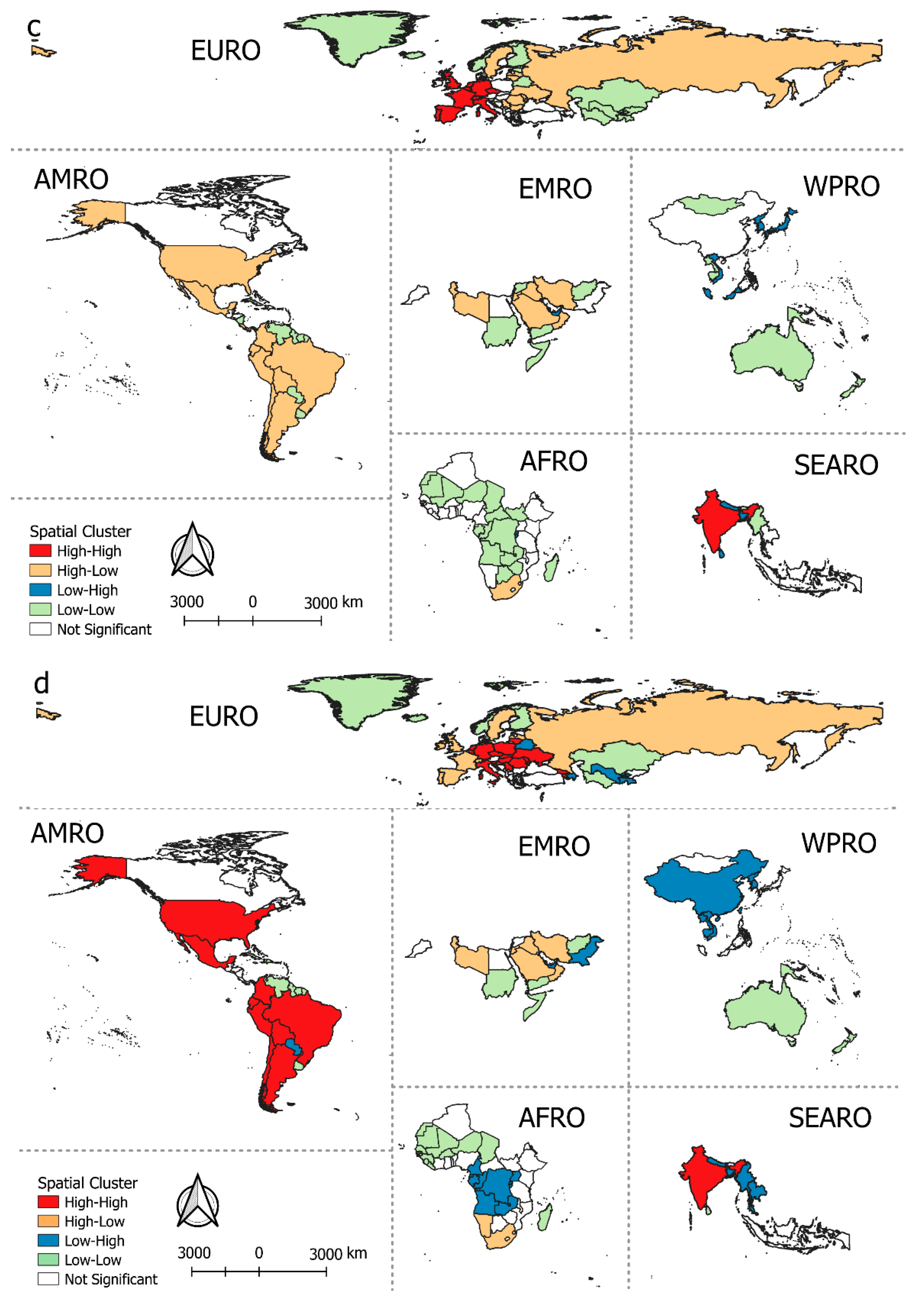
4.4. Bivariate Local Spatial Association Analysis Results
5. Discussion
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Schlagenhauf, P.; Ashra, H. Severe acute respiratory syndrome spreads worldwide. Lancet 2003, 361, 1017. [Google Scholar] [CrossRef] [Green Version]
- Wang, L.; Li, J.; Guo, S.; Xie, N.; Yao, L.; Cao, Y.; Ji, J. Real-time estimation and prediction of mortality caused by COVID-19 with patient information based algorithm. Sci. Total Environ. 2020, 727, 138394. [Google Scholar] [CrossRef] [PubMed]
- Lancet, T. Emerging understandings of 2019-nCoV. Lancet (Lond. Engl.) 2020, 395, 311. [Google Scholar] [CrossRef] [Green Version]
- Li, Q.; Guan, X.; Wu, P.; Wang, X.; Zhou, L.; Tong, Y.; Xing, X. Early transmission dynamics in Wuhan, China, of novel coronavirus–infected pneumonia. N. Engl. J. Med. 2020. [Google Scholar] [CrossRef]
- Chan, J.F.W.; Yuan, S.; Kok, K.H.; To, K.K.W.; Chu, H.; Yang, J.; Tsoi, H.W. A familial cluster of pneumonia associated with the 2019 novel coronavirus indicating person-to-person transmission: A study of a family cluster. Lancet 2020, 395, 514–523. [Google Scholar] [CrossRef] [Green Version]
- Wang, D.; Hu, B.; Hu, C.; Zhu, F.; Liu, X.; Zhang, J.; Zhao, Y. Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus–infected pneumonia in Wuhan, China. JAMA 2020, 323, 1061–1069. [Google Scholar] [CrossRef] [PubMed]
- Novel Coronavirus (2019-nCoV) Situation Report-1 February 2021. Available online: https://www.who.int/publications/m/item/weekly-operational-update-on-covid-19---1-february-2021 (accessed on 1 February 2021).
- Dowd, J.B.; Andriano, L.; Brazel, D.M.; Rotondi, V.; Block, P.; Ding, X.; Mills, M.C. Demographic science aids in understanding the spread and fatality rates of COVID-19. Proc. Natl. Acad. Sci. USA 2020, 117, 9696–9698. [Google Scholar] [CrossRef] [Green Version]
- Dudel, C.; Riffe, T.; Acosta, E.; van Raalte, A.A.; Myrskyla, M. Monitoring trends and differences in COVID-19 case fatality rates using decomposition methods: Contributions of age structure and age-specific fatality. medRxiv 2020. [Google Scholar] [CrossRef]
- Anderson, R.M.; Heesterbeek, H.; Klinkenberg, D.; Hollingsworth, T.D. How will country-based mitigation measures influence the course of the COVID-19 epidemic? Lancet 2020, 395, 931–934. [Google Scholar] [CrossRef]
- Jia, J.S.; Lu, X.; Yuan, Y.; Xu, G.; Jia, J.; Christakis, N.A. Population flow drives spatio-temporal distribution of COVID-19 in China. Nature 2020, 582, 389–394. [Google Scholar] [CrossRef]
- Pope Iii, C.A.; Burnett, R.T.; Thun, M.J.; Calle, E.E.; Krewski, D.; Ito, K.; Thurston, G.D. Lung cancer, cardiopulmonary mortality, and long-term exposure to fine particulate air pollution. JAMA 2020, 287, 1132–1141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Osseiran, N.; Chriscaden, K. Air Pollution Levels Rising in Many of the World’s Poorest Cities; WHO: Geneva, Switherlands, 2016. [Google Scholar]
- Huang, J.B.; Cheng, S.Y.; Wu, K.H.; Cheng, F.J. Association between Particulate Matter Exposure and Short-term Prognosis in Patients with Pneumonia. Aerosol Air Qual. Res. 2020, 20, 89–96. [Google Scholar] [CrossRef]
- Ogen, Y. Assessing nitrogen dioxide (NO2) levels as a contributing factor to the coronavirus (COVID-19) fatality rate. Sci. Total Environ. 2020, 726, 138605. [Google Scholar] [CrossRef] [PubMed]
- Yongjian, Z.; Jingu, X.; Fengming, H.; Liqing, C. Association between short-term exposure to air pollution and COVID-19 infection: Evidence from China. Sci. Total Environ. 2020, 727, 138704. [Google Scholar] [CrossRef]
- Bray, I.; Gibson, A.; White, J. Coronavirus disease 2019 mortality: A multivariate ecological analysis in relation to ethnicity, population density, obesity, deprivation and pollution. Public Health 2020, 185, 261. [Google Scholar] [CrossRef] [PubMed]
- Piazzalunga-Expert, A. Evaluation of the Potential Relationship between Particulate Matter (PM) Pollution and COVID-19 Infection Spread in Italy. Mimeo. 2020. Available online: https://www.ptpz.pl/wp-content/uploads/2020/04/COVID_19_position-paper_ENG1.pdf (accessed on 8 April 2020).
- Yue, H.; Huang, Q.; He, C.; Zhang, X.; Fang, Z. Spatiotemporal patterns of global air pollution: A multi-scale landscape analysis based on dust and sea-salt removed PM2. 5 data. J. Clean. Prod. 2020, 252, 119887. [Google Scholar] [CrossRef]
- Evans, J.; van Donkelaar, A.; Martin, R.V.; Burnett, R.; Rainham, D.G.; Birkett, N.J.; Krewski, D. Estimates of global mortality attributable to particulate air pollution using satellite imagery. Environ. Res. 2013, 120, 33–42. [Google Scholar] [CrossRef]
- Wu, S.; Deng, F.; Hao, Y.; Shima, M.; Wang, X.; Zheng, C.; Qin, Y. Chemical constituents of fine particulate air pollution and pulmonary function in healthy adults: The Healthy Volunteer Natural Relocation study. J. Hazard. Mater. 2013, 260, 183–191. [Google Scholar] [CrossRef]
- Van Donkelaar, A.; Martin, R.V.; Brauer, M.; Hsu, N.C.; Kahn, R.A.; Levy, R.C.; Winker, D.M. Global estimates of fine particulate matter using a combined geophysical-statistical method with information from satellites, models, and monitors. Environ. Sci. Technol. 2016, 50, 3762–3772. [Google Scholar] [CrossRef]
- Bhaduri, B.; Bright, E.; Coleman, P.; Dobson, J. LandScan. Geoinformatics 2002, 5, 34–37. [Google Scholar]
- Wang, J.; Tang, K.; Feng, K.; Lv, W. High Temperature and High Humidity Reduce the Transmission of COVID-19. 2020. SSRN 3551767. Available online: https://ssrn.com/abstract=3551767 (accessed on 9 March 2020). [CrossRef] [Green Version]
- Misumi, I.; Starmer, J.; Uchimura, T.; Beck, M.A.; Magnuson, T.; Whitmire, J.K. Obesity Expands a Distinct Population of T Cells in Adipose Tissue and Increases Vulnerability to Infection. Cell Rep. 2019, 27, 514–524. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stefan, N.; Birkenfeld, A.L.; Schulze, M.B.; Ludwig, D.S. Obesity and impaired metabolic health in patients with COVID-19. Nat. Rev. Endocrinol. 2020, 16, 341–342. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kass, D.A.; Duggal, P.; Cingolani, O. Obesity could shift severe COVID-19 disease to younger ages. Lancet (Lond. Engl.) 2020, 395, 1544–1545. [Google Scholar] [CrossRef]
- Spearman, C. The proof and measurement of association between two things. Apa Psycnet 1961. [Google Scholar] [CrossRef]
- Kabe, D.G. Stepwise multivariate linear regression. J. Am. Stat. Assoc. 1963, 58, 770–773. [Google Scholar] [CrossRef]
- Griffith, D.A. A linear regression solution to the spatial autocorrelation problem. J. Geogr. Syst. 2000, 2, 141–156. [Google Scholar] [CrossRef]
- Griffith, D.; Chun, Y.; Li, B. Spatial Regression Analysis Using Eigenvector Spatial Filtering; Academic Press: Cambridge, MA, USA, 2019. [Google Scholar]
- Griffith, D.A. Spatial Autocorrelation and Spatial Filtering: Gaining Understanding through Theory and Scientific Visualization; Springer Science & Business Media: Berlin/Heidelberg, Germany, 2003. [Google Scholar]
- Landis, R.S. Standardized regression coefficients. Encycl. Stat. Behav. Sci. 2005. [Google Scholar] [CrossRef]
- Brunsdon, C.; Fotheringham, A.S.; Charlton, M.E. Geographically weighted regression: A method for exploring spatial nonstationarity. Geogr. Anal. 1996, 28, 281–298. [Google Scholar] [CrossRef]
- Fotheringham, A.S.; Oshan, T.M. Geographically weighted regression and multicollinearity: Dispelling the myth. J. Geogr. Syst. 2016, 18, 303–329. [Google Scholar] [CrossRef]
- Anselin, L.; Syabri, I.; Smirnov, O. Visualizing multivariate spatial correlation with dynamically linked windows. In Proceedings of the CSISS Workshop on New Tools for Spatial Data Analysis, Santa Barbara, CA, USA, 10–11 May 2002. [Google Scholar]
- Patanavanich, R.; Glantz, S.A. Smoking is associated with COVID-19 progression: A meta-analysis. Nicotine Tob. Res. 2020, 22, 1653–1656. [Google Scholar] [CrossRef] [PubMed]
- Tobler, W.R. A computer movie simulating urban growth in the Detroit region. Econ. Geogr. 1970, 46 (Suppl. 1), 234–240. [Google Scholar] [CrossRef]
- Pérez-Rodríguez, J.V.; Ledesma-Rodríguez, F.; Santana-Gallego, M. Testing dependence between GDP and tourism’s growth rates. Tour. Manag. 2015, 48, 268–282. [Google Scholar] [CrossRef]
- COVID, T.C.; Stephanie, B.; Virginia, B.; Nancy, C.; Aaron, C.; Ryan, G.; Katherine, R. Geographic Differences in COVID-19 Cases, Deaths, and Incidence-United States. 2020. Available online: https://www.cdc.gov/mmwr/volumes/69/wr/pdfs/mm6915e4-H.pdf (accessed on 17 April 2020).
- Wu, X.; Nethery, R.C.; Sabath, B.M.; Braun, D.; Dominici, F. Exposure to air pollution and COVID-19 mortality in the United States. medRxiv 2020. [Google Scholar] [CrossRef] [Green Version]
- Fattorini, D.; Regoli, F. Role of the chronic air pollution levels in the Covid-19 outbreak risk in Italy. Environ. Pollut. 2020, 114732. [Google Scholar] [CrossRef] [PubMed]
- Hsiang, S.; Allen, D.; Annan-Phan, S.; Bell, K.; Bolliger, I.; Chong, T.; Lau, P. The effect of large-scale anti-contagion policies on the COVID-19 pandemic. Nature 2020, 584, 262–267. [Google Scholar] [CrossRef]
- Chen, S.; Yang, J.; Yang, W.; Wang, C.; Bärnighausen, T. COVID-19 control in China during mass population movements at New Year. Lancet 2020, 395, 764–766. [Google Scholar] [CrossRef] [Green Version]
- Cheng, C.; Barceló, J.; Hartnett, A.S.; Kubinec, R.; Messerschmidt, L. COVID-19 Government Response Event Dataset (CoronaNet v. 1.0). Nat. Hum. Behav. 2020, 4, 756–768. [Google Scholar] [CrossRef]
- Marquès, M.; Rovira, J.; Nadal, M.; Domingo, J.L. Effects of air pollution on the potential transmission and mortality of COVID-19: A preliminary case-study in Tarragona Province (Catalonia, Spain). Environ. Res. 2020, 192, 110315. [Google Scholar] [CrossRef]
- Andersen, L.M.; Harden, S.R.; Sugg, M.M.; Runkle, J.D.; Lundquist, T.E. Analyzing the spatial determinants of local Covid-19 transmission in the United States. Sci. Total Environ. 2020, 754, 142396. [Google Scholar] [CrossRef]
- Heroy, S. Metropolitan-scale COVID-19 outbreaks: How similar are they? arXiv 2020, arXiv:2004.01248. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Datasets | Description and Source |
|---|---|
| COVID-19 cases | The country-level number of COVID-19 confirmed cases and deaths per million population until 31st January 2021 from WHO (covering 251 countries and regions) (https://covid19.who.int/, accessed on 8 April 2020) |
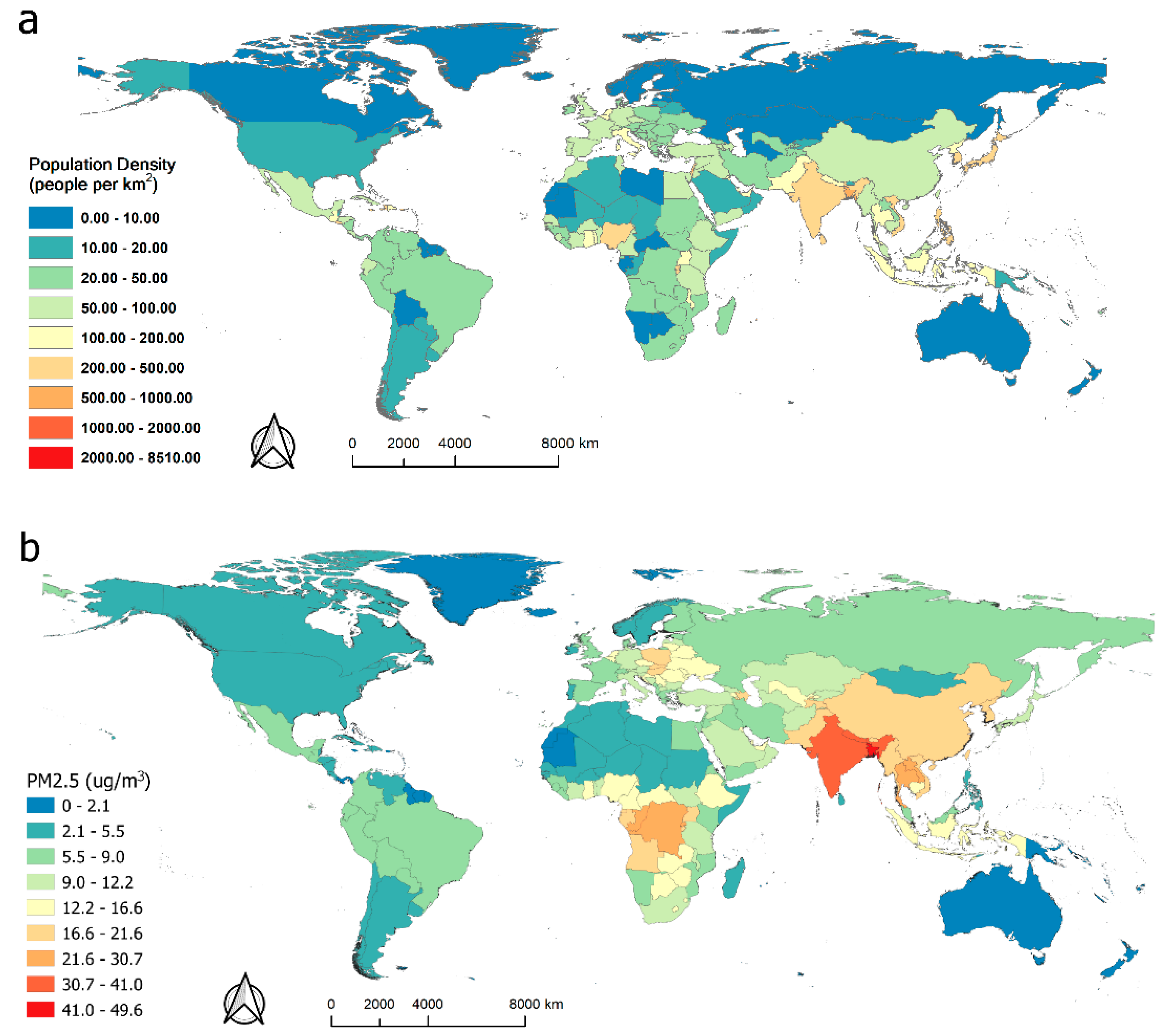
| Population density | The population density dataset was derived from the total population size of each country and region in 2018 collected from LandScan (https://landscan.ornl.gov/landscan-datasets, accessed on 8 April 2020) |
| PM2.5 concentration | The country-level annual average PM2.5 concentration in 2016 collected from Atmospheric Composition Analysis Group (http://fizz.phys.dal.ca/~atmos/martin/?page_id=140, accessed on 8 April 2020) |
| GDP per capita | Current GDP per capita of each country measured in US dollars in 2019 collected from the World Bank (https://data.worldbank.org/indicator/NY.GDP.MKTP.PP.KD, accessed on 8 April 2020) |
| Obesity rate | The prevalence of obesity in adults aged 18 and above in 2016 collected from WHO (https://apps.who.int/gho/data/view.main.REGION2480A?lang=en, accessed on 8 April 2020) |
| Smoking rate | The percentage of people aged 15 and older who currently smoke in 2016 collected from the World Bank (https://data.worldbank.org/indicator/SH.PRV.SMOK, accessed on 8 April 2020) |
| Hospital accommodation | The country-level number of hospital beds per 1000 people in 2015 collected from the World Bank (https://data.worldbank.org/indicator/SH.MED.BEDS.ZS, accessed on 8 April 2020) |
| Confirmed | Deaths | Population | PM2.5 | GDP | Smoking Rate | Hospital Beds | Obesity Rate | |
|---|---|---|---|---|---|---|---|---|
| Confirmed | 1.00 | |||||||
| Deaths | 0.905 ** | 1.00 | ||||||
| Population | 0.544 ** | 0.521 ** | 1.00 | |||||
| PM2.5 | 0.415 ** | 0.419 ** | 0.613 ** | 1.00 | ||||
| GDP | 0.474 ** | 0.445 ** | 0.345 ** | 0.201 ** | 1.00 | |||
| Smoking rate | 0.278 ** | 0.258 ** | 0.032 | 0.132 ** | 0.078 | 1.00 | ||
| Hospital Beds | 0.462 ** | 0.409 ** | −0.030 | 0.142 * | 0.126 * | 0.377 ** | 1.00 | |
| Obesity rate | 0.271 ** | 0.337 ** | 0.322 ** | 0.082 | 0.339 ** | 0.238 ** | 0.241 ** | 1.00 |
| Variable | Cumulative Confirmed (β) | p-Value | Cumulative Deaths (β) | p-Value | VIF |
|---|---|---|---|---|---|
| GDP per capita | 0.150 | <0.001 | 0.133 | <0.001 | 1.215 |
| Smoking rate | 0.021 | 0.001 | 0.018 | 0.004 | 1.402 |
| Hospital beds | −0.102 | 0.002 | −0.062 | 0.001 | 1.760 |
| Obesity rate | 0.077 | 0.021 | 0.064 | 0.046 | 1.511 |
| PM2.5 | 0.013 | 0.048 | 0.022 | 0.036 | 1.325 |
| Population density | 0.018 | 0.046 | 0.017 | 0.047 | 1.476 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yu, X.; Wong, M.S.; Kwan, M.P.; Nichol, J.E.; Zhu, R.; Heo, J.; Chan, P.W.; Chin, D.C.W.; Kwok, C.Y.T.; Kan, Z. COVID-19 Infection and Mortality: Association with PM2.5 Concentration and Population Density—An Exploratory Study. ISPRS Int. J. Geo-Inf. 2021, 10, 123. https://0-doi-org.brum.beds.ac.uk/10.3390/ijgi10030123
Yu X, Wong MS, Kwan MP, Nichol JE, Zhu R, Heo J, Chan PW, Chin DCW, Kwok CYT, Kan Z. COVID-19 Infection and Mortality: Association with PM2.5 Concentration and Population Density—An Exploratory Study. ISPRS International Journal of Geo-Information. 2021; 10(3):123. https://0-doi-org.brum.beds.ac.uk/10.3390/ijgi10030123
Chicago/Turabian StyleYu, Xinyu, Man Sing Wong, Mei Po Kwan, Janet Elizabeth Nichol, Rui Zhu, Joon Heo, Pak Wai Chan, David C. W. Chin, Coco Yin Tung Kwok, and Zihan Kan. 2021. "COVID-19 Infection and Mortality: Association with PM2.5 Concentration and Population Density—An Exploratory Study" ISPRS International Journal of Geo-Information 10, no. 3: 123. https://0-doi-org.brum.beds.ac.uk/10.3390/ijgi10030123