
Interocular Symmetry Analysis of Corneal Elevation Using the Fellow Eye as the Reference Surface and Machine Learning



Abstract
:1. Introduction
2. Materials and Methods
2.1. Creating Pancorneal Difference Matrices
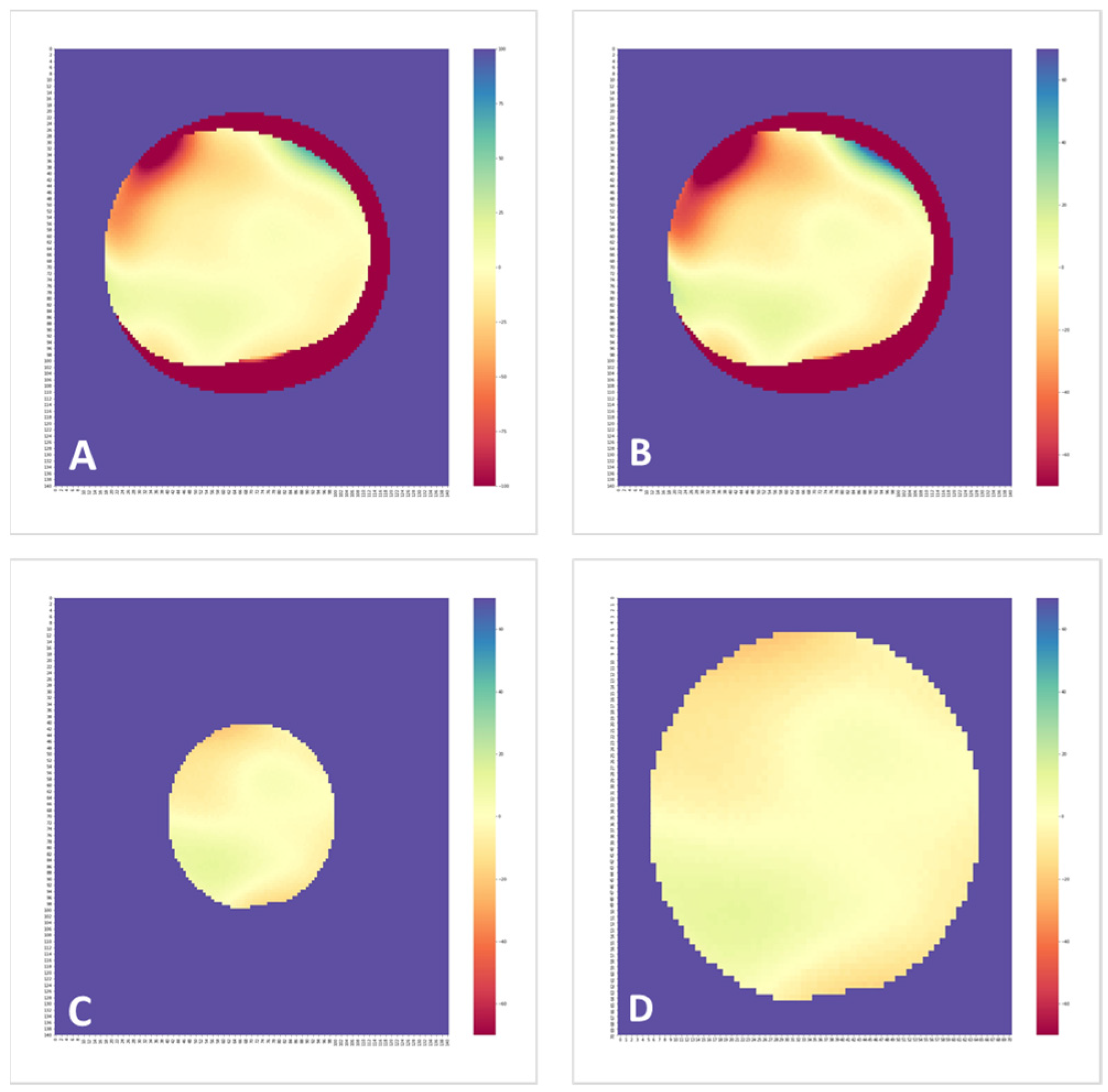
2.2. Creating Elevation Difference Colormaps
2.3. Feature Engineering
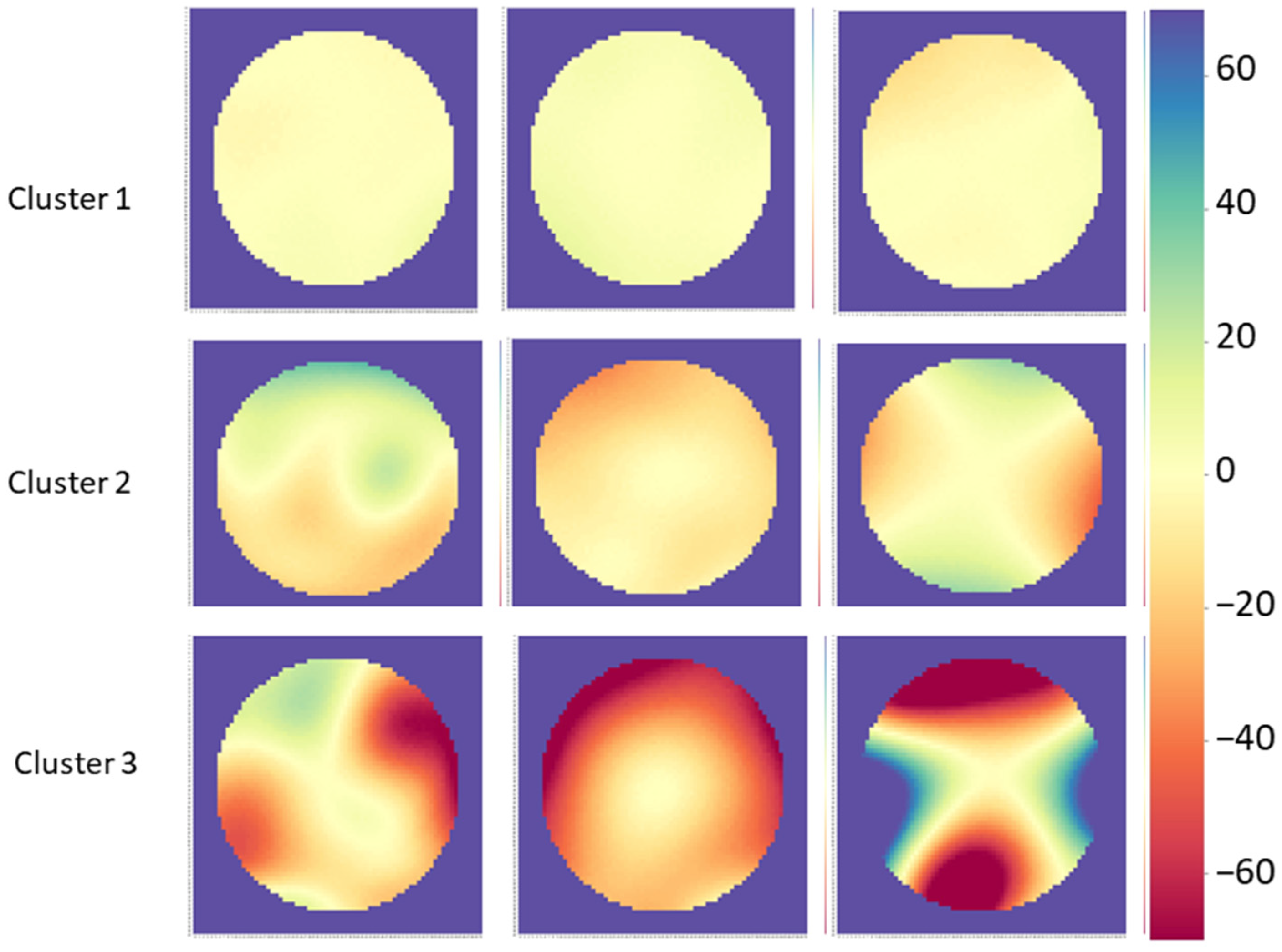
2.4. Cluster Analysis
2.5. Adding Other Indices
3. Results
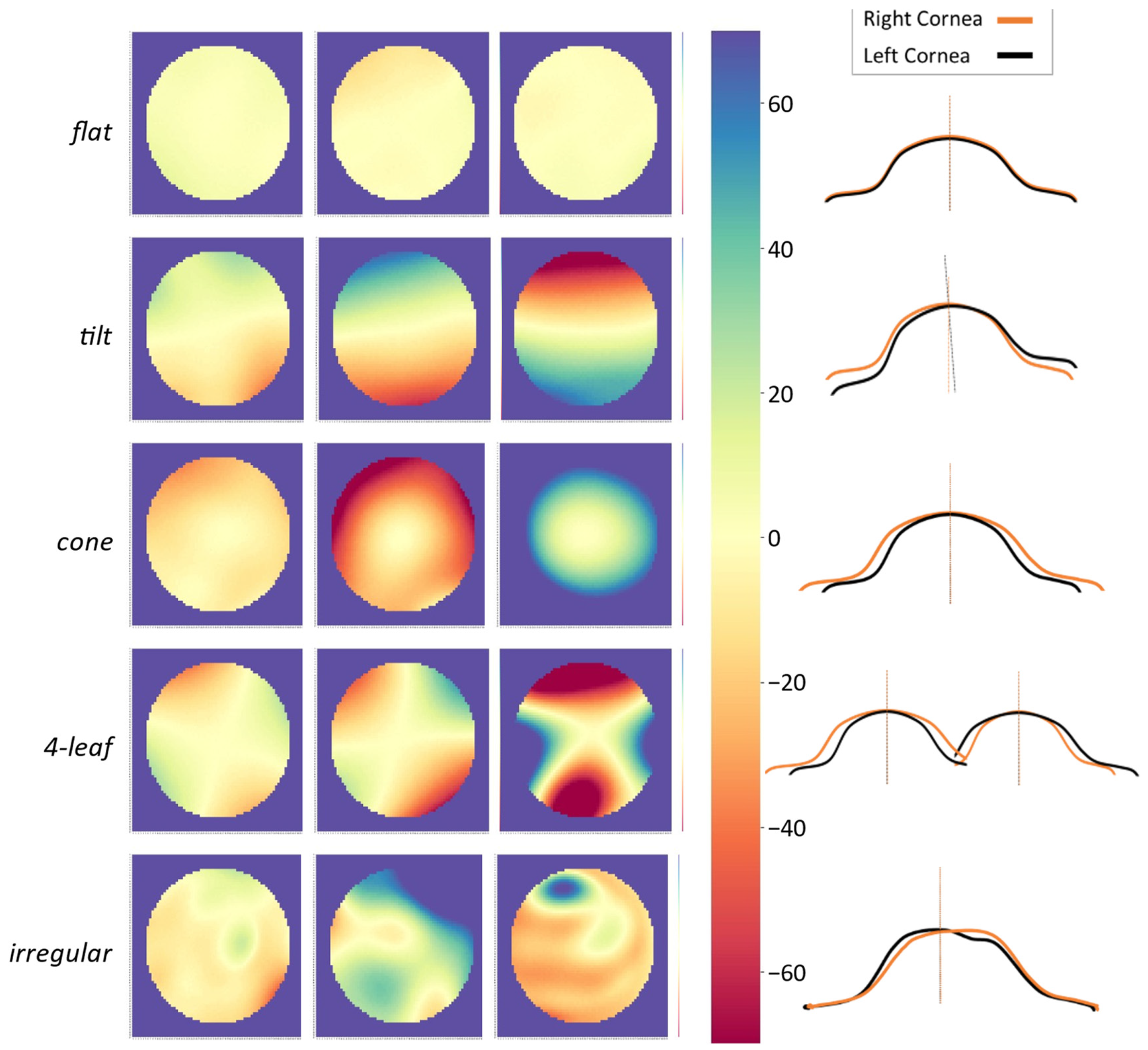
3.1. Symmetry Patterns in Colormaps
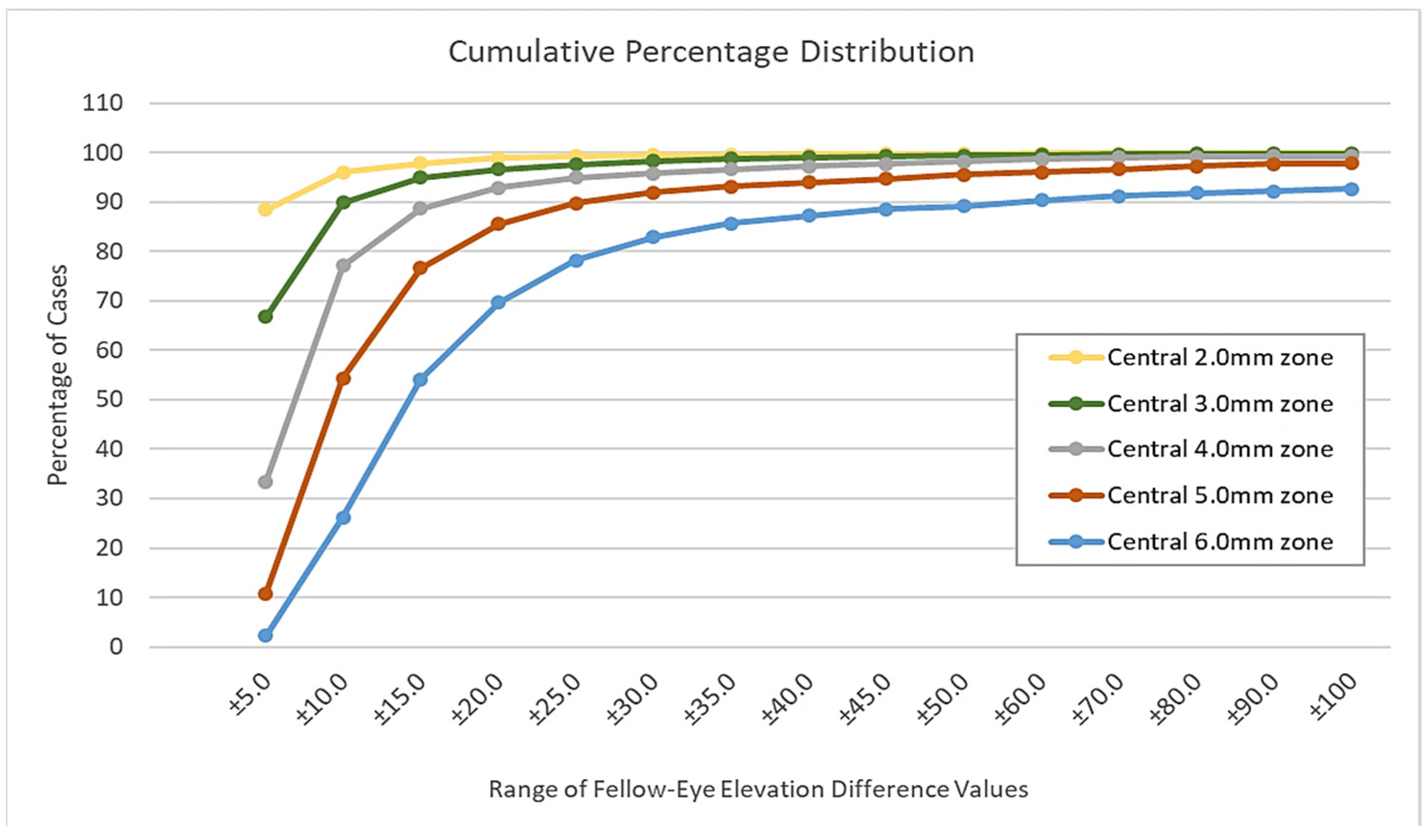
3.2. Data Exploration and Feature Engineering
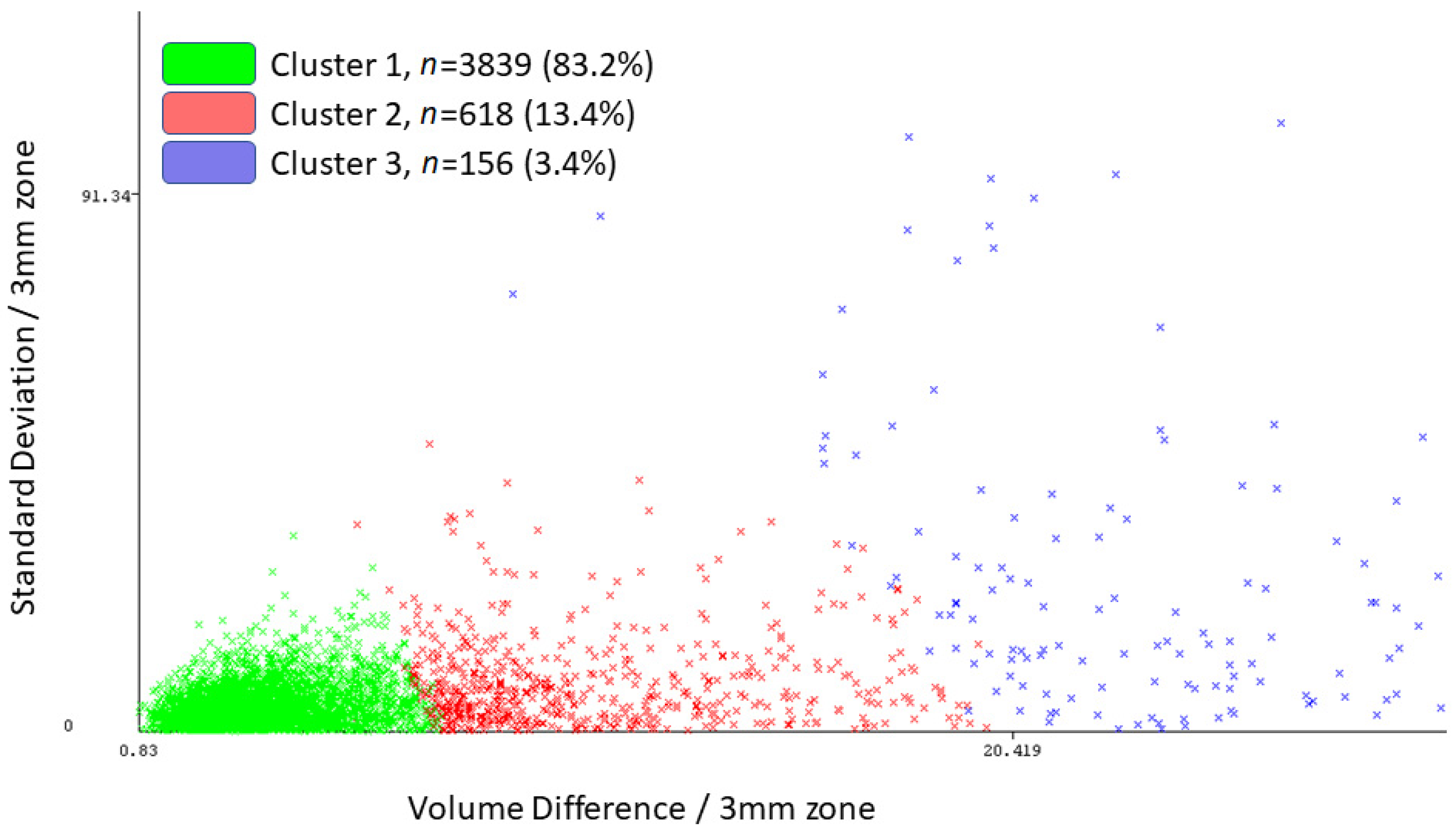
3.3. Unsupervised Machine Learning
3.4. Assessing Clusters Using Parameters Other Than Elevation
4. Discussion
5. Patents
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dowling, J.E.; Dowling Jr, J.L. Vision: How It Works and What Can Go Wrong; MIT Press: Cambridge, MA, USA, 2016. [Google Scholar]
- Nilsson, S.F.E.; Hoeve, J.V.; Wu, S.; Kaufman, P.L.; Alm, A. Adler’s Physiology of the Eye E-Book; Elsevier Health Sciences: Amsterdam, The Netherlands, 2011; ISBN 978-0-323-08116-0.0. [Google Scholar]
- Freddo, T.F.; Chaum, E. Anatomy of the Eye and Orbit: The Clinical Essentials; Wolters Kluwer Health: Philadelphia, PA, USA, 2017; ISBN 978-1-4698-7328-2. [Google Scholar]
- Daxecker, F. Christoph Scheiner’s Eye Studies. Doc. Ophthalmol. 1992, 81, 27–35. [Google Scholar] [CrossRef]
- Maguire, L.J.; Singer, D.E.; Klyce, S.D. Graphic Presentation of Computer-Analyzed Keratoscope Photographs. Arch. Ophthalmol. Chic. 1987, 105, 223–230. [Google Scholar] [CrossRef] [PubMed]
- Bogan, S.J.; Waring, G.O., III; Ibrahim, O.; Drews, C.; Curtis, L. Classification of Normal Corneal Topography Based on Computer-Assisted Videokeratography. Arch. Ophthalmol. 1990, 108, 945–949. [Google Scholar] [CrossRef] [PubMed]
- Rabinowitz, Y.S.; Yang, H.; Brickman, Y.; Akkina, J.; Riley, C.; Rotter, J.I.; Elashoff, J. Videokeratography Database of Normal Human Corneas. Br. J. Ophthalmol. 1996, 80, 610–616. [Google Scholar] [CrossRef] [Green Version]
- Motlagh, M.N.; Moshirfar, M.; Murri, M.S.; Skanchy, D.F.; Momeni-Moghaddam, H.; Ronquillo, Y.C.; Hoopes, P.C. Pentacam® Corneal Tomography for Screening of Refractive Surgery Candidates: A Review of the Literature, Part I. Med. Hypothesis Discov. Innov. Ophthalmol. 2019, 8, 177–203. [Google Scholar]
- Zhang, X.; Munir, S.Z.; Sami Karim, S.A.; Munir, W.M. A Review of Imaging Modalities for Detecting Early Keratoconus. Eye Lond. Engl. 2021, 35, 173–187. [Google Scholar] [CrossRef]
- Pentacam Interpretation Guideline - Third Edition. Available online: https://www.pentacam.com/fileadmin/user_upload/pentacam.de/downloads/interpretations-leitfaden/interpretation_guideline_3rd_edition_0915.pdf (accessed on 13 December 2020).
- Belin, M.W.; Kundu, G.; Shetty, N.; Gupta, K.; Mullick, R.; Thakur, P. ABCD: A New Classification for Keratoconus. Indian J. Ophthalmol. 2020, 68, 2831–2834. [Google Scholar] [CrossRef]
- Doctor, K.; Vunnava, K.P.; Shroff, R.; Kaweri, L.; Lalgudi, V.G.; Gupta, K.; Kundu, G. Simplifying and Understanding Various Topographic Indices for Keratoconus Using Scheimpflug Based Topographers. Indian J. Ophthalmol. 2020, 68, 2732–2743. [Google Scholar] [CrossRef]
- Hashemi, H.; Mehravaran, S. Day to Day Clinically Relevant Corneal Elevation, Thickness, and Curvature Parameters Using the Orbscan II Scanning Slit Topographer and the Pentacam Scheimpflug Imaging Device. Middle East Afr. J. Ophthalmol. 2010, 17, 44–55. [Google Scholar] [CrossRef]
- Klyce, S.D. Chasing the Suspect: Keratoconus. Br. J. Ophthalmol. 2009, 93, 845–847. [Google Scholar] [CrossRef]
- Cheng, C.Y.; Liu, J.H.; Chiang, S.C.; Chen, S.J.; Hsu, W.M. Statistics in Ophthalmic Research: Two Eyes, One Eye or the Mean? Zhonghua Yi Xue Za Zhi Chin. Med. J. Free China Ed 2000, 63, 885–892. [Google Scholar]
- Armstrong, R.A. Statistical Guidelines for the Analysis of Data Obtained from One or Both Eyes. Ophthalmic Physiol. Opt. J. Br. Coll. Ophthalmic Opt. Optom. 2013, 33, 7–14. [Google Scholar] [CrossRef]
- Zhang, H.G.; Ying, G. Statistical Approaches in Published Ophthalmic Clinical Science Papers: A Comparison to Statistical Practice Two Decades Ago. Br. J. Ophthalmol. 2018, 102, 1188–1191. [Google Scholar] [CrossRef]
- Dingeldein, S.A.; Klyce, S.D. The Topography of Normal Corneas. Arch. Ophthalmol. Chic. 1989, 107, 512–518. [Google Scholar] [CrossRef]
- Corbett, M.C.; O’Brart, D.P.S.; Saunders, D.C.; Rosen, E.S. The Topography of the Normal Cornea. Eur. J. Implant Refract. Surg. 1994, 6, 286–297. [Google Scholar] [CrossRef]
- Bao, F.; Chen, H.; Yu, Y.; Yu, J.; Zhou, S.; Wang, J.; Wang, Q.; Elsheikh, A. Evaluation of the Shape Symmetry of Bilateral Normal Corneas in a Chinese Population. PLoS ONE 2013, 8, e73412. [Google Scholar] [CrossRef]
- Durr, G.M.; Auvinet, E.; Ong, J.; Meunier, J.; Brunette, I. Corneal Shape, Volume, and Interocular Symmetry: Parameters to Optimize the Design of Biosynthetic Corneal Substitutes. Investig. Ophthalmol. Vis. Sci. 2015, 56, 4275–4282. [Google Scholar] [CrossRef]
- Cavas-Martínez, F.; Piñero, P.P.; Fernández-Pacheco, D.G.; Mira, J.; Cañavate, F.J.F.; Alió, J.L. Assessment of Pattern and Shape Symmetry of Bilateral Normal Corneas by Scheimpflug Technology. Symmetry 2018, 10, 453. [Google Scholar] [CrossRef] [Green Version]
- Myrowitz, E.H.; Kouzis, A.C.; O’Brien, T.P. High Interocular Corneal Symmetry in Average Simulated Keratometry, Central Corneal Thickness, and Posterior Elevation. Optom. Vis. Sci. Off. Publ. Am. Acad. Optom. 2005, 82, 428–431. [Google Scholar] [CrossRef]
- Khachikian, S.S.; Belin, M.W.; Ciolino, J.B. Intrasubject Corneal Thickness Asymmetry. J. Refract. Surg. 2008, 24, 606–609. [Google Scholar] [CrossRef]
- Falavarjani, K.G.; Modarres, M.; Joshaghani, M.; Azadi, P.; Afshar, A.E.; Hodjat, P. Interocular Differences of the Pentacam Measurements in Normal Subjects. Clin. Exp. Optom. 2010, 93, 26–30. [Google Scholar] [CrossRef]
- Li, Y.; Bao, F.J. Interocular Symmetry Analysis of Bilateral Eyes. J. Med. Eng. Technol. 2014, 38, 179–187. [Google Scholar] [CrossRef]
- Xu, G.; Hu, Y.; Zhu, S.; Guo, Y.; Xiong, L.; Fang, X.; Liu, J.; Zhang, Q.; Huang, N.; Zhou, J.; et al. A Multicenter Study of Interocular Symmetry of Corneal Biometrics in Chinese Myopic Patients. Sci. Rep. 2021, 11, 5536. [Google Scholar] [CrossRef] [PubMed]
- Fotouhi, A.; Hashemi, H.; Shariati, M.; Emamian, M.H.; Yazdani, K.; Jafarzadehpur, E.; Koohian, H.; Khademi, M.R.; Hodjatjalali, K.; Kheirkhah, A.; et al. Cohort Profile: Shahroud Eye Cohort Study. Int. J. Epidemiol. 2013, 42, 1300–1308. [Google Scholar] [CrossRef]
- About ShECS. Available online: http://en.shecs.info/ (accessed on 15 December 2020).
- Frank, E.; Hall, M.A.; Witten, I.H. The WEKA Workbench. Online Appendix for “Data Mining: Practical Machine Learning Tools and Techniques”, 4th ed.; Morgan Kaufmann: San Francisco, CA, USA, 2016. [Google Scholar]
- Fathy, A.; Lopes, B.T.; Ambrósio, R.; Wu, R.; Abass, A. The Efficiency of Using Mirror Imaged Topography in Fellow Eyes Analyses of Pentacam HR Data. Symmetry 2021, 13, 2132. [Google Scholar] [CrossRef]
- Fraenkel, D.; Hamon, L.; Daas, L.; Flockerzi, E.; Suffo, S.; Eppig, T.; Seitz, B. Tomographically Normal Partner Eye in Very Asymmetrical Corneal Ectasia: Biomechanical Analysis. J. Cataract Refract. Surg. 2021, 47, 366–372. [Google Scholar] [CrossRef] [PubMed]
- Alzaben, Z.; Gammoh, Y.; Freixas, M.; Zaben, A.; Zapata, M.A.; Koff, D.N. Inter-Ocular Asymmetry in Anterior Corneal Aberrations Using Placido Disk-Based Topography. Clin. Ophthalmol. Auckl. 2020, 14, 1451–1457. [Google Scholar] [CrossRef] [PubMed]
- Crahay, F.-X.; Debellemanière, G.; Tobalem, S.; Ghazal, W.; Moran, S.; Gatinel, D. Quantitative Comparison of Corneal Surface Areas in Keratoconus and Normal Eyes. Sci. Rep. 2021, 11, 6840. [Google Scholar] [CrossRef]
- Saad, A.; Guilbert, E.; Gatinel, D. Corneal Enantiomorphism in Normal and Keratoconic Eyes. J. Refract. Surg. 2014, 30, 542–547. [Google Scholar] [CrossRef] [Green Version]
- Galletti, J.D.; Vázquez, P.R.R.; Minguez, N.; Delrivo, M.; Bonthoux, F.F.; Pförtner, T.; Galletti, J.G. Corneal Asymmetry Analysis by Pentacam Scheimpflug Tomography for Keratoconus Diagnosis. J. Refract. Surg. 2015, 31, 116–123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Naderan, M.; Rajabi, M.T.; Zarrinbakhsh, P. Intereye Asymmetry in Bilateral Keratoconus, Keratoconus Suspect and Normal Eyes and Its Relationship with Disease Severity. Br. J. Ophthalmol. 2017, 101, 1475–1482. [Google Scholar] [CrossRef] [PubMed]
- Henriquez, M.A.; Izquierdo, L.; Belin, M.W. Intereye Asymmetry in Eyes with Keratoconus and High Ammetropia: Scheimpflug Imaging Analysis. Cornea 2015, 34, S57–S60. [Google Scholar] [CrossRef] [PubMed]
- Eppig, T.; Langenbucher, A.; Papavasileiou, K.; Spira-Eppig, C.; Goebels, S.; Seitz, B.; El-Husseiny, M.; Lenhart, M.; Szentmáry, N. Asymmetry between Left and Right Eyes in Keratoconus Patients Increases with the Severity of the Worse Eye. Curr. Eye Res. 2018, 43, 848–855. [Google Scholar] [CrossRef]
- Pentacam_Guideline_3rd_0218_k.Pdf. Available online: https://www.pentacam.com/fileadmin/user_upload/pentacam.de/downloads/interpretations-leitfaden/Pentacam_Guideline_3rd_0218_k.pdf (accessed on 15 December 2021).
- Belin, M.W.; Khachikian, S.S.; Ambrósio, R.J.; Salomão, M. Keratoconus/Ectasia Detection with the Oculus Pentacam: Belin/Ambrósio Enhanced Ectasia Display. Highlights Ophthalmol. 2007, 35, 5–12. [Google Scholar]
- Henriquez, M.A.; Izquierdo, L.J.; Mannis, M.J. Intereye Asymmetry Detected by Scheimpflug Imaging in Subjects with Normal Corneas and Keratoconus. Cornea 2013, 32, 779–782. [Google Scholar] [CrossRef]
- Dienes, L.; Kránitz, K.; Juhász, É.; Gyenes, A.; Takács, Á.; Miháltz, K.; Nagy, Z.Z.; Kovács, I. Evaluation of Intereye Corneal Asymmetry in Patients with Keratoconus. A Scheimpflug Imaging Study. PLoS ONE 2014, 9, e108882. [Google Scholar] [CrossRef] [Green Version]
- Kovács, I.; Miháltz, K.; Kránitz, K.; Juhász, É.; Takács, Á.; Dienes, L.; Gergely, R.; Nagy, Z.Z. Accuracy of Machine Learning Classifiers Using Bilateral Data from a Scheimpflug Camera for Identifying Eyes with Preclinical Signs of Keratoconus. J. Cataract Refract. Surg. 2016, 42, 275–283. [Google Scholar] [CrossRef]
- Hashemi, H.; Asharlous, A.; Yekta, A.; Ostadimoghaddam, H.; Mohebi, M.; Aghamirsalim, M.; Khabazkhoob, M. Enantiomorphism and Rule Similarity in the Astigmatism Axes of Fellow Eyes: A Population-Based Study. J. Optom. 2019, 12, 44–54. [Google Scholar] [CrossRef]
- Ostadimoghaddam, H.; Fotouhi, A.; Hashemi, H.; Yekta, A.A.; Heravian, J.; Hemmati, B.; Jafarzadehpur, E.; Rezvan, F.; Khabazkhoob, M. The Prevalence of Anisometropia in Population Base Study. Strabismus 2012, 20, 152–157. [Google Scholar] [CrossRef]
- Dobson, V.; Harvey, E.M.; Miller, J.M.; Clifford-Donaldson, C.E. Anisometropia Prevalence in a Highly Astigmatic School-Aged Population. Optom. Vis. Sci. Off. Publ. Am. Acad. Optom. 2008, 85, 512–519. [Google Scholar] [CrossRef] [Green Version]
- O’Donoghue, L.; McClelland, J.F.; Logan, N.S.; Rudnicka, A.R.; Owen, C.G.; Saunders, K.J. Profile of Anisometropia and Aniso-Astigmatism in Children: Prevalence and Association with Age, Ocular Biometric Measures, and Refractive Status. Investig. Ophthalmol. Vis. Sci. 2013, 54, 602–608. [Google Scholar] [CrossRef] [PubMed]
- Belin, M.W.; Khachikian, S.S. An Introduction to Understanding Elevation-Based Topography: How Elevation Data Are Displayed—A Review. Clin. Exp. Ophthalmol. 2009, 37, 14–29. [Google Scholar] [CrossRef] [PubMed]
- Hayashi, K.; Kawahara, S.; Manabe, S.; Hirata, A. Changes in Irregular Corneal Astigmatism with Age in Eyes with and without Cataract Surgery. Investig. Ophthalmol. Vis. Sci. 2015, 56, 7988–7998. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Emamian, M.H.; Hashemi, H.; Khabazkhoob, M.; Malihi, S.; Fotouhi, A. Cohort Profile: Shahroud Schoolchildren Eye Cohort Study (SSCECS). Int. J. Epidemiol. 2019, 48, 27. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Attribute | Full n = 4613 | Cluster 1 n = 3839 | Cluster 2 n = 618 | Cluster 3 n = 156 |
|---|---|---|---|---|
| Central 95% Range/6.0 mm | 20.7 | 14.1 | 42.1 | 97.0 |
| Absolute Mean/3.0 mm | 0.8 | 0.6 | 1.2 | 4.5 |
| Standard Deviation/3.0 mm | 2.0 | 1.3 | 3.7 | 11.4 |
| Volume Difference/3.0 mm | 5.7 | 4.3 | 8.2 | 30.8 |
| Zone | Statistic | Full Sample n = 4613 | Cluster 1 n = 3839 | Cluster 2 n = 618 | Cluster 3 n = 156 |
|---|---|---|---|---|---|
| 2.0 mm | Abs-Mean | 0.5 ± 2.1 | 0.3 ± 0.3 | 0.6 ± 0.6 | 3.5 ± 10.7 |
| SD | 1.3 ± 2.0 | 0.9 ± 0.4 | 2.2 ± 1.2 | 7.4 ± 8.1 | |
| Min | −2.8 ± 3.6 | −2.0 ± 1.1 | −4.8 ± 2.6 | −15.4 ± 11.4 | |
| Max | 2.9 ± 6.1 | 2.0 ± 1.2 | 5.0 ± 3.2 | 17.2 ± 28.3 | |
| Range | 5.7 ± 8.6 | 3.9 ± 1.6 | 9.8 ± 4.7 | 32.5 ± 34.3 | |
| Abs-Max | 3.7 ± 6.5 | 2.5 ± 1.1 | 6.2 ± 3.0 | 21.9 ± 28.1 | |
| 3.0 mm | Abs-Mean | 0.8 ± 2.3 | 0.6 ± 0.5 | 1.2 ± 1.1 | 5.5 ± 11.2 |
| SD | 2.0 ± 3.1 | 1.3 ± 0.5 | 3.7 ± 1.5 | 12.5 ± 12.0 | |
| Min | −4.8 ± 6.6 | −3.2 ± 1.8 | −8.7 ± 4.2 | −28.0 ± 21.9 | |
| Max | 2.9 ± 6.1 | 2.0 ± 1.2 | 5.0 ± 3.2 | 17.2 ± 28.3 | |
| Range | 9.6 ± 14.3 | 6.4 ± 2.5 | 17.5 ± 6.7 | 57.6 ± 54.0 | |
| Abs-Max | 6.3 ± 9.8 | 4.2 ± 1.8 | 11.1 ± 4.6 | 38.5 ± 38.3 | |
| 4.0 mm | Abs-Mean | 1.3 ± 2.8 | 0.9 ± 0.7 | 1.8 ± 1.6 | 8.0 ± 12.6 |
| SD | 2.9 ± 4.5 | 1.9 ± 0.9 | 5.6 ± 2.2 | 18.9 ± 16.3 | |
| Min | −7.5 ± 10.5 | −5.0 ± 2.9 | −14.2 ± 7.0 | −44.0 ± 34.2 | |
| Max | 7.8 ± 15.4 | 5.0 ± 6.9 | 15.1 ± 16.5 | 46.7 ± 53.4 | |
| Range | 15.3 ± 23.0 | 10.0 ± 7.4 | 29.3 ± 18.3 | 90.7 ± 76.1 | |
| Abs-Max | 10.2 ± 16.5 | 6.8 ± 6.8 | 19.2 ± 16.0 | 60.7 ± 52.1 | |
| 5.0 mm | Abs-Mean | 1.8 ± 3.5 | 1.3 ± 1.1 | 2.6 ± 2.5 | 11.0 ± 14.4 |
| SD | 4.4 ± 6.9 | 2.8 ± 2.7 | 8.6 ± 6.0 | 26.9 ± 21.0 | |
| Min | −11.1 ± 15.1 | −7.3 ± 4.3 | −21.7 ± 11.3 | −63.3 ± 48.0 | |
| Max | 13.6 ± 35.5 | 9.1 ± 27.1 | 26.8 ± 46.7 | 71.8 ± 78.3 | |
| Range | 24.7 ± 43.3 | 16.4 ± 27.8 | 48.5 ± 48.4 | 135.1 ± 105 | |
| Abs-Max | 17.4 ± 36.4 | 11.7 ± 26.8 | 33.8 ± 45.7 | 92.1 ± 75.3 | |
| 6.0 mm | Abs-Mean | 2.6 ± 4.7 | 1.9 ± 2.3 | 4.0 ± 5.0 | 14.0 ± 16.9 |
| SD | 7.3 ± 13.3 | 5.0 ± 9.6 | 13.8 ± 15.2 | 38.0 ± 28.2 | |
| Min | −16.0 ± 20.9 | −10.7 ± 6.4 | −31.5 ± 18.1 | −85.4 ± 64.6 | |
| Max | 31.3 ± 92.6 | 23.8 ± 83.4 | 53.3 ± 109.0 | 129.6 ± 149.8 | |
| Range | 47.3 ± 99.3 | 34.5 ± 84.3 | 84.7 ± 110.6 | 214.9 ± 175.5 | |
| Abs-Max | 36.8 ± 92.4 | 27.6 ± 82.8 | 64.1 ± 106.7 | 154.4 ± 141.8 |
| Parameter | Total | Cluster 1 | Cluster 2 | Cluster 3 | p-Value * | |
|---|---|---|---|---|---|---|
| n = 4613 | n = 3839 | n = 618 | n = 156 | |||
| Apical Thickness (µm) | OD | 529.9 ± 33.7 | 530.9 ± 32.0 | 527.6 ± 34.5 | 515.4 ± 59.2 | <0.001 |
| OS | 530.6 ± 33.8 | 531.5 ± 32.2 | 527.9 ± 35.3 | 519.6 ± 55.4 | <0.001 | |
| i-dif | 9.6 ± 13.2 | 8.0 ± 6.4 | 11.4 ± 11.1 | 39.7 ± 51.7 | <0.001 | |
| Minimum Thickness (µm) | OD | 524.5 ± 37.0 | 526.6 ± 32.1 | 521.2 ± 34.7 | 486.6 ± 93.7 | <0.001 |
| OS | 525.2 ± 35.6 | 527.2 ± 32.3 | 521.0 ± 35.9 | 493.5 ± 73.8 | <0.001 | |
| i-dif | 10.3 ± 20.0 | 8.1 ± 6.4 | 12.0 ± 12.1 | 56.8 ± 89.5 | <0.001 | |
| Maximum Keratometry (D) | OD | 44.2 ± 1.7 | 44.1 ± 1.6 | 44.5 ± 1.9 | 45.5 ± 3.2 | <0.001 |
| OS | 44.2 ± 1.8 | 44.1 ± 1.6 | 44.6 ± 1.9 | 45.8 ± 3.8 | <0.001 | |
| i-dif | 0.5 ± 0.8 | 0.3 ± 0.3 | 0.7 ± 0.6 | 2.4 ± 3.2 | <0.001 | |
| Mean Keratometry (D) | OD | 43.7 ± 1.7 | 43.7 ± 1.5 | 43.8 ± 1.8 | 44.0 ± 3.3 | 0.017 |
| OS | 43.8 ± 1.7 | 43.7 ± 1.5 | 43.9 ± 1.8 | 44.3 ± 3.3 | <0.001 | |
| i-dif | 0.4 ± 0.6 | 0.3 ± 0.2 | 0.6 ± 0.5 | 2.3 ± 2.5 | <0.001 | |
| Corneal Astigmatism (D) | OD | 0.9 ± 1.1 | 0.8 ± 0.5 | 1.3 ± 1.1 | 3.0 ± 4.2 | <0.001 |
| OS | 0.9 ± 1.1 | 0.8 ± 0.5 | 1.4 ± 1.3 | 3.0 ± 3.9 | <0.001 | |
| i-dif | 0.5 ± 1.1 | 0.4 ± 0.3 | 1.0 ± 1.1 | 3.3 ± 4.7 | <0.001 | |
| Pentacam Category | Parameter | Total | Cluster 1 | Cluster 2 | Cluster 3 |
|---|---|---|---|---|---|
| (n = 4613) | (n = 3839) | (n = 618) | (n = 156) | ||
| Bilateral-normal QS-OK | n | 2975 (64.5%) | 2696 (90.6%) | 257 (8.6%) | 22 (0.7%) |
| Ap-thick | 8.2 ± 6.6 | 8.0 ± 6.2 | 10.0 ± 8.7 | 14.4 ± 10.3 | |
| Min-thick | 8.3 ± 6.5 | 8.1 ± 6.2 | 9.9 ± 8.6 | 12.5 ± 10.7 | |
| MaxK | 0.3 ± 0.3 | 0.3 ± 0.3 | 0.6 ± 0.6 | 0.9 ± 1.3 | |
| MeanK | 0.3 ± 0.3 | 0.3 ± 0.2 | 0.4 ± 0.4 | 1.4 ± 1.2 | |
| Cor-ast | 0.4 ± 0.5 | 0.3 ± 0.3 | 1.0 ± 1.0 | 1.9 ± 2.1 | |
| KS-abnormal QS-OK | n | 684 (14.8%) | 512 (74.9%) | 144 (21.1%) | 28 (4.1%) |
| Ap-thick | 9.5 ± 9.4 | 8.1 ± 6.7 | 11.4 ± 10.3 | 25.8 ± 22.1 | |
| Min-thick | 10.0 ± 11.8 | 8.0 ± 6.5 | 11.9 ± 9.7 | 36.3 ± 37.6 | |
| MaxK | 0.5 ± 1.0 | 0.4 ± 0.3 | 0.7 ± 0.7 | 2.3 ± 4.3 | |
| MeanK | 0.5 ± 0.7 | 0.3 ± 0.2 | 0.7 ± 0.6 | 2.0 ± 2.2 | |
| Cor-ast | 0.6 ± 1.3 | 0.4 ± 0.3 | 1.0 ± 1.1 | 3.3 ± 4.9 | |
| KCN-1-2 QS-OK | n | 84 (1.8%) | 30 (35.7%) | 36 (42.9%) | 18 (21.4%) |
| Ap-thick | 15.8 ± 14.1 | 8.6 ± 7.3 | 14.9 ± 10.5 | 29.6 ± 19.0 | |
| Min-thick | 16.9 ± 17.6 | 9.2 ± 7.2 | 14.4 ± 10.2 | 34.5 ± 27.6 | |
| MaxK | 1.2 ± 1.1 | 0.6 ± 0.4 | 1.1 ± 0.9 | 2.3 ± 1.6 | |
| MeanK | 0.9 ± 1.0 | 0.4 ± 0.3 | 0.9 ± 0.6 | 1.8 ± 1.6 | |
| Cor-ast | 1.0 ± 1.0 | 0.5 ± 0.4 | 1.0 ± 1.0 | 1.7 ± 1.5 | |
| KCN-3-4 QS-OK | n | 10 (0.2%) | 0 (0.0%) | 4 (40.0%) | 6 (60.0%) |
| Ap-thick | 33.2 ± 34.1 | 16.0 ± 6.8 | 44.7 ± 40.9 | ||
| Min-thick | 29.4 ± 28.8 | 18.3 ± 9.8 | 36.8 ± 35.7 | ||
| MaxK | 3.7 ± 4.4 | 2.1 ± 0.8 | 4.8 ± 5.6 | ||
| MeanK | 3.2 ± 4.4 | 1.9 ± 0.5 | 4.0 ± 5.8 | ||
| Cor-ast | 1.7 ± 1.3 | 1.9 ± 0.9 | 1.6 ± 1.6 |
| Parameter | 1 | 2 | 3 | 4 | 5 |
|---|---|---|---|---|---|
| Row 1 |  |  |  |  |  |
| ΔAst | 6.2 | 5.6 | 5.6 | 4.0 | 3.7 |
| ΔmaxK | 0.54 | 0.41 | 0.12 | 0.33 | 0.00 |
| ΔpAx | 7.0 | 3.0 | 19.0 | 23.0 | 34.0 |
| ΔpThin | 1.0 | 4.0 | 4.0 | 21.0 | 36.0 |
| ΔmaxEle | 12.0 | 17.0 | 23.0 | 13.0 | 18.0 |
| Row 2 |  |  |  |  |  |
| ΔAst | 3.5 | 3.4 | 2.5 | 1.2 | 1.0 |
| ΔmaxK | 0.28 | 0.24 | 1.77 | 0.61 | 0.91 |
| ΔpAx | 6.0 | 1.0 | 5.0 | 25.0 | 11.0 |
| ΔpThin | 1.0 | 10.0 | 2.0 | 27.0 | 15.0 |
| ΔmaxEle | 12.0 | 12.0 | 7.0 | 27.0 | 14.0 |
| Parameter | 1 | 2 | 3 | 4 | 5 |
|---|---|---|---|---|---|
| Row 3 |  |  |  | ||
| ΔAst | 0.5 | 0.7 | 0.6 | ||
| ΔmaxK | 5.11 | 3.27 | 2.61 | ||
| ΔpAx | 35.0 | 3.0 | 22.0 | ||
| ΔpThin | 31.0 | 2.0 | 25.0 | ||
| ΔmaxEle | 11.0 | 27.0 | 9.0 | ||
| Row 4 |  |  |  |  | |
| ΔAst | 0.2 | 0.1 | 0.1 | 0.9 | |
| ΔmaxK | 0.06 | 0.70 | 0.68 | 0.00 | |
| ΔpAx | 22.0 | 22.0 | 20.0 | 19.0 | |
| ΔpThin | 1.0 | 20.0 | 17.0 | 19.0 | |
| ΔmaxEle | 9.0 | 22.0 | 13.0 | 15.0 | |
| Row 5 |  |  |  |  |  |
| ΔAst | 0.4 | 0.2 | 0.3 | 0.2 | 0.4 |
| ΔmaxK | 0.54 | 0.70 | 0.06 | 0.34 | 0.06 |
| ΔpAx | 9.0 | 0.0 | 10.0 | 14.0 | 7.0 |
| ΔpThin | 8.0 | 1.0 | 10.0 | 12.0 | 7.0 |
| ΔmaxEle | 23.0 | 17.0 | 17.0 | 16.0 | 13.0 |
| First Author [Ref #] | Studied Sample | Reference Surface | Anterior Elevation Measure | Mean Interocular Difference (µm) |
|---|---|---|---|---|
| Falavarjani [25] | 275 normal | Float BFS with auto diameter | Maximum in the central 4.0 mm | 2.2 (range, 0–21) |
| Durr * [21] | 3835 normal | Average BFS of all eyes | Average elevation in the central 6.0 mm † | Range ± 6.0 |
| Saad * [35] | 51 normal 32 KCN | Default float BFS | Maximum/at thinnest point | Normal: 0.0 ± 0.0/0.0 ± 0.0 KCN: 0.02 ± 0.01/0.02 ± 0.01 |
| Galletti [36] | 177 normal 44 intermediate 121 KCN | No mention | At thinnest corneal location | Central 98% range Normal: 4.0 KCN: 31.0 |
| Naderan [37] | 306 normal 68 suspect 446 KCN | 8.0 mm BFS | At thinnest point within the central 3.0 mm | Normal: 1.3 ± 0.7 KCS: 5.5 ± 4.8 KCN: 14.0 ± 10.4 |
| Henriquez [38] | 341 normal 50 high ammetropia 294 KCN | 8.0 mm BFS | Maximum/at thinnest point | Normal: 1.4 ± 1.4/1.1 ± 1.0 KCN: 10.3 ± 11.0/8.7 ± 9.9 |
| Eppig [39] | 68 normal 350 KCN | No mention | Elevation deviation | Normal: 0.46 ± 0.39 KCN: 7.8 ± 7.4 |
| Current Project | 4615 general population | Raw data (the fellow eye) | Values and descriptive statistics of all corresponding points in the central 2.0–6.0 mm | See Table 2 and Table 3 |
| First Author [Ref #] | Group | Corneal Thickness (μm) | Simulated Keratometry (D) | ||||
|---|---|---|---|---|---|---|---|
| Central | Thinnest | Steep | Flat | Mean | Diff | ||
| Myrowitz * [23] | normal | - | 8.0 ± 7.0 | - | - | 0.5 ± 0.4 | - |
| Khachikian [24] | normal | 8.8 ± 7.2 | 9.0 ± 8.3 | - | - | - | - |
| Henriquez [42] | normal | 10.2 ± 7.9 | 11.0 ± 8.2 | 0.3 ± 0.3 | 0.3 ± 0.2 | - | - |
| KCN | 25.9 ± 24.1 | 30.2 ± 29.1 | 3.8 ± 4.2 | 2.7 ± 3.3 | - | - | |
| Henriquez [38] | normal | 10.3 ± 7.9 | 11.0 ± 8.2 | - | - | - | - |
| KCN | 25.9 ± 24.1 | 30.2 ± 29.1 | - | - | - | - | |
| Dienes [43] | normal | 5.6 ± 4.9 | 6.6 ± 5.3 | 0.4 ± 0.4 | 0.4 ± 0.4 | - | - |
| KCN | 30.1 ± 35.8 | 39.7 ± 36.4 | 4.4 ± 5.1 | 2.7 ± 3.6 | - | - | |
| Kovács [44] | normal | 6.3 ± 6.9 | 6.9 ± 7.5 | 0.3 ± 0.2 | 0.3 ± 0.2 | - | - |
| KCN | 29.9 ± 34.3 | 39.8 ± 29.1 | 3.3 ± 2.6 | 2.8 ± 3.1 | - | - | |
| Naderan [37] | normal | 4.3 ± 1.6 | 5.9 ± 2.2 | 0.3 ± 0.2 | 0.2 ± 0.2 | 0.2 ± 0.2 | 0.1 ± 0.1 |
| suspect | 12.8 ± 10.0 | 13.7 ± 10.9 | 1.0 ± 1.2 | 0.6 ± 0.8 | 0.7 ± 0.8 | 1.0 ± 0.8 | |
| KCN | 29.4 ± 28.5 | 33.6 ± 33.2 | 4.3 ± 4.2 | 3.4 ± 3.7 | 3.7 ± 3.8 | 1.8 ± 1.5 | |
| Eppig [39] | normal | 6.0 ± 5.0 | 6.0 ± 5.0 | - | - | 0.2 ± 0.2 | 0.4 ± 0.4 |
| KCN | 34.0 ± 30.0 | 37.0 ± 32.0 | - | - | 3.8 ± 4.0 | 2.0 ± 1.7 | |
| Saad * [35] | normal | 5.4 ± 4.9 | 6.0 ± 5.0 | 0.3 ± 0.3 | 0.4 ± 0.3 | - | 0.3 ± 0.3 |
| KCN | 33.9 ± 37.0 | 35.7 ± 34.5 | 4.1 ± 2.9 | 2.4 ± 2.9 | - | 2.1 ± 2.3 | |
| Current Project † | Cluster 1 | 8.0 ± 6.3 | 8.1 ± 6.4 | 0.3 ± 0.3 | 0.3 ± 0.3 | 0.3 ± 0.2 | 0.3 ± 0.3 |
| Cluster 2 | 11.3 ± 10.5 | 11.9 ± 10.8 | 0.7 ± 0.7 | 0.8 ± 0.8 | 0.6 ± 0.5 | 1.0 ± 1.1 | |
| Cluster 3 | 41.1 ± 53.6 | 58.3 ± 92.5 | 2.5 ± 3.3 | 3.1 ± 3.8 | 2.3 ± 2.6 | 3.4 ± 4.9 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mehravaran, S.; Dehzangi, I.; Rahman, M.M. Interocular Symmetry Analysis of Corneal Elevation Using the Fellow Eye as the Reference Surface and Machine Learning. Healthcare 2021, 9, 1738. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare9121738
Mehravaran S, Dehzangi I, Rahman MM. Interocular Symmetry Analysis of Corneal Elevation Using the Fellow Eye as the Reference Surface and Machine Learning. Healthcare. 2021; 9(12):1738. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare9121738
Chicago/Turabian StyleMehravaran, Shiva, Iman Dehzangi, and Md Mahmudur Rahman. 2021. "Interocular Symmetry Analysis of Corneal Elevation Using the Fellow Eye as the Reference Surface and Machine Learning" Healthcare 9, no. 12: 1738. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare9121738