
Diaphragmatic Mobility and Chest Expansion in Patients with Scapulocostal Syndrome: A Cross-Sectional Study


Abstract
:
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants
2.3. Procedures
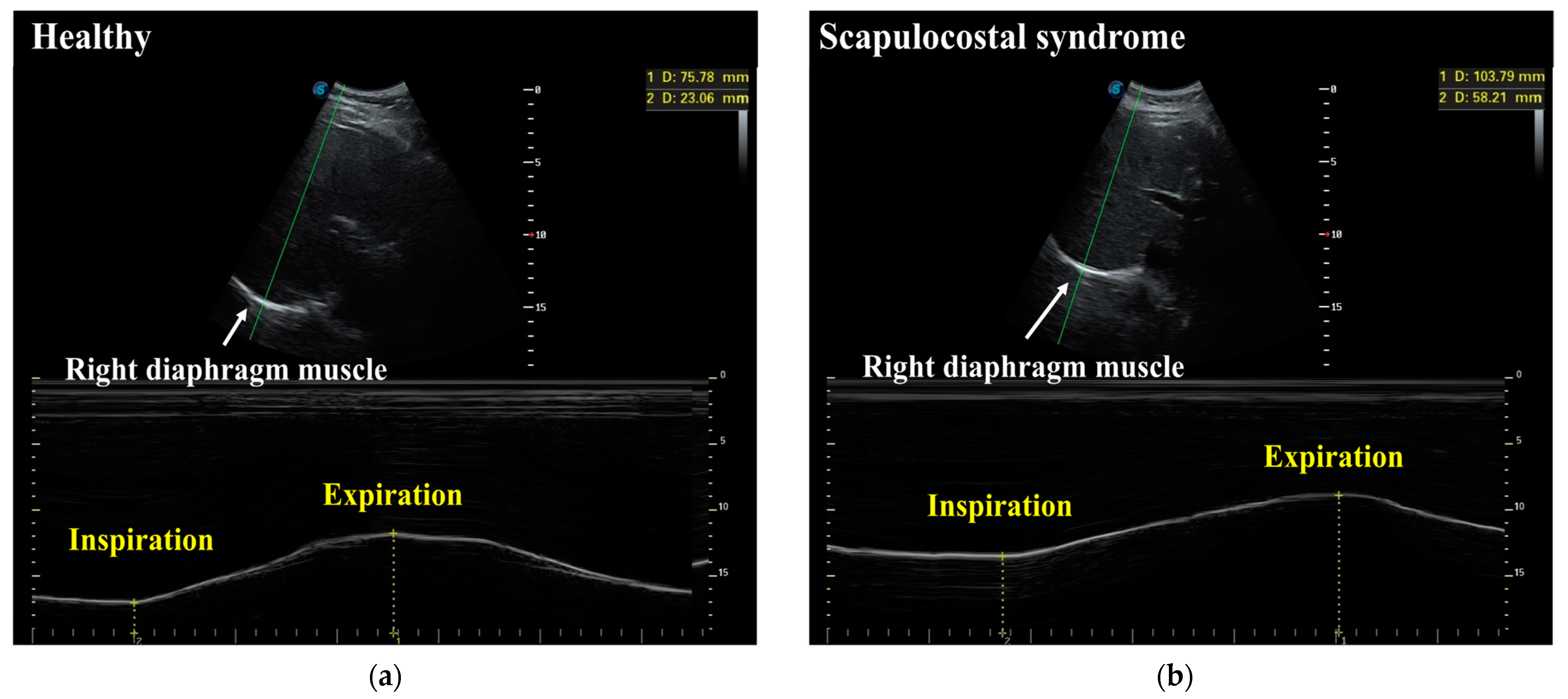
2.3.1. Diaphragmatic Mobility
2.3.2. Chest Expansion
2.4. Statistical Analysis
3. Results
3.1. Demographic Data and Baseline Clinical Characteristics
3.2. Diaphragmatic Mobility and Chest Expansion between the SCS Group and the Healthy Group
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Abrams, B. Scapulocostal syndrome. In Pain Management; Waldman, S.D., Ed.; Saunders: Philadelphia, PA, USA, 2011; Volume 2, pp. 588–592. [Google Scholar]
- Briggs, A.M.; Smith, A.J.; Straker, L.M.; Bragge, P. Thoracic spine pain in the general population: Prevalence, incidence and associated factors in children, adolescents and adults. A systematic review. BMC Musculoskelet. Disord. 2009, 10, 77. [Google Scholar] [CrossRef] [Green Version]
- Ozdemir, F.; Karaoglu, L.; Ozfirat, O. The lifetime and point prevalence of neck, upper back and low back pain of the people living in central Malatya with influencing factors. Agri J. Turk. Soc. Algol. 2013, 25, 27–35. [Google Scholar] [CrossRef]
- Paine, R.; Voight, M.L. The role of the scapula. Int. J. Sports Phys. Ther. 2013, 8, 617–629. [Google Scholar] [CrossRef]
- Taghizadeh, S.; Pirouzi, S.; Hemmati, L.; Khaledi, F.; Sadat, A. Clinical Evaluation of Scapular Positioning in Patients with Nonspecific Chronic Low Back Pain: A Case-Control Study. J. Chiropr. Med. 2017, 16, 195–198. [Google Scholar] [CrossRef] [Green Version]
- Yach, B.; Linens, S.W. The Relationship between Breathing Pattern Disorders and Scapular Dyskinesis. Athl. Train. Sports Health Care 2019, 11, 63–70. [Google Scholar] [CrossRef]
- Cobanoglu, G.; Zorlular, A.; Polat, E.A.; Akaras, E. The relationship between scapular and core muscle endurance in professional athletes. Ann. Med. Res. 2019, 26, 1295–1300. [Google Scholar]
- Bradley, H.; Esformes, J. Breathing pattern disorders and functional movement. Int. J. Sports Phys. Ther. 2014, 9, 28–39. [Google Scholar]
- Janssens, L.; Pijnenburg, M.; Claeys, K.; McConnell, A.K.; Troosters, T.; Brumagne, S. Postural Strategy and Back Muscle Ox- ygenation during Inspiratory Muscle Loading. Med. Sci. Sports Exerc. 2013, 45, 1355–1362. [Google Scholar] [CrossRef]
- Mohan, V.; Paungmali, A.; Sitilertpisan, P.; Hashim, U.F.; Mazlan, M.B.; Nasuha, T.N. Respiratory characteristics of individuals with non-specific low back pain: A cross-sectional study. Nurs. Health Sci. 2018, 20, 224–230. [Google Scholar] [CrossRef] [Green Version]
- Calvo-Lobo, C.; Almazán-Polo, J.; Becerro-De-Bengoa-Vallejo, R.; Losa-Iglesias, M.E.; Palomo-López, P.; Rodríguez-Sanz, D.; López-López, D. Ultrasonography comparison of diaphragm thickness and excursion between athletes with and without lumbopelvic pain. Phys. Ther. Sport 2019, 37, 128–137. [Google Scholar] [CrossRef]
- Ahmad, A.; Kamel, K.M.; Mohammed, R.G. Effect of forward head posture on diaphragmatic excursion in subjects with non-specific chronic neck pain. A case-control study. Physiother. Q. 2022, 28, 9–13. [Google Scholar]
- American Thoracic Society/European Respiratory Society. ATS/ERS Statement on Respiratory Muscle Testing. Am. J. Respir. Crit. Care Med. 2002, 166, 518–624. [Google Scholar] [CrossRef]
- Houston, J.G.; Fleet, M.; Cowan, M.D.; McMillan, N.C. Comparison of ultrasound with fluoroscopy in the Assessment of suspected hemidiaphragmatic movement abnormality. Clin. Radiol. 1995, 50, 95–98. [Google Scholar] [CrossRef]
- Wang, H.Y.; Chen, C.C.; Hsiao, S.F. Relationships between respiratory muscle strength and daily living function in children with cerebral palsy. Res. Dev. Disabil. 2012, 33, 1176–1182. [Google Scholar] [CrossRef]
- Reddy, R.S.; Alahmari, K.A.; Silvian, P.S.; Ahmad, I.A.; Kakarparthi, V.N.; Rengaramanujam, K. Reliability of Chest Wall Mobility and Its Correlation with Lung Functions in Healthy Nonsmokers, Healthy Smokers, and Patients with COPD. Can. Respir. J. 2019, 2019, 5175949. [Google Scholar] [CrossRef]
- Debouche, S.; Pitance, L.; Robert, A.; Liistro, G.; Reychler, G. Reliability and Reproducibility of Chest Wall Expansion Measurement in Young Healthy Adults. J. Manip. Physiol. Ther. 2016, 39, 443–449. [Google Scholar] [CrossRef]
- Tanrangka, N.; Bennett, M.; Bennett, S. The relationship between diaphragmatic mobility and chest wall expansion in cerebral palsy. Eur. Respir. J. 2018, 52, PA3893. [Google Scholar]
- Barnett, S.B.; Harr, G.R.T.; Rott, H.D.; Duck, F.A.; Maeda, K. International recommendations and guidelines for the safe use of diagnostic ultrasound in medicine. Ultrasound Med. Biol. 2000, 26, 355–366. [Google Scholar] [CrossRef]
- Matamis, D.; Soilemezi, E.; Tsagourias, M.; Akoumianaki, E.; Dimassi, S.; Boroli, F.; Richard, J.C.M.; Brochard, L. Sonographic evaluation of the diaphragm in critically ill patients. Technique and clinical applications. Intensive Care Med. 2013, 39, 801–810. [Google Scholar] [CrossRef]
- Boussuges, A.; Gole, Y.; Blanc, P. Diaphragmatic Motion Studied by M-Mode Ultrasonography. Chest 2009, 135, 391–400. [Google Scholar] [CrossRef]
- Mohan, V.; Hashim, U.F.; Md Dom, S.; Sitilerpisan, P.; Paungmali, A. Reliability of diaphragmatic mobility assessment using a real time ultrasound among non-specific low back pain. Bangladesh J. Med. Sci. 2017, 16, 443–447. [Google Scholar] [CrossRef] [Green Version]
- Simons, D.G.; Travell, J.G.; Simons, L.S. Myofascial pain and disfunction. In The Trigger Point Manual, 2nd ed.; Williams & Wilkins: Baltimore, MD, USA, 1999; Volume 1. [Google Scholar]
- Buttagat, V.; Eungpinichpong, W.; Chatchawan, U.; Arayawichanon, P. Herapeutic effects of traditional Thai massage on pain, muscle tension and anxiety in patients with scapulocostal syndrome: A randomized single-blinded pilot study. J. Bodyw. Mov. Ther. 2012, 16, 57–63. [Google Scholar] [CrossRef]
- Noh, D.K.; Lee, J.J.; You, J.H. Diaphragm Breathing Movement Measurement Using Ultrasound and Radiographic Imaging: A Concurrent Validity. Biomed. Mater. Eng. 2014, 24, 947–952. [Google Scholar] [CrossRef]
- Yamaguti, W.P.D.S.; Sakamoto, E.T.; Panazzolo, D.; Peixoto, C.D.C.; Cerri, G.G.; Albuquerque, A.L.P. Diaphragmatic mobility in healthy subjects during incentive spirometry with a flow-oriented device and with a volume-oriented device. J. Bras. Pneumol. 2010, 36, 738–745. [Google Scholar] [CrossRef] [Green Version]
- Bordoni, B.; Zanier, E. Anatomic connections of the diaphragm influence of respiration on the body system. J. Multidiscip. Healthc. 2013, 6, 281–291. [Google Scholar] [CrossRef] [Green Version]
- Waldman, S.D. Shoulder Pain Syndromes. In Atlas of Uncommon Pain Syndromes, 3rd ed.; Saunders Elsevier: Philadelphia, PA, USA, 2014; pp. 96–98. [Google Scholar]
- Fernández-De-Las-Peñas, C. Interaction between Trigger Points and Joint Hypomobility: A Clinical Perspective. J. Man. Manip. Ther. 2009, 17, 74–77. [Google Scholar] [CrossRef]
- Kapreli, E.; Vourazanis, E.; Strimpakos, N. Neck pain causes respiratory dysfunction. Med. Hypotheses 2008, 70, 1009–1013. [Google Scholar] [CrossRef]
- Hodges, P.W.; Butler, J.E.; McKenzie, D.K.; Gandevia, S.C. Contraction of the human diaphragm during rapid postural adjustments. J. Physiol. 1997, 505, 539–548. [Google Scholar] [CrossRef]
- Hodges, P.W.; Gandevia, S.C. Activation of the human diaphragm during a repetitive postural task. J. Physiol. 2000, 522, 165–175. [Google Scholar] [CrossRef]
- Kim, J.W.; Kang, M.H.; Oh, J.S. Patients with Low Back Pain Demonstrate Increased Activity of the Posterior Oblique Sling Muscle during Prone Hip Extension. PMR 2014, 6, 400–405. [Google Scholar] [CrossRef]
- Laudner, K.G.; Williams, J.G. The relationship between latissimus dorsi stiffness and altered scapular kinematics among asymptomatic collegiate swimmers. Phys. Ther. Sport 2013, 14, 50–53. [Google Scholar] [CrossRef]
- Schmerl, M.; Sangster, J. Clinical update. Scapulocostal syndrome. Australas. Chiropr. Osteopat. J. Chiropr. Osteopath. Coll. Australas. 2002, 10, 85–86. [Google Scholar]
- Key, J.; Clift, A.; Condie, F.; Harley, C. A model of movement dysfunction provides a classification system guiding diagnosis and therapeutic care in spinal pain and related musculoskeletal syndromes: A paradigm shift—Part 1. J. Bodyw. Mov. Ther. 2008, 12, 7–21. [Google Scholar] [CrossRef]
- Zafar, H.; Albarrati, A.; Alghadir, A.H.; Iqbal, Z.A. Effect of Different Head-Neck Postures on the Respiratory Function in Healthy Males. BioMed Res. Int. 2018, 2018, 4518269. [Google Scholar] [CrossRef] [Green Version]
- Lin, F.; Parthasarathy, S.; Taylor, S.J.; Pucci, D.; Hendrix, R.W.; Makhsous, M. Effect of Different Sitting Postures on Lung Capacity, Expiratory Flow, and Lumbar Lordosis. Arch. Phys. Med. Rehabil. 2006, 87, 504–509. [Google Scholar] [CrossRef]
- Chaitow, L. Functional movement and breathing dysfunction. J. Bodyw. Mov. Ther. 2016, 20, 455–456. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Characteristics | SCS Group (n = 29) | Healthy Group (n = 29) | p Value |
|---|---|---|---|
| Mean ± SD | Mean ± SD | ||
| Age (years) | 26.86 ± 4.22 | 26.86 ± 4.22 | 1.000 |
| Gender (female:male) | 17:12 | 17:12 | |
| Weight (kg) | 56.36 ± 8.57 | 56.17 ± 8.48 | 0.933 |
| Height (cm) | 164.00 ± 9.87 | 164.55 ± 9.32 | 0.828 |
| BMI (kg/m2) | 20.86 ± 1.46 | 20.64 ± 1.40 | 0.566 |
| Affected muscle | |||
| Levator scapulae (%) | 10 (34.48%) | 0 | |
| Upper trapezius (%) | 8 (27.59%) | 0 | |
| Rhomboid (%) | 11 (37.93) | 0 | |
| Exercise (yes:no) | 13:16 | 23:6 |
| Characteristics | SCS Group (n = 29) | Healthy Group (n = 29) | Difference (95% CI) | p Value |
|---|---|---|---|---|
| Mean ± SD | Mean ± SD | |||
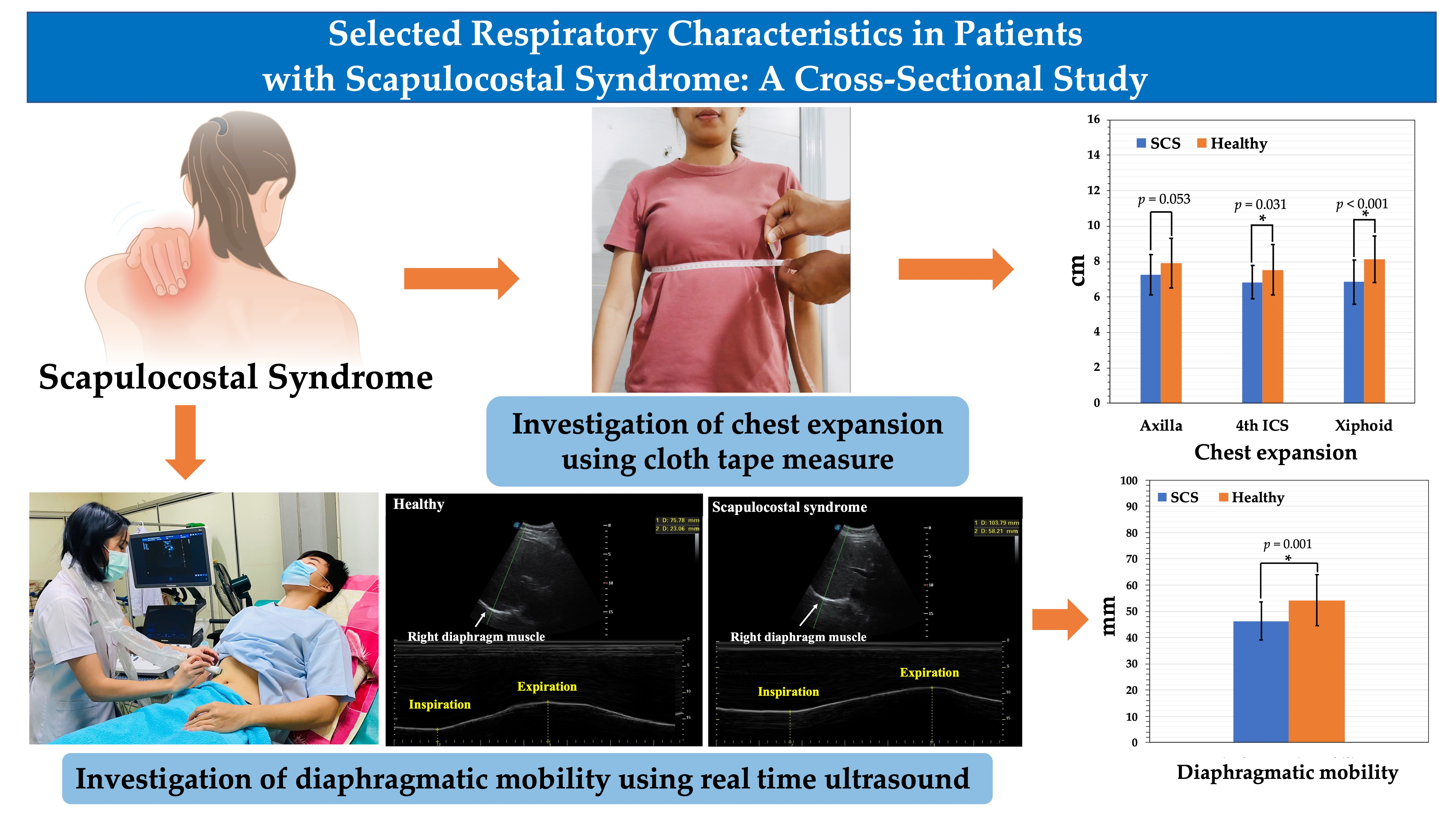
| Diaphragmatic mobility (mm) | 46.24 ± 7.26 | 54.18 ± 9.74 | −7.94 (−12.46 to −3.41) | 0.001 * |
| Chest expansion (cm) | ||||
| 1. Axilla: mean | 7.26 ± 1.13 | 7.92 ± 1.39 | −0.66 (−1.33 to 0.01) | 0.053 |
| 2. 4th ICS: mean | 6.83 ± 0.94 | 7.54 ± 1.43 | −0.71 (−1.34 to −0.07) | 0.031 * |
| 3. Xiphoid: mean | 6.86 ± 1.25 | 8.13 ± 1.32 | −1.27 (−1.95 to −0.60) | <0.001 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Srijessadarak, T.; Arayawichanon, P.; Kanpittaya, J.; Boonprakob, Y. Diaphragmatic Mobility and Chest Expansion in Patients with Scapulocostal Syndrome: A Cross-Sectional Study. Healthcare 2022, 10, 950. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare10050950
Srijessadarak T, Arayawichanon P, Kanpittaya J, Boonprakob Y. Diaphragmatic Mobility and Chest Expansion in Patients with Scapulocostal Syndrome: A Cross-Sectional Study. Healthcare. 2022; 10(5):950. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare10050950
Chicago/Turabian StyleSrijessadarak, Thanaporn, Preeda Arayawichanon, Jaturat Kanpittaya, and Yodchai Boonprakob. 2022. "Diaphragmatic Mobility and Chest Expansion in Patients with Scapulocostal Syndrome: A Cross-Sectional Study" Healthcare 10, no. 5: 950. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare10050950