
The Effect of Early Applied Robot-Assisted Physiotherapy on Functional Independence Measure Score in Post-Myocardial Infarction Patients

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
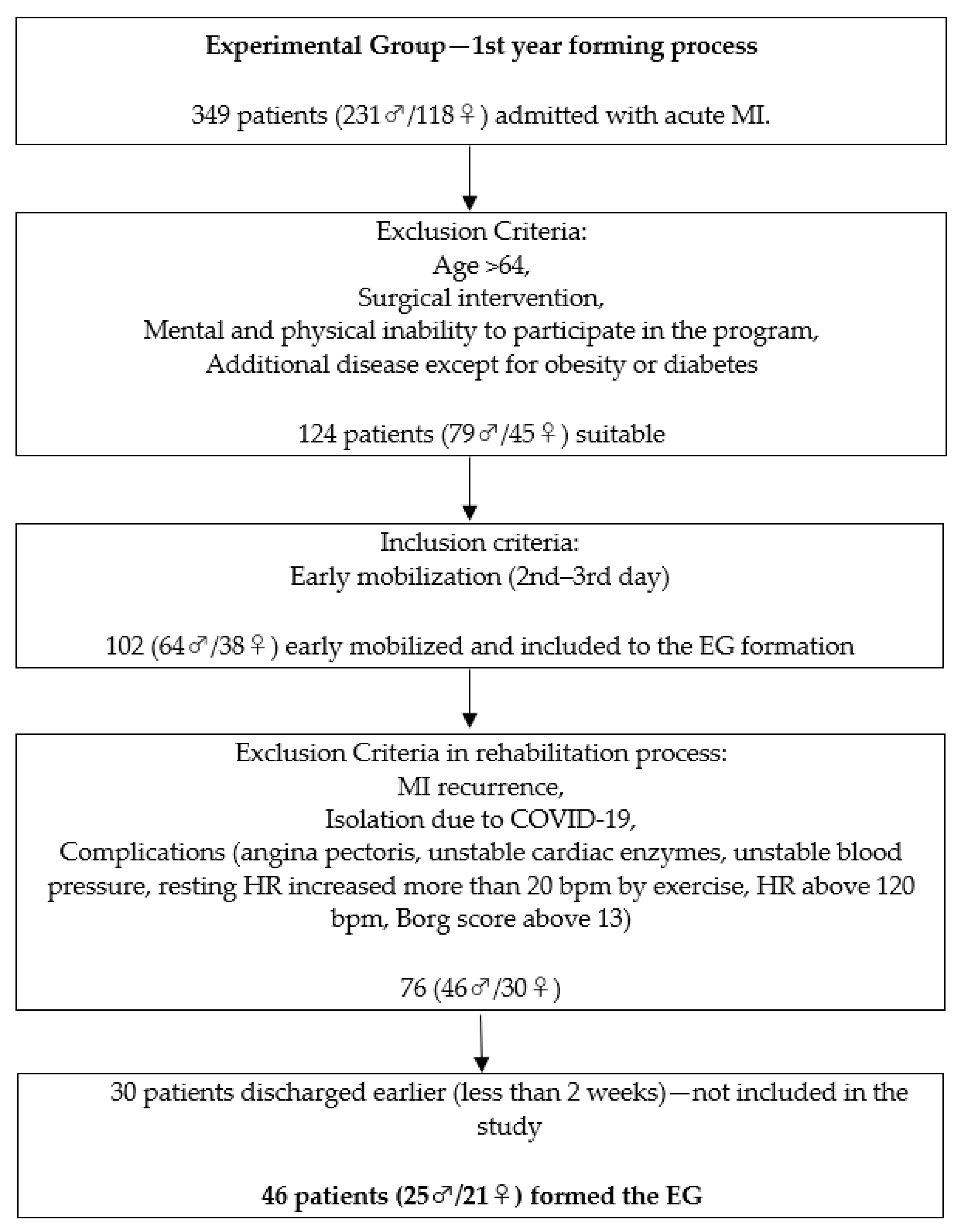
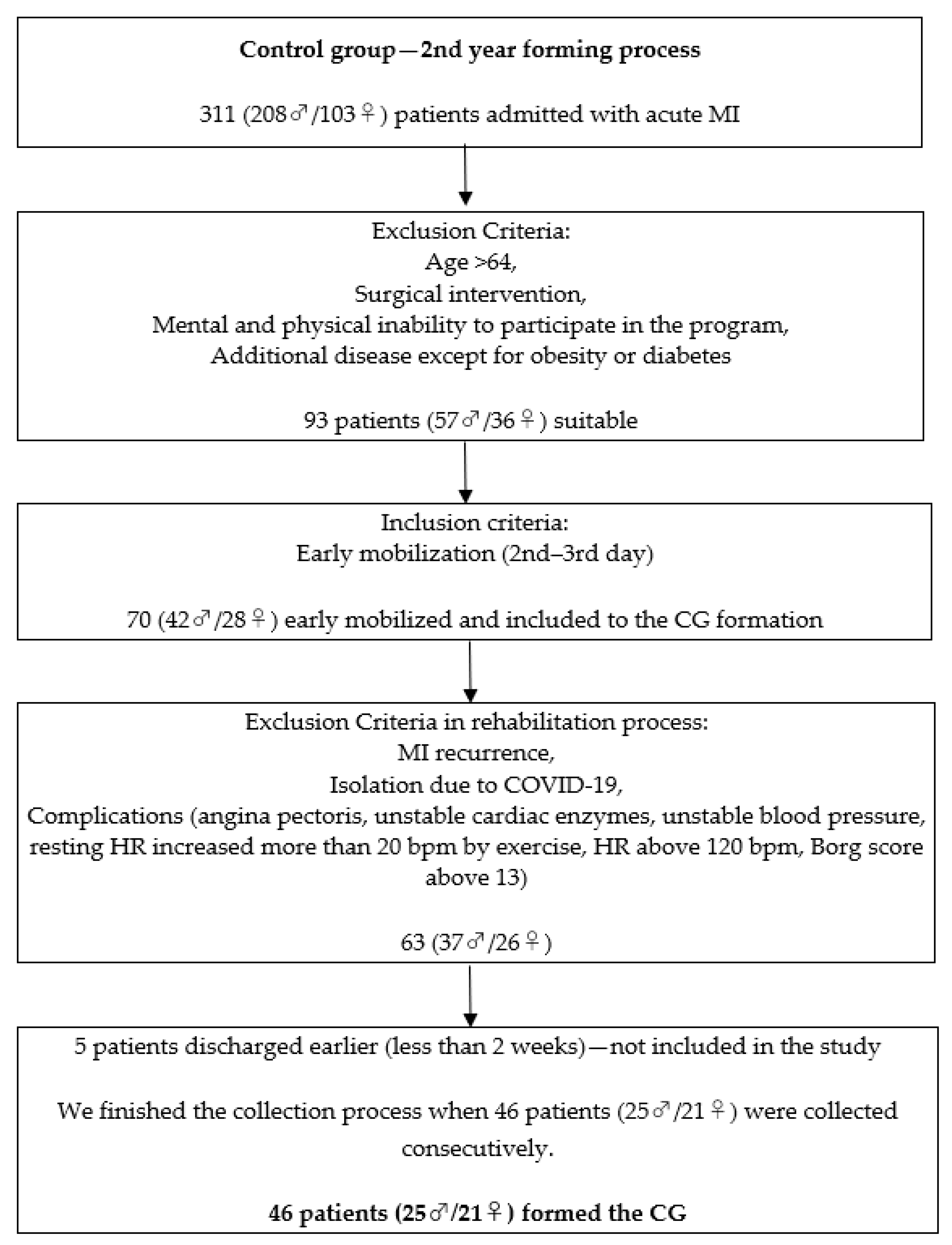
2.1. Subjects and Experimental Setup
- Individuals after MI, ICD codes—10: I21;
- Age < 64;
- At least 1 days of physiotherapy training before discharge;
- Mental and physical ability to participate in the program;
- No active angina pectoris, stable cardiac enzymes, stable blood pressure, pulse, and respiratory rate within a range that allowed the patient to exercise;
- Early mobilization (2nd–3rd day of hospitalization);
- No surgical intervention (catheterization not included).
- Exclusion criteria:
- Early discharge from the unit (less than 14 days of physiotherapy program);
- Complicated recovery;
- MI recurrence;
- Late mobilization (more than third day);
- Additional disease except for obesity or diabetes;
- Isolation due to COVID-19.
2.2. Intervention
2.3. Assessment
2.4. Sample Size and Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Jayaraj, J.C.; Davatyan, K.; Subramanian, S.S.; Priya, J. Epidemiology of myocardial infarction. Myocard. Infarct. 2019, 3, 10. [Google Scholar] [CrossRef]
- Fischerová, B. Specifika akutního infarktu myokardu ve stáří. Interní Med. Pro Praxi. 2008, 10, 110–112. [Google Scholar]
- Mumthas, A.; Abraham Varghese, V. Arrhythmia pattern in patients with acute myocardial infarction. IAIM 2019, 6, 142–148. [Google Scholar]
- Rosengren, A.; Wallentin, L.; Simoons, M.; Gitt, A.K.; Behar, S.; Battler, A.; Hasdai, D. Age, clinical presentation, and outcome of acute coronary syndromes in the Euroheart acute coronary syndrome survey. Eur. Heart J. 2006, 27, 789–795. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mozaffarian, D.; Benjamin, E.J.; Go, A.S.; Arnett, D.K.; Blaha, M.J.; Cushman, M.; de Ferranti, S.; Després, J.P.; Fullerton, H.J.; Howard, V.J.; et al. American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke statistics—2015 update: A report from the American Heart Association. Circulation 2015, 131, e29–e322. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dostál, O.; Bělohlávek, J.; Kovárník, P. Infarkt myokardu u starších pacientů. Kardiol. Rev. 2007, 9, 82–88. [Google Scholar]
- Fischbacher, C.M.; Bhopal, R.; Povey, C.; Steiner, M.; Chalmers, J.; Mueller, G.; Jamieson, J.; Knowles, D. Record linked retrospective cohort study of 4.6 million people exploring ethnic variations in disease: Myocardial infarction in South Asians. BMC Public Health 2007, 7, 142. [Google Scholar] [CrossRef] [Green Version]
- Berger, A.K.; Schulman, K.A.; Gersh, B.J.; Pirzada, S.; Breall, J.A.; Johnson, A.E.; Every, N.R. Primary coronary angioplasty vs thrombolysis for the management of acute myocardial infarction in elderly patients. Jama 1999, 28, 341–348. [Google Scholar] [CrossRef]
- Clark, A.M.; King-Shier, K.M.; Thompson, D.R.; Spaling, M.A.; Duncan, A.S.; Stone, J.A.; Jaglal, S.B.; Angus, J.E. A qualitative systematic review of influences on attendance at cardiac rehabilitation programs after referral. Am. Heart J. 2012, 164, 835–845. [Google Scholar] [CrossRef]
- Dietz, V. Body weight supported gait training: From laboratory to clinical setting. Brain Res. Bull. 2008, 30, 459–463. [Google Scholar] [CrossRef]
- Chaloupka, V. Rehabilitace nemocných po infarktu myokardu. Interní Med. Pro Praxi 2005, 6, 74–78. [Google Scholar]
- Želízko, M. Akutní infarkt myokardu s elevacemi ST úseku: Realita-výsledky registru NRKI (Sjezd ČKS 2007). In Proceedings of the XV Annual Congress of Czech Cardiologic Society, Brno, Czech Republic, 13–16 May 2007. [Google Scholar]
- Špinar, J.; Vítovec, J. Jak dobře žít s nemocným srdcem; Grada: Praha, Czech Republic, 2007; ISBN 978-80-247-1822-4. [Google Scholar]
- Mocan, M.; Mocan, B. Cardiac rehabilitation for older patients with cardiovascular pathology using robotic systems—A survey. Balneo Res. J. 2019, 10, 33–36. [Google Scholar] [CrossRef]
- Siverová, J.; Bužgová, R. Reminiscence v péči o seniory s demencí. Ceská a Slovenská Psychiatrie 2016, 112. Available online: https://0-scholar-google-com.brum.beds.ac.uk/scholar?hl=en&as_sdt=0%2C5&q=Siverov%C3%A1%2C+J.%3B+Bu%C5%BEgov%C3%A1%2C+R.+Reminiscence+v+p%C3%A9%C4%8Di+o+seniory+s+demenc%C3%AD&btnG= (accessed on 20 March 2022).
- Prokazova, P.R.; Piradov, M.A.; Ryabinkina, Y.V.; Kunzevich, G.I.; Gnedovskaya, E.V.; Popova, L.A. Robot-assisted therapy using the MOTOmed letto 2 for the integrated early rehabilitation of stroke patients admitted to the intensive care unit. Hum. Physiol. 2016, 42, 885–890. [Google Scholar] [CrossRef]
- De Beer, C.R.; Van Rooijen, A.J.; Pretorius, J.P.; Rheeder, P.; Becker, P.J.; Paruk, F. Muscle strength and endurance to predict successful extubation in mechanically ventilated patients: A pilot study evaluating the utility of upper-limb muscle strength and ergometry. S. Afr. J. Crit. Care 2018, 34, 44–49. [Google Scholar] [CrossRef] [Green Version]
- Ramírez, J.J.L.; García, E.D.; Valladares, Y.C.; García, M.A.F.; Capetillo, N.A.M.; Martínez, V.M.V. Eficacia del Thera Trainer Tigo 510 en el tratamiento rehabilitador de niños con parálisis cerebral. Revista Cubana de Medicina Física y Rehabilitación 2021, 13, 1–16. [Google Scholar]
- Meyer, S.; Verheyden, G.; Kempeneers, K.; Michielsen, M. Arm-hand boost therapy during inpatient stroke rehabilitation: A pilot randomized controlled trial. Front. Neurol. 2021, 12, 247. [Google Scholar] [CrossRef]
- Hamilton, B.B.; Laughlin, J.A.; Fiedler, R.C.; Granger, C.V. Interrater reliability of the 7-level functional independence measure (FIM). Scand. J. Rehabil. Med. 1994, 26, 115–119. [Google Scholar]
- Linacre, J.M.; Heinemann, A.W.; Wright, B.D.; Granger, C.V.; Hamilton, B.B. The structure and stability of the Functional Independence Measure. Arch. Phys. Med. Rehabil. 1994, 75, 127–132. [Google Scholar] [CrossRef]
- Ammann-Reiffer, C.; Bastiaenen, C.H.; Meyer-Heim, A.D.; van Hedel, H.J. Effectiveness of robot-assisted gait training in children with cerebral palsy: A bicenter, pragmatic, randomized, cross-over trial (PeLoGAIT). BMC Pediatrics 2017, 17, 64. [Google Scholar] [CrossRef] [Green Version]
- Schoenrath, F.; Markendorf, S.; Brauchlin, A.E.; Seifert, B.; Wilhelm, M.J.; Czerny, M.; Riener, R.; Falk, V.; Schmied, C.M. Robot-Assisted Training Early after Cardiac Surgery. J. Card. Surg. 2015, 30, 574–580. [Google Scholar] [CrossRef] [PubMed]
- Chang, W.H.; Kim, Y.H. Robot-assisted therapy in stroke rehabilitation. J. Stroke 2013, 15, 174. [Google Scholar] [CrossRef] [PubMed]
- Franceschini, M.; Mazzoleni, S.; Goffredo, M.; Pournajaf, S.; Galafate, D.; Criscuolo, S.; Agosti, M.; Posteraro, F. Upper limb robot-assisted rehabilitation versus physical therapy on subacute stroke patients: A follow-up study. J. Bodyw. Mov. Ther. 2020, 1, 194–208. [Google Scholar] [CrossRef] [PubMed]
- Belas dos Santos, M.; Barros de Oliveira, C.; Dos Santos, A.; Garabello Pires, C.; Dylewski, V.; Arida, R.M. A comparative study of conventional physiotherapy versus robot-assisted gait training associated to physiotherapy in individuals with ataxia after stroke. Behav. Neurol. 2018, 2018, 2892065. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, F.M.; Chaves, M.E.; Oliveira, V.C.; Martins, J.S.; Vimieiro, C.; Van Petten, A.M. Effect of Robot-Assisted Therapy on Participation of People with Limited Upper Limb Functioning: A Systematic Review with GRADE Recommendations. Occup. Ther. Int. 2021, 2021, 6649549. [Google Scholar] [CrossRef]
- Villafañe, J.H.; Taveggia, G.; Galeri, S.; Bissolotti, L.; Mullè, C.; Imperio, G.; Valdes, K.; Borboni, A.; Negrini, S. Efficacy of short-term robot-assisted rehabilitation in patients with hand paralysis after stroke: A randomized clinical trial. Hand 2018, 13, 95–102. [Google Scholar] [CrossRef] [Green Version]
- Hátlová, B.; Fleischmann, O.; Chytrý, V. Osobnost a aktivní životní styl seniorů ve věku 65–75 let. Psychol. A Její Kontexty (Psychol. Its Contexts) 2017, 8, 41–53. [Google Scholar]
- Gras, G.; Vitiello, V.; Yang, G.Z. Cooperative control of a compliant manipulator for robotic-assisted physiotherapy. In Proceedings of the 2014IEEE International Conference on Robotics and Automation (ICRA), 31 May–7 June, Hong Kong, China; pp. 339–346.
- Iosa, M.; Morone, G.; Bragoni, M.; De Angelis, D.; Venturiero, V.; Coiro, P.; Pratesi, L.; Paolucci, S. Driving electromechanically assisted Gait Trainer for people with stroke. J. Rehabil. Res. Dev. 2011, 48, 135–146. [Google Scholar] [CrossRef]
- Rocon, E.; Pons, J.L. Exoskeletons in Rehabilitation Robotics: Tremor Suppression; Springer: Berlin/Heidelberg, Germany, 2011; Volume 69. [Google Scholar]
- Glowinski, S.; Obst, M.; Majdanik, S.; Potocka-Banaś, B. Dynamic model of a humanoid exoskeleton of a lower limb with hydraulic actuators. Sensors 2021, 21, 3432. [Google Scholar] [CrossRef]
- Flemr, L. Pohybové Aktivity Ve Vědě a Praxis; Karolinum Press: Prague, Czech Republic, 2014; ISBN 978-80-246-2621-5. [Google Scholar]
- Bayon, C.; Raya, R.; Lara, S.L.; Ramirez, O.; Serrano, J.; Rocon, E. Robotic therapies for children with cerebral palsy: A systematic review. Transl. Biomed. 2016, 7, 44. [Google Scholar] [CrossRef] [Green Version]
- Baňárová, P.; Petríková-Rosiová, I.; Durcová, A. Ako motivovať ľudí k pravidelnému cvičeniu v rámci primárnej prevencie vzniku vertebrogénnych porúch funkčného pôvodu. Rehabilitácia 2016, 53, 25–34. [Google Scholar]



{kind=link}
{kind=link}
| Characteristic | CG | EG | Sig. (p-Value) |
|---|---|---|---|
| N (Male/Female) | 46 (25/21) | 46 (25/21) | - |
| Age (60.9 ± 2.32) | 60.8 ± 2.56 | 60.9 ± 2.08 | 0.96 |
| BMI (32.2 ± 4.84) | 31.8 ± 5.04 | 32.7 ± 4.63 | 0.21 |
| Diabetes duration (7.3 ± 3.48) | 7.1 ± 2.99 | 7.5 ± 3.93 | 0.63 |
| 1st day of rehabilitation program | |||
| Borg score (10.3 ± 1.76) | 10.5 ± 1.50 | 10.1 ± 1.97 | 0.38 |
| HR—rest (76.2 ± 8.29) | 77.7 ± 8.71 | 74.7 ± 7.66 | 0.14 |
| HR—effort (95.0 ± 5.80) | 96.0 ± 5.49 | 93.9 ± 5.97 | 0.10 |
| 7th day of the rehabilitation program | |||
| Borg score (10.5 ± 1.67) | 10.46 ± 1.70 | 10.59 ± 1.65 | 0.73 |
| HR—rest (75.0 ± 7.73) | 75.8 ± 7.64 | 74.15 ± 7.81 | 0.34 |
| HR—effort (96.5 ± 5.60) | 97.2 ± 5.11 | 95.9 ± 6.05 | 0.13 |
| FIM Category | Admission | 14 Days of Rehabilitation | Difference | Cohen’s d | Admission/14 Days of Rehabilitation Sig. (p-Value) |
|---|---|---|---|---|---|
| ADL (8–56) | |||||
| CG | 45.11 ± 3.29 | 48.11 ± 3.99 | 2.98 ± 2.24 | 0.82 | 0.00 |
| EG | 45.67 ± 3.91 | 50.67 ± 3.49 | 5.02 ± 2.82 | 1.36 | 0.00 |
| MOTOR (5–35) | |||||
| CG | 16.52 ± 1.07 | 18.70 ± 1.44 | 2.17 ± 0.93 | 1.71 | 0.00 |
| EG | 16.61 ± 1.45 | 20.09 ± 1.63 | 3.48 ± 1.09 | 2.25 | 0.00 |
| SOCIAL (5–35) | |||||
| CG | 30.09 ± 2.31 | 31.38 ± 1.96 | 1.28 ± 1.36 | 0.60 | 0.00 |
| EG | 30.02 ± 2.22 | 31.07 ± 2.21 | 1.04 ± 1.03 | 0.47 | 0.00 |
| TOTAL SCORE (18–126) | |||||
| CG | 91.72 ± 4.65 | 98.17 ± 4.82 | 6.46 ± 3.17 | 1.36 | 0.00 |
| EG | 92.30 ± 5.07 | 101.83 ± 4.91 | 9.52 ± 3.06 | 1.91 | 0.00 |
| FIM Category | Type III Sum of Squares | df | Mean Square | F | Sig. (p-Value) |
|---|---|---|---|---|---|
| ADL | |||||
| Time * Group | 46.00 | 1 | 46.00 | 13.99 | 0.00 * |
| Motor | |||||
| Time * Group | 19.57 | 1 | 19.57 | 38.24 | 0.00 * |
| Social | |||||
| Time * Group | 0.66 | 1 | 0.66 | 0.90 | 0.35 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bartík, P.; Vostrý, M.; Hudáková, Z.; Šagát, P.; Lesňáková, A.; Dukát, A. The Effect of Early Applied Robot-Assisted Physiotherapy on Functional Independence Measure Score in Post-Myocardial Infarction Patients. Healthcare 2022, 10, 937. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare10050937
Bartík P, Vostrý M, Hudáková Z, Šagát P, Lesňáková A, Dukát A. The Effect of Early Applied Robot-Assisted Physiotherapy on Functional Independence Measure Score in Post-Myocardial Infarction Patients. Healthcare. 2022; 10(5):937. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare10050937
Chicago/Turabian StyleBartík, Peter, Michal Vostrý, Zuzana Hudáková, Peter Šagát, Anna Lesňáková, and Andrej Dukát. 2022. "The Effect of Early Applied Robot-Assisted Physiotherapy on Functional Independence Measure Score in Post-Myocardial Infarction Patients" Healthcare 10, no. 5: 937. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare10050937