
Pharmacists’ Seasonal Influenza Vaccine Recommendations


1
Department of Medical Sciences, Private University in the Principality of Liechtenstein, 9495 Triesen, Liechtenstein
2
Kantonsspital St. Gallen, 9007 St. Gallen, Switzerland
*
Author to whom correspondence should be addressed.
Pharmacy 2022, 10(3), 51; https://0-doi-org.brum.beds.ac.uk/10.3390/pharmacy10030051
Submission received: 13 March 2022
/
Revised: 6 April 2022
/
Accepted: 14 April 2022
/
Published: 25 April 2022
(This article belongs to the Special Issue Community-Based Pharmacy Practice Quality Improvement and Research)
Abstract
:Seasonal influenza vaccination rates among European countries remain low despite the World Health Organization’s recommendations to vaccinate high-risk groups. Healthcare worker recommendations are strong predictors of increased vaccination uptake in the population. Therefore, this study aimed to analyze seasonal influenza vaccination recommendation behavior among pharmacists towards high-risk groups including patients, coworkers, and pharmacists’ family members during the COVID-19 pandemic. This cross-sectional, questionnaire-based research was conducted in Switzerland during the flu season and sent to all members of the Swiss Pharmacist Association. In December 2020, 569 community pharmacists completed the online survey. The influenza vaccination recommendation rates for high-risk patients were 93.6% for the elderly, 70.7% for pregnant women, 65.2% for immunocompromised people, and 60.3% for patients with chronic diseases. Pharmacists tend to recommend influenza immunization to patients more than to family members and colleagues. Holding a certification to administer immunization and personal influenza vaccine history were the main predictors for recommending influenza vaccination to patients, family members, and colleagues. Our results indicated that influenza vaccination recommendation rates in our whole sample of pharmacists, were higher for vaccinated and immunizing pharmacists. Ensuring high vaccinations rates and high ratio of immunizing pharmacists may be important in promoting seasonal influenza vaccination in the general population.
1. Introduction
Seasonal influenza causes annual disease outbreaks and poses a significant health risk. Influenza-associated respiratory disease has been reported to be attributable to approximately 291,243 to 645,832 annual deaths worldwide, most of which occur in the elderly (aged ≥65 years) [1]. Pregnant, immunocompromised, and chronically ill women have an increased risk of hospitalization and complications [2]. The Swiss Federal Office of Public Health and the World Health Organization recommend seasonal influenza vaccination (SIV) for these susceptible populations [3,4]. Flu vaccination is an effective strategy for reducing influenza-related hospitalization and mortality [5]. However, the actual SIV rates in Switzerland remained low, declining from approximately 16.4% in 2007 to 14.1% in 2012. SIV for high-risk groups was 38.5% for people aged ≥65 years, 5.1% for pregnant women, and 20–50% for patients suffering from chronic diseases. Other European countries have reported similar SIV rates [6,7].
Improving SIV rates during the COVID-19 pandemic is particularly important, as Influenza and COVID-19 share many symptoms [8]. This strategy was crucial at the time of the study, as no COVID-19 vaccine was available in Switzerland [9].
Flu vaccination in pharmacies has been reported to improve its uptake [10]. Several countries worldwide, have authorized their pharmacists to deliver vaccines; however, since the COVID-19 pandemic, many countries have recently changed their stance [11]. Pharmacist-based immunization programs are estimated to have the potential to affect >600 million individuals worldwide [12]. In 2015, the Swiss government widened the scope of community pharmacy practice to include various vaccine administrations, while COVID-19 immunization was added after in February 2021 [13,14]. Community pharmacists (CPs) receive certification to administer vaccines after completing a 4-day training course that covers theory and practice. Every two years, CPs must fulfill a continuing education obligation to maintain their certification.
Professional health recommendations are another effective way to improve SIV uptake. Recommendations from a healthcare worker (HCW) have been reported to have a great impact on vaccination rates, achieving success rates of >80% [15,16,17,18,19,20]. Patients visit a community pharmacy approximately 10 more times than their primary care physicians, allowing CPs several opportunities to act as educators by providing accurate information and recommendations regarding vaccines [21].
Only a few studies have focused on SIV recommendations rates, and most of these studies assessed physicians recommendations behavior, ranging from 0% in Asian countries to 95.9% in Western European countries [20,22,23,24,25,26,27,28].
This study aimed to estimate Swiss pharmacists’ SIV recommendation rates in the general population during the COVID-19 pandemic and to identify possible demographic factors associated with providing recommendations. In addition, this research helped to gain further insight into CPs willingness to offer COVID-19 vaccination in their pharmacies.
2. Materials and Methods
2.1. Study Design and Participants
This questionnaire-based research was conducted during the seasonal influenza season of 2020–2021, among CPs. On 1 December 2020, the Swiss Association of Pharmacists (Pharmasuisse, Bern-Liebefeld, Switzerland) distributed an invitation link to all its members, approximately 5900 pharmacists.
Before commencing the voluntary survey, participants were informed regarding the objectives and methodology of the study. The participants were asked to complete the survey in 3 weeks, and no incentives were offered to them. Confidentiality and anonymity of the gathered information were maintained, and no data identifying a participant were collected. All data were gathered using an online survey software (SoSci Survey, Munich, Germany).
2.2. Development and Calibration of the Questionnaire
An anonymous questionnaire was designed and adapted to the specificities of the Swiss Health System after reviewing existing survey tools from previous empirical research [29,30,31,32]. The feasibility of the survey in French and German was evaluated in a pilot study of several CPs. Based on the feedback, minor changes were incorporated to improve the final questionnaire. The data obtained from these CPs were excluded in the analysis. Only complete questionnaires were included in the final results and then translated into English.
The survey had several questions related to sociodemographics, certification to administer vaccines, personal SIV status in the previous season, and SIV recommendation behavior. Participants who recommended SIV only to the high-risk group could then select a single or multiple subgroup. Additionally, in relation to the COVID-19 pandemic, CPs were asked whether they would offer COVID-19 vaccination to patients once available. Variables related to willingness to offer COVID-19 vaccination were evaluated on a 5-point Likert scale, which was dichotomized into “likely” (including “likely” and “very likely”), “undecided”, and “unlikely” (including “unlikely” and “very unlikely”).
2.3. Data Analysis
All data analyses were performed using IBM SPSS, version 26.0 (IBM Corp., 2019, Armonk, NY, USA). Only fully completed questionnaires were used for the analyses. To determine significant associations, logistic regression was used to calculate odds ratios (ORs) with 95% confidence intervals. Statistical tests were considered significant when p values were <0.05.
2.4. Ethics Approval
Our project was voluntary and used fully anonymized data; thus, ethical approval for this study was waived by the ethics committee of Zurich.
3. Results
3.1. Demographics
The questionnaire was sent to approximately 5900 pharmacists, of whom 569 completed the questionnaire (response rate ≈ 9.64%). Five questionnaires were excluded, as responses were provided by pharmacists that were not working in community pharmacy settings. The final sample included 564 CPs (Table 1). The majority of the remaining participants were authorized to administer injections (n = 374, 66.3%).
3.2. Pharmacist Characteristics
Pharmacist demographics are reported in Table 1. Most pharmacists were female (413, 72.5%), worked in an urban setting (487, 86.3%), and were aged >40 years (346, 61.4%). The majority of respondents worked in medium-sized teams of 3 to 5 pharmacists, 389 (69.0%) were authorized to administer injections (n = 374, 66.3%), and almost half (48%) received SIV in the 2019/2020 season.
3.3. Certification
Among 192 non-certified pharmacists, 53 (32.8%) indicated that they were planning to become certified, 70 (36.5%) indicated that they were not planning to become certified, and 59 (30.7%) were unsure. Those who were planning to become certified were significantly more likely to be female, aged <40 years, and practicing in a team with fewer pharmacists. Most pharmacists received certification in 2016 (n = 74, 19.9%), 2017 (n = 101, 27.2%), and 2018 (n = 89, 23.9%).
3.4. COVID-19 Vaccine
The majority (314, 84.4%) of certified pharmacists were willing to offer COVID-19 vaccination to patients if they were legally allowed, once a vaccine would be available. Of the pharmacists, 98 (26.3%) were undecided, and 13 (0.8%) were against offering COVID-19 vaccinations.
3.5. SIV Recommendations to High-Risk Groups
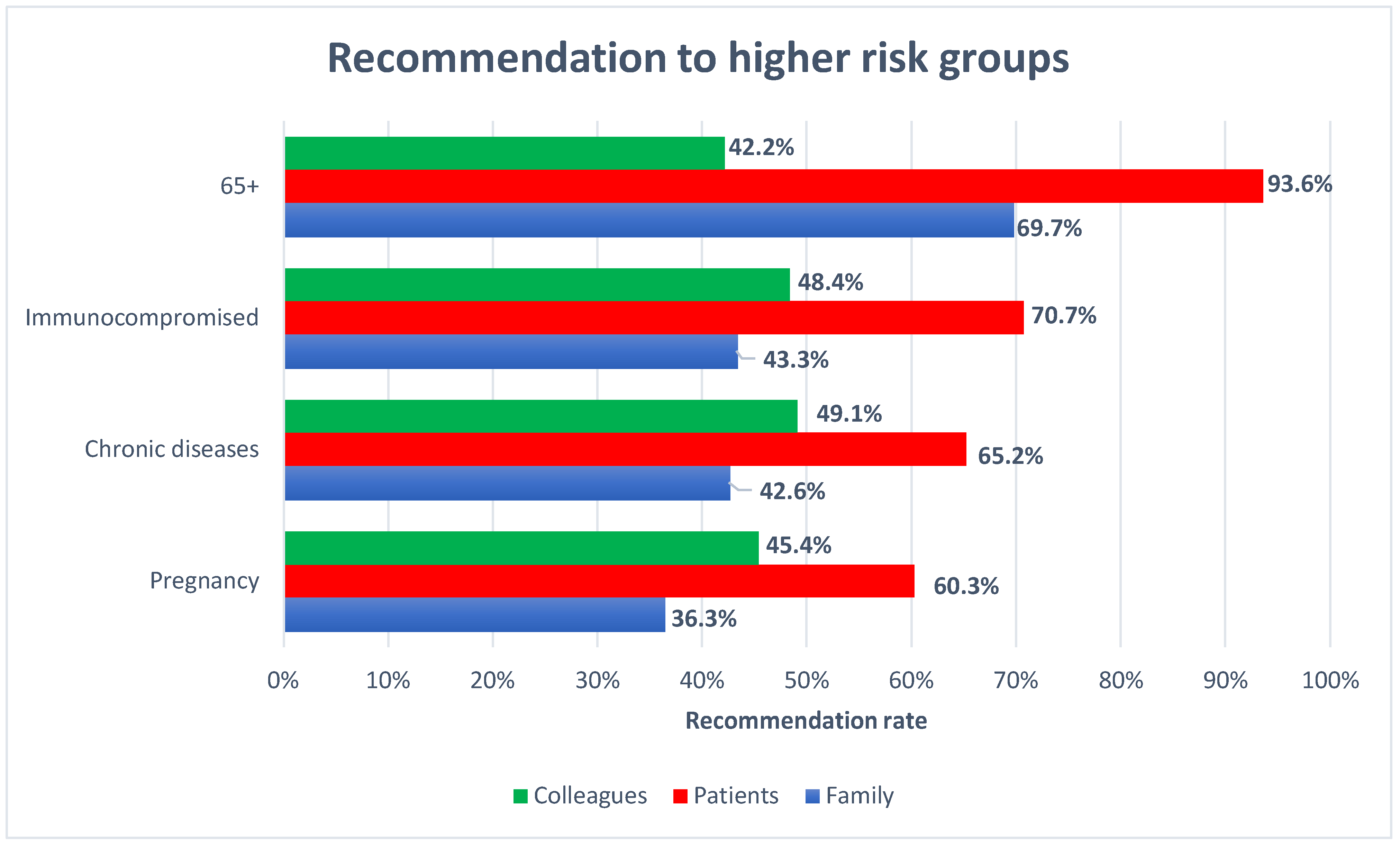
Figure 1 summarizes the frequency of CP recommendations for high-risk groups. The recommendation rates for the elderly, immunocompromised patients, patients suffering from chronic diseases, and pregnant women were 93.6%, 70.7%, 65.2%, and 60.3%, respectively. For each subgroup, patients received recommendations more frequently than pharmacist’s family members or colleagues.
3.6. SIV Recommendations to Family Members
Overall, 23.2% of the CPs recommended SIV to their own family regardless of belonging to a high-risk group, while 51.2% recommended it to at least 1 subgroup. In the multivariate analysis (Table 2), having a certification to vaccinate and personal SIV status were associated with a higher probability of recommending SIV for each group. A rural practice area was a positive predictor for recommending SIV to people with chronic disease and to the elderly. However, CPs aged <30 years were less likely to recommend SIV to immunocompromised family members and to family members suffering from chronic diseases.
3.7. SIV Recommendations to Patients
Of all the CPs, almost one-third (33.2%) recommended SIV to patients regardless of their risk status, and 62.1% recommended it to at least 1 vulnerable group. Multivariate regression analysis (Table 3) revealed that certification to administer the vaccine was significantly associated with recommendation uptake in all subgroups, while personal SIV history was associated with recommendations for pregnant women, immunocompromised people, and people with chronic diseases.
3.8. SIV Recommendations to Coworkers
Of all the CPs, 32.3% recommended SIV to colleagues regardless of them belonging to a high-risk group, while 27.7% recommended SIV to coworkers belonging to a subgroup. Table 4 presents the factors that significantly contributed to the SIV recommendations according to the multivariate regression analyses. Pharmacists’ past vaccination status and holding a certification to administer vaccines was significantly associated with all risk groups, while CPs aged ≥50 years were more likely to recommend SIV to all subgroups, except to pregnant colleagues. Hierarchy played a role in some subgroups; pharmacy owners and managers were more willing to recommend the vaccine to some of the subgroups.
4. Discussion
To the best of our knowledge, this study is the first to generate important insights into Swiss CPs’ SIV recommendations. A wide range of results have been reported in similar studies conducted in other countries for other healthcare professionals [20,22,23,24,25,26,27,28]. An overall recommendation similar to other European countries, for example, 60.1% of CPs recommended SIV to pregnant patients, whereas the European average for different HCWs was 58.9% [25]. Gynecologists in East Germany have recommended SIV to the elderly, with a slightly higher rate of 95.9% [28]. In Spain, pharmacists recommended SIV more frequently to people with chronic disorders (94.8%) and slightly less frequently to immunocompromised patients (63.7%) [32].
In 2012, Swiss SIV rates for people aged 65+ years, pregnant patients, and patients suffering from chronic diseases were 38.5%, 5.1%, and 20–50%, respectively [6]. These vaccination rates were significantly lower than the recommendation rates in our study. The discrepancy between the number of immunizations and the recommendation reported by HCWs is consistent with the literature and could be due to the fact that not all healthcare professionals that recommend SIV are offering vaccination in everyday practice [22,33,34].
Although we did not investigate the reasons for recommending SIV, other studies have identified that the main reasons were national guidelines, relevant training on SIV, and personal vaccination status. Being aware of national guidelines and the influenza vaccine priority group increased the likelihood of recommending SIVs [22,23]. Other studies have revealed that improving HCWs’ knowledge of SIV and influenza may increase the odds of recommending SIV [20,23,27,35]. These results suggest the importance of educating HCWs on the scientific importance of the vaccine and prevention of the disease. These two predictors were addressed during a rigorous immunization certification training program. In addition to practice-based activities, CPs are trained on vaccine-preventable diseases, vaccines, and national vaccination guidelines. This could explain why CPs with certification to administer vaccines were more likely to recommend SIV. Common findings in previous studies have indicated that HCW SIV history was a strong predictor of SIV recommendations in patients [20,22,23,25,27,31]. However, our study did not completely converge with these findings, as this was a common predictor of recommendations in all subgroups excepts for patients aged ≥65 years.
Barriers to the SIV recommendations should also be addressed. The main predictors addressed in the literature regarding the willingness to recommend SIV were safety concerns, lack of awareness of national guidelines, and cost issues. Concerns on side effects and lower vaccine confidence have been associated with lower recommendation rates [23,25,28,36]. In previous studies, a lack of awareness of national guidelines was associated with a lower likelihood of recommending SIV for pregnant women [22,34]. These topics are addressed during the immunization certification training program and might explain why non-certified CPs deliver fewer SIV recommendations. The lack of adequate reimbursement by insurance and recommendation interviews being too time-consuming were cited by various HCWs [27,28,34]. In Switzerland, only SIV at the physician’s office are reimbursed, as opposed to the British model, where pharmacy-based SIV for high-risk groups are reimbursed by health insurance [37,38]. This might also be a reason why CPs in our study recommended SIV to a lesser extent in pregnant patients, immunocompromised patients, and patients suffering from chronic diseases. In Switzerland, CPs are not allowed to vaccinate these higher-risk groups, with a few exceptions, and they will not be able to make a financial gain from that recommendation. CPs may also be more hesitant to make recommendations to these patients because it may be more a physician’s role in providing the vaccine. Similar findings were observed among primary physicians and obstetrician–gynecologists when recommending SIV vaccines to pregnant women [25].
To conduct effective recommendation conversation, CPs should be aware of patients’ reasons for refusing SIV to address them accordingly. The common barriers to SIV reported in the literature are underestimated risk of severe influenza, lack of knowledge of having an indication for influenza vaccination, fear of side effects, and cost related to vaccination [17,18,19]. This is particularly true, as SIV performed in pharmacies is not reimbursed for most patients.
If vaccinated and certified CPs are more likely to recommend vaccines to patients, families, and coworkers, increasing the proportion of certified and vaccinated CPs is important. Hence, Swiss universities started to offer immunization certification programs to pharmacy students during the last year of their masters. Future studies could also investigate what leads current CPs to be certified or vaccinated and assess the barriers, as 36.5% reported unwillingness to attend a certification course, and 30.7% were still unsure.
Receiving a recommendation by any provider is often cited as a strong predictor of immunization, and overcoming vaccination hesitancy may decrease the inhibition threshold for future years [15,16,17,18,19,20,39]. Although CPs are not legally allowed to administer SIV to all higher-risk groups, they may encourage patients to receive the vaccine from a different provider, which may likely increase the vaccination rates of the general population in a snowball system. The uptake of influenza vaccination was observed when routine SIV recommendations were implemented in conjunction with increased access to vaccination [19].
This study had some important limitations. First, this was a cross-sectional study, which only reflects the current recommendation behavior and does not describe changes over time. Second, the participation rate was low, and we cannot exclude the possibility that the CPs that participated had a higher interest in the subject and different recommendation practices than those who refused to participate. Third, SIV recommendation behavior during the COVID-19 pandemic might be higher as interest in SIV was higher during the pandemic and might not reflect practices during non-pandemic years [40]. This may have affected the generalization of the results, and the recommendation rates may have been overestimated. Fourth, self-reported behaviors may be susceptible to recall bias and could result in the overestimation of positive recommendation behavior; however, the survey was conducted during the seasonal influenza season, which could limit this effect. Lastly, the findings are not representative of all Swiss CPs, as we included only those that had membership in the Swiss Pharmacist Association.
Nonetheless, our study has some strengths, such as the use of a nationwide web survey available in German and French. Moreover, to the best of our knowledge, this is the first study to assess recommendation behaviors among Swiss CPs.
5. Conclusions
A personal vaccination history and certification to administer immunization among CPs may contribute to higher SIV recommendations for patients, family members, and colleagues. The elderly had the highest recommendation rates, as these were the primary risk groups that CPs were allowed to vaccinate. To increase CPs’ compliance to actively recommend SIV, regulators should implement an appropriate vaccination course even for non-immunizing CPs and focus on SIV campaigns towards pharmacists. Future work should include measuring the impact of CP recommendations on vaccination rates.
Author Contributions
Conceptualization, R.L., M.T.; methodology, R.L., M.T.; formal analysis, R.L.; writing —original draft preparation, R.L.; writing —review & editing, R.L., M.T.; visualization, R.L.; supervision M.T. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
The data presented in this study are available upon request from the corresponding author.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Iuliano, A.D.; Roguski, K.M.; Chang, H.H.; Muscatello, D.J.; Palekar, R.; Tempia, S.; Cohen, C.; Gran, J.M.; Schanzer, D.; Cowling, B.J.; et al. Estimates of global seasonal influenza-associated respiratory mortality: A modelling study. Lancet 2018, 391, 1285–1300. [Google Scholar] [CrossRef]
- Zolotusca, L.; Jorgensen, P.; Popovici, O.; Pistol, A.; Popovici, F.; Widdowson, M.-A.; Alexandrescu, V.; Ivanciuc, A.; Cheng, P.-Y.; Gross, D.; et al. Risk factors associated with fatal influenza, Romania, October 2009–May 2011. Influenza Other Respir. Viruses 2014, 8, 8–12. [Google Scholar] [CrossRef] [Green Version]
- WHO. WHO Regional Office for Europe Recommendations on Influenza Vaccination for the 2020/2021 Season during the Ongoing COVID-19 Pandemic. 2020. Available online: http://apps.who.int/bookorders (accessed on 2 April 2022).
- Swiss Federal Office of Public Health. Recommendations for Influenza Vaccination (Empfehlungen zur Grippeimpfung). 2011. Available online: https://www.bag.admin.ch/dam/bag/de/dokumente/mt/i-und-b/richtlinien-empfehlungen/empfehlungen-spezifische-erreger-krankheiten/grippe/grippe-empfehlungen-grippeimpfung.pdf.download.pdf/emp-r-e-2011-grippeimpfung.pdf (accessed on 2 April 2022).
- Zhang, Y.; Seale, H.; Yang, P.; MacIntyre, C.R.; Blackwell, B.; Tang, S.; Wang, Q. Factors associated with the transmission of pandemic (H1N1) 2009 among hospital healthcare workers in Beijing, China. Influenza Other Respi. Viruses 2013, 7, 466–471. [Google Scholar] [CrossRef] [Green Version]
- Zürcher, K.; Zwahlen, M.; Berlin, C.; Egger, M.; Fenner, L. Trends in influenza vaccination uptake in Switzerland: Swiss Health Survey 2007 and 2012. Swiss Med. Wkly. 2019, 149, w14705. [Google Scholar] [CrossRef] [Green Version]
- Rizzo, C.; Rezza, G.; Ricciardi, W. Strategies in recommending influenza vaccination in Europe and US. Hum. Vaccin. Immunother. 2018, 14, 693–698. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, X.; Kulkarni, D.; Dozier, M.; Hartnup, K.; Paget, J.; Campbell, H.; Nair, H. Usher Network for COVID-19 Evidence Reviews (UNCOVER) Group Influenza Vaccination Strategies for 2020–2021 in the Context of COVID-19. J. Glob. Health 2020, 10, 021102. Available online: http://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/pubmed/33312512 (accessed on 2 April 2022). [CrossRef]
- Swissmedic. Current Status of Authorisations for Combating COVID-19. Available online: https://www.swissmedic.ch/swissmedic/en/home/news/coronavirus-covid-19/stand-zl-bekaempfung-covid-19.html (accessed on 2 April 2022).
- Anderson, C.; Thornley, T. Who uses pharmacy for flu vaccinations? Population profiling through a UK pharmacy chain. Int. J. Clin. Pharm. 2016, 38, 218–222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Czech, M.; Balcerzak, M.; Antczak, A.; Byliniak, M.; Piotrowska-Rutkowska, E.; Drozd, M.; Juszczyk, G.; Religioni, U.; Vaillancourt, R.; Merks, P. Flu Vaccinations in Pharmacies—A Review of Pharmacists Fighting Pandemics and Infectious Diseases. Int. J. Environ. Res. Public Health 2020, 17, 7945. [Google Scholar] [CrossRef]
- FIP IPF. An Overview of Current Pharmacy Impact on Immunisation—A Global Report 2016. The Hague: International Pharmaceutical Federation (FIP). 2016. Available online: https://fip.org/files/fip/publications/FIP_report_on_Immunisation.pdf (accessed on 2 April 2022).
- The Swiss Confederation. SR 811.11 Bundesgesetz Über Die Universitären Medizinalberufe (Federal Law on the University Medical Professions). Available online: https://www.fedlex.admin.ch/eli/cc/2007/537/de (accessed on 2 April 2022).
- Regierungsrat des Kantons Zürich Verordnung Über Die Universitären Medizinalberufe (MedBV) (Änderung Vom 3 Februar 2021). Available online: https://www.zh.ch/bin/zhweb/publish/regierungsratsbeschluss-unterlagen./2021/110/V%20ueber%20die%20universitaeren%20Medizinalberufe%20Aend%202021-02-03.pdf (accessed on 2 April 2022).
- Pandolfi, E.; Marino, M.G.; Carloni, E.; Romano, M.; Gesualdo, F.; Borgia, P.; Carloni, R.; Guarino, A.; Giannattasio, A.; Tozzi, A.E. The effect of physician’s recommendation on seasonal influenza immunization in children with chronic diseases. BMC Public Health 2012, 12, 984. [Google Scholar] [CrossRef] [Green Version]
- Lv, M.; Fang, R.; Wu, J.; Pang, X.; Deng, Y.; Lei, T.; Xie, Z. The free vaccination policy of influenza in Beijing, China: The vaccine coverage and its associated factors. Vaccine 2016, 34, 2135–2140. [Google Scholar] [CrossRef]
- Casalino, E.; Ghazali, A.; Bouzid, D.; Antoniol, S.; Pereira, L.; Kenway, P.; Choquet, C. Patient’s behaviors and missed opportunities for vaccination against seasonal epidemic influenza and evaluation of their impact on patient’s influenza vaccine uptake. PLoS ONE 2018, 13, e0193029. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wheelock, A.; Thomson, A.; Sevdalis, N. Social and psychological factors underlying adult vaccination behavior: Lessons from seasonal influenza vaccination in the US and the UK. Expert Rev. Vaccines 2013, 12, 893–901. [Google Scholar] [CrossRef] [PubMed]
- Yi, B.; Zhou, S.; Song, Y.; Chen, E.; Lao, X.; Cai, J.; Greene, C.M.; Feng, L.; Zheng, J.; Yu, H.; et al. Innovations in adult influenza vaccination in China, 2014–2015: Leveraging a chronic disease management system in a community-based intervention. Hum. Vaccin. Immunother. 2018, 14, 947–951. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Song, Y.; Zhang, T.; Chen, L.; Yi, B.; Hao, X.; Zhou, S.; Zhang, R.; Greene, C. Increasing seasonal influenza vaccination among high risk groups in China: Do community healthcare workers have a role to play? Vaccine 2017, 35, 4060–4063. [Google Scholar] [CrossRef] [PubMed]
- Haddock, R. The Expanding Role of Today’s Community Pharmacists. Available online: https://www.fdsrx.com/expanding-role-community-pharmacists/ (accessed on 15 February 2022).
- Praphasiri, P.; Ditsungneon, D.; Greenbaum, A.; Dawood, F.S.; Yoocharoen, P.; Stone, D.M.; Olsen, S.J.; Lindblade, K.A.; Muangchana, C. Do Thai Physicians Recommend Seasonal Influenza Vaccines to Pregnant Women? A Cross-Sectional Survey of Physicians’ Perspectives and Practices in Thailand. PLoS ONE 2017, 12, e0169221. [Google Scholar] [CrossRef]
- Ye, L.; Chen, J.; Fang, T.; Cui, J.; Li, H.; Ma, R.; Sun, Y.; Li, P.; Dong, H.; Xu, G. Determinants of healthcare workers’ willingness to recommend the seasonal influenza vaccine to diabetic patients: A cross-sectional survey in Ningbo, China. Hum. Vaccin. Immunother. 2018, 14, 2979–2986. [Google Scholar] [CrossRef]
- Nichol, K.L.; Zimmerman, R. Generalist and Subspecialist Physicians’ Knowledge, Attitudes, and Practices Regarding Influenza and Pneumococcal Vaccinations for Elderly and Other High-Risk Patients. Arch. Intern. Med. 2001, 161, 2702. [Google Scholar] [CrossRef] [Green Version]
- Morales, K.F.; Menning, L.; Lambach, P. The faces of influenza vaccine recommendation: A Literature review of the determinants and barriers to health providers’ recommendation of influenza vaccine in pregnancy. Vaccine 2020, 38, 4805–4815. [Google Scholar] [CrossRef]
- Li, R.; Xie, R.; Yang, C.; Rainey, J.; Song, Y.; Greene, C. Identifying ways to increase seasonal influenza vaccine uptake among pregnant women in China: A qualitative investigation of pregnant women and their obstetricians. Vaccine 2018, 36, 3315–3322. [Google Scholar] [CrossRef]
- Vishram, B.; Letley, L.; Jan Van Hoek, A.; Silverton, L.; Donovan, H.; Adams, C.; Green, D.; Edwards, A.; Yarwood, J.; Bedford, H.; et al. Vaccination in pregnancy: Attitudes of nurses, midwives and health visitors in England. Hum. Vaccin. Immunother. 2018, 14, 179–188. [Google Scholar] [CrossRef]
- Bödeker, B.; Seefeld, L.; Buck, S.; Ommen, O.; Wichmann, O. Wie werden die Impfempfehlungen gegen saisonale Influenza und gegen humane Papillomaviren in gynäkologischen Praxen umgesetzt? Bundesgesundheitsblatt-Gesundh.-Gesundh. 2016, 59, 396–404. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kraut, A.; Graff, L.; McLean, D. Behavioral change with influenza vaccination: Factors influencing increased uptake of the pandemic H1N1 versus seasonal influenza vaccine in health care personnel. Vaccine 2011, 29, 8357–8363. [Google Scholar] [CrossRef]
- Ziegler, B.; Alsabbagh, W.; Houle, S.; Wenger, L.; Church, D.; Waite, N. Protecting our patients by protecting ourselves. Can. Pharm. J. Rev. Pharm. Can. 2016, 149, 246–255. [Google Scholar] [CrossRef] [Green Version]
- Dolan, S.M.; Cox, S.; Tepper, N.; Ruddy, D.; Rasmussen, S.A.; MacFarlane, K. Pharmacists’ knowledge, attitudes, and practices regarding influenza vaccination and treatment of pregnant women. J. Am. Pharm. Assoc. 2012, 52, 43–56. [Google Scholar] [CrossRef] [PubMed]
- Toledo, D.; Soldevila, N.; Guayta-Escolies, R.; Lozano, P.; Rius, P.; Gascón, P.; Domínguez, A. Knowledge of and Attitudes to Influenza Vaccination among Community Pharmacists in Catalonia (Spain). 2013–2014 Season: A Cross Sectional Study. Int. J. Environ. Res. Public Health 2017, 14, 756. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lu, P.J.; Santibanez, T.A.; Williams, W.W.; Zhang, J.; Ding, H.; Bryan, L.; O’Halloran, A.; Greby, S.M.; Bridges, C.B.; Graitcer, S.B.; et al. Surveillance of influenza vaccination coverage--United States, 2007–2008 through 2011-12 influenza seasons. Morb. Mortal. Wkly. Rep. Surveill. Summ. 2013, 62, 1–28. [Google Scholar]
- Panda, B.; Stiller, R.; Panda, A. Influenza vaccination during pregnancy and factors for lacking compliance with current CDC guidelines. J. Matern. Neonatal Med. 2011, 24, 402–406. [Google Scholar] [CrossRef]
- Ridda, I.; Lindley, I.R.; Gao, Z.; McIntyre, P.; MacIntyre, C.R. Differences in attitudes, beliefs and knowledge of hospital health care workers and community doctors to vaccination of older people. Vaccine 2008, 26, 5633–5640. [Google Scholar] [CrossRef]
- Karlsson, L.C.; Lewandowsky, S.; Antfolk, J.; Salo, P.; Lindfelt, M.; Oksanen, T.; Kivimäki, M.; Soveri, A. The association between vaccination confidence, vaccination behavior, and willingness to recommend vaccines among Finnish healthcare workers. PLoS ONE 2019, 14, e0224330. [Google Scholar] [CrossRef]
- Pharmasuisse. Impfen und Impfberatung. Available online: https://www.pharmasuisse.org/de/1159/Impfen-und-Impfberatung.htm (accessed on 2 April 2022).
- NHS. Find a Pharmacy that Offers the NHS Flu Vaccine. Available online: https://www.nhs.uk/service-search/pharmacy/pharmacy-nhs-flu-vaccine-service (accessed on 2 April 2022).
- Yi, S.; Nonaka, D.; Nomoto, M.; Kobayashi, J.; Mizoue, T. Predictors of the Uptake of A (H1N1) Influenza Vaccine: Findings from a Population-Based Longitudinal Study in Tokyo. PLoS ONE 2011, 6, e18893. [Google Scholar] [CrossRef] [Green Version]
- Paguio, J.A.; Yao, J.S.; Dee, E.C. Silver lining of COVID-19: Heightened global interest in pneumococcal and influenza vaccines, an infodemiology study. Vaccine 2020, 38, 5430–5435. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
CPs’ recommendation overview.


{kind=link}
Table 1.
Characteristics of Survey Respondents.
| Characteristics | N | % |
|---|---|---|
| Sex | ||
| Female | 409 | 72.5% |
| Male | 155 | 27.5% |
| Age | ||
| <30 | 74 | 13.1% |
| 30–39 | 144 | 25.5% |
| 40–49 | 173 | 30.7% |
| 50+ | 173 | 30.7% |
| Certification | ||
| Yes | 372 | 66.0% |
| No | 192 | 34.0% |
| Practice area | ||
| Rural | 77 | 13.7% |
| Urban | 487 | 86.3% |
| Position | ||
| Owner | 93 | 16.5% |
| Manager | 152 | 27.0% |
| Assistant manager | 227 | 40.2% |
| Non-managerial | 92 | 16.3% |
| CP per team | ||
| 1 to 2 | 153 | 27.1% |
| 3 to 5 | 389 | 69.0% |
| 6+ | 22 | 3.9% |
| SIV season 2019/2020 | ||
| Yes | 271 | 48.0% |
| No | 293 | 52.0% |
Table 2.
Season influenza vaccination recommendations to family members.
| Pregnant Women | Chronic Disease | Immunocompromised | Aged 65+ Years | |||||
|---|---|---|---|---|---|---|---|---|
| OR | 95% CI | OR | 95% CI | OR | 95% CI | OR | 95% CI | |
| Sex | ||||||||
| Female | 1.14 | 0.74–1.77 | 0.78 | 0.51–1.19 | 0.80 | 0.52–1.22 | 0.81 | 0.52–1.25 |
| Male | – | – | – | – | – | – | – | – |
| Age | ||||||||
| <30 | 0.52 | 0.26–1.05 | 0.42 * | 0.22–0.80 | 0.49 * | 0.26–0.92 | 1.22 | 0.63–2.35 |
| 30–39 | 1.40 | 0.84–2.31 | 0.94 | 0.57–1.54 | 0.89 | 0.54–1.46 | 0.98 | 0.59–1.64 |
| 40–49 | 1.01 | 0.63–1.62 | 0.92 | 0.58–1.46 | 0.69 | 0.43–1.09 | 1.45 | 0.88–2.37 |
| 50+ | – | – | – | – | – | – | – | – |
| Certification | ||||||||
| Yes | 2.02 * | 1.33–3.08 | 2.15 * | 1.44–3.23 | 2.17 * | 1.45–3.25 | 1.85 * | 1.24–2.76 |
| No | – | – | – | – | – | – | – | – |
| Practice area | ||||||||
| Rural | 1.48 | 0.87–2.52 | 2.38 * | 1.39–4.07 | 0.64 | 0.38–1.10 | 3.09 * | 1.55–6.17 |
| Urban | – | – | – | – | – | – | – | – |
| Position | ||||||||
| Owner | 0.99 | 0.52–1.88 | 0.76 | 0.40–1.43 | 0.75 | 0.40–1.42 | 0.75 | 0.37–1.50 |
| Manager | 1.18 | 0.66–2.11 | 0.80 | 0.45–1.42 | 0.94 | 0.53–1.67 | 0.74 | 0.40–1.38 |
| Assistant manager | 0.55 | 0.32–0.94 | 0.62 | 0.36–1.05 | 0.71 | 0.42–1.21 | 0.67 | 0.38–1.18 |
| Non-managerial | – | – | – | – | – | – | – | – |
| SIV status 2019/20 | ||||||||
| Yes | 2.80 * | 1.92–4.09 | 2.79 * | 1.94–4.02 | 3.28 * | 2.27–4.72 | 2.24 * | 1.51–3.33 |
| No | – | – | – | – | – | – | – | – |
| CP per team | ||||||||
| 1 to 2 | 0.55 | 0.20–1.48 | 0.58 | 0.22–1.55 | 0.87 | 0.32–2.34 | 1.60 | 0.59–4.33 |
| 3 to 5 | 0.84 | 0.33–2.15 | 0.94 | 0.37–2.39 | 1.24 | 0.48–3.21 | 1.21 | 0.48–3.10 |
| 6+ | – | – | – | – | – | – | – | – |
* p < 0.05.
Table 3.
Season influenza vaccination recommendations to patients.
| Pregnant Women | Chronic Disease | Immunocompromised | Aged 65+ Years | |||||
|---|---|---|---|---|---|---|---|---|
| OR | 95% CI | OR | 95% CI | OR | 95% CI | OR | 95% CI | |
| Sex | ||||||||
| Female | 1.35 | 0.90–2.04 | 1.25 | 0.83–1.89 | 0.85 | 0.55–1.32 | 0.45 | 0.19–1.16 |
| Male | – | – | – | – | – | – | – | – |
| Age | ||||||||
| <30 | 0.93 | 0.51–1.71 | 0.96 | 0.51–1.81 | 0.70 | 0.36–1.35 | 1.31 | 0.32–5.27 |
| 30–39 | 0.77 | 0.47–1.26 | 0.76 | 0.46–1.25 | 0.70 | 0.41–1.20 | 0.40 | 0.16–0.97 |
| 40–49 | 1.05 | 0.66–1.67 | 1.02 | 0.63–1.63 | 0.55 | 0.34–0.89 | 1.21 | 0.45–3.29 |
| 50+ | – | – | – | – | - | – | – | – |
| Certification | ||||||||
| Yes | 1.28–2.76 | 1.95 * | 1.33–2.87 | 1.52 * | 1.02–2.26 | 2.43 * | 1.17–5.05 | |
| No | – | – | – | – | – | – | – | – |
| Practice area | ||||||||
| Rural | 0.58 | 0.34–1.01 | 0.47 | 0.26–0.85 | 0.79 | 0.45–1.40 | 0.33 | 0.08–1.44 |
| Urban | – | – | – | – | – | – | – | – |
| Position | ||||||||
| Owner | 1.24 | 0.66–2.34 | 0.97 | 0.51–1.85 | 1.13 | 0.58–2.17 | 1.69 | 0.45–6.30 |
| Manager | 1.52 | 0.86–2.71 | 1.10 | 0.62–1.95 | 1.39 | 0.77–2.49 | 1.33 | 0.44–4.01 |
| Assistant manager | 0.79 | 0.47–1.32 | 1.09 | 0.65–1.86 | 1.34 | 0.79–2.28 | 0.95 | 0.37–2.45 |
| Non-managerial | – | – | – | – | – | – | – | – |
| SIV status 2019/20 | ||||||||
| Yes | 1.80 * | 1.25–2.58 | 1.78 * | 1.23–2.59 | 1.72 * | 1.17–2.53 | 0.59 | 0.29–1.22 |
| No | – | – | – | – | – | – | – | – |
| CP per team | ||||||||
| 1 to 2 | 0.66 | 0.25–1.74 | 1.17 | 0.45–3.05 | 1.10 | 0.40–2.98 | 0.50 | 0.06–4.59 |
| 3 to 5 | 1.05 | 0.42–2.66 | 1.32 | 0.53–3.29 | 1.07 | 0.42–2.77 | 0.50 | 0.06–4.14 |
| 6+ | – | – | – | – | – | – | – | – |
* p < 0.05.
Table 4.
Season influenza vaccination recommendations to colleagues.
| Pregnant Women | Chronic Disease | Immunocompromised | Aged 65+ Years | |||||
|---|---|---|---|---|---|---|---|---|
| OR | 95% CI | OR | 95% CI | OR | 95% CI | OR | 95% CI | |
| Sex | ||||||||
| Female | 1.36 | 0.90–2.06 | 1.12 | 0.74–1.68 | 1.06 | 0.70–1.60 | 1.20 | 0.79–1.83 |
| Male | – | – | – | – | – | – | – | – |
| Age | ||||||||
| <30 | 0.92 | 0.50–1.69 | 0.36 * | 0.19–0.67 | 0.47 * | 0.25–0.86 | 0.41 * | 0.22–0.77 |
| 30–39 | 0.88 | 0.54–1.43 | 0.57 * | 0.35–0.93 | 0.56 * | 0.34–0.91 | 0.52 * | 0.32–0.85 |
| 40–49 | 0.75 | 0.48–1.18 | 0.51 * | 0.32–0.80 | 0.37 * | 0.24–0.59 | 0.36 * | 0.23–0.58 |
| 50+ | – | – | – | – | - | – | – | – |
| Certification | ||||||||
| Yes | 2.10 * | 1.42–3.11 | 2.42 * | 1.64–3.58 | 1.80 * | 1.22–2.65 | 2.02 * | 1.35–3.01 |
| No | – | – | – | – | – | – | – | – |
| Practice area | ||||||||
| Rural | 0.65 | 0.39–1.09 | 0.90 | 0.54–1.50 | 0.89 | 0.53–1.48 | 0.71 | 0.42–1.19 |
| Urban | – | – | – | – | – | – | – | – |
| Position | ||||||||
| Owner | 2.41 * | 1.28–4.52 | 1.91 * | 1.01–3.62 | 1.95 * | 1.03–3.68 | 1.32 | 0.70–2.48 |
| Manager | 1.63 | 0.93–2.84 | 2.13 * | 1.21–3.77 | 2.68 * | 1.51–4.76 | 1.73 | 0.98–3.07 |
| Assistant manager | 0.77 | 0.46–1.29 | 1.31 | 0.78–2.20 | 1.40 | 0.83–2.37 | 0.90 | 0.53–1.53 |
| Non-managerial | – | – | – | – | – | – | – | – |
| SIV status 2019/20 | ||||||||
| Yes | 1.56 * | 1.08–2.23 | 1.57 * | 1.09–2.24 | 1.94 * | 1.35–2.77 | 1.92 * | 1.34–2.76 |
| No | – | – | – | – | – | – | – | – |
| CP per team | ||||||||
| 1 to 2 | 0.57 | 0.22–1.49 | 1.51 | 0.58–3.92 | 1.16 | 0.45–3.03 | 1.02 | 0.39–2.70 |
| 3 to 5 | 0.42 | 0.17–1.05 | 1.00 | 0.40–2.51 | 0.85 | 0.34–2.11 | 1.02 | 0.41–2.58 |
| 6+ | – | – | – | – | – | – | – | – |
* p < 0.05.
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Langer, R.; Thanner, M. Pharmacists’ Seasonal Influenza Vaccine Recommendations. Pharmacy 2022, 10, 51. https://0-doi-org.brum.beds.ac.uk/10.3390/pharmacy10030051
AMA Style
Langer R, Thanner M. Pharmacists’ Seasonal Influenza Vaccine Recommendations. Pharmacy. 2022; 10(3):51. https://0-doi-org.brum.beds.ac.uk/10.3390/pharmacy10030051
Chicago/Turabian StyleLanger, Roland, and Mirjam Thanner. 2022. "Pharmacists’ Seasonal Influenza Vaccine Recommendations" Pharmacy 10, no. 3: 51. https://0-doi-org.brum.beds.ac.uk/10.3390/pharmacy10030051
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.