
Factors Influencing Self-Reported Medication Use in the Survey of Health Aging and Retirement in Europe (SHARE) Dataset


Department of Geriatrics, Halle University Hospital, 06120 Halle, Germany
*
Author to whom correspondence should be addressed.
Healthcare 2021, 9(12), 1752; https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare9121752
Submission received: 25 November 2021
/
Revised: 14 December 2021
/
Accepted: 16 December 2021
/
Published: 18 December 2021
Abstract
:The validity of self-reported medication use in epidemiological studies is an important issue in healthcare research. Here we investigated factors influencing self-reported medication use for multiple diagnoses in the seventh wave of the Survey of Health Aging and Retirement in Europe (SHARE) dataset in n = 77,261 participants (ages: mean = 68.47, standard deviation = 10.03 years). The influence of mental, physical, and sociodemographic parameters on medication self-report was analyzed with logistic regressions and mediation models. Depression, memory function, and polypharmacy influenced the self-report of medication use in distinct disorders to varying degrees. In addition, sociodemographic factors, knowledge about diagnosis, the presence of several chronic illnesses, and restrictions of daily instrumental activities explained the largest proportion of variance. In the mediation model, polypharmacy had an indirect effect via depression and memory on self-reported medication use. Factors influencing medication self-report vary between different diagnoses, highlighting the complexity of medication knowledge. Therefore, it is essential to assess the individual parameters and their effect on medication behavior. Relying solely on medication self-reports is insufficient, as there is no way to gage their reliability. Thus, self-reported medication intake should be used with caution to indicate the actual medication knowledge and use.
1. Introduction
The Survey of Health Aging and Retirement in Europe (SHARE) is a cross-national panel study that includes data on health, social and economic status, and social and family networks of the representative samples of community-based populations from many European countries [1]. So far, several studies have explored the aspects of polypharmacy or the association between distinct medication records and clinical or social factors, e.g., sleep medication use with a sleep disorder or pain medication use with musculoskeletal pain [2,3,4]. However, the primary factors driving the knowledge of medication and behavior remain unidentified [5]. In SHARE, medication use and medical diagnoses are recorded via self-reports for predefined selection of drug classes or disorders, e.g., drugs for hypertension [6,7]. However, this approach has some limitations that must be acknowledged when using self-reported data to proxy for actual medication knowledge or usage. Studies based on self-reported medication use highly depend on the accuracy of those self-reports to draw accurate and reliable conclusions from the available data [8]. However, self-reported medication behavior can be measured using a large bandwidth of different methods [8,9,10], and no consensus has yet been reached regarding its reliability and best practices. For instance, some studies found self-report of medication to be reliable and comparable to objective measures such as pill count, whereas other studies raise the issue that self-report is subjected to recall errors and bias [9,11,12,13]. Errors in self-reporting of medication are linked to general knowledge about medication, attitudes toward health and treatment, and adherence to medication [14]. Particularly, knowledge about the prescribed and self-reported medication is influenced by cognitive function, mood disorders, and the number of drugs taken [12,13,14,15,16]. As an alternative, the accuracy of self-reported medication use can be verified by comparing it with other measures, e.g., prescriptions, healthcare insurance claims, or general practice medical records [10,17,18,19].
However, although available, these objective reports are not frequently used in clinical research and furthermore do not necessarily capture actual medication intake either [19]. Therefore, it is crucial to understand the parameters that influence self-reports of medication [12,13,20]. Several influential factors have previously been proposed, including cognitive deficits (poor recall) or intended nondisclosure, age, polypharmacy, poor health, and social desirability bias or stigmatization [12,13,21,22,23,24,25,26]. However, the influence of these factors varies between studies and diagnoses, and no consensus has been reached regarding their effects [5,14]. Given the high impact of cognitive deficits, mood disorders, physical functioning, and polypharmacy on medication knowledge and behavior [14], we aimed to study the effect of these factors on self-reporting of medication for several diagnoses provided in the SHARE dataset [6].
2. Materials and Methods
2.1. Study Sample
SHARE is a biennial longitudinal survey of the aging process in individuals in several European Union countries and Israel. The survey collects a multitude of information regarding health, socioeconomic status, and social and family networks. Details about the sampling procedure have been published elsewhere [1]. So far, SHARE has conducted eight panel waves. Here, we analyzed data from the seventh wave (release 7-1-1), which were collected between March and October 2017. SHARE targets all persons above 50 years of age who speak the country’s primary language, who are physically and mentally able to participate, and who are not institutionalized/in hospital or out of the country during the sampling time. Further details about the sampling procedures and criteria can be found in the respective documentation files [1,6,7]. An overview of the study cohort included in the present analyses is provided in Table 1.
2.2. Extracted Variables
Data on medication use were collected by asking participants, “Do you currently take drugs at least once a week for (1) high blood cholesterol, (2) high blood pressure, (3) coronary diseases, (4) other heart diseases, (6) diabetes, (7) joint pain, (8) other pain, (9) sleep problems, (10) anxiety or depression, (11) osteoporosis, (12) stomach burns, (13) chronic bronchitis, (14) suppressing inflammation (only glucocorticoids or steroids), (15) none, (16) other?” Participants had the option to choose “refuse,” “don’t know,” “select,” or “not select.”
In addition, the following variables were extracted from the dataset:
The presence of distinct disorders “ever diagnosed/currently having”: (1) heart attack, (2) high blood pressure or hypertension, (3) high blood cholesterol, (4) stroke, (5) diabetes or high blood sugar, (6) chronic lung disease, (7) cancer, (8) stomach or duodenal ulcer, peptic ulcer, (9) Parkinson’s disease, (10) cataracts, (11) hip fracture or femoral fracture, (12) other fractures, (13) Alzheimer’s disease, dementia, senility, (14) other affective/emotional disorders, (15) rheumatoid arthritis, (16) osteoarthritis/other rheumatism, (17) chronic kidney disease, (18) none, (19) other. Participants had the option to choose “refuse,” “don’t know,” “select,” or “not select.” The variable “Number of chronic diseases” was based on the number of chronic diseases reported by each individual.
Regarding sociodemographic factors, age was calculated according to “Year of birth” subtracted from 2017, when wave 7 was conducted. Gender had “male” or “female” as possible answers.
In addition to sociodemographic factors, based on the previously cited literature, cognition, restrictions in performance of daily activities, and mood were included as further covariates to understand how self-report of medication can be influenced.
To estimate patients’ cognition, the 10-word recall test was used for immediate and delayed episodic memory [27,28]. The test consisted of verbal registration and recall of a list of ten words immediately (first trial) and once after a delay time (delayed recall). The total scores of the two tests ranged from 0 to 10 and corresponded to the number of words the respondent could recall. Baseline cognitive function in SHARE was also measured in verbal fluency and numeracy. Based on previous studies, forgetting to take medication was identified as the most common reason for nonadherent behavior [25]; therefore, we used delayed episodic memory (delayed recall) as a cognitive measure in our study. Patients were categorized into poorer memory (<5 words correct) and better memory (≥5 words correct) groups [6,7].
The limitations with instrumental activities of everyday life (IADL) index [29] was used to describe the number of limitations with seven instrumental activities of everyday life [30]. It ranges from 0 to 7, with higher values indicating more difficulties with these activities and thus impaired mobility of the respondent.
Depression was defined using the total score on the EURO-D scale [31]. It covers 12 symptom domains: depressed mood, pessimism, suicidality, guilt, sleep, interest, irritability, appetite, fatigue, concentration, enjoyment, and tearfulness. Each item is scored 0 (symptom not present) or 1 (symptom present), and the item scores are summed to produce a scale ranging from 0 to 12. Respondents were divided into non-depressed (EURO-D <3) and depressed (EURO-D ≥4) groups [6,7,31,32,33].
2.3. Statistical Analysis
All statistical analyses were performed with R version 3.6.2 (R Foundation for Statistical Computing, Vienna, Austria), with a p-value < 0.05 indicating statistical significance. Values were given as means and standard deviations, and categorical variables were presented as numbers or percentages. Descriptive statistics were used to characterize the cohort. The association between several parameters and self-reported medication use was studied using univariate Spearman’s correlation and binomial logistic regression models (backward selection). The significance levels for variables entering the linear regression model and removing from the model were set at 0.05 and 0.1, respectively. We excluded autocorrelation and multicollinearity prior to analysis (variance inflation factor and tolerance) [34].
A mediation model was used to study the impact of polypharmacy on self-reported medication use [35,36]. Memory and depression were used as moderator(s) of the relationship between polypharmacy and self-reported medication use. Additionally, age, sex, IADL, and the number of chronic disorders were entered as covariates. The statistical significance of the direct and indirect effects was evaluated using 10,000 bootstrap samples to create bias-corrected confidence intervals (CIs; 95%). The relationship between all variables involved in the mediation analysis was approximately linear, as assessed by visually inspecting the scatterplots after LOESS smoothing. Since the pure effect of mediation is described by the indirect effect, this is the most important criterion for mediation, regardless of the other prerequisites [37,38].
3. Results
The descriptive statistics of the investigated cohort are provided in Table 1 and detailed in the initial dataset publications [6].
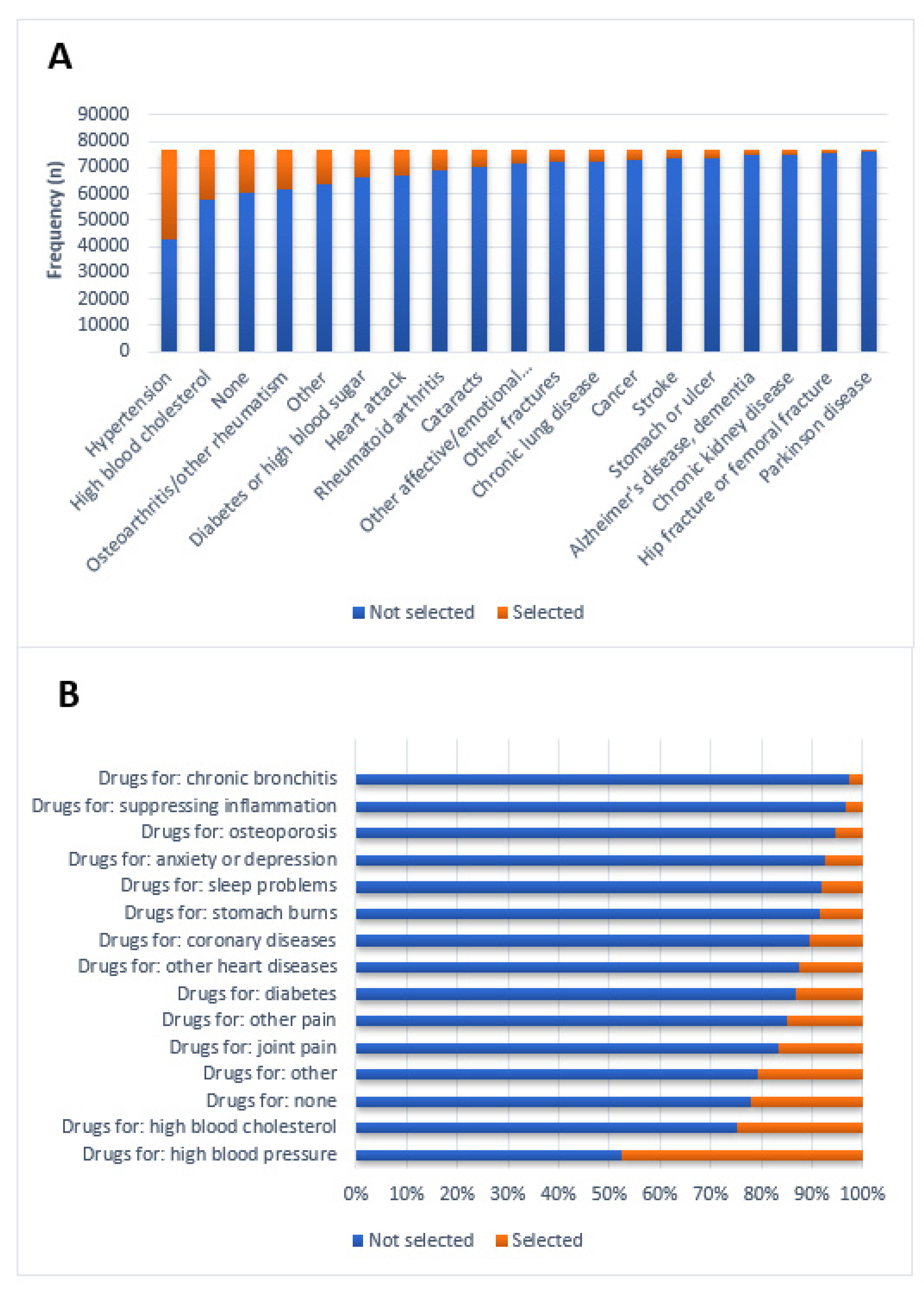
The most common self-reported disorders and conditions were hypertension, high blood cholesterol, and osteoarthritis (Figure 1A). Accordingly, most self-reported drugs were prescribed for these conditions (Figure 1B).
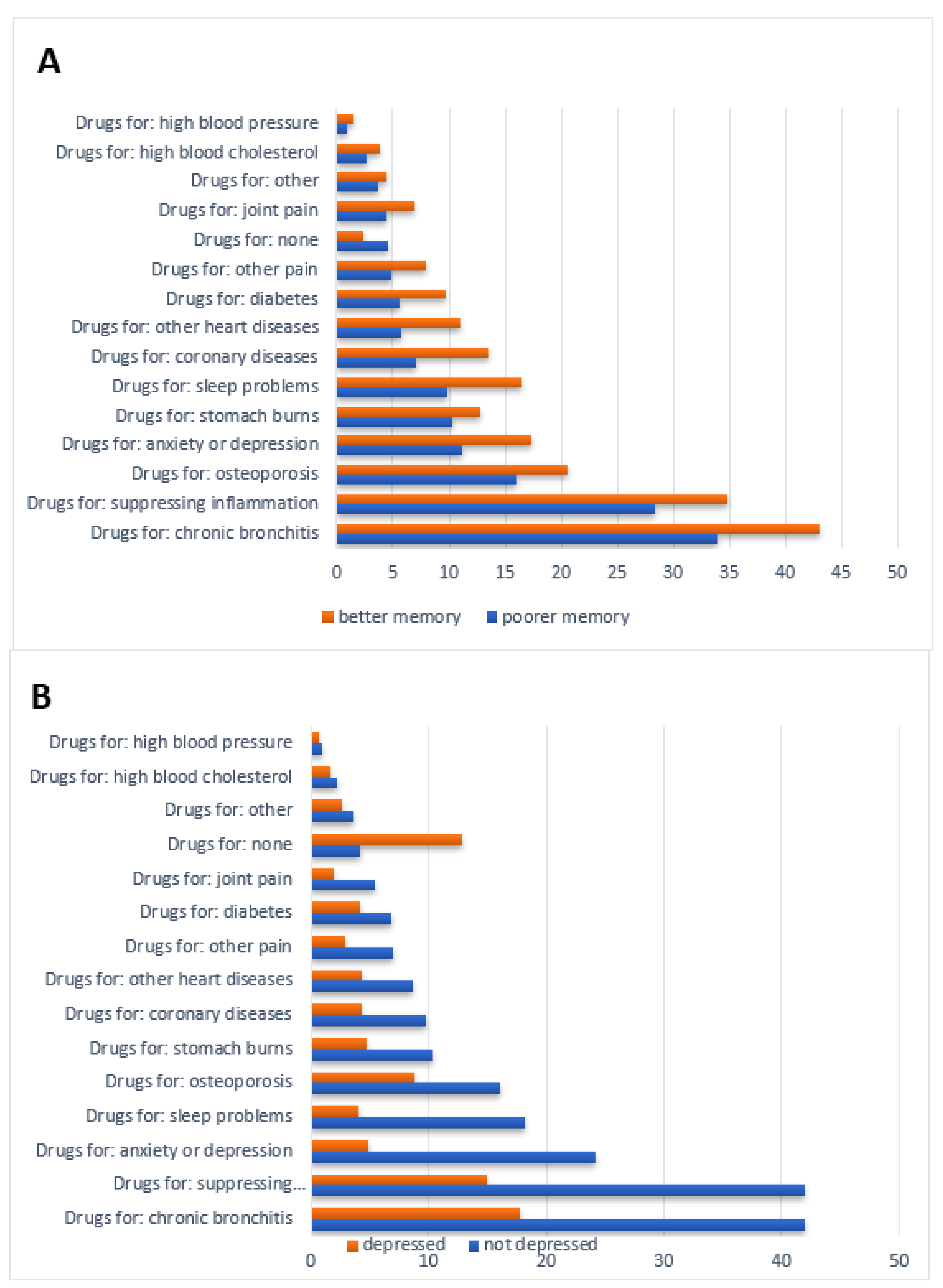
In the univariate analyses, the frequency and ratio between selected and not-selected drugs differed between people with poor and better memory (Figure 2A) and between those with and without depression (Figure 2B).
The reports of distinct disorders and—if available—the use of corresponding drugs were highly correlated, indicating that people who can select the correct diagnosis can also select the appropriate medication (Table 2). These correlations were comparable between patients with good and poor memory function (Supplementary Materials Table S1).
Logistic regression was used to further study the association between selected/not selected distinct drug classes, with memory (delayed recall of ten-word list), depression (EURO-D), gender, age, the number of chronic disorders, polypharmacy (yes/no), and selected corresponding diagnosis (present/absent) as independent variables. Correlations between predictor variables were low (r < 0.70), indicating that multicollinearity was not a confounding factor in the analysis. Exemplary findings on hypertension are presented in the paragraphs below; further analyses on other diagnoses are given in the Supplementary Materials.
As one example, the explained variance of memory, depression, and polypharmacy was 6% for antihypertensive drugs (Nagelkerke’s R² = 0.057) (Model 1 in Table 3). After entering age, the number of chronic disorders, IADL, gender, and report of hypertension as a diagnoses as additional independent variables, the explained variance increased to 72%. However, in the final model, memory and depression were no longer the significant predictors of the self-reported use of antihypertensive drugs (Model 2 in Table 3). Findings for drugs used for diabetes, chronic lung diseases, high cholesterol, anxiety, pain, and stomach problems are provided in Supplementary Materials Tables S2–S7. Results for drugs where no single corresponding disorder was recorded are provided in Supplementary Materials Tables S8–S15.
Of note, 1885 (2.5%) participants reported having dementia in the list of available diagnoses. There was a weak correlation between delayed recall of the ten-word list and the presence of dementia (r = 22,120.16, p < 0.001). As this might cause bias, analyses were repeated after the exclusion of people with dementia. This did not remarkably change the former results (Supplementary Materials Table S15).
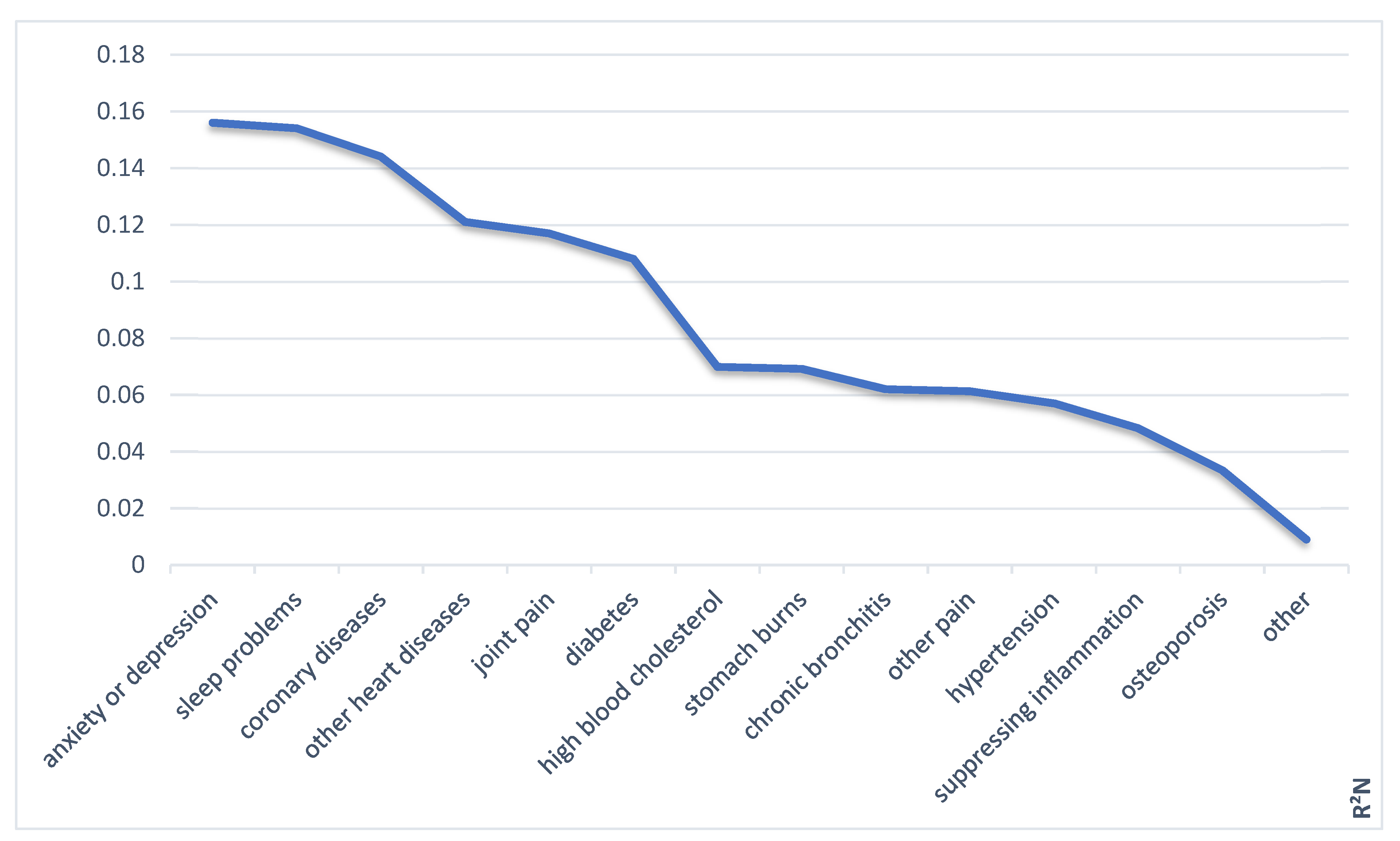
In summary, the combination of polypharmacy, memory deficits, and depression contributed in varying degrees to the self-report of medication use (Figure 3).
As demonstrated in the logistic regressions for all diagnoses assessed in this analysis, polypharmacy influences self-reported medication. Therefore, we used a mediation model to explore how polypharmacy exerts this influence. Based on previous literature, we hypothesized that the effect of polypharmacy could be mediated by depression (i.e., nondisclosure) or cognitive deficits (i.e., memory problems).
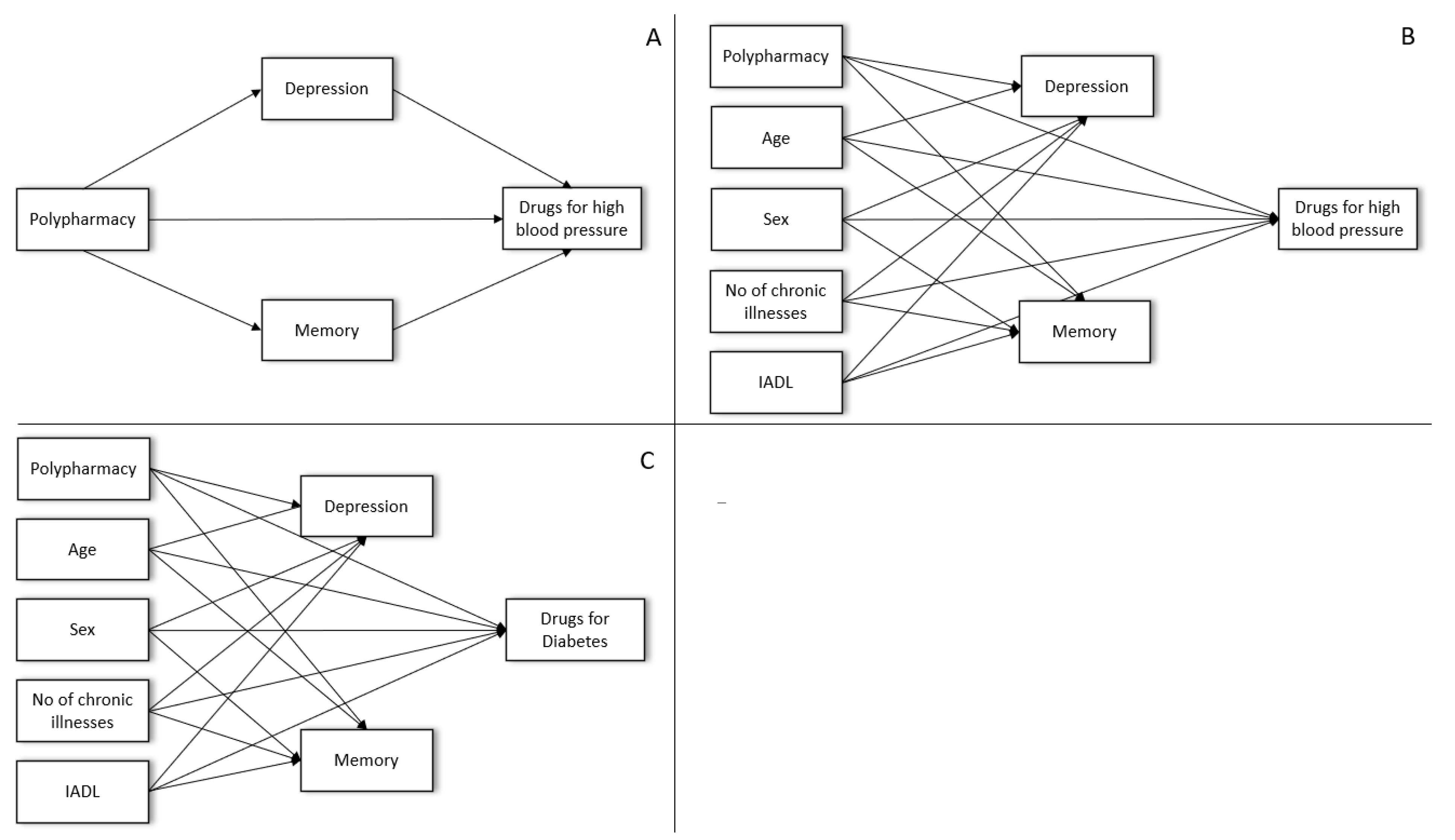
A simple mediation model is displayed in Figure 4A for the self-report of antihypertensive medication use. In this initial model, polypharmacy had a significant direct effect on the self-reported medication. In addition, there was an indirect effect of polypharmacy via depression and memory on self-reported medication (Figure 4). After entering covariates to the model, only the indirect effect through depression remained significant (Figure 4B). For diabetic medication as another example of a frequent diagnosis, both depression and memory mediated the effect of polypharmacy on self-reported diabetes medication use (Figure 4C) (see Supplementary Materials Table S16 for the full model).
4. Discussion
Using the SHARE dataset, which contains representative data on many diagnoses, we were able to demonstrate that various factors, including polypharmacy, several chronic disorders, knowledge about the diagnosis, depression, memory, restrictions in IADL, and gender might influence the self-reported medication use to different degrees. As in previous studies, all the factors, except for polypharmacy and knowledge of diagnosis, varied in their influence on the diagnoses [12,14,21].
As shown in previous studies, polypharmacy influences the self-report of medication. An increasing number of daily medications is linked to poorer knowledge when medication regimes become too complex [12,25,39]. Polypharmacy is also associated with increased age, depression, memory loss, and poor physical functioning [40] and it can be regarded as an indicator of general poorer health [14,41]. Therefore, it is possible that patients taking various medications are more likely to forget some of them when asked to report their medication. Similarly, as shown in our mediation analysis, polypharmacy itself was linked to depression, memory, and sociodemographic factors. This relationship also shows that factors related to medication behavior are not fully separable. Furthermore, they may be linked to the report itself and to the probability of getting specific prescriptions because of health reasons. The influence of polypharmacy in particular is highly relevant, as polypharmacy poses a risk for patients since not all prescribed medications are necessarily appropriate. Several methods have been developed to detect such inappropriate medication; however, it is essential to keep in mind the influence of the number of medications alone on self-reported medication use [42,43,44], to detect potentially harmful medication regimes.
Knowledge about the corresponding diagnoses strongly increased the chances of selecting medications, indicating that both have the same underlying principle of health knowledge. This is also shown by the correlations between the selection of diagnosis and corresponding medication in our analyses [5,12,14].
Similar to polypharmacy, the presence of multiple chronic disorders influenced medication reports [14,21]. However, the direction of this influence varied across diagnoses. Patients who might be accustomed to having an illness for a long time might remember them better. However, multiple chronic disorders might be linked to overall poor health and polypharmacy, again leading to difficulties in reporting all medications [14,45].
Depression and cognition have often been recognized as critical factors influencing medication behavior [5,14,15], although their influence varied across the different diagnoses reported in this study. It is essential to keep in mind that like polypharmacy, depression and cognition are reciprocally linked to health and may affect the medication report itself and actual prescription probability as health factors. Therefore, it is crucial to understand how depression and cognition influence the medication report itself, e.g., via motivational deficits, and how they are related to medication behavior and actual health. Our analyses revealed no difference in the results when excluding people reporting dementia and showed that cognition had little effect on knowledge of diagnosis and medication. However, it should be noted that there was no neuropsychological testing involved in the SHARE data collection, but the proportion of participants with reported cognitive disorders was low [1,6,7,46]. This comparability of results across people with and without cognitive impairment suggests that although cognition may influence medication reports, there is a difference between the general report of the overall presence of medication and more finely tuned knowledge, such as the exact name, dosage, or time of administration [14,25,47]. The varying direction of influence of depression and cognition in this study suggests that they are not exclusively linked to the medication report as would be expected if they had exerted their influence through nondisclosure due to the lack of motivation or forgetting. However, as shown in the mediation models, depression, polypharmacy, and cognition may not only be driving forces influencing medication knowledge but also generally concomitant symptoms of specific diagnoses and associated health factors.
Accordingly, depression, memory, and polypharmacy did not explain much of the variance of medication selection on their own. This indicates that other factors must be considered, such as age, number of diagnoses, gender differences, IADL, and the knowledge of the diagnosis. However, these factors also varied between different diagnoses, again highlighting the complexity and individuality of medication knowledge [5,12,45].
One necessary restriction of self-reported medication is the dissociation between medication knowledge, i.e., reporting prescribed medication, and actual medication behavior (e.g., taking it, adherence). This analysis only assessed self-reported medication knowledge on a superficial level. The often-cited impact of depression and cognition may act on actual medication behavior and adherence more than on the report alone. However, there was no objective measure of medication in this dataset, such as counting pills or comparison with pharmacy records [5,13]. Therefore, an objective assessment of actual medication for comparison is not provided; statements can only be made about the overall knowledge about prescribed medication and not about the medication behavior. Similarly, no assessment can be made for patients who did not select medications because there is no objective measure assessing if this information is correct. This again highlights the importance of including objective measures of medication taken to gage the adherence levels of patients.
Although the SHARE dataset presents several advantages, especially the large sample size and the inclusion of 28 different countries, it also poses certain limitations. First, SHARE is based on self-report that may not capture the medication knowledge or health status of the participants accurately [9,10]. Similarly, people who repeatedly agree to participate in large-scale research projects are more likely to be healthy and motivated. Thus, it is possible that a large group of people with more severe health problems is not represented in this survey, mainly as only noninstitutionalized participants were recruited. In SHARE, the magnitude of nonresponse and panel attrition may generate sample selection bias, limiting the representativeness of the database and the generalizability of results [7].
Similarly, reports across several countries with varying health systems and living standards may not be entirely comparable, despite the advantages promised by internationality and large sample sizes. However, the SHARE data are much more complex than conventional survey data due to their cross-national and multidisciplinary nature. This enables the exploration of the complex relationship between different life domains, individuals, family, social networks, states, and across the entire life course over time [6,7]. Furthermore, for this study, neither depression nor cognition was assessed in clinical testing. However, both measures have been validated previously and are frequently used in the literature [28,31,33].
Overall, although self-reports have been reported as relatively comparable to objective measures that can be helpful to find individual problems with medication [10,11], the results of this analysis reveal that medication self-reports are influenced by various factors, suggesting that they do not necessarily portray actual medication behavior [5,13,45]. Factors influencing medication reports vary between diagnoses, highlighting the complexity of medication knowledge and adherence and the need for assessing the interplay of parameters and their effect on medication behavior individually [12,13,23,45,47,48]. Relying solely on medication self-reports is insufficient, as there is no way to gage the validity of those reports. Based on the self-report alone, it is impossible to tell if the identified variables of influence affect the self-report alone, the actual health status, or both. Thus, in scientific research and clinical practice, medication self-reports should be used with caution as single indicators of medication behavior.
Supplementary Materials
The following are available online at https://0-www-mdpi-com.brum.beds.ac.uk/article/10.3390/healthcare9121752/s1. Supplementary Materials Table S1. Univariate Spearman correlations between self-reports of disorders/conditions and medication use in people with impaired (ten words list learning delayed recall total <5 correct) and unimpaired memory, Supplementary Materials Table S2. Binomial Logistic Regression: Drugs for diabetes, Supplementary Materials Table S3. Binomial Logistic Regression: Drugs for chronic bronchitis, Supplementary Materials Table S4. Binomial Logistic Regression: Drugs for high blood cholesterol, Supplementary Materials Table S5. Binomial Logistic Regression: Drugs for anxiety or depression, Supplementary Materials Table S6. Binomial Logistic Regression: Drugs for joint pain, Supplementary Materials Table S7. Binomial Logistic Regression: Drugs for stomach burn, Supplementary Materials Table S8. Binomial Logistic Regression: Drugs for sleep problems, Supplementary Materials Table S9. Binomial Logistic Regression: Drugs for coronary diseases, Supplementary Materials Table S10. Binomial Logistic Regression: Drugs for other heart diseases, Supplementary Materials Table S11. Binomial Logistic Regression: Drugs for other pain, Supplementary Materials Table S12. Binomial Logistic Regression: Drugs for osteoporosis, Supplementary Materials Table S13. Binomial Logistic Regression: Drugs for suppressing inflammation (only glucocorticoids or steroids), Supplementary Materials Table S14. Binomial Logistic Regression: Drugs for other, Supplementary Materials Table S15. Binominal Logistic regression: Drugs for Hypertension (after excluding people with Alzheimer’s disease, dementia, senility), Supplementary Materials Table S16. Mediation model for Drugs for diabetes
Author Contributions
Conceptualization, T.P.; methodology, T.P.; formal analysis, T.P. and A.S.; data curation, A.S.; writing—original draft preparation, A.S.; writing—review and editing, T.P.; funding acquisition, T.P. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by a Bundesministerium für Forschung und Bildung (BMBF) grant to T.P. (01GY1804).
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Institutional Ethics Committee of Jena University Hospital (approval number 5290-10/17).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
This study uses data from SHARE Wave 7 (10.6103/SHARE.w7.711), see Börsch-Supan et al. (2013) for methodological details [1]. Further information on the seventh wave can be found at Bergmann et al. (2019) and Börsch-Supan et al. (2020) [6,7]. Data collected and generated in the SHARE projects are available free of charge for scientific research without any restrictions on specific research purposes. The SHARE data collection has been funded by the European Commission through FP5 (QLK6-CT-2001-00360), FP6 (SHARE-I3: RII-CT-2006-062193, COMPARE: CIT5-CT-2005-028857, SHARELIFE: CIT4-CT-2006-028812), FP7 (SHARE-PREP: GA N°211909, SHARE-LEAP: GA N°227822, SHARE M4: GA N°261982, DASISH: GA N°283646) and Horizon 2020 (SHARE-DEV3: GA N°676536, SHARE-COHsESION: GA N°870628, SERISS: GA N°654221, SSHOC: GA N°823782) and by DG Employment, Social Affairs and Inclusion. Additional funding from the German Ministry of Education and Research, the Max Planck Society for the Advancement of Science, the U.S. National Institute on Aging (U01_AG09740-13S2, P01_AG005842, P01_AG08291, P30_AG12815, R21_AG025169, Y1-AG-4553-01, IAG_BSR06-11, OGHA_04-064, HHSN271201300071C) and from various national funding sources is gratefully acknowledged (see www.share-project.org, last accessed on 23 November 2021).
Acknowledgments
We acknowledge the financial support within the funding program Open Access Publishing by the German Research Foundation (DFG).
Conflicts of Interest
The authors declare no conflict of interests.
References
- Börsch-Supan, A.; Brandt, M.; Hunkler, C.; Kneip, T.; Korbmacher, J.; Malter, F.; Schaan, B.; Stuck, S.; Zuber, S. Data resource profile: The survey of health, ageing and retirement in europe (share). Int. J. Epidemiol. 2013, 42, 992–1001. [Google Scholar] [CrossRef]
- van de Straat, V.; Buffel, V.; Bracke, P. Medicalization of sleep problems in an aging population: A longitudinal cross-national study of medication use for sleep problems in older european adults. J. Aging Health 2017, 30, 816–838. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Midão, L.; Giardini, A.; Menditto, E.; Kardas, P.; Costa, E. Polypharmacy prevalence among older adults based on the survey of health, ageing and retirement in europe. Arch. Gerontol. Geriatr. 2018, 78, 213–220. [Google Scholar] [CrossRef] [PubMed]
- Shuldiner, J.; Tur-Sinai, A.; Bentur, N. Musculoskeletal pain medication use in middle age and older adults in 15 european countries and israel. Pain Manag. Nurs. 2020, 21, 165–171. [Google Scholar] [CrossRef] [PubMed]
- Gellad, W.F.; Grenard, J.L.; Marcum, Z.A. A systematic review of barriers to medication adherence in the elderly: Looking beyond cost and regimen complexity. Am. J. Geriatr. Pharmacother. 2011, 9, 11–23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Börsch-Supan, A. Survey of Health, Ageing and Retirement in Europe (Share) Wave 7, Release version 7.1.1. SHARE-ERIC. Data Set; Available online: http://www.share-project.org/data-documentation/waves-overview/wave-7.html (accessed on 25 November 2021).
- Bergmann, M.; Scherpenzeel, A.; Börsch-Supan, A. Share Wave 7 Methodology: Panel Innovations and Life Histories; Munich Center for the Economics of Aging (MEA): Munich, Germany, 2019. [Google Scholar]
- Hafferty, J.D.; Campbell, A.I.; Navrady, L.B.; Adams, M.J.; MacIntyre, D.; Lawrie, S.M.; Nicodemus, K.; Porteous, D.J.; McIntosh, A.M. Self-reported medication use validated through record linkage to national prescribing data. J. Clin. Epidemiol. 2018, 94, 132–142. [Google Scholar] [CrossRef] [Green Version]
- Klungel, O.H.; de Boer, A.; Paes, A.H.; Herings, R.M.; Seidell, J.C.; Bakker, A. Influence of question structure on the recall of self-reported drug use. J. Clin. Epidemiol. 2000, 53, 273–277. [Google Scholar] [CrossRef]
- Nielsen, M.W.; Søndergaard, B.; Kjøller, M.; Hansen, E.H. Agreement between self-reported data on medicine use and prescription records vary according to method of analysis and therapeutic group. J. Clin. Epidemiol. 2008, 61, 919–924. [Google Scholar] [CrossRef]
- Cotterchio, M.; Kreiger, N.; Darlington, G.; Steingart, A. Comparison of self-reported and physician-reported antidepressant medication use. Ann. Epidemiol. 1999, 9, 283–289. [Google Scholar] [CrossRef]
- Richardson, K.; Kenny, R.A.; Peklar, J.; Bennett, K. Agreement between patient interview data on prescription medication use and pharmacy records in those aged older than 50 years varied by therapeutic group and reporting of indicated health conditions. J. Clin. Epidemiol. 2013, 66, 1308–1316. [Google Scholar] [CrossRef] [PubMed]
- Stirratt, M.J.; Dunbar-Jacob, J.; Crane, H.M.; Simoni, J.M.; Czajkowski, S.; Hilliard, M.E.; Aikens, J.E.; Hunter, C.M.; Velligan, D.I.; Huntley, K.; et al. Self-report measures of medication adherence behavior: Recommendations on optimal use. Transl. Behav. Med. 2015, 5, 470–482. [Google Scholar] [CrossRef] [Green Version]
- Yap, A.F.; Thirumoorthy, T.; Kwan, Y.H. Systematic review of the barriers affecting medication adherence in older adults. Geriatr. Gerontol. Int. 2016, 16, 1093–1101. [Google Scholar] [CrossRef] [PubMed]
- Reinhard, M.J.; Hinkin, C.H.; Barclay, T.R.; Levine, A.J.; Marion, S.; Castellon, S.A.; Longshore, D.; Newton, T.; Durvasula, R.S.; Lam, M.N.; et al. Discrepancies between self-report and objective measures for stimulant drug use in hiv: Cognitive, medication adherence and psychological correlates. Addict. Behav. 2007, 32, 2727–2736. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Insel, K.; Morrow, D.; Brewer, B.; Figueredo, A. Executive function, working memory, and medication adherence among older adults. J. Gerontol. Ser. B 2006, 61, P102–P107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Monster, T.B.; Janssen, W.M.; de Jong, P.E.; de Jong-van den Berg, L.T. Pharmacy data in epidemiological studies: An easy to obtain and reliable tool. Pharmacoepidemiol. Drug Saf. 2002, 11, 379–384. [Google Scholar] [CrossRef] [PubMed]
- Klungel, O.H.; de Boer, A.; Paes, A.H.; Herings, R.M.; Seidell, J.C.; Bakker, A. Agreement between self-reported antihypertensive drug use and pharmacy records in a population-based study in the netherlands. Pharm. World Sci. 1999, 21, 217–220. [Google Scholar] [CrossRef]
- Lam, W.Y.; Fresco, P. Medication adherence measures: An overview. BioMed Res. Int. 2015, 2015, 217047. [Google Scholar] [CrossRef] [Green Version]
- Nguyen, T.M.; La Caze, A.; Cottrell, N. What are validated self-report adherence scales really measuring? A systematic review. Br. J. Clin. Pharmacol. 2014, 77, 427–445. [Google Scholar] [CrossRef]
- Van den Brandt, P.A.; Petri, H.; Dorant, E.; Goldbohm, R.A.; Van de Crommert, S. Comparison of questionnaire information and pharmacy data on drug use. Pharm. Weekbl. Sci. Ed. 1991, 13, 91–96. [Google Scholar] [CrossRef]
- Rauma, P.H.; Koivumaa-Honkanen, H.; Kröger, H.; Tuppurainen, M.T.; Kauhanen, J.; Honkanen, R.J. The relationship between self-reported and registry-based data on use of psychoactive medications in postmenopausal women. BMC Psychiatry 2013, 13, 180. [Google Scholar] [CrossRef] [Green Version]
- Duncan, N.A.; Kronenberger, W.G.; Roberson, C.P.; Janson, I.A.; Shapiro, A.D. Adherence is a human behaviour, assessing it requires multimethod evaluation with validated measures: Comment on guedes VG et al (2019). Haemophilia 2020, 26, 934–936. [Google Scholar] [CrossRef] [PubMed]
- Guedes, V.G.; Corrente, J.E.; Farrugia, A.; Thomas, S.; Wachholz, P.A.; de Oliveira Vidal, E.I. Comparing objective and self-reported measures of adherence in haemophilia. Haemophilia 2019, 25, 821–830. [Google Scholar] [CrossRef] [PubMed]
- Prell, T.; Grosskreutz, J.; Mendorf, S.; Franke, G.H.; Witte, O.W.; Kunze, A. Clusters of non-adherence to medication in neurological patients. Res. Soc. Adm. Pharm. 2019, 15, 1419–1424. [Google Scholar] [CrossRef]
- Haapea, M.; Miettunen, J.; Lindeman, S.; Joukamaa, M.; Koponen, H. Agreement between self-reported and pharmacy data on medication use in the northern finland 1966 birth cohort. Int. J. Methods Psychiatr. Res. 2010, 19, 88–96. [Google Scholar] [CrossRef]
- Goldstein, B. Cognitive Psychology: Connecting Mind, Research, and Everyday Experience, 3rd ed.; Wadsworth: Belmont, CA, USA, 2011. [Google Scholar]
- Harris, S.J.; Dowson, J.H. Recall of a 10-word list in the assessment of dementia in the elderly. Br. J. Psychiatry J. Ment. Sci. 1982, 141, 524–527. [Google Scholar] [CrossRef]
- Lawton, M.P.; Brody, E.M. Assessment of older people: Self-maintaining and instrumental activities of daily living. Gerontologist 1969, 9, 179–186. [Google Scholar] [CrossRef] [PubMed]
- Nicholas, S.; Huppert, F.; McWilliams, B.; Melzer, D. Health, Wealth and Lifestyles of the Older Population in England: The 2002 English Longitudinal Study of Ageing; IFS: Chicago, IL, USA, 2003. [Google Scholar]
- Prince, M.J.; Reischies, F.; Beekman, A.T.F.; Fuhrer, R.; Jonker, C.; Kivela, S.L.; Lawlor, B.A.; Lobo, A.; Magnusson, H.; Fichter, M.; et al. Development of the euro–d scale—A european union initiative to compare symptoms of depression in 14 european centres. Br. J. Psychiatry 1999, 174, 330–338. [Google Scholar] [CrossRef]
- Larraga, L.; Saz, P.; Dewey, M.E.; Marcos, G.; Lobo, A. Validation of the spanish version of the euro-d scale: An instrument for detecting depression in older people. Int. J. Geriatr. Psychiatry 2006, 21, 1199–1205. [Google Scholar] [CrossRef] [PubMed]
- Guerra, M.; Ferri, C.; Llibre, J.; Prina, A.M.; Prince, M. Psychometric properties of euro-d, a geriatric depression scale: A cross-cultural validation study. BMC Psychiatry 2015, 15, 12. [Google Scholar] [CrossRef] [Green Version]
- Fox, J.; Weisberg, S. An R Companion to Applied Regression, 3rd ed.; Sage: Thousand Oaks, CA, USA, 2019. [Google Scholar]
- Rosseel, Y. Lavaan: An R package for structural equation modeling. J. Stat. Softw. 2012, 48, 1–36. [Google Scholar] [CrossRef] [Green Version]
- Gallucci, M. Jamm: Jamovi Advanced Mediation Models. [Jamovi Module]. Available online: https://jamovi-amm.github.io/ (accessed on 16 September 2021).
- Rucker, D.D.; Preacher, K.J.; Tormala, Z.L.; Petty, R.E. Mediation analysis in social psychology: Current practices and new recommendations. Soc. Pers. Psychol. Compass 2011, 5, 359–371. [Google Scholar] [CrossRef]
- Zhao, X.; Lynch, J.G., Jr.; Chen, Q. Reconsidering baron and kenny: Myths and truths about mediation analysis. J. Consum. Res. 2010, 37, 197–206. [Google Scholar] [CrossRef]
- Hoel, R.W.; Giddings Connolly, R.M.; Takahashi, P.Y. Polypharmacy management in older patients. Mayo Clin. Proc. 2021, 96, 242–256. [Google Scholar] [CrossRef] [PubMed]
- Ozkok, S.; Aydin, C.O.; Sacar, D.E.; Catikkas, N.M.; Erdogan, T.; Kilic, C.; Karan, M.A.; Bahat, G. Associations between polypharmacy and physical performance measures in older adults. Arch. Gerontol. Geriatr. 2021, 98, 104553. [Google Scholar] [CrossRef]
- Schüz, B.; Wolff, J.K.; Warner, L.M.; Ziegelmann, J.P.; Wurm, S. Multiple illness perceptions in older adults: Effects on physical functioning and medication adherence. Psychol. Health 2014, 29, 442–457. [Google Scholar] [CrossRef]
- Chandrasekhar, D.; Samjas, M.; Pattani, D. Evaluation of potentially inappropriate medications among hospitalized geriatric patients in tertiary care referral hospital using stopp/start criteria. Clin. Epidemiol. Glob. Health 2019, 7, 268–273. [Google Scholar] [CrossRef] [Green Version]
- Gangannagaripalli, J.; Porter, I.; Davey, A.; Cabello, I.R.; Greenhalgh, J.; Anderson, R.; Briscoe, S.; Hughes, C.; Payne, R.; Cockcroft, E.; et al. Stopp/start interventions to improve medicines management for people aged 65 years and over: A realist synthesis. Health Serv. Deliv. Res 2021, 9, 23. [Google Scholar] [CrossRef]
- Alshammari, H.; Al-Saeed, E.; Ahmed, Z.; Aslanpour, Z. Reviewing potentially inappropriate medication in hospitalized patients over 65 using explicit criteria: A systematic literature review. Drug Healthc. Patient Saf. 2021, 13, 183–210. [Google Scholar] [CrossRef]
- Mukhtar, O.; Weinman, J.; Jackson, S.H. Intentional non-adherence to medications by older adults. Drugs Aging 2014, 31, 149–157. [Google Scholar] [CrossRef]
- Börsch-Supan, A.J.; Bristle, K.; Andersen-Ranberg, A.; Brugiavini, F.; Jusot, H.L.; Weber, G. Health and Socio-Economic Status Over the Life Course. First Results from Share Waves 6 and 7; De Gruyter: Berlin, Germany, 2019. [Google Scholar]
- Holt, E.W.; Rung, A.L.; Leon, K.A.; Firestein, C.; Krousel-Wood, M.A. Medication adherence in older adults: A qualitative study. Educ. Gerontol. 2014, 40, 198–211. [Google Scholar] [CrossRef] [Green Version]
- Tsai, K.T.; Chen, J.H.; Wen, C.J.; Kuo, H.K.; Lu, I.S.; Chiu, L.S.; Wu, S.C.; Chan, D.C. Medication adherence among geriatric outpatients prescribed multiple medications. Am. J. Geriatr. Pharmacother. 2012, 10, 61–68. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
(A) Frequencies of self-reported diseases and (B) frequencies of self-reported medication use (selected) or nonuse (not selected) in the entire cohort (n = 76,876).
Figure 1.
(A) Frequencies of self-reported diseases and (B) frequencies of self-reported medication use (selected) or nonuse (not selected) in the entire cohort (n = 76,876).

Figure 2.
(A) The ratio of drugs not selected/selected for use depending on memory function as indicated by the ten-word list learning delayed recall (poorer memory <5 words correct, better memory ≥5 words correct). (B) The ratio of drugs not selected/selected for use depending on their depression status (EURO-D <3 or ≥4).
Figure 2.
(A) The ratio of drugs not selected/selected for use depending on memory function as indicated by the ten-word list learning delayed recall (poorer memory <5 words correct, better memory ≥5 words correct). (B) The ratio of drugs not selected/selected for use depending on their depression status (EURO-D <3 or ≥4).

Figure 3.
Explained variance (R²N) of self-reported medication use by memory, depression, and polypharmacy in corresponding binominal logistic regressions.
Figure 3.
Explained variance (R²N) of self-reported medication use by memory, depression, and polypharmacy in corresponding binominal logistic regressions.

Figure 4.
Mediation models. (A) Simple mediation model for hypertension, including only depression and memory. (B) A comprehensive mediation model for hypertension. (C). Comprehensive mediation model for diabetes. Note: IADL = instrumental activities of daily living.
Figure 4.
Mediation models. (A) Simple mediation model for hypertension, including only depression and memory. (B) A comprehensive mediation model for hypertension. (C). Comprehensive mediation model for diabetes. Note: IADL = instrumental activities of daily living.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
Summary of cohort characteristics.
| Variable | M | Mdn | SD | IQR | |
|---|---|---|---|---|---|
| Age (years) | 68.5 | 68 | 10.0 | 61–76 | |
| Depression (EURO-D) | 2.4 | 2 | 2.3 | 1–4 | |
| Memory (delayed recall for ten words list learning) | 3.7 | 4 | 2.2 | 2–5 | |
| n | % | ||||
| Sex | Male | 33,150 | 42.9 | ||
| Female | 44,111 | 57.1 | |||
| Number of chronic diseases | Refusal | 39 | 0.1 | ||
| Don’t know | 118 | 0.2 | |||
| 0 | 16,061 | 20.9 | |||
| 1 | 21,187 | 27.6 | |||
| 2 | 16,463 | 21.4 | |||
| 3 | 11,096 | 14.4 | |||
| 4 | 6233 | 8.1 | |||
| 5 | 3123 | 4.1 | |||
| 6 | 1455 | 1.9 | |||
| 7 | 627 | 0.8 | |||
| 8 | 295 | 0.4 | |||
| 9 | 116 | 0.2 | |||
| 10 | 42 | 0.1 | |||
| 11 | 18 | 0.0 | |||
| 12 | 7 | 0.0 | |||
| 13 | 2 | 0.0 | |||
| Limitations with instrumental activities of daily living | Refusal | 35 | 0.0 | ||
| Don’t know | 107 | 0.1 | |||
| 0 | 61,575 | 80.6 | |||
| 1 | 5919 | 7.8 | |||
| 2 | 2367 | 3.1 | |||
| 3 | 1592 | 2.1 | |||
| 4 | 1158 | 1.5 | |||
| 5 | 827 | 1.1 | |||
| 6 | 679 | 0.9 | |||
| 7 | 633 | 0.8 | |||
| 8 | 487 | 0.6 | |||
| 9 | 980 | 1.3 | |||
| Taking at least five different drugs on a typical day | Refusal | 20 | 0.0 | ||
| Don’t know | 135 | 0.2 | |||
| Yes | 18,320 | 30.5 | |||
| No | 41,615 | 69.3 | |||
Note: M = mean, Mdr = median, IQR = interquartile range, SD = standard deviation.
Table 2.
Correlation between the reporting of distinct disorders and drug use.
| Ever Diagnosed/Currently Have | Drugs for | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| High Blood Cholesterol | High Blood Pressure | Coronary Diseases | Other Heart Diseases | Diabetes | Chronic Bronchitis | Anxiety or Depression | Joint Pain | Stomach Burns | Other Pain | Sleep Problems | Osteoporosis | Suppressing Inflammation | None | |
| High blood cholesterol | 0.704 | 0.243 | 0.145 | 0.121 | 0.170 | 0.052 | 0.074 | 0.094 | 0.119 | 0.067 | 0.095 | 0.073 | 0.037 | −0.229 |
| High blood pressure or hypertension | 0.255 | 0.825 | 0.153 | 0.163 | 0.190 | 0.053 | 0.056 | 0.128 | 0.088 | 0.084 | 0.083 | 0.049 | 0.041 | −0.421 |
| Heart attack | 0.182 | 0.174 | 0.437 | 0.513 | 0.107 | 0.076 | 0.052 | 0.098 | 0.087 | 0.073 | 0.096 | 0.042 | 0.053 | −0.174 |
| Diabetes or high blood sugar | 0.221 | 0.213 | 0.128 | 0.101 | 0.882 | 0.052 | 0.057 | 0.088 | 0.072 | 0.056 | 0.073 | 0.022 | 0.035 | −0.189 |
| Chronic lung disease | 0.052 | 0.063 | 0.097 | 0.100 | 0.052 | 0.524 | 0.070 | 0.103 | 0.102 | 0.080 | 0.087 | 0.074 | 0.096 | −0.082 |
| Other affective/ emotional disorders | 0.057 | 0.045 | 0.062 | 0.066 | 0.041 | 0.078 | 0.537 | 0.119 | 0.122 | 0.133 | 0.257 | 0.081 | 0.074 | −0.098 |
| Rheumatoid arthritis | 0.069 | 0.107 | 0.073 | 0.093 | 0.069 | 0.084 | 0.093 | 0.359 | 0.113 | 0.171 | 0.114 | 0.155 | 0.134 | −0.123 |
| Osteoarthritis/other rheumatism | 0.081 | 0.088 | 0.063 | 0.072 | 0.041 | 0.076 | 0.088 | 0.338 | 0.141 | 0.173 | 0.123 | 0.224 | 0.114 | −0.137 |
| Stomach or duodenal ulcer, peptic ulcer | 0.059 | 0.057 | 0.072 | 0.074 | 0.040 | 0.090 | 0.089 | 0.111 | 0.330 | 0.116 | 0.098 | 0.084 | 0.078 | −0.064 |
| Alzheimer’s disease, dementia, senility | 0.037 | 0.036 | 0.088 | 0.055 | 0.051 | 0.047 | 0.146 | 0.060 | 0.043 | 0.069 | 0.114 | 0.049 | 0.045 | −0.057 |
| Stroke | 0.109 | 0.128 | 0.313 | 0.150 | 0.084 | 0.066 | 0.081 | 0.070 | 0.068 | 0.077 | 0.098 | 0.050 | 0.051 | −0.087 |
Corresponding drug use and disorders are highlighted in bold. n = 76,743, for all correlations p < 0.001.
Table 3.
Exemplary binomial logistic regression: drugs for hypertension.
| Predictor. | p | Odds Ratio | 95% CI Lower | 95% CI Upper | Model Fit Measures | Overall Model Test | |||
|---|---|---|---|---|---|---|---|---|---|
| R²N | AIC | χ² | df | p | |||||
| Model 1 | |||||||||
| Intercept | <0.001 | 4.162 | 3.673 | 4.715 | 0.0570 | 14330 | 477 | 3 | < 0.001 |
| Depression | <0.001 | 0.956 | 0.939 | 0.973 | |||||
| Memory | 0.007 | 0.974 | 0.956 | 0.993 | |||||
| Polypharmacy No–Yes | <0.001 | 0.372 | 0.338 | 0.409 | |||||
| Model 2 | |||||||||
| Intercept | <0.001 | 0.0413 | 0.0206 | 0.0825 | 0.7221 | 6379 | 8439 | 8 | <0.001 |
| Depression | 0.333 | 0.9846 | 0.9540 | 1.0160 | |||||
| Memory | 0.395 | 1.0146 | 0.9813 | 1.0491 | |||||
| Polypharmacy No–Yes | <0.001 | 0.3342 | 0.2849 | 0.3920 | |||||
| Age | <0.001 | 1.0403 | 1.0316 | 1.0491 | |||||
| Number of chronic Illnesses | <0.001 | 0.8597 | 0.8137 | 0.9084 | |||||
| Instrumental activities of daily life (IADL) | 0.022 | 0.9474 | 0.9047 | 0.9922 | |||||
| Sex: Female–Male | 0.031 | 0.8637 | 0.7559 | 0.9868 | |||||
| Hypertension: Selected–Not selected | <0.001 | 156.4674 | 130.6701 | 187.3576 | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Schönenberg, A.; Prell, T. Factors Influencing Self-Reported Medication Use in the Survey of Health Aging and Retirement in Europe (SHARE) Dataset. Healthcare 2021, 9, 1752. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare9121752
AMA Style
Schönenberg A, Prell T. Factors Influencing Self-Reported Medication Use in the Survey of Health Aging and Retirement in Europe (SHARE) Dataset. Healthcare. 2021; 9(12):1752. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare9121752
Chicago/Turabian StyleSchönenberg, Aline, and Tino Prell. 2021. "Factors Influencing Self-Reported Medication Use in the Survey of Health Aging and Retirement in Europe (SHARE) Dataset" Healthcare 9, no. 12: 1752. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare9121752
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.