
Self-Participation Experiences among Well-Adapted Hemodialysis Patients


1
Department of Nursing, Taoyuan Chang Gung Memorial Hospital, National Taipei University of Nursing and Health Sciences, Taoyuan City 33372, Taiwan
2
School of Nursing, National Taipei University of Nursing and Health Sciences, Taipei City 112303, Taiwan
3
Shin Kong Wu Ho-Su Memorial Hospital, Taipei City 111045, Taiwan
4
Department of Hemodialysis, Shin Kong Wu Ho-Su Memorial Hospital, Taipei City 111045, Taiwan
*
Authors to whom correspondence should be addressed.
Healthcare 2021, 9(12), 1742; https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare9121742
Submission received: 9 November 2021
/
Revised: 13 December 2021
/
Accepted: 16 December 2021
/
Published: 17 December 2021
(This article belongs to the Collection Health Care and Services for Elderly Population)
Abstract
:A successful self-participation experience empowers patients to adapt to living with hemodialysis. However, few studies regarding the subjective experiences of such patient participation have been conducted. This study’s purpose was to describe hemodialysis patients’ perspectives on integrating hemodialysis into a new life regarding self-participation experience. A qualitative study using the grounded theory method was applied. Thirty-two well-adaptive hemodialysis Taiwanese patients attended in-depth interviews. “Integrating hemodialysis into a new life journey” was identified as the core category guiding the entire self-participation experience of hemodialysis patients. The three antecedent themes were “Sense of worthlessness”, “Life is still worth living”, and “Friendly and joyful atmosphere of the hemodialysis room”. Once the patients went through the three antecedent themes, they gradually began making efforts to participate more fully in their hemodialysis. Within this participation experience, the hemodialysis patients exhibited these four interactive themes: “Overcoming one’s predicament”, “Integrating self-care skills into my life”, “Resuming previous roles and tasks”, and “Adapting to independent living”. Finally, most adaptive patients master the hemodialysis life. Encouraging patients to discover that their life is worth living and providing a friendly and joyful atmosphere in hemodialysis units are the keys to facilitating patients’ self-participation more fully.
1. Introduction
Each patient is an expert regarding his or her own body, symptoms, and conditions [1]. When patients are able to influence and participate in their own healthcare, they can view a disease from their own perspectives while considering their personal habits, potential, rights, opportunities, preferences, experiences, feelings, and fears in the decision-making process of their treatment [2,3]. Thus, the World Health Organization (WHO) believes that the development of patient empowerment, involvement, and participation is linked to the promotion of patient safety. Patient participation is defined as patient involvement in decision-making in their health care, safety management, and compliance with prescriptions [4]. Patients with end-stage chronic kidney disease (CKD) typically undergo hemodialysis three times per week, with each session requiring 3~4 h of dialysis time. The discomforts associated with hemodialysis include limitations of the patients’ fluid and food intake and physical activity, as well as pain, itching, fatigue, weakness, feelings of inadequacy, and negative perceptions. These may include role restrictions and social isolation, which impose physical, mental, and, sometimes, economic and social burdens on dialysis patients [5,6,7,8,9,10]. Consequently, hemodialysis patients are unable to undergo normal lives. Thus, we uncover how hemodialysis (HD) patients go through the negative experience and return to normal life.
Many recent studies have indicated that CKD requires long-term self-management or individual strategies for coping with stress [5,11,12]. Thus, CKD patients must reinterpret their disease, establish new life perspectives, and attempt to better adapt to the long-term living conditions associated with their disease, allowing them to enhance their self-worth [2,13,14,15]. During the decision-making process, patients encounter the “bridge” in patient participation. This bridge allows the patient to translate his or her knowledge, experiences, and individualized learning into behavior that may improve his or her quality of life, or the patient is able to completely express his or her feelings, physical, and mental states [2]. The participation process contributes to decision-making and shared self-determination or self-care into daily life, enabling the patient to develop a new life [2].
However, previous studies have focused on empowerment [2,15,16,17,18,19] and self-management [15], healthcare professional perspectives of patient participation [12,16,20,21], as well as working-age HD adults experiences of participation [10]. Thus, the present study was designed as a qualitative study that describes the perspective of well-adapted hemodialysis patients regarding their self-participation experience. The findings of this study may help healthcare professionals to understand the self-participation experiences of hemodialysis patients, and apply the findings to help unadjusted HD patients undergoing the HD trajectory become involved in their HD treatment and management.
2. Materials and Methods
2.1. Study Design
A qualitative study was conducted applying the grounded theory method that enables researchers to study a specific phenomenon or process and uncover new stories based on the collection and analysis of real-world data. The participants were recruited from an outpatient hemodialysis clinic with 126 beds at a medical center in Taiwan using purposive sampling. The sampling criteria for participants were as follows: (a) had already adapted to life as a hemodialysis patient and was leading a normal life; (b) was aged 20 years or older (c) had been undergoing hemodialysis three times a week for at least one year, and (d) they identified themselves as undergoing well-adapted HD, although some interviewed HD patients were very long HD survivors who still have a vivid memory of initial self-participation experiences and were willing to share these experiences. The well-adapted patients were referred by attending physicians or the head nurse.
2.2. Ethics Statement and Data Collection
The study protocol was approved by the Institutional Review Board (IRB) of a medical center in northern Taiwan (ethical approval number: 20180304R). In order to ensure informed consent and to protect the participants’ anonymity, confidentiality, and interests, the participants were provided with sufficient time to read the consent form. All participants were chosen to be interviewed once during a scheduled dialysis session in a private room at their dialysis centers, in order to save time and reserve energy, without nurses or family in the private room. Prior to beginning the interview, the purpose of the study was explained again, and the included patients provided signed informed consent. The female first researcher was a nephrology nurse practitioner. SLY interviewed each interviewee using an interview guide to conduct face-to-face interviews (Table 1). All interviews were audio-recorded.
2.3. Interview Content and Analysis
For the purpose of preventing presupposition bias and to ensure consistency of the interview content, open questions jointly developed by the three researchers were used in the interviews, during which the interviewees could provide vivid descriptions of their life experiences regarding HD self-participation. Open-ended interview prompts were also utilized to encourage the interviewees to provide in-depth accounts. Prompts and exploratory questions were utilized, and verbatim records were made until theoretical saturation was reached. The content of each interview was converted into an interview record within 48 h after recording. Comparative methods were used consistently to analyze the transcripts.
Verbatim transcripts of interviews and field notes were analyzed using the constant comparative method for repeatedly comparing the existed categories and content. Four steps were executed during the coding process: (1) open coding: the researcher repeatedly reviewed each interview transcript to obtain insight into the meaningful phrases and sentences by line-by-line; (2) axial coding: the related subcategories were clustered to generate main themes; (3) selective coding, which integrated the axial coders; and (4) determination of the initial diagram: all subcategories were testified to find out the core category, build up the storyline and develop an initial substantive theory about the self-participation experiences, until category saturation was achieved and no new major themes arose. Four criteria were applied to evaluate the trustworthiness of this study: (a) credibility, (b) transferability, (c) dependability, and (d) confirmability [12]. This was achieved by recruiting participants with a broad range of diverse backgrounds, a peer-review coding process, transcribed, audio-taped interview notes, and theoretical and methodological notes, to ensure the objectivity of data collection and classification.
3. Results
This study screened and recruited 32 HD patients, including 15 male patients and 17 female patients, with an average age of 61.72 years (Table 2) and an average HD period of 9.06 years. No participants were on the waiting list for kidney transplantation.
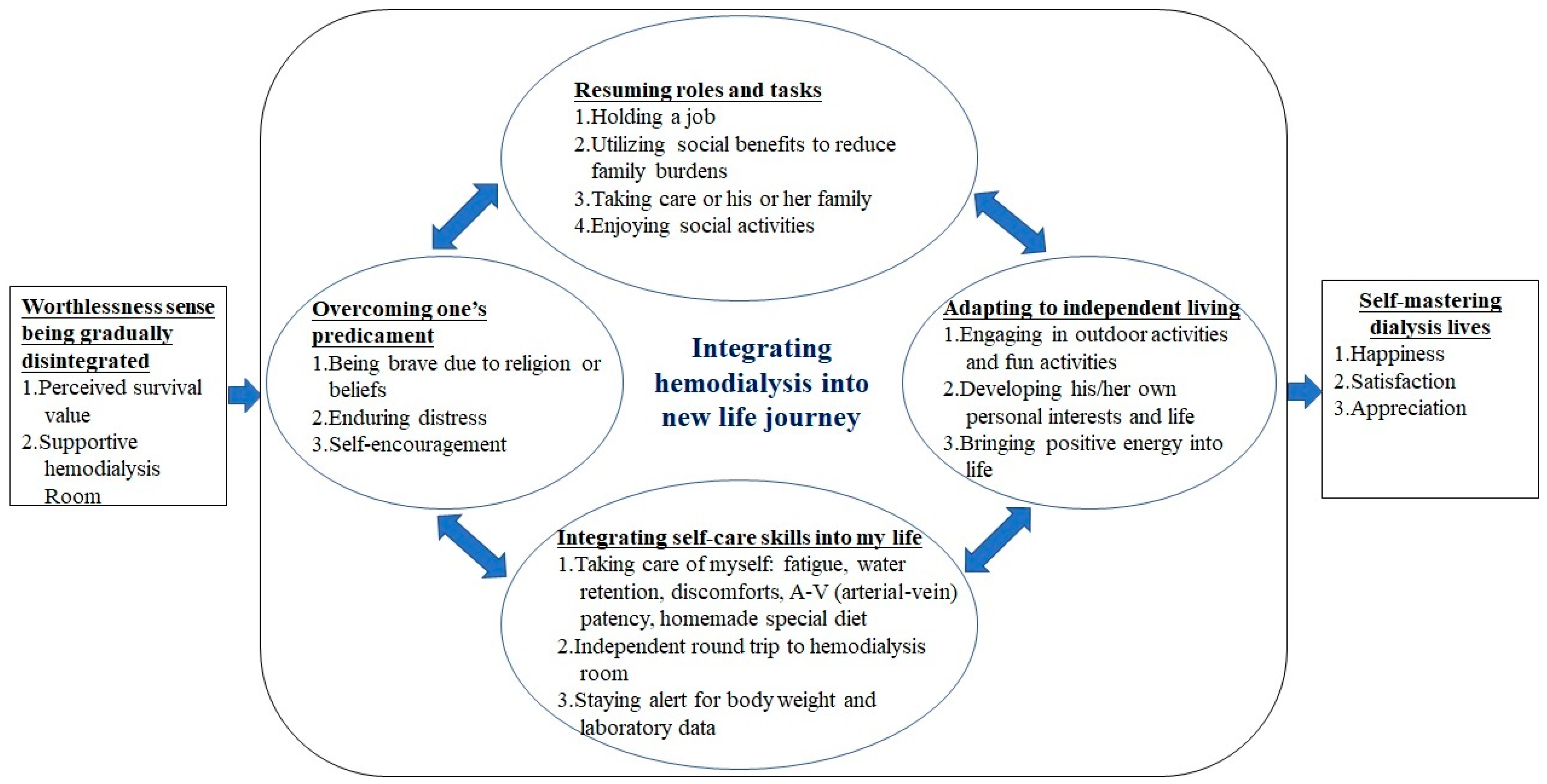
Initially, the HD patients often self-reported feeling that they were “worthless” individuals. When affected by these feelings, the patients experienced fear, sadness, and negative feelings arising from their need to rely on others and the discrimination that they faced. However, these patients discovered that “life is still worth living” and recognize the “friendly and joyful atmosphere of the HD room.” Consequently, these two forces would drive them to participate in their treatment more completely and gradually integrate hemodialysis into their new life journeys. Six themes emerged during this process (Figure 1).
3.1. Antecedent Theme: Sense of Worthlessness Being Gradually Disintegrated
Perceived Survival Value and Supportive Hemodialysis Room
Self-perceived survival value and a “friendly and pleasant atmosphere in the HD room” initiated patients’ self-participation. Upon learning that they required HD, patients experienced negative feelings arising from their need to depend on others and the discrimination that they would face. In some cases, patients may even discontinue the treatment or become pessimistic. People who felt a “Sense of worthlessness” indicated that they experienced numerous negative feelings because HD patients are subjected to several restrictions in their daily lives and must rely on a machine and the hospital for the remainder of their days. In some cases, patients may even be disparaged by their relatives, friends, and neighbors, or experience a sense of worthlessness due to their disability or the fear that they will become a burden to their family and friends and be incapable of living independently.
“The doctor told me that I had to go on hemodialysis, and I refused. I insisted on not going and ran away from the problem. …A man who is told that he needs hemodialysis feels worthless. My wife was always crying…”.(P10)
“When I knew that I had to undergo HD, I was in pain and fearful. My girlfriend kept asking about the situation that we couldn’t get married, work, or raise our children. With tears in her eyes, she told me that it was alright because I wouldn’t die immediately. I am able to live a long life while I’m on HD. For the sake of my marriage and children, I decided to do it…”.(P07)
“I cried from the pain of the needle insertion. I had to restrict my daily food intake, and I had no freedom. I asked them how they could be happy. This was when I learned about the many types of local anesthetics”.(P11)
“Initially, I didn’t know anyone when I started my hemodialysis. I listened to what the others (fellow dialysis patients) were talking about and whether they had the same symptoms as I did. I figured that I should follow what they were doing, and it’ll be effective…”.(P05)
3.2. Interactive Themes
3.2.1. Overcoming One’s Predicament
The HD patients were brave enough to confront the tough situation by relying on their religion or beliefs; they engaged in self-talk to endure the distress caused by HD needle insertions, forced themselves to achieve better results through various methods, and thereby adapted to the discomfort of HD through positive feedback from self-encouragement.
“As a devout Christian, I felt that God was punishing me. However, in my prayers, He told me that He has his reasons, and I should accept this ordeal. Every time I had a needle inserted, I thought about God sending his angels to lift away my pain. I attempted the methods of the others (fellow HD patients). I felt myself improving… because these methods were helpful”.(P04)
3.2.2. Integrating Self-Care Skills into My Life
The patients’ integration of self-care skills into their lives occurred during the self-participation experience. Hemodialysis imposes various life restrictions, including those related to electrolyte balance (diet) and fluid management. After four hours of HD, the arm in which the HD needle was inserted will be mostly immobilized and cannot be turned; hence, only one arm is freely movable. Furthermore, the patients must gradually acquire HD skills. Based on these circumstances, the patients needed to learn the following self-care life skills: water restrictions, fatigue management, traveling to the HD center by oneself, self-preparation of a homemade diet to maintain good energy and nutrition, self-relief of discomforts, maintaining AV-Shunt function patency and staying alert for changes in weight and laboratory measurements.
“I was unable to restrict my water intake…In summer, I would suck and swallow a lot of ice…and I swallowed more than I spit out. Then, someone taught me how to make iced lemon water, which seemed to help cope with my water restrictions. I would place lemon water in a bottle, freeze it and drink after exercising. It was effective, as I would drink the amount of ice that melted…”.(P24)
“They (fellow dialysis patients) taught me that I could drink more. I may not drink four hours prior to hemodialysis, but I could drink more during each session and during meals. I thought to myself that I could eat more if I didn’t increase my weight; I could eat less if my blood potassium was not controlled. I ensured that vegetables were cooked. When I drank water during each session, I wouldn’t exceed my restrictions or have low blood pressure. I didn’t feel weak, as I had enough nutrients. Therefore, I would take a bus by myself to the hemodialysis room and arrange a taxi by myself to go home”.(P01)
“Blood vessel care is very important. I am afraid of the occlusion of the AV shunt at night, and I don’t even dare to sleep. It would result in me being unable to “wash” my kidneys (dialysis). I want to use an L-shaped pillow to prevent occlusion. When I wake up, I will touch the blood vessel. If the flow is not strong, I will strengthen my grasping muscles and let the blood flow improve ”.(P15)
3.2.3. Resuming Roles and Tasks
When an HD patient has integrated HD into his or her daily life, he or she will be able to gradually assume the roles and tasks of a normal person, including holding a job, utilizing social benefits to reduce family burdens, caring for his or her family, and enjoying social activities. As a result, the HD patient will experience a reduction in stress related to post-hemodialysis discomfort and achieve a better physical and mental state.
“I love beauty, but my face disappears after hemodialysis. Today, I will wear makeup. I will be beautiful when taking hemodialysis. As long as I look happy, others will feel the same. I look more beautiful”.(P06)
“Now, I am able to perform carpentry and sell my own creations. My wife no longer has to endure many hardships... I feel more like a man now that I have more self-worth and a sense of self-accomplishment”.(P08)
3.2.4. Adapting to Independent Living
The patients were required to make independent arrangements to engage in outdoor activities and fun activities, develop their own personal interests and life, bring positive energy into their lives, and help their families or others understand that they were living well.
“I would always check with the hemodialysis centre in Tainan located nearest to my hometown before treatment. Traveling locally isn’t a problem for me, and I have been to Japan. I would undergo my hemodialysis sessions before departing”.(P09)
“The blood vessel on my arm is unsightly. Since I enjoy making handicrafts, I would buy fabrics and stitch to make armbands that are beautiful and special: other fellow HD patients felt the same way, so I would give armbands to them. I felt happy”.(P20)
3.3. Consequence Theme: Self-Mastering Dialysis Lives
Regarding happiness, satisfaction, and appreciation, when the HD patients engaged in HD self-participation and adapted to HD through the four interactive themes of behaviors that mutually influenced each other, they began to attain joy and satisfaction in their lives after HD because they now had control, and learned to better appreciate themselves.
“I am always able to overcome any difficulty all along..., I am grateful… I just want my family to be healthy and happy, as I am able to take care of myself. I feel happy as I take daily HD … several conversations and the government subsidies are also viewed as remunerations. You can see that we’re pretty well off, too”.(P22)
“I was left alone after my parents passed on. I used to be scared of the two needle insertions during each hemodialysis session because I was timid and susceptible to pain. However, now I don’t require anesthesia. I told myself to handle one thing at a time. I now have higher self-esteem since I grew from being fearful and timid to an independent person. I feel blessed and free all the time”.(P19)
4. Discussion
To the best of our knowledge, this was the first study to explore the Taiwanese hemodialysis self-participation experience using the grounded theory method. This study shows that the antecedent theme of “Worthlessness sense being gradually disintegrated” contains “Perceived survival value” and “Supportive hemodialysis room” and four interactive themes: “Overcoming one’s predicament”, “Integrating self-care skills into my life”, “Resuming roles and tasks”, and “Adapting to independent living”; and finally, consequence theme of “Self-mastering dialysis lives”.
4.1. Antecedent Theme: Worthlessness Sense Being Gradually Disintegrated
Patients may develop a sense of worthlessness or depression-induced thoughts. Depression is a commonly encountered psychological problem among HD patients [22,23,24] and may even affect the mortality rate of the HD patient population [25,26]. Supporting the depressed patients in discovering the value of life and providing a friendly environment in the HD room will initiate patients’ self-participation in their treatment. In the present study, “friendships with others in the dialysis room” was the foremost precursor factor for self-participation. Patients were encouraged to make friends with other patients in the same HD room, and the supporting group helped them to overcome their fear, discomfort, and boredom during hemodialysis. Nurses should not only work on their HD skills but also on creating a friendly, relaxed, and light-hearted atmosphere, in which patients are praised for braving the pain of needle insertion and encouraged to overcome their feelings of exhaustion. In some cases, arrangements were even made to seat HD patients with a successful self-participation track record beside patients who were undergoing their first HD session or patients who had not adapted well to the process. By joining a group, patients were no longer fighting the disease on their own, but instead, worked alongside individuals with the same condition and with whom they shared a common treatment. This approach provides patients with space where they can talk about the suffering caused by the disease and find joy and a sense of belonging in their struggles.
Previous studies showed that adjustment to ESRD was a dynamic and constant process [27]; HD patients experienced three periods of adjustment (beginning 1–3 weeks from the first dialysis, or honeymoon period, 3–12 months of frustration period, and the long period of adjustment) [28] This process is contrary to our research. The possible reason is that our participants are all well-adapted HD patients, which confirms the advantages and importance of HD self-participation. A 2008 study proposed that the emotion-regulation strategies employed by HD patients play a significant role in their attitudes towards the disease [29,30]. The results of that study were consistent with the findings from the present study, indicating that the atmosphere of an HD room is a factor that influences the emotions of HD patients. Due to the side effects of post-hemodialysis discomfort, the various restrictions in their lives, and the frustrations that they face, HD patients were reported to need to draw strength from their religion or beliefs and strengthen their problem-solving skills and ability to adapt: the findings from those studies are consistent with those from the present study [29,30,31]. These patients utilize strategies characterized by self-encouragement and self-talk to force themselves to endure the pain of needle insertions; they also attempt several methods until they are able to integrate post-hemodialysis discomfort into their lives. Furthermore, they also incorporate self-rewards into their downshifted or slow-paced lives.
The introduction of religious or spiritual interventions for chronic HD patients helps trigger positive emotions during stress and influences overall health (measured using quality of life indices), including patients’ commitment and adherence to hemodialysis [32,33,34]. A systematic review of 33 studies examining spiritual aspects of patients with end-stage renal disease (ESRD) demonstrated a positive correlation between spirituality and the well-being of patients with ESRD. Six of those quantitative studies revealed a relationship between spirituality and the quality of life of HD patients, and generated findings similar to the data from the present study, namely, the role of religion and beliefs in the ability to overcome difficulties. Some scholars have also proposed that coping strategies characterized by problem-centered participation are linked to improvements in the survival, physical function, and mental health of hemodialysis patients [35].
4.2. Interactive Themes: Overcoming One’s Predicament, Integrating Self-Care Skills into My Life, Resuming Roles and Tasks, and Adapting to Independent Living
Patients undergoing HD attempt various methods and learn a number of techniques to help them adapt to hemodialysis-related problems in areas such as transportation (e.g., to the HD center), diet, fluid intake, exhaustion, blood pressure fluctuations, and cramps. These methods help patients to reduce the obstacles created by HD in their daily lives and the burden on their families, as well as to build their confidence in playing their roles and taking on tasks, obtain positive feedback relating to their efforts, and maintain their social lives. In recent years, many studies have shown that the promotion of problem-centered participation was recommended to lengthen the lifespan and improve the quality of life of HD patients [11,35].
In the present study, the theme exhibited by the self-participating HD patients emphasized the attainment of results concerning self-awareness, self-efficacy, and self-control. The patients actively participated in individualized learning to acquire the HD skills they needed to utilize social resources, regain control over their lives, and understand how they would be able to achieve and appreciate the outcomes related to self-participation in HD. Throughout this process, the HD patients continued to integrate HD into their new life journeys.
The present study found that participants expressed that as they gradually resume their roles and lives, they would regain self-confidence and adapt to an independent life. After hemodialysis, patients needed to rebuild their lifestyles to accommodate the hemodialysis schedule. In many cases, patients would travel back and forth independently from home to the HD center and needed to learn how to deal with their discomforts when they were alone before and after dialysis. Their daily activities were different from those of their peers and friends. Therefore, teaching patients to be alone and help themselves during activities, shopping or entertainment is an important step in self-participation. Because of self-participation in HD life, they would perceive the usefulness of self-care, self-efficacy, and health status in coping, compliance with fluid and food restrictions, sleep disorders, symptom distress, as well as adjustment of anxiety, emotional distress, and dialysis stress [36,37]. Participants expressed that as they gradually resumed their roles and lives, they regained self-confidence and adapted to an independent life. After HD, patients needed to rebuild their lifestyle to accommodate the HD schedule. In addition, participants expressed that through self-participation, the dialysis life has been integrated into their life, and considering the complications of kidney transplantation, such as infections and rejections and other life-threatening side effects, the process of choosing treatment methods can be used as a reference for future research.
4.3. Consequence Theme: Self-Mastering Dialysis Lives
While HD patients are actively involved in hemodialysis lifestyles, they have the problem-solving ability of symptom management. They are able to find happiness and interests, fulfil their expectations toward life, express a positive perspective on hemodialysis (e.g., treat the dialysis room as work; the dialysis room is the only place you can sleep and relax during work in the world), appreciate when the disease results in benefits (e.g., health is more important than making money or school grade), and experience wellness and good family relationships.
In this study, the four interactive themes exhibited by the self-participating hemodialysis patients emphasized the attainment of results in relation to self-awareness, self-efficacy, and self-control. The patients actively participated in individualized learning to acquire the hemodialysis skills they needed to utilize social resources, regain control over their lives, and understand how they would be able to achieve and appreciate the final outcome related to self-participation in hemodialysis. Throughout this process, the core category was “integrating hemodialysis into my life journey”.
The present study reached data saturation with a sample of 32 HD patients. Since the sample consisted of only well-adapted HD patients from northern Taiwan who had engaged in self-participation, the results obtained for the experiences of these patients are limited regarding the understanding the experiences of self-participation of unadjusted HD patients, which is a limitation of this study. Therefore, future studies may explore the experience of self-participation among unadjusted HD patients. The results from this qualitative study will serve as a reference for the construction of an HD self-participation scale. We believe that incorporating the findings of the present study will help HD patients acquire self-participation HD skills, such that they are able to build new healthy lives for themselves.
5. Conclusions
More complete self-participation in hemodialysis positively influences HD patients, allowing them to acquire skills that help incorporate the restrictions of hemodialysis into their lives. In terms of psychological outlook, the HD patients’ willingness to continue living was main finding of our study. Therefore, this requires that nurses recognize patients with lower-level emotional and psychological needs. Secondly, they must provide their professional knowledge and assistance in order to encourage self-participation and motivation to overcome the various life limitations of hemodialysis. Nurses should encourage patients to express their negative emotions or depressive feelings, which appears to reduce such feelings. Nurses should focus on strengthening patients’ will to live, the joy of life, and the discovery of fun in life to increase their self-confidence and perceptions of self-worth. These measures may allow HD patients to gradually construct their roles and tasks, and to transition to the self-mastery of dialysis in their daily lives.
Author Contributions
Study design, L.-Y.S. and L.-I.T.; data collection, L.-Y.S.; data analysis, L.-Y.S. and L.-I.T.; manuscript preparation: L.-Y.S., L.-I.T. and S.-C.C. and final manuscript approval, L.-Y.S., L.-I.T., S.-C.C. and M.-L.H. All authors have read and agreed to the published version of the manuscript.
Funding
This study received funding from Shin Kong Wu Ho-Su Memorial Hospital (DN-PC-107-001) and Chang Gung Memorial Research Grand of the Chang Gung Medical Foundation (CMRPG5J0121).
Institutional Review Board Statement
The study was approved by the institutional review board (IRB) of a medical centre in northern Taiwan (ethical approval number: 20180304R). The study was initiation once the participants provided them consent and signed the consent form.
Informed Consent Statement
Written informed consent to use this data in publications has been obtained from all the participants.
Data Availability Statement
The datasets used and analyzed during the current study are available from the first author and the corresponding authors on reasonable request.
Acknowledgments
The authors would like to thank the participants for sharing their valuable experiences sincerely.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviation
HD—hemodialysis.
References
- Borkman, T. Experiential Knowledge: A New Concept for the Analysis of Self-Help Groups. Soc. Serv. Rev. 1976, 50, 445–456. [Google Scholar] [CrossRef] [Green Version]
- Castro, E.M.; Van Regenmortel, T.; Vanhaecht, K.; Sermeus, W.; Van Hecke, A. Patient empowerment, patient participation and patient-centeredness in hospital care: A concept analysis based on a literature review. Patient Educ. Couns. 2016, 99, 1923–1939. [Google Scholar] [CrossRef] [PubMed]
- Wiig, S.; Team, Q.; Storm, M.; Aase, K.; Gjestsen, M.T.; Solheim, M.; Harthug, S.; Robert, G.; Fulop, N. Investigating the use of patient involvement and patient experience in quality improvement in Norway: Rhetoric or reality? BMC Health Serv. Res. 2013, 13, 206–213. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Exploring Patient Participation in Reducing Health-Care-Related Safety Risks. Available online: https://apps.who.int/iris/bitstream/handle/10665/326442/9789289002943-eng.pdf. (accessed on 10 October 2021).
- Alikari, V.; Tsironi, M.; Matziou, V.; Babatsikou, F.; Psillakis, K.; Fradelos, E.; Zyga, S. Adherence to Thera-peutic Regimen in Adults Patients Undergoing Hemodialysis: The Role of Demographic and Clinical Characteristics. Int. Arch. Nurs. Health Care 2018, 4, 96. [Google Scholar]
- El-Majzoub, S.; Mucsi, I.; Li, M.; Moussaoui, G.; Lipman, M.L.; Looper, K.J.; Novak, M.; Rej, S. Psychosocial Distress and Health Service Utilization in Patients Undergoing Hemodialysis: A Prospective Study. J. Psychosom. Res. 2019, 60, 385–392. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.-C.; Han, C.-Y.; Pan, I.-J. A Qualitative Approach of Psychosocial Adaptation Process in Patients Undergoing Long-term Hemodialysis. Asian Nurs. Res. 2015, 9, 35–41. [Google Scholar] [CrossRef]
- Reid, C.; Seymour, J.; Jones, C. A Thematic Synthesis of the Experiences of Adults Living with Hemodialysis. Clin. J. Am. Soc. Nephrol. 2016, 11, 1206–1218. [Google Scholar] [CrossRef] [Green Version]
- Chiaranai, C. The lived experience of patients receiving hemodialysis treatment for end-stage renal disease: A qualitative study. J. Nurs. Res. 2016, 24, 101–108. [Google Scholar] [CrossRef] [PubMed]
- Andersen-Hollekim, T.; Solbjør, M.; Kvangarsnes, M.; Hole, T.; Landstad, B.J. Narratives of patient participation in haemo-dialysis. J. Clin. Nurs. 2020, 29, 2293–2305. [Google Scholar] [CrossRef]
- Hwang, H.C.; Kim, H.R.; Han, D.H.; Hong, J.S.; Jeong, S.-H.; Shin, J.-H.; Kim, S.-H.; Hwang, J.H.; Kim, S.M. Influence of Major Coping Strategies on Treatment Non-adherence and Severity of Comorbid Conditions in Hemodialysis Patients. J. Korean Med. Sci. 2018, 33, e148. [Google Scholar] [CrossRef]
- Aasen, E.M.; Kvangarsnes, M.; Heggen, K. Nurses’ perceptions of patient participation in hemodialysis treatment. Nurs. Ethic 2012, 19, 419–430. [Google Scholar] [CrossRef]
- Barr, P.J.; Scholl, I.; Bravo, P.; Faber, M.J.; Elwyn, G.; McAllister, M. Assessment of patient empowerment—a systematic review of measures. PLoS ONE 2015, 10, e0126553. [Google Scholar]
- Pulvirenti, M.; McMillan, J.; Lawn, S. Empowerment, patient centred care and self-management. Health Expect. 2012, 17, 303–310. [Google Scholar] [CrossRef]
- Kim, E.S. Development and effect of a rational-emotive-behaviour-therapy-based self-management programme for early renal dialysis patients. J. Clin. Nurs. 2018, 27, 4179–4191. [Google Scholar] [CrossRef] [PubMed]
- Aasen, E.M. A comparison of the discursive practices of perception of patient participation in haemodialysis units. Nurs. Ethic 2014, 22, 341–351. [Google Scholar] [CrossRef]
- Fried, T.R. Shared decision making—Finding the sweet spot. N. Engl. J. Med. 2016, 374, 104–106. [Google Scholar] [CrossRef] [PubMed]
- Lin, M.-Y.; Liu, M.F.; Hsu, L.-F.; Tsai, P.-S. Effects of self-management on chronic kidney disease: A meta-analysis. Int. J. Nurs. Stud. 2017, 74, 128–137. [Google Scholar] [CrossRef]
- Spatz, E.S.; Krumholz, H.M.; Moulton, B.W. Prime Time for Shared Decision Making. JAMA 2017, 317, 1309–1310. [Google Scholar] [CrossRef] [PubMed]
- Andersen-Hollekim, T.; Landstad, B.J.; Solbjør, M.; Kvangarsnes, M.; Hole, T. Nephrologists’ experiences with patient participation when long-term dialysis is required. BMC Nephrol. 2021, 22, 58. [Google Scholar] [CrossRef] [PubMed]
- Årestedt, L.; Martinsson, C.; Hjelm, C.; Uhlin, F.; Eldh, A.C. Patient participation in dialysis care—A qualitative study of patients’ and health professionals’ perspectives. Health Expect. 2019, 22, 1285–1293. [Google Scholar] [CrossRef]
- Chen, S.F.; Wang, I.J.; Lang, H.C. Risk of major depression in patients with chronic renal failure on different treatment modalities: A matched-cohort and population-based study in Taiwan. Hemodial. Int. 2016, 20, 98–105. [Google Scholar] [CrossRef] [PubMed]
- Kopple, J.D.; Shapiro, B.B.; Feroze, U.; Kim, J.C.; Zhang, M.; Li, Y.; Martin, D.J. Hemodialysis treatment engenders anxiety and emotional distress. Clin. Nephrol. 2017, 88, 205–217. [Google Scholar] [CrossRef]
- Li, Y.-N.; Shapiro, B.; Kim, J.C.; Zhang, M.; Porszasz, J.; Bross, R.; Feroze, U.; Upreti, R.; Martin, D.; Kalantar-Zadeh, K. As-sociation between quality of life and anxiety, depression, physical activity and physical performance in maintenance he-modialysis patients. Chronic Dis. Transl. Med. 2016, 2, 110–119. [Google Scholar] [PubMed] [Green Version]
- Shafiee, M.A.; Chamanian, P.; Shaker, P.; Shahideh, Y.; Broumand, B. The Impact of Hemodialysis Frequency and Duration on Blood Pressure Management and Quality of Life in End-Stage Renal Disease Patients. Healthcare 2017, 5, 52. [Google Scholar] [CrossRef] [Green Version]
- Lopes, A.A.; Lantz, B.; Morgenstern, H.; Wang, M.; Bieber, B.; Gillespie, B.W.; Li, Y.; Painter, P.; Jacobson, S.H.; Rayner, H.C.; et al. Associations of Self-Reported Physical Activity Types and Levels with Quality of Life, Depression Symptoms, and Mortality in Hemodialysis Patients: The DOPPS. Clin. J. Am. Soc. Nephrol. 2014, 9, 1702–1712. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taylor, F.; Taylor, C.; Baharani, J.; Nicholas, J.; Combes, G. Integrating emotional and psychological support into the end-stage renal disease pathway: A protocol for mixed methods research to identify patients’ lower-level support needs and how these can most effectively be addressed. BMC Nephrol. 2016, 17, 111. [Google Scholar] [CrossRef] [Green Version]
- Gerogianni, S.K.; Babatsikou, F.P. Psychological aspects in chronic renal failure. Health Sci. J. 2014, 8, 205. [Google Scholar]
- Gillanders, S.; Wild, M.; Deighan, C.; Gillanders, D. Emotion Regulation, Affect, Psychosocial Functioning, and Well-being in Hemodialysis Patients. Am. J. Kidney Dis. 2008, 51, 651–662. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gurkan, A.; Pakyuz, S.; Demir, T. Stress Coping Strategies in Hemodialysis and Kidney Transplant Patients. Transplant. Proc. 2015, 47, 1392–1397. [Google Scholar] [CrossRef]
- Mok, E.; Tam, B.; Rm, E.M.B.M.; Bsc, B.T. Stressors and coping methods among chronic haemodialysis patients in Hong Kong. J. Clin. Nurs. 2001, 10, 503–511. [Google Scholar] [CrossRef]
- Al-Ghabeesh, S.H.; Alshraifeen, A.A.; Saifan, A.R.; Bashayreh, I.H.; Alnuaimi, K.M.; Masalha, H.A. Spirituality in the Lives of Patients with End-Stage Renal Disease: A Systematic Review. J. Relig. Health 2018, 57, 2461–2477. [Google Scholar] [CrossRef]
- Al Zaben, F.; Khalifa, D.A.; Sehlo, M.G.; Al Shohaib, S.; Binzaqr, S.A.; Badreg, A.M.; Alsaadi, R.A.; Koenig, H.G. Reli-gious involvement and health in dialysis patients in Saudi Arabia. J. Relig. Health 2015, 54, 713–730. [Google Scholar] [CrossRef]
- Ramos, K.; Erkanli, A.; Koenig, H.G. Effects of religious versus conventional cognitive–behavioral therapy (CBT) on sui-cidal thoughts in major depression and chronic medical illness. Psychol. Relig. Spiritual. 2018, 10, 79. [Google Scholar] [CrossRef]
- Niihata, K.; Fukuma, S.; Akizawa, T.; Fukuhara, S. Association of coping strategies with mortality and health-related qual-ity of life in hemodialysis patients: The Japan Dialysis Outcomes and Practice Patterns Study. PLoS ONE 2017, 12, e0180498. [Google Scholar] [CrossRef] [Green Version]
- Lev, E.L.; Owen, S.V. A prospective study of adjustment to hemodialysis. ANNA J. 1998, 25, 495. [Google Scholar] [PubMed]
- Martinez, B.B.; Custodio, R.P. Relationship between mental health and spiritual wellbeing among hemodialysis patients: A correlation study. Sao Paulo Med. J. 2014, 132, 23–27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
Figure 1.
The conceptual framework of integrating hemodialysis into my new life journey.


{kind=link}
Table 1.
Interview guideline.
| Interview Questions |
|---|
| 1. What was your impression of your first hemodialysis session? What did you do then? What has changed since then? 2. What did you learn during the hemodialysis experience that helped you to adapt to it? 3. What kind of help did you receive during this process? 4. Can you talk about your self-care preparations for today’s hemodialysis session and post-dialysis period? 5. What type of assistance do you desire most during this process? 6. Based on your experience, what helped you the most to familiarize yourself with hemodialysis treatments? 7. Over what aspects do you feel you have control? What aspects do you not have control of? Why do you feel that way? 8. As someone who has experienced this process, how would you advise a new hemodialysis patient regarding the preparations for commencing self-participation in haemodialysis care? |
Table 2.
Characteristics of the participants.
| Gender | Age (Years) | Education Level | Occupation | Marital Status | HD Duration in Years | Perceived Health Status |
|---|---|---|---|---|---|---|
| F | 58 | High school | Housewife | Married | 20 | Fair |
| F | 55 | University | None | Widowed | 20 | Fair |
| F | 55 | University | Housewife | Married | 20 | Fine |
| M | 57 | University | None | Married | 10 | Ordinary |
| M | 45 | High school | Service industry | Married | 19 | Ordinary |
| F | 58 | High school | Housewife | Married | 25 | Ordinary |
| M | 72 | Elementary school | Service industry | Married | 2.5 | Ordinary |
| M | 78 | Secondary school | None | Married | 1 | Ordinary |
| F | 63 | Elementary school | None | Married | 10 | Ordinary |
| F | 64 | High school | Housewife | Married | 6 | Fair |
| F | 84 | None | None | Widowed | 5 | Fair |
| M | 48 | College | Part time | Divorce | 3 | Ordinary |
| F | 85 | Secondary school | None | Married | 10 | Ordinary |
| F | 66 | Secondary school | Housewife | Married | 13 | Ordinary |
| F | 33 | University | Worker | Single | 18 | Ordinary |
| M | 42 | University | None | Single | 3 | Ordinary |
| M | 66 | Elementary school | Housewife | Married | 6 | Ordinary |
| M | 62 | College | None | Married | 12 | Ordinary |
| F | 58 | High school | None | Single | 3 | Ordinary |
| F | 60 | Secondary school | Retired | Single | 8 | Ordinary |
| M | 64 | University | Retired | Married | 1.5 | Ordinary |
| M | 53 | University | Chief | Married | 3.5 | Fair |
| F | 67 | Secondary school | Retired | Married | 10 | Ordinary |
| M | 57 | High school | None | Divorce | 8 | Ordinary |
| M | 63 | University | Retired | Married | 4 | Fine |
| F | 47 | University | None | Widowed | 3 | Ordinary |
| M | 81 | Elementary school | None | Widowed | 3 | Ordinary |
| F | 54 | Elementary school | None | Married | 8 | Ordinary |
| M | 65 | High school | Retired | Married | 1 | Ordinary |
| F | 76 | Secondary school | None | Married | 3.5 | Ordinary |
| F | 72 | Secondary school | Housewife | Married | 20 | Ordinary |
| M | 67 | High school | Driver | Married | 10 | Ordinary |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Szu, L.-Y.; Tsao, L.-I.; Chen, S.-C.; Ho, M.-L. Self-Participation Experiences among Well-Adapted Hemodialysis Patients. Healthcare 2021, 9, 1742. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare9121742
AMA Style
Szu L-Y, Tsao L-I, Chen S-C, Ho M-L. Self-Participation Experiences among Well-Adapted Hemodialysis Patients. Healthcare. 2021; 9(12):1742. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare9121742
Chicago/Turabian StyleSzu, Li-Yun, Lee-Ing Tsao, Shu-Chuan Chen, and May-Lien Ho. 2021. "Self-Participation Experiences among Well-Adapted Hemodialysis Patients" Healthcare 9, no. 12: 1742. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare9121742
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.