The Requirements for New Tools for Use by Pilots and the Aviation Industry to Manage Risks Pertaining to Work-Related Stress (WRS) and Wellbeing, and the Ensuing Impact on Performance and Safety



Abstract
:1. Introduction
1.1. Introduction to the Problem
1.2. Theoretical Background
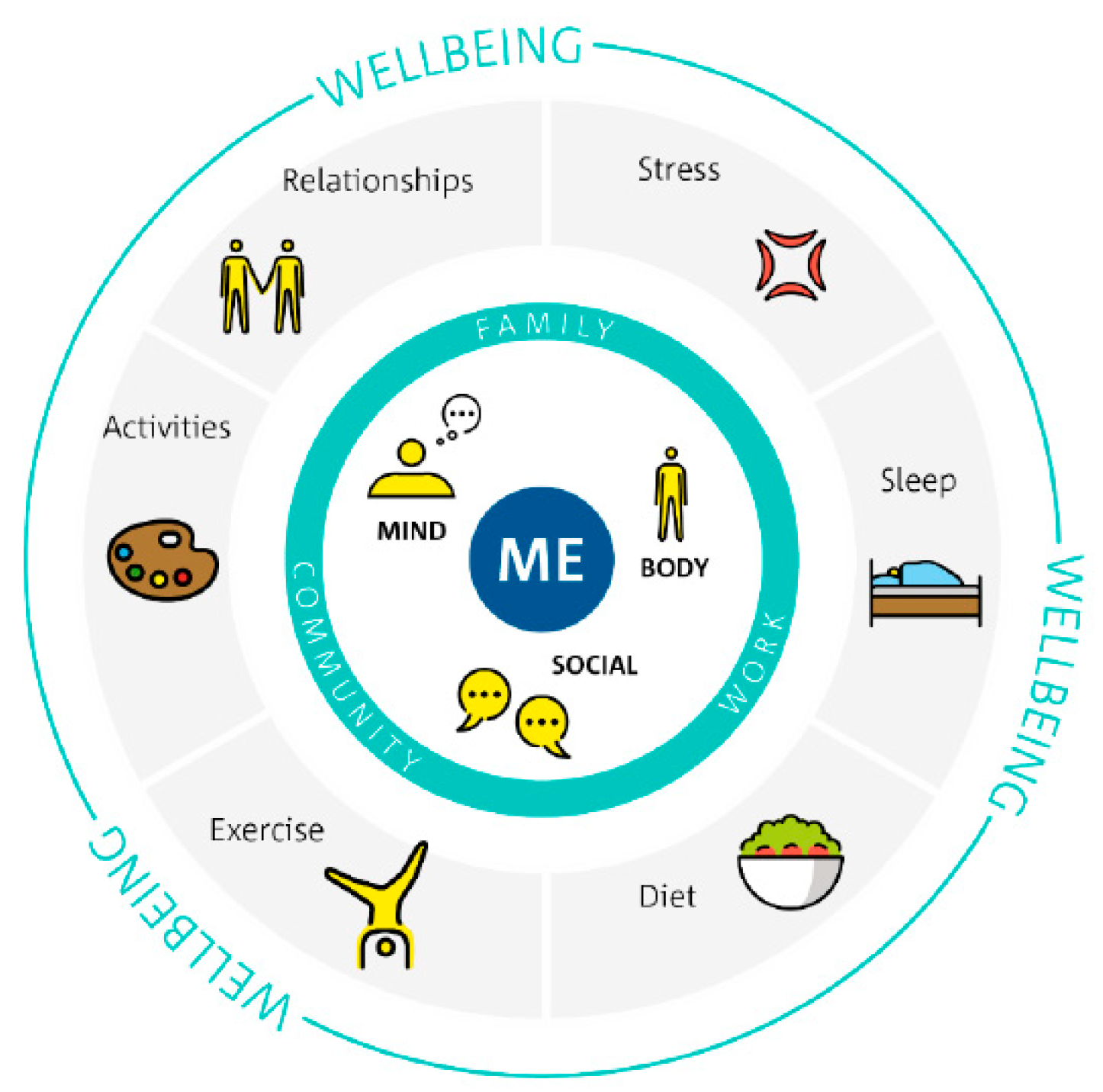
1.2.1. Wellbeing
1.2.2. Stress and Work-Related Stress (WRS)
1.2.3. Work-Related Stress (WRS)
1.2.4. Stress Coping Styles and Strategies
1.2.5. Mental Health
1.2.6. Management of Mental Health Problems
1.2.7. Mental Wellbeing at Work
1.2.8. Stress and Wellbeing Management in the Workplace
1.2.9. Resilience and Self-Efficacy
1.3. Pilot: Stress, Sources of Stress and Stress Coping
1.3.1. Types and Sources of Stress
1.3.2. Impact of Stress
1.3.3. Pilot Stress Coping Styles
1.3.4. Pilot Coping Factors and Stress Coping Strategies
1.4. Pilot Wellbeing and Mental Health
1.5. Safety Management Systems, Performance Monitoring, and Safety-II
1.6. Existing Tools and Interventions to Support Pilot Wellness and Stress Management
1.7. Self Monitoring, Wearables, and Health Apps
1.8. The Quantified Self at Work
1.9. Data Protection
1.10. COVID-19 Crisis and Pilot Wellbeing
2. Materials and Methods
2.1. Methodological Framework
2.2. Research Overview
- Promoting an understanding of pilot lived experience and the allied wellbeing/performance/safety problems from a systems perspective
- Advancing a behavior model supporting the conceptualization of the problem, its impact, and the solution challenge
- Identifying the requirements for solutions at different levels (i.e., pilots, airlines, and other aviation stakeholders)
2.3. Part 1
2.4. Part 2
2.5. Part 3
2.6. Part 4
2.7. Part 5
3. Results
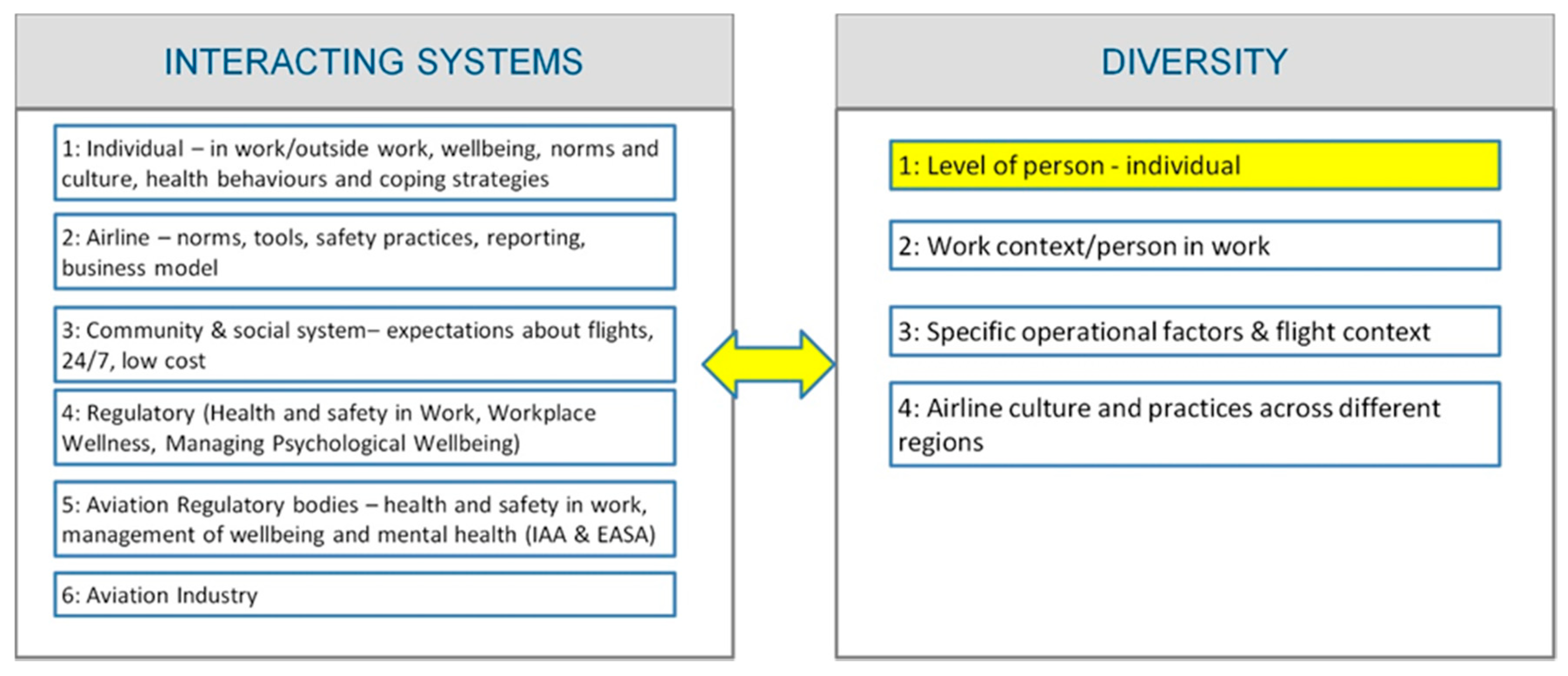
3.1. Understanding the Problem
- Pilot level (lived experience, practices/behavior, culture)
- Airline level
- Community level (i.e., social system)
- Health and safety regulation
- Aviation regulation
- Broader aviation system
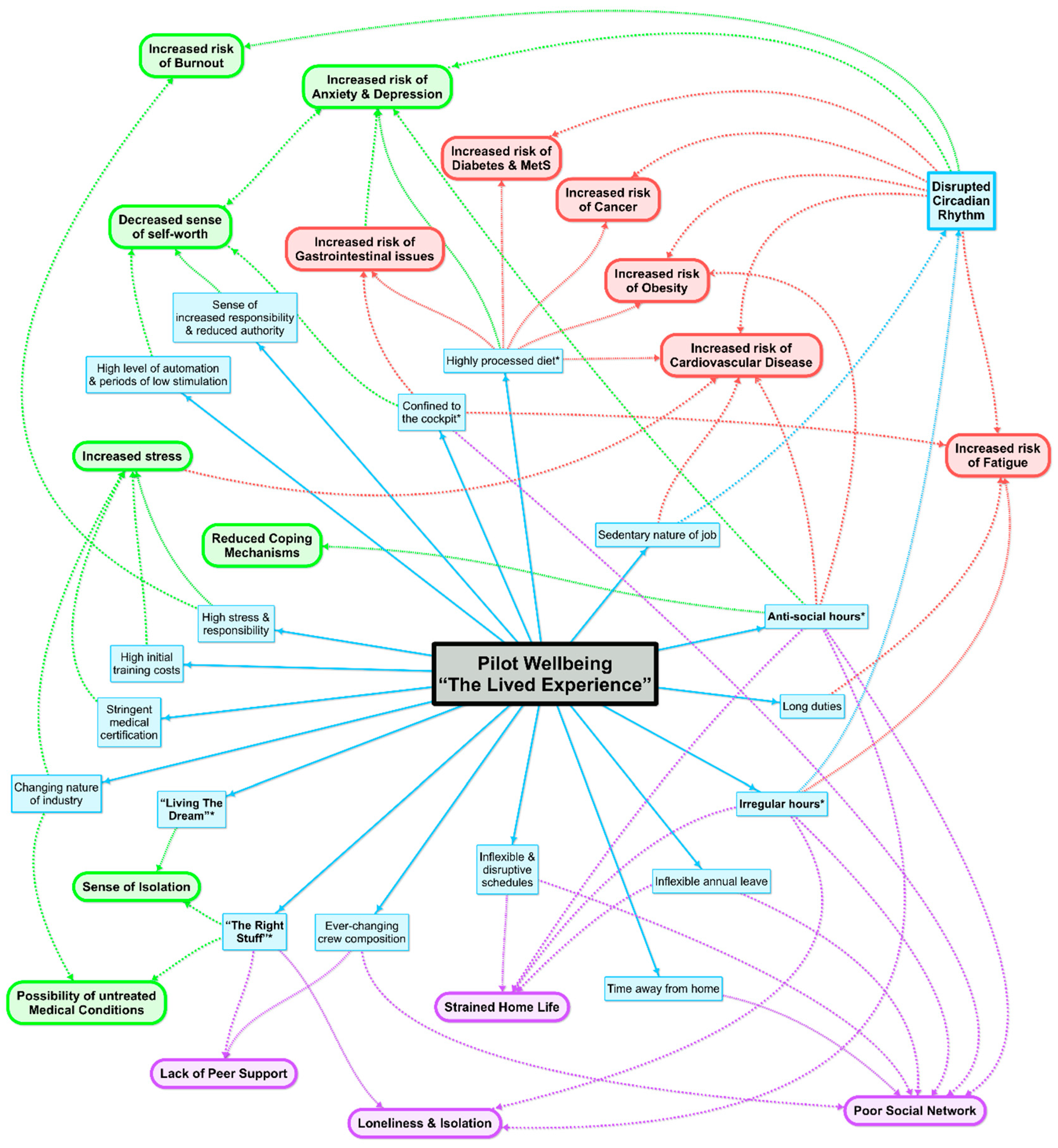
3.2. Pilot Wellbeing Behavior Model
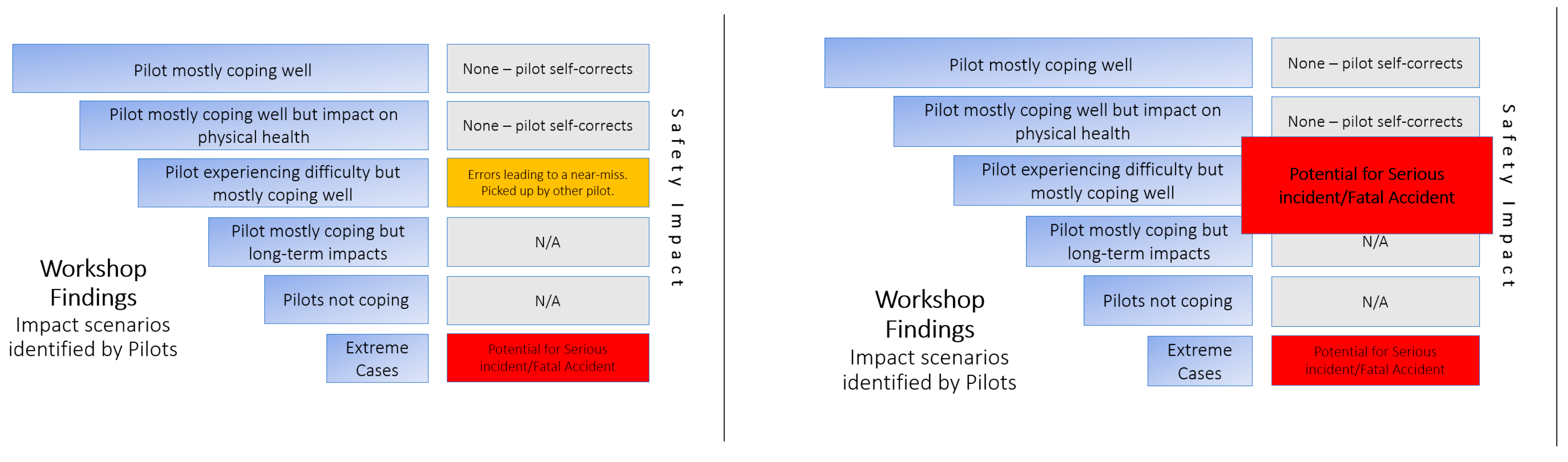
- Pilot mostly coping well
- Pilot mostly coping well but impact on physical health
- Pilot experiencing difficulties but mostly coping well
- Pilot mostly coping but long-term impacts
- Pilot not coping
- Extreme cases
3.3. Challenges Associated with COVID-19
3.4. Proposed Technologies and Behaviour Change
3.5. Tool Concepts and Framework
3.6. Wellness Assessment Concept Underpinning Technologies/Tools
3.7. Data Protection, Privacy, and Pilot Safeguards
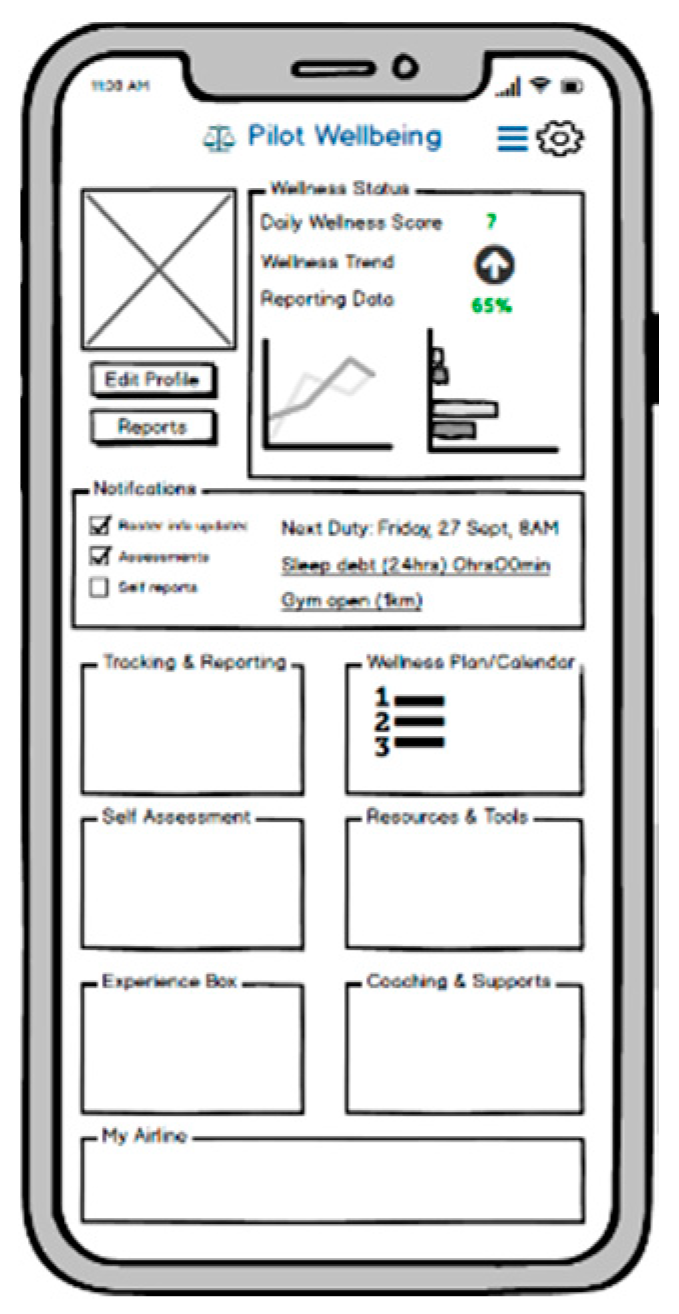
3.8. Tool 1: Pilot Self Management (Off Duty)
3.8.1. Objectives and Functions
- Wellness tracking, assessment, and reporting
- Provision of general resources/information and relaxation exercises
- Personalized tips/information, assessment, and wellness plans
- Self-assessment tools
- Virtual coaching and access to support
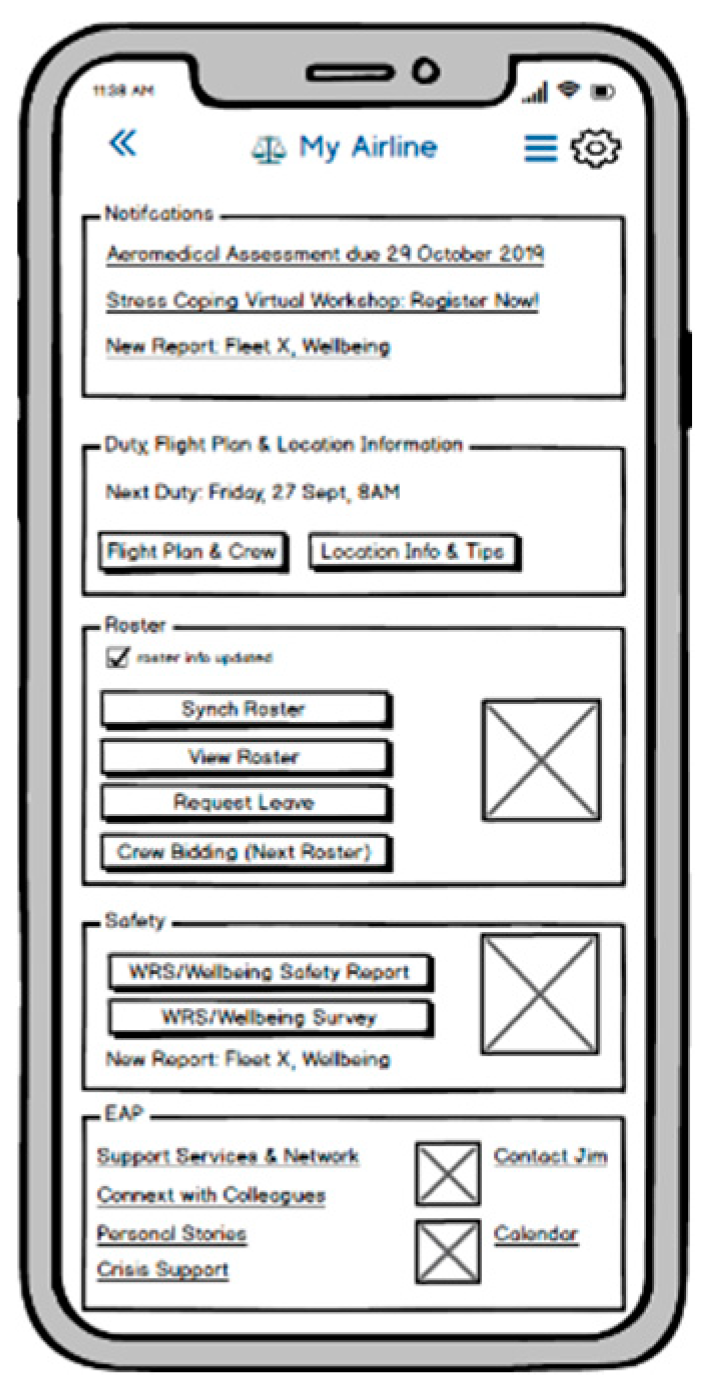
- Link to airline information systems (for example, roster, notices, safety information)
- Link to airline SMS
- Reporting of wellness issues and safety events
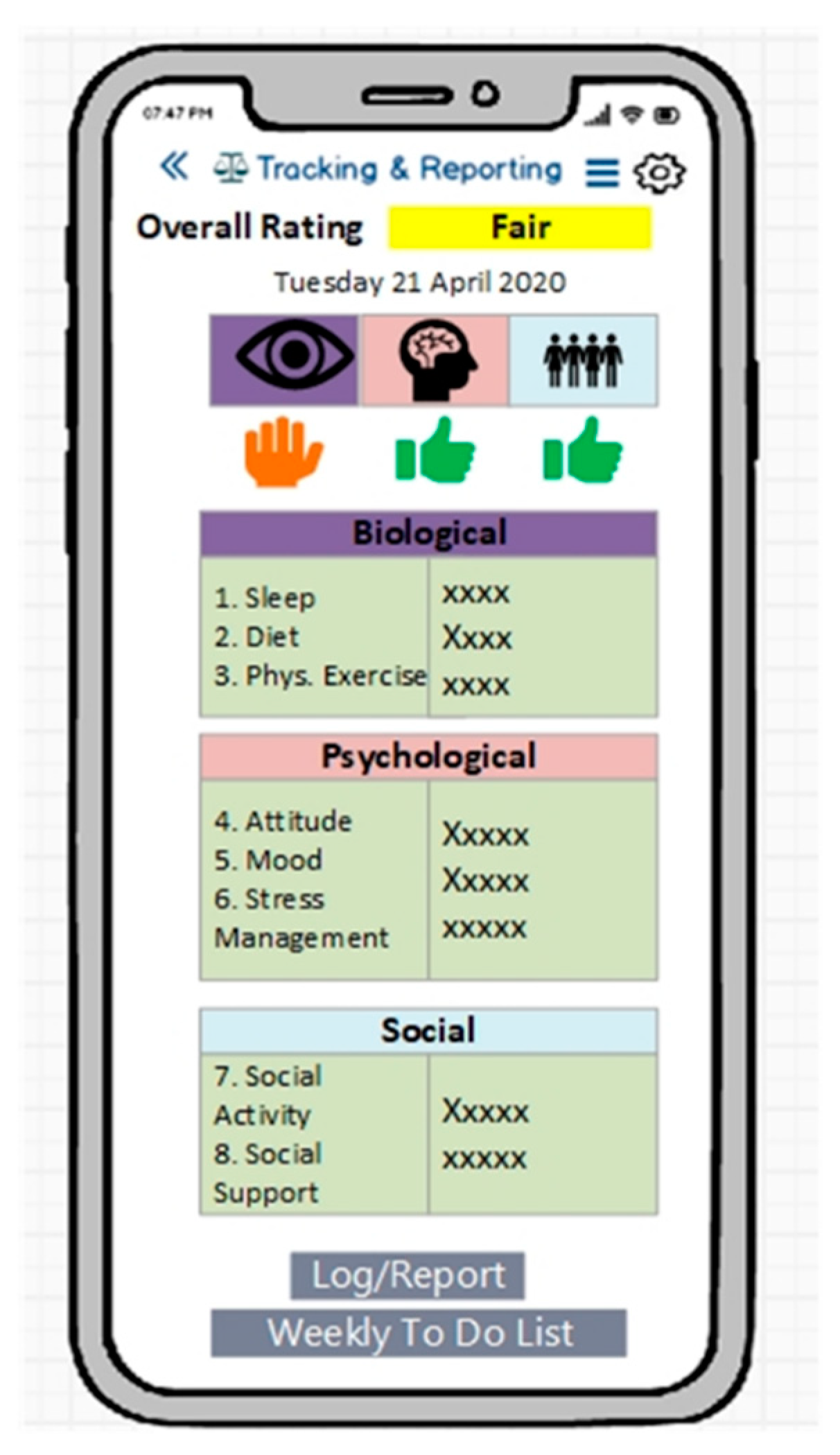
3.8.2. Wellbeing Assessment and Associated Checklists
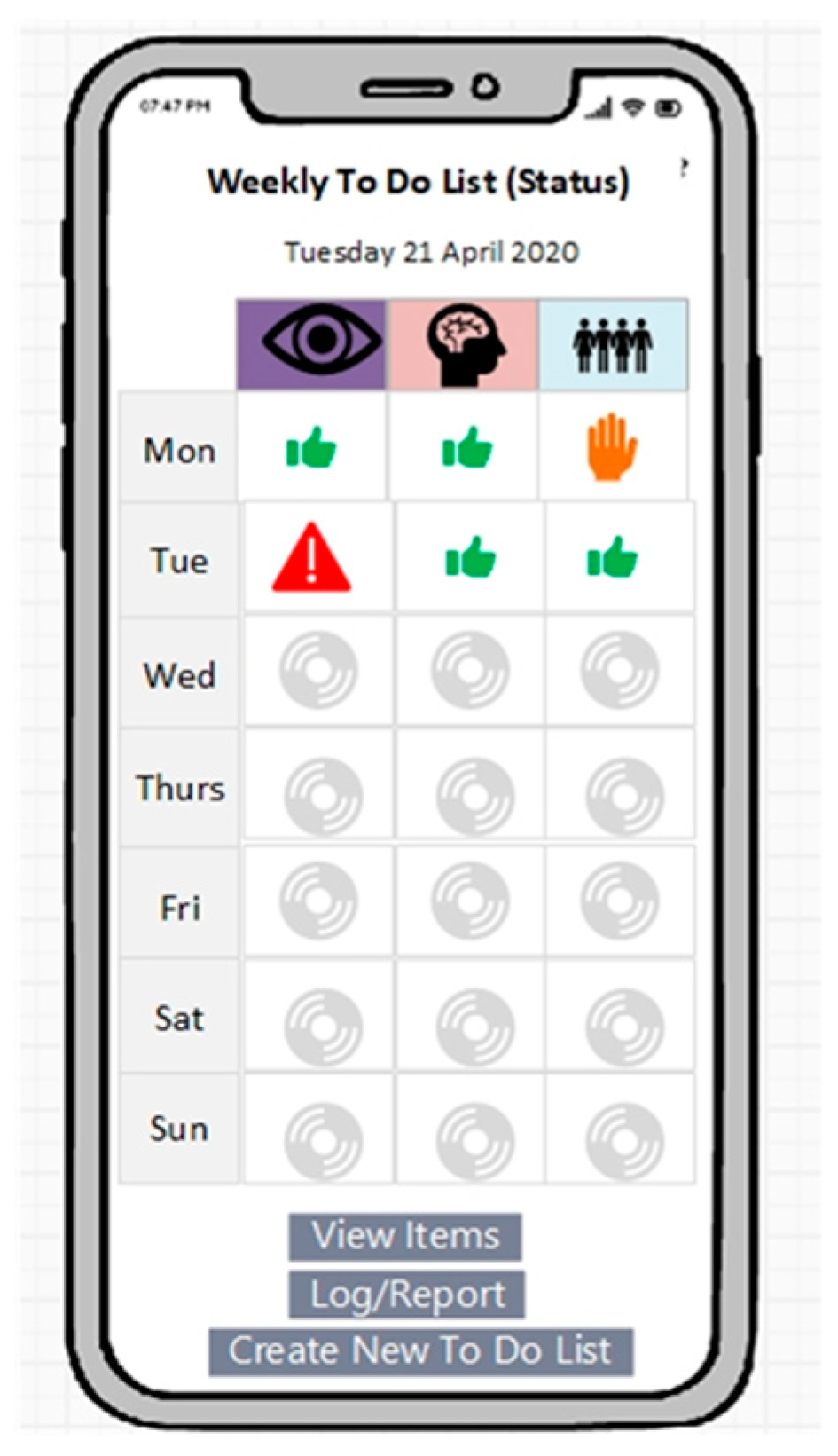
3.8.3. Wellbeing Management: Weekly Plan and Review
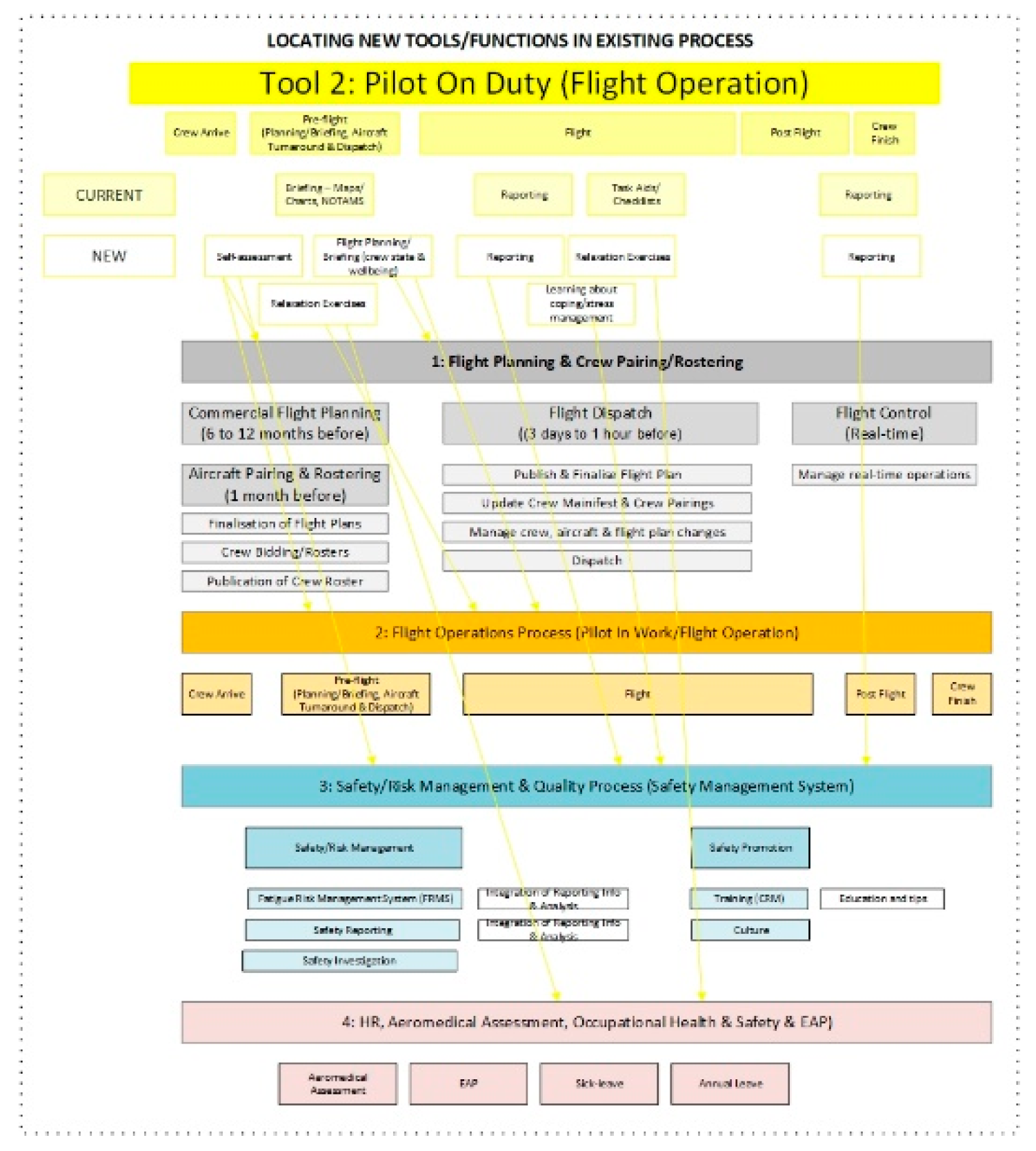
3.9. Tool 2: Pilot Operational Tools (On Duty)
- Enable joint assessment of crew state at the pre-flight stage
- Enable reporting in relation to WRS and wellbeing threats
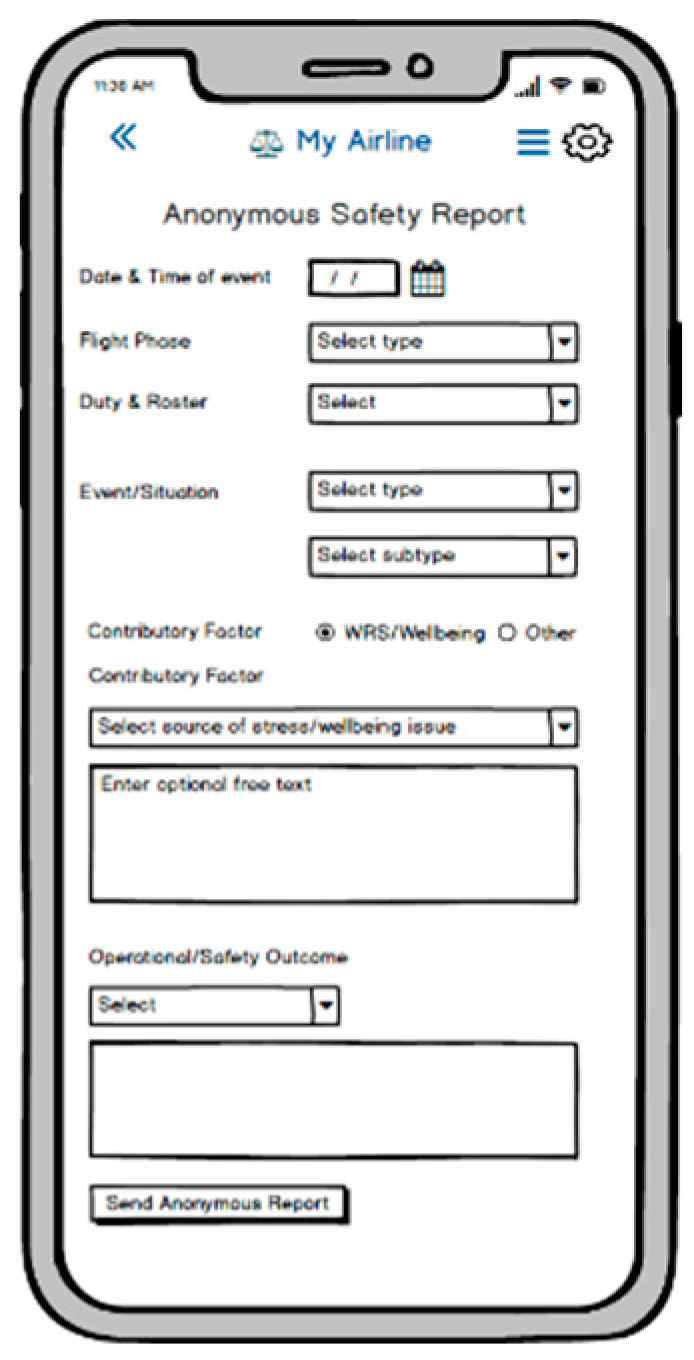
- Enable safety reporting
- Reporting of WRS/wellbeing issues and safety event (in flight)
- Enable access to support services within airline
- Provide support in crisis situations
3.10. Safety Promotion and Training Tools and Technologies
4. Discussion
4.1. Framing Problem, Need for Stakeholder Engagement, and Behaviour Change
4.2. Tripple Bottom Line and Ethics/Business/Legal Case
4.3. Problem to Be Addressed and Impact Scenarios
4.4. Safety Quantification and Wellbeing Culture
4.5. Concept of Pilot, Professionalism, and Wellbeing Culture
4.6. Theoretical Foundations for Tools
4.7. COVID and Need for Resilience and Immediate Changes
4.8. Relevance to Other Aviation Professionals and Others
4.9. Limitations and Areas for Further Research
4.10. Next Steps
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A. Field Research and Data Analysis Methods

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Part 1: A | Semi-Structured Interviews with Pilots | Semi-structured scoping interviews were conducted with N = 103 commercial pilots. The interviews were conducted opportunistically by Captain Paul Cullen and took the form of a casual conversation between peers. Participants obtained an informal briefing and verbal consent was established. Written consent was not elicited. Participants were informed that interview data was not being shared with others and that the findings were to be used to advance a model of the lived experience of being a pilot. Pilots were asked open ended questions about sources of WRS and the lived experience of being a pilot. They were also asked about the health impact/outcomes of these issues. These interviews were conducted on a preliminary exploratory basis. Research findings were documented after the event and not at the time. |
| Part 1: C | Participatory Workshops with Pilots | The workshops had two objectives:
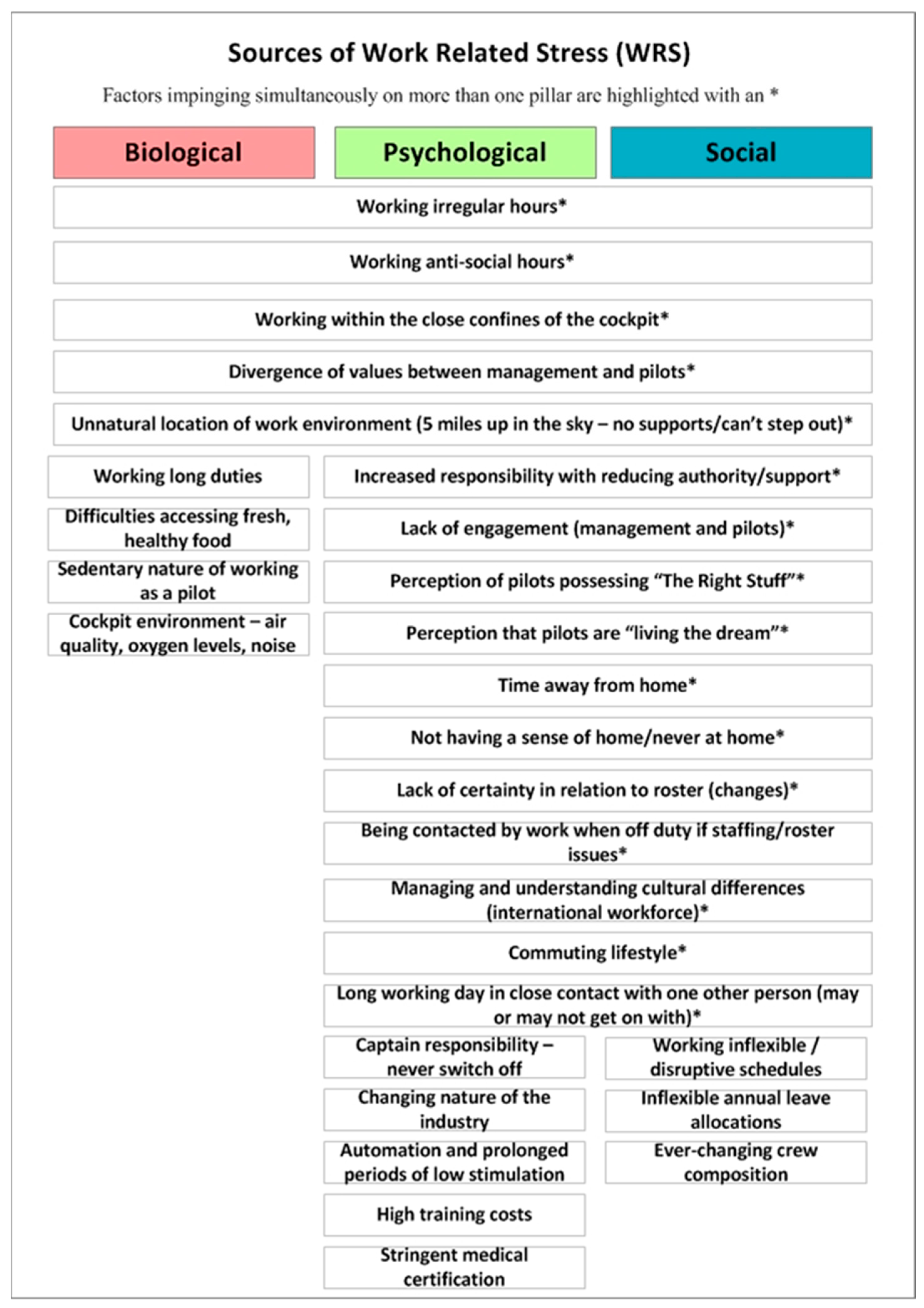
Three workshops were undertaken with 33 commercial pilots (workshop 1: N = 12, workshop 2: N = 10, workshop 3: N = 11). The workshops were undertaken between March and May 2018. A workshop presentation was compiled for each of the three workshops. This presentation provided the structuring framework for each of the workshops and guided the interaction between the workshop facilitator and the workshop participants. In the case of all three workshops, the workshops started with a short presentation about project goals and concepts. Participants were then invited to provide written consent for their participation in the workshop. There were some differences between the workshop structure/format and specific questions posed to participants in workshop 1, 2, and 3. In workshop 1, specific pilot personae were presented to participants. Each participant received a printed page with the personae information. These included descriptions of three different pilots—with different situations and each experiencing a spectrum of suffering. The workshop facilitator reviewed the different persona and invited feedback. Participants were then presented with the preliminary definition of the sources of WRS—grouped in terms of the biopsychosocial framework. In relation to sources of WRS, participants were invited to review and edit the list of sources presented. Following this, participants were presented with a preliminary safety case and three worked examples, corresponding to the biopsychological framework of health and wellbeing. Participants discussed the safety case and associated worked examples. There was then a group discussion concerning the relationship between WRS, pilot wellbeing, pilot performance, and flight safety. Workshop 2 was designed to address the findings of workshop 1. There were two format changes. First, the personae were not presented to pilots. Secondly, the preliminary safety case and worked example was replaced with a definition of six impact scenarios which emerged in workshop 1.Participants were invited to review/validate the six scenarios. Participants were invited to provide feedback about the scenarios defined in workshop 1—specifically in relation to impact on (1) wellbeing, (2) performance, and (3) safety. This was followed by a group discussion concerning the relationship between WRS, wellbeing, performance, and safety. In workshop 3, the integrated findings of workshop 1 and 2 were presented to participants. In relation to the six impact scenarios, participants also provided an estimation of the frequency in which such a situation would arise. In all three workshops, participants were invited to complete a homework exercise. At the end of each workshop, there was a full participant debriefing. The workshops were led by two human factors researchers (JC and PC). During each of the three workshops, the researchers alternated roles between leading the workshop and recording workshop notes. This followed the structured agenda. In each case, the researcher recorded workshop notes on their computer. Ethics approval for the workshops and additional interviews (to happen after the workshops) was granted by the School of Psychology, Trinity College Dublin (TCD)—in February 2018. |
| Part 2: E | Survey Design | This involved an anonymous web-based survey targeted at commercial pilots. The survey ran over a fifteen-month period (between 7th November 2018 and the 24 January 2020). The survey examined the effects of work-related stress (WRS) on pilot wellbeing and the associated impact on both pilot performance and flight safety. The survey also investigated pilot coping methods and pilot perception of the airline role in relation to managing WRS and wellbeing issues. The survey incorporated several standardized instruments to measure levels of common mental health issues. This includes the Patient Health Questionnaire-9 (PHQ-9), the Oldenburg Burnout (OLBI 8), and the Oldenburg Burnout (Modified Instrument). First, pilots received a short briefing about the study and its background. The electronic consent was then completed. Following this, relevant survey questions were answered. This was followed by a debriefing. Pilots were recruited using social media platforms such as LinkedIn and Twitter. The survey was powered by the SurveyMonkey service and did not collect any identifying information about the person. Further, no internet protocol (IP) addresses were collected. It was assumed that each participant was a pilot and only completed one survey. Several questions in the survey required knowledge that would only be readily available to pilots. An active pilot (co-author in this study: PC) reviewed surveys for potential non-pilot participants. All surveys passed this screening. Ethics approval was granted by the School of Psychology, Trinity College Dublin (TCD), in August 2018. |
| Part 4 B | Survey: Data Analysis | The purpose of the data analysis was to (1) identify sources of WRS and wellbeing impact, (2) measure depression levels in pilots, (3) examine the use of coping strategies (CS), and (4) examine the relationship between coping strategies used by pilots and their mental health—secifically depression severity levels.
|
| Ordered Logistic Regression Model and Interpreting the Odds Ratio | The objective was to model the relationship between each frequency level of each coping strategy and PHQ-9 Scores. Following this, we interpreted the odds ratio, to assess statistically significant coping strategies. Logistic regression is a statistical method for analyzing a dataset in which there are one or more independent variables that determine an outcome. The outcome is measured with a dichotomous variable (in which there are only two possible outcomes). The response variable Y is assumed to be binary (i.e., either a failure or success). In our case, we took the two outcomes of the response variable to be: (1) pilot has a PHQ-9 score below 10 (Y_i = 0) or (2) pilot has a PHQ-9 score of at least 10 (Y_i = 1). We are interested in drawing inferences on coping strategies and how they are related to depression severity levels, that is co-relation not causality (coping strategy causing the PHQ score to be below 10 or vice versa). This analysis does not consider interaction between different coping methods. Interpretation of results addressed the odds ratio. If the odds ratio is less than 1, then it is associated with a probability of having a lower depression severity level. Statistically significant coping strategies were set at p = 0.05. For more, please see Table A3, Table A4 and Table A5. It should be noted that the p-value tells us only whether a coping strategy at a certain frequency level was statistically significant. The odds ratio is what tells us whether that coping strategy is associated with a higher (if >1) or lower (<1) depression severity level. |
Appendix B
| Part | # | Objective and Description | Method | Stakeholder Involvement | Outcomes | Date | Status | Key References |
|---|---|---|---|---|---|---|---|---|
| 1 | A | Advancement of initial lived experience model | Semi-structured interviews with pilots | Pilots, (N = 103) | Lived experience model 1 | May 2015 to June 2017 | Complete | |
| B | Analysis of airline processes to manage pilot WRS and wellbeing (including MH) and associated regulation | Literature review | N/A | Airline process mapping Evaluation of regulation | January 2016 to June 2017 | Complete | [7] | |
| C | Validation of lived experience model—phase 1 Assessment of impact of WRS on wellbeing, performance, and safety | Participatory workshops | Pilots (N = 33) | Lived experience model 2 Preliminary impact model Impact scenarios | April to May 2018 | Complete | [8] | |
| 2 | A | Analysis of problem | Modelling problem from human factors/systems perspective. | N/A | Problem Definition | June 2018 to December 2018 | Complete | [7] |
| B | Validation of lived experience model—phase 2 | Survey with pilots (N = 325)—phase 1 | Pilots (N = 325) | Lived experience model 3 Preliminary assessment of coping strategies | Jan to April 2019 | Complete | [7] | |
| C | Analysis of coping strategies | Initial data analysis | N/A | Preliminary assessment of coping strategies | April to May 2019 | Complete | [7] | |
| D | Specification of interventions and tools requirements—airline and pilot levels Situate concepts in relation to therapeutic/clinical approaches | Research analysis | N/A | Interventions and tools requirements—airline level Interventions and tools requirements—pilot level | April to July 2019 | Complete | [7] | |
| E | Validation of lived experience model—phase 3 | Survey with pilots (N = 1050)—phase 2 | Pilots (N = 1050) | Lived experience model 4 | March 2019 to January 2020 | Complete | ||
| 3 | A | Specification of tool framework Specification of preliminary prototypes (Tool 1 and 2) Specification of airline process | Preliminary prototype development Process Mapping—as is and future process Analysis and Advancement of tool framework | N/A | Tool framework (Tool 1, 2, 3, 4, and 5) Prototypes for Tool 1 and 2 Process maps (as is/future) | August 2019 to September 2019 | Complete | N/A |
| B | Preliminary validation of tools framework with stakeholders Preliminary validation of Tool 1 and 2 with stakeholders | Preliminary validation research with airlines Preliminary validation research with software companies Preliminary review with regulatory authority (EASA and IAA) | N = 7 | Updated framework Updated prototypes for Tool 1 and 2 | September to October 2019 | Complete | N/A | |
| C | Analysis of customer/airline need and customer/airline journey | Specification of existing and future customer journey | N = 2 | Customer journey maps | December 2019 | Complete | N/A | |
| 4 | A | Specification of problem/change requirements from systems perspective Specification of behaviour change framework Further specification of tools | Analysis of problem Application of Fogg model of behaviour change Prototype development using Balsamiq | N/A | Definition of problem in relation to five interacting systems Behaviour change framework Prototypes for Tool 1 and Tool 2 Checklist specifications | Jan to Feb 2020 | Complete | [16] |
| B | Understanding pilot use of coping strategies—specifically in relation to depression severity | Analysis of survey findings (N = 1050) Regression model and odds ratio | N/A | Analysis of coping strategies | January 2020 to April 2020 | Complete | [16] | |
| C | Further specification of tools Specification of risk algorithm | Prototype development using Balsamiq | N/A | Tool 1 and 2 specification Preliminary risk algorithm | January 2020 to April 2020 | Complete | N/A | |
| 5 | A | Review in context of COVID need | Interviews with stakeholders/experts in the field Collaborative workshops with stakeholders | Panel of pilots, industry experts, aeromedical assessment experts (N = 9) | Tools framework Review of coping strategies and associated tools concepts Checklist specification | March to April 2020 | Complete | N/A |
Appendix C: Lived Experience Model (High Level)

Appendix D. Sources of WRS (Pre COVID-19)

Appendix E. COVID-19, Wellness Positives and Challenges
| # | Operational Scenario | Wellness Positives | Wellbeing Challenges and Sources of Stress |
|---|---|---|---|
| 1 | In work | Salary and financial wellbeing Getting out of the house Purpose obtained from job | Flying in a different environment Keeping track of changing schedule Managing childcare while working Financial wellbeing—reduced salary Uncertainty as to future financial security Different treatment of colleagues—guilt, discrimination Uncertainty about status of co-pilot (severity of suffering) Potential bereavement Social isolation Loss of social network Difficulties maintaining social network Potential illness/health challenges in family |
| 2 | Out of work | Improved sleep Improved diet More time with family Opportunity to take exercise (albeit limited with government rules/2 km) | Financial wellbeing—reduced salary or unemployment Uncertainty as to financial security Social isolation Loss of social network Difficulties maintaining social network Loneliness Not enough ‘me time’ Too much time with family Lack of routine Emotional instability Social isolation Loss of social network Difficulties maintaining social network Potential illness/health challenges in family Potential bereavement |
| 3 | Returning to work | Getting out of the house Purpose obtained from job Social interaction | Emotional instability Loss of social network Job proficiency and potential loss of confidence Training and competency—out of practice Ability to assess own wellbeing and MH If suffering, confidence in own ability to do the job safely Uncertainty about status of co-pilot (severity of suffering) Potential bereavement Bereavement Health challenges in family |
Appendix F. Tools and Processes




Appendix G. Provisional Risk Assessment Algorithm
| Classification | Factor | Factor | Risk Rating (Based on Data Picture) | ||
|---|---|---|---|---|---|
| H | M | L | |||
| Biological | 1 | Sleep and fatigue | |||
| 2 | Physical Exercise | ||||
| 3 | Diet | ||||
| Psychological | 4 | How feeling (stress) | |||
| 5 | Emotional stability and mood | ||||
| Social | 6 | Talking to others/seeing people | |||
| Overall Biological Rating | H M L | ||||
| Overall Psychological Rating | H M L | ||||
| Overall Social Rating | H M L | ||||
| Overall Wellness Risk Rating | H M L | ||||
Appendix H. Auto Harvesting Pilot Wellness Information
| Classification | Factor | Factor | Specific Info | Wellness App or Other App (Auto Harvesting) | Example Other Apps/Auto Harvesting |
|---|---|---|---|---|---|
| Biological | 1 | Sleep and fatigue | No. of hours sleep Sleep deficit Sleep disruption Sleep displacement | If using other, get from that Otherwise, 1 or 2 questions | From Crew Alert (if using) Or Garmin or Fitbit |
| 2 | Physical Exercise | No of steps | Garmin or Fitbit | ||
| 3 | Eating | 1 question? | |||
| 4 | Hydration | 1 question? | |||
| Psychological | 5 | How feeling (stress) | Heartrate Perceived stress (self-report) | If not other app, 1 question each day? | Garmin has heartrate If using MH app, take self-report from that |
| 6 | Emotional stability and mood | If not other app, 1 question each day? | If using MH app, take from that | ||
| Social | 7 | Taking to/contact with family | |||
| Talking to others/seeing people | 1 question each day? If using mobile phone calendar, quick question about what penciled in—did you do X? |
Appendix I. Prototype Examples (Tool 1)





Appendix J. Extended I am Safe Checklist
| I | Illness and Wellbeing | Do I have an illness or any symptoms of an illness? Am I feeling good/well? How is my overall health and wellbeing? Physical health? Emotional/Psychological Health? What is my mood and attitude like? Social Health? Have I seen family/friends? Getting help/support if needed? |
| M | Medication | Have I been taking prescription or over-the-counter drugs? |
| S | Stress and Stress Coping | Am I under psychological pressure from the job? Worried about financial matters, health problems or family discord? Am I actively managing my stress? Exercise? Social? Do I need help? |
| A | Alcohol | Have I been drinking within eight hours? Within 24 h? |
| F | Fatigue | Am I tired and not adequately rested? Have I been managing my sleep? |
| E | Eating and Exercise | Am I adequately nourished and hydrated? Am I taking physical exercise? |
References
- Elkington, J. Enter the Triple Bottom Line. 1994. Available online: https://johnelkington.com/archive/TBL-elkington-chapter.pdf (accessed on 11 October 2019).
- Elkington, J. Cannibals with Forks: The Triple Bottom Line of 21st Century Business; Capstone: Oxford, UK, 1999. [Google Scholar]
- Elkington, J. 25 Years Ago I Coined the Phrase “Triple Bottom Line.” Here’s Why It’s Time to Rethink It. Harvard Business Review. 2018. Available online: https://hbr.org/2018/06/25-years-ago-i-coined-the-phrase-triple-bottom-line-heres-why-im-giving-up-on-it (accessed on 11 October 2019).
- Sengenberger, W. The International Labour Organization: Goals, Functions and Political Impact; Friedrich Ebert Stiftung: Berlin, Germany, 2013. [Google Scholar]
- International Labour Organisation. Decent Work Agenda. 2020. Available online: https://www.ilo.org/global/topics/decent-work/lang--en/index.htm (accessed on 24 April 2020).
- Rodgers, G.; Lee, E.; Swepston, L.; Van Daele, J. The International Labour Organization and the Quest for Social Justice, 1919–2009 (PDF); International Labour Organization: Geneva, Switzerland, 2019; Available online: https://www.ilo.org/wcmsp5/groups/public/@dgreports/@dcomm/@publ/documents/publication/wcms_104643.pdf (accessed on 23 January 2020).
- Cahill, J.; Cullen, P.; Gaynor, R. Interventions to support the Management of WRS & Wellbeing Issues for Commercial Pilots. Cogn. Technol. Work 2019. [Google Scholar] [CrossRef]
- Cahill, J.; Cullen, P.; Gaynor, K. Estimating the Impact of Work-Related Stress on Pilot Wellbeing and Flight Safety’. In Proceedings of the 2nd International Symposium on Human Mental Workload: Models and Applications (H-WORKLOAD 2018), Netherlands Aerospace Centre (NLR), Amsterdam, The Netherlands, 20–21 September 2018. [Google Scholar]
- European Aviation Safety Agency (EASA) rules European Union Aviation Safety Agency (EASA). Commission Regulation (EU) No 965/2012 on Air Operations and associated EASA Decisions (AMC, GM and CS-FTL.1), Consolidated version for Easy Access Rules, Revision 12 March 2019. Part ORO, Annex II, Part ORO, ORO.GEN.200 Management Systems and associated Acceptable Means of Compliance (AMCs) and Guidance Material (GMs). 2019. Available online: https://www.easa.europa.eu/sites/default/files/dfu/Air%20OPS%20Easy%20Access%20Rules_Rev.12_March%202019.pdf (accessed on 2 May 2018).
- Bureau d’Enquêtes et d’Analyses pour la Sécurité de l’Aviation Civile (BEA). Accident on 24 March 2015 at Prads-Haute-Bléone (Alpes-de-Haute-Provence, France) to the Airbus A320-211 registered D-AIPX operated by Germanwings. Final Report; March 2016. Available online: https://www.bea.aero/uploads/tx_elydbrapports/BEA2015-0125.en-LR.pdf (accessed on 2 May 2018).
- Atherton, M. A question of psychology. 2019. Available online: https://www.aerosociety.com/news/a-question-of-psychology/ (accessed on 6 March 2019).
- European Union Aviation Safety Agency (EASA). Part-ORO—Organisation Requirements for Air Operations. 2017. Available online: https://www.easa.europa.eu/acceptable-means-compliance-and-guidance-material-group/part-oro-organisation-requirements-air (accessed on 17 July 2019).
- Anthony, T. Avoiding another Germanwings. In Proceedings of the International Pilot Peer Assist Conference (IPPAC), South Fort Worth, TX, USA, 25–26 October 2019; Available online: http://pilotpeerassist.com/international-pilot-peer-assist-conference/ (accessed on 13 May 2020).
- Atherton, M. Mental Wellbeing & Human Performance Seminar. Published by the RaeS. 2020. Available online: https://youtu.be/pT8uB7fVV44 (accessed on 11 May 2020).
- Dickens, P. Cleared for Take-off. A Pilot’s Guide to Returning to Flying. 2020. Available online: https://www.core-ap.co.uk/challenging-times (accessed on 11 May 2020).
- Cahill, J.; Cullen PAnwer, S.; Gaynor, K.; Wilson, S. Pilot Work Related Stress (WRS), Effects on Wellbeing and Mental Health, and Coping Methods. Part of the Mental Wellbeing & Human Performance Seminar. Published by the RaeS. 2020. Available online: https://youtu.be/pT8uB7fVV44 (accessed on 11 May 2020).
- Flight Safety Foundation. An Aviation Professional’s Guide to Wellbeing. 2020. Available online: https://flightsafety.org/wp-content/uploads/2020/04/Guide-to-Wellbeing.pdf (accessed on 11 May 2020).
- European Union Aviation Safety Agency (EASA). Together 4 Safety. 2020. Available online: https://www.easa.europa.eu/easa-and-you/safety-management/safety-promotion/ (accessed on 11 May 2020).
- Josephs, L. American Airlines Cutting International Summer Schedule by 60% as Coronavirus Drives Down Demand. CNBC News. 2 April 2020. Available online: https://www.cnbc.com/2020/04/02/coronavirus-update-american-airlines-cuts-summer-international-flights-by-60percent-as-demand-suffers.html (accessed on 30 April 2020).
- Sobieralski, J. COVID-19 and Airline Employment: Insights from Historical Uncertainty Shocks to the Industry. 2020. Available online: https://0-www-sciencedirect-com.brum.beds.ac.uk/science/article/pii/S2590198220300348 (accessed on 30 April 2020).
- Engel, G. The need for a new medical model: A challenge for biomedical science. Science 1977, 196, 126–129. [Google Scholar] [CrossRef]
- Ghaemi, S. The rise and fall of the biopsychosocial model. Br. J. Psychiatry 2009, 195, 3–4. [Google Scholar] [CrossRef] [Green Version]
- Borrell-Carrió, F.; Suchman, A.L.; Epstein, R.M. The biopsychosocial model 25 years later: Principles, practice, and scientific inquiry. Ann. Fam. Med. 2004, 2, 576–582. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lehman, B.J.; David, D.M.; Gruber, J.A. Rethinking the biopsychosocial model of health: Understanding health as a dynamic system. Soc. Pers. Psychol. Compass 2017, 11, e12328. [Google Scholar] [CrossRef] [Green Version]
- World Health Organisation (WHO). Stress at the Workplace. Available online: https://www.who.int/occupational_health/topics/stressatwp/en/#:~:text=Work-related%20stress%20is%20the%20response%20people%20may%20have,as%20well%20as%20little%20control%20over%20work%20processes (accessed on 12 May 2020).
- Flinchbaugh, C.; Luth, M.; Li, P. A Challenge or a Hindrance? Understanding the Effects of Stressors and Thriving on Life Satisfaction. Int. J. Stress Manag. 2015, 22. [Google Scholar] [CrossRef]
- Houtman, I.; Jettinghoff, K. Raising Awareness of Stress at Work in Developing Countries a modern hazard in a traditional working environment. In WHO Protecting Workers Health; Series 6; WHO Press: Geneva, Switzerland, 2007. [Google Scholar]
- Skybrary. Stress and Stress Management. Available online: https://www.skybrary.aero/index.php/Stress_and_Stress_Management(OGHFA_BN) (accessed on 12 May 2020).
- Lazarus, R.S. Theory-based stress measurement. Psychol. Inq. 1990, 1, 3–13. [Google Scholar] [CrossRef]
- Leka, S.; Griffiths, A.; Cox, T. Work Organisation & Stress: Systematic Problem Approaches for Employers, Managers and Trade Union Representatives; Protecting Work-ers’ Health Series: No. 3; World Health Organization: Geneva, Switzerland, 2003. [Google Scholar]
- Theorell, T.; Karasek, R.A. Current issues relating to psychosocial job strain and cardiovascular disease research. J. Occup Health Psychol. 1996, 1, 9–26. [Google Scholar] [CrossRef]
- Joseph, C. Stress Coping Strategies in Indian Military Pilots: Preliminary Observations. Int. J. Aviat. Aeronauctics Aerosp. 2016, 3. [Google Scholar] [CrossRef] [Green Version]
- Lazarus, R.; Folkman, S. Stress, Appraisal, and Coping; Springer: New York, NY, USA, 1984. [Google Scholar]
- Morimoto, H.; Shimada, H. The Relationship between Psychological Distress and Coping Strategies: Their Perceived Acceptability Within a Socio-Cultural Context of Employment, and the Motivation Behind Their Choices. Int. J. Stress Manag. 2015, 22, 159–182. [Google Scholar] [CrossRef]
- World Health Organisation (WHO). Mental Health. Available online: https://www.who.int/mental_health/en/ (accessed on 12 May 2020).
- Clark, D.M. Realizing the Mass Public Benefit of Evidence-Based Psychological Therapies: The IAPT Program. Annu. Rev. Clin. Psychol. 2018, 14, 159–183. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ijaz, S.; Davies, P.; Williams, C.J.; Kessler, D.; Lewis, G.; Wiles, N. Psychological therapies for treatment-resistant depression in adults. Cochrane Database Syst. Rev. 2018. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pompoli, A.; Furukawa, T.A.; Imai, H.; Tajika, A.; Efthimiou, O.; Salanti, G. Psychological therapies for panic disorder with or without agoraphobia in adults: A network meta-analysis. Cochrane Database Syst. Rev. 2016. [Google Scholar] [CrossRef] [PubMed]
- National Institute for Health and Clinical Excellence (NICE). Common Mental Health Problems: Identification and Pathways to Care. Clinical Guideline [CG123]. 25 May 2011. Available online: https://www.nice.org.uk/guidance/cg123/chapter/1-guidance (accessed on 12 May 2020).
- National Institute for Health and Clinical Excellence (NICE). Mental Wellbeing at Work. Public Health Guideline [PH22]. 5 November 2009. Available online: https://www.nice.org.uk/guidance/ph22 (accessed on 12 May 2020).
- Tetrick, L.; Winslow, C. Workplace Stress Management Interventions and Health Promotion (April 2015). Annu. Rev. Organ. Psychol. Organ. Behav. 2015, 2, 583–603. Available online: https://ssrn.com/abstract=2594246 (accessed on 20 May 2020). [CrossRef] [Green Version]
- Ruotsalainen, J.; Serra, C.; Marine, A.; Verbeek, J. Systematic review of interventions for reducing occupational stress in health care workers. Scand. J. Work Environ. Health 2008, 34, 169–178. [Google Scholar] [CrossRef]
- Karasek, R. Stress prevention through work reorganization: A summary of 19 international case studies. In ILO: Conditions of Work. Digest—Preventing Stress at Work; International Labour Organisation: Geneva, Switzerland, 1992; Volume 11, pp. 23–41. [Google Scholar]
- Tarro, L.; Llauradó, E.; Ulldemolins, G.; Hermoso, P.; Solà, R. Effectiveness of Workplace Interventions for Improving Absenteeism, Productivity, and Work Ability of Employees: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Int. J. Environ. Res. Public Health 2020, 17, 1901. [Google Scholar] [CrossRef] [Green Version]
- Odeen, M.; Magnussen, L.H.; Maeland, S.; Larun, L.; Eriksen, H.R.; Tveito, T.H. Systematic review of active workplace interventions to reduce sickness absence. Occup. Med. 2013, 63, 7–16. [Google Scholar] [CrossRef] [Green Version]
- Kenny, A. Aristotle: The Eudemian Ethics; Oxford University Press: Oxford, UK, 2011. [Google Scholar]
- Seligman, M. Authentic Happiness: Using the New Positive Psychology to Realize Your Potential for Lasting Fulfillment; Free Press: New York, NY, USA, 2002. [Google Scholar]
- Fikretoglu, D.; McCreary, D.R. Psychological Resilience: A Brief Review of Definitions, and Key Theoretical, Conceptual, and Methodological Issues. Technical Report DRDC Toronto TR 2012-012. 2012. Available online: www.cradpdf.drdc-rddc.gc.ca/PDFS/unc121/p536951_A1b.pdf (accessed on 3 July 2018).
- Bandura, A. Self-efficacy mechanism in human agency. Am. Psychol. 1982, 37, 122–147. [Google Scholar] [CrossRef]
- Jordan, T.R.; Khubchandani, J.; Wiblishauser, M. The Impact of Perceived Stress and Coping Adequacy on the Health of Nurses: A Pilot Investigation. Nurs. Res. Pract. 2016, 2016. [Google Scholar] [CrossRef] [Green Version]
- Blazer, D.G. Self-efficacy and depression in late life: A primary prevention proposal. Aging Ment. Health 2002, 6, 315–324. [Google Scholar] [CrossRef]
- Harris, D. Human Performance on the Flight Deck; Ashgate Publishing Limited; Taylor & Francis Group: Surrey, UK, 2011. [Google Scholar]
- Moriarty, D. Practical Human Factors for Pilots; Academic Press: London, UK, 2015. [Google Scholar]
- Roscoe, A.H. Stress and workload in pilots. Aviat. Space Environ. Med. 1978, 49, 630–633. [Google Scholar] [PubMed]
- Stokes, A.; Kite, K. Flight Stress: Stress, Fatigue and Performance in Aviation; Routledge: London, UK, 1994. [Google Scholar]
- Eurocontrol. Human Factors Module Critical Incident Stress Management. Available online: https://www.skybrary.aero/bookshelf/books/4578.pdf (accessed on 11 June 2020).
- Civil Aviation Authority. Aeronautical Information Circular. Post-Traumatic Stress. Available online: https://www.skybrary.aero/bookshelf/books/2628.pdf (accessed on 11 June 2020).
- Fine, P.M.; Hartman, B.O. Psychiatric strengths and weaknesses of typical Air Force pilots. In Brooks Air Force Base; Report No SAM- TR-68-121; USAF School of Aerospace Medicine: South Fort Worth, TX, USA, 1968. [Google Scholar] [CrossRef] [Green Version]
- Picano, J. An empirical assessment of stress-coping styles in military pilots. Aviat. Spaceenviron. Med. 1990, 61, 356–360. [Google Scholar]
- Cooper, C.; Sloan, S. Occupational and psychological stress among commercial airline pi-lots. J. Occup. Med. 1985, 27, 570–576. [Google Scholar] [CrossRef] [PubMed]
- Karlins, M.; Koss, F.; McCully, L. The spousal factor in pilot stress. Aviat. Space Environ. Med. 1989, 60, 1112–1115. [Google Scholar]
- Bennett, S.A. A longitudinal ethnographic study of aircrews’ lived experience of flying operations at a low-cost airline. Risk Manag. Int. J. 2006, 8, 92–117. [Google Scholar] [CrossRef]
- Meland, A.; Fonne, V.; Wagstaff, A.; Pensgaard, A.M. Mindfulness-based mental training in a high-performance combat aviation population: A one-year intervention study and two-year follow-up. Int. J. Aviat. Psychol. 2015, 25, 48–61. [Google Scholar] [CrossRef]
- Caldwell, J. Fatigue in the aviation environment: An overview of the causes and effects as well as recommended countermeasures. Aviat. Space Environ. Med. 1997, 68, 932–938. [Google Scholar]
- Bor, R.; Eriksen, C.; Oakes, M.; Scragg, P. (Eds.) Pilot mental health assessment and support. In A Practitioner’s Guide; Routledge: Abington, UK, 2016. [Google Scholar]
- Feijó, D.; Luiz, R.R.; Camara, V.M. Common mental disorders amonst civil aviation pilots. Aviat. Space Environ. Med. 2012, 83, 509–513. [Google Scholar] [CrossRef] [PubMed]
- Wu, A.C.; Donnelly-McLay, D.; Weisskopf, M.G.; McNeely, E.; Betancourt, T.S.; Allen, J.G. Airplane pilot mental health and suicidal thoughts: A cross-sectional descriptive study via anonymous web-based survey. Environ. Health 2016, 15, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Pasha, T.; Stokes, P. Reflecting on the Germanwings Disaster: A Systematic Review of Depression and Suicide in Commercial Airline Pilots. Front. Psychiatry 2018, 9, 89. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Hagan, A.D.; Issartel, J.; Nevill, A.; Warrington, G. Flying into Depression. Workplace Health Saf. 2017, 65, 109–117. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- International Civil Aviation Authority (ICAO). Annex 19—Safety Management. 2013. Available online: https://www.icao.int/safety/SafetyManagement/Documents/Annex%2019%20-%20ICAO%20presentation%20-%20self%20instruction%2024September2013.pdf (accessed on 17 July 2019).
- International Civil Aviation Authority (ICAO). Safety Management Manual (SMM), Document 9859, 3rd ed. Available online: https://www.skybrary.aero/bookshelf/books/644.pdf (accessed on 2 May 2020).
- Cahill, J.; McDonald, N.; Losa, G. Enhancing human performance and overall flight safety through improvements in airline system information flow. In Proceedings of the 28th Conference of the European Association for Aviation Psychology, Valencia, Spain, 27–31 October 2008. [Google Scholar]
- Cahill, J. Flight Crew Task Performance and the Requirements for a New Tool Supporting the Pre-flight, Flight Planning and Briefing Task. Doctoral Dissertation, Trinity College Dublin, Dublin, Ireland, Thesis 9479.1, TCD E-Thesis Access. 2010. Available online: http://stella.catalogue.tcd.ie/iii/encore/record/C__Rb16723129__Scahill%2C%20joan__Orightresult__U__X4?lang=eng&suite=cobalt (accessed on 19 January 2020).
- Skybrary. Fatigue Risk Mangement Systems. 2019. Available online: https://www.skybrary.aero/index.php/Fatigue_Risk_Management_System(FRMS) (accessed on 23 January 2019).
- Gibbs, S. Peer support programme for pilots. In Pilot Mental Health Assessment and Support; Bor, R., Eriksen, C., Oakes, M., Scragg, P., Eds.; Routledge: Abington, UK, 2016. [Google Scholar]
- Spencer-Thomas, S. Up on the High Wire: Promoting Resiliency during Tough Times. In Proceedings of the International Pilot Peer Assist Conference (IPPAC), South Fort Worth, TX, USA, 25–26 October 2019; Available online: http://pilotpeerassist.com/international-pilot-peer-assist-conference/ (accessed on 12 May 2020).
- Jeppesen. Crew Fleet Crew Alert. Available online: http://ww1.jeppesen.com/industry-solutions/aviation/commercial/crew-fleet-CrewAlert.jsp (accessed on 12 May 2020).
- European Union Aviation Safety Agency (EASA). Guidance for CRM implementation. 2017. Available online: https://www.easa.europa.eu/document-library/general-publications/crm-training-implementation (accessed on 17 July 2019).
- Cahill, J.; Mc Donald, N.; Losa, G. Intelligent Planning and the Design of a New Risk Based, Intelligent Flight Plan. Cogn. Technol. Work 2011, 13, 43–66. [Google Scholar] [CrossRef]
- Federal Aviation Authority (FAA). Single Pilot Crew Resource Management. 2015. Available online: https://www.faa.gov/news/safety_briefing/2015/media/SE_Topic_15_03.pdf (accessed on 12 May 2020).
- Houston, S. Pilot Risk Management: There’s a Checklist for That! 2019. Available online: https://www.thebalancecareers.com/the-i-m-safe-checklist-282948 (accessed on 12 May 2020).
- Federal Aviation Authority (FAA). Personal Minimums Checklist’ Federal Aviation Authority. (2009). PAVE—Personal Minimums Checklists (2020). Available online: https://www.faa.gov/training_testing/training/fits/guidance/media/personal%20minimums%20checklist.pdf (accessed on 12 May 2020).
- Federal Aviation Authority. PAVE—Personal Minimums Checklists. 2020. Available online: https://www.faa.gov/regulations_policies/handbooks_manuals/aviation/phak/media/02_phak_toc.pdf (accessed on 12 May 2020).
- Ironside, R. Germanwings’ crash report sees Qantas bid to help gauge pilots’ mental health. Available online: https://www.heraldsun.com.au/technology/germanwings-crash-report-sees-qantas-bid-to-help-gauge-pilots-mental-health/news-story/ae6b6efb5428033fcca134ff40c39471?from=herald%20sun_rss (accessed on 12 May 2020).
- Ingre, M.; Van Leeuwen, W.; Klemets, T.; Ullvetter, C.; Hough, S.; Kecklund, G.; Karlsson, D.; Åkerstedt, T. Validating and Extending the Three Process Model of Alertness in Airline Operations. PLOS 2014. [Google Scholar] [CrossRef]
- Flightman. Our Products. 2020. Available online: http://www.flightman.com/our-products/ (accessed on 12 May 2020).
- Kudret, S.; Erdogan, B.; Bauer, T. Self-Monitoring Personality Trait at Work: An Integrative Narrative Review and Future Research Directions. J. Organ. Behav. 2018. [Google Scholar] [CrossRef]
- Koo, S.H.; Fallon, K. Explorations of wearable technology for tracking self and others. Fash Text 2018, 5, 8. [Google Scholar] [CrossRef] [Green Version]
- Boulos, M.N.K.; Brewer, A.C.; Karimkhani, C.; Buller, D.B.; Dellavalle, R.P. Mobile medical and health apps: State of the art, concerns, regulatory control, and certification. Online J. Public Health Inform. 2014, 5, e229. [Google Scholar]
- Till, C.; Petersen, A.; Tanner, C.; Munsie, M. Creating “automatic subjects”: Corporate wellness and self-tracking. Health Interdiscip. J. Soc. Study Healthilln. Med. 2019, 23, 418. [Google Scholar] [CrossRef] [Green Version]
- Hull, G.; Pasquale, F. Toward a critical theory of corporate wellness. BioSocieties 2018, 13, 190–212. [Google Scholar] [CrossRef]
- Moore, P.; Robinson, A. The quantified self: What counts in the neoliberal workplace. New Media Soc. 2016, 18, 2774–2792. [Google Scholar] [CrossRef]
- Moore, P.; Piwek, L. Regulating wellbeing in the brave new quantified workplace. Empl. Relat. 2017, 308–316. [Google Scholar] [CrossRef] [Green Version]
- European Parliament. Directive (EU) 2016/680 of the European Parliament and of the Council of 27 April 2016 on the Protection of Natural Persons with Regard to the Processing of Personal Data by Competent Authorities for the Purposes of the Prevention, Investigation, Detection or Prosecution of Criminal Offences or the Execution of Criminal Penalties, and on the Free Movement of such Data, and Repealing Council Framework Decision 2008/977/JHA. Available online: https://eur-lex.europa.eu/eli/dir/2016/680/oj/eng (accessed on 12 May 2020).
- Data Protection Commission. Quick Guide to the Principles of Data Protection. 2020. Available online: https://www.dataprotection.ie/sites/default/files/uploads/2019-11/Guidance%20on%20the%20Principles%20of%20Data%20Protection_Oct19.pdf (accessed on 12 May 2020).
- Cullen, P.; Cahill, J.; Gaynor, K. Turbulent Times. 2020. Available online: https://www.tcd.ie/cihs/assets/pdf/TurbulentTimes.pdf (accessed on 12 May 2020).
- International Standards Organisation (ISO). Standard 6385. Ergonomics Principles in the Design of Work Systems. 2016. Available online: https://www.iso.org/standard/63785.html (accessed on 12 May 2020).
- Baxter, G.; Sommerville, I. Socio-technical systems: From design methods to systems engineering. Interact. Comput. 2011, 23, 4–17. [Google Scholar] [CrossRef] [Green Version]
- Fogg, B.J. The Small Changes that Change Everything; Houghton Mifflin Harcourt: Boston, CA, USA, 2020. [Google Scholar]
- Fogg, B.J. A Behaviour Model for Persuasive Design. In Proceedings of the 4th International Conference on Persuasive Technology. Persuasive ’09; ACM: New York, NY, USA, 2009; pp. 40:1–40:7. ISBN 9781605583761. [Google Scholar] [CrossRef]
- Waterson, P.E. A critical review of the systems approach within patient safety research. Ergonomics 2009, 52, 1185–1195. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carayon, P.; Schoofs Hundt, A.; Karsh, B.T.; Gurses, A.P.; Alvarado, C.J.; Smith, M.; Flatley Brennan, P. Work system design for patient safety: The SEIPS model. Qual. Saf. Health Care 2006, 15 (Suppl. S1), i50–i58. [Google Scholar] [CrossRef]
- Osterwalder, A.; Pigneur, Y.; Clark, T. Business Model Generation: A Handbook for Visionaries, Game Changers, and Challengers; Strategyzer Series; John Wiley & Sons: Hoboken, NJ, USA, 2010. [Google Scholar]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The PHQ-9: Validity of a brief depression screening measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef] [PubMed]






| Part | # | Objective and Description | Method | Stakeholder Involvement |
|---|---|---|---|---|
| 1 | A | Advancement of initial lived experience model. | Preliminary, semi-structured and explorative interviews with pilots | Pilots, (N = 103) |
| B | Analysis of airline processes to manage pilot WRS and wellbeing (including MH) and associated regulation. | Literature review | N/A | |
| C | Validation of the lived experience model—phase 1. Assessment of the impact of WRS on pilot health, human performance, and flight safety. | Participatory workshops with pilots | Pilots (N = 33) | |
| 2 | A | Analysis of problem. Specification of problem and change requirements from a systems perspective. | Modelling problem from human factors/systems perspective | N/A |
| B | Validation of lived experience model—phase 2. | Survey with pilots (N = 325) —phase 1 | Pilots (N = 325) | |
| C | Analysis of coping strategies. | Initial data analysis following first wave of survey | N/A | |
| D | Specification of interventions and tools requirements—airline and pilot levels. Situate concepts in relation to therapeutic/clinical approaches. | Research analysis | N/A | |
| E | Validation of lived experience model—phase 3. | Survey with pilots (N = 1050) —phase 2 | Pilots (N = 1050) | |
| 3 | A | Specification of tools framework. Specification of preliminary prototypes (Tool 1 and 2). Specification of airline process—existing and to be. | Preliminary prototype development Process mapping—as is and future process Analysis and advancement of tool framework | N/A |
| B | Preliminary validation of tools framework with stakeholders. Preliminary validation of Tool 1 and 2 with stakeholders. | Preliminary validation research with airlines Preliminary validation research with software companies Preliminary review with regulatory authority (European Aviation Safety Authority (EASA) and Irish Aviation Authority (IAA) | (N = 7) | |
| C | Business analysis and development of business model canvas (BMC) about the aviation industry. Analysis of customer need. Analysis of customer journey. | Specification of business logic and allied tools concept from perspective of stakeholder need Specification of existing and future customer journey | N = 1 | |
| 4 | A | Refinement of problem analysis from a systems perspective. Specification of problem and solution in context of a behavior change framework. | Analysis of problem Application of Fogg model of behavior change to problem and solution specification. | N/A |
| B | Understanding pilot use of coping strategies in relation to depression severity. Specification of risk algorithm. | Analysis of survey findings (N = 1050) Regression model and odds ratio | N/A | |
| C | Further specification of tools. | Prototype development using Balsamiq | N/A | |
| 5 | A | Review of problem in context of COVID need. | Collaborative workshops/discussion with stakeholders Documentation of problems | Panel of pilots and industry experts (N = 9) |
| # | Level | Description | Example Problems |
|---|---|---|---|
| 1 | Pilot level (lived experience, practices/behavior, culture) | In work Outside work Home/work interface | Attitudes to mental health Health behaviors amongst pilots Machoism and culture Reporting and disclosure culture |
| 2 | Airline | Sociotechnical system level—processes, training, technologies, business model, and culture and values Link to wider aviation community and industry | Inflexible working schedules Presenteeism, restrictions on sick leave and difficulties reporting sick Machoism and culture Reporting and disclosure culture Nature of airline Employee Assistance Programe (EAP) and access to support Design of existing safety management system (lack of focus on risks relating to the human factor) |
| 3 | Community and social system | Public expectations, pricing, 24/7, health system, and access to support | Public expectations, pricing, 24/7, also health system and access to support |
| 4 | Health and safety in work (regulator/regulation) | Health and safety authorities at national and European level | Current strategy for evaluating WRS Current strategy for managing psychological wellbeing in work and associated stress |
| 5 | Aviation regulator and regulation | Aviation authorities at national and European level | Regulation pertaining to safety/risk management, HF management, wellbeing and mental health monitoring and assessment Design of existing regulation—mental health assessment, aeromedical assessment |
| 6 | Broader aviation industry | Technology providers, aircraft manufacturers, insurance companies | Current process for insuring airlines—flight safety, human assets/pilots Available technology to support wellness management for pilots |
| # | Factor | Positive | Negative | None | TBD |
|---|---|---|---|---|---|
| 1 | Use of coping mechanisms—sleep, exercise, supports, diet | * | |||
| 2 | Awareness of issue/challenges/suffering | * | |||
| 3 | Normalisation of problem/suffering | * | |||
| 4 | Concern for own health (self or family) | * | |||
| 5 | Positive attitude to seeking help/support | * | |||
| 6 | Pre-existing MH issue | * | |||
| 7 | Existing health and wellbeing (if fatigue, burnout/exhaustion) | * | |||
| 8 | Shift pattern/shift time | * | |||
| 9 | Work contract | * | |||
| 10 | Type of operation | * | |||
| 11 | Male/Female | * | |||
| 12 | Social capital and network | * | |||
| 13 | Existing habits and behaviours (sleep, diet, exercise) | * | |||
| 14 | Interest in physical exercise | * | |||
| 15 | Convenience and access (24/7) | * | |||
| 16 | Pilot education and awareness schemes | * | |||
| 17 | Social acceptability and demonstration of ‘socially desirable’ values and practices (self-care) | * |
| Description | System Level |
|---|---|
| Pilot interest in developing/augmenting their health and wellbeing | 1, 2 |
| Health attitudes of family and social network | 1, 3 |
| Social supports from family and social network | 3 |
| Improved experience of home/work interface | 1, 2 |
| Public acceptability—addressing MH and wellbeing challenges | 1, 2, 3 |
| Flight safety | 2, 3 |
| Work policy | 2 |
| Commercial reasons—reduction in costs of absenteeism, operational changes, flight cancellations, due to pilot illness | 2 |
| Work incentives and rewards | 2 |
| Social acceptability | 2 |
| Productivity and reduction in absenteeism costs | 3 |
| Normalisation of health and wellbeing supports across all industries | 4 |
| Regulatory support | 5 |
| Aviation industry embrace requirement for change | 6 |
| Integrated approach across the aviation industry—solve the problem at different levels (actors, process, operational timeline, etc.) | 6 |
| Acceptance that these issues exist for all workers and not just pilots and must be addressed | 6 |
| Description | System Level |
|---|---|
| Piot advocacy | 1, 2 |
| Culture change at pilot level—normalisation of MH, acceptability of self-care | 1, 2 |
| Use of new digital tools for pilots—supporting awareness, monitoring, and self-management of health | 1, 2 |
| Culture change at airline industry level | 2 |
| Airline support—new training, enhancements to airline safety management systems SMS, wellbeing supports/EAP | 2 |
| Acceptance of holistic model of pilot wellness (including factors pertaining to all three pillars) | 2 |
| Management of pilot wellbeing as a risk within an airline safety management system | 2 |
| Acceptance of MH and wellbeing challenges—community | 3 |
| Change in terms of public expectation—24/7 and low cost | 3 |
| Enhancements to existing health systems—public and private | 3 |
| Normalisation of health and wellbeing supports across all industries | 4 |
| Regulatory support—particularly in area of data protection | 5 |
| Availability of new technologies supporting stress coping and healthy behaviour | 6 |
| Transparency in terms of technology design in relation to how data is shared and data protection | 6 |
| Description | System Level |
|---|---|
| Pilot awareness of need to develop resilience and cope | 1 |
| Culture of presenteeism | 1 |
| Pilot attitudes to health and wellbeing and practice of resilience | 1 |
| Managing privacy issues | 1, 2 |
| Pilot trust in system | 1, 2 |
| Airline business models and work contracts for pilots | 1, 2 |
| Existing pilot culture (not declaring suffering, presenteeism, macho culture) | 1, 2 |
| Existing industry culture (stigma around MH and wellness challenges) | 3 |
| Lack of support within community for pilots—impact of job on wellbeing | 3 |
| Public expectations—expectation of low costs flights, 24/7 operations, flexibility for consumer | 3 |
| Existing approach across all industries re management of health and wellbeing in work—lack of focus on psychosocial dimensions | 4 |
| Aviation regulatory requirements | 5 |
| Lack of transparency in terms of technology design—specifically, in relation to how data is shared and data protection | 6 |
| Target Behaviour | WRS and wellbeing awareness and education | Increased awareness of WRS and wellbeing (including MH) |
| Acceptability of MH/self-management of wellbeing and MH | Increased acceptability of MH Normalisation of MH Acceptability of self-care | |
| Self-management behaviour | Promote coping Shift to self-management Cultural change | |
| Safety behaviour | Interface between life in and outside work | |
| Motivation | Safety, health and wellbeing, work policy, health attitudes, social acceptability, work incentives and rewards, etc. | |
| Ability | Health, time availability, work flexibility, family support | |
| Prompt | (1) Mobile apps + (2) airline tools—profiles info and model of behaviour/trends (artificial intellgience + machine learning—available to airlines to direct rostering/planning + tools for other stakeholders (EAP, aeromedical examiner etc.) | |
| Wellbeing Pillar | Example | High Level Assessment H M L |
|---|---|---|
| Biological | Sleep, diet, exercise | |
| Psychological | Stress management, attitude, emotions, how feeling | |
| Social | Seeing and talking to other people, getting help when needed | |
| Overall rating | ||
| Wellbeing Pillar | Area | Current Status: How Am I Feeling/Doing? Rating? H M L | What I Am Going to Do? What Am I Doing? H M L | Overall Risk Rating H M L |
|---|---|---|---|---|
| Biological | Sleep and fatigue | |||
| Physical Exercise | ||||
| Diet | ||||
| Psychological | How feeling (stress) | |||
| Emotional stability and mood | ||||
| Social | Talking to others/seeing people | |||
| Overall rating | ||||
| Wellbeing Pillar | Area | Current Status | What I Am Going to Do? Weekly Plan—Target Actions for This Week | Review (Day 7)—How Did I Get on? Implications for Next Week. |
|---|---|---|---|---|
| Biological | Sleep | |||
| Physical Exercise | ||||
| Diet | ||||
| Psychological | Managing stress | |||
| Attitude and Mood | ||||
| Social | Talking to others, seeing people, getting help if needed |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cahill, J.; Cullen, P.; Anwer, S.; Gaynor, K.; Wilson, S. The Requirements for New Tools for Use by Pilots and the Aviation Industry to Manage Risks Pertaining to Work-Related Stress (WRS) and Wellbeing, and the Ensuing Impact on Performance and Safety. Technologies 2020, 8, 40. https://0-doi-org.brum.beds.ac.uk/10.3390/technologies8030040
Cahill J, Cullen P, Anwer S, Gaynor K, Wilson S. The Requirements for New Tools for Use by Pilots and the Aviation Industry to Manage Risks Pertaining to Work-Related Stress (WRS) and Wellbeing, and the Ensuing Impact on Performance and Safety. Technologies. 2020; 8(3):40. https://0-doi-org.brum.beds.ac.uk/10.3390/technologies8030040
Chicago/Turabian StyleCahill, Joan, Paul Cullen, Sohaib Anwer, Keith Gaynor, and Simon Wilson. 2020. "The Requirements for New Tools for Use by Pilots and the Aviation Industry to Manage Risks Pertaining to Work-Related Stress (WRS) and Wellbeing, and the Ensuing Impact on Performance and Safety" Technologies 8, no. 3: 40. https://0-doi-org.brum.beds.ac.uk/10.3390/technologies8030040