
Spatiotemporal Analysis of COVID-19 Spread with Emerging Hotspot Analysis and Space–Time Cube Models in East Java, Indonesia

 , ,
, ,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
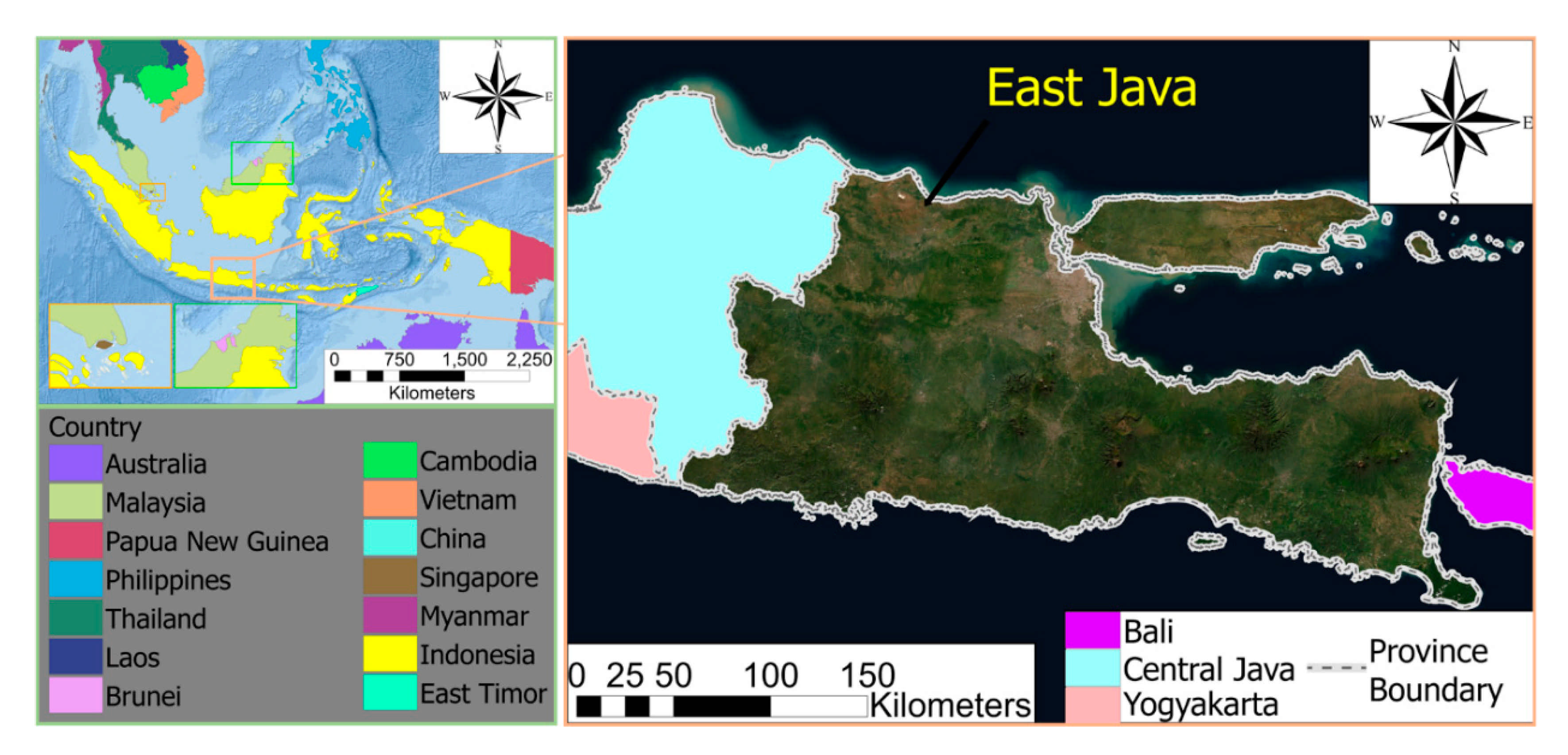
2.1. Study Area
2.2. Data Source
2.3. Analysis Method
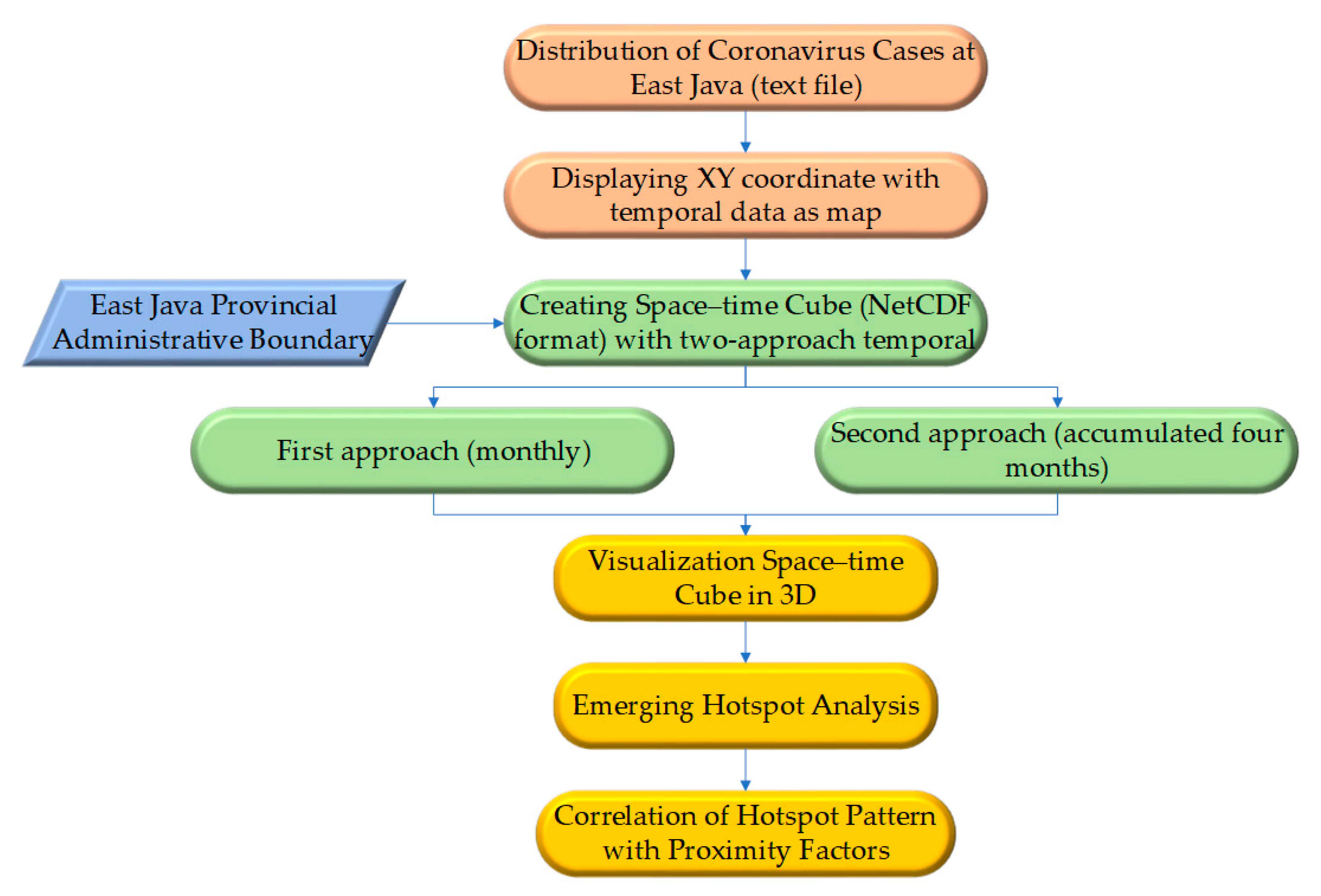
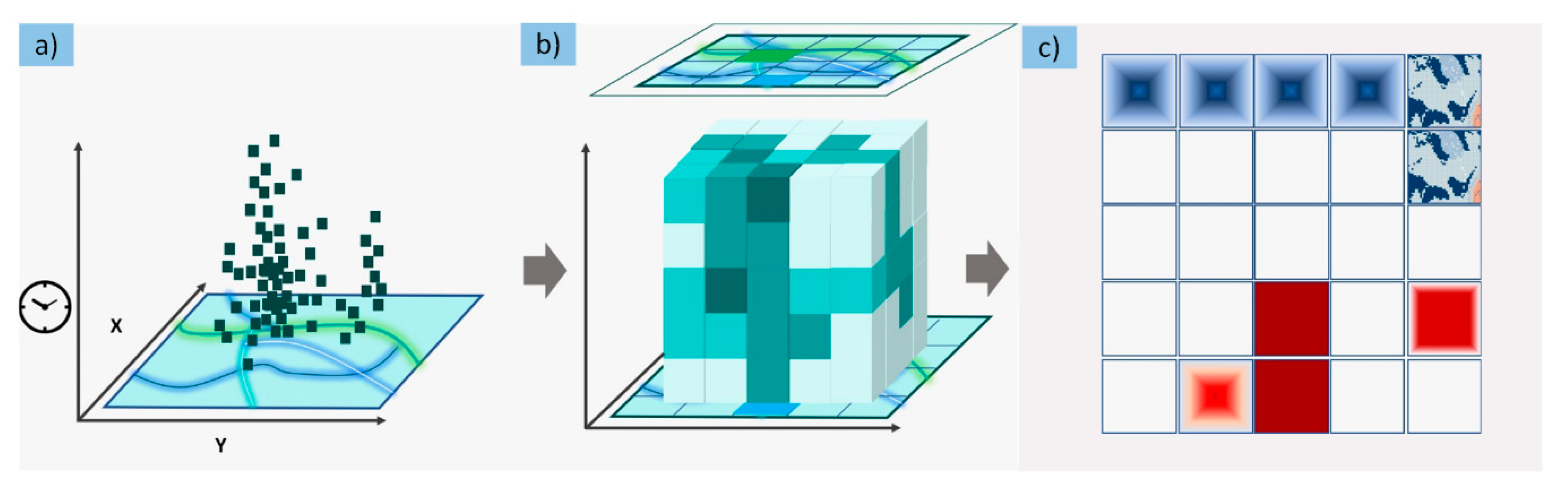
2.3.1. Spatiotemporal Analytics Framework
2.3.2. Emerging Hotspot Analysis
2.3.3. Correlations of Hotspot Patterns with Proximity Factors
3. Results
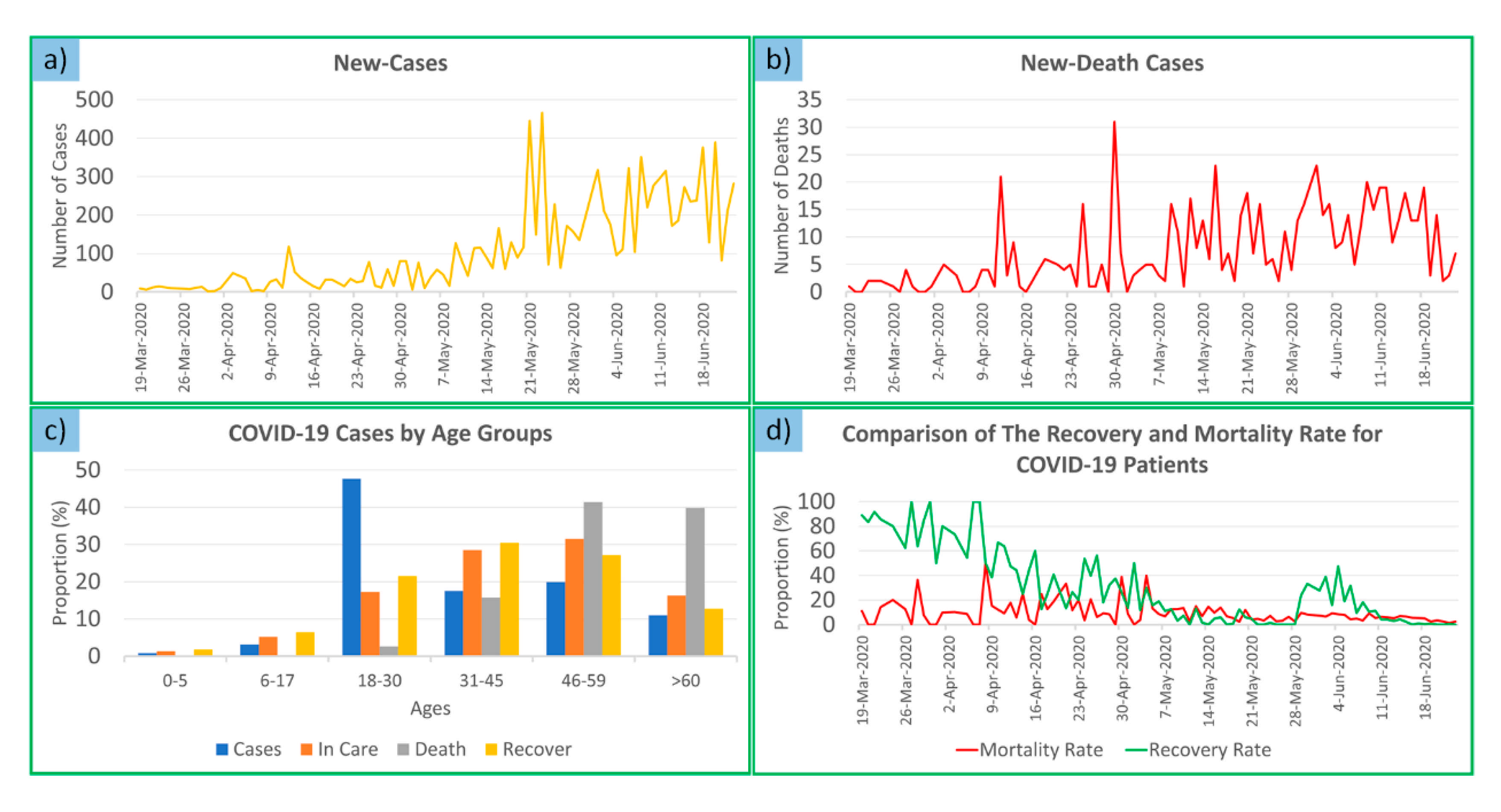
3.1. Analysis of Data on Nonspatial Trends and Demographic Characteristics of the COVID-19 Disease in East Java Province
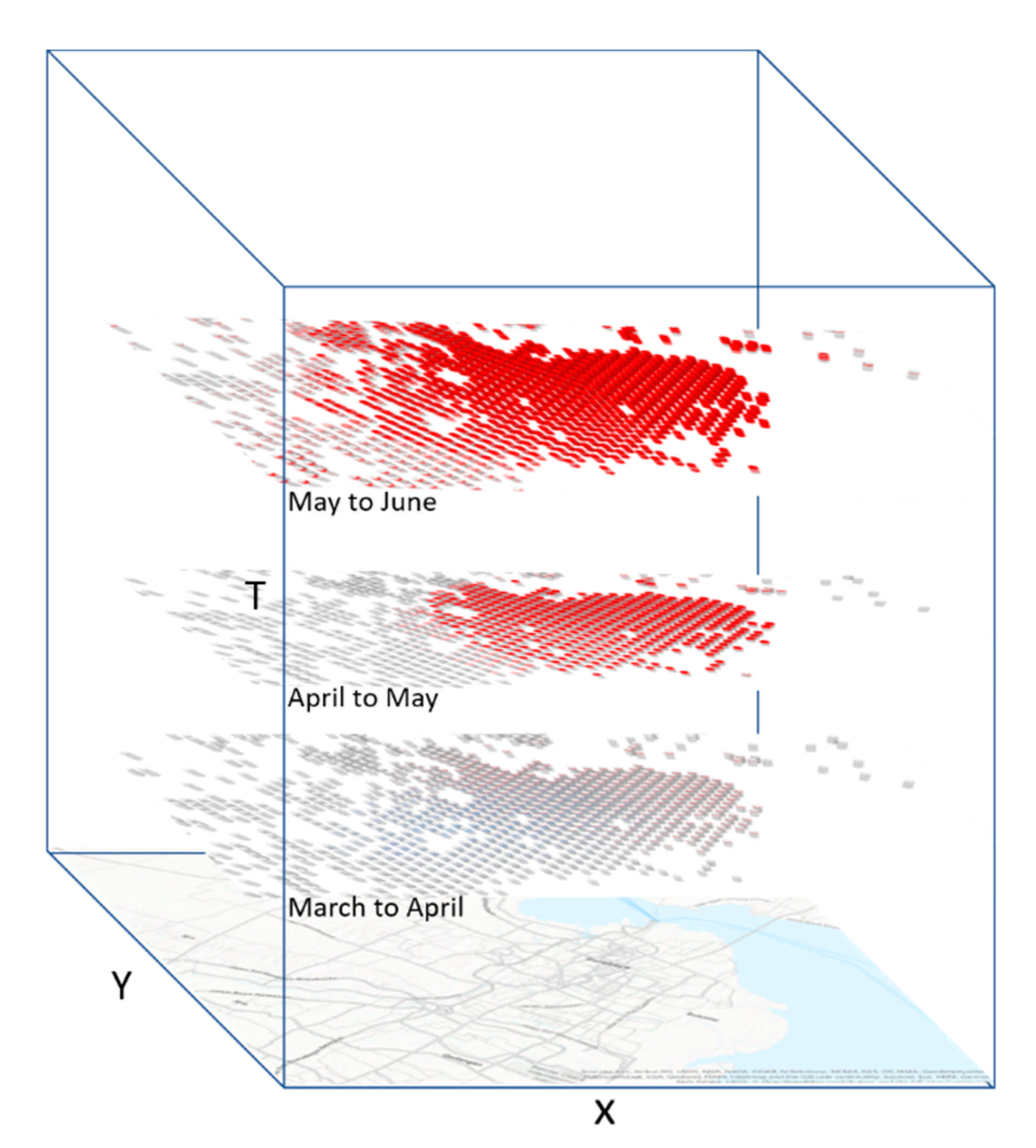
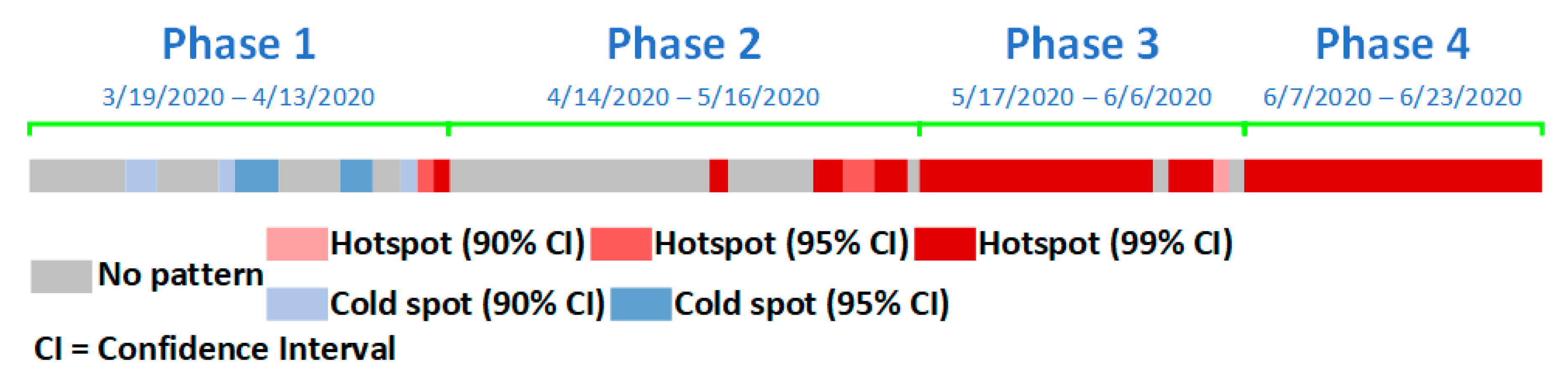
3.2. 3D Visualization of the STC Model for Hotspot Spatiotemporal Trend
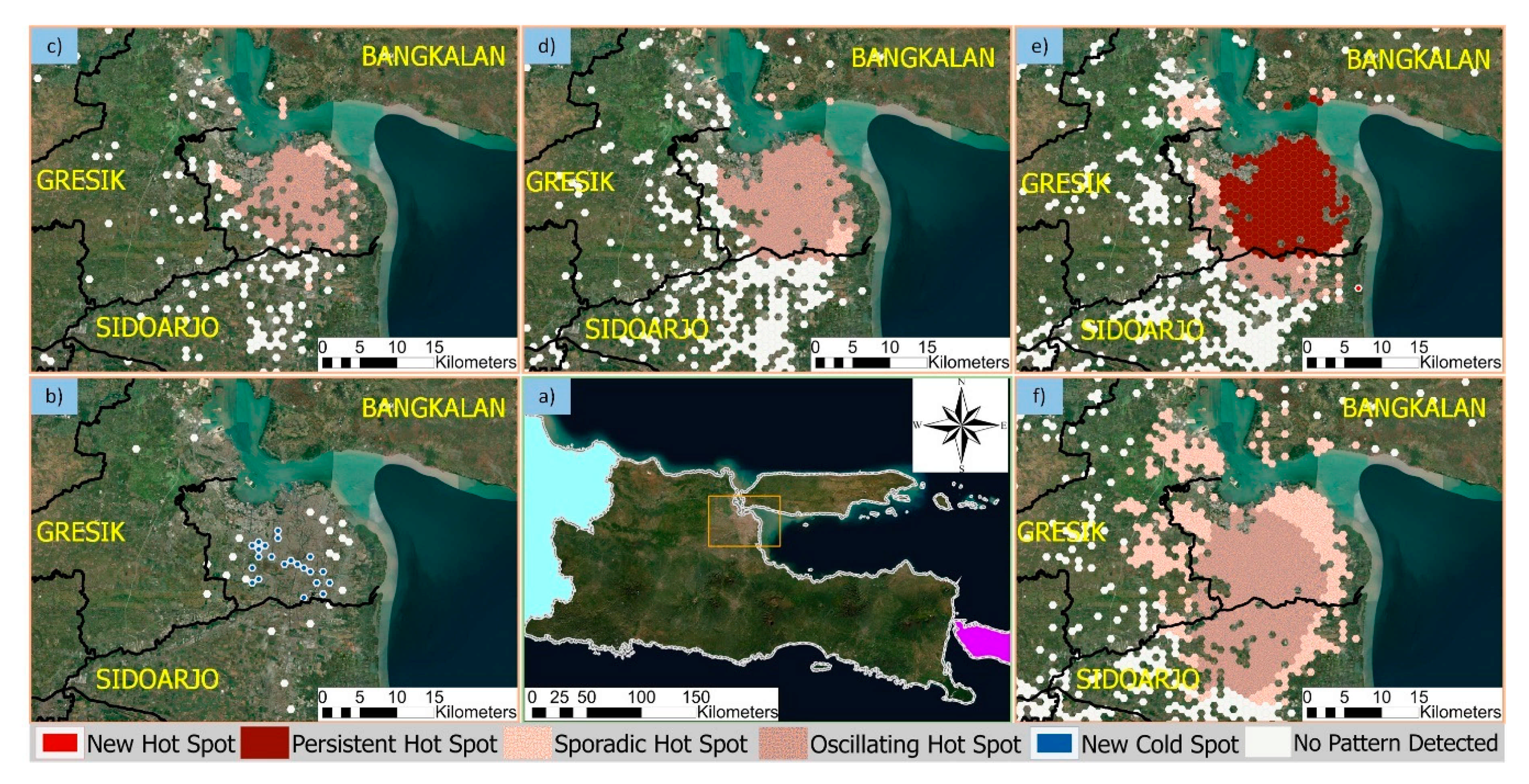
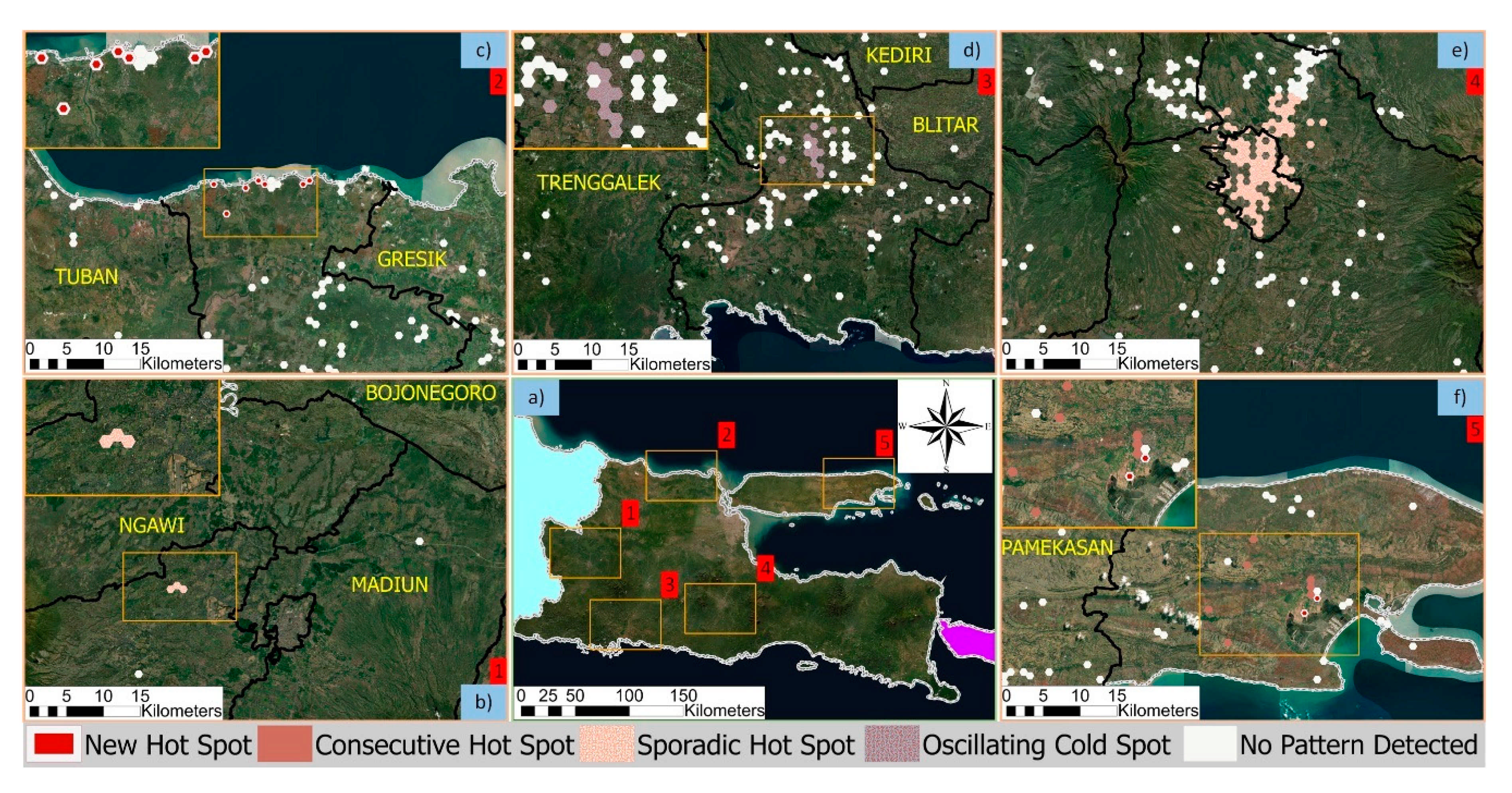
3.3. Emerging Hotspot Analysis (Monthly and Accumulated Four Months)
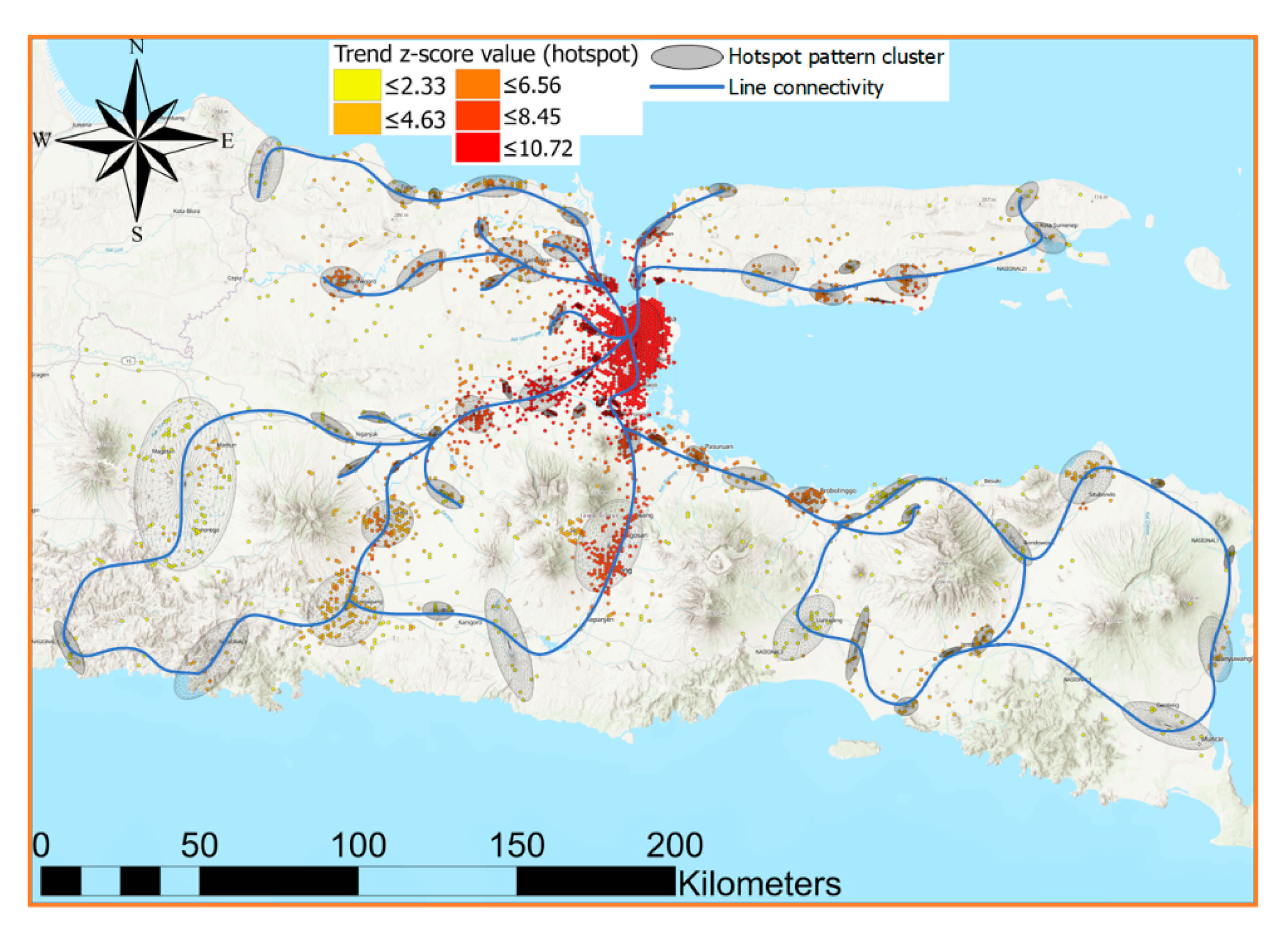
3.4. Correlations of Hotspot Patterns with Proximity Factors
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A



Appendix B
Appendix C

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Pattern | Symbology | Definition |
|---|---|---|
| No Pattern Detected |  | No pattern detected |
| Intensifying Hotspot |  | Locations that become hotspots are statistically significant during 90% of time step intervals, including final time step intervals. The intensity of high clustering amounts in each time step increases overall and is statistically significant. |
| Persistent Hotspot |  | Locations that become hotspots are statistically significant for 90% of time step intervals in the absence of trends indicating an increase or decrease in clustering intensity over time. |
| Oscillating Hotspot |  | A statistically significant hotspot for the last time step interval has a history as a statistically significant cold spot previously. Less than 90% of time step intervals have become statistically significant hotspots. |
| Sporadic Hotspot |  | The location of the hotspot is on-again rather than off-again. Less than 90% of time step intervals become statistically significant hotspots, and no time step interval is a statistically significant cold spot. |
| New Hotspot |  | The location is a statistically significant hotspot for final time step intervals and has never been a statistically significant hotspot before. |
| Diminishing Hotspot |  | Locations that become hotspots are statistically significant during 90% of time step intervals, including final time step intervals. The intensity of the high number of groupings at each time step decreased statistically significantly overall. |
| Historical Hotspot |  | The most recent period is not hot, but at least 90% of time step intervals have become statistically significant hotspots. |
| Consecutive Hotspot |  | Locations with one hotspot path are statistically significant without any interference in final time step intervals. Locations were never statistically significant hotspots before the last hotspot was run, and less than 90% of all bins were statistically significant hotspots. |
| Pattern | Symbology | Definition |
|---|---|---|
| No Pattern Detected |  | No pattern detected |
| Intensifying Cold spot |  | Locations that become cold spots are statistically significant during 90% of time step intervals, including final time step intervals. The intensity of low clustering amounts at each step time increases overall and is statistically significant. |
| Persistent Cold spot |  | Locations that become cold spots are statistically significant during 90% of time step intervals in the absence of trends indicating an increase or decrease in clustering intensity over time. |
| Oscillating Cold spot |  | A statistical cold spot for the last time step interval has a history as a statistically significant hotspot during the previous step time. Less than 90% of time step intervals have become statistically significant cold spots. |
| Sporadic Cold spot |  | Cold spot location is on-again rather than off-again. Less than 90% of time step intervals become statistically significant cold spots, and no time step interval is a statistically significant hotspot. |
| New Cold spot |  | The location is a statistically significant cold spot for final time step intervals and has never been a statistically significant cold spot before. |
| Diminishing Cold spot |  | Locations that become cold spots are statistically significant during 90% of time step intervals, including final time step intervals. The low number-grouping intensity at each time step experiences a statistically significant overall decrease. |
| Historical Cold spot |  | The most recent period is not cold, but at least 90% of time step intervals have become statistically significant cold spots. |
| Consecutive Cold spot |  | Locations with one cold spot track are statistically significant without any interruptions in final time step intervals. Locations were never statistically significant cold spots before the last cold spot was run, and less than 90% of all bins were statistically significant cold spots. |
References
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Desjardins, M.; Hohl, A.; Delmelle, E. Rapid surveillance of COVID-19 in the United States using a prospective space-time scan statistic: Detecting and evaluating emerging clusters. Appl. Geogr. 2020, 118, 102202. [Google Scholar] [CrossRef]
- Roser, M.; Ritchie, H.; Ortiz-Ospina, E.; Hasell, J. Coronavirus Pandemic (COVID-19)—Statistics and Research. Available online: https://ourworldindata.org/coronavirus (accessed on 10 August 2020).
- Gugus Tugas Penanganan COVID-19. Peta Sebaran COVID-19. Available online: https://covid19.go.id/peta-sebaran (accessed on 23 September 2020).
- Ruan, Q.; Yang, K.; Wang, W.; Jiang, L.; Song, J. Clinical predictors of mortality due to COVID-19 based on an analysis of data of 150 patients from Wuhan, China. Intensiv. Care Med. 2020, 46, 846–848. [Google Scholar] [CrossRef] [Green Version]
- Mahase, E. Coronavirus: Covid-19 has killed more people than SARS and MERS combined, despite lower case fatality rate. BMJ 2020, 368, m641. [Google Scholar] [CrossRef] [Green Version]
- Wu, Z.; McGoogan, J.M. Characteristics of and Important Lessons from the Coronavirus Disease 2019 (COVID-19) Outbreak in China: Summary of a Report of 72 314 Cases from the Chinese Center for Disease Control and Prevention. JAMA 2020, 323, 1239–1242. [Google Scholar] [CrossRef]
- Kemenkes, R.I. COVID-19 Dalam Angka per 3 Juli 2020. Available online: https://www.kemkes.go.id/article/view/20070500001/covid-19-dalam-angka-per-3-juli-2020.html (accessed on 23 September 2020).
- WHO. Advice on the Use of Masks in the Context of COVID-19; WHO: Geneva, Switzerland, 2020. [Google Scholar]
- De Ridder, D.; Sandoval, J.; Vuilleumier, N.; Stringhini, S.; Spechbach, H.; Joost, S.; Kaiser, L.; Guessous, I. Geospatial digital monitoring of COVID-19 cases at high spatiotemporal resolution. Lancet Digit. Health 2020, 2, e393–e394. [Google Scholar] [CrossRef]
- Kemenkes, R.I. Hindari Lansia Dari Covid 19. Available online: http://padk.kemkes.go.id/article/read/2020/04/23/21/hindari-lansia-dari-covid-19.html (accessed on 23 September 2020).
- Galvin, C.J.; Li, Y.-C.; Malwade, S.; Syed-Abdul, S. COVID-19 preventive measures showing an unintended decline in infectious diseases in Taiwan. Int. J. Infect. Dis. 2020, 98, 18–20. [Google Scholar] [CrossRef] [PubMed]
- WHO. Overview of Public Health and Social Measures in the Context of COVID-19; WHO: Geneva, Switzerland, 2020. [Google Scholar]
- Liu, J.; Zhou, J.; Yao, J.; Zhang, X.; Li, L.; Xu, X.; He, X.; Wang, B.; Fu, S.; Niu, T.; et al. Impact of meteorological factors on the COVID-19 transmission: A multi-city study in China. Sci. Total Environ. 2020, 726, 138513. [Google Scholar] [CrossRef]
- Caspi, G.; Shalit, U.; Kristensen, S.L.; Aronson, D.; Caspi, L.; Rossenberg, O.; Shina, A.; Caspi, O. Climate Effect on COVID-19 Spread Rate: An Online Surveillance Tool. medRxiv 2020. [Google Scholar] [CrossRef] [Green Version]
- Bhagat, R.K.; Wykes, M.S.D.; Dalziel, S.B.; Linden, P.F. Effects of ventilation on the indoor spread of COVID-19. J. Fluid Mech. 2020, 903, 1. [Google Scholar] [CrossRef]
- Asyary, A.; Veruswati, M. Sunlight exposure increased Covid-19 recovery rates: A study in the central pandemic area of Indonesia. Sci. Total Environ. 2020, 729, 139016. [Google Scholar] [CrossRef]
- Kohlmeier, M. Avoidance of vitamin D deficiency to slow the COVID-19 pandemic. BMJ Nutr. Prev. Health 2020, 3, 67–73. [Google Scholar] [CrossRef] [PubMed]
- Baker, T.R.; Battersby, S.; Bednarz, S.W.; Bodzin, A.M.; Kolvoord, B.; Moore, S.; Sinton, D.; Uttal, D. A Research Agenda for Geospatial Technologies and Learning. J. Geogr. 2014, 114, 118–130. [Google Scholar] [CrossRef] [Green Version]
- Saran, S.; Singh, P.; Kumar, V.; Chauhan, P. Review of Geospatial Technology for Infectious Disease Surveillance: Use Case on COVID-19. J. Indian Soc. Remote. Sens. 2020, 48, 1121–1138. [Google Scholar] [CrossRef]
- Sarfo, A.K.; Karuppannan, S. Application of Geospatial Technologies in the COVID-19 Fight of Ghana. Trans. Indian Natl. Acad. Eng. 2020, 5, 193–204. [Google Scholar] [CrossRef]
- Johns Hopkins University Coronavirus Resource Center. COVID-19 Dashboard by the Center for Systems Science and Engineering (CSSE) at Johns Hopkins University (JHU). Available online: https://0-coronavirus-jhu-edu.brum.beds.ac.uk/map.html (accessed on 29 October 2020).
- Saha, A.; Gupta, K.; Patil, M. Urvashi Monitoring and epidemiological trends of coronavirus disease (COVID-19) around the world. Matrix Sci. Medica 2020, 4, 121. [Google Scholar] [CrossRef]
- Songchitruksa, P.; Zeng, X. Getis–Ord Spatial Statistics to Identify Hot Spots by Using Incident Management Data. Transp. Res. Rec. J. Transp. Res. Board 2010, 2165, 42–51. [Google Scholar] [CrossRef]
- Hruby, F.; Castellanos, I.; Ressl, R. Cartographic Scale in Immersive Virtual Environments. KN J. Cartogr. Geogr. Inf. 2020, 1–7. [Google Scholar] [CrossRef]
- Lütjens, M.; Kersten, T.P.; Dorschel, B.; Tschirschwitz, F. Virtual Reality in Cartography: Immersive 3D Visualization of the Arctic Clyde Inlet (Canada) Using Digital Elevation Models and Bathymetric Data. Multimodal Technol. Interact. 2019, 3, 9. [Google Scholar] [CrossRef] [Green Version]
- Keil, J.; Edler, D.; Schmitt, T.; Dickmann, F. Creating Immersive Virtual Environments Based on Open Geospatial Data and Game Engines. KN J. Cartogr. Geogr. Inf. 2021, 1–13. [Google Scholar] [CrossRef]
- Kveladze, I.; Kraak, M.-J.; Van Elzakker, C.P. A Methodological Framework for Researching the Usability of the Space-Time Cube. Cartogr. J. 2013, 50, 201–210. [Google Scholar] [CrossRef]
- Kveladze, I.; Kraak, M.-J.; Van Elzakker, C.P. The space-time cube as part of a GeoVisual analytics environment to support the understanding of movement data. Int. J. Geogr. Inf. Sci. 2015, 29, 2001–2016. [Google Scholar] [CrossRef]
- Marek, L.; Tuček, P.; Pászto, V. Using geovisual analytics in Google Earth to understand disease distribution: A case study of campylobacteriosis in the Czech Republic (2008–2012). Int. J. Health Geogr. 2015, 14, 7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kveladze, I.; Kraak, M.-J.; Van Elzakker, C.P. Cartographic Design and the Space–Time Cube. Cartogr. J. 2018, 56, 73–90. [Google Scholar] [CrossRef]
- Paul, R.; Arif, A.A.; Adeyemi, O.; Ms, S.G.; Han, D. Progression of COVID-19 From Urban to Rural Areas in the United States: A Spatiotemporal Analysis of Prevalence Rates. J. Rural Health 2020. [Google Scholar] [CrossRef]
- Hohl, A.; Delmelle, E.M.; Desjardins, M.R.; Lan, Y. Daily surveillance of COVID-19 using the prospective space-time scan statistic in the United States. Spat. Spatio-Temporal Epidemiol. 2020, 34, 100354. [Google Scholar] [CrossRef]
- Mo, C.; Tan, D.; Mai, T.; Bei, C.; Qin, J.; Pang, W.; Zhang, Z. An analysis of spatiotemporal pattern for COIVD-19 in China based on space-time cube. J. Med. Virol. 2020, 92, 1587–1595. [Google Scholar] [CrossRef] [Green Version]
- Kang, Y.; Cho, N.; Son, S. Spatiotemporal characteristics of elderly population’s traffic accidents in Seoul using space-time cube and space-time kernel density estimation. PLoS ONE 2018, 13, e0196845. [Google Scholar] [CrossRef] [Green Version]
- Nielsen, C.C.; Amrhein, C.G.; Shah, P.S.; Aziz, K.; Osornio-Vargas, A.R. Spatiotemporal Patterns of Small for Gestational Age and Low Birth Weight Births and Associations with Land Use and Socioeconomic Status. Environ. Health Insights 2019, 13, 117863021986992. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, Y.; Ge, L.; Liu, J.; Liu, H.; Yu, L.; Wang, N.; Zhou, Y.; Ding, X. Analyzing hemorrhagic fever with renal syndrome in Hubei Province, China: A space–time cube-based approach. J. Int. Med Res. 2019, 47, 3371–3388. [Google Scholar] [CrossRef] [Green Version]
- Rex, F.E.; Borges, C.A.D.S.; Käfer, P.S. Spatial analysis of the COVID-19 distribution pattern in São Paulo State, Brazil. Ciência Saúde Coletiva 2020, 25, 3377–3384. [Google Scholar] [CrossRef]
- De Jong, W.; Rusli, M.; Bhoelan, S.; Rohde, S.; Rantam, F.A.; Noeryoto, P.A.; Hadi, U.; Van Gorp, E.C.M.; Goeijenbier, M. Endemic and emerging acute virus infections in Indonesia: An overview of the past decade and implications for the future. Crit. Rev. Microbiol. 2018, 44, 487–503. [Google Scholar] [CrossRef]
- East Java Government. East Java’s COVID-19 RADAR. Available online: https://radarcovid19.jatimprov.go.id/ (accessed on 30 June 2020).
- ESRI. ArcGIS Pro|2D, 3D & 4D GIS Mapping Software. Available online: https://www.esri.com/en-us/arcgis/products/arcgis-pro/overview (accessed on 23 January 2021).
- ESRI. Emerging Hot Spot Analysis (Space Time Pattern Mining)—ArcGIS Pro|Documentation. Available online: https://pro.arcgis.com/en/pro-app/tool-reference/space-time-pattern-mining/emerginghotspots.htm (accessed on 10 September 2020).
- Kondo, K. Hot and Cold Spot Analysis Using Stata. Stata J. Promot. Commun. Stat. Stata 2016, 16, 613–631. [Google Scholar] [CrossRef] [Green Version]
- ESRI. How Emerging Hot Spot Analysis works—ArcGIS Pro|Documentation. Available online: https://pro.arcgis.com/en/pro-app/tool-reference/space-time-pattern-mining/learnmoreemerging.htm (accessed on 11 September 2020).
- Ord, J.K.; Getis, A. Local Spatial Autocorrelation Statistics: Distributional Issues and an Application. Geogr. Anal. 1995, 27, 286–306. [Google Scholar] [CrossRef]
- Dubin, R.A. Spatial autocorrelation and neighborhood quality. Reg. Sci. Urban Econ. 1992, 22, 433–452. [Google Scholar] [CrossRef]
- ESRI. Modeling Spatial Relationships—ArcGIS Pro|Documentation. Available online: https://pro.arcgis.com/en/pro-app/tool-reference/spatial-statistics/modeling-spatial-relationships.htm#guid-f063a8f5-9459-42f9-bf41-4e66fbbcc415 (accessed on 10 September 2020).
- Harris, N.L.; Goldman, E.; Gabris, C.; Nordling, J.; Minnemeyer, S.; Ansari, S.; Lippmann, M.; Bennett, L.; Raad, M.; Hansen, M.; et al. Using spatial statistics to identify emerging hot spots of forest loss. Environ. Res. Lett. 2017, 12, 024012. [Google Scholar] [CrossRef]
- Mann, H.B. Nonparametric Tests Against Trend Author. Econometrica 1945, 13, 245–259. [Google Scholar] [CrossRef]
- Kendall, M.G. Rank Correlation, 4th ed.; Charles Griffin & Company Limited: London, UK, 1970. [Google Scholar]
- Kriegel, H.; Kröger, P.; Sander, J.; Zimek, A. Density-based clustering. Wiley Interdiscip. Rev. Data Min. Knowl. Discov. 2011, 1, 231–240. [Google Scholar] [CrossRef]
- Campello, R.J.G.B.; Moulavi, D.; Sander, J. Density-Based Clustering Based on Hierarchical Density Estimates; Springer: Berlin/Heidelberg, Germany; pp. 160–172.
- Yuill, R.S. The Standard Deviational Ellipse; An Updated Tool for Spatial Description. Geogr. Ann. Ser. B Hum. Geogr. 1971, 53, 28–39. [Google Scholar] [CrossRef]
- Open Street Map (OSM). Available online: https://www.openstreetmap.org (accessed on 6 July 2020).
- Taylor, R. Interpretation of the Correlation Coefficient: A Basic Review. J. Diagn. Med. Sonogr. 1990, 6, 35–39. [Google Scholar] [CrossRef]
- Toharudin, T.; Pontoh, R.S.; Zahroh, S.; Akbar, A.; Sunengsih, N. Impact of large scale social restriction on the COVID-19 cases in East Java. Commun. Math. Biol. Neurosci. 2020, 2020, 1–19. [Google Scholar] [CrossRef]
- Hasani, A. PSBB Fails to Flatten COVID-19 Curve in East Java: Task Force. Available online: https://www.thejakartapost.com/news/2020/05/08/psbb-fails-to-flatten-covid-19-curve-in-east-java-task-force.html (accessed on 24 September 2020).
- Isfandiari, M.A. Dua Penyebab Utama Kasus Covid-19 di Jawa Timur Terparah Hingga Melampaui DKI Jakarta. Available online: https://theconversation.com/dua-penyebab-utama-kasus-covid-19-di-jawa-timur-terparah-hingga-melampaui-dki-jakarta-142378 (accessed on 1 October 2020).
- Wicaksana, P. UNAIR Epidemiology Expert Explains Why East Java Become New Epicenter of Covid-19. Available online: http://news.unair.ac.id/en/2020/06/29/unair-epidemiology-expert-explains-why-east-java-become-new-epicenter-of-covid-19/ (accessed on 23 September 2020).
- Purba, D.O. Covid-19 di Jatim Tembus 10.092 Kasus, Waspada Attack Rate Surabaya Meningkat. Available online: https://surabaya.kompas.com/read/2020/06/24/05200071/covid-19-di-jatim-tembus-10092-kasus-waspada-attack-rate-surabaya-meningkat (accessed on 20 September 2020).
- Birch, C.P.; Oom, S.P.; Beecham, J.A. Rectangular and hexagonal grids used for observation, experiment and simulation in ecology. Ecol. Model. 2007, 206, 347–359. [Google Scholar] [CrossRef]
- ESRI. Why Hexagons?—ArcGIS Pro|Documentation. Available online: https://pro.arcgis.com/en/pro-app/tool-reference/spatial-statistics/h-whyhexagons.htm (accessed on 9 September 2020).
- Wimberly, M.C.; Giacomo, P.; Kightlinger, L.; Hildreth, M.B. Spatio-Temporal Epidemiology of Human West Nile Virus Disease in South Dakota. Int. J. Environ. Res. Public Health 2013, 10, 5584–5602. [Google Scholar] [CrossRef] [PubMed]
- Mala, S.; Jat, M.K. Geographic information system based spatio-temporal dengue fever cluster analysis and mapping. Egypt. J. Remote. Sens. Space Sci. 2019, 22, 297–304. [Google Scholar] [CrossRef]
- Cafer, A.; Rosenthal, M. COVID-19 in the Rural South: A Perfect Storm of Disease, Health Access, and Co-Morbidity; APCRL Policy Briefs; University of Mississippi: Oxford, MS, USA, 2020. [Google Scholar]
- Gomes, D.S.; Andrade, L.A.; Ribeiro, C.J.N.; Peixoto, M.V.S.; Lima, S.V.M.A.; Duque, A.M.; Cirilo, T.M.; Góes, M.A.O.; Lima, A.G.C.F.; Santos, M.B.; et al. Risk clusters of COVID-19 transmission in northeastern Brazil: Prospective space–time modelling. Epidemiol. Infect. 2020, 148, 1–23. [Google Scholar] [CrossRef]
- Derrible, S.; Kennedy, C. Characterizing metro networks: State, form, and structure. Transportation 2009, 37, 275–297. [Google Scholar] [CrossRef]
- Levinson, D.M. Network Structure and City Size. PLoS ONE 2012, 7, e29721. [Google Scholar] [CrossRef] [PubMed]
- Anenberg, S.C.; Achakulwisut, P.; Brauer, M.; Moran, D.; Apte, J.S.; Henze, D.K. Particulate matter-attributable mortality and relationships with carbon dioxide in 250 urban areas worldwide. Sci. Rep. 2019, 9, 11552. [Google Scholar] [CrossRef]
- Bouffanais, R.; Lim, S.S. Cities—Try to predict superspreading hotspots for COVID-19. Nat. Cell Biol. 2020, 583, 352–355. [Google Scholar] [CrossRef]
- ESRI. Create Space Time Cube by Aggregating Points (Space Time Pattern Mining)—ArcGIS Pro | Documentation. Available online: https://pro.arcgis.com/en/pro-app/latest/tool-reference/space-time-pattern-mining/create-space-time-cube.htm (accessed on 28 January 2021).









| Proximity Factors | March | April | May | June | All-Months |
|---|---|---|---|---|---|
| Dis-to-road | 0.361 * | 0.391 ** | 0.330 ** | 0.311 ** | 0.382 ** |
| Road density (km/km2) | 0.644 ** | 0.688 ** | 0.542 ** | 0.435 ** | 0.501 ** |
| Dis-to-urban center | 0.601 ** | 0.564 ** | 0.708 ** | 0.727 ** | 0.639 ** |
| Dis-to-ATMs | 0.309 ** | 0.324 ** | 0.568 ** | 0.612 ** | 0.495 ** |
| Dis-to-attraction | 0.523 ** | 0.378 ** | 0.547 ** | 0.302 ** | 0.465 ** |
| Dis-to-bank | 0.390 ** | 0.512 ** | 0.582 ** | 0.665 ** | 0.587 ** |
| Dis-to-bus | 0.221 | 0.371 ** | 0.384 ** | 0.655 ** | 0.263 ** |
| Dis-to-cafe | 0.527 ** | 0.522 ** | 0.579 ** | 0.471 ** | 0.614 ** |
| Dis-to-restaurant | 0.465 ** | 0.520 ** | 0.582 ** | 0.403 ** | 0.589 ** |
| Dis-to-fuel | 0.421 ** | 0.573 ** | 0.664 ** | 0.630 ** | 0.629 ** |
| Dis-to-lodging | 0.502 ** | 0.568 ** | 0.450 ** | 0.488 ** | 0.578 ** |
| Dis-to-rail | 0.414 ** | 0.303 ** | 0.613 ** | 0.408 ** | 0.437 ** |
| Dis-to-shopping | 0.529 ** | 0.568 ** | 0.521 ** | 0.589 ** | 0.577 ** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Purwanto, P.; Utaya, S.; Handoyo, B.; Bachri, S.; Astuti, I.S.; Utomo, K.S.B.; Aldianto, Y.E. Spatiotemporal Analysis of COVID-19 Spread with Emerging Hotspot Analysis and Space–Time Cube Models in East Java, Indonesia. ISPRS Int. J. Geo-Inf. 2021, 10, 133. https://0-doi-org.brum.beds.ac.uk/10.3390/ijgi10030133
Purwanto P, Utaya S, Handoyo B, Bachri S, Astuti IS, Utomo KSB, Aldianto YE. Spatiotemporal Analysis of COVID-19 Spread with Emerging Hotspot Analysis and Space–Time Cube Models in East Java, Indonesia. ISPRS International Journal of Geo-Information. 2021; 10(3):133. https://0-doi-org.brum.beds.ac.uk/10.3390/ijgi10030133
Chicago/Turabian StylePurwanto, Purwanto, Sugeng Utaya, Budi Handoyo, Syamsul Bachri, Ike Sari Astuti, Kresno Sastro Bangun Utomo, and Yulius Eka Aldianto. 2021. "Spatiotemporal Analysis of COVID-19 Spread with Emerging Hotspot Analysis and Space–Time Cube Models in East Java, Indonesia" ISPRS International Journal of Geo-Information 10, no. 3: 133. https://0-doi-org.brum.beds.ac.uk/10.3390/ijgi10030133