
The International Pharmacy Game: A Comparison of Implementation in Seven Universities World-Wide

 ,
,  , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Methodologies for Implementation and Conduct of the Pharmacy Game
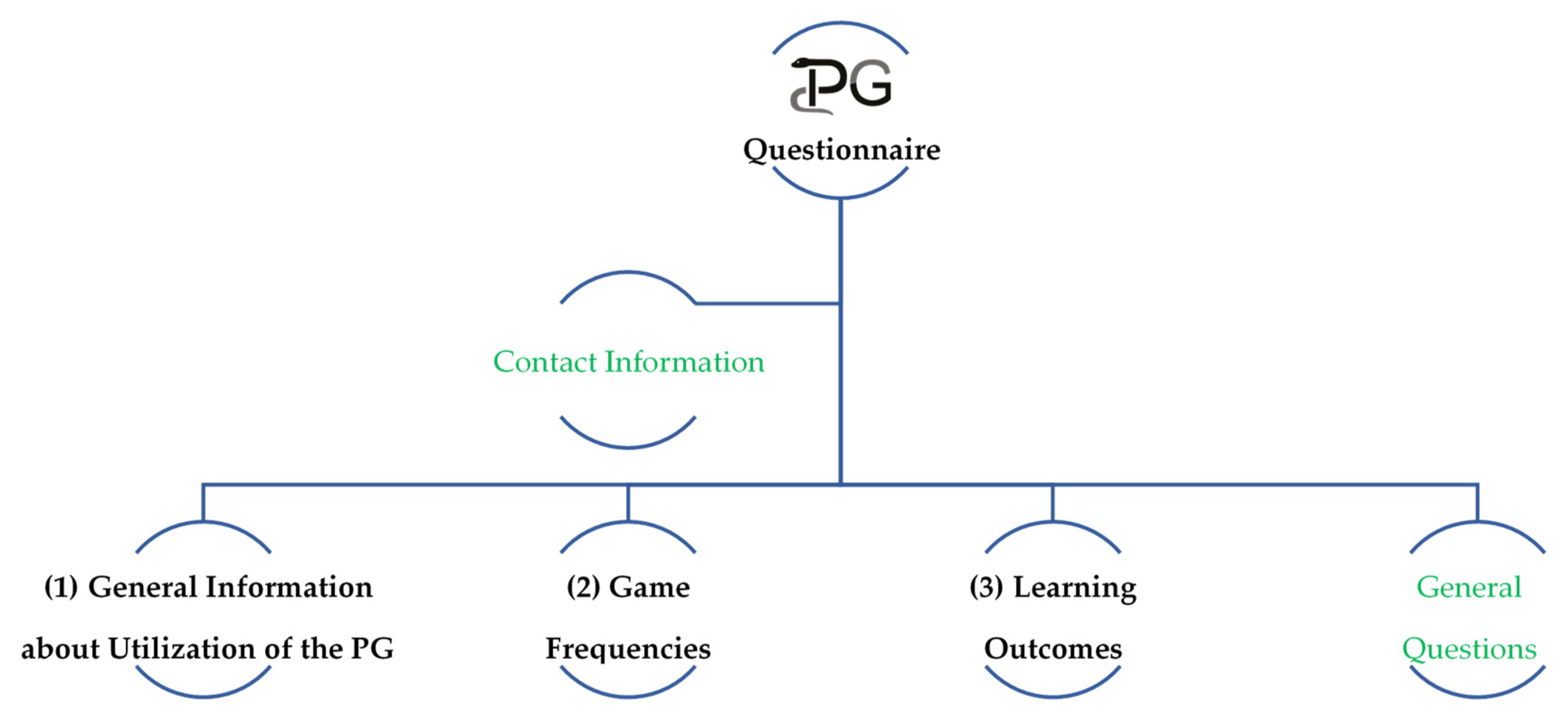
Questionnaire Design, Distribution, and Data Analyses
2.2. Study Design and Methodologies for Assessment Approaches and Student Performance in the Different Universities
Patient Case Selection, Content, and Data Analyses
3. Results
3.1. Implementation and Conduct of the Pharmacy Game
3.1.1. General Information about Utilization of the Pharmacy Game
3.1.2. Game Frequencies and Game Management Staff
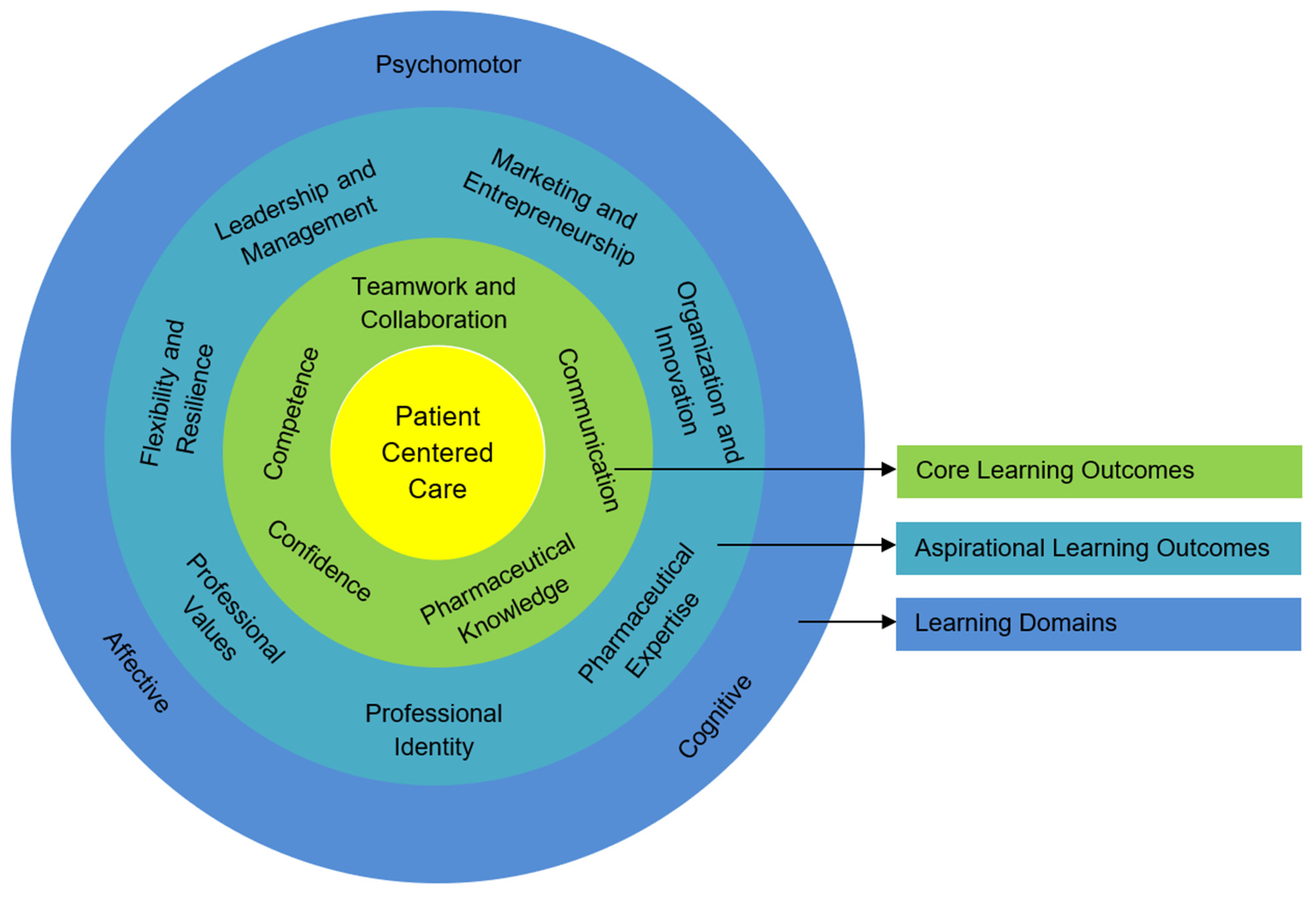
3.1.3. Learning Outcomes and Assessments
3.1.4. Additional Aspects Identified within the Pharmacy Game
3.2. Student Performance on the Patient Case in the Different Universities
4. Discussion
4.1. Main Findings
4.2. Interpretation
4.2.1. Implementation and Conduct of the Pharmacy Game
4.2.2. Student Performances on the Patient Case in the Different Universities
4.3. Strengths and Limitations
4.4. Research Implications
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| University | Additional Participant Experiences |
|---|---|
| University of Groningen |
|
| Utrecht University |
|
| University of Nottingham |
|
| Griffith University |
|
| University of Bath |
|
| Vilnius University |
|
References
- Graafland, M.; Schraagen, J.M.; Schijven, M.P. Systematic review of serious games for medical education and surgical skills training. BJS 2012, 99, 1322–1330. [Google Scholar] [CrossRef]
- Cain, J.; Piascik, P. Are Serious Games a Good Strategy for Pharmacy Education? Am. J. Pharm. Educ. 2015, 79, 1–6. [Google Scholar] [CrossRef]
- Drummond, D.; Hadchouel, A.; Tesnière, A. Serious games for health: Three steps forwards. Adv. Simul. 2017, 2, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Sauvé, L.; Renaud, L.; Kaufman, D.; Marquis, J.-S. Distinguishing between Games and Simulations: A Systematic Review. J. Educ. Technol. Soc. 2007, 10, 247–256. [Google Scholar]
- Fens, T.; Dantuma-Wering, C.M.; Taxis, K. The Pharmacy Game-GIMMICS® a Simulation Game for Competency-Based Education. Pharm. 2020, 8, 198. [Google Scholar] [CrossRef]
- Bedwell, W.L.; Pavlas, D.; Heyne, K.; Lazzara, E.H.; Salas, E. Toward a Taxonomy Linking Game Attributes to Learning. Simul. Gaming 2012, 43, 729–760. [Google Scholar] [CrossRef]
- Okuda, Y.; Bryson, E.O.; DeMaria, S.; Jacobson, L.; Quinones, J.; Shen, B.; Levine, A.I. The Utility of Simulation in Medical Education: What Is the Evidence? Mt. Sinai J. Med. A J. Transl. Pers. Med. 2009, 76, 330–343. [Google Scholar] [CrossRef]
- Gaba, D.M.; Calnan, M.W.; Sanford, E. The future vision of simulation in health care. Qual. Saf. Health Care 2004, 13, i2–i10. [Google Scholar] [CrossRef] [Green Version]
- Austin, A.; Rudolf, F.; Fernandez, J.; Ishimine, P.; Murray, M.; Suresh, P.; McDaniel, M.; Shishlov, K.; Oyama, L. COVID-19 educational innovation: Hybrid in-person and virtual simulation for emergency medicine trainees. AEM Educ. Train. 2021, 5, 1–3. [Google Scholar] [CrossRef]
- Kim, B. Understanding Gamification; Library Technology Reports; American Library Association: Chicago, IL, USA, 2015; Chapter 2; Volume 51. [Google Scholar]
- Dicheva, D.; Dichev, C.; Agre, G.; Angelova, G. Gamification in Education: A Systematic Mapping Study. J. Educ. Technol. Soc. 2015, 18, 75–88. [Google Scholar]
- Hamari, J.; Koivisto, J.; Sarsa, H. Does Gamification Work? A Literature Review of Empirical Studies on Gamification. In Proceedings of the 47th Hawaii International Conference on System Sciences, Waikoloa, HI, USA, 6–9 January 2014. [Google Scholar]
- Al-Azawi, R.; Al-Faliti, F.; Al-Blushi, M. Educational Gamification Vs. Game Based Learning: Comparative Study. Int. J. Innov. Manag. Technol. 2016, 131–136. [Google Scholar] [CrossRef]
- van Der Werf, J.J.; Dekens-Konter, J.; Brouwers, J.R. A New Model for Teaching Pharmaceutical Care Services Management. Pharm. Educ. 2004, 4, 165–169. [Google Scholar] [CrossRef] [Green Version]
- Hirsch, A.C.; Parihar, H.S. A Capstone Course with a Comprehensive and Integrated Review of the Pharmacy Curriculum and Student Assessment as a Preparation for Advanced Pharmacy Practice Experiences. Am. J. Pharm. Educ. 2014, 78, 1–8. [Google Scholar] [CrossRef]
- Phillips, B.B.; Newsome, A.S.; Bland, C.; Palmer, R.; Smith, K.; DeRemer, D.L.; Phan, S.V. Pharmacy Student Performance in a Capstone Course Utilizing the Pharmacists’ Patient Care Process. Am. J. Pharm. Educ. 2019, 83, 1823–1831. [Google Scholar] [CrossRef]
- Harden, R. What is a spiral curriculum? Med. Teach. 1999, 21, 141–143. [Google Scholar] [CrossRef]
- Deci, E.; Ryan, R.M. Self-determination theory: A macrotheory of human motivation, development, and health. Can. Psychol. 2008, 49, 182–185. [Google Scholar] [CrossRef] [Green Version]
- Orsini, C.; Evans, P.; Jerez, O. How to encourage intrinsic motivation in the clinical teaching environment? A systematic review from the self-determination theory. J. Educ. Eval. Health Prof. 2015, 12, 1–10. [Google Scholar] [CrossRef]
- Koster, A.S.; Schalekamp, T.; Meijerman, I. Implementation of Competency-Based Pharmacy Education (CBPE). Pharmacy 2017, 5, 10. [Google Scholar] [CrossRef]
- Wolters, M.; van Paassen, J.; Minjon, L.; Hempenius, M.; Blokzijl, M.-R.; Blom, L. Design of a Pharmacy Curriculum on Patient Centered Communication Skills. Pharmacy 2021, 9, 22. [Google Scholar] [CrossRef] [PubMed]
- Mylrea, M.F.; Gupta, T.S.; Glass, B.D. Developing Professional Identity in Undergraduate Pharmacy Students: A Role for Self-Determination Theory. Pharmacy 2017, 5, 16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koster, A.S.; Mantel-Teeuwisse, A.K.; Woerdenbag, H.J.; Mulder, W.M.C.; Wilffert, B.; Schalekamp, T.; Buurma, H.; Wilting, I.; Westein, M.P.D. Alignment of CanMEDS-based Undergraduate and Postgraduate Pharmacy Curricula in The Netherlands. Pharmacy 2020, 8, 117. [Google Scholar] [CrossRef]
- Bloom, B.S.; Engelhart, M.D.; Furst, E.J.; Hill, W.H.; Krathwohl, D.R. Taxonomy of Educational Objectives, Handbook I: The Cognitive Domain; David McKay Co. Inc.: New York, NY, USA, 1956; Volume 19, ISBN 0-582-28010-9. [Google Scholar]
- Anderson, L.W.; Krathwohl, D.R. A Taxonomy for Learning, Teaching, and Assessing: A Revision of Bloom’s Taxonomy of Educational Objectives; Longman: New York, NY, USA, 2001. [Google Scholar]
- Brookfield, S. Becoming a Critically Reflective Teacher; Wiley: San Francisco, CA, USA, 1995. [Google Scholar]
- Sillius, A. GIMMICS: How to Organize, Manage and Control a Pharmacy Practice Game. In E-Learning: Design, Development and Delivery; University of Groningen: Groningen, The Netherlands, 2005. [Google Scholar]
- Van Rossem, I.; Devroey, D.; De Paepe, K.; Puttemans, F.; Petit, P.; Schol, S.; DeRidder, S.; Vandevoorde, J. A Training Game for Students Considering Family Medicine: An Educational Project Report. J. Med. Life 2020, 12, 411–418. [Google Scholar]
- Hope, D.; Rogers, G.; Grant, G.; King, M. Experiential Learning in a Gamified Pharmacy Simulation: A Qualitative Exploration Guided by Semantic Analysis. Pharmacy 2021, 9, 81. [Google Scholar] [CrossRef]
- Schaafsma, E.; Dantuma, C.; Pilon, K.; de Gier, H. GIMMICS: A simulation of pharmacy practice. In Proceedings of the ESCP–SFPC International Workshop Acquisition of Pharmaceutical Skills: Simulation, Serious Games, Innovative Approaches, Nice, France, 22–23 June 2015; pp. 968–969. [Google Scholar]
- Schaafsma, E.; Dantuma-Wering, C.; Van Wieren, D.; Sarre, S.; De Paepe, K. A Pharmacy Game: Experiencing the Possibilities of an Active and Reflective Learning Style. In Proceedings of the 16th International Social Pharmacy Workshop: Communication and Information in Pharmacy, Lisbon, Portugal, 23–26 August 2010. [Google Scholar]
- Heersche, A.; Hazen, A.C.M.; van Paassen, J.G.; Schalekamp, T.; Verdel, B.M.; van Wieren-de Wijer, B.M.A.; Bouvy, M.L. GIMMICS: A Bridge between Academic Learning and Community Pharmacy. In Proceedings of the European Association of Faculties of Pharmacy Annual Conference, Ankara, Turkey, 16–18 May 2013. [Google Scholar]
- Verdel, B.M.; van Wieren-de Wijer, B.M.A.; van Paassen, J.G.; Hazen, A.C.M.; Bouvy, M.L. GIMMICS: A Pharmacy Game in an Academic Setting. In Proceedings of the Monash Pharmacy Education Symposium: Teaching for Learning, Prato, Italy, 8–10 July 2013. [Google Scholar]
- Boyd, M.; Solanki, V.; Anderson, C.; Sonnex, K.; Brydges, S. Pharmacy Leadership and Management Module: An Evaluation of the Student Experience and Its Perceived Usefulness for Future Employment. In Proceedings of the Monash Pharmacy Education Symposium, Prato, Italy, 9–12 July 2017; p. 270. [Google Scholar]
- Boyd, M.; Solanki, V.; Anderson, C.; Sonnex, K.; Brydges, S. Pharmacy Leadership and Management: A New High Fidelity Simulation to Prepare Students for Their Future Practise. In Proceedings of the Monash Pharmacy Education Symposium, Prato, Italy, 9–12 July 2017; p. 284. [Google Scholar]
- Solanki, V.; Boyd, M.; Anderson, C.; Sonnex, K.; Brydges, S. Using Performance and Leadership Mentors to Support Students during a Simulated Pharmacy Business Module. In Proceedings of the Monash Pharmacy Education Symposium, Prato, Italy, 9–12 July 2017; p. 291. [Google Scholar]
- Solanki, V.; Boyd, M.; Sonnex, K.; Brydges, S.; Anderson, C. Pharmacy Leadership and Management: Student Perspectives of Team-Working in a Simulated Pharmacy Business Module. In Proceedings of the Pharmacy Education Conference, Manchester, UK, 26 June 2017; p. 185. [Google Scholar]
- Hope, D.L.; Rogers, G.D.; Grant, G.D.; King, M.A. Affective Learning in a Serious Pharmacy Game. In Proceedings of the European Association of Faculties of Pharmacy Conference, Krakow, Poland, 15–17 May 2019. [Google Scholar]
- Hope, D.L.; Rogers, G.D.; Grant, G.D.; King, M.A. Impact of a Serious Pharmacy Game on Senior Students’ Professional Competencies: A Controlled Trial. In Proceedings of the European Association of Faculties of Pharmacy Conference, Krakow, Poland, 15–17 May 2019. [Google Scholar]
- Hope, D.L.; Rogers, G.D.; Grant, G.D.; King, M.A. Ecological Momentary Assessment in a Gamified Simulation. In Proceedings of the European Association of Faculties of Pharmacy Conference, Valletta, Malta, 9–11 November 2020. [Google Scholar]
- Hope, D.L.; Rogers, G.D.; Grant, G.D.; King, M.A. Experiential Learning in a Gamified Simulation Detected by Semantic Analysis. In Proceedings of the European Association of Faculties of Pharmacy Conference, Valletta, Malta, 9–11 November 2020. [Google Scholar]
- Hope, D.; Rogers, G.; Grant, G.; King, M. Can an Extended Immersive Pharmacy Simulation Game Influence Students’ Perceptions of Their Professional Competencies? In Proceedings of the Health Services Research and Pharmacy Practice Conference, Nottingham, UK, 10–11 April 2017; pp. 25–26. [Google Scholar]
- Babar, Z.-U.-D. (Ed.) Pharmacy Practice Research Methods; Springer International Publishing: Berlin/Heidelberg, Germany, 2015. [Google Scholar] [CrossRef]
- Ogrinc, G.; Armstrong, G.E.; Dolansky, M.A.; Singh, M.K.; Davies, L. SQUIRE-EDU (Standards for QUality Improvement Reporting Excellence in Education). Acad. Med. 2019, 94, 1461–1470. [Google Scholar] [CrossRef]
- Sandelowski, M. Whatever Happened to Qualitative Description? Res. Nurs. Health 2000, 23, 334–340. [Google Scholar] [CrossRef]
- Given, L. The SAGE Encyclopedia of Qualitative Research Methods; SAGE: Los Angeles, CA, USA, 2008. [Google Scholar]
- Hsieh, H.-F.; Shannon, S.E. Three approaches to qualitative content analysis. Qual. Health Res. 2005, 15, 1277–1288. [Google Scholar] [CrossRef]
- European Commission. European Credit Transfer and Accumulation System (ECTS). Available online: https://ec.europa.eu/education/resources-and-tools/european-credit-transfer-and-accumulation-system-ects_en (accessed on 28 February 2021).
- Miller, G.E. The assessment of clinical skills/competence/performance. Acad. Med. 1990, 65, S63–S67. [Google Scholar] [CrossRef]
- Seybert, A.L.; Smithburger, P.L.; Benedict, N.J.; Kobulinsky, L.R.; Kane-Gill, S.L.; Coons, J.C. Evidence for simulation in pharmacy education. J. Am. Coll. Clin. Pharm. 2019, 2, 686–692. [Google Scholar] [CrossRef]
- Aburahma, M.H.; Mohamed, H.M. Educational Games as a Teaching Tool in Pharmacy Curriculum. Am. J. Pharm. Educ. 2015, 79, 1–9. [Google Scholar] [CrossRef]
- Patel, J. Using Game Format in Small Group Classes for Pharmacotherapeutics Case Studies. Am. J. Pharm. Educ. 2008, 72, 1–5. [Google Scholar] [CrossRef] [Green Version]
- Barclay, S.M.; Jeffres, M.N.; Bhakta, R. Educational Card Games to Teach Pharmacotherapeutics in an Advanced Pharmacy Practice Experience. Am. J. Pharm. Educ. 2011, 75, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tietze, K.J. A Bingo Game Motivates Students to Interact with Course Material. Am. J. Pharm. Educ. 2007, 71, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Chen, A.M.H.; Plake, K.S.; Yehle, K.S.; Kiersma, M.E. Impact of the Geriatric Medication Game on Pharmacy Students’ Attitudes Toward Older Adults. Am. J. Pharm. Educ. 2011, 75, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Roche, V.F.; Alsharif, N.Z.; Ogunbadeniyi, A.M. Reinforcing the Relevance of Chemistry to the Practice of Pharmacy through the Who Wants To Be A Med Chem Millionaire? Learning Game. Am. J. Pharm. Educ. 2004, 68, 1–9. [Google Scholar]
- Oliver, C.H.; Hurd, P.D.; Beavers, M.; Gibbs, E.; Goeckner, B.; Miller, K. Experiential Learning About the Elderly: The Geriatric Medication Game. Am. J. Pharm. Educ. 1995, 59, 155–157. [Google Scholar]
- Evans, S.; Lombardo, M.; Belgeri, M.; Fontane, P. The Geriatric Medication Game in Pharmacy Education. Am. J. Pharm. Educ. 2005, 69, 304–310. [Google Scholar] [CrossRef] [Green Version]
- Neill, M.A.; Wotton, K. High-Fidelity Simulation Debriefing in Nursing Education: A Literature Review. Clin. Simul. Nurs. 2011, 7, e161–e168. [Google Scholar] [CrossRef]
- Aura, S.M.; Sormunen, M.; Jordan, S.E.; Tossavainen, K.A.; Turunen, H. Learning Outcomes Associated with Patient Simulation Method in Pharmacotherapy Education. Simul. Health J. Soc. Simul. Health 2015, 10, 170–177. [Google Scholar] [CrossRef]
- Kapralos, B.; Johnston, C.; Finney, K.; Dubrowski, A. A Serious Game for Training Health Care Providers in Interprofessional Care of Critically-Ill and Chronic Care Patients. J. Emerg. Technol. Web Intell. 2011, 3, 273–281. [Google Scholar] [CrossRef] [Green Version]
- Schindel, T.J.; Yuksel, N.; Breault, R.; Daniels, J.; Varnhagen, S.; Hughes, C.A. Perceptions of pharmacists’ roles in the era of expanding scopes of practice. Res. Soc. Adm. Pharm. 2017, 13, 148–161. [Google Scholar] [CrossRef] [PubMed]
- Australian Pharmacy Council. Accreditation Standards for Pharmacy Programs. Available online: https://www.pharmacycouncil.org.au/resources/pharmacy-program-standards/ (accessed on 20 June 2021).
- World Health Professions Alliance. Interprofessional Collaborative Practice. Available online: https://www.whpa.org/activities/interprofessional-collaborative-practice (accessed on 11 January 2021).
- Vuurberg, G.; Vos, J.; Christoph, L.; de Vos, R. The effectiveness of interprofessional classroom-based education in medical curricula: A systematic review. J. Interprofessional Educ. Pract. 2019, 15, 157–167. [Google Scholar] [CrossRef]
- Guraya, S.Y.; Barr, H. The effectiveness of interprofessional education in healthcare: A systematic review and meta-analysis. Kaohsiung J. Med. Sci. 2018, 34, 160–165. [Google Scholar] [CrossRef]
- Vyas, D.; Bray, B.S.; Wilson, M.N. Use of Simulation-based Teaching Methodologies in US Colleges and Schools of Pharmacy. Am. J. Pharm. Educ. 2013, 77, 1–5. [Google Scholar] [CrossRef] [Green Version]
- Masters, C.; Baker, V.O.; Jodon, H. Multidisciplinary, Team-Based Learning: The Simulated Interdisciplinary to Multidisciplinary Progressive-Level Education (SIMPLE©) Approach. Clin. Simul. Nurs. 2013, 9, e171–e178. [Google Scholar] [CrossRef]
- Ponte, P.R.; Gross, A.H.; Milliman-Richard, Y.J.; Lacey, K. Interdisciplinary Teamwork and Collaboration an Essential Element of a Positive Practice Environment. Annu. Rev. Nurs. Res. 2010, 28, 159–189. [Google Scholar] [CrossRef]
- Hedges, A.R.; Johnson, H.J.; Kobulinsky, L.R.; Estock, J.L.; Eibling, D.; Seybert, A.L. Effects of Cross-Training on Medical Teams’ Teamwork and Collaboration: Use of Simulation. Pharmacy 2019, 7, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cropp, C.D.; Beall, J.; Buckner, E.; Wallis, F.; Barron, A. Interprofessional Pharmacokinetics Simulation: Pharmacy and Nursing Students’ Perceptions. Pharmacy 2018, 6, 70. [Google Scholar] [CrossRef] [Green Version]
- Abraham, O.; Feathers, A.; Grieve, L.; Babichenko, D. Developing and piloting a serious game to educate children about over-the-counter medication safety. J. Pharm. Health Serv. Res. 2019, 10, 235–241. [Google Scholar] [CrossRef]
- Dankbaar, M.E.W.; Richters, O.; Kalkman, C.J.; Prins, G.; Cate, O.T.J.T.; Van Merrienboer, J.J.G.; Schuit, S.C.E. Comparative effectiveness of a serious game and an e-module to support patient safety knowledge and awareness. BMC Med. Educ. 2017, 17, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Graudins, L.V.; Dooley, M.J. Medication Safety: Experiential Learning for Pharmacy Students and Staff in a Hospital Setting. Pharmacy 2016, 4, 38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Richey Smith, C.E.; Ryder, P.; Bilodeau, A.; Schultz, M. Use of an Online Game to Evaluate Health Professions Students’ Attitudes toward People in Poverty. Am. J. Pharm. Educ. 2016, 80, 1–8. [Google Scholar] [CrossRef] [PubMed]


| University | University of Groningen | Utrecht University | Vrije Universiteit Brussel | University of Nottingham | Griffith University | University of Bath | Vilnius University |
|---|---|---|---|---|---|---|---|
| Country | The Netherlands | The Netherlands | Belgium | England | Australia | England | Lithuania |
| Year * | 2000 | 2004 | 2008 | 2015 | 2016 | 2018 | 2019 |
| Name of the game | GIMMICS | GIMMICS/ PharmacyGame | GIMMICS | GPPG | PharmG | GPMS | GIMMICS Vilnius |
| Case Management System (CAMS) ** | Y | A | A | Y | A | N | N |
| Actor Registration System (ARS) ** | Y | A | A | A | A | N | N |
| Prescription Generator ** | Y | A | N | A | A | A | A |
| Mandatory Activity | Y | Y | Y | Y | Y | Y | Y |
| Type of Course | S | S | I | S | I | S | S |
| Associated ECs | Y | Y | Y | N | N | Y | Y |
| Number of ECs | 8 | 7.5 | 30 | - | - | 6 | 5 |
| Annual Iterations | 3 | 4 | 1 | 4 | 1 | 3–4 | 1 |
| Game Days per Game | 25 | 20–25 | 20 | 36 | 15 | 12 | 12 |
| Students per Game | 20–36 | 30–49 | 60 | 60 | 50 | 30 | 24–26 |
| Students per Team | 5–6 | 5–7 | 12 | 6 | 5–8 | 5 | 5–6 |
| Staff per Game (FTE) | 2–3 | 2-4 | 4 | 2 | 5 | 2 | 2 |
| Team Assessment | Y | Y | Y | Y | Y | Y | Y |
| Individual Assessment | Y | Y | Y | Y | Y | Y | N |
| University | Collaboration With: | Collaborative Activities: |
|---|---|---|
| University of Groningen |
|
|
| Utrecht University |
|
|
| Vrije Universiteit Brussel |
|
|
| University of Nottingham |
|
|
| Griffith University |
|
|
| University of Bath |
|
|
| Vilnius University |
|
|
| Student Outcomes | University of Groningen | Utrecht University | University of Nottingham | Griffith University | University of Bath | Vilnius University |
|---|---|---|---|---|---|---|
| Best reported aspects | Patient questioning, history-taking | Patient-focused communication, explanation of not being able to provide a prescription medicine | Patient-focused communication, good dermatology and product knowledge | Patient-focused communication, including active listening and rapport-building | Detailed counselling on use of emollients and topical corticosteroids, including the application of finger tip units | Assessment of the condition, provided appropriate treatment and involved their patient in the treatment decision |
| Aspects for improvement | Non-pharmacological advice, the specific dosing information, conversation length | Trigger identification | Shared decision-making and non-pharmacological management advice | Detailed medication counselling, including provision of finger tip units advice with corticosteroid counselling | Differential diagnosis, shared decision-making and non-pharmacological management advice | Trigger identification, active listening and making the patient feel at ease |
| Appropriate (differential) diagnosis | 71% (5 out of 7 pharmacies) | 43% * (3 out of 7 pharmacies) | 95% (19 out of 20 pharmacies) | 87% (7 out of 8 pharmacies) | 71% (12 out of 17 pharmacies) | 100% (4 out of 4 pharmacies) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fens, T.; Hope, D.L.; Crawshaw, S.; Tommelein, E.; Dantuma-Wering, C.; Verdel, B.M.; Trečiokienė, I.; Solanki, V.; van Puijenbroek, E.P.; Taxis, K. The International Pharmacy Game: A Comparison of Implementation in Seven Universities World-Wide. Pharmacy 2021, 9, 125. https://0-doi-org.brum.beds.ac.uk/10.3390/pharmacy9030125
Fens T, Hope DL, Crawshaw S, Tommelein E, Dantuma-Wering C, Verdel BM, Trečiokienė I, Solanki V, van Puijenbroek EP, Taxis K. The International Pharmacy Game: A Comparison of Implementation in Seven Universities World-Wide. Pharmacy. 2021; 9(3):125. https://0-doi-org.brum.beds.ac.uk/10.3390/pharmacy9030125
Chicago/Turabian StyleFens, Tanja, Denise L. Hope, Sarah Crawshaw, Eline Tommelein, Claudia Dantuma-Wering, Bertha Maria Verdel, Indrė Trečiokienė, Vibhu Solanki, Eugène P. van Puijenbroek, and Katja Taxis. 2021. "The International Pharmacy Game: A Comparison of Implementation in Seven Universities World-Wide" Pharmacy 9, no. 3: 125. https://0-doi-org.brum.beds.ac.uk/10.3390/pharmacy9030125