
Short-Term Effect of Kinesio Taping of Lower-Leg Proprioceptive Neuromuscular Facilitation Pattern on Gait Parameter and Dynamic Balance in Chronic Stroke with Foot Drop


Abstract
:1. Introduction
2. Materials and Methods
2.1. Research Design
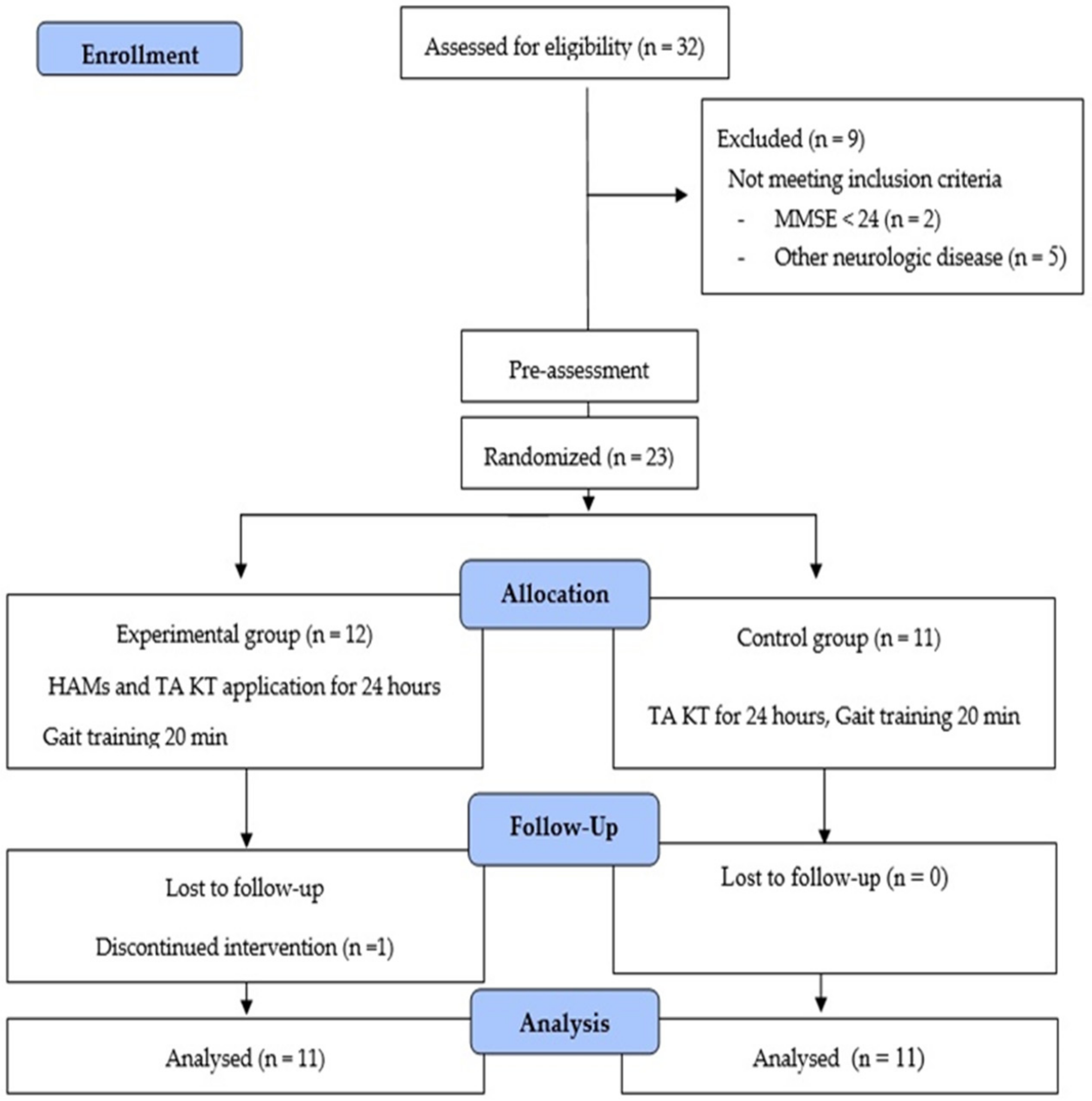
2.2. Participants and Procedure
2.3. Intervention (Applying Kinesiology Taping)
2.4. Outcome Measures
2.5. Statistical Analysis
3. Results
4. Discussion
Limitation of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chen, I.-H.; Yang, Y.-R.; Cheng, S.-J.; Chan, R.-C.; Wang, R.-Y. Neuromuscular and Biomechanical Strategies of Turning in Ambulatory Individuals Post-Stroke. Chin. J. Physiol. 2014, 57, 128–136. [Google Scholar] [CrossRef] [PubMed]
- Xu, B.; Yan, T.; Yang, Y.; Ou, R.; Huang, S. Effect of normal-walking-pattern-based functional electrical stimulation on gait of the lower extremity in subjects with ischemic stroke: A self controlled study. NeuroRehabilitation 2016, 38, 163–169. [Google Scholar] [CrossRef]
- Adegoke, B.O.A.; Olaniyi, O.; Akosile, C.O. Weight Bearing Asymmetry and Functional Ambulation Performance in Stroke Survivors. Glob. J. Health Sci. 2012, 4, 87–94. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chisholm, A.E.; Perry, S.D.; McIlroy, W.E. Correlations between ankle–foot impairments and dropped foot gait deviations among stroke survivors. Clin. Biomech. 2013, 28, 1049–1054. [Google Scholar] [CrossRef]
- Perry, J.; Bunfield, J.M. Gait Analysis: Normal and Pathological Function, 2th ed.; Slack Incorporated: New York, NY, USA, 2010; pp. 551–555. [Google Scholar]
- Sabut, S.; Kumar, R.; Lenka, P.; Mahadevappa, M. Surface EMG analysis of tibialis anterior muscle in walking with FES in stroke subjects. In Proceedings of the IEEE Engineering in Medicine and Biology Society, Buenos Aires, Argentina, 31 August–4 September 2010; IEEE: New York, NY, USA, 2010; Volume 2010, pp. 5839–5842. [Google Scholar]
- Blaya, J.A.; Herr, H. Adaptive Control of a Variable-Impedance Ankle-Foot Orthosis to Assist Drop-Foot Gait. IEEE Trans. Neural Syst. Rehabil. Eng. 2004, 12, 24–31. [Google Scholar] [CrossRef]
- Sheffler, L.R.; Hennessey, M.T.; Naples, G.G.; Chae, J. Peroneal nerve stimulation versus an ankle foot orthosis for correction of foot drop in stroke: Impact on functional ambulation. Neurorehabil. Neural Repair. 2006, 20, 355–360. [Google Scholar] [CrossRef] [PubMed]
- Bae, Y.-H.; Kim, H.G.; Min, K.S.; Lee, S.M. Effects of Lower-Leg Kinesiology Taping on Balance Ability in Stroke Patients with Foot Drop. Evid. Based Complement. Altern. Med. 2015, 2015, 1–5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, M.; Pei, Z.-W.; Xiong, B.-D.; Meng, X.-M.; Chen, X.-L.; Liao, W.-J. Use of Kinesio taping in lower-extremity rehabilitation of post-stroke patients: A systematic review and meta-analysis. Complement. Ther. Clin. Pract. 2019, 35, 22–32. [Google Scholar] [CrossRef] [PubMed]
- Choi, Y.-K.; Nam, C.-W.; Lee, J.-H.; Park, Y.-H. The Effects of Taping Prior to PNF Treatment on Lower Extremity Proprioception of Hemiplegic Patients. J. Phys. Ther. Sci. 2013, 25, 1119–1122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cayco, C.S.; Gorgon, E.J.R.; Lazaro, R.T. Effects of proprioceptive neuromuscular facilitation on balance, strength, and mobility of an older adult with chronic stroke: A case report. J. Bodyw. Mov. Ther. 2017, 21, 767–774. [Google Scholar] [CrossRef] [PubMed]
- Guiu-Tula, F.X.; Cabanas-Valdés, R.; Sitjà-Rabert, M.; Urrútia, G.; Gómara-Toldrà, N. The Efficacy of the proprioceptive neuromuscular facilitation (PNF) approach in stroke rehabilitation to improve basic activities of daily living and quality of life: A systematic review and meta-analysis protocol. BMJ Open 2017, 7, e016739. [Google Scholar] [CrossRef] [Green Version]
- Chaturvedi, P.; Singh, A.K.; Kulshreshtha, D.; Maurya, P.K.; Thacker, A.K. Proprioceptive neuromuscular facilitation (PNF) vs. task specific training in acute stroke: The effects on neuroplasticity. MOJ Anat. Physiol. 2018, 5, 1. [Google Scholar] [CrossRef] [Green Version]
- Alagappan, P. A case report on proprioceptive neuromuscular facilitation on balance and gait in hemiparetic patient. Indian J. Physiother. Occup. Ther. 2019, 13, 115. [Google Scholar] [CrossRef]
- Seo, K.; Park, S.H.; Park, K. The effects of stair gait training using proprioceptive neuromuscular facilitation on stroke patients’ dynamic balance ability. J. Phys. Ther. Sci. 2015, 27, 1459–1462. [Google Scholar] [CrossRef] [Green Version]
- Adler, S.S.; Beckers, D.; Buck, M. PNF in Practice: An Illustrated Guide, 3rd ed.; Springer: Berlin/Heidelberg, Germany, 2000; pp. 158–171. [Google Scholar]
- Kase, K.; Wallis, J.; Kase, T. Clinical Therapeutic Applications of the Kinesio Taping Method, 2nd ed.; Kinesio Taping Association: Dalls, TX, USA, 2003; pp. 20–27. [Google Scholar]
- Cohen, J. Eta-Squared and Partial Eta-Squared in Fixed Factor Anova Designs. Educ. Psychol. Meas. 1973, 33, 107–112. [Google Scholar] [CrossRef]
- Kinesiology Taping. Available online: https://www.physio-pedia.com/Kinesiology_Taping (accessed on 21 February 2021).
- Słupik, A.; Dwornik, M.; Białoszewski, D.; Zych, E. Effect of Kinesio Taping on bioelectrical activity of vastus medialis muscle. Preliminary report. Ortop. Traumatol. Rehabil. 2008, 9, 644–651. [Google Scholar]
- Koseoglu, B.F.; Dogan, A.; Tatli, H.U.; Ozcan, D.S.; Polat, C.S. Can kinesio tape be used as an ankle training method in the rehabilitation of the stroke patients? Complement. Ther. Clin. Pract. 2017, 27, 46–51. [Google Scholar] [CrossRef]
- Lee, S.M.; Lee, J.H. Effect of balance taping using kinesiology tape for a hamstring muscle injury and traumatic knee pain in an amateur university football player: A case report. Medicine 2018, 97. [Google Scholar] [CrossRef]
- Kressig, R.W.; Beauchet, O. Guidelines for clinical applications of spatio-temporal gait analysis in older adults. Aging Clin. Exp. Res. 2006, 18, 174–176. [Google Scholar] [CrossRef]
- Cho, K.H.; Lee, H.J.; Lee, W.H. Test–retest reliability of the GAITRite walkway system for the spatio-temporal gait parameters while dual-tasking in post-stroke patients. Disabil. Rehabil. 2015, 37, 512–516. [Google Scholar] [CrossRef] [PubMed]
- Faria, C.D.; Teixeira-Salmela, L.F.; Nadeau, S. Effects of the Direction of Turning on the Timed Up & Go Test with Stroke Subjects. Top. Stroke Rehabil. 2009, 16, 196–206. [Google Scholar] [CrossRef] [PubMed]
- Hiengkaew, V.; Jitaree, K.; Chaiyawat, P. Minimal Detectable Changes of the Berg Balance Scale, Fugl-Meyer Assessment Scale, Timed “Up & Go” Test, Gait Speeds, and 2-Minute Walk Test in Individuals with Chronic Stroke With Different Degrees of Ankle Plantarflexor Tone. Arch. Phys. Med. Rehabil. 2012, 93, 1201–1208. [Google Scholar] [CrossRef]
- Salbach, N.M.; Mayo, N.E.; Hanley, J.A.; Richards, C.L.; Wood-Dauphinee, S. Psychometric Evaluation of the Original and Canadian French Version of the Activities-Specific Balance Confidence Scale Among People With Stroke. Arch. Phys. Med. Rehabil. 2006, 87, 1597–1604. [Google Scholar] [CrossRef]
- Jang, S.N.; Cho, S.I.; Ou, S.W.; Lee, E.S.; Baik, H.W. The validity and reliability of Korean fall efficacy scale (FES) and activities-specific balance confidence scale (ABC). J. Korean Geriatr. Soc. 2003, 7, 255–268. [Google Scholar]
- Botner, E.M.; Miller, W.C.; Eng, J.J. Measurement properties of the Activities-specific Balance Confidence Scale among individuals with stroke. Disabil. Rehabil. 2005, 27, 156–163. [Google Scholar] [CrossRef] [PubMed]
- Bakeman, R. Recommended effect size statistics for repeated measures designs. Behav. Res. Methods 2005, 37, 379–384. [Google Scholar] [CrossRef] [PubMed]
- De Quervain, I.A.; Simon, S.R.; Leurgans, S.; Pease, W.S.; McAllister, D. Gait pattern in the early recovery period after stroke. J. Bone Joint. Surg. Am. 1996, 78, 1506–1514. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Piazza, S.J.; Delp, S.L. The influence of muscles on knee flexion during the swing phase of gait. J. Biomech. 1996, 29, 723–733. [Google Scholar] [CrossRef]
- Mulroy, S.; Gronley, J.; Weiss, W.; Newsam, C.; Perry, J. Use of cluster analysis for gait pattern classification of patients in the early and late recovery phases following stroke. Gait Posture 2003, 18, 114–125. [Google Scholar] [CrossRef]
- Kim, W.-I.; Choi, Y.-K.; Lee, J.-H.; Park, Y.-H. The Effect of Muscle Facilitation Using Kinesio Taping on Walking and Balance of Stroke Patients. J. Phys. Ther. Sci. 2014, 26, 1831–1834. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DePaul, V.; Patterson, K.K.; Inness, E.L.; Mansfield, A.; Mochizuki, G.; McIlroy, W. Relationship Between Step Length, Cadence and Capacity to Increase Gait Velocity After Recent Stroke. Arch. Phys. Med. Rehabil. 2014, 95, e31–e32. [Google Scholar] [CrossRef]
- Boeskov, B.; Carver, L.T.; Von Essen-Leise, A.; Henriksen, M. Kinesthetic Taping Improves Walking Function in Patients with Stroke: A Pilot Cohort Study. Top. Stroke Rehabil. 2014, 21, 495–501. [Google Scholar] [CrossRef]
- Persson, C.U.; Hansson, P.-O.; Sunnerhagen, K.S. Clinical tests performed in acute stroke identify the risk of falling during the first year: Postural stroke study in Gothenburg (POSTGOT). J. Rehabil. Med. 2011, 43, 348–353. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bower, K.; Thilarajah, S.; Pua, Y.-H.; Williams, G.; Tan, D.; Mentiplay, B.; Denehy, L.; Clark, R. Dynamic balance and instrumented gait variables are independent predictors of falls following stroke. J. Neuroeng. Rehabil. 2019, 16, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Schinkel-Ivy, A.; Inness, E.L.; Mansfield, A. Relationships between fear of falling, balance confidence, and control of balance, gait, and reactive stepping in individuals with sub-acute stroke. Gait Posture 2016, 43, 154–159. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ekiz, T.; Aslan, M.D.; Özgirgin, N. Effects of Kinesio Tape application to quadriceps muscles on isokinetic muscle strength, gait, and functional parameters in patients with stroke. J. Rehabil. Res. Dev. 2015, 52, 323–332. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Experimental Group (n = 11) | Control Group (n = 11) | p-Value | |
|---|---|---|---|
| Sex (male/female) | 8/3 | 7/4 | 0.647 * |
| Diagnosis (infarction/hemorrhage) | 7/4 | 3/8 | 0.19 * |
| Age (years) | 46.3 ± 7.1 | 53.8 ± 12.8 | 0.474 † |
| Onset time (months) | 19.6 ± 13.7 | 23.2 ± 14.0 | 0.556 † |
| Height (cm) | 168.2 ± 9.5 | 162.9 ± 7.5 | 0.167 † |
| Weight (kg) | 68.5 ± 8.8 | 65.3 ± 10.0 | 0.431 † |
| MMSE (score) | 28.5 ± 2.3 | 27.4 ± 2.0 | 0.209 † |
| MAS (score) | 1.0 ± 0.8 | 1.5 ± 0.7 | 0.096 † |
| Gait spatiotemporal parameter | |||
| Velocity (m/s) | 0.38 ± 0.37 69.50 ± 27.31 30.69 ± 13.14 61.95 ± 27.17 | 0.40 ± 0.25 69.84 ± 69.84 32.43 ± 15.46 59.75 ± 30.19 | 0.086 0.976 0.779 0.859 |
| Cadence (step/min) | 37.30 ± 29.73 | 34.14 ± 19.60 | 0.771 |
| Step length (cm) | 41.88 ± 19.40 | 44.77 ± 29.37 | 0.788 |
| Variables | Experimental Group (n = 11) | Control Group (n = 11) | Group * Time | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Baseline | 24 h | p | Baseline | 24 h | p | F (1, 21) | p | η2 | |
| Gait spatiotemporal parameter | |||||||||
| Velocity (m/s) | 0.38 ± 0.37 | 0.50 ±0.48 | 0.013 | 0.40 ± 0.25 | 0.42 ± 0.23 | 0.079 | 5.541 | 0.029 | 0.217 |
| Cadence (step/s) | 69.50 ± 27.31 | 77.24 ± 27.17 | 0.002 | 69.84 ± 69.84 | 70.48 ± 28.94 | 0.768 | 6.477 | 0.019 | 0.245 |
| Step length (cm) | 30.69 ± 13.14 | 35.53 ± 15.73 | 0.002 | 32.43 ± 15.46 | 34.32 ± 15.98 | 0.003 | 5.312 | 0.032 | 0.210 |
| Stride length (cm) | 61.95 ± 27.17 | 69.83 ± 33.62 | 0.005 | 59.75 ± 30.19 | 61.69 ± 32.69 | 0.086 | 6.017 | 0.023 | 0.231 |
| TUG (s) | 37.30 ± 29.73 | 27.36 ± 20.66 | 0.007 | 34.14 ± 19.60 | 32.78 ± 21.10 | 0.380 | 6.905 | 0.016 | 0.257 |
| ABC (score) | 41.88 ± 19.40 | 68.52 ± 22.78 | 0.001 | 44.77 ± 29.37 | 54.09 ± 28.50 | 0.005 | 15.222 | 0.001 | 0.432 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, D.; Bae, Y. Short-Term Effect of Kinesio Taping of Lower-Leg Proprioceptive Neuromuscular Facilitation Pattern on Gait Parameter and Dynamic Balance in Chronic Stroke with Foot Drop. Healthcare 2021, 9, 271. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare9030271
Lee D, Bae Y. Short-Term Effect of Kinesio Taping of Lower-Leg Proprioceptive Neuromuscular Facilitation Pattern on Gait Parameter and Dynamic Balance in Chronic Stroke with Foot Drop. Healthcare. 2021; 9(3):271. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare9030271
Chicago/Turabian StyleLee, Dongyun, and Youngsook Bae. 2021. "Short-Term Effect of Kinesio Taping of Lower-Leg Proprioceptive Neuromuscular Facilitation Pattern on Gait Parameter and Dynamic Balance in Chronic Stroke with Foot Drop" Healthcare 9, no. 3: 271. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare9030271