Wearable Inertial Sensing for ICT Management of Fall Detection, Fall Prevention, and Assessment in Elderly



Abstract
:1. Introduction
2. Materials and Methods
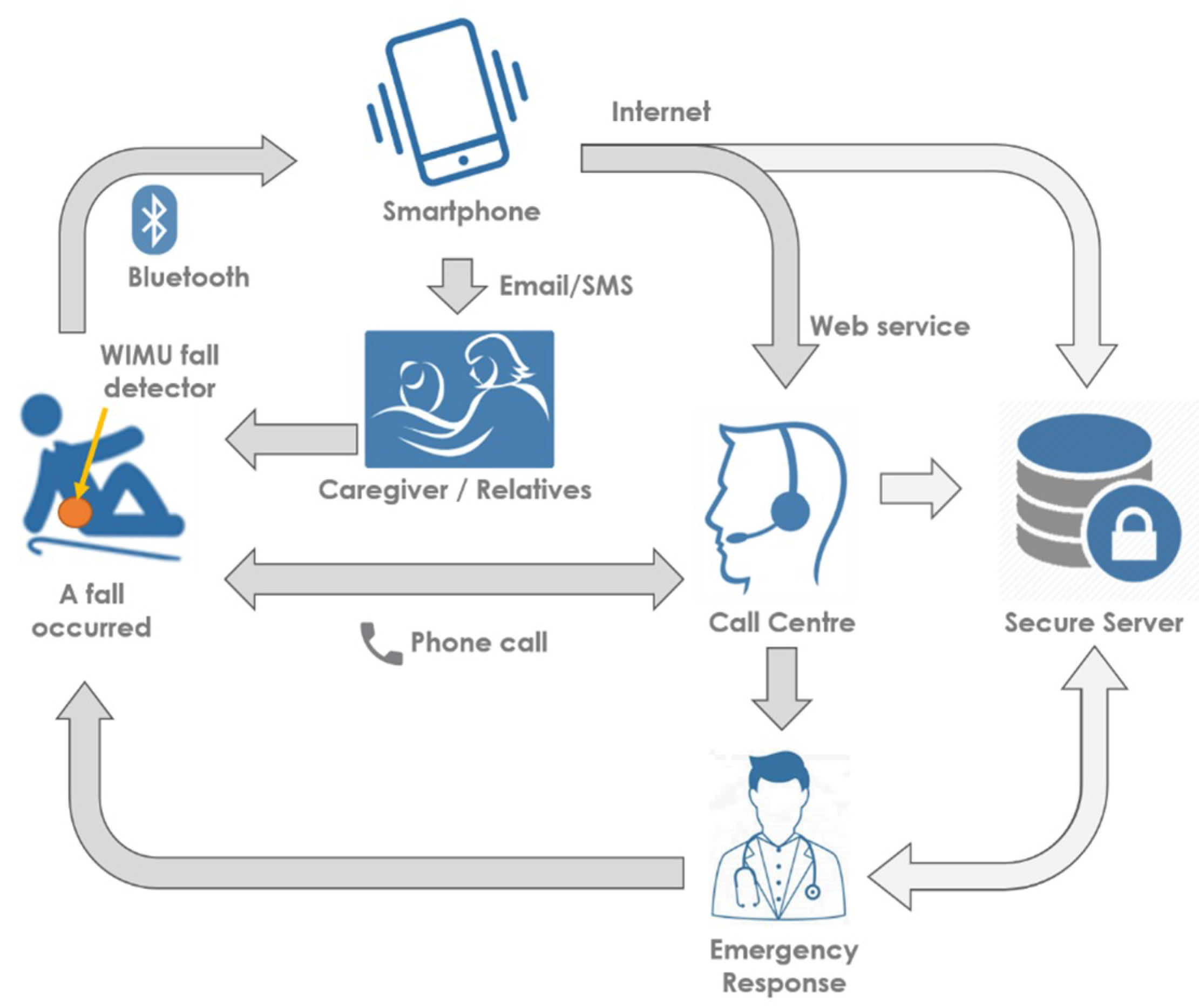
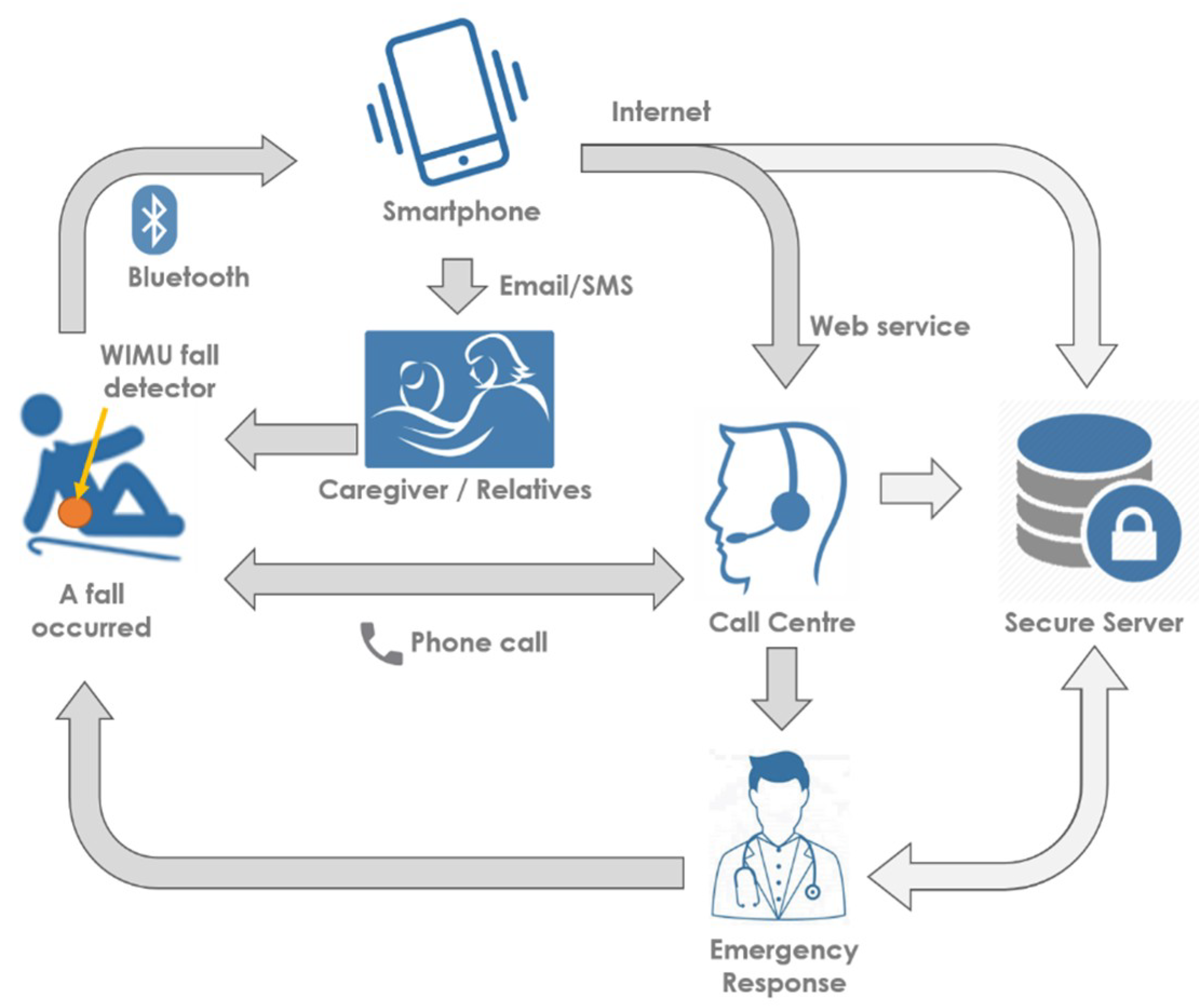
2.1. The Overall ICT Solution
- access to HTML/Java streams that allow interactive, top-down browsing of patient data, using a unique, time-limited URL;
- access to PDF format summary reports of the patient data covering a specified period of time, normally 28-day blocks;
- subscription to specific types of low-level physiological data and interventions that have been recorded for or by the patient within the system.
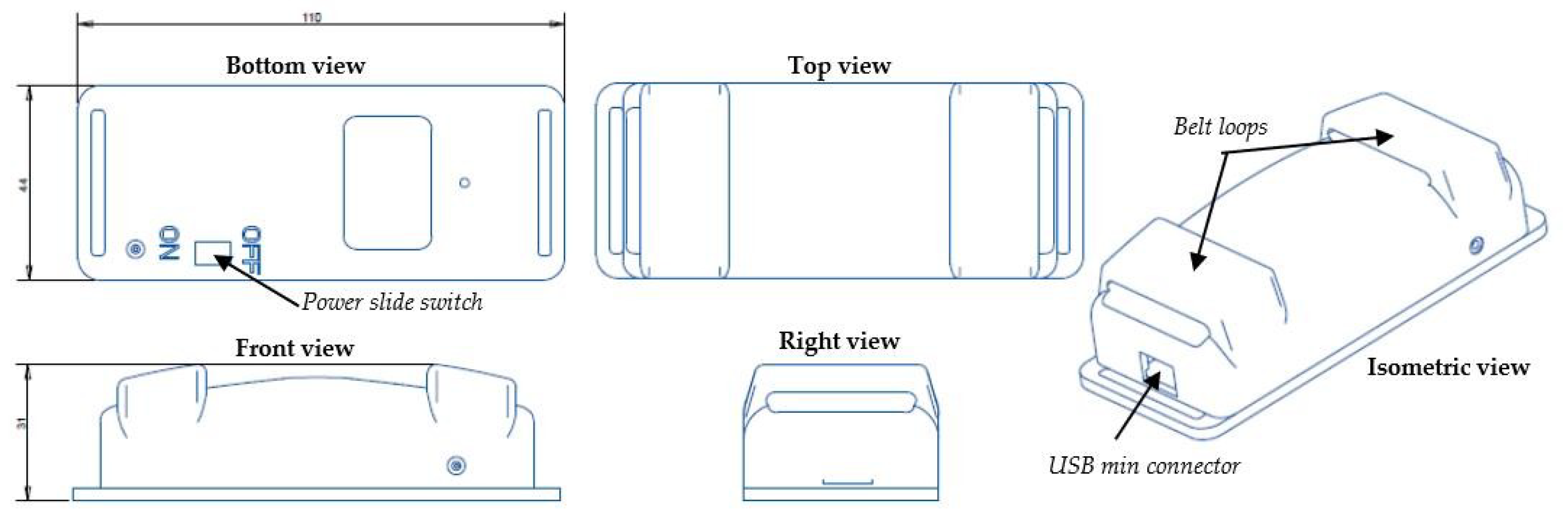
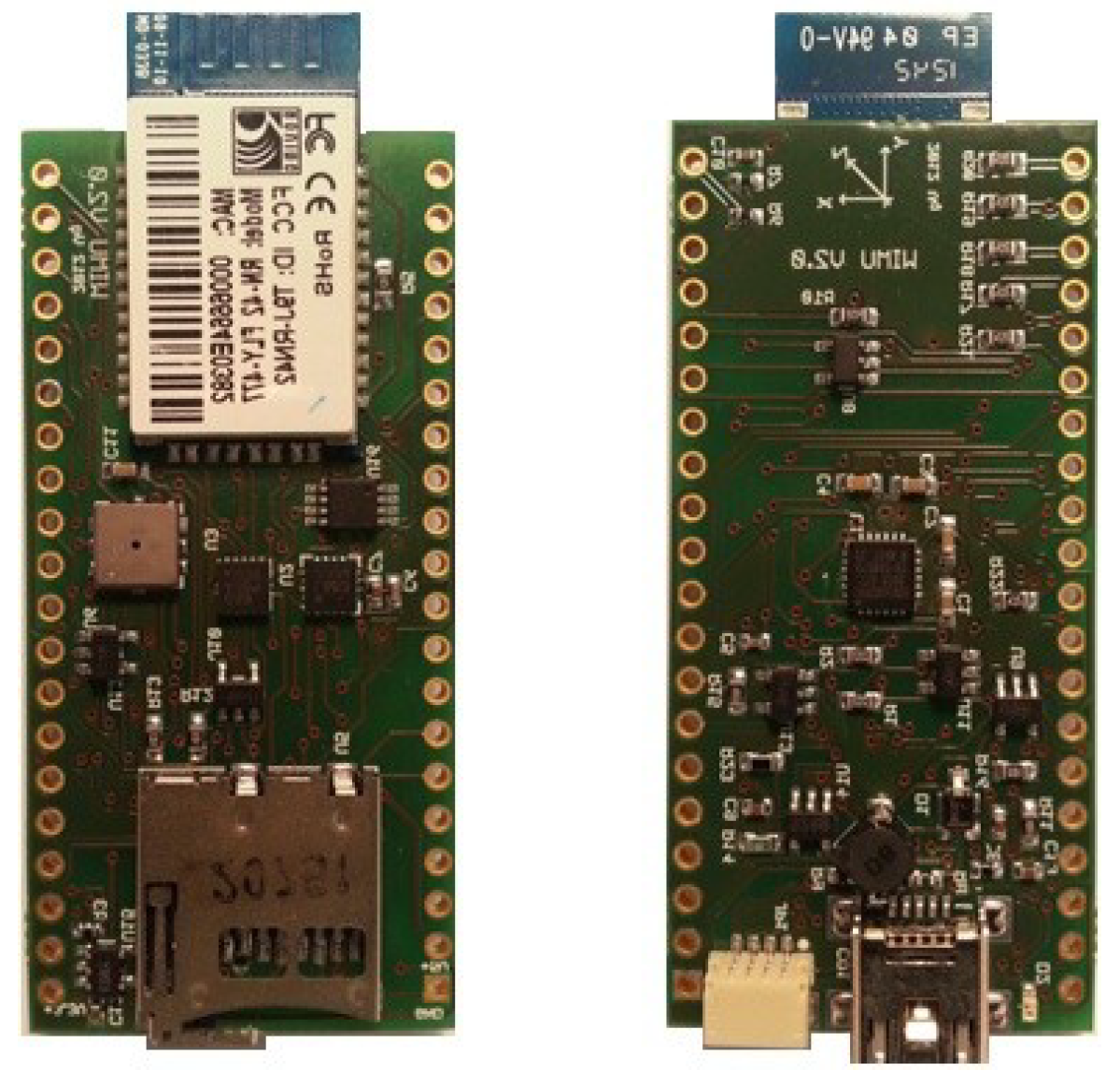
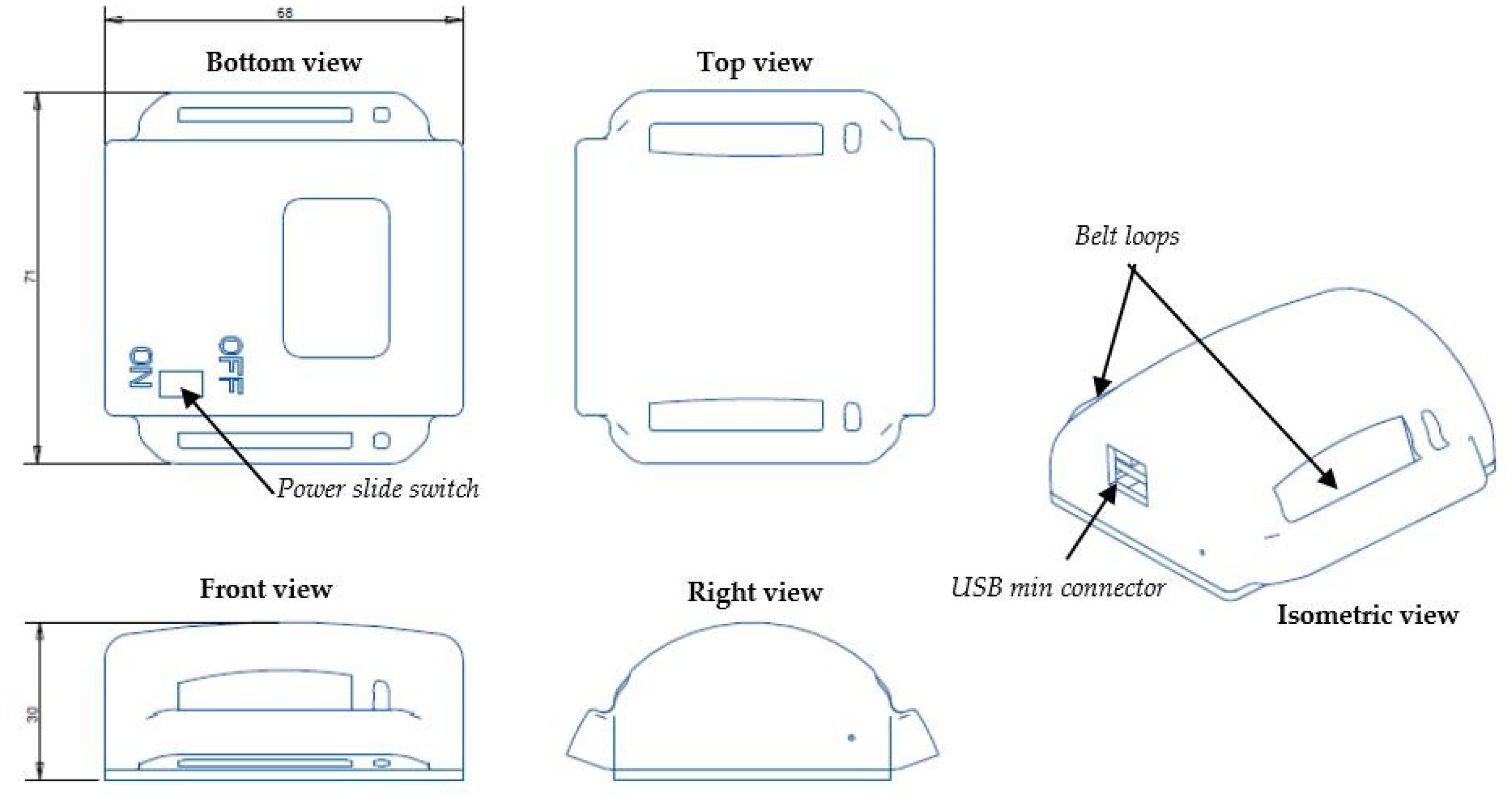
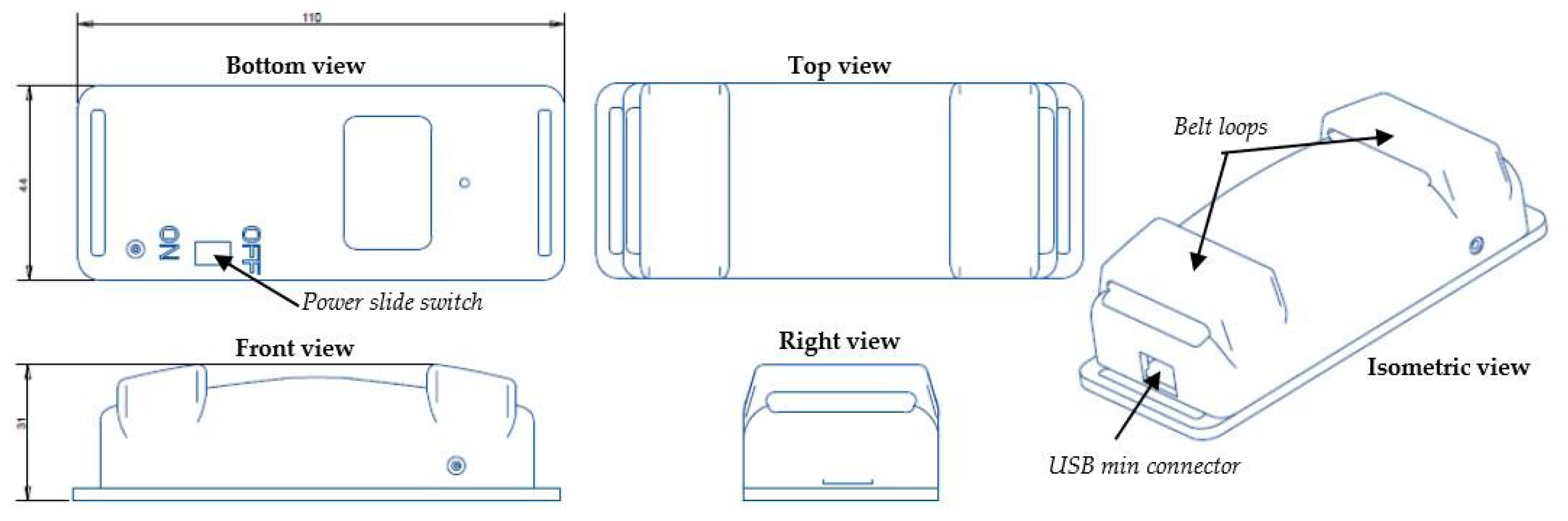
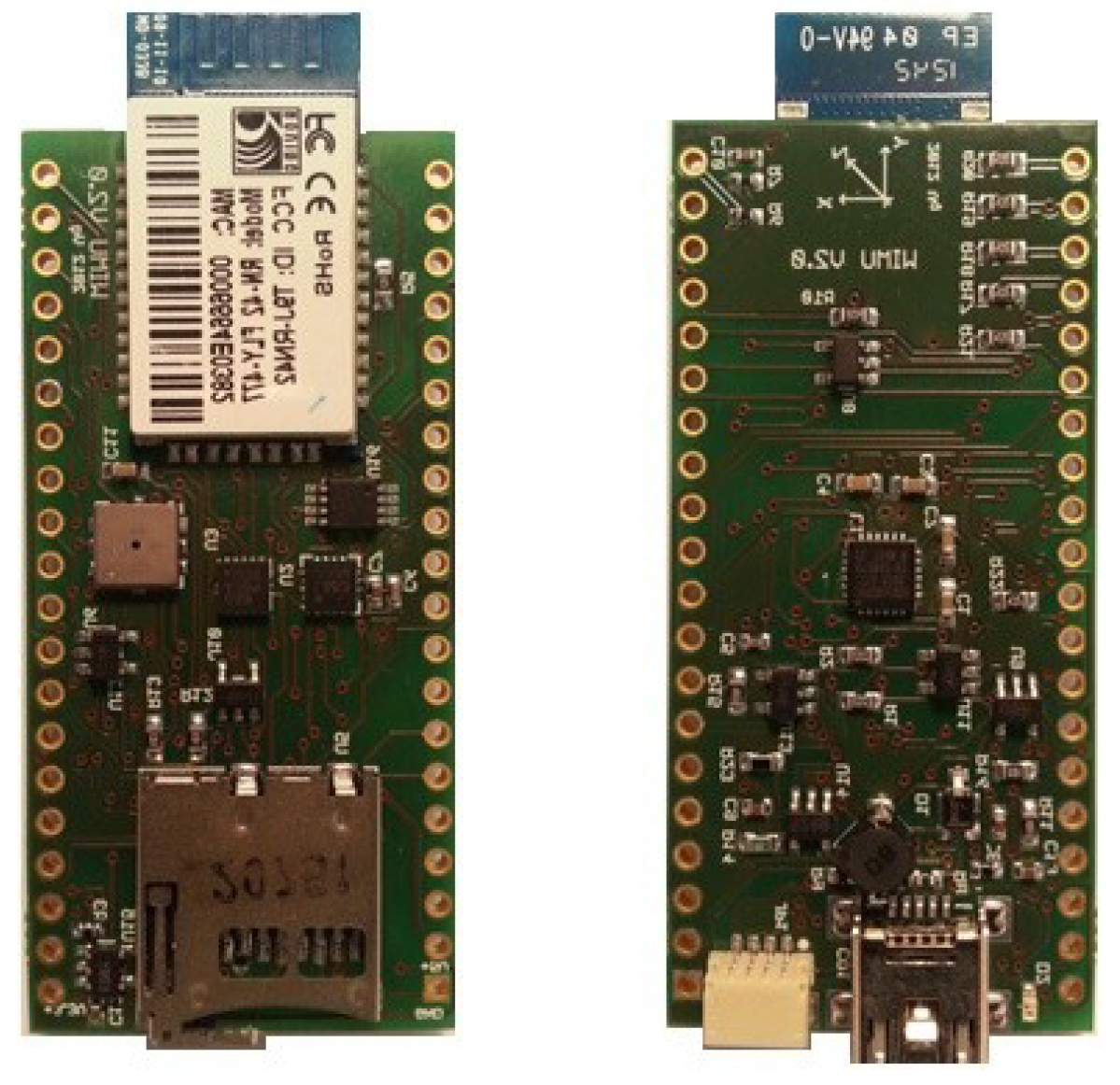
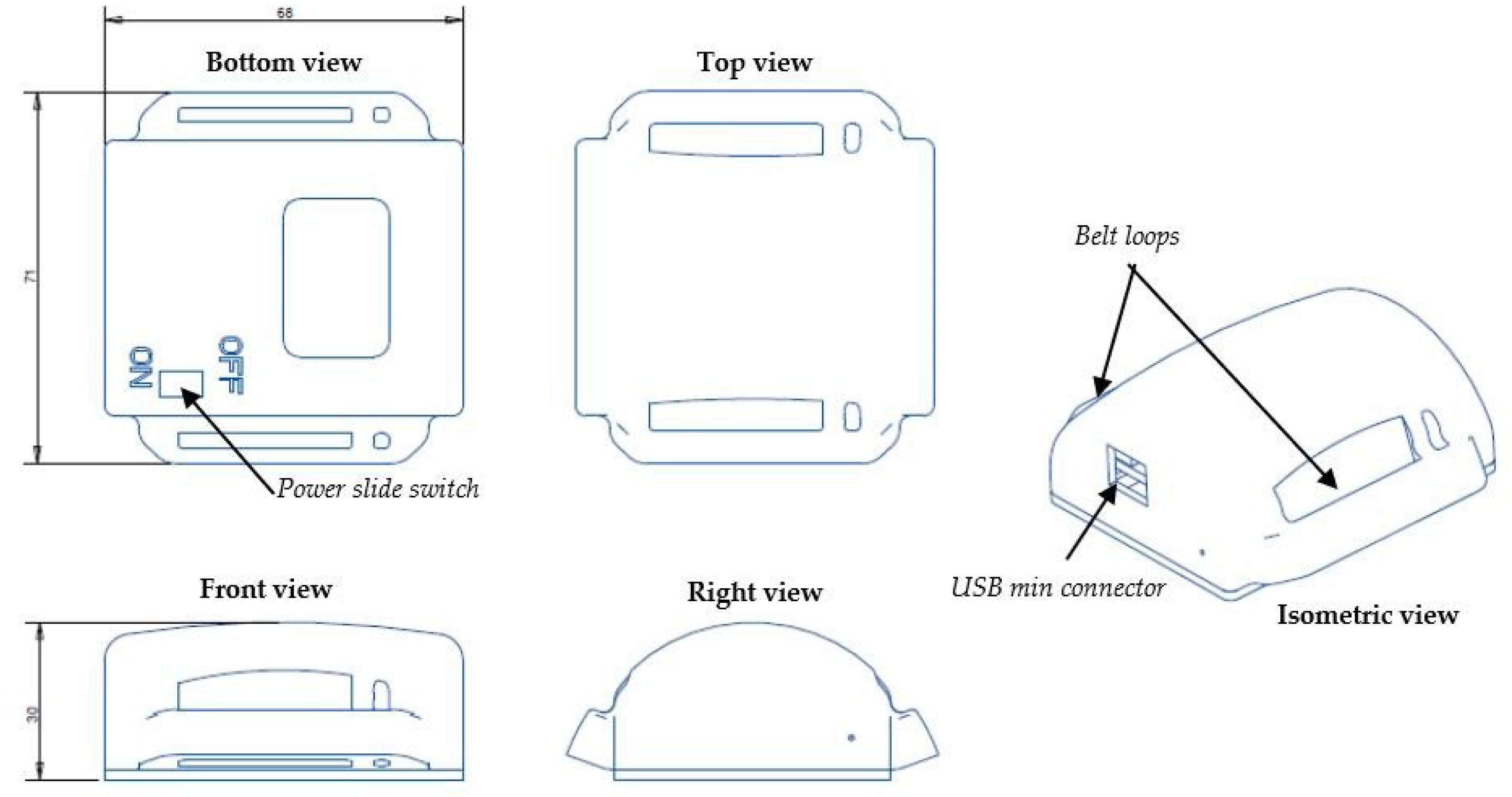
2.2. The Hardware
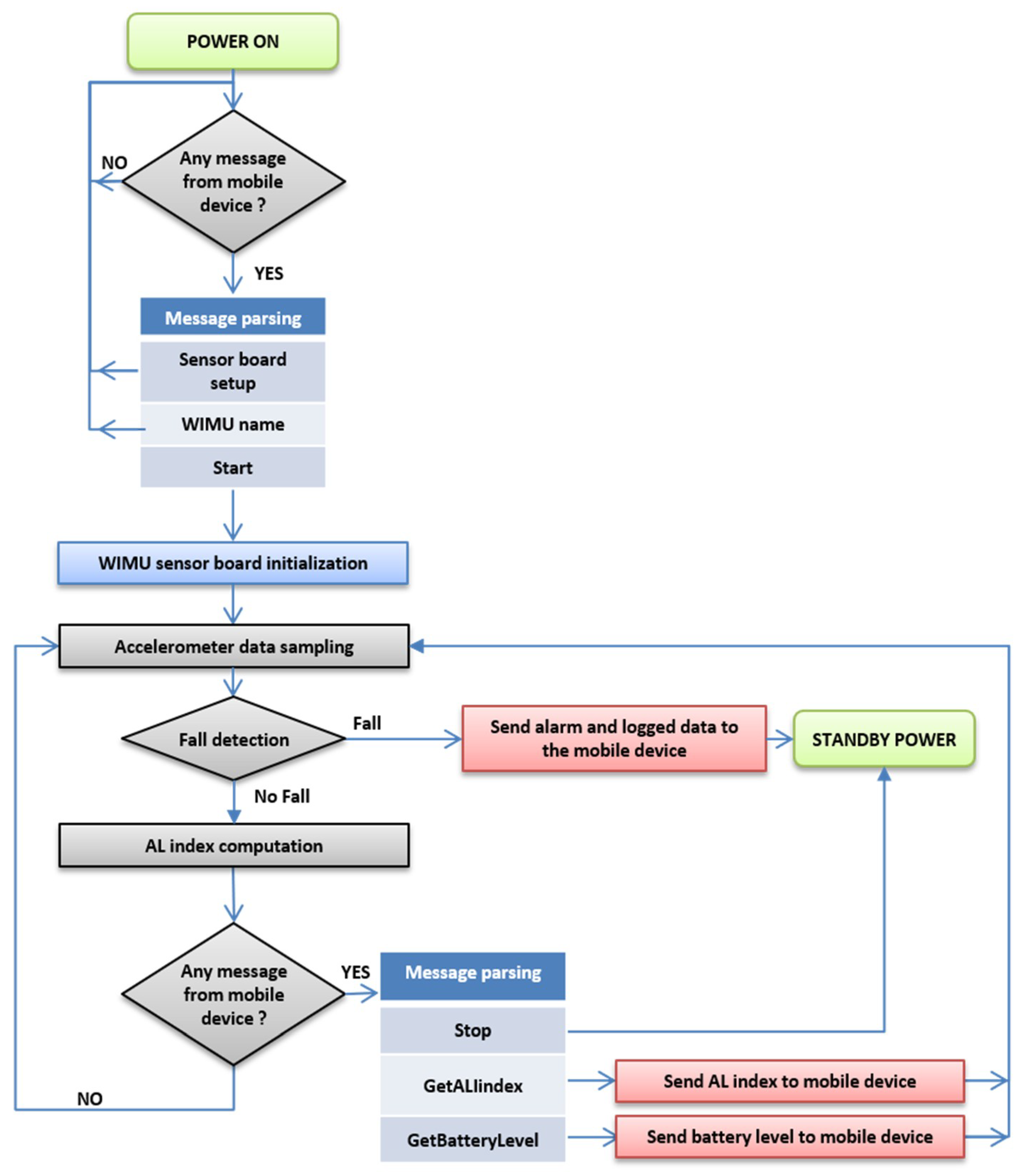
2.3. The Fall Detector: Functionalities
- automatic fall detection—a built-in algorithm of fall detection identifies impacts that may be related to falls, generates and displays alarms, and sends them to the Android device using BT connectivity;
- automatic logging (and subsequent transfer to the Android device)—acceleration data occurring in a time window around the fall event are stored; this is a useful feature to keep track of fall events and use the logged data for post-hoc processing, e.g., further refinement and tuning of the built-in fall detection algorithm;
- parsing and managing of a list of commands coming from the mobile device to change the parameters of the algorithms, obtain battery information, and troubleshoot possible device errors.
- estimation of the activity level (AL)—the built-in algorithm of AL estimation helps keep track of the intensity of the physical activity of the patient during the day.
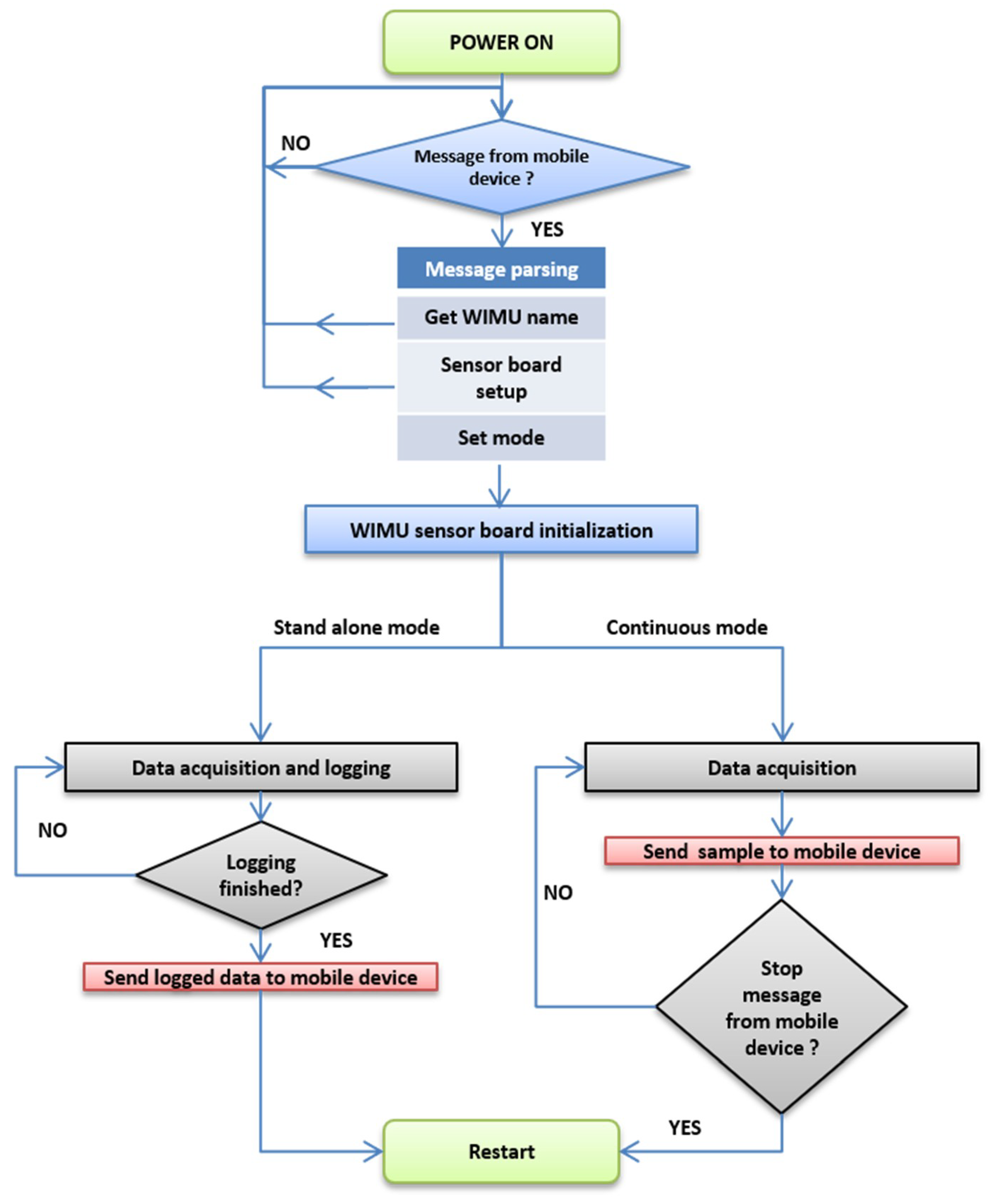
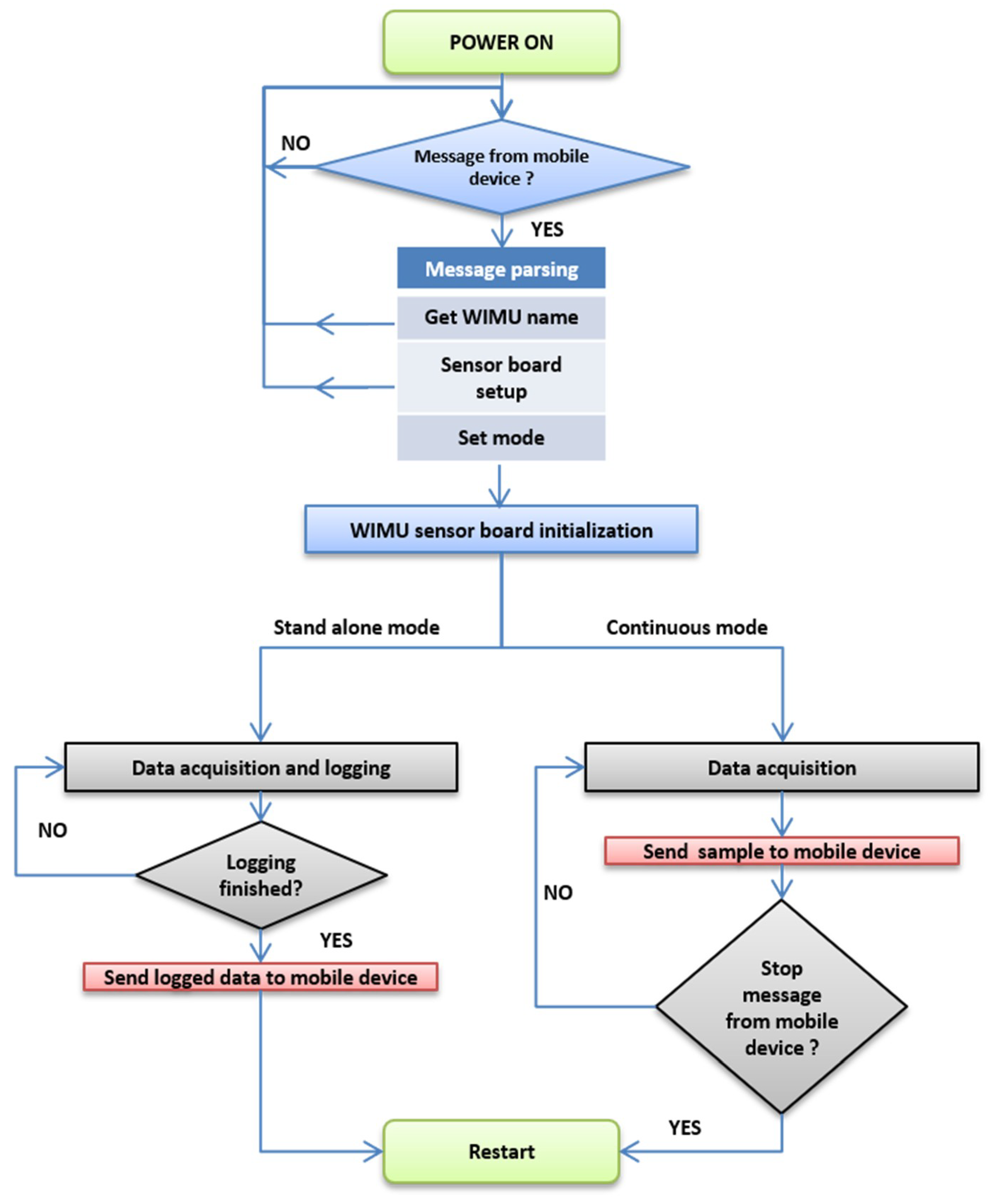
2.4. The Data Logger: Functionalities
- standalone mode—the data are stored in the internal memory of the device, which is capable of storing records lasting six minutes;
- continuous mode—the data are transferred sample-by-sample to the Android mobile device; the maximum duration of a data record will depend on the battery duration (about four hours) of the wearable device. Considering the sampling rate (100 Hz) and a sensory data frame length of 38 bytes, the max data length collected in four hours is about 60 MB.
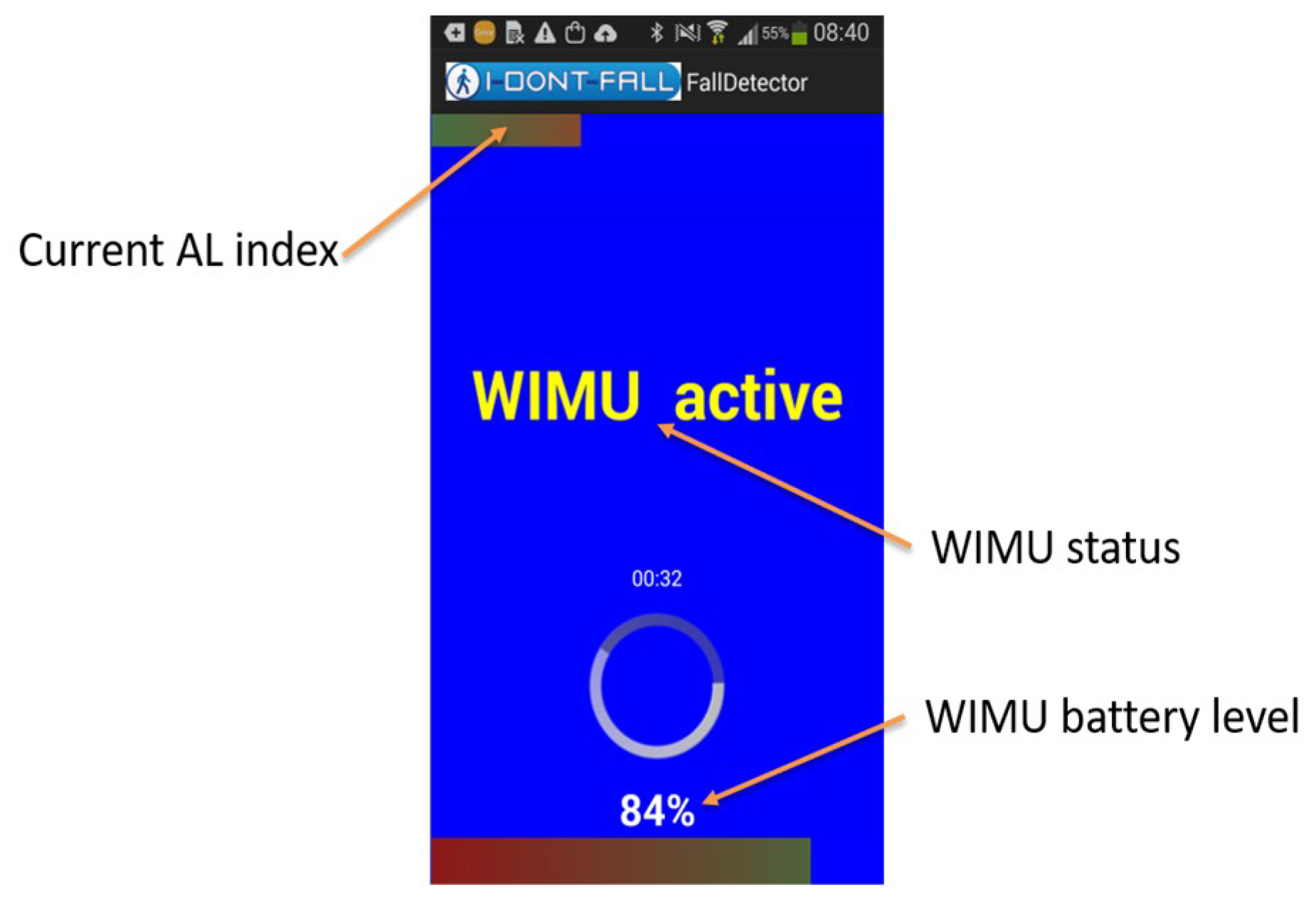
2.5. The Android Mobile Device
- periodic check of the connection with WIMU;
- periodic check of the connection with the call-center;
- acquisition of the ADL index and WIMU’s battery level;
- alarm management;
- propagate the alarm to different recipients (see Table 2);
- upload of acceleration data logged by the WIMU in a time window around the fall event.
- the selection of standalone mode (the logging duration can be specified) or continuous mode;
- acquisition of the WIMU battery level;
- acquisition of the data collected by the WIMU (at the end of the experiment for the standalone mode, sample-by-sample in continuous mode);
- calculation and displaying of the Fast Fourier Transform (FFT) of the data acquired by the WIMU during a diagnostic test data acquisition. This tool is useful to let the user periodically check the correct functionality of the instrument.
2.6. Instrumentation of the Six-Minutes Walking Test
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Bergen, G.; Stevens, M.R.; Burns, E.R. Falls and fall injuries among adults aged ≥ 65 years—United States 2014. MMWR Morb Mortal Wkly Rep 2016, 65, 993–998. [Google Scholar] [CrossRef] [PubMed]
- Fasano, A.; Plotnik, M.; Bove, F.; Berardelli, A. The neurobiology of falls. Neurol. Sci. 2012, 33, 1215–1223. [Google Scholar] [CrossRef] [PubMed]
- Friedman, S.M.; Munoz, B.; West, S.K.; Rubin, G.S.; Fried, L.P. Falls and fear of falling: Which comes first? A longitudinal prediction model suggests strategies for primary and secondary prevention. J. Am. Geriatr. Soc. 2002, 50, 1329–1335. [Google Scholar] [CrossRef] [PubMed]
- Lannin, N.A.; Clemenson, L.; McCluskey, A.; Lin, C.-W.C.; Cameron, I.D.; Barras, S. Feasibility and results of randomised pilot-study of pre-discharge occupational therapy home visits. BMC Health Serv. Res. 2007, 7, 42. [Google Scholar] [CrossRef] [PubMed]
- Kraskowsky, L.H.; Finlayson, M. Factors affecting older adults’ use of adaptive equipment: Review of the literature. Am. J. Occup. Ther. 2001, 55, 303–310. [Google Scholar] [CrossRef] [PubMed]
- Hammond, A. What is the role of the occupational therapist? Best Pract. Res. Clin. Rheumatol. 2004, 18, 491–505. [Google Scholar] [CrossRef] [PubMed]
- Ambrose, A.F.; Paul, G.; Hausdorff, J.M. Risk factors for falls among older adults: A review of the literature. Maturitas 2013, 75, 51–61. [Google Scholar] [CrossRef] [PubMed]
- Cummings, S.R.; Nevitt, M.C.; Kidd, S. Forgetting falls: The limited accuracy of recall of falls in the elderly. J. Am. Geriatr. Soc. 1988, 36, 613–616. [Google Scholar] [CrossRef]
- Menz, H.B.; Lord, S.R.; Fitzpatrick, R.C. Acceleration patterns of the head and pelvis when walking on level and irregular surfaces. Gait Posture 2003, 18, 35–46. [Google Scholar] [CrossRef]
- Moe-Nillsen, R.; Aaslund, M.C.; Hodt-Billington, C.; Helbostad, J.L. Gait variability measures may represent different constructs. Gait Posture 2010, 32, 98–101. [Google Scholar] [CrossRef] [PubMed]
- Silva, P.A.; Nunes, F.; Vasconcelos, A.; Kerwin, M.; Moutinho, R.; Teixeira, P. Using the smartphone accelerometer to monitor fall risk while playing a game: The design and usability evaluation of dance! Don’t fall. In Foundations of Augmented Cognition; Springer: Berlin, Germany, 2013; pp. 754–763. [Google Scholar]
- Garcia, J.A.; Pisan, Y.; Tan, T.C.; Navarro, K.F. Assessing the Kinect’s capabilities to perform a time-based clinical test for fall risk assessment in older people. In Entertainment Computing–ICEC 2014; Springer: Berlin, Germany, 2014; pp. 100–107. [Google Scholar]
- Taylor, M.J.; Shawis, T.; Impson, R.; Ewins, K.; McCormick, D.; Griffin, M. Nintendo Wii as a training tool in falls prevention rehabilitation: Case studies. J. Am. Geriatr. Soc. 2012, 60, 1781–1783. [Google Scholar] [CrossRef] [PubMed]
- Williams, M.A.; Soiza, R.L.; Jenkinson, A.M.; Stewart, A. Exercising with Computers in Later Life (EXCELL)-pilot and feasibility study of the acceptability of the Nintendo WiiFit in community-dwelling fallers. BMC Res. Notes 2010, 3, 238. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abbate, S.; Avvenuti, M.; Bonatesta, F.; Cola, G.; Corsini, P.; Vecchio, A. A smartphone-based fall detection system. Pervasive Mob. Comput. 2012, 8, 883–899. [Google Scholar] [CrossRef]
- Yu, M.; Rhuma, A.; Naqvi, S.M.; Wang, L.; Chambers, J. A posture recognition-based fall detection system for monitoring an elderly person in a smart home environment. IEEE Trans. Inform. Technol. Biomed. 2012, 16, 1274–1286. [Google Scholar]
- Fortino, G.; Gravina, R. Fall-MobileGuard: A smart real-time fall detection system. In Proceedings of the 10th EAI International Conference on Body Area Networks, Sydney, Australia, 28–30 September 2015; pp. 44–50. [Google Scholar]
- Chen, J.; Kwong, K.; Chang, D.; Luk, J.; Bajcsy, R. Wearable sensors for reliable fall detection. In Proceedings of the 2005 IEEE Engineering in Medicine and Biology 27th Annual Conference, Shanghai, China, 17–18 January 2006; pp. 3551–3554. [Google Scholar]
- Doughty, K.; Lews, R.; Mcintosh, A. The design of practical and reliable fall detector for community and institutional telecare. J. Telemed. Telecare 2000, 6, 150–154. [Google Scholar] [CrossRef]
- Bianchi, F.; Redmond, S.J.; Narayanan, M.R.; Cerutti, S.; Lovell, N.H. Barometric pressure and triaxial accelerometry-based falls event detection. IEEE Trans. Neural Syst. Rehabil. Eng. 2010, 18, 619–627. [Google Scholar] [CrossRef] [PubMed]
- Wu, G.; Xue, S. Portable preimpact fall detector with inertial sensor. IEEE Trans. Neural Syst. Rehabil. Eng. 2008, 16, 178–183. [Google Scholar] [PubMed]
- Hamm, J.; Money, A.G.; Atwal, A.; Paraskevopoulos, I. Fall prevention intervention technologies: A conceptual framework and survey of the state of the art. J Biomech Inform. 2016, 59, 319–345. [Google Scholar] [CrossRef] [PubMed]
- Sabatini, A.M.; Ligorio, G.; Mannini, A.; Genovese, V.; Pinna, L. Prior-to-and post-impact fall detection using inertial and barometric altimeter measurements. IEEE Trans. Neural Syst. Rehabil. Eng. 2016, 24, 774–783. [Google Scholar] [CrossRef] [PubMed]
- Bair, W.; Prettyman, M.G.; Beamer, B.A.; Rogers, M.W. Kinematic and behavioral analyses of protective stepping strategies and risk for falls among community living older adults. Clin. Biomech. 2016, 36, 74–82. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zijlstra, W.; Hof, A.L. Assessment of spatio-temporal gait parameters from trunk accelerations during human walking. Gait Posture 2003, 18, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Taylor, M.E.; Delbaere, K.; Mikolaizak, A.S.; Lord, S.R.; Close, J.C.T. Gait parameter risk factors for falls under simple and dual task conditions in cognitively impaired older people. Gait Posture 2013, 37, 126–130. [Google Scholar] [CrossRef] [PubMed]
- Gillain, S.; Boutaayamou, M.; Beaudart, C.; Demonceau, M.; Bruyère, O.; Reginster, J.Y.; Garraux, G.; Petermans, J. Assessing gait parameters with accelerometer-based methods to identify older adults at risk of falls: A systematic review. Eur. Geriatr. Med. 2018, 9, 435–448. [Google Scholar] [CrossRef]
- Hausdorff, J.M.; Eldelberg, H.K.; Mitchell, S.L.; Goldberger, A.L.; Wei, J.Y. Increased gait unsteadiness in community-dwelling elderly fallers. Arch. Phys. Med. Rehab. 1997, 78, 278–283. [Google Scholar] [CrossRef]
- IDONTFALL Project. Available online: http://www.idontfall.eu/ (accessed on 29 September 2018).
- Genovese, V.; Mannini, A.; Sabatini, A.M. IDONTFALL Deliverable D3.1: Detailed Technical Specification of Fall Detection and Prevention Services. 2012. Available online: http://www.idontfall.eu/sites/default/files/deliverables (accessed on 29 September 2018).
- Barban, F.; Annicchiarico, R.; Melideo, M.; Federici, A.; Lombardi, M.G.; Giuli, S.; Ricci, C.; Adriano, F.; Griffini, I.; Silvestri, F.; et al. Reducing fall risk with combined motor and cognitive training in elderly fallers. Brain Sci. 2017, 7, 19. [Google Scholar] [CrossRef] [PubMed]
- Bourke, A.K.; O’Donovan, K.J.; O’Laighin, G. The identification of vertical velocity profiles using an inertial sensor to investigate pre-impact detection of falls. Med. Eng. Phys. 2008, 30, 937–946. [Google Scholar] [CrossRef] [PubMed]
- Bellanca, J.L.; Lowry, K.A.; VanSwearingen, J.M.; Brach, J.S.; Redfern, M.S. Harmonic ratios: A quantification of step to step symmetry. J. Biomech. 2013, 46, 828–831. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Menz, H.B.; Lord, S.R.; Fitzpatrick, R.C. Acceleration patterns of the head and pelvis when walking are associated with risk of falling in community-dwelling older people. J. Gerontol. (Series A: Biol Sci Med Sci) 2003, 58, M446–M452. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Device | Low Pass Filter Cut Off Frequency (Hz) | Sensing Range | Sensitivity-Resolution |
|---|---|---|---|
| Accelerometer | 1200 | ±4 g (1 g = 9.81 m/s2) | 0.000488 g/LSB |
| Gyroscope | 256 | ± 2000 °/s | 0.0696 (°/s)/LSB |
| Magnetometer | ± 0.88 Gauss | 0.00729 Gauss/LSB | |
| Pressure sensor | +9000 m, ..., 500 m above the sea level | 0.01 hPa |
| Internet | Telephone Network | |||
|---|---|---|---|---|
| Alarm Recipient | Web Service | SMS | Pre-Recorded Phone Calls | |
| Call centre | ✓ | |||
| Family and friends | ✓ | ✓ | ✓ | |
| Patient Fall-Risk Level | ||
|---|---|---|
| Low-Risk | High-Risk | |
| Walked distance (D), m | 281 ± 100 | 183 ± 58 *** |
| Cadence, spm | 103 ± 13 | 90 ± 15 *** |
| Stride time (Tstride), s | 1.19 ± 0.18 | 1.37 ± 0.23 ** |
| Stride time variability (COV), % | 6.7 ± 3.1 | 8.5 ± 3.9 |
| RMS (vertical acceleration), m/s2 | 1.68 ± 0.59 | 1.05 ± 0.41 *** |
| HRML | 1.66 ± 0.36 | 1.70 ± 0.42 |
| HRVT | 1.93 ± 0.67 | 1.65 ± 0.56 |
| HRAP | 1.69 ± 0.64 | 1.46 ± 0.38 |
| D | Tstride | COV | RMS | HRML | HRVT | HRAP | |
|---|---|---|---|---|---|---|---|
| D | 1.00 | ||||||
| Tstride | −0.28 | 1.00 | |||||
| COV | 0.56 ** | 0.21 | 1.00 | ||||
| RMS | 0.73 ** | −0.32 | −0.59 ** | 1.00 | |||
| HRML | −0.10 | −0.55 ** | −0.13 | −0.021 | 1.00 | ||
| HRVT | 0.48 * | −0.28 | −0.63 ** | 0.70 ** | 0.27 | 1.00 | |
| HRAP | 0.42 * | −0.27 | −0.59 ** | 0.64 ** | 0.35 | 0.88 ** | 1.00 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Genovese, V.; Mannini, A.; Guaitolini, M.; Sabatini, A.M. Wearable Inertial Sensing for ICT Management of Fall Detection, Fall Prevention, and Assessment in Elderly. Technologies 2018, 6, 91. https://0-doi-org.brum.beds.ac.uk/10.3390/technologies6040091
Genovese V, Mannini A, Guaitolini M, Sabatini AM. Wearable Inertial Sensing for ICT Management of Fall Detection, Fall Prevention, and Assessment in Elderly. Technologies. 2018; 6(4):91. https://0-doi-org.brum.beds.ac.uk/10.3390/technologies6040091
Chicago/Turabian StyleGenovese, Vincenzo, Andrea Mannini, Michelangelo Guaitolini, and Angelo Maria Sabatini. 2018. "Wearable Inertial Sensing for ICT Management of Fall Detection, Fall Prevention, and Assessment in Elderly" Technologies 6, no. 4: 91. https://0-doi-org.brum.beds.ac.uk/10.3390/technologies6040091