
Patients’ Perceptions and Satisfaction with the Outpatient Telemedicine Clinics during COVID-19 Era in Saudi Arabia: A Cross-Sectional Study

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
2.2. Sample Size Estimation
2.3. Sampling Procedure
2.4. Inclusion and Exclusion Criteria
2.5. Ethical Consideration
2.6. Data Collection Procedure
2.7. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO. Telemedicine: Opportunities and Developments in Member States. Report on the Second Global Survey on eHealth; World Health Organization: Geneva, Switzerland, 2010. [Google Scholar]
- Wootton, R. Telemedicine. BMJ 2001, 323, 557–560. [Google Scholar] [CrossRef]
- Mechanic, O.J.; Persaud, Y.; Kimball, A.B. Telehealth Systems. 2021. Available online: https://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/books/NBK459384/ (accessed on 10 September 2021).
- Mamlin, B.W.; Tierney, W.M. The Promise of Information and Communication Technology in Healthcare: Extracting Value From the Chaos. Am. J. Med. Sci. 2016, 351, 59–68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dekker, P.K.; Bhardwaj, P.; Singh, T.; Bekeny, J.C.; Kim, K.G.; Steinberg, J.S.; Evans, K.K.; Song, D.H.; Attinger, C.E.; Fan, K.L. Telemedicine in the Wake of the COVID-19 Pandemic: Increasing Access to Surgical Care. Plast. Reconstr. Surg. Glob. Open 2021, 9, e3228. [Google Scholar] [CrossRef]
- Galiero, R.; Pafundi, P.C.; Nevola, R.; Rinaldi, L.; Acierno, C.; Caturano, A.; Salvatore, T.; Adinolfi, L.E.; Costagliola, C.; Sasso, F.C. The Importance of Telemedicine during COVID-19 Pandemic: A Focus on Diabetic Retinopathy. J. Diabetes Res. 2020, 2020, 9036847. [Google Scholar] [CrossRef] [PubMed]
- Lakshin, G.; Banek, S.; Keese, D.; Rolle, U.; Schmedding, A. Telemedicine in the pediatric surgery in Germany during the COVID-19 pandemic. Pediatric Surg. Int. 2021, 37, 389–395. [Google Scholar] [CrossRef] [PubMed]
- Boxer, R.J. Advantages and utilization of telemedicine. mHealth 2019, 5, 12. [Google Scholar] [CrossRef] [PubMed]
- Kichloo, A.; Albosta, M.; Dettloff, K.; Wani, F.; El-Amir, Z.; Singh, J.; Aljadah, M.; Chakinala, R.C.; Kanugula, A.K.; Solanki, S.; et al. Telemedicine, the current COVID-19 pandemic and the future: A narrative review and perspectives moving forward in the USA. Fam. Med. Community Health 2020, 8, e000530. [Google Scholar] [CrossRef]
- Gajarawala, S.N.; Pelkowski, J.N. Telehealth benefits and barriers. J. Nurse Pract. 2021, 17, 218–221. [Google Scholar] [CrossRef] [PubMed]
- Monaghesh, E.; Hajizadeh, A. The role of telehealth during COVID-19 outbreak: A systematic review based on current evidence. BMC Public Health 2020, 20, 1193. [Google Scholar] [CrossRef] [PubMed]
- Dinesen, B.; Nonnecke, B.; Lindeman, D.; Toft, E.; Kidholm, K.; Jethwani, K.; Young, H.M.; Spindler, H.; Oestergaard, C.U.; Southard, J.A. Personalized telehealth in the future: A global research agenda. J. Med. Internet Res. 2016, 18, e5257. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berger, S.; Saut, A.M.; Berssaneti, F.T. Using patient feedback to drive quality improvement in hospitals: A qualitative study. BMJ Open 2020, 10, e037641. [Google Scholar] [CrossRef] [PubMed]
- Wong, E.; Mavondo, F.; Fisher, J. Patient feedback to improve quality of patient-centred care in public hospitals: A systematic review of the evidence. BMC Health Serv. Res. 2020, 20, 530. [Google Scholar] [CrossRef] [PubMed]
- Kruse, C.S.; Krowski, N.; Rodriguez, B.; Tran, L.; Vela, J.; Brooks, M. Telehealth and patient satisfaction: A systematic review and narrative analysis. BMJ Open 2017, 7, e016242. [Google Scholar] [CrossRef] [PubMed]
- Hardavella, G.; Aamli-Gaagnat, A.; Saad, N.; Rousalova, I.; Sreter, K.B. How to give and receive feedback effectively. Breathe 2017, 13, 327–333. [Google Scholar] [CrossRef] [PubMed]
- Ramaswamy, A.; Yu, M.; Drangsholt, S.; Ng, E.; Culligan, P.J.; Schlegel, P.N.; Hu, J.C. Patient Satisfaction With Telemedicine During the COVID-19 Pandemic: Retrospective Cohort Study. J. Med. Internet Res. 2020, 22, e20786. [Google Scholar] [CrossRef]
- Abdel Nasser, A.; Mohammed Alzahrani, R.; Al-Falah, C.A.; Muwafak Jreash, D.; Talea Almouled, N.; Salem Bakula, D.; Abed Ra’Oof, R. Measuring the Patients’ Satisfaction About Telemedicine Used in Saudi Arabia During COVID-19 Pandemic. Cureus 2021, 13, e13382. [Google Scholar] [CrossRef] [PubMed]
- MOH. Telemedicine. Available online: https://www.moh.gov.sa/en/Ministry/Information-and-services/Pages/Telemedicine.aspx (accessed on 21 September 2021).
- Alharbi, K.; Aldosari, M.; Alhassan, A.; Alshallal, K.; Altamimi, A.; Altulaihi, B. Patient satisfaction with virtual clinic during Coronavirus disease (COVID-19) pandemic in primary healthcare, Riyadh, Saudi Arabia. J. Fam. Community Med. 2021, 28, 48–54. [Google Scholar] [CrossRef]
- Koonin, L.M.; Hoots, B.; Tsang, C.A.; Leroy, Z.; Farris, K.; Jolly, B.; Antall, P.; McCabe, B.; Zelis, C.B.; Tong, I. Trends in the use of telehealth during the emergence of the COVID-19 pandemic—United States, January–March 2020. Morb. Mortal. Wkly. Rep. 2020, 69, 1595. [Google Scholar] [CrossRef] [PubMed]
- Holtz, B.E. Patients perceptions of telemedicine visits before and after the coronavirus disease 2019 pandemic. Telemed. E-Health 2021, 27, 107–112. [Google Scholar] [CrossRef] [PubMed]
- Khan, Z.A.; Zahoor, A.; Afzal, I.; Butt, U.; Siddiqui, A.M.; Khan, Z.; Shah, I.A.; Shah, J.A. Evaluation of Patient Perception and Satisfaction Toward the Use of Telemedicine During Pandemic of Novel Coronavirus in Pakistan. Telemed. E-Health 2021, 10, 1174–1179. [Google Scholar] [CrossRef]
- Grossman, Z.; Chodick, G.; Reingold, S.M.; Chapnick, G.; Ashkenazi, S. The future of telemedicine visits after COVID-19: Perceptions of primary care pediatricians. Isr. J. Health Policy Res. 2020, 9, 53. [Google Scholar] [CrossRef]
- Lagasse, J. Most Consumers Want to Keep Telehealth after the COVID-19 Pandemic. Available online: https://www.healthcarefinancenews.com/news/most-consumers-want-keep-telehealth-after-covid-19-pandemic (accessed on 24 October 2021).
- Mubaraki, A.A.; Alrabie, A.D.; Sibyani, A.K.; Aljuaid, R.S.; Bajaber, A.S.; Mubaraki, M.A. Advantages and disadvantages of telemedicine during the COVID-19 pandemic era among physicians in Taif, Saudi Arabia. Saudi Med. J. 2021, 42, 110–115. [Google Scholar] [CrossRef] [PubMed]
- Park, H.; Choi, S.O. Digital Innovation Adoption and Its Economic Impact Focused on Path Analysis at National Level. J. Open Innov. Technol. Market Complex. 2019, 5, 56. [Google Scholar] [CrossRef] [Green Version]
- Millan PhD, J.; Yunda PhD, L.; Valencia, A. Analysis of Economic and Business Factors Influencing Disruptive Innovation in Telehealth. Nova 2017, 15, 125–136. [Google Scholar] [CrossRef] [Green Version]
- Alsheddi, A.; Sharma, D.; Talukder, M. Investigating the Determinants of Innovation Adoption in Saudi Arabia. Int. Rev. Bus. Res. Pap. 2019, 15, 37–59. [Google Scholar] [CrossRef]
- Adams, L.; Lester, S.; Hoon, E.; van der Haak, H.; Proudman, C.; Hall, C.; Whittle, S.; Proudman, S.; Hill, C.L. Patient satisfaction and acceptability with telehealth at specialist medical outpatient clinics during the COVID-19 pandemic in Australia. Intern. Med. J. 2021, 51, 1028–1037. [Google Scholar] [CrossRef] [PubMed]
- Scott, R.; Mars, M. Telehealth in the developing world: Current status and future prospects. Smart Homecare Technol. TeleHealth 2015, 3, 25–37. [Google Scholar] [CrossRef] [Green Version]
- Zhang, X.; Zaman, B.U. Adoption mechanism of telemedicine in underdeveloped country. Health Inform. J. 2020, 26, 1088–1103. [Google Scholar] [CrossRef]
- Mittal, S.; Mehar, M. Socio-economic Factors Affecting Adoption of Modern Information and Communication Technology by Farmers in India: Analysis Using Multivariate Probit Model. J. Agric. Educ. Ext. 2016, 22, 199–212. [Google Scholar] [CrossRef]
- Lam, K.; Lu, A.D.; Shi, Y.; Covinsky, K.E. Assessing telemedicine unreadiness among older adults in the United States during the COVID-19 pandemic. JAMA Intern. Med. 2020, 180, 1389–1391. [Google Scholar] [CrossRef] [PubMed]
- Orrange, S.; Patel, A.; Mack, W.J.; Cassetta, J. Patient Satisfaction and Trust in Telemedicine During the COVID-19 Pandemic: Retrospective Observational Study. JMIR Hum. Factors 2021, 8, e28589. [Google Scholar] [CrossRef]
- UN. International Day of Older Persons. Available online: https://www.un.org/en/observances/older-persons-day (accessed on 20 October 2021).
- Raghupathi, V.; Raghupathi, W. The influence of education on health: An empirical assessment of OECD countries for the period 1995–2015. Arch. Public Health 2020, 78, 20. [Google Scholar] [CrossRef] [Green Version]
- Alhajri, N.; Simsekler, M.C.E.; Alfalasi, B.; Alhashmi, M.; AlGhatrif, M.; Balalaa, N.; Al Ali, M.; Almaashari, R.; Al Memari, S.; Al Hosani, F.; et al. Physicians’ Attitudes Toward Telemedicine Consultations During the COVID-19 Pandemic: Cross-sectional Study. JMIR Med. Inf. 2021, 9, e29251. [Google Scholar] [CrossRef]
- Weißenfeld, M.M.; Goetz, K.; Steinhäuser, J. Facilitators and barriers for the implementation of telemedicine from a local government point of view—A cross-sectional survey in Germany. BMC Health Serv. Res. 2021, 21, 919. [Google Scholar] [CrossRef] [PubMed]
- Andrews, E.; Berghofer, K.; Long, J.; Prescott, A.; Caboral-Stevens, M. Satisfaction with the use of telehealth during COVID-19: An integrative review. Int. J. Nurs. Stud. Adv. 2020, 2, 100008. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variables | Frequency (n) | % |
|---|---|---|
| Age group (in years) (mean ± SD) | 42.9 ± 9.1 | |
| Gender Male Female | 396 324 | 55.0 45.0 |
| Marital status Married Single | 468 252 | 65.0 35.0 |
| Education level Less than University/College University/College | 126 594 | 17.5 82.5 |
| Employment Government Self-employed/Private Unemployed | 458 120 142 | 63.6 16.7 19.7 |
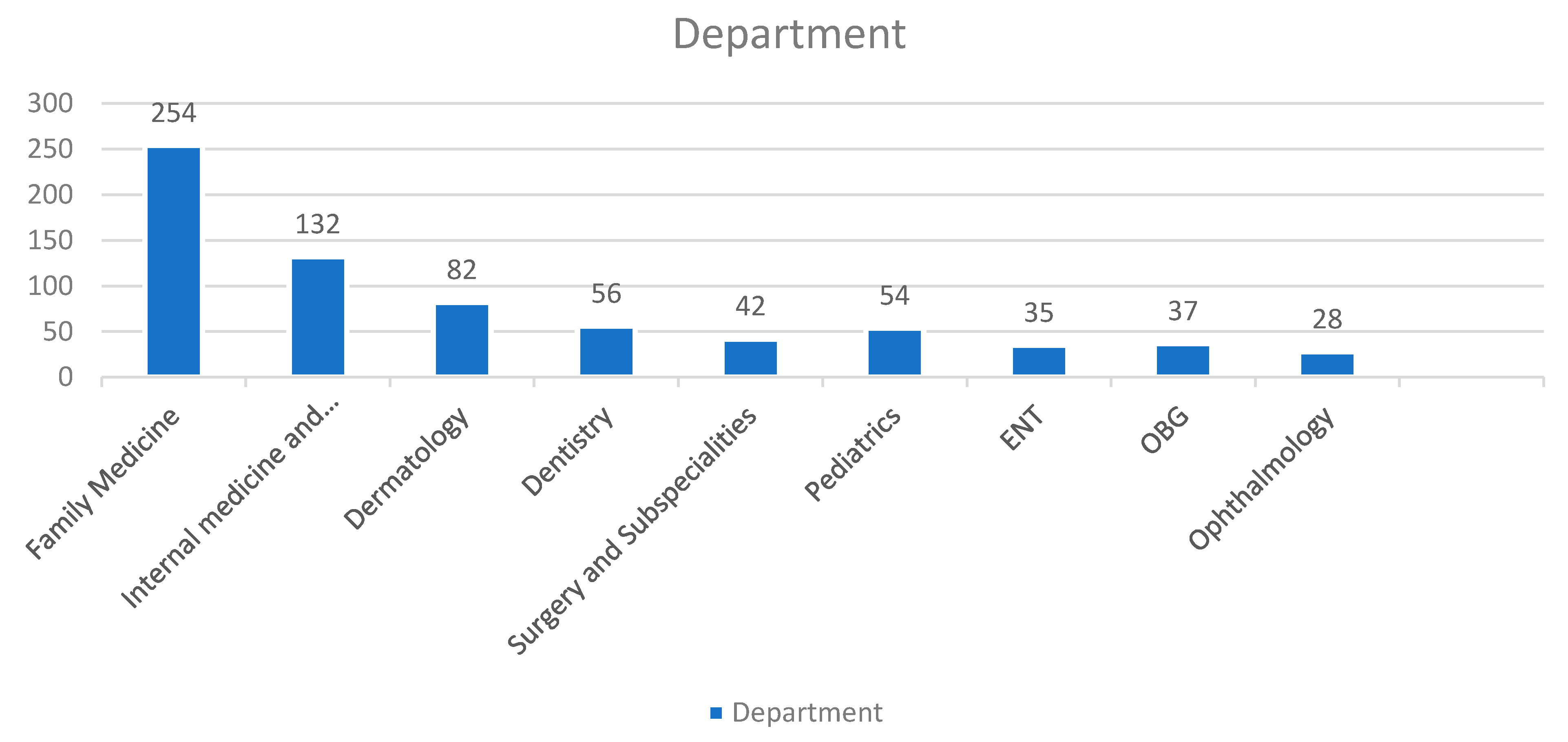
| Telemedicine consultation at PHC General hospital Specialty hospital | 302 340 78 | 41.9 47.2 10.8 |
| Telemedicine consultation experience before the pandemic Yes No | 209 511 | 29.0 71.0 |
| Variables | Mean ± SD | p-Value (Two Tailed) |
|---|---|---|
| Age (in years) * ≤40 years >40 years | 32.93 ± 4.4 30.31 ± 4.7 | <0.01 |
| Gender * Male Female | 31.41 ± 4.9 31.23 ± 3.8 | 0.691 |
| Marital status * Married Single | 32.76 ± 5.4 30.59 ± 6.4 | 0.004 |
| Education * University/College Less than University/College | 31.79 ± 4.1 31.26 ± 5.9 | 0.374 |
| Employment status ** Government Self-employed/Private Unemployed | 31.43 ± 4.3 32.02 ± 3.8 31.75 ± 5.1 | 0.652 |
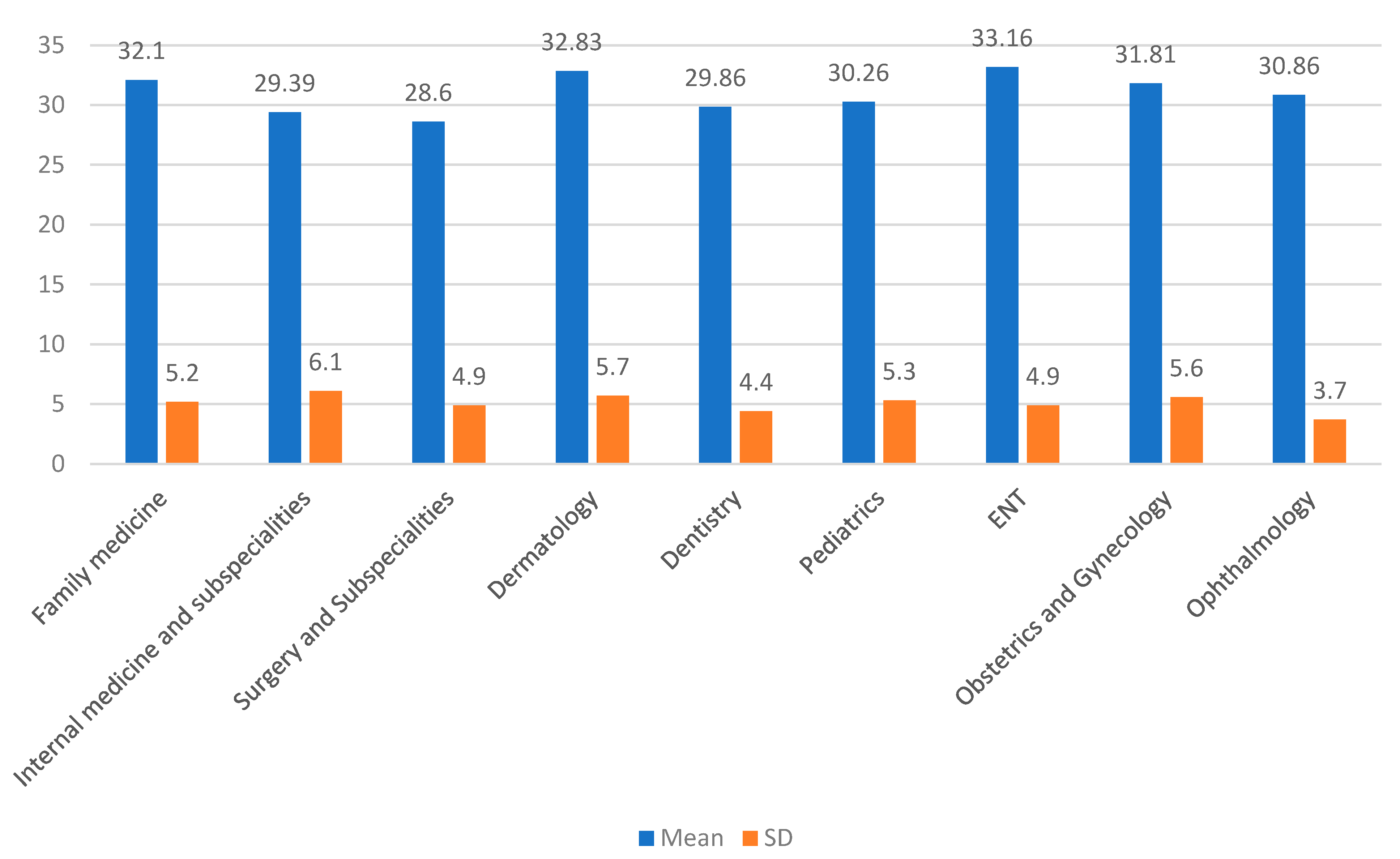
| Telemedicine consultation at ** PHC General hospital Specialty hospital | 32.46 ± 5.7 32.74 ± 4.9 30.18 ± 5.1 | 0.07 |
| Telemedicine consultation experience before the pandemic * Yes No | 31.23 ± 3.4 32.14 ± 3.7 | 0.105 |
| Perceptions | Frequency (n) | % |
|---|---|---|
| Has the COVID-19 pandemic changed your desire to be seen in person by a healthcare provider? Yes No Not sure | 326 186 208 | 45.3 25.8 28.9 |
| Do you think anything was missed or not addressed because you were not seen in person? Yes No Not sure | 284 214 222 | 39.4 29.7 30.8 |
| Willingness to participate in another telemedicine consultation during the COVID-19 pandemic Yes No Not sure | 490 124 106 | 68.1 17.2 14.7 |
| Preference towards telemedicine consultation once the COVID-19 pandemic is over. Yes No Not sure | 536 126 58 | 74.4 17.5 8.1 |
| Perceived advantages towards telemedicine Availability of healthcare provider Convenience No time off from work No travel Time saving Safety Visits not rushed None | 329 571 289 128 452 96 85 53 | 45.7 79.3 40.1 17.8 62.8 13.3 11.8 7.4 |
| Perceived disadvantages towards telemedicine Technological difficulties Less personal interaction Poor communication None | 382 219 248 110 | 53.1 30.4 34.4 15.3 |
| Recommendation for telemedicine care improvement Improvement in scheduling/coordination Improved technology Incorporation of diagnostic recommendation None | 281 320 162 91 | 39.0 44.4 22.5 12.6 |
| Characteristics | Total Sample (n = 720) | Poor and Average Satisfaction | Multivariate Analysis * No vs. Yes | p Value ** | |
|---|---|---|---|---|---|
| No (n = 394) n (%) | Yes (n = 326) n (%) | Adjusted OR (95% CI) | |||
| Age (in years) ≤40 years >40 years | 286 434 | 190 204 | 96 230 | Ref 1.59 (1.04–2.44) | 0.031 |
| Gender Female Male | 324 396 | 174 220 | 150 176 | Ref 0.55 (0.89–0.63) | 0.554 |
| Marital status Single Married | 252 468 | 166 228 | 86 240 | Ref 1.51 (0.96–1.91) | 0.072 |
| Education University/College Less than University/College | 594 126 | 326 68 | 268 58 | Ref 1.68 (1.07–2.15) | 0.025 |
| Employment status Government Self-employed/Private Unemployed | 458 120 142 | 226 72 96 | 232 48 46 | Ref 1.38 (0.81–2.35) 0.98 (0.56–1.74) | 0.237 0.932 |
| Telemedicine consultation at PHC General hospital Specialty hospital | 302 340 78 | 203 167 24 | 99 173 54 | Ref 0.57 (0.31–1.05) 1.73 (1.21–2.47) | 0.70 0.03 |
| Previous telemedicine consultation Yes No | 209 511 | 130 264 | 79 247 | Ref 3.28 (2.32–4.65) | <0.001 |
| Consultation department Family medicine Internal medicine and subspecialities General Surgery and subspecialties Dentistry Other departments | 254 132 42 56 236 | 156 62 26 18 132 | 98 70 16 38 104 | Ref 1.52 (0.95–2.43) 1.08 (0.51–2.28) 1.31 (0.92–2.13) 1.48 (0.98–2.24) | 0.081 0.844 0.142 0.061 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Thirunavukkarasu, A.; Alotaibi, N.H.; Al-Hazmi, A.H.; Alenzi, M.J.; Alshaalan, Z.M.; Alruwaili, M.G.; Alruwaili, T.A.M.; Alanazi, H.; Alosaimi, T.H. Patients’ Perceptions and Satisfaction with the Outpatient Telemedicine Clinics during COVID-19 Era in Saudi Arabia: A Cross-Sectional Study. Healthcare 2021, 9, 1739. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare9121739
Thirunavukkarasu A, Alotaibi NH, Al-Hazmi AH, Alenzi MJ, Alshaalan ZM, Alruwaili MG, Alruwaili TAM, Alanazi H, Alosaimi TH. Patients’ Perceptions and Satisfaction with the Outpatient Telemedicine Clinics during COVID-19 Era in Saudi Arabia: A Cross-Sectional Study. Healthcare. 2021; 9(12):1739. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare9121739
Chicago/Turabian StyleThirunavukkarasu, Ashokkumar, Nasser Hanas Alotaibi, Ahmad Homoud Al-Hazmi, Mohammed Jayed Alenzi, Ziad Mansour Alshaalan, Mohammed Ghazi Alruwaili, Thamer Alshami Marghel Alruwaili, Hassan Alanazi, and Turki Hanas Alosaimi. 2021. "Patients’ Perceptions and Satisfaction with the Outpatient Telemedicine Clinics during COVID-19 Era in Saudi Arabia: A Cross-Sectional Study" Healthcare 9, no. 12: 1739. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare9121739