
A Design Study of Orthotic Shoe Based on Pain Pressure Measurement Using Algometer for Calcaneal Spur Patients

 , ,
, ,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Barrett, S.J.; O’Malley, R. Plantar fasciitis and other causes of heel pain. Am. Fam. Physician 1999, 59, 2200–2206. [Google Scholar]
- Zhou, B.; Zhou, Y.; Tao, X.; Yuan, C.; Tang, K. Classification of Calcaneal Spurs and Their Relationship with Plantar Fasciitis. J. Foot Ankle Surg. 2015, 54, 594–600. [Google Scholar] [CrossRef] [PubMed]
- Johal, K.S.; Milner, S.A. Plantar fasciitis and the calcaneal spur: Fact or fiction? Foot Ankle Surg. 2012, 18, 39–41. [Google Scholar] [CrossRef]
- Kuyucu, E.; Koçyiğit, F.; Erdil, M. The association of calcaneal spur length and clinical and functional parameters in plantar fasciitis. Int. J. Surg. 2015, 21, 28–31. [Google Scholar] [CrossRef] [PubMed]
- Malay, D.S. Plantar fasciitis and heel spur syndrome: A retrospective analysis. In Reconstructive Surgery of the Foot and Leg: Update ’96; Vickers, N.S., Ed.; Podiatry Institute Publishing: Tucker, GA, USA, 1996; pp. 39–43. [Google Scholar]
- Bartold, S.J. The plantar fascia as a source of pain—Biomechanics, presentation and treatment. J. Bodyw. Mov. Ther. 2004, 8, 214–226. [Google Scholar] [CrossRef]
- Brinks, A.; Koes, B.W.; Volkers, A.C.W.; Verhaar, J.A.N.; Bierma-Zeintra, S.M.A. Adverse effects of extra-articular corticosteroid injections: A systematic review. BMC Musculoskelet. Disord. 2010, 11, 206. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Turlik, M.; Donatelli, T.; Veremis, M. A comparison of shoe inserts in relieving mechanical heel pain. Foot 1999, 9, 84–87. [Google Scholar] [CrossRef] [Green Version]
- Thomas, J.L.; Christensen, J.C.; Kravitz, S.R.; Mendicino, R.W.; Schuberth, J.M.; Vanore, J.V.; Weil, L.S., Sr.; Zlotoff, H.J.; Bouché, R.; Baker, J.; et al. The Diagnosis and Treatment of Heel Pain: A Clinical Practice Guideline—Revision 2010. J. Foot Ankle Surg. 2010, 40, 329–340. [Google Scholar] [CrossRef]
- Jason Chia, K.K.; Suresh, S.; Kuah, A.; Ong, J.L.; Phua, J.M.; Seah, A.L. Comparative trial of the foot pressure patterns between corrective orthotics, formthotics, bone spur and flat insoles in patients with chronic plantar fasciitis. Ann. Acad. Med. Singap. 2009, 38, 869–875. [Google Scholar] [PubMed]
- Giddings, V.L.; Beaupré, G.S.; Whalen, R.T.; Carter, D.R. Calcaneal loading during walking and running. Med. Sci. Sports Exerc. 2000, 32, 627–634. [Google Scholar] [CrossRef]
- Özdemır, H.; Söyüncü, Y.; Özgörgen, M.; Dabak, K. Effects of Changes in Heel Fat Pad Thickness and Elasticity on Heel Pain. J. Am. Podiatr. Med. Assoc. 2004, 94, 47–52. [Google Scholar] [CrossRef]
- Sayed-Noor, A.S.; Englund, E.; Wretenberg, P.; Sjoden, G.O. Pressure-Pain Threshold Algometric Measurement in Patients with Greater Trochanteric Pain After Total Hip Arthroplasty. Clin. J. Pain 2008, 24, 232–236. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thomas, G.-N.; Lars, A.-N. Assessment of mechanisms in localized and widespread musculoskeletal pain. Nat. Rev. Rheumatol. 2010, 6, 599–606. [Google Scholar] [CrossRef]
- Walton, D.; MacDermid, J.; Nielson, W.; Teasell, R.; Nailer, T.; Maheu, P. A Descriptive Study of Pressure Pain Threshold at 2 Standardized Sites in People with Acute or Subacute Neck Pain. J. Orthop. Sports Phys. Ther. 2011, 41, 651–657. [Google Scholar] [CrossRef] [Green Version]
- Park, G.; Kim, C.W.; Park, S.B.; Kim, M.J.; Jang, S.H. Reliability and Usefulness of the Pressure Pain Threshold Measurement in Patients with Myofascial Pain. Ann. Rehabil. Med. 2011, 35, 412–417. [Google Scholar] [CrossRef] [Green Version]
- Özdolap, N.; Sarikaya, S.; Kokturk, F. Evaluation of Pain Pressure Threshold and Widespread Pain in Chronic Low Back Pain. FTR-Turk. Fiz. Tip ve Rehabil. Derg. 2014, 60, 32–36. [Google Scholar] [CrossRef]
- Mutlu, E.K.; Ozdincler, A.R. Reliability and responsiveness of algometry for measuring pressure pain threshold in patients with knee osteoarthritis. J. Phys. Ther. Sci. 2015, 27, 1961–1965. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saban, B.; Masharawi, Y. Pain Threshold Tests in Patients with Heel Pain Syndrome. Foot Ankle Int. 2016, 37, 730–736. [Google Scholar] [CrossRef]
- Sandro, R.; Pergine, V. Insole Foe Sports Shoes, Particularly for Golf. U.S. Patent 2008.0086909, 17 April 2008. [Google Scholar]
- Wibowo, D.B.; Harahap, R.; Widodo, A.; Haryadi, G.D.; Ariyanto, M. The effectiveness of raising the heel height of shoes to reduce heel pain in patients with calcaneal spurs. J. Phys. Ther. Sci. 2017, 29, 2068–2074. [Google Scholar] [CrossRef] [Green Version]
- Haryadi, G.D.; Wibowo, D.B.; Ariyanto, M.; Suprihanto, A. Digital Scanning Method for Evaluation of Dimensional Parameters and Identification of Foot Type. Indonesian Patent No. IDS000002253, 2 April 2019. [Google Scholar]
- Holy Redeemer. Pain Level Chart. Available online: http://www.holyredeemer.com/Uploads/Public/Documents/2011%20Pain%20Level%20Chart.pdf (accessed on 23 October 2020).
- Wagner Instruments. Wagner FPTX Series Economy Manual Pain Threshold Testers. Pain TestTM Algometer, USA. Available online: http://www.wagnerinstruments.com/products/PAIN-TEST-Algometers (accessed on 20 June 2021).
- World Health Organization. Obesity: Preventing and Managing the Global Epidemic; WHO: Geneva, Switzerland, 2000. [Google Scholar]
- Navarro-Flores, E.; Becerro-de-Bengoa-Vallejo, R.; Calvo-Lobo, C.; Losa-Iglesias, M.E.; Palomo-López, P.; Mazoteras-Pardo, V.; Romero-Morales, C.; López-López, D. Influence of foot pain on frailty symptoms in an elderly population: A case-control study. Sao Paulo Med. J. 2021, 139, 319–324. [Google Scholar] [CrossRef]
- Kennedy, S. Stepping Out—Designing Foot Orthotics. The O&P Edge. 2003. Available online: www.oandp.com/edge (accessed on 20 July 2021).
- Wibowo, D.B.; Suprihanto, A.; Caesarendra, W.; Khoeron, S.; Glowacz, A.; Irfan, M. A Simple Foot Plantar Pressure Measurement Platform System Using Force-Sensing Resistors. Appl. Syst. Innov. 2020, 3, 33. [Google Scholar] [CrossRef]
- Wibowo, D.B.; Widodo, A.; Haryadi, G.D.; Caesarendra, W.; Harahap, R. Effect of in-shoe foot orthosis contours on heel pain due to calcanea spur. Appl. Sci. 2019, 9, 493. [Google Scholar] [CrossRef] [Green Version]
- Navarro-Flores, E.; Losa-Iglesias, M.E.; Becerro-De-Bengoa-Vallejo, R.; López-López, D.; Rodríguez-Sanz, D.; Palomo-López, P.; Calvo-Lobo, C. Translation and Test–Retest of the Spanish Podiatry Health Questionnaire (PHQ-S). Int. J. Environ. Res. Public Health 2018, 15, 2205. [Google Scholar] [CrossRef] [PubMed] [Green Version]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
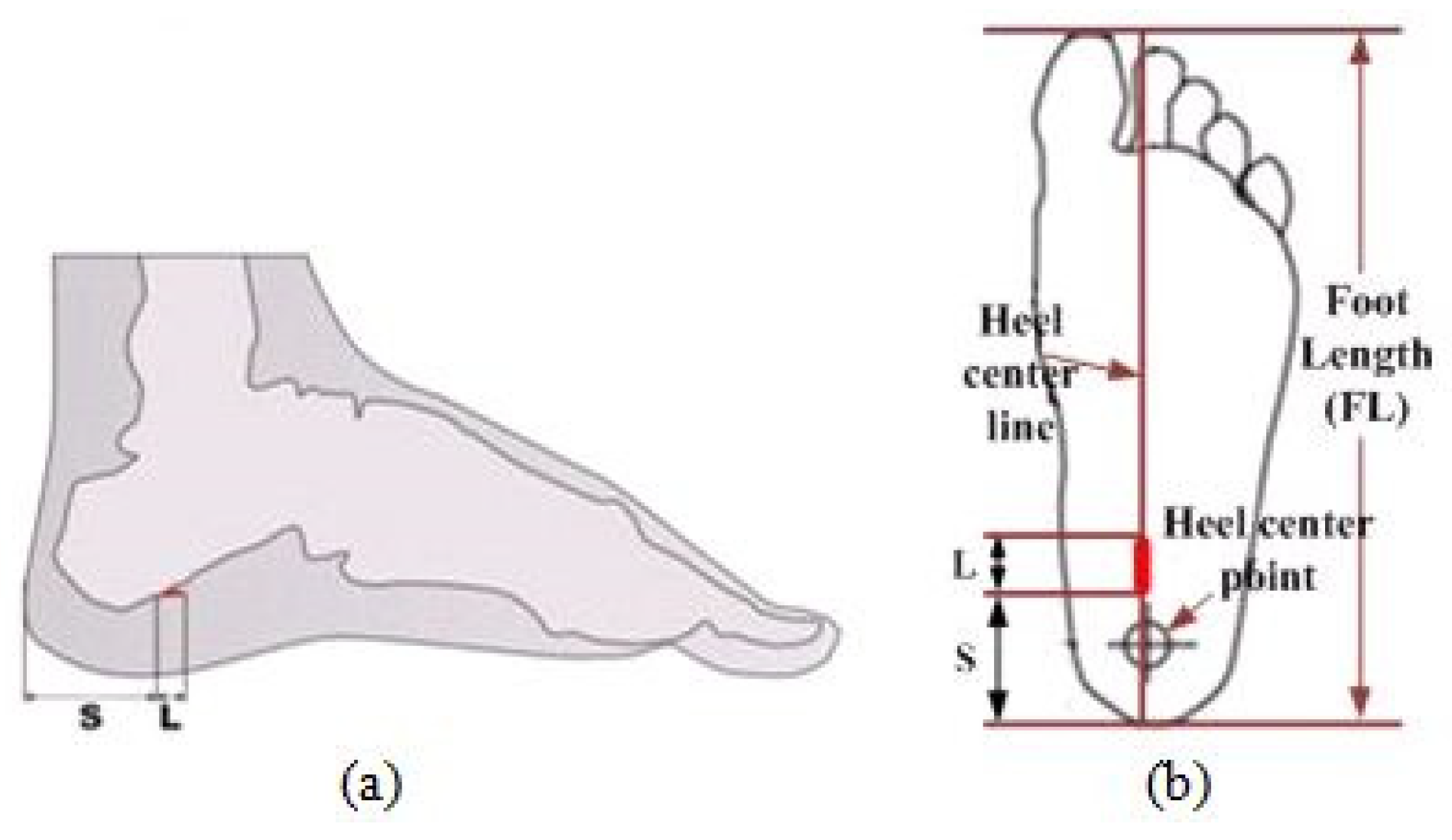
| Subj. No. | Gender | Age (years) | Weight (kg) | Height (cm) | Occupation | S Dimension (mm) | L Dimension (mm) | ||
|---|---|---|---|---|---|---|---|---|---|
| Left Foot | Right Foot | Left Foot | Right Foot | ||||||
| 1 | Female | 68 | 59.4 | 149 | Housewife | 38.0 | - | 5.0 | - |
| 2 | Male | 73 | 49.4 | 145 | Unemployed | 34.0 | 34.0 | 4.0 | 3.5 |
| 3 | Female | 60 | 49.3 | 157 | Housewife | - | 36.0 | - | 1.5 |
| 4 | Female | 65 | 50.3 | 153 | Housewife | - | 38.0 | - | 4.0 |
| 5 | Male | 47 | 57.5 | 152 | Factory worker | 39.0 | - | 5.0 | - |
| 6 | Male | 47 | 55.4 | 150 | Unemployed | 41.0 | 42.0 | 3.0 | 2.0 |
| 7 | Male | 50 | 56.2 | 157 | Factory worker | 36.0 | 35.0 | 2.0 | 4.0 |
| 8 | Male | 63 | 65.6 | 151 | Public servant | 39.0 | - | 7.0 | - |
| 9 | Female | 54 | 61.6 | 167 | Public servant | - | 30.0 | - | 6.0 |
| 10 | Female | 56 | 66.1 | 148 | Factory worker | 38.0 | 39.0 | 7.0 | 4.0 |
| 11 | Female | 38 | 51.3 | 152 | Unemployed | 34.0 | 34.0 | 1.5 | 2.0 |
| 12 | Female | 63 | 66.3 | 163 | Public servant | 35.0 | 34.0 | 2.0 | 4.0 |
| 13 | Female | 50 | 60.7 | 159 | Factory worker | 35.0 | 36.0 | 5.0 | 6.0 |
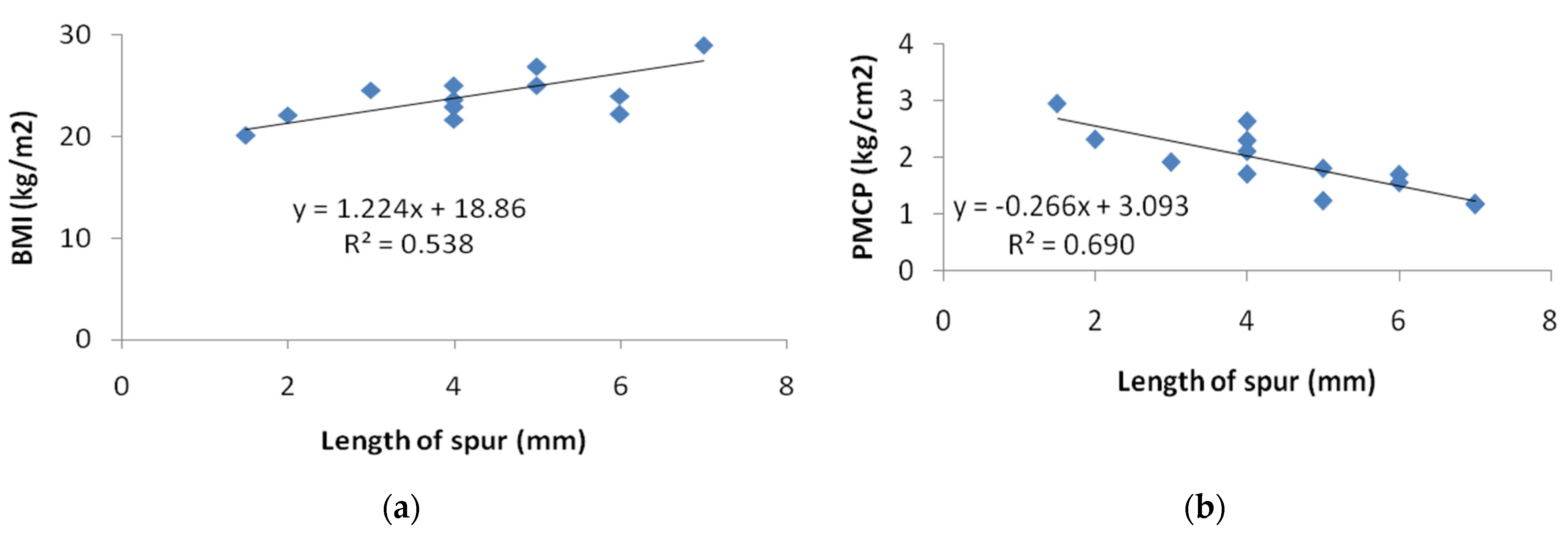
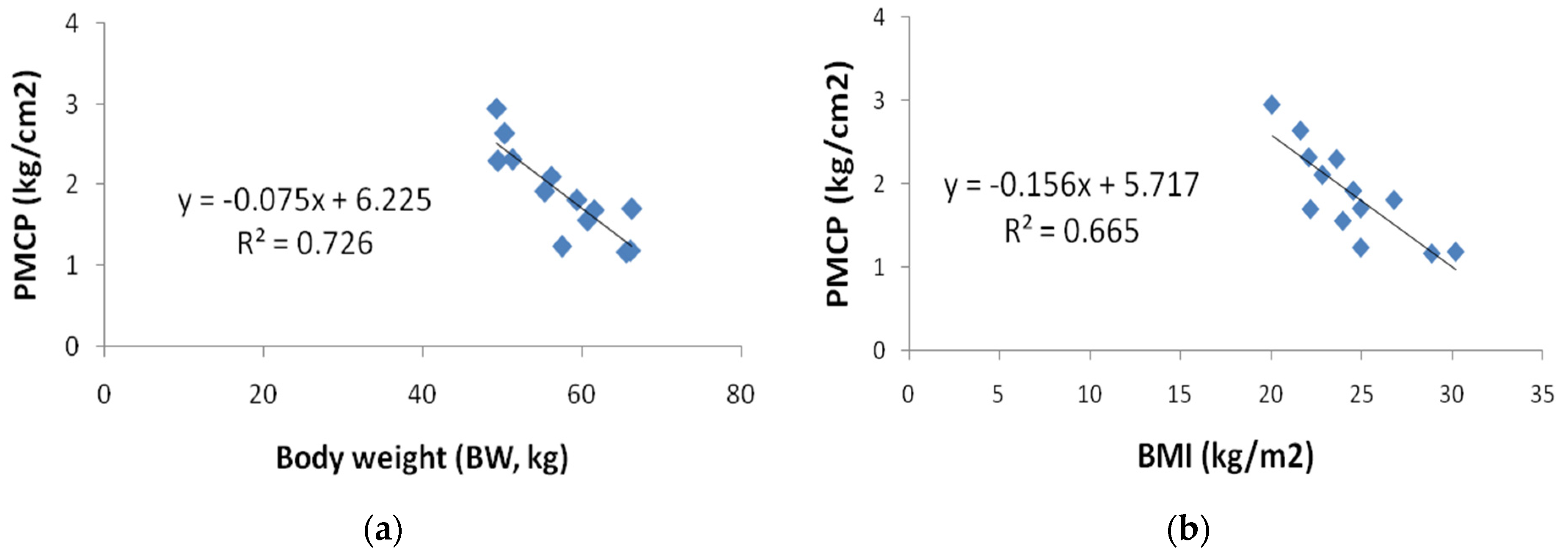
| Subject No. | BMI (kg/m2) | Occupation | Length of Spur (mm) | PMCP Test | ||
|---|---|---|---|---|---|---|
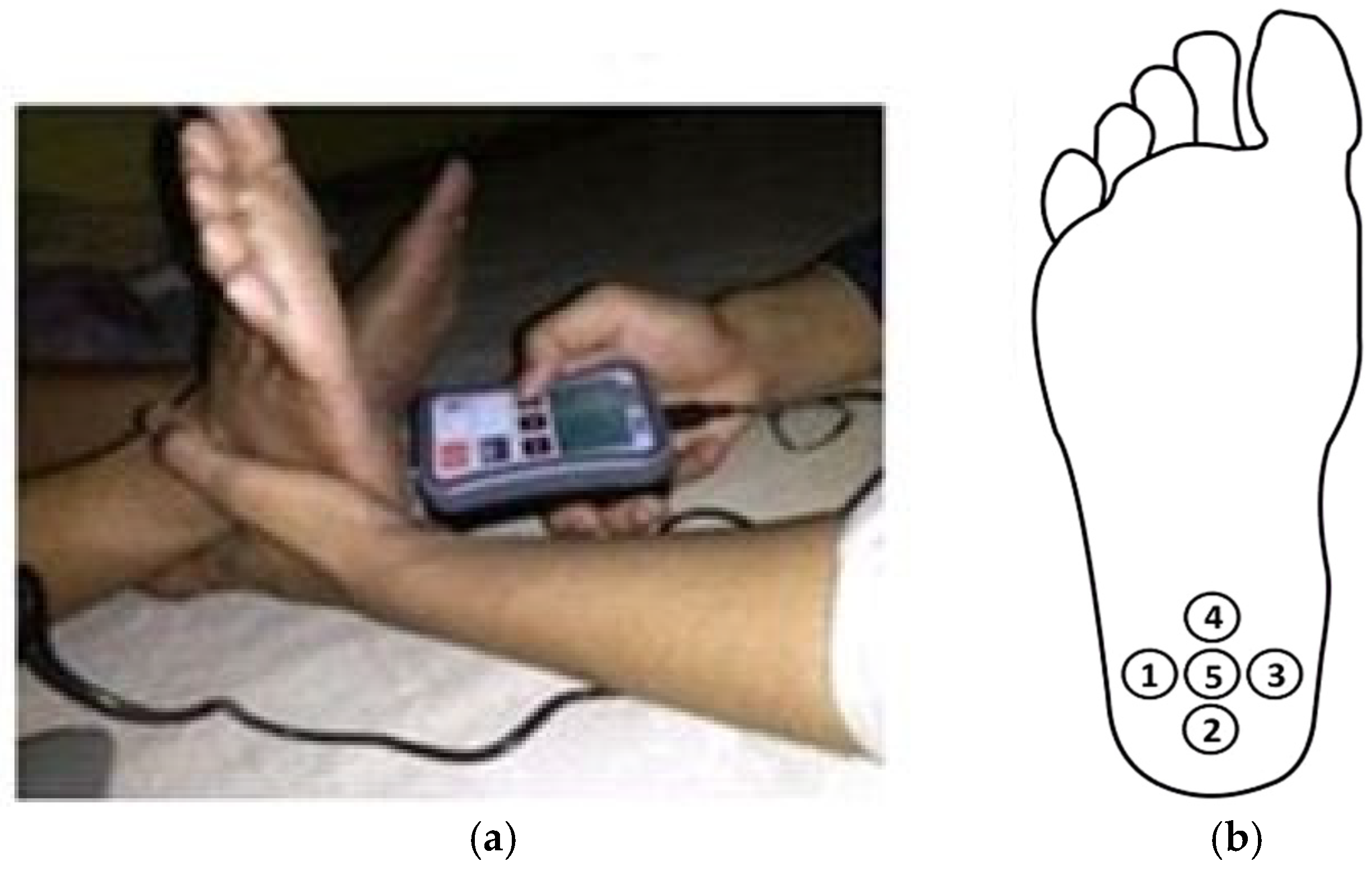
| Value (kg/cm2) | Foot Tested | Point Test Location | ||||
| 1 | 26.81 | Housewife | 5 | 1.81 | Left | 5 |
| 3 | 20.06 | 1.5 | 2.95 | Right | 4 | |
| 4 | 21.64 | 4 | 2.64 | Right | 4 | |
| 2 | 23.64 | Unemployed | 4 | 2.3 | Left | 5 |
| 6 | 24.56 | 3 | 1.92 | Left | 4 | |
| 11 | 22.1 | 2 | 2.32 | Right | 1 | |
| 5 | 24.97 | Worker | 5 | 1.24 | Left | 4 |
| 7 | 22.85 | 4 | 2.11 | Right | 4 | |
| 8 | 28.89 | 7 | 1.17 | Left | 2 | |
| 9 | 22.19 | 6 | 1.7 | Right | 1 | |
| 10 | 30.21 | 7 | 1.19 | Left | 4 | |
| 12 | 24.97 | 4 | 1.71 | Right | 1 | |
| 13 | 23.98 | 6 | 1.56 | Right | 1 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wibowo, D.B.; Suprihanto, A.; Caesarendra, W.; Glowacz, A.; Harahap, R.; Tadeusiewicz, R.; Kańtoch, E.; Abas, P.E. A Design Study of Orthotic Shoe Based on Pain Pressure Measurement Using Algometer for Calcaneal Spur Patients. Technologies 2021, 9, 62. https://0-doi-org.brum.beds.ac.uk/10.3390/technologies9030062
Wibowo DB, Suprihanto A, Caesarendra W, Glowacz A, Harahap R, Tadeusiewicz R, Kańtoch E, Abas PE. A Design Study of Orthotic Shoe Based on Pain Pressure Measurement Using Algometer for Calcaneal Spur Patients. Technologies. 2021; 9(3):62. https://0-doi-org.brum.beds.ac.uk/10.3390/technologies9030062
Chicago/Turabian StyleWibowo, Dwi Basuki, Agus Suprihanto, Wahyu Caesarendra, Adam Glowacz, Rudiansyah Harahap, Ryszard Tadeusiewicz, Eliasz Kańtoch, and Pg Emeroylariffion Abas. 2021. "A Design Study of Orthotic Shoe Based on Pain Pressure Measurement Using Algometer for Calcaneal Spur Patients" Technologies 9, no. 3: 62. https://0-doi-org.brum.beds.ac.uk/10.3390/technologies9030062