Adverse Effects of Anabolic-Androgenic Steroids: A Literature Review



 ,
, 
Abstract
:1. Introduction
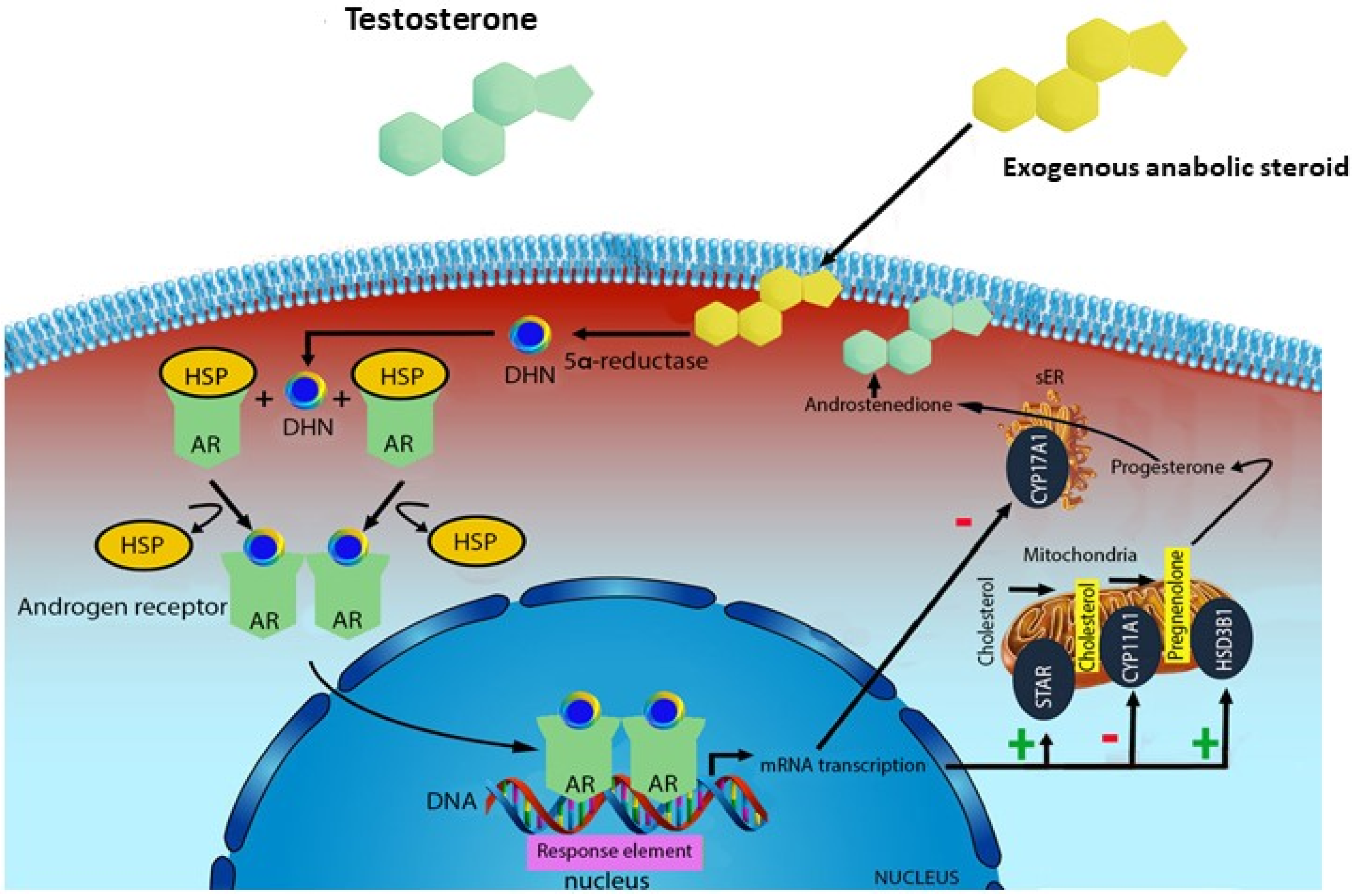
2. Phisiology of AASs
3. Pathophysiology of AASs
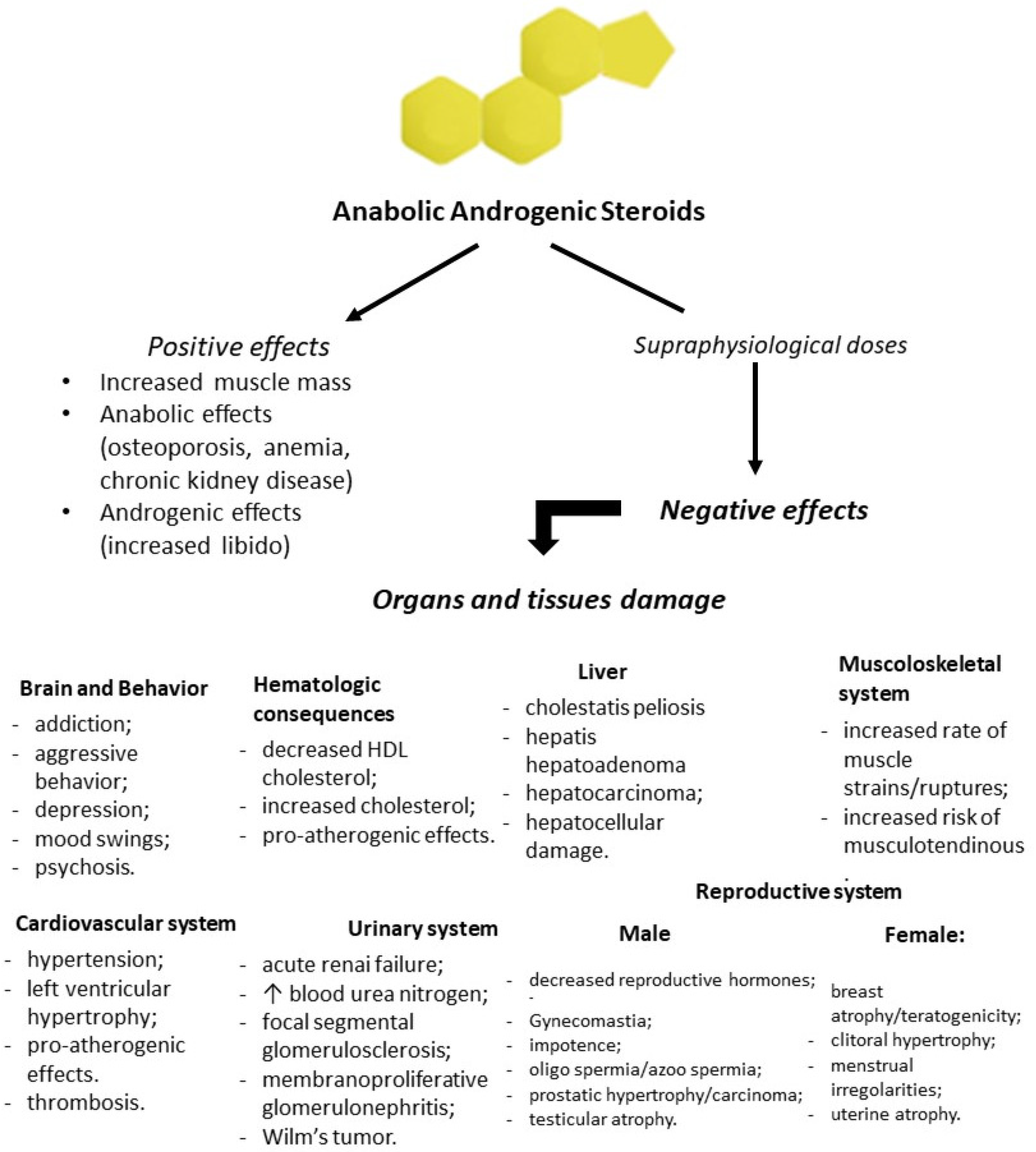
4. AAS Use and Adverse Effects
4.1. Autopsy Findings
4.2. Brain and Behavior
4.3. Cardiovascular System
4.4. Liver
4.5. Urinary System
4.6. Muscoloskeletal System
4.7. Reproductive System
4.8. Hematologic Consequences
4.9. AASs and Cancer
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Roman, M.; Roman, D.L.; Ostafe, V.; Ciorsac, A.; Isvoran, A. Computational assessment of pharmacokinetics and biological effects of some anabolic and androgen steroids. Pharm. Res. 2018, 35, 41. [Google Scholar] [CrossRef] [PubMed]
- Patanè, F.G.; Liberto, A.; Maglitto, A.N.M.; Malandrino, P.; Esposito, M.; Amico, F.; Cocimano, G.; Li Rosi, G.; Condorelli, D.; Di Nunno, N.; et al. Nandrolone Decanoate: Use, Abuse and Side Effects. Medicina 2020, 56, 606. [Google Scholar] [CrossRef] [PubMed]
- Mullen, C.; Whalley, B.J.; Schifano, F.; Baker, J.S. Anabolic androgenic steroid abuse in the United Kingdom: An update. Br. J. Pharmacol. 2020, 177, 2180–2198. [Google Scholar] [CrossRef]
- Basaria, S. Androgen abuse in athletes: Detection and consequences. J. Clin. Endocrinol. Metab. 2010, 95, 1533–1543. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- El Osta, R.; Almont, T.; Diligent, C.; Hubert, N.; Eschwège, P.; Hubert, J. Anabolic steroids abuse and male infertility. Basic Clin. Androl. 2016, 26, 2. [Google Scholar] [CrossRef] [Green Version]
- Joseph, J.F.; Parr, M.K. Synthetic androgens as designer supplements. Curr. Neuropharmacol. 2015, 13, 89–100. [Google Scholar] [CrossRef] [Green Version]
- Hakansson, A.; Mickelsson, K.; Wallin, C.; Berglund, M. Anabolic androgenic steroids in the general population: User characteristics and associations with substance use. Eur. Addict. Res. 2012, 18, 83–90. [Google Scholar] [CrossRef]
- Kanayama, G.; Kaufman, M.J.; Pope, H.G., Jr. Public health impact of androgens. Curr. Opin. Endocrinol. Diabetes Obes. 2018, 25, 218. [Google Scholar] [CrossRef]
- Rahnema, C.D.; Crosnoe, L.E.; Kim, E.D. Designer steroids-over-the-counter supplements and their androgenic component: Review of an increasing problem. Andrology 2015, 3, 150–155. [Google Scholar] [CrossRef] [Green Version]
- Kanayama, G.; Hudson, J.I.; Pope, H.G., Jr. Illicit anabolic–androgenic steroid use. Horm. Behav. 2010, 58, 111–121. [Google Scholar] [CrossRef] [Green Version]
- Anawalt, B.D. Diagnosis and management of anabolic androgenic steroid use. J. Clin. Endocrinol. Metab. 2019, 104, 2490–2500. [Google Scholar] [CrossRef] [PubMed]
- Kicman, A.T. Pharmacology of anabolic steroids. Br. J. Pharmacol. 2008, 154, 502–521. [Google Scholar] [CrossRef]
- Sessa, F.; Salerno, M.; Di Mizio, G.; Bertozzi, G.; Messina, G.; Tomaiuolo, B.; Pisanelli, D.; Maglietta, F.; Ricci, P.; Pomara, C. Anabolic androgenic steroids: Searching new molecular biomarkers. Front. Pharmacol. 2018, 9, 1321. [Google Scholar] [CrossRef] [PubMed]
- Alsiö, J.; Birgner, C.; Björkblom, L.; Isaksson, P.; Bergström, L.; Schiöth, H.B.; Lindblom, J. Impact of nandrolone decanoate on gene expression in endocrine systems related to the adverse effects of anabolic androgenic steroids. Basic Clin. Pharmacol. Toxicol. 2009, 105, 307–314. [Google Scholar] [CrossRef] [PubMed]
- Cheung, A.S.; Grossmann, M. Physiological basis behind ergogenic effects of anabolic androgens. Mol. Cell. Endocrinol. 2018, 464, 14–20. [Google Scholar] [CrossRef]
- Fortunato, R.S.; Marassi, M.P.; Chaves, E.A.; Nascimento, J.H.; Rosenthal, D.; Carvalho, D.P. Chronic administration of anabolic androgenic steroid alters murine thyroid function. Med. Sci. Sports Exerc. 2006, 38, 256–261. [Google Scholar] [CrossRef] [PubMed]
- Nieschlag, E.; Vorona, E. Doping with anabolic androgenic steroids(AAS): Adverse effects on non-reproductive organs and functions. Rev. Endocr. Metab. Disord. 2015, 16, 199–211. [Google Scholar] [CrossRef]
- Arazi, H.; Mohammadjafari, H.; Asadi, A. Use of anabolic androgenic steroids produces greater oxidative stress responses to resistance exercise in strength-trained men. Toxicol. Rep. 2017, 4, 282–286. [Google Scholar] [CrossRef]
- Frankenfeld, S.P.; Oliveira, L.P.; Ortenzi, V.H.; Rego-Monteiro, I.C.; Chaves, E.A.; Ferreira, A.C.; Leitao, A.C.; Carvalho, D.P.; Fortunato, R.S. The anabolic androgenic steroid nandrolone decanoate disrupts redox homeostasis in liver, heart and kidney of male Wistar rats. PLoS ONE 2014, 9, e102699. [Google Scholar] [CrossRef]
- Frankenfeld, S.P.; de Oliveira, L.P.; Ignacio, D.L.; Coelho, R.G.; Mattos, M.N.; Ferreira, A.C.; Carvalho, D.P.; Fortunato, R.S. Nandrolone decanoate inhibits gluconeogenesis and decreases fasting glucose in Wistar male rats. J. Endocrinol. 2014, 220, 143–153. [Google Scholar] [CrossRef] [Green Version]
- Chaves, E.A.; Pereira, P.P., Jr.; Fortunato, R.S.; Masuda, M.O.; de Carvalho, A.C.; de Carvalho, D.P.; Oliveira, M.F.; Nascimento, J.H. Nandrolone decanoate impairs exercise-induced cardioprotection: Role of antioxidant enzymes. J. Steroid Biochem. Mol. Biol. 2006, 99, 223–230. [Google Scholar] [CrossRef] [PubMed]
- Cerretani, D.; Neri, M.; Cantatore, S.; Ciallella, C.; Riezzo, I.; Turillazzi, E.; Fineschi, V. Looking for organ damages due to anabolic-androgenic steroids(AAS): Is oxidative stress the culprit? Mini Rev. Org. Chem. 2013, 10, 393–399. [Google Scholar] [CrossRef]
- Turillazzi, E.; Neri, M.; Cerretani, D.; Cantatore, S.; Frati, P.; Moltoni, L.; Busardò, F.P.; Pomara, C.; Riezzo, I.; Fineschi, V. Lipid peroxidation and apoptotic response in rat brain areas induced by long-term administration of nandrolone: The mutual crosstalk between ROS and NF-kB. J. Cell. Mol. Med. 2016, 20, 601–612. [Google Scholar] [CrossRef] [PubMed]
- Basile, J.R.; Binmadi, N.O.; Zhou, H.; Yang, Y.; Paoli, A.; Proia, P. Supraphysiological doses of performance enhancing anabolic-androgenic steroids exert direct toxic effects on neuron-like cells. Front. Cell Neurosci. 2013, 7, 69. [Google Scholar] [CrossRef] [Green Version]
- Joukar, S.; Vahidi, R.; Farsinejad, A.; Asadi-Shekaari, M.; Shahouzehi, B. Ameliorative effects of endurance exercise with two different intensities on nandrolone decanoate-induced neurodegeneration in rats: Involving redox and apoptotic systems. Neurotox. Res. 2017, 32, 41–49. [Google Scholar] [CrossRef]
- D’Errico, S.; Di Battista, B.; Di Paolo, M.; Fiore, C.; Pomara, C. Renal heat shock proteins over-expression due to anabolic androgenic steroids abuse. Mini Rev. Med. Chem. 2011, 11, 446–450. [Google Scholar] [CrossRef]
- Chrostowski, K.; Kwiatkowska, D.; Pokrywka, A.; Stanczyk, D.; Wójcikowska-Wójcik, B.; Grucza, R. Renin-angiotensin-aldosterone system in bodybuilders using supraphysiological doses of anabolic-androgenic steroids. Biol. Sport 2011, 28, 11. [Google Scholar] [CrossRef] [Green Version]
- D’Andrea, A.; Caso, P.; Salerno, G.; Scarafile, R.; De Corato, G.; Mita, C.; Di Salvo, G.; Severino, S.; Cuomo, S.; Liccardo, B.; et al. Left ventricular early myocardial dysfunction after chronic misuse of anabolic androgenic steroids: A Doppler myocardial and strain imaging analysis. Br. J. Sports Med. 2007, 41, 149–155. [Google Scholar] [CrossRef]
- Lopes, R.A.; Neves, K.B.; Pestana, C.R.; Queiroz, A.L.; Zanotto, C.Z.; Chignalia, A.Z.; Valim, Y.M.; Silveira, L.R.; Curti, C.; Tostes, R.C. Testosterone induces apoptosis in vascular smooth muscle cells via extrinsic apoptotic pathway with mitochondria-generated reactive oxygen species involvement. Am. J. Physiol. Heart Circ. Physiol. 2014, 306, H1485–H1494. [Google Scholar] [CrossRef] [Green Version]
- Hackett, D.A.; Johnson, N.A.; Chow, C.M. Training practices and ergogenic aids used by male bodybuilders. J. Strength Cond. Res. 2013, 27, 1609–1617. [Google Scholar] [CrossRef]
- Sjöqvist, F.; Garle, M.; Rane, A. Use of doping agents, particularly anabolic steroids, in sports and society. Lancet 2008, 371, 1872–1882. [Google Scholar] [CrossRef]
- Turillazzi, E.; Perilli, G.; Di Paolo, M.; Neri, M.; Riezzo, I.; Fineschi, V. Side effects of AAS abuse: An overview. Mini Rev. Med. Chem. 2011, 11, 374–389. [Google Scholar] [CrossRef] [PubMed]
- Van Amsterdam, J.; Opperhuizen, A.; Hartgens, F. Adverse health effects of anabolic–androgenic steroids. Regul. Toxicol. Pharmacol. 2010, 57, 117–123. [Google Scholar] [CrossRef] [PubMed]
- Petersson, A.; Garle, M.; Holmgren, P.; Druid, H.; Krantz, P.; Thiblin, I. Toxicological findings and manner of death in autopsied users of anabolic androgenic steroids. Drug Alcohol Depend. 2006, 81, 241–249. [Google Scholar] [CrossRef] [PubMed]
- Frati, P.; Busardo, F.P.; Cipolloni, L.; De Dominicis, E.; Fineschi, V. Anabolic androgenic steroid(AAS) related deaths: Autoptic, histopathological and toxicological findings. Curr. Neuropharmacol. 2015, 13, 146–159. [Google Scholar] [CrossRef] [Green Version]
- Darke, S.; Torok, M.; Duflou, J. Sudden or unnatural deaths involving anabolic-androgenic steroids. J. Forensic Sci. 2014, 59, 1025–1028. [Google Scholar] [CrossRef]
- Di Paolo, M.; Agozzino, M.; Toni, C.; Luciani, A.B.; Molendini, L.; Scaglione, M.; Inzani, F.; Pasotti, M.; Buffi, F.; Arbustini, E. Sudden anabolic steroid abuse-related death in athletes. Int. J. Cardiol. 2007, 114, 114–117. [Google Scholar] [CrossRef] [PubMed]
- Hernández-Guerra, A.I.; Tapia, J.; Menéndez-Quintanal, L.M.; Lucena, J.S. Sudden cardiac death in anabolic androgenic steroids abuse: Case report and literature review. Forensic Sci. Res. 2019, 4, 267–273. [Google Scholar] [CrossRef]
- Caraci, F.; Pistarà, V.; Corsaro, A.; Tomasello, F.; Giuffrida, M.L.; Sortino, M.A.; Nicoletti, F.; Copani, A. Neurotoxic properties of the anabolic androgenic steroids nandrolone and methandrostenolone in primary neuronal cultures. J. Neurosci. Res. 2011, 89, 592–600. [Google Scholar] [CrossRef]
- Karimooy, F.N.; Bideskan, A.E.; Pour, A.M.; Hoseini, S.M. Neurotoxic Effects of Stanozolol on Male Rats’ Hippocampi: Does Stanozolol cause apoptosis? Biomol. Concepts 2019, 10, 73–81. [Google Scholar] [CrossRef]
- Gomes, F.G.; Fernandes, J.; Campos, D.V.; Cassilhas, R.C.; Viana, G.M.; D’Almeida, V.; de Moraes Rego, M.K.; Buainain, P.I.; Cavalheiro, E.A.; Arida, R.M. The beneficial effects of strength exercise on hippocampal cell proliferation and apoptotic signaling is impaired by anabolic androgenic steroids. Psychoneuroendocrinology 2014, 50, 106–117. [Google Scholar] [CrossRef] [PubMed]
- Sessa, F.; Salerno, M.; Cipolloni, L.; Bertozzi, G.; Messina, G.; Di Mizio, G.; Asmundo, A.; Pomara, C. Anabolic-androgenic steroids and brain injury: miRNA evaluation in users compared to cocaine abusers and elderly people. Aging 2020, 12. [Google Scholar] [CrossRef]
- Bjørnebekk, A.; Westlye, L.T.; Walhovd, K.B.; Jørstad, M.L.; Sundseth, Ø.Ø.; Fjell, A.M. Cognitive performance and structural brain correlates in long-term anabolic-androgenic steroid exposed and nonexposed weightlifters. Neuropsychology 2019, 33, 547. [Google Scholar] [CrossRef] [PubMed]
- Bjørnebekk, A.; Walhovd, K.B.; Jørstad, M.L.; Due-Tønnessen, P.; Hullstein, I.R.; Fjell, A.M. Structural brain imaging of long-term anabolic-androgenic steroid users and nonusing weightlifters. Biol. Psychiatry 2017, 82, 294–302. [Google Scholar] [CrossRef] [Green Version]
- Kaufman, M.J.; Janes, A.C.; Hudson, J.I.; Brennan, B.P.; Kanayama, G.; Kerrigan, A.R.; Jensen, J.E.; Pope, H.G., Jr. Brain and cognition abnormalities in long-term anabolic-androgenic steroid users. Drug Alcohol Depend. 2015, 152, 47–56. [Google Scholar] [CrossRef] [Green Version]
- Kanayama, G.; Kean, J.; Hudson, J.I.; Pope, H.G., Jr. Cognitive deficits in long-term anabolic-androgenic steroid users. Drug Alcohol Depend. 2013, 130, 208–214. [Google Scholar] [CrossRef] [Green Version]
- Kaufman, M.J.; Kanayama, G.; Hudson, J.I.; Pope, H.G., Jr. Supraphysiologic-dose anabolic–androgenic steroid use: A risk factor for dementia? Neurosci. Biobehav. Rev. 2019, 100, 180–207. [Google Scholar] [CrossRef]
- Piacentino, D.; Kotzalidis, G.D.; Del Casale, A.; Aromatario, M.R.; Pomara, C.; Girardi, P.; Sani, G. Anabolic-androgenic steroid use and psychopathology in athletes. A systematic review. Curr. Neuropharmacol. 2015, 13, 101–121. [Google Scholar] [CrossRef] [Green Version]
- Rashid, H.; Ormerod, S.; Day, E. Anabolic androgenic steroids: What the psychiatrist needs to know. Adv. Psychiatr. Treat. 2007, 13, 203–211. [Google Scholar] [CrossRef] [Green Version]
- Joksimovic, J.; Selakovic, D.; Jovicic, N.; Mitrovic, S.; Mihailovic, V.; Katanic, J.; Milovanovic, D.; Rosic, G. Exercise Attenuates Anabolic Steroids-Induced Anxiety via Hippocampal NPY and MC4 Receptor in Rats. Front. Neurosci. 2019, 13, 172. [Google Scholar] [CrossRef]
- Hauger, L.E.; Sagoe, D.; Vaskinn, A.; Arnevik, E.A.; Leknes, S.; Jørstad, M.L.; Bjørnebekk, A. Anabolic androgenic steroid dependence is associated with impaired emotion recognition. Psychopharmacology 2019, 236, 2667–2676. [Google Scholar] [CrossRef] [PubMed]
- Almeida, O.P.; Yeap, B.B.; Hankey, G.J.; Jamrozik, K.; Flicker, L. Low Free Testosterone Concentration as a Potentially Treatable Cause of Depressive Symptoms in Older Men; Arch. Gen. Psychiatry: Chicago, IL, USA, 2008; Volume 12, pp. 283–289. ISSN 0003-990X. [Google Scholar]
- Bueno, A.; Carvalho, F.B.; Gutierres, J.M.; Lhamas, C.; Andrade, C.M. A comparative study of the effect of the dose and exposure duration of anabolic androgenic steroids on behavior, cholinergic regulation, and oxidative stress in rats. PLoS ONE 2017, 12, e0177623. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Henderson, L.P.; Penatti, C.A.; Jones, B.L.; Yang, P.; Clark, A.S. Anabolic androgenic steroids and forebrain GABAergic transmission. Neuroscience 2006, 138, 793–799. [Google Scholar] [CrossRef] [PubMed]
- Kouvelas, D.; Pourzitaki, C.; Papazisis, G.; Dagklis, T.; Dimou, K.; Kraus, M.M. Nandrolone abuse decreases anxiety and impairs memory in rats via central androgenic receptors. Int. J. Neuropsychopharmacol. 2008, 11, 925–934. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Melloni, R.H., Jr.; Ricci, L.A. Adolescent exposure to anabolic/androgenic steroids and the neurobiology of offensive aggression: A hypothalamic neural model based on findings in pubertal Syrian hamsters. Horm. Behav. 2010, 58, 177–191. [Google Scholar] [CrossRef] [PubMed]
- Quaglio, G.; Fornasiero, A.; Mezzelani, P.; Moreschini, S.; Lugoboni, F.; Lechi, A. Anabolic steroids: Dependence and complications of chronic use. Intern. Emerg. Med. 2009, 4, 289–296. [Google Scholar] [CrossRef]
- Elfverson, M.; Johansson, T.; Zhou, Q.; Le Grevès, P.; Nyberg, F. Chronic administration of the anabolic androgenic steroid nandrolone alters neurosteroid action at the sigma-1 receptor but not at the sigma-2 or NMDA receptors. Neuropharmacology 2011, 61, 1172–1181. [Google Scholar] [CrossRef]
- Sato, S.M.; Schulz, K.M.; Sisk, C.L.; Wood, R.I. Adolescents and androgens, receptors and rewards. Horm. Behav. 2008, 53, 647–658. [Google Scholar] [CrossRef] [Green Version]
- Bertozzi, G.; Sessa, F.; Albano, G.D.; Sani, G.; Maglietta, F.; Roshan, M.H.; Li Volti, G.; Bernardini, R.; Avola, R.; Pomara, C.; et al. The role of anabolic androgenic steroids in disruption of the physiological function in discrete areas of the central nervous system. Mol. Neurobiol. 2018, 55, 5548–5556. [Google Scholar] [CrossRef]
- Bertozzi, G.; Salerno, M.; Pomara, C.; Sessa, F. Neuropsychiatric and Behavioral Involvement in AAS Abusers. A Literature Review. Medicina 2019, 55, 396. [Google Scholar] [CrossRef] [Green Version]
- Liu, J.D.; Wu, Y.Q. Anabolic-androgenic steroids and cardiovascular risk. Chin. Med. J. 2019, 132, 2229. [Google Scholar] [CrossRef] [PubMed]
- Vasilaki, F.; Tsitsimpikou, C.; Tsarouhas, K.; Germanakis, I.; Tzardi, M.; Kavvalakis, M.; Ozcagli, E.; Kouretas, D.; Tsatsakis, A.M. Cardiotoxicity in rabbits after long-term nandrolone decanoate administration. Toxicol. Lett. 2016, 241, 143–151. [Google Scholar] [CrossRef] [PubMed]
- Pereira-Junior, P.P.; Chaves, E.A.; Costa-e-Sousa, R.H.; Masuda, M.O.; de Carvalho, A.C.; Nascimento, J.H. Cardiac autonomic dysfunction in rats chronically treated with anabolic steroid. Eur. J. Appl. Physiol. 2006, 96, 487–494. [Google Scholar] [CrossRef] [PubMed]
- Riezzo, I.; Di Paolo, M.; Neri, M.; Bello, S.; Cantatore, S.; D’Errico, S.; Dinucci, D.; Parente, R.; Pomara, C.; Rabozzi, R.; et al. Anabolic steroid-and exercise-induced cardio-depressant cytokines and myocardial β1 receptor expression in CD1 mice. Curr. Pharm. Biotechnol. 2011, 12, 275–284. [Google Scholar] [CrossRef]
- Christou, G.A.; Christou, K.A.; Nikas, D.N.; Goudevenos, J.A. Acute myocardial infarction in a young bodybuilder taking anabolic androgenic steroids: A case report and critical review of the literature. Eur. J. Prev. Cardiol. 2016, 23, 1785–1796. [Google Scholar] [CrossRef]
- Achar, S.; Rostamian, A.; Narayan, S.M. Cardiac and metabolic effects of anabolic-androgenic steroid abuse on lipids, blood pressure, left ventricular dimensions, and rhythm. Am. J. Cardiol. 2010, 106, 893–901. [Google Scholar] [CrossRef] [Green Version]
- Golestani, R.; Slart, R.H.; Dullaart, R.P.; Glaudemans, A.W.; Zeebregts, C.J.; Boersma, H.H.; Tio, R.A.; Dierckx, R.A. Adverse cardiovascular effects of anabolic steroids: Pathophysiology imaging. Eur. J. Clin. Investig. 2012, 42, 795. [Google Scholar] [CrossRef] [Green Version]
- Alves, M.J.; Dos Santos, M.R.; Dias, R.G.; Akiho, C.A.; Laterza, M.C.; Rondon, M.U.; Moreau, R.L.; Negrao, C.E. Abnormal neurovascular control in anabolic androgenic steroids users. Med. Sci. Sports Exerc. 2010, 42, 865–871. [Google Scholar] [CrossRef]
- Baggish, A.L.; Weiner, R.B.; Kanayama, G.; Hudson, J.I.; Picard, M.H.; Hutter, A.M., Jr.; Pope, H.G., Jr. Long-term anabolic-androgenic steroid use is associated with left ventricular dysfunction. Circ. Heart Fail. 2010, 3, 472–476. [Google Scholar] [CrossRef] [Green Version]
- Seara, F.A.; Barbosa, R.A.; de Oliveira, D.F.; Gran da Silva, D.L.; Carvalho, A.B.; Freitas Ferreira, A.C.; Nascimento, J.H.; Olivares, E.L. Administration of anabolic steroid during adolescence induces long-term cardiac hypertrophy and increases susceptibility to ischemia/reperfusion injury in adult Wistar rats. J. Steroid Biochem. Mol. Biol. 2017, 171, 34–42. [Google Scholar] [CrossRef]
- Rasmussen, J.J.; Schou, M.; Madsen, P.L.; Selmer, C.; Johansen, M.L.; Ulriksen, P.S.; Dreyer, T.; Kumler, T.; Plesner, L.L.; Faber, J.; et al. Cardiac systolic dysfunction in past illicit users of anabolic androgenic steroids. Am. Heart J. 2018, 203, 49–56. [Google Scholar] [CrossRef]
- Nottin, S.; Nguyen, L.D.; Terbah, M.; Obert, P. Cardiovascular effects of androgenic anabolic steroids in male bodybuilders determined by tissue Doppler imaging. Am. J. Cardiol. 2006, 97, 912–915. [Google Scholar] [CrossRef]
- Rocha, F.L.; Carmo, E.C.; Roque, F.R.; Hashimoto, N.Y.; Rossoni, L.V.; Frimm, C.; Aneas, I.; Negrao, C.E.; Krieger, J.E.; Oliveira, E.M. Anabolic steroids induce cardiac renin-angiotensin system and impair the beneficial effects of aerobic training in rats. Am. J. Physiol. Heart Circ. Physiol. 2007, 293, H3575–H3583. [Google Scholar] [CrossRef] [Green Version]
- Akçakoyun, M.; Alizade, E.; Gündoğdu, R.; Bulut, M.; Tabakci, M.M.; Açar, G.; Avci, A.; Simsek, Z.; Fidan, S.; Demir, S.; et al. Long-term anabolic androgenic steroid use is associated with increased atrial electromechanical delay in male bodybuilders. Biomed. Res. Int. 2014. [Google Scholar] [CrossRef]
- Angell, P.; Chester, N.; Green, D.; Somauroo, J.; Whyte, G.; George, K. Anabolic steroids and cardiovascular risk. Sports Med. 2012, 42, 119–134. [Google Scholar] [CrossRef]
- Marocolo, M.; Silva-Neto, J.A.; Neto, O.B. Acute interruption of treatment with nandrolone decanoate is not sufficient to reverse cardiac autonomic dysfunction and ventricular repolarization disturbances in rats. Steroids 2018, 132, 12–17. [Google Scholar] [CrossRef]
- Phillis, B.D.; Abeywardena, M.Y.; Adams, M.J.; Kennedy, J.A.; Irvine, R.J. Nandrolone potentiates arrhythmogenic effects of cardiac ischemia in the rat. Toxicol. Sci. 2007, 99, 605–611. [Google Scholar] [CrossRef]
- Olivares, E.L.; Silveira, A.L.; Fonseca, F.V.; Silva-Almeida, C.; Côrtes, R.S.; Pereira-Junior, P.P.; Nascimento, J.H.; Reis, L.C. Administration of an anabolic steroid during the adolescent phase changes the behavior, cardiac autonomic balance and fluid intake in male adult rats. Physiol. Behav. 2014, 126, 15–24. [Google Scholar] [CrossRef] [Green Version]
- Esperón, C.G.; Lopez-Cancio, E.; Bermejo, P.G.; Dávalos, A. Anabolic Androgenic Steroids and Stroke. In Neuropathology of Drug Addictions and Substance Misuse, 2nd ed.; Preedy, V.R., Ed.; Academic Press: London, UK, 2016; pp. 981–990. ISBN 978-0-12-800212-4. [Google Scholar]
- Baggish, A.L.; Weiner, R.B.; Kanayama, G.; Hudson, J.I.; Lu, M.T.; Hoffmann, U.; Pope, H.G., Jr. Cardiovascular toxicity of illicit anabolic-androgenic steroid use. Circulation 2017, 135, 1991–2002. [Google Scholar] [CrossRef] [Green Version]
- Bond, P.; Llewellyn, W.; Van Mol, P. Anabolic androgenic steroid-induced hepatotoxicity. Med. Hypotheses 2016, 93, 150–153. [Google Scholar] [CrossRef]
- Neri, M.; Bello, S.; Bonsignore, A.; Cantatore, S.; Riezzo, I.; Turillazzi, E.; Fineschi, V. Anabolic androgenic steroids abuse and liver toxicity. Mini Rev. Med. Chem. 2011, 11, 430–437. [Google Scholar] [CrossRef] [PubMed]
- Solimini, R.; Rotolo, M.C.; Mastrobattista, L.; Mortali, C.; Minutillo, A.; Pichini, S.; Pacifici, I.; Palmi, I. Hepatotoxicity associated with illicit use of anabolic androgenic steroids in doping. Eur. Rev. Med. Pharmacol. Sci. 2017, 21, 7–16. [Google Scholar] [PubMed]
- Vieira, R.P.; Franca, R.F.; Damaceno-Rodrigues, N.R.; Dolhnikoff, M.; Caldini, E.G.; Carvalho, C.R.; Ribeiro, W. Dose-dependent hepatic response to subchronic administration of nandrolone decanoate. Med. Sci. Sports Exerc. 2008, 40, 842. [Google Scholar] [CrossRef] [PubMed]
- Schwingel, P.A.; Cotrim, H.P.; Salles, B.R.; Almeida, C.E.; dos Santos, C.R., Jr.; Nachef, B.; Andrade, A.R.; Zoppi, C.C. Anabolic-androgenic steroids: A possible new risk factor of toxicant-associated fatty liver disease. Liver Int. 2011, 31, 348–353. [Google Scholar] [CrossRef] [PubMed]
- Riezzo, I.; Turillazzi, E.; Bello, S.; Cantatore, S.; Cerretani, D.; Di Paolo, M.; Fiaschi, A.I.; Frati, P.; Neri, M.; Pedretti, M.; et al. Chronic nandrolone administration promotes oxidative stress, induction of pro-inflammatory cytokine and TNF-α mediated apoptosis in the kidneys of CD1 treated mice. Toxicol. Appl. Pharmacol. 2014, 280, 97–106. [Google Scholar] [CrossRef]
- Kahal, A.; Allem, R. Reversible effects of anabolic steroid abuse on cyto-architectures of the heart, kidneys and testis in adult male mice. Biomed. Pharmacother. 2018, 106, 917–922. [Google Scholar] [CrossRef]
- Brasil, G.A.; de Lima, E.M.; do Nascimento, A.M.; Caliman, I.F.; de Medeiros, A.R.; Silva, M.S.; de Abreu, G.R.; dos Reis, A.M.; de Andrade, T.U.; Bissoli, N.S. Nandrolone decanoate induces cardiac and renal remodeling in female rats, without modification in physiological parameters: The role of ANP system. Life Sci. 2015, 137, 65–73. [Google Scholar] [CrossRef]
- Josiak, K.; Jankowska, E.A.; Piepoli, M.F.; Banasiak, W.; Ponikowski, P. Skeletal myopathy in patients with chronic heart failure: Significance of anabolic-androgenic hormones. J. Cachexia Sarcopenia Muscle 2014, 5, 287–296. [Google Scholar] [CrossRef] [Green Version]
- Hoseini, L.; Roozbeh, J.; Sagheb, M.; Karbalay-Doust, S.; Noorafshan, A. Nandrolone decanoate increases the volume but not the length of the proximal and distal convoluted tubules of the mouse kidney. Micron 2009, 40, 226–230. [Google Scholar] [CrossRef]
- Carson, J.A.; Manolagas, S.C. Effects of sex steroids on bones and muscles: Similarities, parallels, and putative interactions in health and disease. Bone 2015, 80, 67–78. [Google Scholar] [CrossRef] [Green Version]
- Casavant, M.J.; Blake, K.; Griffith, J.; Yates, A.; Copley, L.M. Consequences of use of anabolic androgenic steroids. Pediatr. Clin. N. Am. 2007, 54, 677–690. [Google Scholar] [CrossRef]
- Andrews, M.A.; Magee, C.D.; Combest, T.M.; Allard, R.J.; Douglas, K.M. Physical effects of anabolic-androgenic steroids in healthy exercising adults: A systematic review and meta-analysis. Curr. Sports Med. Rep. 2018, 17, 232–241. [Google Scholar] [CrossRef]
- Caminiti, G.; Volterrani, M.; Iellamo, F.; Marazzi, G.; Massaro, R.; Miceli, M.; Mammi, C.; Piepoli, M.; Fini, M.; Rosano, G.M. Effect of long-acting testosterone treatment on functional exercise capacity, skeletal muscle performance, insulin resistance, and baroreflex sensitivity in elderly patients with chronic heart failure: A double-blind, placebo-controlled, randomized study. J. Am. Coll. Cardiol. 2009, 54, 919–927. [Google Scholar] [CrossRef]
- Marqueti, R.C.; Prestes, J.; Stotzer, U.S.; Paschoal, M.; Leite, R.D.; Perez, S.E.; de Araujo, H.S. MMP-2, jumping exercise and nandrolone in skeletal muscle. Int. J. Sports Med. 2008, 29, 559–563. [Google Scholar] [CrossRef]
- Paschoal, M.; de Cássia Marqueti, R.; Perez, S.; Selistre-de-Araujo, H.S. Nandrolone inhibits VEGF mRNA in rat muscle. Int. J. Sports Med. 2009, 30, 775–778. [Google Scholar] [CrossRef]
- Marqueti, R.C.; Prestes, J.; Wang, C.C.; Ramos, O.H.; Perez, S.E.; Nakagaki, W.R.; Carvalho, H.F.; Selistre-de-Araujo, H.S. Biomechanical responses of different rat tendons to nandrolone decanoate and load exercise. Scand. J. Med. Sci. Sports 2011, 21, e91–e99. [Google Scholar] [CrossRef]
- Marqueti, R.C.; Prestes, J.; Paschoal, M.; Ramos, O.H.; Perez, S.E.; Carvalho, H.F.; Selistre-de-Araujo, H.S. Matrix metallopeptidase 2 activity in tendon regions: Effects of mechanical loading exercise associated to anabolic-androgenic steroids. Eur. J. Appl. Physiol. 2008, 104, 1087. [Google Scholar] [CrossRef]
- Pomara, C.; Barone, R.; Marino Gammazza, A.; Sangiorgi, C.; Barone, F.; Pitruzzella, A.; Locorotondo, N.; Di Gaudio, F.; Salerno, M.; Maglietta, F.; et al. Effects of nandrolone stimulation on testosterone biosynthesis in leydig cells. J. Cell. Physiol. 2016, 231, 1385–1391. [Google Scholar] [CrossRef] [Green Version]
- Armstrong, J.M.; Avant, R.A.; Charchenko, C.M.; Westerman, M.E.; Ziegelmann, M.J.; Miest, T.S.; Trost, L.W. Impact of anabolic androgenic steroids on sexual function. Transl. Androl. Urol. 2018, 7, 483. [Google Scholar] [CrossRef]
- Coward, R.M.; Rajanahally, S.; Kovac, J.R.; Smith, R.P.; Pastuszak, A.W.; Lipshultz, L.I. Anabolic steroid induced hypogonadism in young men. J. Urol. 2013, 190, 2200–2205. [Google Scholar] [CrossRef]
- Barone, R.; Pitruzzella, A.; Marino Gammazza, A.; Rappa, F.; Salerno, M.; Barone, F.; Sangiorgi, C.; D’Amico, D.; Locorotondo, N.; Di Gaudio, F.; et al. Nandrolone decanoate interferes with testosterone biosynthesis altering blood–testis barrier components. J. Cell. Mol. Med. 2017, 21, 1636–1647. [Google Scholar] [CrossRef] [PubMed]
- García-Manso, J.M.; Esteve, T.V. Consequences of the Use of Anabolic-Androgenic Steroids for Male Athletes’ Fertility. In Exercise and Human Reproduction; Vaamonde, D., du Plessis, S.S., Agarwal, A., Eds.; Springer: New York, NY, USA, 2016; pp. 153–165. ISBN 978-1-4939-3402-7. [Google Scholar]
- Rahnema, C.D.; Lipshultz, L.I.; Crosnoe, L.E.; Kovac, J.R.; Kim, E.D. Anabolic steroid–induced hypogonadism: Diagnosis and treatment. Fertil. Steril. 2014, 101, 1271–1279. [Google Scholar] [CrossRef] [PubMed]
- Tatem, A.J.; Beilan, J.; Kovac, J.R.; Lipshultz, L.I. Management of anabolic steroid-induced infertility: Novel strategies for fertility maintenance and recovery. World J. Mens. Health 2020, 38, 141–150. [Google Scholar] [CrossRef] [PubMed]
- Agledahl, I.; Brodin, E.; Svartberg, J.; Hansen, J.B. Plasma free tissue factor pathway inhibitor(TFPI) levels and TF-induced thrombin generation ex vivo in men with low testosterone levels. Thromb. Haemost. 2009, 101, 471–477. [Google Scholar] [CrossRef] [Green Version]
- Liljeqvist, S.; Helldén, A.; Bergman, U.; Söderberg, M. Pulmonary embolism associated with the use of anabolic steroids. Eur. J. Intern. Med. 2008, 19, 214–215. [Google Scholar] [CrossRef]
- Thiblin, I.; Garmo, H.; Garle, M.; Holmberg, L.; Byberg, L.; Michaëlsson, K.; Gedeborg, R. Anabolic steroids and cardiovascular risk: A national population-based cohort study. Drug Alcohol Depend. 2015, 152, 87–92. [Google Scholar] [CrossRef]
- Jin, H.; Lin, J.; Fu, L.; Mei, Y.F.; Peng, G.; Tan, X.; Wang, D.M.; Wang, W.; Li, Y.G. Physiological testosterone stimulates tissue plasminogen activator and tissue factor pathway inhibitor and inhibits plasminogen activator inhibitor type 1 release in endothelial cells. Biochem. Cell Biol. 2007, 85, 246–251. [Google Scholar] [CrossRef]
- Chang, S.; Münster, A.B.; Gram, J.; Sidelmann, J.J. Anabolic androgenic steroid abuse: The effects on thrombosis risk, coagulation, and fibrinolysis. Semin. Thromb. Hemost. 2018, 44, 734–746. [Google Scholar] [CrossRef]
- Bertozzi, G.; Sessa, F.; Maglietta, F.; Cipolloni, L.; Salerno, M.; Fiore, C.; Fortarezza, P.; Ricci, P.; Turillazzi, E.; Pomara, C. Immunodeficiency as a side effect of anabolic androgenic steroid abuse: A case of necrotizing myofasciitis. Forensic Sci. Med. Pathol. 2019, 15, 616–621. [Google Scholar] [CrossRef]
- Salerno, M.; Cascio, O.; Bertozzi, G.; Sessa, F.; Messina, A.; Monda, V.; Cipolloni, L.; Biondi, A.; Daniele, A.; Pomara, C. Anabolic androgenic steroids and carcinogenicity focusing on Leydig cell: A literature review. Oncotarget 2018, 9, 19415. [Google Scholar] [CrossRef] [Green Version]
- Hashimoto, H.; Vertino, P.M.; Cheng, X. Molecular coupling of DNA methylation and histone methylation. Epigenomics 2010, 2, 657–669. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Medei, E.; Marocolo, M.; de Carvalho Rodrigues, D.; Arantes, P.C.; Takiya, C.M.; Silva, J.; Rondinelli, E.; Goldenberg, R.C.; Campos de Carvalho, A.C.; Nascimento, J.H. Chronic treatment with anabolic steroids induces ventricular repolarization disturbances: Cellular, ionic and molecular mechanism. J. Mol. Cell. Cardiol. 2010, 49, 165–175. [Google Scholar] [CrossRef] [PubMed]
- Schwarzenbach, H. Impact of physical activity and doping on epigenetic gene regulation. Drug Test. Anal. 2011, 3, 682–687. [Google Scholar] [CrossRef] [PubMed]
- Souza, L.D.; da Cruz, L.A.; Cerqueira, E.D.; Meireles, J.R. Micronucleus as biomarkers of cancer risk in anabolic androgenic steroids users. Hum. Exp. Toxicol. 2017, 36, 302–310. [Google Scholar] [CrossRef] [PubMed]
- Agriesti, F.; Tataranni, T.; Pacelli, C.; Scrima, R.; Laurenzana, I.; Ruggieri, V.; Cela, O.; Mazzoccoli, C.; Salerno, M.; Sessa, F.; et al. Nandrolone induces a stem cell-like phenotype in human hepatocarcinoma-derived cell line inhibiting mitochondrial respiratory activity. Sci. Rep. 2020, 10, 1–17. [Google Scholar] [CrossRef] [Green Version]
- Tentori, L.; Graziani, G. Doping with growth hormone/IGF-1, anabolic steroids or erythropoietin: Is there a cancer risk? Pharmacol. Res. 2007, 55, 359–369. [Google Scholar] [CrossRef]
- Kanayama, G.; Pope, H.G., Jr.; Hudson, J.I. Associations of anabolic-androgenic steroid use with other behavioral disorders: An analysis using directed acyclic graphs. Psychol. Med. 2018, 48, 2601–2608. [Google Scholar] [CrossRef]
- Brooks, J.H.; Ahmad, I.; Easton, G. Anabolic steroid use. Br. Med. J. 2016, 355. [Google Scholar] [CrossRef]
- Grönbladh, A.; Nylander, E.; Hallberg, M. The neurobiology and addiction potential of anabolic androgenic steroids and the effects of growth hormone. Brain Res. Bull. 2016, 126, 127–137. [Google Scholar] [CrossRef]
- Riezzo, I.; De Carlo, D.; Neri, M.; Nieddu, A.; Turillazzi, E.; Fineschi, V. Heart disease induced by AAS abuse, using experimental mice/rats models and the role of exercise-induced cardiotoxicity. Mini Rev. Med. Chem. 2011, 11, 409–424. [Google Scholar] [CrossRef]
- Pagonis, T.A.; Angelopoulos, N.V.; Koukoulis, G.N.; Hadjichristodoulou, C.S. Psychiatric side effects induced by supraphysiological doses of combinations of anabolic steroids correlate to the severity of abuse. Eur. Psychiatry 2006, 21, 551–562. [Google Scholar] [CrossRef]
- Baker, J.S.; Graham, M.R.; Davies, B. Steroid and prescription medicine abuse in the health and fitness community: A regional study. Eur. J. Intern. Med. 2006, 17, 479–484. [Google Scholar] [CrossRef]
- Nagata, J.M.; Ganson, K.T.; Gorrell, S.; Mitchison, D.; Murray, S.B. Association between legal performance-enhancing substances and use of anabolic-androgenic steroids in young adults. JAMA Pediatr. 2020. [Google Scholar] [CrossRef]
- Bates, G.; Van Hout, M.C.; Teck, J.T.W.; McVeigh, J. Treatments for people who use anabolic androgenic steroids: A scoping review. Harm Reduct. J. 2019, 16, 75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sessa, F.; Salerno, M.; Bertozzi, G.; Cipolloni, L.; Messina, G.; Aromatario, M.; Polo, L.; Turillazzi, E.; Pomara, C. miRNAs as novel biomarkers of chronic kidney injury in anabolic-androgenic steroid users: An experimental study. Front. Pharmacol. 2020, 11, 1454. [Google Scholar] [CrossRef] [PubMed]
- Torrisi, M.; Pennisi, G.; Russo, I.; Amico, F.; Esposito, M.; Liberto, A.; Cocimano, G.; Salerno, M.; Li Rosi, G.; Di Nunno, N.; et al. Sudden Cardiac Death in Anabolic-Androgenic Steroid Users: A Literature Review. Medicina 2020, 56, 587. [Google Scholar] [CrossRef] [PubMed]
- Mottram, D.R.; Alan, J.G. Anabolic steroids. Best Pract. Res. Clin. Endocrinol. Metab. 2000, 14, 55–69. [Google Scholar] [CrossRef]
- Albano, G.D.; Sessa, F.; Messina, A.; Monda, V.; Bertozzi, G.; Maglietta, F.; Giugliano, P.; Vacchiano, G.; Marsala, G.; Salerno, M. AAS and organs damage: A focus on Nandrolone effects. Acta Med. Mediterr. 2017, 6, 939–946. [Google Scholar] [CrossRef]
- Sessa, F.; Maglietta, F.; Bertozzi, G.; Salerno, M.; Di Mizio, G.; Messina, G.; Montana, A.; Ricci, P.; Pomara, C. Human brain injury and mirnas: An experimental study. Int. J. Mol. Sci. 2019, 20, 1546. [Google Scholar] [CrossRef] [Green Version]
- Monda, V.; Salerno, M.; Sessa, F.; Bernardini, R.; Valenzano, A.; Marsala, G.; Zammit, C.; Avola, R.; Carotenuto, M.; Messina, G.; et al. Functional changes of orexinergic reaction to psychoactive substances. Mol. Neurobiol. 2018, 55, 6362–6368. [Google Scholar] [CrossRef]
- Sessa, F.; Franco, S.; Picciocchi, E.; Geraci, D.; Chisari, M.G.; Marsala, G.; Polito, A.N.; Sorrentino, M.; Tripi, G.; Salerno, M.; et al. Addictions substance free during lifespan. Acta Med. Mediter. 2018, 34, 2081–2087. [Google Scholar]
- Monda, V.; Salerno, M.; Fiorenzo, M.; Villano, I.; Viggiano, A.; Sessa, F.; Triggiani, A.I.; Cibelli, G.; Valenzano, A.; Marsala, G.; et al. Role of sex hormones in the control of vegetative and metabolic functions of middle-aged women. Front. Physiol. 2017, 8, 773. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pomara, C.; Neri, M.; Bello, S.; Fiore, C.; Riezzo, I.; Turillazzi, E. Neurotoxicity by synthetic androgen steroids: Oxidative stress, apoptosis, and neuropathology: A review. Curr. Neuropharmacol. 2015, 13, 132–145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pomara, C.; D’Errico, S.; Riezzo, I.; De Cillis, G.P.; Fineschi, V. Sudden cardiac death in a child affected by Prader-Willi syndrome. Int. J. Legal Med. 2005, 119, 153–157. [Google Scholar] [CrossRef] [PubMed]
- Fineschi, V.; Neri, M.; Di Donato, S.; Pomara, C.; Riezzo, I.; Turillazzi, E. An immunohistochemical study in a fatality due to ovarian hyperstimulation syndrome. Int. J. Legal Med. 2006, 120, 293–299. [Google Scholar] [CrossRef] [PubMed]
- Neri, M.; Riezzo, I.; Pomara, C.; Schiavone, S.; Turillazzi, E. Oxidative-nitrosative stress and myocardial dysfunctions in sepsis: Evidence from the literature and postmortem observations. Mediat. Inflamm. 2016, 2016, 3423450. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Organ/System | Author(s) | Year of Publication | Adverse Effects |
|---|---|---|---|
| Brain and Behavior | Bertozzi, et al. | 2019 | ↓ orbitofrontal cortex; lack of inhibitory control. |
| Hauger, et al. | 2019 | ↓ memory, ↓ anxiety ↑ depression. | |
| Joksimovic, et al. | 2019 | ↓ orbitofrontal cortex; lack of inhibitory control. | |
| Karimooy, et al. | 2019 | Neurodegeneration; histopathologic changes in hippocampus. | |
| Bertozzi, et al. | 2018 | ↑ aggressiveness. | |
| Bjørnebekk, et al. | 2017 | Lower cognitive functions, motor and executive performance; ↓ gray matter, cortical and putamen volume. | |
| Bueno, et al. | 2017 | Neurodegeneration. | |
| Turillazzi, et al. | 2016 | Neurodegeneration; hippocampus, striatum and frontal cortex injury. | |
| Joukar, et al. | 2017 | Neurodegeneration. | |
| Kaufman, et al. | 2015 | ↑↑ right amygdala volume. | |
| Piacentino, et al. | 2015 | ↓ memory, ↑ aggressiveness, ↓ anxiety ↑ depression. | |
| Gomes, et al. | 2014 | Neurodegeneration. | |
| Basile, et al. | 2013 | Neurodegeneration. | |
| Kanayama, et al. | 2013 | Cognitive dysfunction. | |
| Elfverson, et al. | 2011 | ↑ aggressiveness. | |
| Melloni, Jr., et al. | 2010 | Anxiety-like behavior. | |
| Kouvelas, et al. | 2008 | ↓ memory, ↓ anxiety. | |
| Sato, et al. | 2008 | ↑ aggressiveness. | |
| Rashid, et al. | 2007 | ↓ memory, ↑ aggressiveness, ↓ anxiety ↑ depression. | |
| Henderson, et al. | 2006 | behavioral effects. | |
| Cardiovascular system | Marocolo, et al. | 2018 | Arrhythmic events; cardiac hypertrophy. |
| Rasmussen, et al. | 2018 | Hypertension; left ventricular hypertrophy. | |
| Baggish, et al. | 2017 | ↑ left ventricular mass index; ↑ left ventricular walls; myocardial mechanical dysfunction. myocardial infarction. | |
| Seara, et al. | 2017 | ↑ left ventricular mass index; ↑ left ventricular walls; myocardial mechanical dysfunction. | |
| Christou, et al. | 2016 | Abnormal plasma lipoproteins. | |
| Esperón, et al. | 2016 | Atherosclerotic plaque. | |
| Vasilaki, et al. | 2016 | Cardiac injury | |
| Akçakoyun et al. | 2014 | Arrhythmic events. | |
| Angell, et at. | 2012 | Arrhythmic events; impairment of cardiac repolarization. | |
| Golestani, et al. | 2012 | ↓ plasma levels of HDL cholesterol; ↑ LDL cholesterol levels; arrhythmic events. | |
| Chrostowski, et al. | 2011 | Increased synthesis of heart muscle, left ventricular hypertrophy and hypertension. | |
| Riezzo, et al. | 2011 | Hypertension; left ventricular hypertrophy; pro-atherogenic effects; thrombosis. | |
| Achar, et al. | 2010 | ↓ plasma levels of HDL cholesterol; ↑ LDL cholesterol levels. | |
| Alves, et al. | 2010 | Increased sympathetic activity. | |
| D’Andrea, et al. | 2007 | Left ventricular dysfunction. | |
| Phillis, et al. | 2007 | Arrhythmic events. | |
| Chaves, et al. | 2006 | Oxidative stress. | |
| Nottin, et al. | 2006 | ↓ left ventricle relaxation properties. | |
| Pereira-Junior, et al. | 2006 | Impairment of parasympathetic cardiac modulation; heart rate variability. | |
| Liver | Solimini, et al. | 2017 | Mitochondrial degeneration of hepatic cells. |
| Bond, et al. | 2016 | Hepatotoxicity. | |
| Neri, et al. | 2011 | Hepatotoxicity. | |
| Schwingel, et al. | 2011 | Liver fibrosis process. | |
| Vieira, et al. | 2008 | Liver fibrosis process. | |
| Urinary system | Brasil, et al. | 2015 | Kidney fibrosis. |
| Riezzo, et al. | 2014 | Oxidative stress; Accumulation of mesangial matrix. | |
| D’Errico, et al. | 2011 | Accumulation of mesangial matrix. | |
| Muscoloskeletal system | Carson, et al. | 2015 | ↑ Muscle mass. |
| Marqueti, et al. | 2011 | Tendon damage. | |
| Paschoal, et al. | 2009 | Skeletal muscles injuries. | |
| Reproductive system | Armstrong, et al. | 2018 | Sexual dysfunctions. |
| Barone, et al. | 2017 | Spermatogenesis alteration. | |
| El Osta, et al. | 2016 | Infertility; ↓ number of spermatidis. | |
| García-Manso, et al. | 2016 | Changes in number, diameter and thickness of seminiferous tubules. | |
| Pomara, et al. | 2015 | Impairment of testosterone production. | |
| Rahnema, et al. | 2014 | Hypogonadism. | |
| Coward, et al. | 2013 | Hypogonadism. | |
| Hematologic consequences | Chang, et al. | 2018 | ↑ Thrombosis. |
| Casavant, et al. | 2007 | ↑ hematocrit, ↑ erythrocytosis. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Albano, G.D.; Amico, F.; Cocimano, G.; Liberto, A.; Maglietta, F.; Esposito, M.; Rosi, G.L.; Di Nunno, N.; Salerno, M.; Montana, A. Adverse Effects of Anabolic-Androgenic Steroids: A Literature Review. Healthcare 2021, 9, 97. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare9010097
Albano GD, Amico F, Cocimano G, Liberto A, Maglietta F, Esposito M, Rosi GL, Di Nunno N, Salerno M, Montana A. Adverse Effects of Anabolic-Androgenic Steroids: A Literature Review. Healthcare. 2021; 9(1):97. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare9010097
Chicago/Turabian StyleAlbano, Giuseppe Davide, Francesco Amico, Giuseppe Cocimano, Aldo Liberto, Francesca Maglietta, Massimiliano Esposito, Giuseppe Li Rosi, Nunzio Di Nunno, Monica Salerno, and Angelo Montana. 2021. "Adverse Effects of Anabolic-Androgenic Steroids: A Literature Review" Healthcare 9, no. 1: 97. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare9010097