The Discharge Companion Program: An Interprofessional Collaboration in Transitional Care Model Delivery

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Research Design
2.2. Methodology
2.3. Data Collection
2.4. Data Analysis
3. Results
3.1. Thirty-Day Post-Discharge Readmission
3.2. Clinical Interventions
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Kaiser Family Foundation. Aiming for Fewer Hospital u-turns: The Medicare Hospital Readmission Reduction Program. Available online: http://www.kff.org/medicare/issue-brief/aiming-for-fewer-hospital-u-turns-the-medicare-hospital-readmission-reduction-program/ (accessed on 17 January 2019).
- Zuckerman, R.B.; Ruhter, J.; Epstein, A.M.; Sheingold, S.H.; Orav, E.J. Readmissions, Observation, and the Hospital Readmissions Reduction Program. N. Engl. J. Med. 2016, 374, 1543–1551. [Google Scholar] [CrossRef] [PubMed]
- Patient Protection and Affordable Care Act (PPACA). 2010; 42 U.S.C. § 18001. Available online: http://housedocs.house.gov/energycommerce/ppacacon.pdf (accessed on 18 June 2019).
- Constantino, M.; Frey, B.; Hall, B.; Painter, P. The influence of a post discharge intervention on reducing hospital readmissions in a Medicare population. Popul. Health Manag. 2013, 16, 310–316. [Google Scholar] [CrossRef] [PubMed]
- Harrison, P.L.; Hara, P.A.; Pope, J.E.; Young, M.C.; Rula, E.Y. The Impact of Postdischarge Telephonic Follow-Up on Hospital Readmissions. Popul. Health Manag. 2011, 14, 27–32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anderson, S.L.; Marrs, J.C.; Griend, J.P.V.; Hanratty, R. Implementation of a Clinical Pharmacy Specialist-Managed Telephonic Hospital Discharge Follow-Up Program in a Patient-Centered Medical Home. Popul. Health Manag. 2013, 16, 235–241. [Google Scholar] [CrossRef] [PubMed]
- Altfeld, S.J.; Shier, G.E.; Rooney, M.; Johnson, T.J.; Golden, R.L.; Karavolos, K.; Avery, E.; Nandi, V.; Perry, A.J. Effects of an Enhanced Discharge Planning Intervention for Hospitalized Older Adults: A Randomized Trial. Gerontologist 2012, 53, 430–440. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kilcup, M.; Schultz, D.; Carlson, J.; Wilson, B. Post discharge pharmacist medication reconciliation: Impact on readmission rates and financial savings. J. Am. Pharm. Assoc. 2013, 53, 78–84. [Google Scholar] [CrossRef] [PubMed]
- Kind, A.J.H.; Jensen, L.; Barczi, S.; Bridges, A.; Kordahl, R.; Smith, M.A.; Asthana, S.; Kordahl, B. Low-Cost Transitional Care with Nurse Managers Making Mostly Phone Contact with Patients Cut Rehospitalization At A VA Hospital. Health Aff. 2012, 31, 2659–2668. [Google Scholar] [CrossRef]
- Naylor, M.D.; Hirschman, K.B.; Hanlon, A.L.; Bowles, K.H.; Bradway, C.; McCauley, K.M.; Pauly, M.V. Comparison of evidence-based interventions on outcomes of hospitalized, cognitively impaired older adults. J. Comp. Eff. Res. 2014, 3, 245–257. [Google Scholar] [CrossRef] [Green Version]
- Coleman, E.A.; Parry, C.; Chalmers, S.; Min, S. The care transitions intervention results of a randomized controlled trial. Arch. Intern. Med. 2006, 166, 1822–1828. [Google Scholar] [CrossRef]
- Goldman, L.; Elizabeth, S.; Urmimala, K.; Kessell, E.; Guzman, D.; Schneidermann, M.; Kushel, M. Support from hospital to home for elders: A randomized trial. Ann. Int. Med. 2014, 161, 472–481. [Google Scholar] [CrossRef]
- Schnipper, J.L.; Kirwin, J.L.; Contugno, M.C.; Wahlstrom, S.A.; Brown, B.A.; Tarvin, E.; Bates, D.W. Role of pharmacist counseling in preventing adverse drug events after hospitalization. Arch. Intern. Med. 2006, 166, 565–571. [Google Scholar] [CrossRef] [PubMed]
- Hume, A.; Kirwin, J.; Bieber, H.; Couchenour, R.; Hall, D.; Kennedy, A.; Burkhardt, C. Improving care transitions: Current practice and future opportunities for pharmacists. Pharmacotherapy 2012, 32, e326–e337. [Google Scholar] [PubMed]
- Joint Commission Resources. Partnership for patients hospital engagement network. Available online: http://www.jcrinc.com/assets/1/7/JCR_HEN_2013_Report_final.pdf (accessed on 17 January 2019).
- Rodrigues, C.R.; Harrington, A.R.; Murdock, N.; Holmes, J.T.; Borzadek, E.Z.; Calabro, K.; Slack, M.K. Effect of pharmacy-supported transition-of-care interventions on 30-day readmissions: A systematic review and meta-analysis. Ann. Pharmacother. 2017, 51, 866–889. [Google Scholar] [CrossRef] [PubMed]
- Gardner, R.; Li, Q.; Baier, R.R.; Butterfield, K.; Coleman, E.A.; Gravenstein, S. Is implementation of the care transitions intervention associated with cost avoidance after hospital discharge? J. Gen. Intern. Med. 2014, 29, 878–884. [Google Scholar] [CrossRef] [PubMed]
- Polinski, J.M.; Moore, J.M.; Kyrychenko, P.; Gagnon, M.; Matlin, O.S.; Fredell, J.W.; Shrank, W.H. An insurer’s care transition program emphasizes medication reconciliation, reduces readmissions and costs. Health Aff. 2016, 35, 1222–1229. [Google Scholar] [CrossRef] [PubMed]
- Kirkham, H.S.; Clark, B.L.; Paynter, J.; Lewis, G.H.; Duncan, I. The effect of a collaborative pharmacist–hospital care transition program on the likelihood of 30-day readmission. Am. J. Health Syst. Pharm. 2014, 71, 739–745. [Google Scholar] [CrossRef]
- Jack, B.W.; Chetty, V.K.; Anthony, D.; Greenwald, J.L.; Sanchez, G.M.; Johnson, A.E.; Forsythe, S.R.; O’Donnell, J.K.; Paasche-Orlow, M.K.; Manasseh, C.; et al. A reengineered hospital discharge program to decrease rehospitalization: A randomized trial. Ann. Intern. Med. 2009, 150, 178–187. [Google Scholar] [CrossRef] [PubMed]
- Rochester-Eyeguokan, C.; Pincus, K.; Patel, R.; Reitz, S. The current landscape of transitions of care practice models: A scoping review. Pharmacotherapy 2016, 36, 117–133. [Google Scholar] [CrossRef]
- Hansen, L.O.; Young, R.S.; Hinami, K.; Leung, A.; Williams, M.V. Interventions to reduce 30-day rehospitalization: A systematic review. Ann. Intern. Med. 2011, 155, 520–528. [Google Scholar] [CrossRef]
- Kwan, J.L.; Lo, L.; Sampson, M.; Shojania, K.G. Medication reconciliation during transitions of care as a patient safety strategy: A systematic review. Ann. Intern. Med. 2013, 158 Pt 2, 397–403. [Google Scholar] [CrossRef]
- Burton, L.C.; Anderson, G.F.; Kues, I.W. Using electronic health records to help coordinate care. Milbank Q. 2004, 82, 457–481. [Google Scholar] [CrossRef] [PubMed]



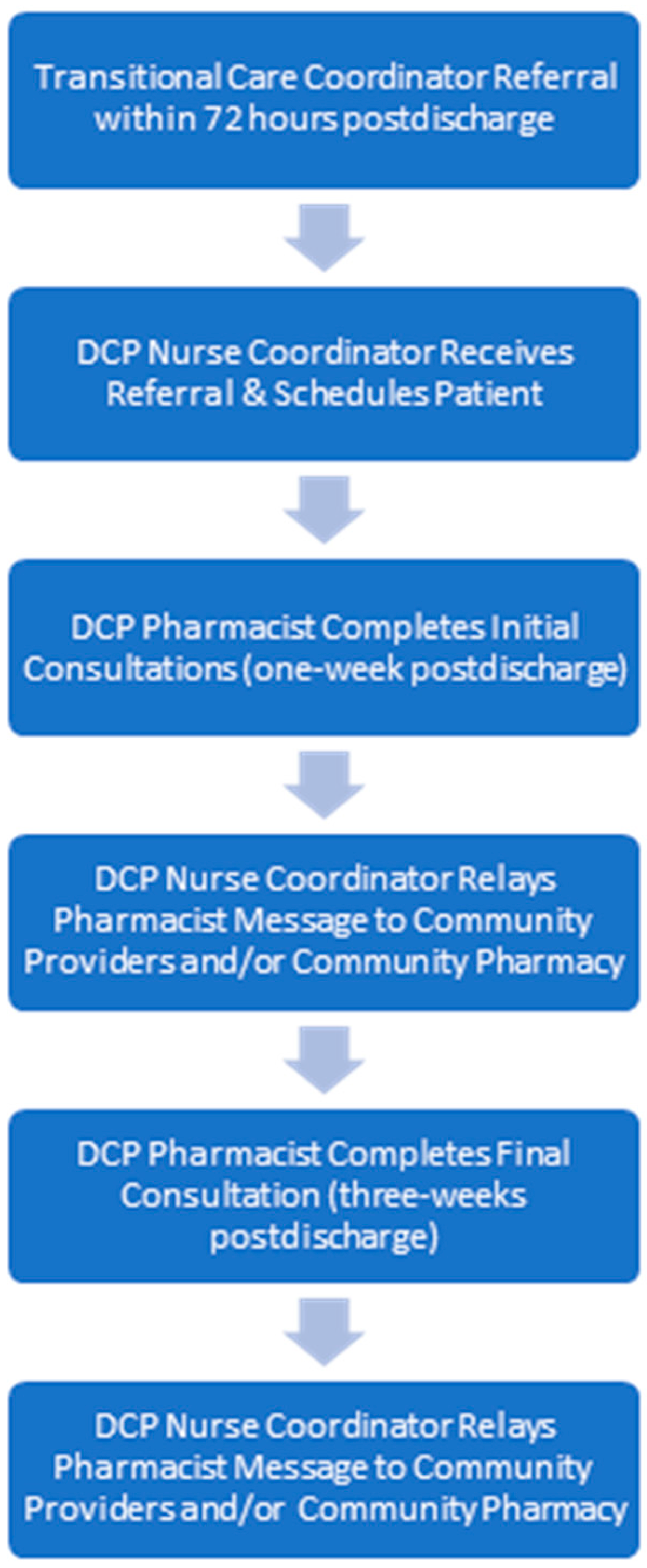{kind=link}
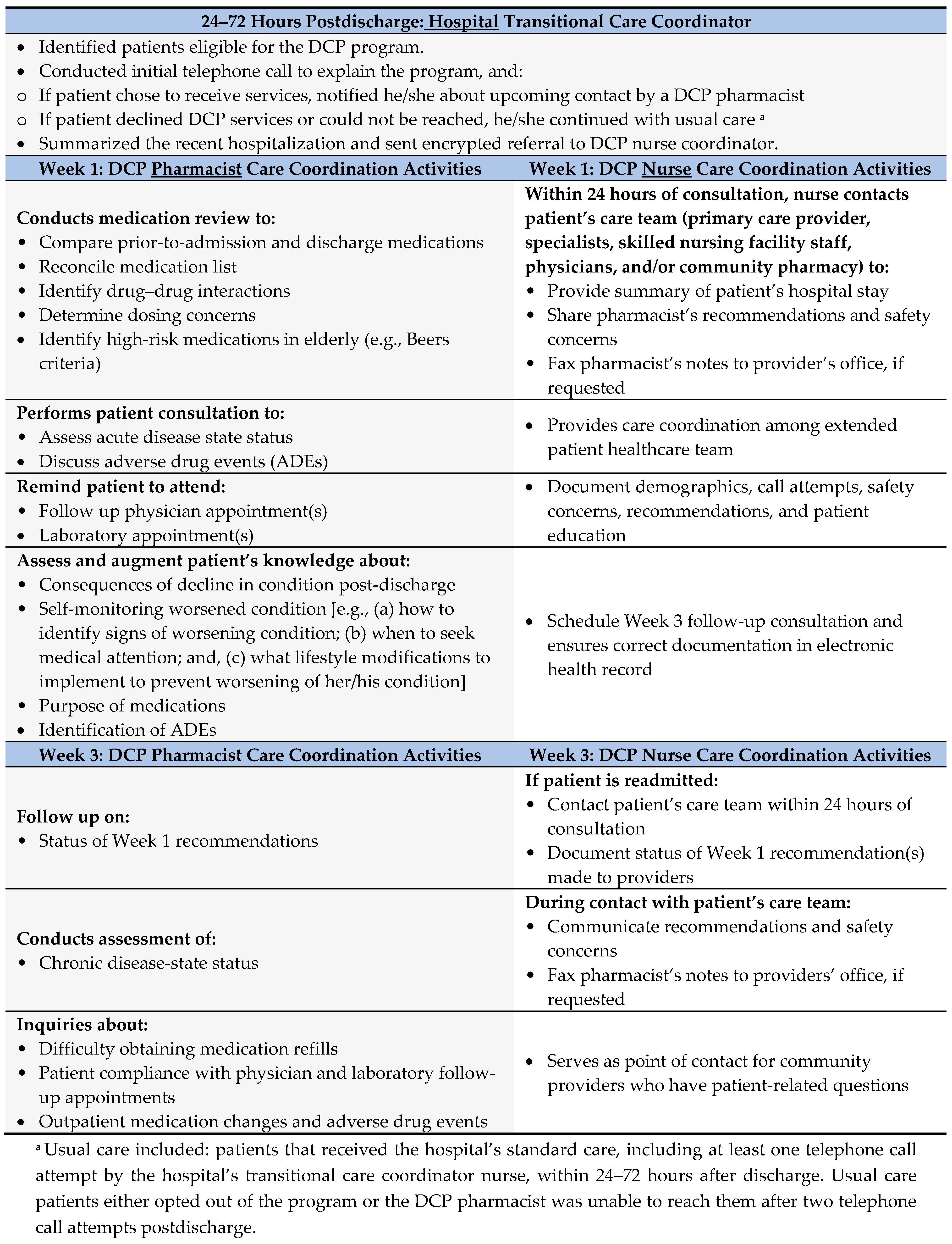{kind=link}
| Characteristic | UC Group (N = 116) | Intervention Group (N = 340) | p-Value |
|---|---|---|---|
| Age, mean (SD) | 76.1 (9.1) | 77.9 (8.4) | <0.04 * |
| Male, n (%) | 73 (63) | 203 (60) | 0.54 |
| White, n (%) | 107 (92) | 318 (93) | 0.61 |
| Hispanic, n (%) | 19 (16) | 59 (17) | 0.94 |
| Program qualifying conditions 1 | 0.14 | ||
| Asthma | 1 (1) | 6 (2) | |
| Chronic obstructive pulmonary disease | 11 (9) | 34 (10) | |
| Diabetes mellitus | 0 (0) | 2 (1) | |
| Heart failure | 50 (43) | 121 (36) | |
| Myocardial infarction | 20 (17) | 53 (16) | |
| Pneumonia | 26 (22) | 61 (18) | |
| Post-coronary artery bypass graft | 6 (5) | 61 (18) | |
| Renal failure | 2 (2) | 2 (1) | |
| Received transitional care coordinator nurse referral to DCP pharmacist, n (%) | 49 (42) | 201 (59) | <0.01 * |
| Discharged to a facility, n (%) | 36 (31) | 91 (27) | 0.46 |
| All-cause readmission rate, n (%) | 20 (17) | 44 (13) | 0.29 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bingham, J.; Campbell, P.; Schussel, K.; Taylor, A.M.; Boesen, K.; Harrington, A.; Leal, S.; Warholak, T. The Discharge Companion Program: An Interprofessional Collaboration in Transitional Care Model Delivery. Pharmacy 2019, 7, 68. https://0-doi-org.brum.beds.ac.uk/10.3390/pharmacy7020068
Bingham J, Campbell P, Schussel K, Taylor AM, Boesen K, Harrington A, Leal S, Warholak T. The Discharge Companion Program: An Interprofessional Collaboration in Transitional Care Model Delivery. Pharmacy. 2019; 7(2):68. https://0-doi-org.brum.beds.ac.uk/10.3390/pharmacy7020068
Chicago/Turabian StyleBingham, Jennifer, Patrick Campbell, Kate Schussel, Ann M. Taylor, Kevin Boesen, Amanda Harrington, Sandra Leal, and Terri Warholak. 2019. "The Discharge Companion Program: An Interprofessional Collaboration in Transitional Care Model Delivery" Pharmacy 7, no. 2: 68. https://0-doi-org.brum.beds.ac.uk/10.3390/pharmacy7020068