
Regenerative Potential of Enamel Matrix Protein Derivative and Acellular Dermal Matrix for Gingival Recession: A Systematic Review and Meta-Analysis

 ,
, 

Abstract
:1. Introduction
2. Methodology
2.1. Focused Question
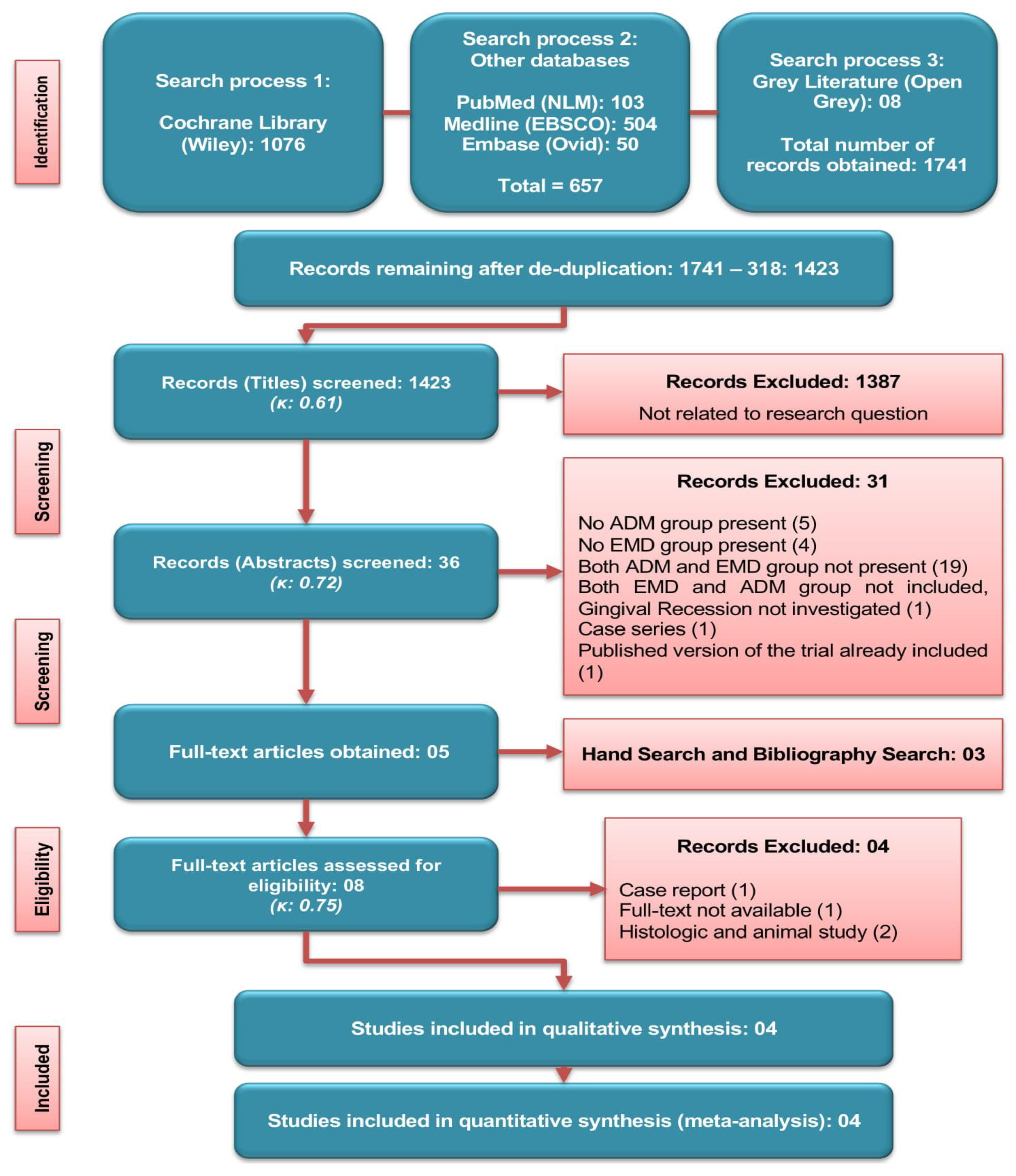
2.2. Literature Search
2.3. Literature Selection
- Controlled Clinical Trials (CCTs) or RCTs in which combination of EMD and ADM is compared to ADM only.
- Millers class I to III gingival recession of ≥2 mm (measured from cemento-enamel junction to the gingival margin).
- Mean follow-up period of ≥6-months.
- Class IV gingival recession.
- Laboratory or animal-based (in vitro and histologic) studies
- Reviews or systematic reviews, case series and case reports studies.
- Studies other than in English Language.
2.4. Literature Screening
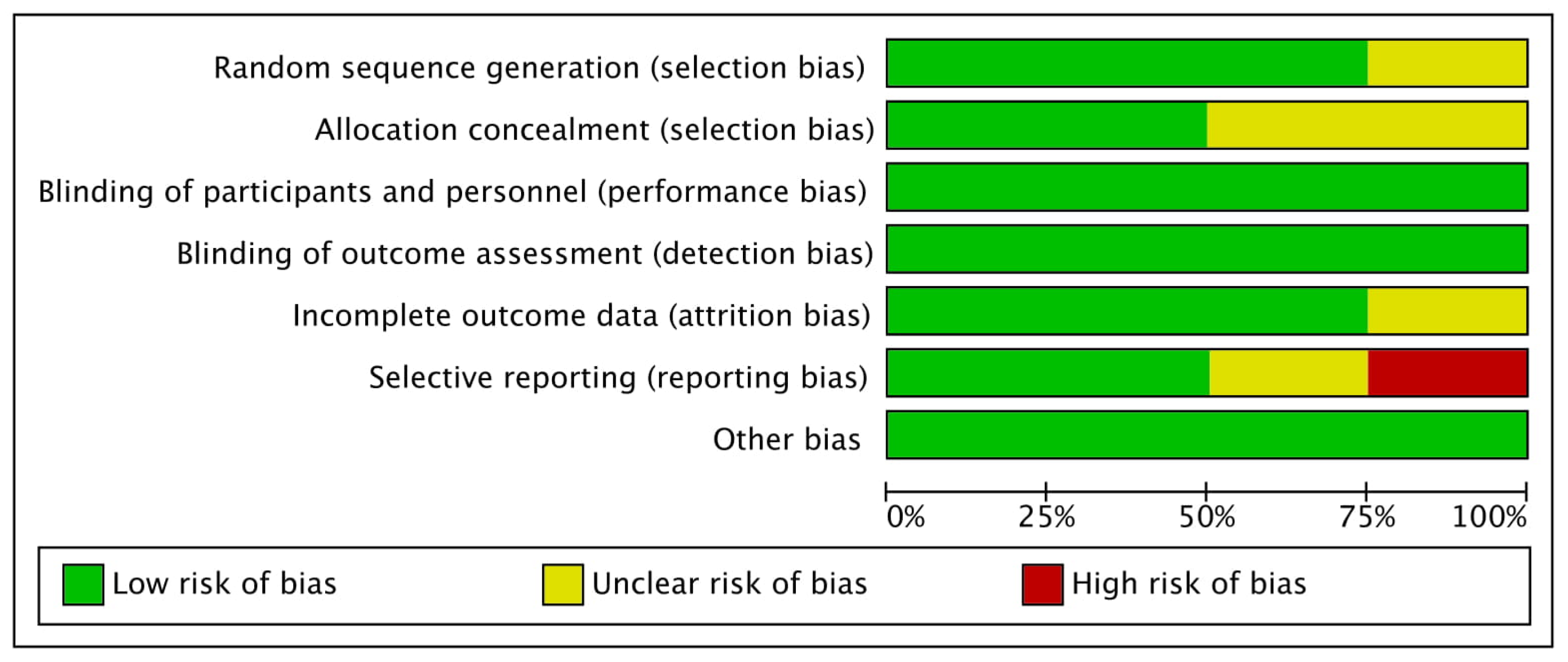
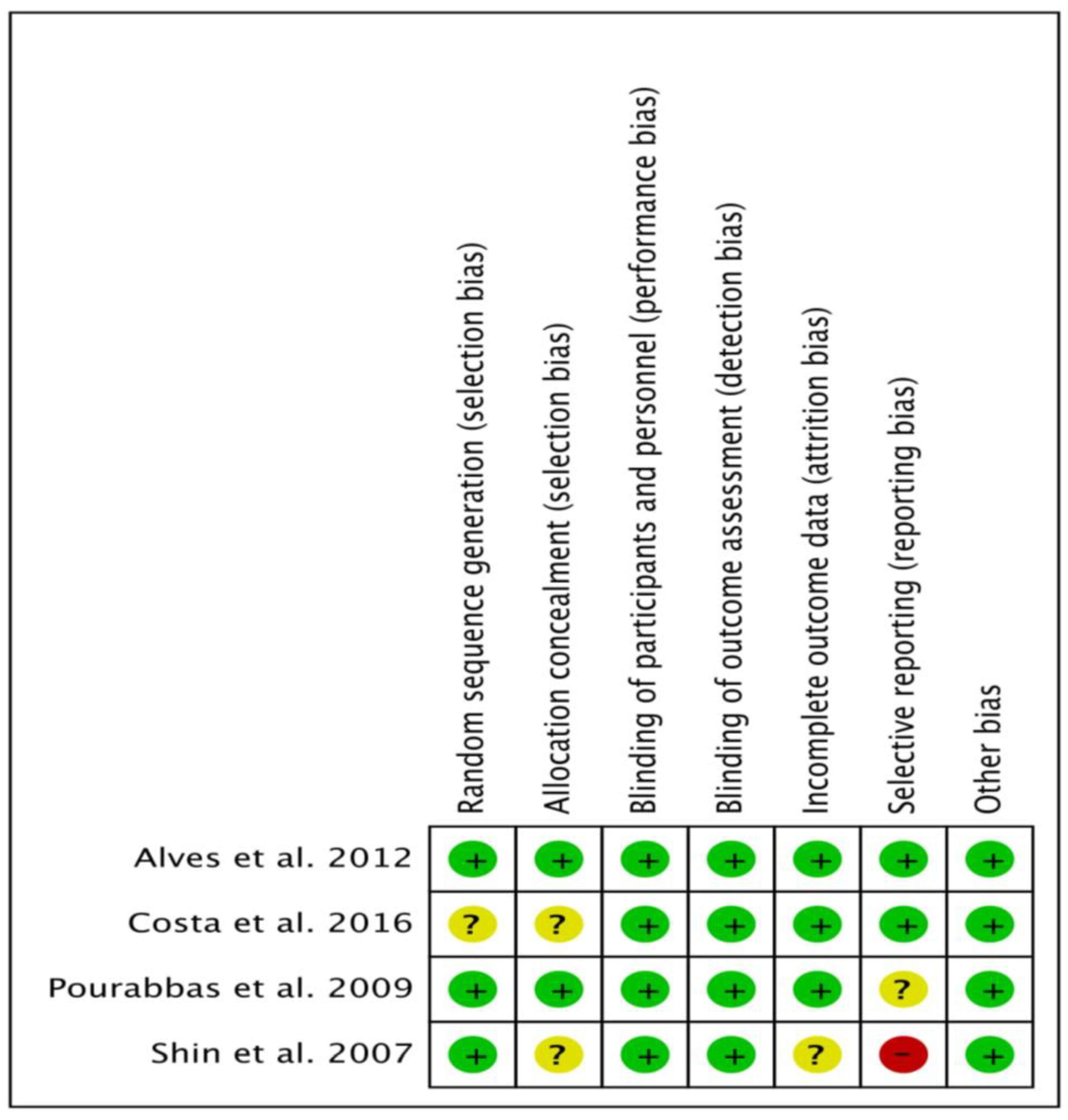
2.5. Assessment of Quality and Bias Risk
- Selection bias
- Performance bias
- Detection bias
- Attrition bias
- Reporting bias and
- Other types of bias
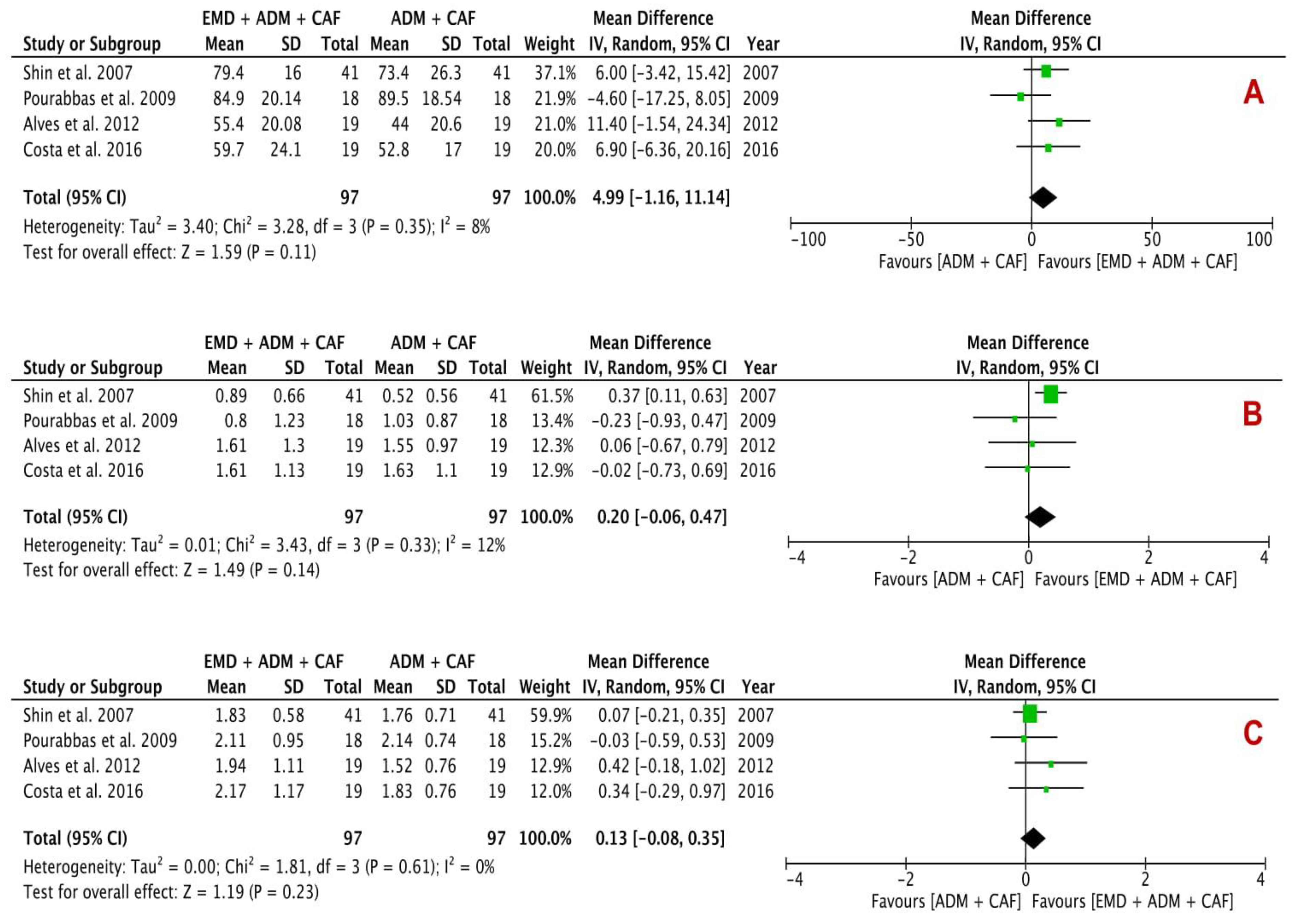
2.6. Data Analysis
2.7. Publication Bias
3. Results
3.1. Study Characteristics

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author/s | Reason for Exclusion |
|---|---|
| Saadoun [50] | Case report |
| Wallace [51] | No full-text available |
| de Oliveira et al. [52] Shirakata et al. [53] | Histologic and animal study |
| Authors | Study Design | Treatment | Antibiotics | Follow-Up (Months) | |
|---|---|---|---|---|---|
| Test Group | Control Group | ||||
| Shin et al. [46] | Single-center Split-mouth RCT Prospective | EMD + ADM + CAF | ADM + CAF | Y | 3, 6 |
| Pourabbas et al. [47] | Single-center Split-mouth RCT Prospective | EMD + ADM + CAF | ADM + CAF | Y | 2, 4, 6 |
| Alves et al. [48] | Single-center Split-mouth RCT Prospective | EMD + ADM + CAF | ADM + CAF | Y | 6 |
| Costa et al. [49] | Single-center Split-mouth RCT Prospective | EMD + ADM + CAF | ADM + CAF | Y | 3, 6, 12 |
3.2. Participant and Defect Characteristics
3.3. Quality Assessment of Included Trials
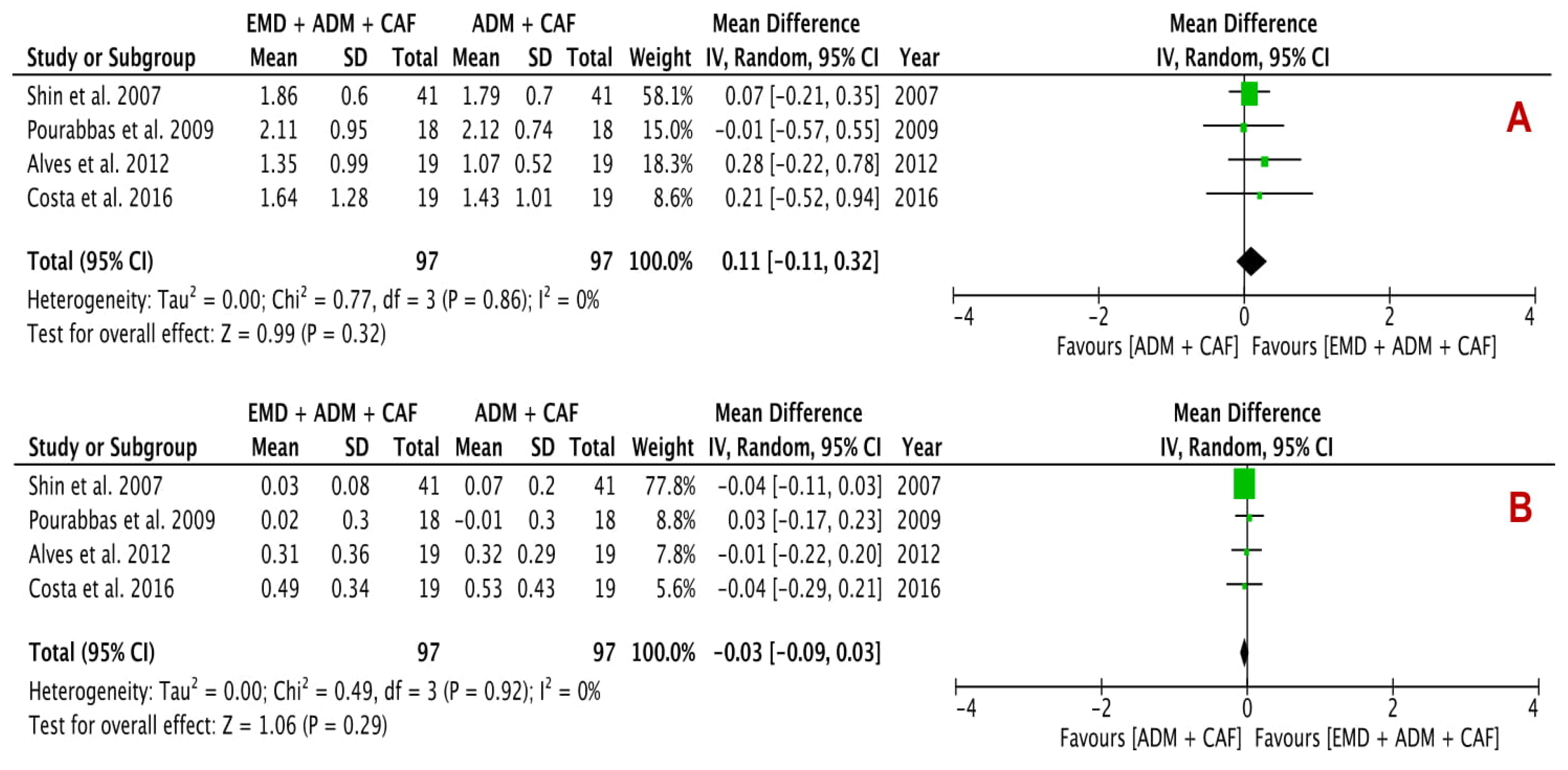
3.4. Effects of Primary and Secondary Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cortellini, P.; Bissada, N.F. Mucogingival conditions in the natural dentition: Narrative review, case definitions, and diagnostic considerations. J. Periodontol. 2018, 89, S204–S213. [Google Scholar] [CrossRef] [Green Version]
- Bouchard, P.; Malet, J.; Borghetti, A. Decision-making in aesthetics: Root coverage revisited. Periodontology 2000 2001, 27, 97–120. [Google Scholar] [CrossRef] [Green Version]
- Zucchelli, G.; Amore, C.; Sforza, N.; Montebugnoli, L.; De Sanctis, M. Bilaminar techniques for the treatment of recession-type defects. A comparative clinical study. J. Clin. Periodontol. 2003, 30, 862–870. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Stathopoulou, P.G. Tunneling Techniques for Root Coverage. Curr. Oral Health Rep. 2019, 6, 237–243. [Google Scholar] [CrossRef]
- Chambrone, L.; Chambrone, D.; Pustiglioni, F.E.; Chambrone, L.A.; Lima, L.A. Can subepithelial connective tissue grafts be considered the gold standard procedure in the treatment of Miller Class I and II recession-type defects? J. Dent. 2008, 36, 659–671. [Google Scholar] [CrossRef] [PubMed]
- Scheyer, E.T.; Sanz, M.; Dibart, S.; Greenwell, H.; John, V.; Kim, D.M.; Langer, L.; Neiva, R.; Rasperini, G. Periodontal soft tissue non–root coverage procedures: A consensus report from the AAP Regeneration Workshop. J. Periodontol. 2015, 86, S73–S76. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cairo, F.; Pagliaro, U.; Nieri, M. Treatment of gingival recession with coronally advanced flap procedures: A systematic review. J. Clin. Periodontol. 2008, 35, 136–162. [Google Scholar] [CrossRef]
- Griffin, T.J.; Cheung, W.S.; Zavras, A.I.; Damoulis, P.D. Postoperative complications following gingival augmentation procedures. J. Periodontol. 2006, 77, 2070–2079. [Google Scholar] [CrossRef]
- Rhee, P.H.; Friedman, C.D.; Ridge, J.A.; Kusiak, J. The use of processed allograft dermal matrix for intraoral resurfacing: An alternative to split-thickness skin grafts. Arch. Otolaryngol. Head Neck Surg. 1998, 124, 1201–1204. [Google Scholar] [CrossRef] [Green Version]
- Wainwright, D. Use of an acellular allograft dermal matrix (AlloDerm) in the management of full-thickness burns. Burns 1995, 21, 243–248. [Google Scholar] [CrossRef]
- Wainwright, D.; Madden, M.; Luterman, A.; Hunt, J.; Monafo, W.; Heimbach, D.; Kagan, R.; Sittig, K.; Dimick, A.; Herndon, D. Clinical evaluation of an acellular allograft dermal matrix in full-thickness burns. J. Burn Care Res. 1996, 17, 124–136. [Google Scholar] [CrossRef]
- Tal, H. Subgingival acellular dermal matrix allograft for the treatment of gingival recession: A case report. J Periodontol. 1999, 70, 1118–1124. [Google Scholar] [CrossRef]
- Harris, R.J. A comparative study of root coverage obtained with an acellular dermal matrix versus a connective tissue graft: Results of 107 recession defects in 50 consecutively treated patients. Int. J. Periodontics Restor. Dent. 2000, 20, 51–59. [Google Scholar]
- Aichelmann-Reidy, M.E.; Yukna, R.A.; Evans, G.H.; Nasr, H.F.; Mayer, E.T. Clinical evaluation of acellular allograft dermis for the treatment of human gingival recession. J. Periodontol. 2001, 72, 998–1005. [Google Scholar] [CrossRef]
- Harris, R.J. Acellular Dermal Matrix Used for Root Coverage: 18-Month Follow-up Observation. Int. J. Periodontics Restor. Dent. 2002, 22, 157–163. [Google Scholar]
- Woodyard, J.G.; Greenwell, H.; Hill, M.; Drisko, C.; Iasella, J.M.; Scheetz, J. The clinical effect of acellular dermal matrix on gingival thickness and root coverage compared to coronally positioned flap alone. J. Periodontol. 2004, 75, 44–56. [Google Scholar] [CrossRef]
- de Resende, D.R.B.; Greghi, S.L.A.; Siqueira, A.F.; Benfatti, C.A.M.; Damante, C.A.; Zangrando, M.S.R. Acellular dermal matrix allograft versus free gingival graft: A histological evaluation and split-mouth randomized clinical trial. Clin. Oral Investig. 2019, 23, 539–550. [Google Scholar] [CrossRef] [PubMed]
- Paolantonio, M.; Dolci, M.; Esposito, P.; D’Archivio, D.; Lisanti, L.; Di Luccio, A.; Perinetti, G. Subpedicle acellular dermal matrix graft and autogenous connective tissue graft in the treatment of gingival recessions: A comparative 1-year clinical study. J. Periodontol. 2002, 73, 1299–1307. [Google Scholar] [CrossRef] [Green Version]
- Tal, H.; Moses, O.; Zohar, R.; Meir, H.; Nemcovsky, C. Root coverage of advanced gingival recession: A comparative study between acellular dermal matrix allograft and subepithelial connective tissue grafts. J. Periodontol. 2002, 73, 1405–1411. [Google Scholar] [CrossRef]
- Cummings, L.C.; Kaldahl, W.B.; Allen, E.P. Histologic evaluation of autogenous connective tissue and acellular dermal matrix grafts in humans. J. Periodontol. 2005, 76, 178–186. [Google Scholar] [CrossRef] [PubMed]
- Harris, R.J. Gingival Augmentation with an Acellular Dermal Matrix: Human Histologic Evaluation of a Case-Placement of the Graft on Periosteum. Int. J. Periodontics Restor. Dent. 2004, 24, 379–385. [Google Scholar]
- Heijl, L. Periodontal regeneration with enamel matrix derivative in one human experimental defect. A case report. J. Clin. Periodontol. 1997, 24, 693–696. [Google Scholar] [PubMed]
- Sculean, A.; Chiantella, G.C.; Windisch, P.; Donos, N. Clinical and Histologic Evaluation of Human lntrabony Defects Treated with an Enamel Matrix Protein Derivative (Emdogain). Int. J. Periodontics Restor. Dent. 2000, 20, 375–381. [Google Scholar]
- Jepsen, S.; Heinz, B.; Jepsen, K.; Arjomand, M.; Hoffmann, T.; Richter, S.; Reich, E.; Sculean, A.; Gonzales, J.R.; Bödeker, R.H.; et al. A randomized clinical trial comparing enamel matrix derivative and membrane treatment of buccal Class II furcation involvement in mandibular molars. Part I: Study design and results for primary outcomes. J. Periodontol. 2004, 75, 1150–1160. [Google Scholar] [CrossRef] [Green Version]
- Francetti, L.; Trombelli, L.; Lombardo, G.; Guida, L.; Cafiero, C.; Roccuzzo, M.; Carusi, G.; Del Fabbro, M. Evaluation of efficacy of enamel matrix derivative in the treatment of intrabony defects: A 24-month multicenter study. Int. J. Periodontics Restor. Dent. 2005, 25, 461–473. [Google Scholar]
- Esposito, M.; Grusovin, M.G.; Papanikolaou, N.; Coulthard, P.; Worthington, H.V. Enamel matrix derivative (Emdogain) for periodontal tissue regeneration in intrabony defects. A Cochrane systematic review. Eur. J. Oral Implantol. 2009, 2, 247–266. [Google Scholar]
- Koop, R.; Merheb, J.; Quirynen, M. Periodontal regeneration with enamel matrix derivative in reconstructive periodontal therapy: A systematic review. J. Periodontol. 2012, 83, 707–720. [Google Scholar] [CrossRef]
- Shaikh, M.S.; Pisani, F.; De Vito, D.; Lone, M.A.; Almasri, M. Long-term Clinical Performance of Regeneration versus Conservative Surgery in the Treatment of Infra-bony Defects: A Systematic Review. J. Int. Acad. Periodontol. 2021, 23, 31–56. [Google Scholar]
- Del Pizzo, M.; Zucchelli, G.; Modica, F.; Villa, R.; Debernardi, C. Coronally advanced flap with or without enamel matrix derivative for root coverage: A 2-year study. J. Clin. Periodontol. 2005, 32, 1181–1187. [Google Scholar] [CrossRef]
- Gestrelius, S.; Andersson, C.; Lidström, D.; Hammarström, L.; Somerman, M. In vitro studies on periodontal ligament cells and enamel matrix derivative. J. Clin. Periodontol. 1997, 24, 685–692. [Google Scholar] [CrossRef]
- Nemcovsky, C.E.; Artzi, Z.; Tal, H.; Kozlovsky, A.; Moses, O. A multicenter comparative study of two root coverage procedures: Coronally advanced flap with addition of enamel matrix proteins and subpedicle connective tissue graft. J. Periodontol. 2004, 75, 600–607. [Google Scholar] [CrossRef]
- Mercado, F.; Hamlet, S.; Ivanovski, S. A 3-year prospective clinical and patient-centered trial on subepithelial connective tissue graft with or without enamel matrix derivative in Class I-II Miller recessions. J. Periodontal Res. 2019, 55, 296–306. [Google Scholar] [CrossRef]
- Hägewald, S.; Spahr, A.; Rompola, E.; Haller, B.; Heijl, L.; Bernimoulin, J.P. Comparative study of Emdogain® and coronally advanced flap technique in the treatment of human gingival recessions: A prospective controlled clinical study. J. Clin. Periodontol. 2002, 29, 35–41. [Google Scholar] [CrossRef]
- Trabulsi, M.; Oh, T.J.; Eber, R.; Weber, D.; Wang, H.L. Effect of enamel matrix derivative on collagen guided tissue regeneration-based root coverage procedure. J. Periodontol. 2004, 75, 1446–1457. [Google Scholar] [CrossRef]
- Alexiou, A.; Vouros, I.; Menexes, G.; Konstantinidis, A. Comparison of enamel matrix derivative (Emdogain) and subepithelial connective tissue graft for root coverage in patients with multiple gingival recession defects: A randomized controlled clinical study. Quintessence Int. 2017, 48, 381–389. [Google Scholar] [PubMed]
- Gapski, R.; Parks, C.A.; Wang, H.L. Acellular dermal matrix for mucogingival surgery: A meta-analysis. J. Periodontol. 2005, 76, 1814–1822. [Google Scholar] [CrossRef] [PubMed]
- Gallagher, S.I.; Matthews, D.C. Acellular dermal matrix and subepithelial connective tissue grafts for root coverage: A systematic review. J. Indian Soc. Periodontol. 2017, 21, 439–448. [Google Scholar]
- Lu, W.; Qi, G.; Ding, Z.; Li, X.; Qi, W.; He, F. Clinical efficacy of acellular dermal matrix for plastic periodontal and implant surgery: A systematic review. Int. J. Oral Maxillofac. Surg. 2019, 49, 1057–1066. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- McHugh, M.L. Interrater reliability: The kappa statistic. Biochemia medica: Biochem Med. 2012, 22, 276–282. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C.; et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. Br. Med. J. 2011, 343, d5928. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cochran, W.G. The combination of estimates from different experiments. Biometrics 1954, 10, 101–129. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef]
- Page, M.J.; Higgins, J.P.; Sterne, J.A. Assessing risk of bias due to missing results in a synthesis. Cochrane Handb. Syst. Rev. Interv. 2019, 349–374. [Google Scholar] [CrossRef]
- Egger, M.; Smith, G.D.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. Br. Med. J. 1997, 315, 629–634. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shin, S.H.; Cueva, M.A.; Kerns, D.G.; Hallmon, W.W.; Rivera-Hidalgo, F.; Nunn, M.E. A comparative study of root coverage using acellular dermal matrix with and without enamel matrix derivative. J. Periodontol. 2007, 78, 411–421. [Google Scholar] [CrossRef]
- Pourabbas, R.; Chitsazi, M.T.; Kosarieh, E.; Olyaee, P. Coronally advanced flap in combination with acellular dermal matrix with or without enamel matrix derivatives for root coverage. Indian J. Dent. Sci. 2009, 20, 320–325. [Google Scholar] [CrossRef]
- Alves, L.B.; Costa, P.P.; Scombatti de Souza, S.L.; de Moraes Grisi, M.F.; Palioto, D.B.; Taba, M., Jr.; Novaes, A., Jr. Acellular dermal matrix graft with or without enamel matrix derivative for root coverage in smokers: A randomized clinical study. J. Clin. Periodontol. 2012, 39, 393–399. [Google Scholar] [CrossRef] [PubMed]
- Costa, P.P.; Alves, L.B.; Souza, S.L.; Grisi, M.F.; Palioto, D.B.; Taba, M., Jr.; Novaes, A.B. Root Coverage in Smokers with Acellular Dermal Matrix Graft and Enamel Matrix Derivative: A 12-Month Randomized Clinical Trial. Int. J. Periodontics Restor. Dent. 2016, 36, 525–531. [Google Scholar] [CrossRef] [Green Version]
- Saadoun, A.P. Root coverage with Emdogain/AlloDerm: A new way to treat gingival recessions. Eur. J. Esthet. Dent. 2008, 3, 46–65. [Google Scholar] [PubMed]
- Wallace, S. Treating human gingival recession defects with acellular dermis matrix and enamel matrix derivative using coronally advanced flaps. Gen. Dent. 2014, 62, e12–e15. [Google Scholar]
- de Oliveira, C.A.; Spolidório, L.C.; Cirelli, J.A.; Marcantonio, R.A.C. Acellular dermal matrix allograft used alone and in combination with enamel matrix protein in gingival recession: Histologic study in dogs. Int. J. Periodontics Restor. Dent. 2005, 25, 595–603. [Google Scholar]
- Shirakata, Y.; Sculean, A.; Shinohara, Y.; Sena, K.; Takeuchi, N.; Bosshardt, D.; Noguchi, K. Healing of localized gingival recessions treated with a coronally advanced flap alone or combined with an enamel matrix derivative and a porcine acellular dermal matrix: A preclinical study. Clin. Oral Investig. 2016, 20, 1791–1800. [Google Scholar] [CrossRef]
- Hujoel, P.; DeRouen, T. Validity issues in split-mouth trials. J. Clin. Periodontol. 1992, 19, 625–627. [Google Scholar] [CrossRef]
- Heitz-Mayfield, L. Systemic antibiotics in periodontal therapy. Aust. Dent. J. 2009, 54, S96–S101. [Google Scholar] [CrossRef]
- Oswal, S.; Ravindra, S.; Sinha, A.; Manjunath, S. Antibiotics in periodontal surgeries: A prospective randomised cross over clinical trial. J. Indian Soc. Periodontol. 2014, 18, 570–574. [Google Scholar] [CrossRef]
- McGuire, M.K.; Cochran, D.L. Evaluation of human recession defects treated with coronally advanced flaps and either enamel matrix derivative or connective tissue. Part 2: Histological evaluation. J. Periodontol. 2003, 74, 1126–1135. [Google Scholar] [CrossRef] [PubMed]
- Carnio, J.; Camargo, P.M.; Kenney, E.B.; Schenk, R.K. Histological evaluation of 4 cases of root coverage following a connective tissue graft combined with an enamel matrix derivative preparation. J. Periodontol. 2002, 73, 1534–1543. [Google Scholar] [CrossRef] [PubMed]
- Shirakata, Y.; Nakamura, T.; Shinohara, Y.; Nakamura-Hasegawa, K.; Hashiguchi, C.; Takeuchi, N.; Imafuji, T.; Sculean, A.; Noguchi, K. Split-mouth evaluation of connective tissue graft with or without enamel matrix derivative for the treatment of isolated gingival recession defects in dogs. Clin. Oral Investig. 2019, 23, 3339–3349. [Google Scholar] [CrossRef]
- Sallum, E.A.; Pimentel, S.P.; Saldanha, J.B.; Nogueira-Filho, G.R.; Casati, M.Z.; Nociti, F.H., Jr.; Sallum, A.W. Enamel matrix derivative and guided tissue regeneration in the treatment of dehiscence-type defects: A histomorphometric study in dogs. J. Periodontol. 2004, 75, 1357–1363. [Google Scholar] [CrossRef] [PubMed]
- Fujita, T.; Yamamoto, S.; Ota, M.; Shibukawa, Y.; Yamada, S. Coverage of gingival recession defects using guided tissue regeneration with and without adjunctive enamel matrix derivative in a dog model. Int. J. Periodontics Restor. Dent. 2011, 31, 247–253. [Google Scholar]
- Pilloni, A.; Paolantonio, M.; Camargo, P.M. Root coverage with a coronally positioned flap used in combination with enamel matrix derivative: 18-month clinical evaluation. J. Periodontol. 2006, 77, 2031–2039. [Google Scholar] [CrossRef]
- Cheng, G.L.; Fu, E.; Tu, Y.K.; Shen, E.C.; Chiu, H.C.; Huang, R.Y.; Yuh, D.Y.; Chiang, C.Y. Root coverage by coronally advanced flap with connective tissue graft and/or enamel matrix derivative: A meta-analysis. J. Periodontal Res. 2015, 50, 220–230. [Google Scholar] [CrossRef]
- Modica, F.; Pizzo, M.D.; Roccuzzo, M.; Romagnoli, R. Coronally advanced flap for the treatment of buccal gingival recessions with and without enamel matrix derivative. A split-mouth study. J. Periodontol. 2000, 71, 1693–1698. [Google Scholar] [CrossRef] [PubMed]
- Discepoli, N.; Mirra, R.; Ferrari, M. Efficacy of Enamel Derivatives to Improve Keratinized Tissue as Adjunct to Coverage of Gingival Recessions: A Systematic Review and Meta-Analysis. Materials 2019, 12, 2790. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Górski, B.; Górska, R.; Wysokińska-Miszczuk, R.; Kaczyński, T. Tunnel technique with enamel matrix derivative in addition to subepithelial connective tissue graft compared with connective tissue graft alone for the treatment of multiple gingival recessions: A randomized clinical trial. Clin. Oral Investig. 2020, 24, 4475–4486. [Google Scholar] [CrossRef]
- Cueva, M.A.; Boltchi, F.E.; Hallmon, W.W.; Nunn, M.E.; Rivera-Hidalgo, F.; Rees, T. A comparative study of coronally advanced flaps with and without the addition of enamel matrix derivative in the treatment of marginal tissue recession. J. Periodontol. 2004, 75, 949–956. [Google Scholar] [CrossRef]
- Thoma, D.S.; Villar, C.C.; Carnes, D.L.; Dard, M.; Patricia Chun, Y.H.; Cochran, D.L. Angiogenic activity of an enamel matrix derivative (EMD) and EMD-derived proteins: An experimental study in mice. J. Clin. Periodontol. 2011, 38, 253–260. [Google Scholar] [CrossRef]
- Kasaj, A.; Meister, J.; Lehmann, K.; Stratul, S.; Schlee, M.; Stein, J.; Willershausen, B.; Schmidt, M. The influence of enamel matrix derivative on the angiogenic activity of primary endothelial cells. J. Periodontal Res. 2012, 47, 479–487. [Google Scholar] [CrossRef]
- Rodrigues, T.L.; Marchesan, J.T.; Coletta, R.D.; Novaes, A.B., Jr.; Grisi, M.F.D.M.; Souza, S.L.; Taba, M., Jr.; Palioto, D.B. Effects of enamel matrix derivative and transforming growth factor-β1 on human periodontal ligament fibroblasts. J. Clin. Periodontol. 2007, 34, 514–522. [Google Scholar] [CrossRef]
- Heng, N.H.; Zahlten, J.; Cordes, V.; Ong, M.M.A.; Goh, B.T.; N’Guessan, P.D.; Pischon, N. Effects of enamel matrix derivative and transforming growth factor-β1 on connective tissue growth factor in human periodontal ligament fibroblasts. J. Periodontol. 2015, 86, 569–577. [Google Scholar] [CrossRef] [PubMed]
- Rasperini, G.; Roccuzzo, M.; Francetti, L.; Acunzo, R.; Consonni, D.; Silvestri, M. Subepithelial connective tissue graft for treatment of gingival recessions with and without enamel matrix derivative: A multicenter, randomized controlled clinical trial. Int. J. Periodontics Restor. Dent. 2011, 31, 132–139. [Google Scholar]
- Miron, R.; Dard, M.; Weinreb, M. Enamel matrix derivative, inflammation and soft tissue wound healing. J. Periodontal Res. 2015, 50, 555–569. [Google Scholar] [CrossRef]
- Lindskog, S. Formation of intermediate cementum. I: Early mineralization of aprismatic enamel and intermediate cementum in monkey. J. Craniofac. Genet. Dev. Biol. 1982, 2, 147–160. [Google Scholar]
- Lindskog, S. Formation of intermediate cementum. II: A scanning electron microscopic study of the epithelial root sheath of Hertwig in monkey. J. Craniofac. Genet. Dev. Biol. 1982, 2, 161–169. [Google Scholar] [PubMed]
- Berlucchi, I.; Francetti, L.; Del Fabbro, M.; Testori, T.; Weinstein, R.L. Enamel matrix proteins (Emdogain) in combination with coronally advanced flap or subepithelial connective tissue graft in the treatment of shallow gingival recessions. Int. J. Periodontics Restor. Dent. 2002, 22, 583–594. [Google Scholar]
- Batista, E.L., Jr.; Batista, F.C.; Novaes, A.B., Jr. Management of soft tissue ridge deformities with acellular dermal matrix. Clinical approach and outcome after 6 months of treatment. J. Periodontol. 2001, 72, 265–273. [Google Scholar] [CrossRef]
- Mörmann, W.; Ciancio, S.G. Blood supply of human gingiva following periodontal surgery: A fluorescein angiographic study. J. Periodontol. 1977, 48, 681–692. [Google Scholar] [CrossRef] [PubMed]
- Retzepi, M.; Tonetti, M.; Donos, N. Comparison of gingival blood flow during healing of simplified papilla preservation and modified Widman flap surgery: A clinical trial using laser Doppler flowmetry. J. Clin. Periodontol. 2007, 34, 903–911. [Google Scholar] [CrossRef]
- Retzepi, M.; Tonetti, M.; Donos, N. Gingival blood flow changes following periodontal access flap surgery using laser Doppler flowmetry. J. Clin. Periodontol. 2007, 34, 437–443. [Google Scholar] [CrossRef] [PubMed]
- Baldi, C.; Pini-Prato, G.; Pagliaro, U.; Nieri, M.; Saletta, D.; Muzzi, L.; Cortellini, P. Coronally advanced flap procedure for root coverage. Is flap thickness a relevant predictor to achieve root coverage? A 19-case series. J. Periodontol. 1999, 70, 1077–1084. [Google Scholar] [CrossRef] [PubMed]
- Barros, R.R.; Novaes, A.B., Jr.; Grisi, M.F.; Souza, S.L.; Taba, M., Jr.; Palioto, D.B. A 6-month comparative clinical study of a conventional and a new surgical approach for root coverage with acellular dermal matrix. J. Periodontol. 2004, 75, 1350–1356. [Google Scholar] [CrossRef] [PubMed]
- Barros, R.R.; Novaes, A.B., Jr.; Grisi, M.F.; Souza, S.L.; Taba, M., Jr.; Palioto, D.B. New surgical approach for root coverage of localized gingival recession with acellular dermal matrix: A 12-month comparative clinical study. J. Esthet. Restor. Dent. 2005, 17, 156–163. [Google Scholar] [CrossRef] [PubMed]
- Zucchelli, G.; De Sanctis, M. Treatment of multiple recession-type defects in patients with esthetic demands. J. Periodontol. 2000, 71, 1506–1514. [Google Scholar] [CrossRef] [PubMed]





| Authors | Participant Characteristics | Defect Characteristics | |||||||
|---|---|---|---|---|---|---|---|---|---|
| n | Mean Age (Years) | Age Range (Years) | Gender (M/F) | Drop-Outs | Smoking | Number of Defects | Defect Type | Type of Tooth | |
| Shin et al. [46] | 14 | 45.4 | 23–62 | 8/6 | 0 | In | 82 | Miller I to III | Non-molars |
| Pourabbas et al. [47] | 15 | NR | 26–63 | 7/8 | 0 | Ex | 36 | Miller I and II | Non-molars |
| Alves et al. [48] | 20 | NR | 30–50 | 7/12 | 1 | In | 38 | Miller I and II | Non-molars |
| Costa et al. [49] | 19 | NR | 30–50 | NR | 0 | In | 38 | Miller I and II | Non-molars |
| Authors | RC (%) | KTW Change (mm) | REC Change (mm) | CAL Change (mm) | PD Change (mm) |
|---|---|---|---|---|---|
| Shin et al. [46] | T: 79.4 ± 16.0 | T: 0.89 ± 0.66 | T: 1.83 ± 0.58 | T: 1.86 ± 0.60 | T: 0.03 ± 0.08 |
| C: 73.4 ± 26.3 | C: 0.52 ± 0.56 | C: 1.76 ± 0.71 | C: 1.79 ± 0.70 | C: 0.07 ± 0.20 | |
| Pourabbas et al. [47] | T: 84.90 ± 20.14 | T: 0.8 ± 1.45 | T: 2.11 ± 1.37 | T: 2.11 ± 0.95 | T: 0.02 ± 0.30 |
| C: 89.5 ± 18.54 | C: 1.03 ± 1.53 | C: 2.14 ± 1.42 | C: 2.12 ± 0.74 | C: -0.01 ± 0.30 | |
| Alves et al. [48] | T: 55.4 ± 20.08 | T: 1.61 ± 1.30 | T: 1.94 ± 1.11 | T: 1.35 ± 0.99 | T: 0.31 ± 0.36 |
| C: 44 ± 20.6 | C: 1.55 ± 0.97 | C: 1.52 ± 0.76 | C: 1.07 ± 0.52 | C: 0.32 ± 0.29 | |
| Costa et al. [49] | T: 59.7 ± 24.1 | T: 1.61 ± 1.13 | T: 2.17 ± 1.17 | T: 1.64 ± 1.28 | T: 0.49 ± 0.34 |
| C: 52.8 ± 17.0 | C: 1.63 ± 1.10 | C: 1.83 ± 0.76 | C: 1.43 ± 1.01 | C: 0.53 ± 0.43 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shaikh, M.S.; Lone, M.A.; Matabdin, H.; Lone, M.A.; Soomro, A.H.; Zafar, M.S. Regenerative Potential of Enamel Matrix Protein Derivative and Acellular Dermal Matrix for Gingival Recession: A Systematic Review and Meta-Analysis. Proteomes 2021, 9, 11. https://0-doi-org.brum.beds.ac.uk/10.3390/proteomes9010011
Shaikh MS, Lone MA, Matabdin H, Lone MA, Soomro AH, Zafar MS. Regenerative Potential of Enamel Matrix Protein Derivative and Acellular Dermal Matrix for Gingival Recession: A Systematic Review and Meta-Analysis. Proteomes. 2021; 9(1):11. https://0-doi-org.brum.beds.ac.uk/10.3390/proteomes9010011
Chicago/Turabian StyleShaikh, Muhammad Saad, Mohid Abrar Lone, Hesham Matabdin, Muneeb Ahmed Lone, Azeem Hussain Soomro, and Muhammad Sohail Zafar. 2021. "Regenerative Potential of Enamel Matrix Protein Derivative and Acellular Dermal Matrix for Gingival Recession: A Systematic Review and Meta-Analysis" Proteomes 9, no. 1: 11. https://0-doi-org.brum.beds.ac.uk/10.3390/proteomes9010011