
Medical Image Processing for Fully Integrated Subject Specific Whole Brain Mesh Generation

Abstract
:1. Introduction
2. Experimental Section
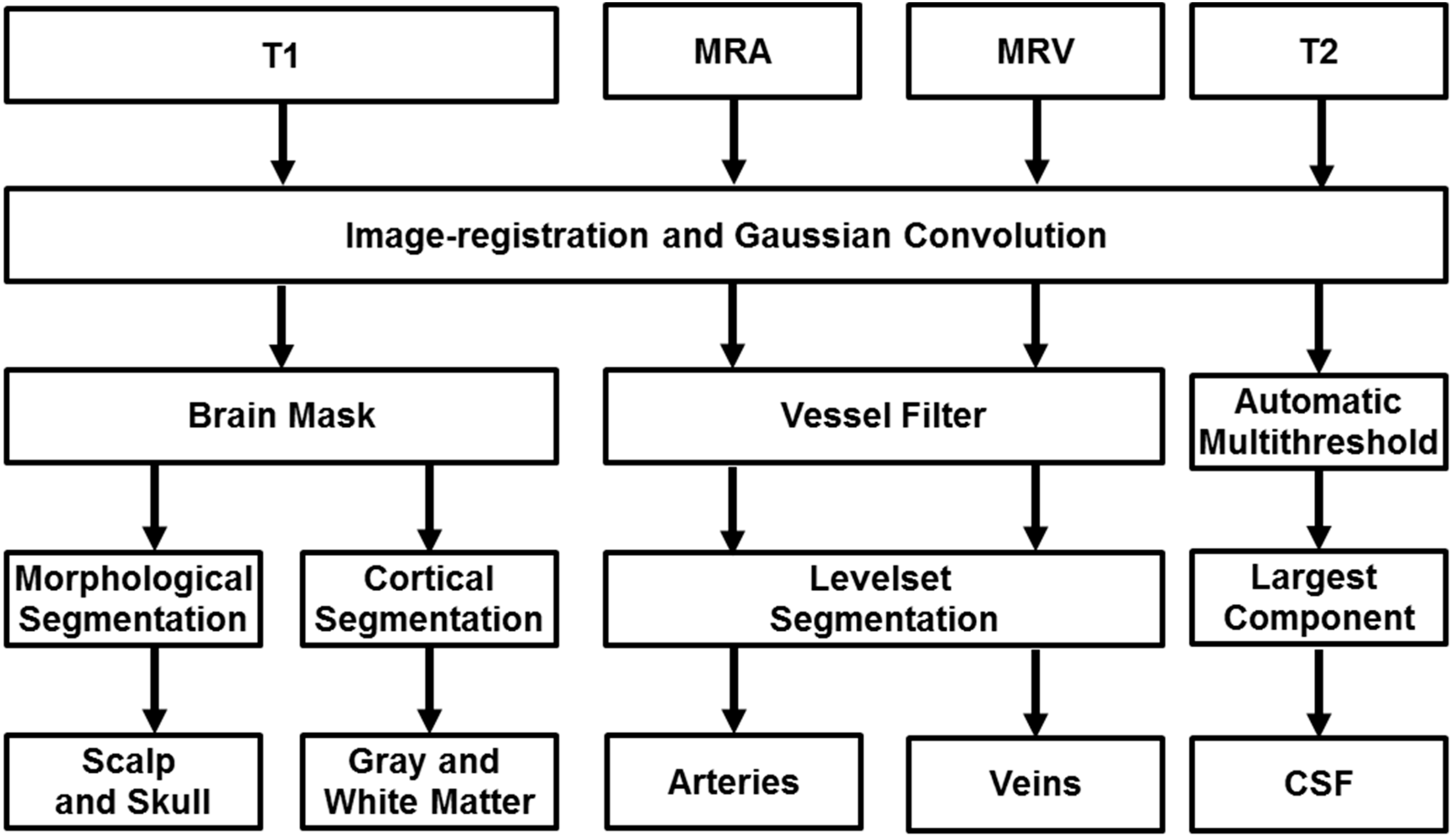
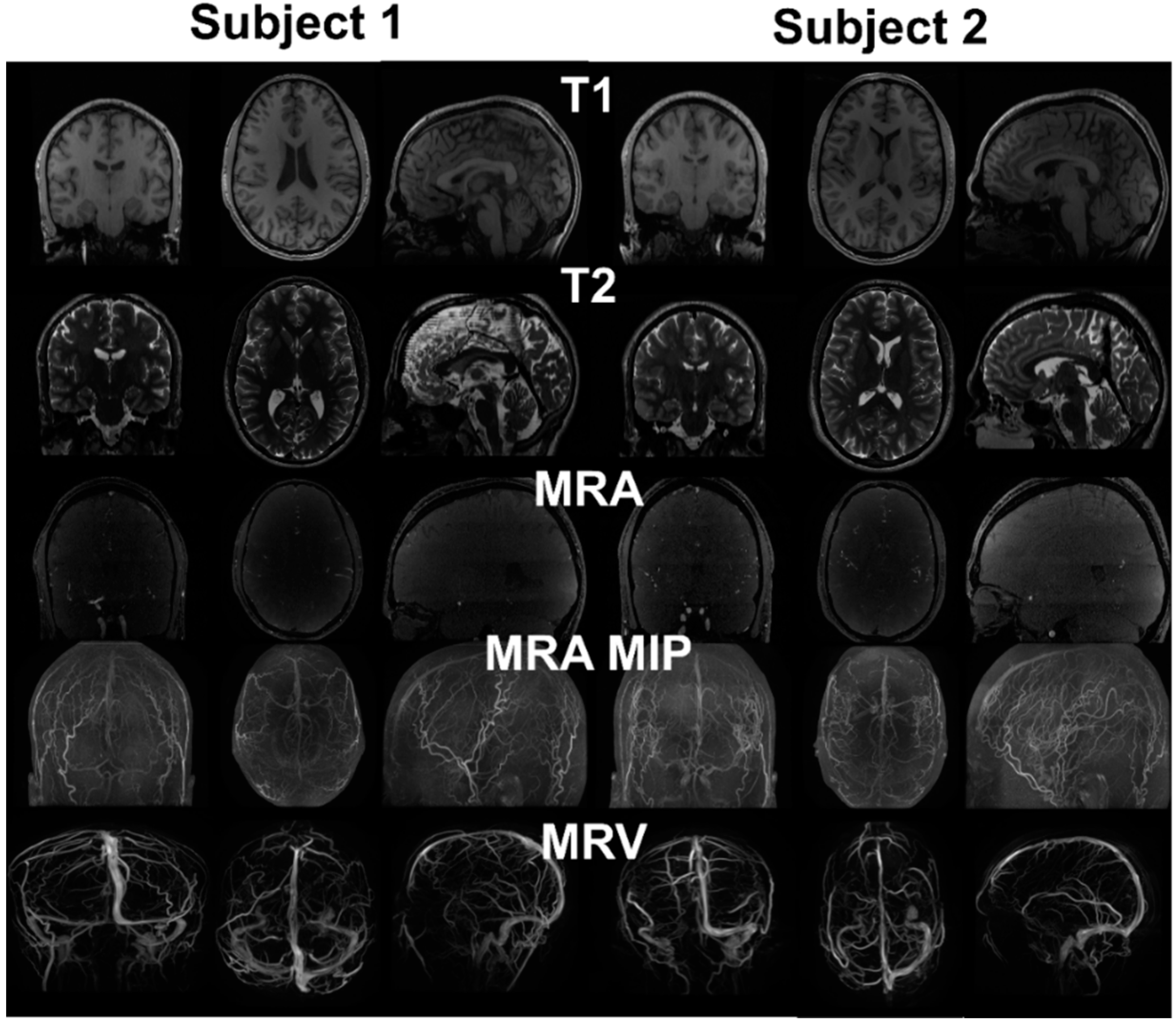
2.1. Image Acquisition

2.2. Surface Segmentation
2.3. Skull and Scalp Segmentation
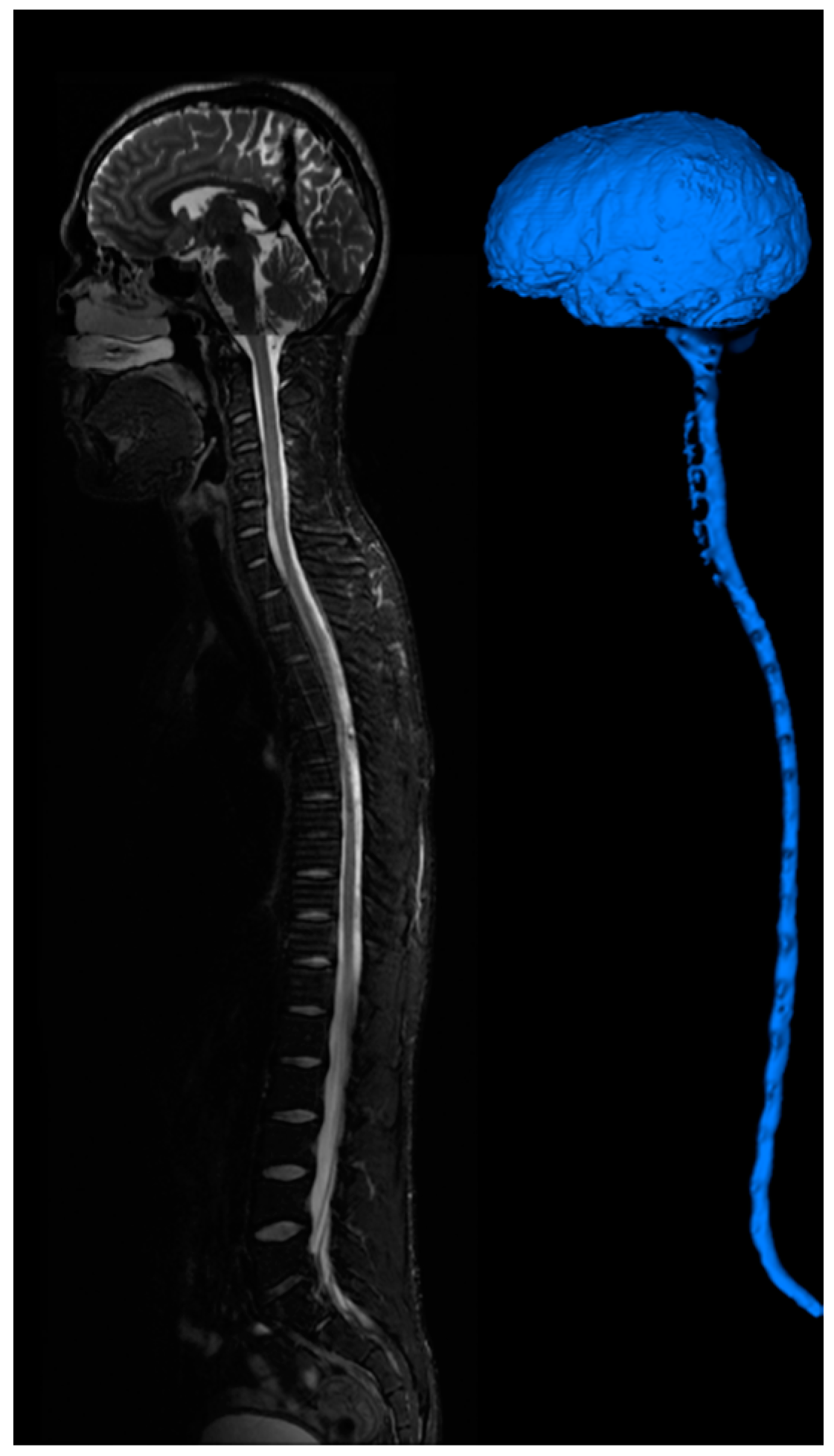
2.4. Cerebrospinal Fluid Space Segmentation
2.5. Mesh Generation
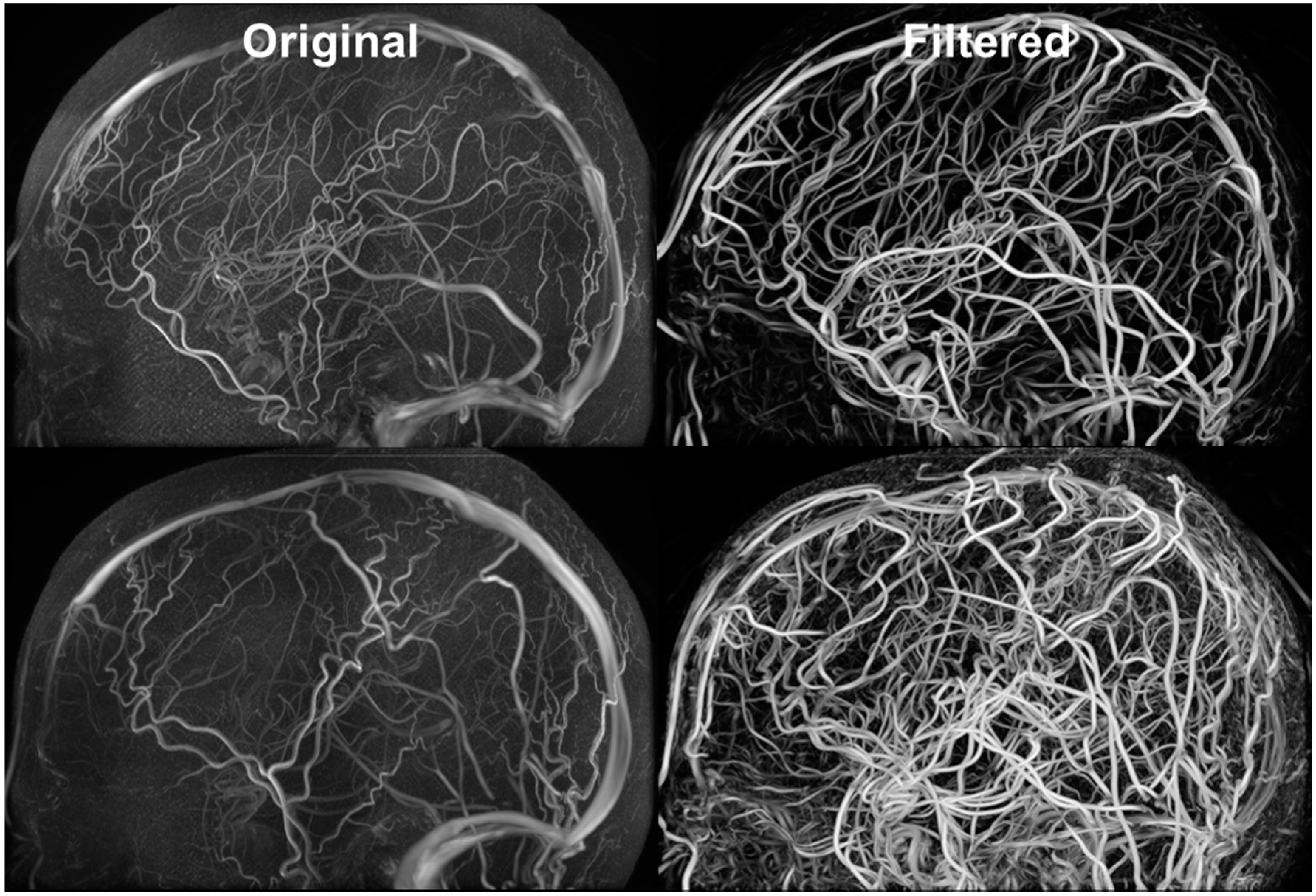
2.6. Cerebral Vasculature Segmentation
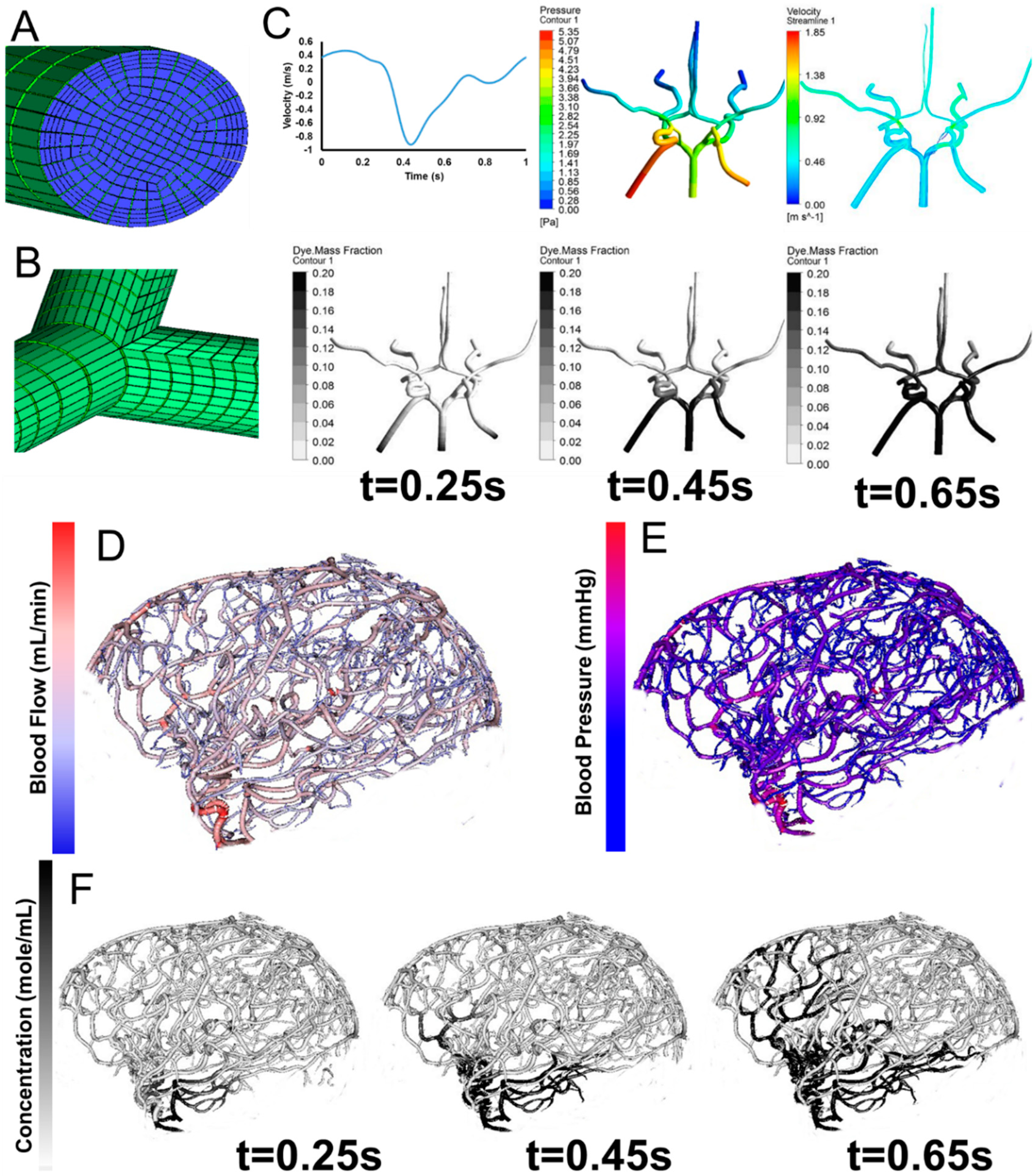
2.7. Vessel Mesh Generation
3. Results and Discussion


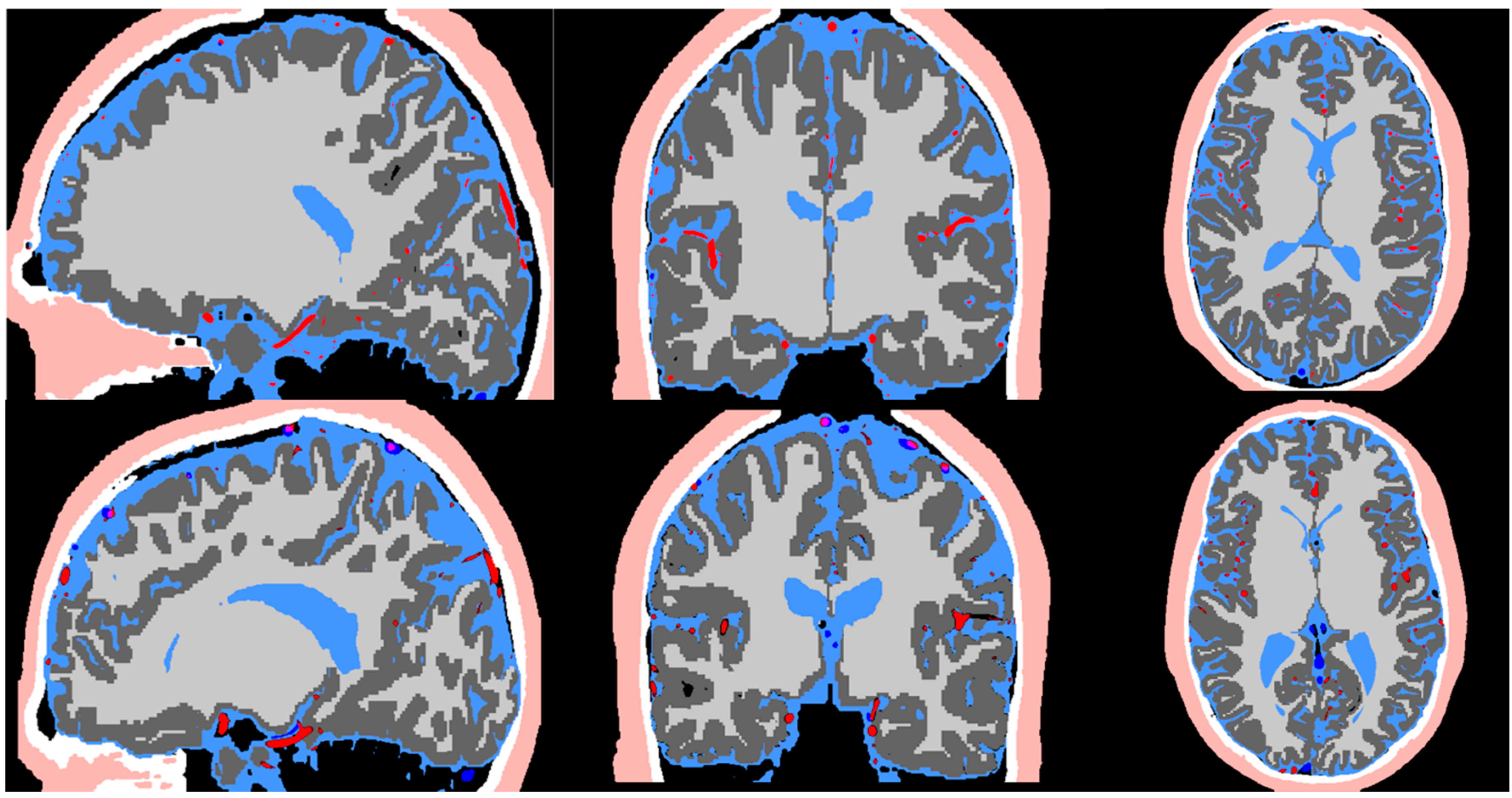
3.1. Cortex Surface Segmentation


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Structure | Subject 1 | Subject 2 | Reported Values | |
|---|---|---|---|---|
| Arteries Volume (mL) | 35.8 | 36.4 | 45 | |
| Veins Volume (mL) | 36.1 | 38.6 | 70 | |
| CSF Volume (mL) | SAS | 35 | 25 | 30 |
| Lateral Ventricles | 13.2 | 21.6 | 16.4 | |
| Third Ventricle | 0.8 | 0.8 | 0.9 | |
| Fourth Ventricle | 1.4 | 1.7 | 1.8 | |
| Spinal CSF | - | 112.6 | 103 | |
| Scalp Surface Area (cm2) | 580 | 590 | 600 | |
| Grey Matter Volume (mL) | 758.6 | 720.4 | 710–980 | |
| Grey Matter Surface Area (cm2) | 2471.4 | 2436.9 | 2400.0 | |
| White Matter Volume (mL) | 546.7 | 538.6 | 260–600 | |
3.2. Skull and Scalp Segmentation
3.3. Cerebrospinal Fluid Space Segmentation
3.4. Vessel Segmentation

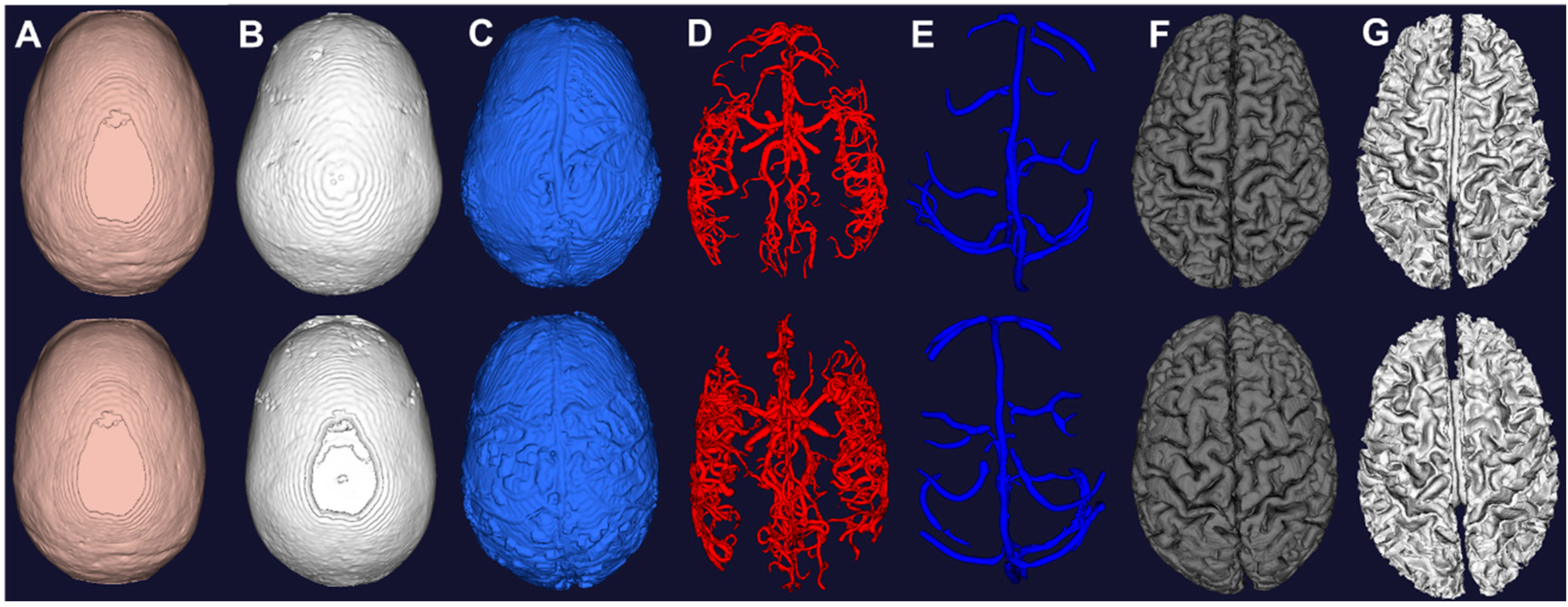
3.5. Whole Brain Mesh Generation
3.6. Parametric Meshing
3.7. Cerebral Hemodynamics Simulation


4. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Doi, K. Computer-aided diagnosis in medical imaging: Historical review, current status and future potential. Comput. Med. Imaging Graph. 2007, 31, 198–211. [Google Scholar] [CrossRef] [PubMed]
- Sundgren, P.C.; Dong, Q.; Gómez-Hassan, D.; Mukherji, S.K.; Maly, P.; Welsh, R. Diffusion tensor imaging of the brain: Review of clinical applications. Neuroradiology 2004, 46, 339–350. [Google Scholar] [CrossRef] [PubMed]
- Wardlaw, J.M.; Mielke, O. Early Signs of Brain Infarction at CT: Observer Reliability and Outcome after Thrombolytic Treatment—Systematic Review. Radiology 2005, 235, 444–453. [Google Scholar] [CrossRef] [PubMed]
- Duncan, J.S.; Ayache, N. Medical image analysis: Progress over two decades and the challenges ahead. IEEE Trans. Pattern Anal. Mach. Intell. 2000, 22, 85–106. [Google Scholar] [CrossRef]
- Milner, J.S.; Moore, J.A.; Rutt, B.K.; Steinman, D.A. Hemodynamics of human carotid artery bifurcations: Computational studies with models reconstructed from magnetic resonance imaging of normal subjects. J. Vasc. Surg. 1998, 28, 143–156. [Google Scholar] [CrossRef] [PubMed]
- Spiegel, M.; Redel, T.; Zhang, Y.J.; Struffert, T.; Hornegger, J.; Grossman, R.G.; Doerfler, A.; Karmonik, C. Tetrahedral vs. polyhedral mesh size evaluation on flow velocity and wall shear stress for cerebral hemodynamic simulation. Comput. Methods Biomech. Biomed. Engin. 2011, 14, 9–22. [Google Scholar] [CrossRef] [PubMed]
- Oshima, M.; Torii, R.; Kobayashi, T.; Taniguchi, N.; Takagi, K. Finite element simulation of blood flow in the cerebral artery. Comput. Methods Appl. Mech. Eng. 2001, 191, 661–671. [Google Scholar] [CrossRef]
- Cebral, J.R.; Castro, M.A.; Appanaboyina, S.; Putman, C.M.; Millan, D.; Frangi, A.F. Efficient pipeline for image-based patient-specific analysis of cerebral aneurysm hemodynamics: Technique and sensitivity. IEEE Trans. Med. Imaging 2005, 24, 457–467. [Google Scholar] [CrossRef] [PubMed]
- Ho, J.; Kleiven, S. Can sulci protect the brain from traumatic injury? J. Biomech. 2009, 42, 2074–2080. [Google Scholar] [CrossRef] [PubMed]
- Ghaffari, M.; Zoghi, M.; Rostami, M.; Abolfathi, N. Fluid Structure Interaction of Traumatic Brain Injury: Effects of Material Properties on SAS Trabeculae. Int. J. Mod. Eng. 2014, 14, 54–62. [Google Scholar]
- Takahashi, T.; Kato, K.; Ishikawa, R.; Watanabe, T.; Kubo, M.; Uzuka, T.; Fujii, Y.; Takahashi, H. 3-D finite element analysis and experimental study on brain injury mechanism. In Proceedings of 2007 29th Annual International Conference of the IEEE on Engineering in Medicine and Biology Society (EMBS), Lyon, France, 22–26 Auguest 2007; pp. 3613–3616.
- Linninger, A.A.; Tsakiris, C.; Zhu, D.C.; Xenos, M.; Roycewicz, P.; Danziger, Z.; Penn, R. Pulsatile cerebrospinal fluid dynamics in the human brain. IEEE Trans. Biomed. Eng. 2005, 52, 557–565. [Google Scholar] [CrossRef] [PubMed]
- Linninger, A.A.; Xenos, M.; Zhu, D.C.; Somayaji, M.R.; Kondapalli, S.; Penn, R.D. Cerebrospinal Fluid Flow in the Normal and Hydrocephalic Human Brain. IEEE Trans. Biomed. Eng. 2007, 54, 291–302. [Google Scholar] [CrossRef] [PubMed]
- Linninger, A.A.; Xenos, M.; Sweetman, B.; Ponkshe, S.; Guo, X.; Penn, R. A mathematical model of blood, cerebrospinal fluid and brain dynamics. J. Math. Biol. 2009, 59, 729–759. [Google Scholar] [CrossRef] [PubMed]
- Linninger, A.A.; Sweetman, B.; Penn, R. Normal and Hydrocephalic Brain Dynamics: The Role of Reduced Cerebrospinal Fluid Reabsorption in Ventricular Enlargement. Ann. Biomed. Eng. 2009, 37, 1434–1447. [Google Scholar] [CrossRef] [PubMed]
- Penn, R.D.; Lee, M.C.; Linninger, A.A.; Miesel, K.; Lu, S.N.; Stylos, L. Pressure gradients in the brain in an experimental model of hydrocephalus. Collections 2009, 116, 1069–1075. [Google Scholar]
- Sweetman, B.; Linninger, A.A. Cerebrospinal Fluid Flow Dynamics in the Central Nervous System. Ann. Biomed. Eng. 2010, 39, 484–496. [Google Scholar] [CrossRef] [PubMed]
- Zhu, D.C.; Xenos, M.; Linninger, A.A.; Penn, R.D. Dynamics of lateral ventricle and cerebrospinal fluid in normal and hydrocephalic brains. J. Magn. Reson. Imaging 2006, 24, 756–770. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.Y.; Joldes, G.R.; Wittek, A.; Miller, K. Patient-specific computational biomechanics of the brain without segmentation and meshing. Int. J. Numer. Meth. Biomed. Engng. 2013, 29, 293–308. [Google Scholar] [CrossRef]
- Alaraj, A.; Luciano, C.J.; Bailey, D.P.; Elsenousi, A.; Roitberg, B.Z.; Bernardo, A.; Banerjee, P.P.; Charbel, F.T. Virtual reality cerebral aneurysm clipping simulation with real-time haptic feedback. Neurosurgery 2015, 11, 52–58. [Google Scholar] [PubMed]
- Alaraj, A.; Charbel, F.T.; Birk, D.; Tobin, M.; Luciano, C.; Banerjee, P.P.; Rizzi, S.; Sorenson, J.; Foley, K.; Slavin, K.; et al. Role of Cranial and Spinal Virtual and Augmented Reality Simulation Using Immersive Touch Modules in Neurosurgical Training. Neurosurgery 2013, 72, 115–123. [Google Scholar] [CrossRef] [PubMed]
- Alaraj, A.; Lemole, M.G.; Finkle, J.H.; Yudkowsky, R.; Wallace, A.; Luciano, C.; Banerjee, P.P.; Rizzi, S.H.; Charbel, F.T. Virtual reality training in neurosurgery: Review of current status and future applications. Surg. Neurol. Int. 2011, 2. [Google Scholar] [CrossRef]
- Yudkowsky, R.; Luciano, C.; Banerjee, P.; Schwartz, A.; Alaraj, A.; Lemole, G.M.; Charbel, F.; Smith, K.; Rizzi, S.; Byrne, R.; et al. Practice on an Augmented Reality/Haptic Simulator and Library of Virtual Brains Improves Residents’ Ability to Perform a Ventriculostomy. Simul. Healthc. J. Soc. Simul. Healthc. 2013, 8, 25–31. [Google Scholar] [CrossRef]
- Alaraj, A.; Tobin, M.K.; Birk, D.M.; Charbel, F.T. Simulation in Neurosurgery and Neurosurgical Procedures. In The Comprehensive Textbook of Healthcare Simulation; Levine, A.I., DeMaria, S., Jr., Schwartz, A.D., Sim, A.J., Eds.; Springer: New York, NY, USA, 2013; pp. 415–423. [Google Scholar]
- Pons, J.P.; Ségonne, E.; Boissonnat, J.D.; Rineau, L.; Yvinec, M.; Keriven, R. High-quality consistent meshing of multi-label datasets. Inf. Process Med. Imaging 2007, 20, 198–210. [Google Scholar] [PubMed]
- Nowinski, W.L.; Belov, D. The Cerefy Neuroradiology Atlas: A Talairach–Tournoux atlas-based tool for analysis of neuroimages available over the internet. NeuroImage 2003, 20, 50–57. [Google Scholar] [CrossRef] [PubMed]
- Nowinski, W.L. The cerefy brain atlases. Neuroinformatics 2005, 3, 293–300. [Google Scholar] [CrossRef] [PubMed]
- Nowinski, W.L. From research to clinical practice: A Cerefy brain atlas story. Int. Congr. Ser. 2003, 1256, 75–81. [Google Scholar] [CrossRef]
- Adams, C.M.; Wilson, T.D. Virtual cerebral ventricular system: An MR-based three-dimensional computer model. Anat. Sci. Educ. 2011, 4, 340–347. [Google Scholar] [CrossRef] [PubMed]
- Dale, A.M.; Fischl, B.; Sereno, M.I. Cortical surface-based analysis. I. Segmentation and surface reconstruction. NeuroImage 1999, 9, 179–194. [Google Scholar] [CrossRef] [PubMed]
- Fischl, B.; Salat, D.H.; Busa, E.; Albert, M.; Dieterich, M.; Haselgrove, C.; van der Kouwe, A.; Killiany, R.; Kennedy, D.; Klaveness, S.; et al. Whole brain segmentation: Automated labeling of neuroanatomical structures in the human brain. Neuron 2002, 33, 341–355. [Google Scholar] [CrossRef] [PubMed]
- Fischl, B.; Liu, A.; Dale, A.M. Automated manifold surgery: Constructing geometrically accurate and topologically correct models of the human cerebral cortex. IEEE Trans. Med. Imaging 2001, 20, 70–80. [Google Scholar] [CrossRef] [PubMed]
- Fischl, B.; Salat, D.H.; van der Kouwe, A.J.W.; Makris, N.; Ségonne, F.; Quinn, B.T.; Dale, A.M. Sequence-independent segmentation of magnetic resonance images. NeuroImage 2004, 23, S69–S84. [Google Scholar] [CrossRef] [PubMed]
- Dogdas, B.; Shattuck, D.W.; Leahy, R.M. Segmentation of skull and scalp in 3-D human MRI using mathematical morphology. Hum. Brain Mapp. 2005, 26, 273–285. [Google Scholar] [CrossRef] [PubMed]
- Liao, P.; Chen, T.; Chung, P. A fast algorithm for multilevel thresholding. J. Inf. Sci. Eng. 2001, 17, 713–727. [Google Scholar]
- Otsu, N. A Threshold Selection Method from Gray-Level Histograms. IEEE Trans. Syst. Man Cybern. 1979, 9, 62–66. [Google Scholar] [CrossRef]
- Lorensen, W.E.; Cline, H.E. Marching Cubes: A High Resolution 3D Surface Construction Algorithm. In Proceedings of the 14th Annual Conference on Computer Graphics and Interactive Techniques, SIGGRAPH ’87, Anaheim, CA, USA, 27–31 July 1987; ACM: New York, NY, USA, 1987; pp. 163–169. [Google Scholar]
- Nielson, G.M.; Hamann, B. The Asymptotic Decider: Resolving the Ambiguity in Marching Cubes. In Proceedings of the 2nd Conference on Visualization ’91 (VIS ’91), San Diego, CA, USA, 22–25 October 1991; IEEE Computer Society Press: Los Alamitos, CA, USA, 1991; pp. 83–91. [Google Scholar]
- Frangi, A.F.; Niessen, W.J.; Vincken, K.L.; Viergever, M.A. Multiscale vessel enhancement filtering. In Medical Image Computing and Computer-Assisted Interventation—MICCAI’98; Lecture Notes in Computer Science; Wells, W.M., Colchester, A., Delp, S., Eds.; Springer: Berlin/Heidelberg, Germany, 1998; pp. 130–137. [Google Scholar]
- Shikata, H.; Hoffman, E.A.; Sonka, M. Automated segmentation of pulmonary vascular tree from 3D CT images. In Proceedings of the SPIE 5369, Medical Imaging 2004: Physiology, Function, and Structure from Medical Images, San Diego, CA, USA, 30 April 2004; Volume 5369, pp. 107–116.
- Erdt, M.; Raspe, M.; Suehling, M. Automatic Hepatic Vessel Segmentation Using Graphics Hardware. In Medical Imaging and Augmented Reality; Lecture Notes in Computer Science; Dohi, T., Sakuma, I., Liao, H., Eds.; Springer: Berlin/Heidelberg, Germany, 2008; pp. 403–412. [Google Scholar]
- Sato, Y.; Nakajima, S.; Shiraga, N.; Atsumi, H.; Yoshida, S.; Koller, T.; Gerig, G.; Kikinis, R. Three-dimensional multi-scale line filter for segmentation and visualization of curvilinear structures in medical images. Med. Image Anal. 1998, 2, 143–168. [Google Scholar] [CrossRef] [PubMed]
- Sethian, J.A. A fast marching level set method for monotonically advancing fronts. Proc. Natl. Acad. Sci. USA 1996, 93, 1591–1595. [Google Scholar] [CrossRef] [PubMed]
- Antiga, L.; Piccinelli, M.; Botti, L.; Ene-Iordache, B.; Remuzzi, A.; Steinman, D.A. An image-based modeling framework for patient-specific computational hemodynamics. Med. Biol. Eng. Comput. 2008, 46, 1097–1112. [Google Scholar] [CrossRef] [PubMed]
- Ghaffari, M.; Hsu, C.-Y.; Linninger, A.A. Automatic reconstruction and generation of structured hexahedral mesh for non-planar bifurcations in vascular network. Comput. Aided Chem. Eng. 2015, in press. [Google Scholar]
- Nowinski, W.L.; Thaung, T.S.L.; Chua, B.C.; Yi, S.H.W.; Ngai, V.; Yang, Y.; Chrzan, R.; Urbanik, A. Three-dimensional stereotactic atlas of the adult human skull correlated with the brain, cranial nerves, and intracranial vasculature. J. Neurosci. Methods 2015, 246, 65–74. [Google Scholar] [CrossRef] [PubMed]
- Ito, H.; Kanno, I.; Iida, H.; Hatazawa, J.; Shimosegawa, E.; Tamura, H.; Okudera, T. Arterial fraction of cerebral blood volume in humans measured by positron emission tomography. Ann. Nucl. Med. 2001, 15, 111–116. [Google Scholar] [CrossRef] [PubMed]
- Lauwers, F.; Cassot, F.; Lauwers-Cances, V.; Puwanarajah, P.; Duvernoy, H. Morphometry of the human cerebral cortex microcirculation: General characteristics and space-related profiles. NeuroImage 2008, 39, 936–948. [Google Scholar] [CrossRef] [PubMed]
- Risser, L.; Plouraboué, F.; Cloetens, P.; Fonta, C. A 3D-investigation shows that angiogenesis in primate cerebral cortex mainly occurs at capillary level. Int. J. Dev. Neurosci. 2009, 27, 185–196. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reichold, J.; Stampanoni, M.; Keller, A.L.; Buck, A.; Jenny, P.; Weber, B. Vascular graph model to simulate the cerebral blood flow in realistic vascular networks. J. Cereb. Blood Flow Metab. 2009, 29, 1429–1443. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lüders, E.; Steinmetz, H.; Jäncke, L. Brain size and grey matter volume in the healthy human brain. Neuroreport 2002, 13, 2371–2374. [Google Scholar] [CrossRef] [PubMed]
- Grant, R.; Condon, B.; Lawrence, A.; Hadley, D.M.; Patterson, J.; Bone, I.; Teasdale, G.M. Human cranial CSF volumes measured by MRI: Sex and age influences. Magn. Reson. Imaging 1987, 5, 465–468. [Google Scholar] [CrossRef] [PubMed]
- Borouchaki, H.; Laug, P.; George, P.-L. Parametric surface meshing using a combined advancing-front generalized Delaunay approach. Int. J. Numer. Methods Eng. 2000, 49, 233–259. [Google Scholar] [CrossRef]
- Meegama, R.G.N.; Rajapakse, J.C. NURBS-Based Segmentation of the Brain in Medical Images. Int. J. Pattern Recognit. Artif. Intell. 2003, 17, 995–1009. [Google Scholar] [CrossRef]
- Zhu, D.; Li, K.; Guo, L.; Liu, T. Bezier Control Points image: A novel shape representation approach for medical imaging. In Proceedings of the 2009 Conference Record of the Forty-Third Asilomar Conference on Signals, Systems and Computers, Pacific Grove, CA, USA, 1–4 November 2009; pp. 1094–1098.
- Lim, S.P.; Haron, H. Surface reconstruction techniques: A review. Artif. Intell. Rev. 2012, 42, 59–78. [Google Scholar] [CrossRef]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hsu, C.-Y.; Schneller, B.; Ghaffari, M.; Alaraj, A.; Linninger, A. Medical Image Processing for Fully Integrated Subject Specific Whole Brain Mesh Generation. Technologies 2015, 3, 126-141. https://0-doi-org.brum.beds.ac.uk/10.3390/technologies3020126
Hsu C-Y, Schneller B, Ghaffari M, Alaraj A, Linninger A. Medical Image Processing for Fully Integrated Subject Specific Whole Brain Mesh Generation. Technologies. 2015; 3(2):126-141. https://0-doi-org.brum.beds.ac.uk/10.3390/technologies3020126
Chicago/Turabian StyleHsu, Chih-Yang, Ben Schneller, Mahsa Ghaffari, Ali Alaraj, and Andreas Linninger. 2015. "Medical Image Processing for Fully Integrated Subject Specific Whole Brain Mesh Generation" Technologies 3, no. 2: 126-141. https://0-doi-org.brum.beds.ac.uk/10.3390/technologies3020126