
Adaptation and Psychometric Evidence of the ARABIC Version of the Diabetes Self-Management Questionnaire (A-DSMQ)


 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Collection
2.2. Instruments
2.2.1. Socio-Demographic Questionnaire and HbA1C
2.2.2. Arabic Version of the Diabetes Self-Management Questionnaire (A-DSMQ)
2.2.3. International Physical Activity Questionnaire (IPAQ)
2.3. Procedure
2.4. Statistical Analysis
3. Results
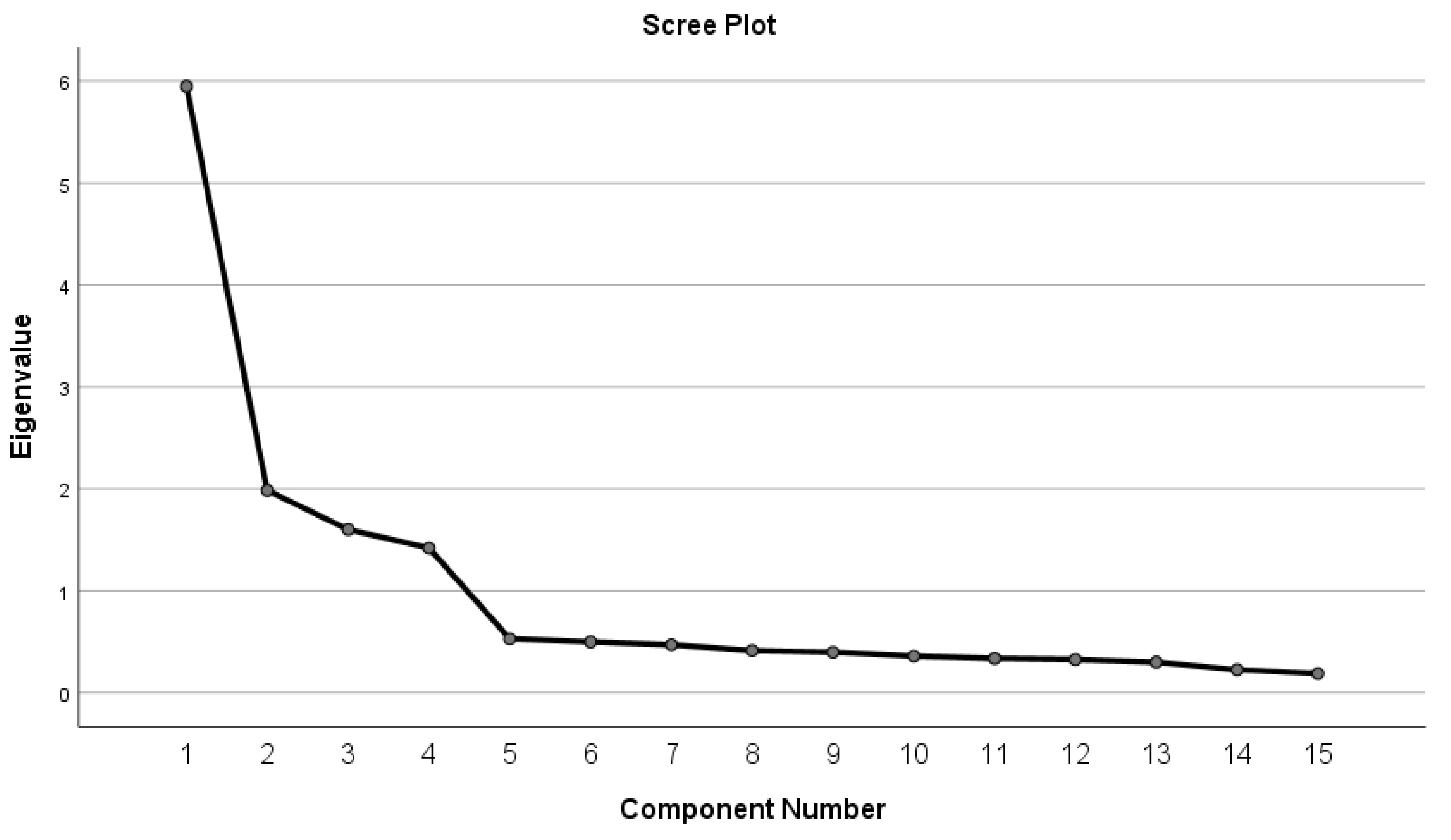
3.1. Descriptive Statistics and PCA
3.2. Reliability
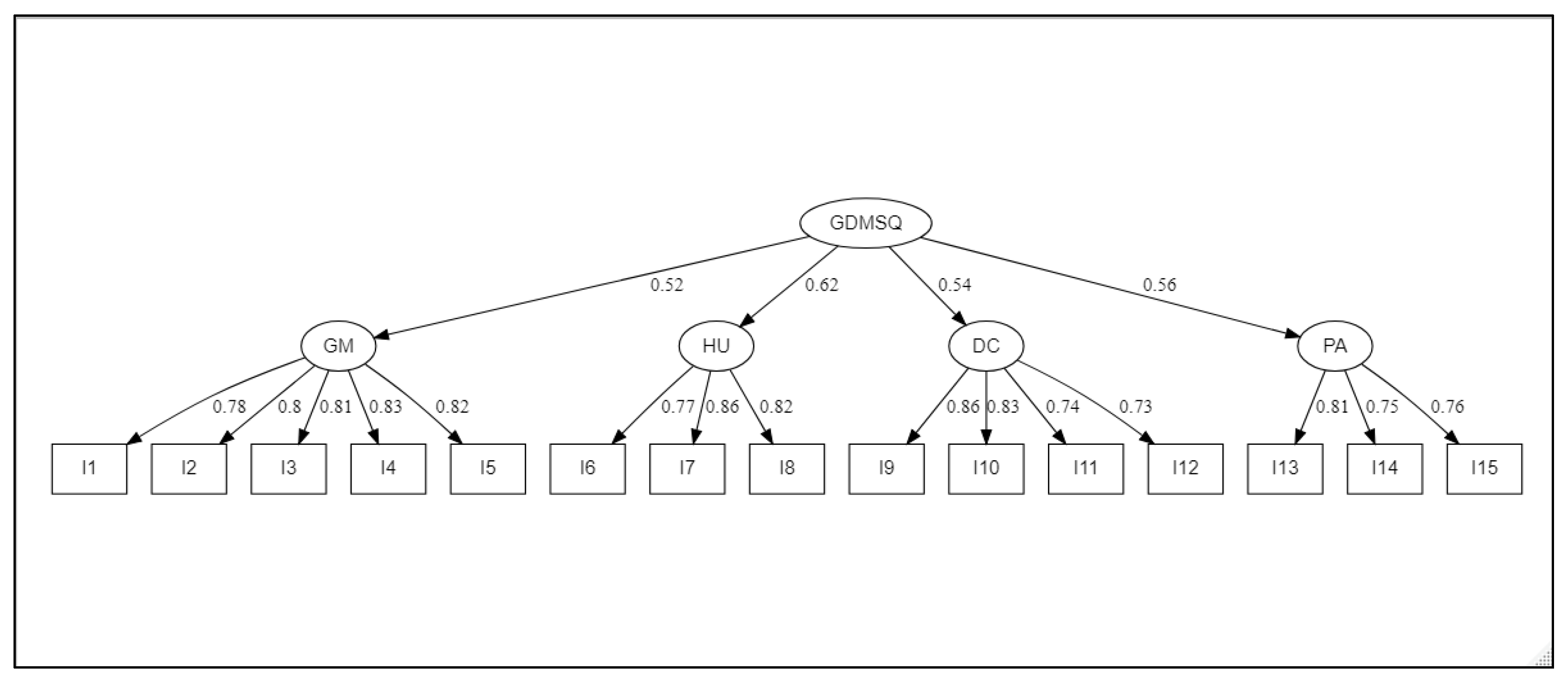
3.3. Confirmatory Factor Analysis
3.4. Concurrent Validity of the A-DSMQ
3.5. Convergent and Discriminant Validity
4. Discussion
Limitation of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Takashi, Y.; Kawanami, D. The Role of Bone-Derived Hormones in Glucose Metabolism, Diabetic Kidney Disease and Cardiovascular Disorders. Int. J. Mol. Sci. 2022, 23, 2376. [Google Scholar] [CrossRef] [PubMed]
- O’Toole, S.M.; Walker, R.J.; Garacci, E.; Dawson, A.Z.; Campbell, J.A.; Egede, L.E. Explanatory role of sociodemographic, clinical, behavioral, and social factors on cognitive decline in older adults with diabetes. BMC Geriatr. 2022, 22, 39. [Google Scholar] [CrossRef] [PubMed]
- Niroomand, M.; Babaniamansour, S.; Aliniagerdroudbari, E.; Golshaian, A.; Meibodi, A.M.; Absalan, A. Distress and depression among patients with diabetes mellitus: Prevalence and associated factors: A cross-sectional study. J. Diabetes Metab. Disord. 2021, 20, 141–151. [Google Scholar] [CrossRef] [PubMed]
- Saad, A.M.; Younes, Z.; Abuali, A.; Farooqi, M.H.; Hassoun, A.A. Diabetes distress and depression among patients with type 2 diabetes: A cross-sectional study. J. Diabetes Endocr. Pract. 2021, 4, 182. [Google Scholar] [CrossRef]
- Twiddy, H.; Frank, B.; Alam, U. A consideration of the psychological aspects to managing patients with painful diabetic neuropathy: An insight into pain management services at a tertiary centre in the UK. Diabetes Ther. 2021, 12, 487–498. [Google Scholar] [CrossRef]
- Ding, C.; Bao, Y.; Bai, B.; Liu, X.; Shi, B.; Tian, L. An update on the economic burden of type 2 diabetes mellitus in China. Expert Rev. Pharm. Outcomes Res. 2022, accepted. [CrossRef]
- Ebrahimipour, H.; Keyvanlo, Z.; Heidarian Miri, H.; Yousefi, M.; Ariafar, M.; Rezazadeh, A.; Pourahmadi, E. Productivity Loss of Diabetes in Iran (South Khorasan Province). J. Res. Health 2021, 11, 403–412. [Google Scholar] [CrossRef]
- Ganasegeran, K.; Hor, C.P.; Jamil, M.F.A.; Loh, H.C.; Noor, J.M.; Hamid, N.A.; Suppiah, P.D.; Abdul Manaf, R.D.; Hock Ch’ng, A.S.; Looi, I. A systematic review of the economic burden of type 2 diabetes in Malaysia. Int. J. Environ. Res. Public Health 2020, 17, 5723. [Google Scholar] [CrossRef]
- American Diabetes Association. Economic costs of diabetes in the US in 2017. Diabetes Care 2018, 41, 917–928. [Google Scholar] [CrossRef] [Green Version]
- Sun, H.; Saeedi, P.; Karuranga, S.; Pinkepank, M.; Ogurtsova, K.; Duncan, B.B.; Stein, C.; Basit, A.; Chan, J.C.N.; Mbanya, J.C.; et al. IDF Diabetes Atlas: Global, Regional and Country-Level Diabetes Prevalence Estimates for 2021 and Projections for 2045. Diabetes Res. Clin. Pract. 2022, 183, 109119. [Google Scholar] [CrossRef]
- El-Kebbi, I.M.; Bidikian, N.H.; Hneiny, L.; Nasrallah, M.P. Epidemiology of type 2 diabetes in the Middle East and North Africa: Challenges and call for action. World J. Diabetes 2021, 12, 1401. [Google Scholar] [CrossRef]
- Forouhi, N.G.; Wareham, N.J. Epidemiology of diabetes. Medicine 2019, 47, 22–27. [Google Scholar] [CrossRef]
- Khor, S.M.; Choi, J.; Won, P.; Ko, S.H. Challenges and Strategies in Developing an Enzymatic Wearable Sweat Glucose Biosensor as a Practical Point-Of-Care Monitoring Tool for Type II Diabetes. Nanomaterials 2022, 12, 221. [Google Scholar] [CrossRef]
- Mallik, R.; Chowdhury, T.A. Pharmacotherapy to delay the progression of diabetic kidney disease in people with type 2 diabetes: Past, present and future. Ther. Adv. Endocrinol. Metab. 2022, 13, 20420188221081600. [Google Scholar] [CrossRef] [PubMed]
- Gong, Q.; Zhang, P.; Wang, J.; Ma, J.; An, Y.; Chen, Y.; Zhang, B.; Feng, X.; Li, H.; Chen, X.; et al. Morbidity and mortality after lifestyle intervention for people with impaired glucose tolerance: 30-year results of the Da Qing Diabetes Prevention Outcome Study. Lancet Diabetes Endocrinol. 2019, 7, 452–461. [Google Scholar] [CrossRef]
- Mechanick, J.I.; Adams, S.; Davidson, J.A.; Fergus, I.V.; Galindo, R.J.; McKinney, K.H.; Petak, S.M.; Sadhu, A.R.; Samson, S.L.; Vedanthan, R.; et al. Transcultural diabetes care in the United States—A position statement by the American Association of Clinical Endocrinologists. Endocr. Pract. 2019, 25, 729–765. [Google Scholar] [CrossRef] [Green Version]
- Wylie, T.A.F.; Shah, C.; Connor, R.; Farmer, A.J.; Ismail, K.; Millar, B.; Morris, A.; Reynolds, R.M.; Robertson, E.; Swindell, R.; et al. Transforming mental well-being for people with diabetes: Research recommendations from Diabetes UK’s 2019 Diabetes and Mental Well-Being Workshop. Diabet. Med. 2019, 36, 1532–1538. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kalra, S.; Jena, B.N.; Yeravdekar, R. Emotional and psychological needs of people with diabetes. Indian J. Endocrinol. Metab. 2018, 22, 696. [Google Scholar] [CrossRef]
- Mathews, E.; Sathish, T.; Joseph, A.; Kodapally, B.; Thulaseedharan, J.V.; Narayan, K.V.; Oldenburg, B.; Thankappan, K.R. Effectiveness and implementation of a lifestyle modification intervention for women with isolated impaired fasting glucose: Study protocol for a hybrid type 2 study in Kerala, India. Wellcome Open Res. 2022, 7, 62. [Google Scholar] [CrossRef]
- Lind, N.; Hansen, D.L.; Rasmussen, S.S.; Nørgaard, K. Real-time continuous glucose monitoring versus self-monitoring of blood glucose in adults with insulin-treated type 2 diabetes: A protocol for a randomised controlled single-centre trial. BMJ Open 2021, 11, e040648. [Google Scholar] [CrossRef]
- Weinstock, R.S.; Aleppo, G.; Bailey, T.S.; Bergenstal, R.M.; Fisher, W.A.; Greenwood, D.A.; Young, L.A. The role of blood glucose monitoring in diabetes management. PMC 2021, 57, 2081–2093. [Google Scholar] [CrossRef]
- Fan, E.Y.; Crawford, A.S.; Nguyen, T.; Judelson, D.; Learned, A.; Chan, J.; Schanzer, A.; Simons, J.P.; Jones, D.W. Hemoglobin A1C Monitoring Practices Prior to Lower Extremity Bypass in Patients with Diabetes Vary Broadly and Do Not Predict Outcomes. J. Vasc. Surg. 2022, in press. [CrossRef]
- Shah, N.A.; Levy, C.J. Emerging technologies for the management of type 2 diabetes mellitus. J. Diabetes 2021, 13, 713–724. [Google Scholar] [CrossRef] [PubMed]
- Martinez, M.; Santamarina, J.; Pavesi, A.; Musso, C.; Umpierrez, G.E. Glycemic variability and cardiovascular disease in patients with type 2 diabetes. BMJ Open Diabetes Res. Care 2021, 9, e002032. [Google Scholar] [CrossRef]
- Gomez-Peralta, F.; Choudhary, P.; Cosson, E.; Irace, C.; Rami-Merhar, B.; Seibold, A. Understanding the clinical implications of differences between GMI and HbA1c. Diabetes Obes. Metab. 2022, 24, 599–608. [Google Scholar] [CrossRef]
- Akalin, S.; Berntorp, K.; Ceriello, A.; Das, A.K.; Kilpatrick, E.S.; Koblik, T.; Munichoodappa, C.S.; Pan, C.Y.; Rosenthall, W.; Shestakova, M.; et al. Intensive glucose therapy and clinical implications of recent data: A consensus statement from the Global Task Force on Glycaemic Control. Int. J. Clin. Pract. 2009, 63, 1421–1425. [Google Scholar] [CrossRef] [PubMed]
- Lu, Y.; Xu, J.; Zhao, W.; Han, H.-R. Measuring self-care in persons with type 2 diabetes: A systematic review. Eval. Health Prof. 2016, 39, 131–184. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mirzaei, H.; Siavash, M.; Shahnazi, H.; Abasi, M.H.; Eslami, A.A. Assessment of the psychometric properties of the Persian version of the diabetes self-management questionnaire (DSMQ) in patients with type 2 diabetes. J. Diabetes Metab. Disord. 2022, 1–9. [Google Scholar] [CrossRef]
- Kong, S.-Y.; Cho, M.-K. Validity and Reliability of the Korean Version of the Self-Care of Diabetes Inventory (SCODI-K). Int. J. Environ. Res. Public Health 2021, 18, 12179. [Google Scholar] [CrossRef]
- Schmitt, A.; Gahr, A.; Hermanns, N.; Kulzer, B.; Huber, J.; Haak, T. The Diabetes Self-Management Questionnaire (DSMQ): Development and evaluation of an instrument to assess diabetes self-care activities associated with glycaemic control. Health Qual. Life Outcomes 2013, 11, 138. [Google Scholar] [CrossRef] [Green Version]
- Schmitt, A.; Hermanns, N.; Kulzer, B.; Reimer, A.; Schall, S.; Haak, T. The Diabetes Self-Management Questionnaire (DSMQ) can detect inadequate self-care behaviour and help identify patients at risk of a negative diabetes prognosis. Diabetologia 2014, 122, 236–239. [Google Scholar]
- Vincze, A.; Losonczi, A.; Stauder, A. The validity of the diabetes self-management questionnaire (DSMQ) in Hungarian patients with type 2 diabetes. Health Qual. Life Outcomes 2020, 18, 344. [Google Scholar] [CrossRef] [PubMed]
- Thojampa, S.; Mawn, B. Psychometric evaluation of the Thai translation of the Diabetes Self-management Questionnaire in type 2 diabetes. Int. J. Nurs. Sci. 2017, 4, 236–238. [Google Scholar] [CrossRef] [PubMed]
- Bukhsh, A.; Lee, S.W.H.; Pusparajah, P.; Schmitt, A.; Khan, T.M. Psychometric properties of the diabetes self-management questionnaire (DSMQ) in Urdu. Health Qual. Life Outcomes 2017, 15, 200. [Google Scholar] [CrossRef] [PubMed]
- Márkus, B.; Hargittay, C.; Iller, B.; Rinfel, J.; Bencsik, P.; Oláh, I.; Kalabay, L.; Vörös, K. Validation of the revised Diabetes Self-Management Questionnaire (DSMQ-R) in the primary care setting. BMC Prim. Care 2022, 23, 2. [Google Scholar] [CrossRef]
- Bekele, B.B.; Negash, S.; Bogale, B.; Tesfaye, M.; Getachew, D.; Weldekidan, F.; Balcha, B. Effect of diabetes self-management education (DSME) on glycated hemoglobin (HbA1c) level among patients with T2DM: Systematic review and meta-analysis of randomized controlled trials. Diabetes Metab. Syndr. Clin. Res. Rev. 2021, 15, 177–185. [Google Scholar] [CrossRef]
- Perlman, J.E.; Gooley, T.A.; McNulty, B.; Meyers, J.; Hirsch, I.B. HbA1c and glucose management indicator discordance: A real-world analysis. Diabetes Technol. Ther. 2021, 23, 253–258. [Google Scholar] [CrossRef]
- Beran, M.; Muzambi, R.; Geraets, A.; Albertorio-Diaz, J.R.; Adriaanse, M.C.; Iversen, M.M.; Kokoszka, A.; Nefs, G.; Nouwen, A.; Pouwer, F.; et al. The bidirectional longitudinal association between depressive symptoms and HbA1c: A systematic review and meta-analysis. Diabet. Med. 2022, 39, e14671. [Google Scholar] [CrossRef]
- Schmitt, A.; Reimer, A.; Hermanns, N.; Huber, J.; Ehrmann, D.; Schall, S.; Kulzer, B. Assessing diabetes self-management with the diabetes self-management questionnaire (DSMQ) can help analyse behavioural problems related to reduced glycaemic control. PLoS ONE 2016, 11, e0150774. [Google Scholar] [CrossRef] [Green Version]
- Al-Hazzaa, H.M. Health-enhancing physical activity among Saudi adults using the International Physical Activity Questionnaire (IPAQ). Public Health Nutr. 2007, 10, 59–64. [Google Scholar] [CrossRef] [Green Version]
- Tabachnick, B.G.; Fidell, L.S.; Ullman, J.B. Using Multivariate Statistics; Pearson: Boston, MA, USA, 2007; Volume 5. [Google Scholar]
- Fidell, A. Discovering Statistics with SPSS; Sage: London, UK, 2009. [Google Scholar]
- Schumacker, R.E.; Lomax, R.G. A Beginner’s Guide to Structural Equation Modeling; Psychology Press: Hove, UK, 2004. [Google Scholar] [CrossRef]
- Steiger, J.H. Point estimation, hypothesis testing, and interval estimation using the RMSEA: Some comments and a reply to Hayduk and Glaser. Struct. Equ. Modeling 2000, 7, 149–162. [Google Scholar] [CrossRef]
- Hu, L.; Bentler, P.M. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Modeling Multidiscip. J. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Cheung, G.W.; Wang, C. Current approaches for assessing convergent and discriminant validity with SEM: Issues and solutions. In Academy of Management Proceedings; Academy of Management: Briarcliff Manor, NY, USA, 2017; p. 12706. [Google Scholar] [CrossRef]
- Aimran, A.N.; Ahmad, S.; Afthanorhan, A.; Awang, Z. The assessment of the performance of covariance-based structural equation modeling and partial least square path modeling. AIP Conf. Proc. 2017, 1842, 030001. [Google Scholar] [CrossRef]
- Ab Hamid, M.R.; Sami, W.; Sidek, M.M. Discriminant validity assessment: Use of Fornell & Larcker criterion versus HTMT criterion. J. Phys. Conf. Ser. 2017, 890, 012163. [Google Scholar] [CrossRef]
- Yun, I.; Joo, H.J.; Park, Y.S.; Park, E.-C. Association between Physical Exercise and Glycated Hemoglobin Levels in Korean Patients Diagnosed with Diabetes. Int. J. Environ. Res. Public Health 2022, 19, 3280. [Google Scholar] [CrossRef] [PubMed]
- Yanai, H.; Adachi, H.; Masui, Y.; Katsuyama, H.; Kawaguchi, A.; Hakoshima, M.; Waragai, Y.; Harigae, T.; Hamasaki, H.; Sako, A. Exercise therapy for patients with type 2 diabetes: A narrative review. J. Clin. Med. Res. 2018, 10, 365. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Variables | Exploratory (n = 208) | Confirmatory (n = 441) | |||
|---|---|---|---|---|---|
| n | % | n | % | ||
| Gender | Female | 121 | 58.17% | 169 | 38.32% |
| Male | 87 | 41.83% | 272 | 61.68% | |
| Socio economic level | Low | 67 | 32.21% | 117 | 26.53% |
| Medium | 80 | 38.46% | 220 | 49.89% | |
| High | 61 | 29.33% | 104 | 23.58% | |
| Academic level | Graduate | 87 | 41.83% | 224 | 50.79% |
| Undergraduate | 121 | 58.17% | 217 | 49.21% | |
| Other disease | Yes | 31 | 14.90% | 52 | 11.79% |
| No | 177 | 85.10% | 389 | 88.21% | |
| Age | Mean ± Std. Deviation | 53.2 ± 8.2 | 53.4 ± 7.4 | ||
| HbA1c value (%) | Mean ± Std. Deviation | 8.2 ± 1.3 | 8.6 ± 1.7 | ||
| Mean | Std. Deviation | Skewness | Kurtosis | Lambda | |
|---|---|---|---|---|---|
| I1 | 1.70 | 1.03 | −0.33 | −1.02 | 0.86 |
| I2 | 1.76 | 0.98 | −0.31 | −0.90 | 0.81 |
| I3 | 1.70 | 1.00 | −0.33 | −0.93 | 0.80 |
| I4 | 1.83 | 0.85 | −0.20 | −0.70 | 0.82 |
| I5 | 1.78 | 0.82 | −0.27 | −0.42 | 0.80 |
| I6 | 1.91 | 0.82 | −0.20 | −0.74 | 0.78 |
| I7 | 1.74 | 0.90 | −0.29 | −0.66 | 0.86 |
| I8 | 1.70 | 0.97 | −0.22 | −0.94 | 0.87 |
| I9 | 1.79 | 0.76 | −0.43 | 0.06 | 0.83 |
| I10 | 1.78 | 0.80 | −0.59 | 0.10 | 0.79 |
| I11 | 1.80 | 0.80 | −0.25 | −0.38 | 0.72 |
| I12 | 1.77 | 0.82 | −0.52 | −0.05 | 0.79 |
| I13 | 1.77 | 0.85 | −0.24 | −0.57 | 0.77 |
| I14 | 1.70 | 0.88 | −0.35 | −0.52 | 0.84 |
| I15 | 1.77 | 0.90 | −0.34 | −0.61 | 0.85 |
| Factors | Items | Scale Mean if Item Deleted | Corrected Item-Total Correlation | Cronbach’s Alpha if Item Deleted | Cronbach’s Alpha |
|---|---|---|---|---|---|
| GM | I1 | 7.08 | 0.823 | 0.869 | 0.904 |
| I2 | 7.01 | 0.749 | 0.885 | ||
| I3 | 7.07 | 0.769 | 0.881 | ||
| I4 | 6.94 | 0.739 | 0.888 | ||
| I5 | 6.99 | 0.738 | 0.889 | ||
| DC | I6 | 3.43 | 0.710 | 0.807 | 0.851 |
| I7 | 3.61 | 0.729 | 0.785 | ||
| I8 | 3.64 | 0.736 | 0.783 | ||
| HU | I9 | 5.36 | 0.692 | 0.768 | 0.828 |
| I10 | 5.37 | 0.637 | 0.791 | ||
| I11 | 5.35 | 0.613 | 0.802 | ||
| I12 | 5.38 | 0.680 | 0.772 | ||
| PA | I13 | 3.47 | 0.650 | 0.822 | 0.838 |
| I14 | 3.54 | 0.743 | 0.733 | ||
| I15 | 3.47 | 0.711 | 0.765 |
| Variable | Mean | Std. Deviation | Skew | C.RS | Kurtosis | C.Rk |
|---|---|---|---|---|---|---|
| I1 | 1.82 | 1.04 | −0.36 | −3.12 | −1.08 | −4.63 |
| I2 | 1.83 | 0.99 | −0.30 | −2.58 | −1.02 | −4.36 |
| I3 | 1.79 | 0.99 | −0.35 | −2.97 | −0.92 | −3.92 |
| I4 | 1.74 | 1.04 | −0.35 | −2.96 | −1.04 | −4.45 |
| I5 | 1.80 | 0.97 | −0.39 | −3.35 | −0.82 | −3.52 |
| I6 | 1.91 | 0.89 | −0.53 | −4.52 | −0.41 | −1.76 |
| I7 | 1.88 | 0.88 | −0.31 | −2.67 | −0.72 | −3.08 |
| I8 | 1.85 | 0.97 | −0.28 | −2.43 | −1.01 | −4.31 |
| I9 | 1.88 | 0.90 | −0.36 | −3.06 | −0.74 | −3.15 |
| I10 | 1.89 | 0.94 | −0.32 | −2.75 | −0.94 | −4.04 |
| I11 | 1.79 | 0.97 | −0.39 | −3.38 | −0.82 | −3.52 |
| I12 | 1.79 | 0.96 | −0.37 | −3.19 | −0.81 | −3.45 |
| I13 | 1.90 | 0.93 | −0.61 | −5.22 | −0.41 | −1.77 |
| I14 | 2.00 | 0.93 | −0.52 | −4.43 | −0.73 | −3.11 |
| I15 | 1.88 | 0.98 | −0.39 | −3.30 | −0.95 | −4.06 |
| GM | HU | DC | PA | A-DSMQ | HbA1C | |
|---|---|---|---|---|---|---|
| HU | 0.32 ** | |||||
| DC | 0.25 ** | 0.23 ** | ||||
| PA | 0.26 ** | 0.22 ** | 0.31 ** | |||
| SS | 0.76 ** | 0.59 ** | 0.66 ** | 0.60 ** | ||
| HbA1C | −0.41 ** | −0.23 ** | −0.28 ** | −0.36 ** | −0.49 ** | |
| IPAQ | 0.23 ** | 0.17 ** | 0.17 ** | 0.47 ** | 0.38 ** | −0.27 ** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kaddech, N.; Guelmami, N.; Bonsaksen, T.; Doggui, R.; Beji, C.; El Ati, J. Adaptation and Psychometric Evidence of the ARABIC Version of the Diabetes Self-Management Questionnaire (A-DSMQ). Healthcare 2022, 10, 951. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare10050951
Kaddech N, Guelmami N, Bonsaksen T, Doggui R, Beji C, El Ati J. Adaptation and Psychometric Evidence of the ARABIC Version of the Diabetes Self-Management Questionnaire (A-DSMQ). Healthcare. 2022; 10(5):951. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare10050951
Chicago/Turabian StyleKaddech, Nabil, Noomen Guelmami, Tore Bonsaksen, Radhouene Doggui, Chiraz Beji, and Jalila El Ati. 2022. "Adaptation and Psychometric Evidence of the ARABIC Version of the Diabetes Self-Management Questionnaire (A-DSMQ)" Healthcare 10, no. 5: 951. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare10050951