A New Therapeutic Strategy for Recurrent Ovarian Cancer―Bevacizumab beyond Progressive Disease

 , and
, and
Abstract
:1. Introduction
2. Concept of Treatment beyond Progressive Disease
3. Clinical Studies Validating the Usefulness of BBP
3.1. BRiTE: The Bevacizumab Regimens’ Investigation of Treatment Effects
3.2. ARIES: The Avastin Registry—Investigation of Effectiveness and Safety (ARIES)
3.3. ML18147: A Randomized Open-Label Phase III Intergroup Study, Effect of Adding Bevacizumab to Cross Over Fluoropyrimidine Based Chemotherapy (CTx) in Patients with Metastatic Colorectal Cancer and Disease Progression under First-Line Standard CTx/Bevacizumab Combination
3.4. TANIA: The Study of Avastin (Bevacizumab) in Combination with Chemotherapy in Patients with Breast Cancer Progressing after First-Line Therapy with Chemotherapy
3.5. WJOG5910L: The Open-Label, Randomized, Phase IIIb Trial Evaluating the Efficacy and Safety of Standard of Care +/− Continuous Bevacizumab Treatment beyond Progression of Disease (PD) in Patients with Advanced Non-Squamous Non-Small Cell Lung Cancer (NSCLC) after First-Line Treatment with Bevacizumab Plus a Platinum Doublet-Containing Chemotherapy Including 100 Patients with Advanced Non-Squamous Non-Small Cell Lung Cancer Who Received Platinum-Based Chemotherapy Plus Bevacizumab and Experienced Disease Progression
4. BBP for Ovarian Cancer
4.1. MITO16/MaNGO-OV2B Study
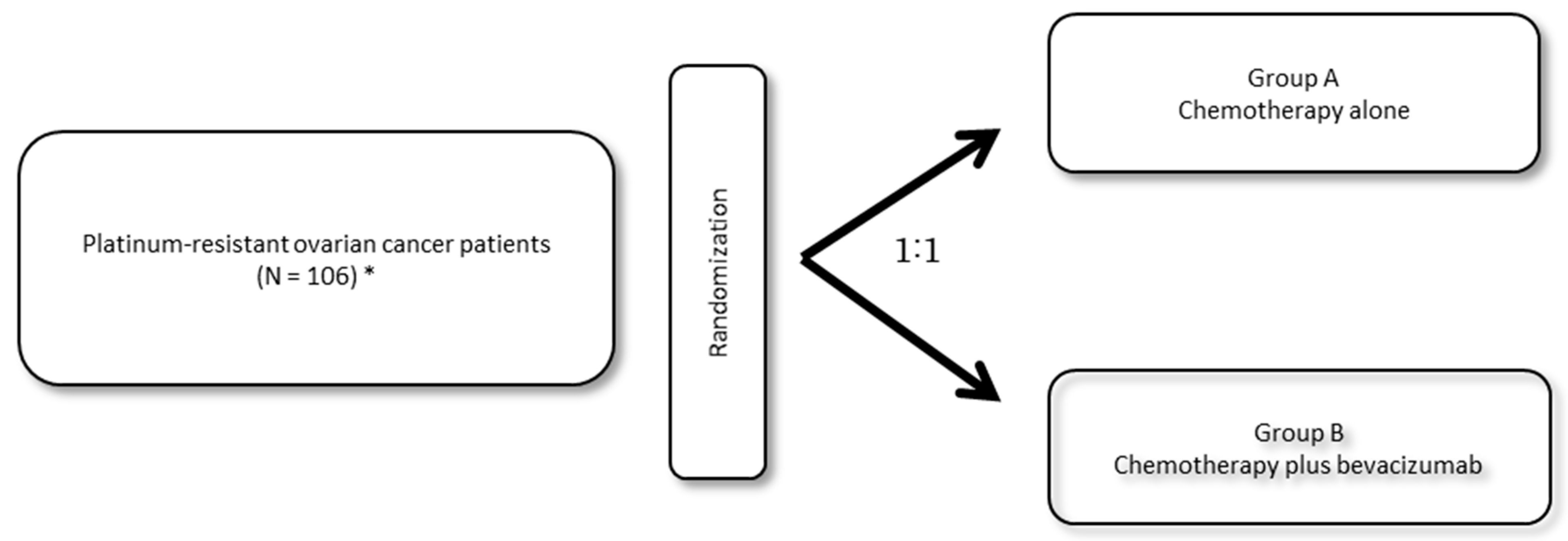
4.2. JGOG3023 Study
5. Is Paclitaxel a Potential Key Anticancer Drug Used in Combination with Bevacizumab?
6. Conclusions
Funding
Conflicts of Interest
References
- Folkman, J. Cancer: Principles & Practice of Oncology, 7th ed.; DeVita, V.T., Jr., Hellman, S., Rosenberg, S.A., Eds.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2005; pp. 2865–2882. [Google Scholar]
- Hanrahan, V.; Currie, M.J.; Gunningham, S.P.; Morrin, H.R.; Scott, P.A.; Robinson, B.A.; Fox, S.B. The Angiogenic Switch for Vascular Endothelial Growth Factor (VEGF)-A, VEGF-B, VEGF-C, and VEGF-D in the Adenoma-Carcinoma Sequence during Colorectal Cancer Progression. J. Pathol. 2003, 200, 183–194. [Google Scholar] [CrossRef] [PubMed]
- Fontanini, G.; Vignati, S.; Boldrini, L.; Chinè, S.; Silvestri, V.; Lucchi, M.; Mussi, A.; Angeletti, C.A.; Bevilacqua, G. Vascular Endothelial Growth Factor is Associated with Neovascularization and Influences Progression of Non-Small Cell Lung Carcinoma. Clin. Cancer Res. 1997, 3, 861–865. [Google Scholar] [PubMed]
- Tewari, K.S.; Sill, M.W.; Penson, R.T.; Huang, H.; Ramondetta, L.M.; Landrum, L.M.; Oaknin, A.; Reid, T.J.; Leitao, M.M.; Michael, H.E.; et al. Bevacizumab for Advanced Cervical Cancer: Final Overall Survival and Adverse Event Analysis of a Randomised, Controlled, Open-Label, Phase 3 Trial (Gynecologic Oncology Group 240). Lancet 2017, 390, 1654–1663. [Google Scholar] [CrossRef]
- Hurwitz, H.; Fehrenbacher, L.; Novotny, W.; Cartwright, T.; Hainsworth, J.; Heim, W.; Berlin, J.; Baron, A.; Griffing, S.; Holmgren, E.; et al. Bevacizumab Plus Irinotecan, Fluorouracil, and Leucovorin for Metastatic Colorectal Cancer. N. Engl. J. Med. 2004, 350, 2335–2342. [Google Scholar] [CrossRef] [PubMed]
- Reck, M.; von Pawel, J.; Zatloukal, P.; Ramlau, R.; Gorbounova, V.; Hirsh, V.; Leighl, N.; Mezger, J.; Archer, V.; Moore, N.; et al. Phase III Trial of Cisplatin Plus Gemcitabine with Either Placebo or Bevacizumab as First-Line Therapy for Nonsquamous Non-Small-Cell Lung Cancer: AVAil. J. Clin. Oncol. 2009, 27, 1227–1234. [Google Scholar] [CrossRef] [PubMed]
- Miller, K.; Wang, M.; Gralow, J.; Dickler, M.; Cobleigh, M.; Perez, E.A.; Shenkier, T.; Cella, D.; Davidson, N.E. Paclitaxel Plus Bevacizumab Versus Paclitaxel Alone for Metastatic Breast Cancer. N. Engl. J. Med. 2007, 357, 2666–2676. [Google Scholar] [CrossRef] [PubMed]
- Chinot, O.L.; Wick, W.; Mason, W.; Henriksson, R.; Saran, F.; Nishikawa, R.; Carpentier, A.F.; Hoang-Xuan, K.; Kavan, P.; Cernea, D.; et al. Bevacizumab Plus Radiotherapy-Temozolomide for Newly Diagnosed Glioblastoma. N. Engl. J. Med. 2014, 370, 709–722. [Google Scholar] [CrossRef] [PubMed]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M. New Response Evaluation Criteria in Solid Tumours: Revised RECIST Guideline (Version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef] [PubMed]
- Grothey, A.; Sugrue, M.M.; Purdie, D.M.; Dong, W.; Sargent, D.; Hedrick, E.; Kozloff, M. Bevacizumab Beyond First Progression is Associated with Prolonged Overall Survival in Metastatic Colorectal Cancer: Results from A Large Observational Cohort Study (BRiTE). J. Clin. Oncol. 2008, 26, 5326–5334. [Google Scholar] [CrossRef] [PubMed]
- Grothey, A.; Flick, E.D.; Cohn, A.L.; Bekaii-Saab, T.S.; Bendell, J.C.; Kozloff, M.; Roach, N.; Mun, Y.; Fish, S.; Hurwitz, H.I. Bevacizumab Exposure Beyond First Disease Progression in Patients with Metastatic Colorectal Cancer: Analyses of the ARIES Observational Cohort Study. Pharmacoepidemiol. Drug Saf. 2014, 23, 726–734. [Google Scholar] [CrossRef] [PubMed]
- Bennouna, J.; Sastre, J.; Arnold, D.; Österlund, P.; Greil, R.; Van Cutsem, E.; von Moos, R.; Viéitez, J.M.; Bouché, O.; Borg, C.; et al. ML18147 Study Investigators. Continuation of Bevacizumab after First Progression in Metastatic Colorectal Cancer (ML18147): A Randomised Phase 3 Trial. Lancet Oncol. 2013, 14, 29–37. [Google Scholar] [CrossRef]
- von Minckwitz, G.; Puglisi, F.; Cortes, J.; Vrdoljak, E.; Marschner, N.; Zielinski, C.; Villanueva, C.; Romieu, G.; Lang, I.; Ciruelos, E.; et al. Bevacizumab Plus Chemotherapy Versus Chemotherapy Alone As Second-Line Treatment for patients with HER2-Negative Locally Recurrent or Metastatic Breast Cancer after First-Line Treatment with Bevacizumab Plus Chemotherapy (TANIA): an Open-Label, Randomised Phase 3 Trial. Lancet Oncol. 2014, 15, 1269–1278. [Google Scholar] [PubMed]
- Takeda, M.; Yamanaka, T.; Seto, T.; Hayashi, H.; Azuma, K.; Okada, M.; Sugawara, S.; Daga, H.; Hirashima, T.; Yonesaka, K.; et al. Bevacizumab Beyond Disease Progression After First-Line Treatment with Bevacizumab Plus Chemotherapy in Advanced Nonsquamous Non-Small Cell Lung Cancer (West Japan Oncology Group 5910L): An Open-Label, Randomized, Phase 2 Trial. Cancer 2016, 122, 1050–1059. [Google Scholar] [CrossRef]
- Burger, R.A.; Brady, M.F.; Bookman, M.A.; Fleming, G.F.; Monk, B.J.; Huang, H.; Mannel, R.S.; Homesley, H.D.; Fowler, J.; Greer, B.E.; et al. Gynecologic Oncology Group. Incorporation of Bevacizumab in the Primary Treatment of Ovarian Cancer. N. Engl. J. Med. 2011, 365, 2473–2483. [Google Scholar] [CrossRef]
- Oza, A.M.; Cook, A.D.; Pfisterer, J.; Embleton, A.; Ledermann, J.A.; Pujade-Lauraine, E.; Kristensen, G.; Carey, M.S.; Beale, P.; Cervantes, A.; et al. ICON7 Trial Investigators. Standard Chemotherapy With or Without Bevacizumab for Women with Newly Diagnosed Ovarian Cancer (ICON7): Overall Survival Results of a Phase 3 Randomised Trial. Lancet Oncol. 2015, 16, 928–936. [Google Scholar] [CrossRef]
- Aghajanian, C.; Blank, S.V.; Goff, B.A.; Judson, P.L.; Teneriello, M.G.; Husain, A.; Sovak, M.A.; Yi, J.; Nycum, L.R. OCEANS: A Randomized, Double-Blind, Placebo-Controlled Phase III Trial of Chemotherapy With or Without Bevacizumab in Patients With Platinum-Sensitive Recurrent Epithelial Ovarian, Primary Peritoneal, or Fallopian Tube Cancer. J. Clin. Oncol. 2012, 30, 2039–2045. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pujade-Lauraine, E.; Hilpert, F.; Weber, B.; Reuss, A.; Poveda, A.; Kristensen, G.; Sorio, R.; Vergote, I.; Witteveen, P.; Bamias, A.; et al. Bevacizumab Combined With Chemotherapy for Platinum-Resistant Recurrent Ovarian Cancer: The AURELIA Open-Label Randomized Phase III Trial. J. Clin. Oncol. 2014, 32, 1302–1308. [Google Scholar] [CrossRef] [PubMed]
- Pignata, S.; Lorusso, D.; Joly, F.; Gallo, C.; Colombo, N.; Sessa, C.; Bamias, A.; Pisano, C.; Selle, F.; Zaccarelli, E.; et al. Chemotherapy Plus or Minus Bevacizumab for Platinum-Sensitive Ovarian Cancer Patients Recurring after a Bevacizumab Containing First Line Treatment: The Randomized Phase 3 Trial: MITO16B-MaNGO OV2B-ENGOT OV17. J. Clin. Oncol. 2018, 36, 5506. [Google Scholar] [CrossRef]
- Shoji, T.; Komiyama, S.; Kigawa, J.; Tanabe, H.; Kato, K.; Itamochi, H.; Fujiwara, H.; Kamiura, S.; Hamano, T.; Sugiyama, T. An Open-Label, Randomized, Phase II Trial Evaluating the Efficacy and Safety of Standard of Care With or Without Bevacizumab in Platinum-Resistant Epithelial Ovarian, Fallopian Tube, or Primary Peritoneal Cancer Patients Previously Treated with Bevacizumab for Front-Line or Platinum-Sensitive Ovarian Cancer: Rationale, Design, and Methods of the Japanese Gynecologic Oncology Group Study JGOG3023. BMC Cancer 2018, 18, 771. [Google Scholar] [PubMed]
- Cannistra, S.A.; Matulonis, U.A.; Penson, R.T.; Hambleton, J.; Dupont, J.; Mackey, H.; Douglas, J.; Burger, R.A.; Armstrong, D.; Wenham, R.; et al. Phase II Study of Bevacizumab in Patients with Platinum-Resistant Ovarian Cancer or Peritoneal Serous Cancer. J. Clin. Oncol. 2007, 25, 5180–5186. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Trial | Design | Cancer Type | Primary Chemotherapy | Regimens | Patients | Primary Endpoint | Results | p Value |
|---|---|---|---|---|---|---|---|---|
| BRiTE10) | cohort | Colorectal cancer | CT+BEV | CT (control) CT+BEV Observation | 531 642 253 | OS | 19.9m 31.8m 12.6m | p < 0.001 |
| ARIES11) | cohort | Colorectal cancer | CT+BEV | CT (control) CT+BEV | 667 438 | PPS | 10.6m 14.4m | p = 0.02 |
| ML1814712) | PIII | Colorectal cancer | CT+BEV | CT (control) CT+BEV | 410 409 | OS | 9.8m 11.2m | p = 0.0062 |
| TANIA13) | PIII | Brest cancer | CT+BEV | CT(control) CT+BEV | 247 247 | PFS (2nd line) | 4.2m 6.3m | p = 0.0068 |
| WJOG5910L14) | PII | Lung cancer | CT+BEV | CT(control) CT+BEV | 50 50 | PFS | 3.4m 4.4m | p = 0.058 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shoji, T.; Eto, H.; Sato, T.; Soma, R.; Fukagawa, D.; Tomabechi, H.; Takatori, E.; Nagasawa, T.; Sato, S.; Kagabu, M.; et al. A New Therapeutic Strategy for Recurrent Ovarian Cancer―Bevacizumab beyond Progressive Disease. Healthcare 2019, 7, 109. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare7030109
Shoji T, Eto H, Sato T, Soma R, Fukagawa D, Tomabechi H, Takatori E, Nagasawa T, Sato S, Kagabu M, et al. A New Therapeutic Strategy for Recurrent Ovarian Cancer―Bevacizumab beyond Progressive Disease. Healthcare. 2019; 7(3):109. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare7030109
Chicago/Turabian StyleShoji, Tadahiro, Hisashi Eto, Takanori Sato, Rikako Soma, Daisuke Fukagawa, Hidetoshi Tomabechi, Eriko Takatori, Takayuki Nagasawa, Seiya Sato, Masahiro Kagabu, and et al. 2019. "A New Therapeutic Strategy for Recurrent Ovarian Cancer―Bevacizumab beyond Progressive Disease" Healthcare 7, no. 3: 109. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare7030109