1. Introduction
All over the world, breastfeeding is recognized as the prime nutrition gaining source for the newborn [
1,
2], at least for the first six months postpartum. The World Health Organization (WHO) also recommended the first six months of birth for exclusive breastfeeding (EBF), considering the key role of breastfeeding for child development and growth, as well as the health benefits of EBF for mothers.
Exclusive breastfeeding can protect the baby from allergies, obesity, constipation, diarrhea and also reduce the risk of childhood infections [
3]. Moreover, breastfeeding can help to improve cognitive and motor development [
4] and decrease sudden infant death syndrome (SIDS) rates [
5]. On the other hand, practicing EBF can protect the mothers from type II diabetes and more importantly ovarian and breast cancers [
6,
7]. Previous literature reports that exclusively breastfed children are at lower risk of having acute respiratory and gastrointestinal infections compared with children who are not breastfed exclusively [
8]. In high human immunodeficiency virus (HIV) prevalence settings, EBF is found to prevent 13% of child deaths [
9]. It has also been shown that the rate of HIV transmission from mother to child is lower in exclusively breastfed children compared with non-EBF children [
10].
Despite the inevitable benefits of EBF, at under 1 month, the global rate of EBF is only 50%, while the rate for infants aged between 1 to 5 months is only 30% [
11]. According to the global breastfeeding scorecard 2019, an overall global prevalence of EBF up to six months is 41%, whereas the initiation of breastfeeding at first hour of birth is only 43% [
12]. The determining factors for practicing EBF is found to vary between countries and even varies within the same country.
The rate of EBF practice, in Bangladesh, a lower-middle-income country [
13], was found to be 55% in 2014 [
1,
14]. Although the rate in 2014 was above the world average, it has fluctuated a lot historically. For example, in 1993 to 2000, the rate was around 42%, in Bangladesh Demographic and Health Surveys in 2004, 2007, 2011 and 2014 the rate was 42%, 43%, 64%, and 55%, respectively. A further decline was noticed with only 47% in 2015, according to ‘The National Food Policy Plan of Action and Country Investment Plan’ of the food ministry released in 2017 [
15]. Such a decline in the EBF rate was our main motivation to investigate the knowledge and attitude of fathers and mothers of this country which may have a significant influence on building the intention of mothers to continue EBF up to six months.
The decline in the EBF rate in Bangladesh may have happened due to discontinuance of activities to promote EBF practices which took place in around 2011 [
16]. Lack of paternal and family support, workplace barriers [
2,
17] such as shorter maternity leave [
17], breastfeeding in unfriendly work environments (as most offices do not have daycare centers and do not allow time and/or space for expressing breastmilk) and long working hours [
16] etc. also may lower the rate.
In such a situation, researchers search for effective and efficient motivators of EBF practices in recent years. Researchers conducted different studies in many settings and geographic contexts and came up with different motivators of EBF practices such as mothers’ knowledge and attitude, fathers’ attitude, previous breastfeeding experience, self-confidence [
18,
19,
20,
21,
22] etc. However, fathers’ EBF knowledge, attitude, and support have rarely been studied in this regard, specifically in the case of Bangladesh. The rationale for considering Bangladesh as a sample country is that it is a small country that has gained a remarkable advancement in female education [
23] in recent years. It is generally expected that higher educated mothers and fathers have better knowledge about the merits of EBF and a stronger attitude to EBF [
24]. Moreover, the country has recently gained the status of a lower middle income economy by the World Bank [
13].
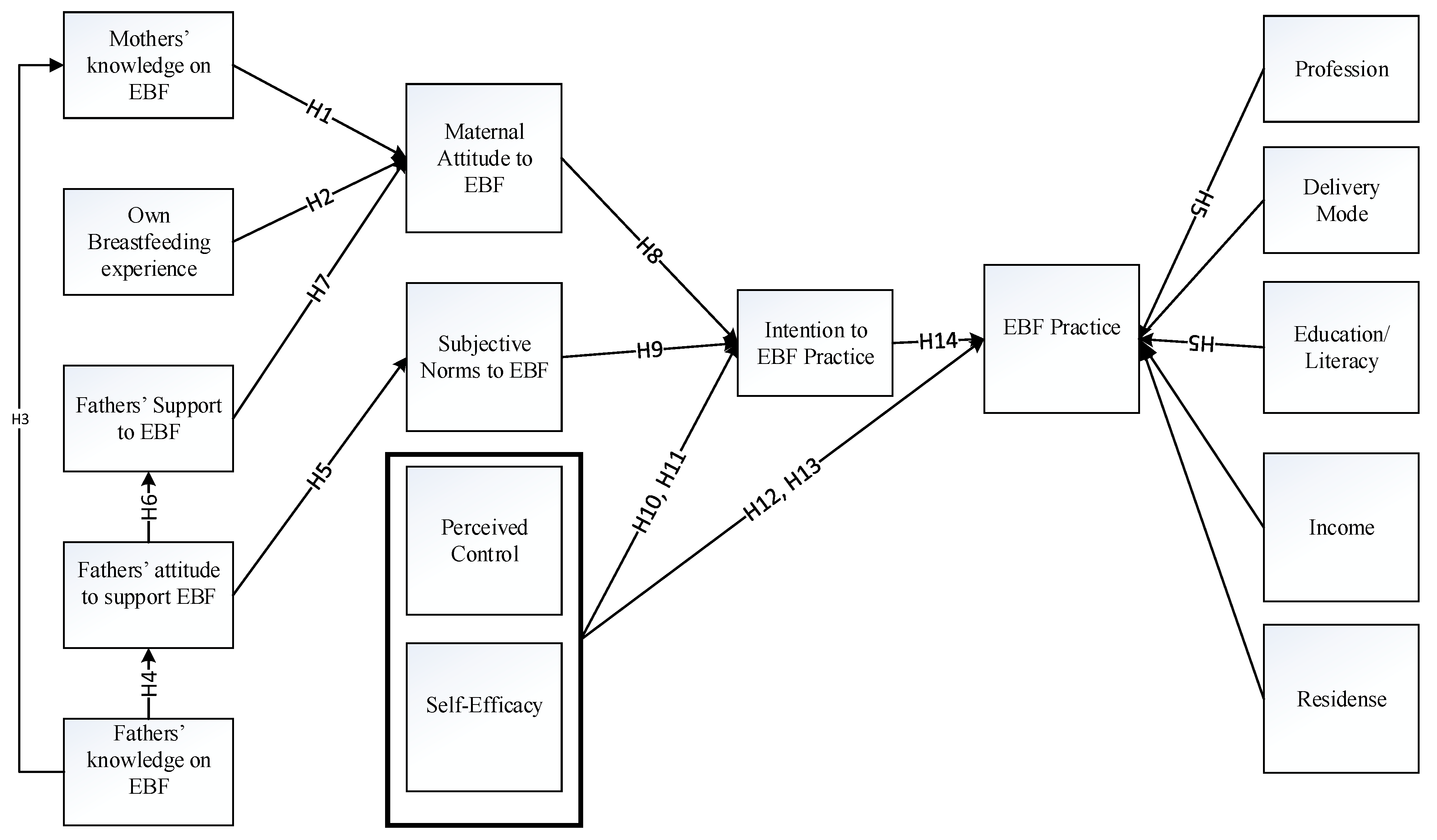
This research study demonstrates several novel points. Firstly, it explores fathers’ factors in achieving EBF success. Secondly, it considers a widely accepted theoretical framework of theory of planned behavior (TPB). Thirdly, the research considers two different dimensions based on subsamples based on delivery mode. Fourthly, data for the research is collected for a nationally distributed sample which may represent the country.
The research found that fathers’ knowledge undoubtedly assisted mothers’ EBF knowledge enrichment which result in a positive attitude of mothers to initiate and continue EBF. Moreover, fathers’ positive attitude to EBF practice by the mother and the support offered him to his wife boost her attitude as well. Thus a highly positive attitude translated into stronger intention to EBF which enhanced the chances of successful EBF practice. Additionally, the research found that perceived behavioral control is important for both sub-sample EBF practice while self-efficacy is found to be ineffective for cesarean delivery subsample. The previous breastfeeding experience is found to be inefficient for both sub-samples and the complete sample. The research also finds that control variables, income and profession is to a slight extent important determining EBF practice, however, residence and education level did not contribute to enrich EBF practices.
3. Materials and Methods
3.1. Design
The study was based on an observational design that includes parents having the youngest children between 0–6 months of age. The study was designed to evaluate the role of paternal, knowledge and attitude, social peer pressures and control factors which can potentially influence maternal intention and practice to EBF. Finally, the impacts of variables were examined to reveal the practical reality existing in Bangladesh in regards to EBF within a TPB framework and with a structural equation model (SEM).
3.2. Settings
The study was conducted in a national representative sample of Bangladesh. The sample was taken from the divisional cities of the country. In Bangladesh, a division (administrative zone) is comprised of several districts and the headquarter of the division is the divisional city. Bangladesh currently has eight divisions namely, Dhaka, Chittagong, Khulna, Rajshahi, Rangpur, Sylhet, Barisal and Mymensingh, whereas Dhaka is the capital of the country as well. The reasons for considering city dwellers were (i) in Bangladesh cities have better educational and work concentration in comparison to suburban or rural areas, (ii) other infrastructures like mobile phone network and internet access are available in all cities but scarce in village areas (iii) people from the districts and the rural regions concentrate to the cities for education and jobs. Thus we expected divisional cities to be representative of the total geographical administrative division and hence sampling from all divisional cities will make the study representative of the country.
3.3. Sampling
To determine the total sample size we employed the procedure proposed by Kothari and Garg [
49] taking moderately educated females as target fraction and find that we should have at least 312 responses. The sample size is determined by dividing the multiplication result of the value of the standard variate, sample proportions, and population size with the summation of the multiplication results of the squared value of standard error and population size less 1, and the value of standard variate and sample proportions. To make the sample more representative, we firstly determined quota for each city which based on the ratio to required total sample and the current population of the city. The data regarding total population, birth, and education percentages come from World Bank’s World Development Indicators [
50], while the data regarding population in each city under consideration came from World Population Review [
51]. Taking 30% data loss into account, the sample size required was 405. Thus we came up with a estimated sample size of 242, 92, 31, 16, 8, 6, 5 and 5 for Dhaka, Chittagong, Khulna, Rajshahi, Rangpur, Sylhet, Barisal and Mymensingh respectively. Secondly, we apply convenience sampling technique to invite parents as potential respondents. Convenience sampling is one of non-probability sampling methods where the participants are selected based on their accessibility [
52] in a non-random fashion. This technique is very useful to undertake in a quick, low expensive way and can foster target community engagement in the study. It often utilizes snowball technique using word of mouth and social media [
53]. To recruit the sample, we published our invitation to volunteer our research via social media such as Facebook mentioning key inclusion criteria and receive 130 primary responses and collected data about their demographics, current living status and the data relevant to our inclusion and exclusion criteria. After excluding non-eligible respondents, we recruited a total of 44 volunteers only. Then we contacted them over phone and shared the inclusion and exclusion specifications of the study and requested them to invite parents from their acquaintance who matched the criteria. Thus we invited a total 954 parental cases to respond to the questionnaire.
The convenience sampling technique may sometimes cause selection bias. However, in our case, recruitment of volunteers via media at the first stage and then via snowball technique, restricted to apply researchers’ choice and ease selection bias. Moreover, the applied quota technique allows the sample represent the country and reduced the potential of selection bias. The study remained unrestricted in respect of the sociodemographic variation of parents i.e., the study accepted equally parental cases from different levels of sociodemographic characteristics such as income level, age, education, race/religion, number of children, husbands’ profession and so, which also helped to reduce the chance of selection bias.
3.4. Inclusion Criteria and Exclusion Criteria
Several inclusion criteria had been followed while selecting the respondents such as (i) fathers and mothers were of at least 18 years of age and of sound mental (not suffering from lunacy, insanity or idiocy) and physical health (not having any physical incapacity easing the potential of the mother to practice EBF and/or the father to support her) who had at least one child aged between 0 to 6 months. Unsound mothers and fathers would have little chance to practice and support EBF; (ii) fathers and mothers had to be capable of reading and listening English and/or Bengali (native language of Bangladesh); (iii) parents should have communication devices (e.g., mobile phone) and either full-time or optional access to the internet (such choice was backed by two major reasons. Firstly, Bangladesh is a Muslim country and culturally conservative enough [
54]. Bangladeshi women and mothers might not feel free to conduct a face to face interview on an issue like breastfeeding. Secondly, the survey was conducted during April to June of 2020 while the outbreak of coronavirus disease 2019 (COVID-19) was a big barrier for a face to face interview. However, more than 90% households in the country own communication devices, mostly mobile phones [
55]. Moreover, most of the people already have access to internet [
56], especially city dwellers. Therefore, there would have been little chance of a communication barrier and selection bias); (iv) mothers who initiated early breastfeeding; (v) parents who lived together at the same residence with their child/children as who live separately, will have little chance to support. The study excluded (i) high-risk infant cases with chronic illness and other complications including anemia, low birth weight, congenital anomalies (for example, cleft palate or cleft lips), etc. as EBF might be hampered due to illness (ii) fathers and mothers with previous mental (for example, generalized anxiety disorder (GAD), social anxiety disorder (SAD), common mental disorders (CMD)) and physical disorders which might have restricted initiation and continuation of breastfeeding; (iii) fathers/mothers who were separated or divorced before or after childbirth as that father will have no chance to support his ex-wife; and (iv) mothers and/or infants who had any other unfavorable properties to be breastfed or to be supported by a father to breastfeed.
3.5. Measurements
This research considered fathers and mothers as separate entities and surveyed fathers and mothers independently to assess mother’s knowledge and attitude which builds the intention to practice EBF and father’s attitude to support mothers in practicing EBF. Questionnaires were used both for fathers and mothers separately. Both of the questionnaires were divided into two parts—the first part contained 11-question demographic information. The second part contained key measurement questions relevant to breastfeeding for mothers and breastfeeding support offered by fathers to the mothers. We relied on recent literature for example [
57,
58] to design the demographic information consisting of current age, education level, personal income, delivery mode for the youngest child, maternity leave, number of children and age of youngest child, region (city) of residence and contact details.
3.5.1. Exclusive Breastfeeding and Practices of EBF
As per WHO [
59], exclusive breastfeeding is termed as giving only breastmilk to the baby from the first hour of birth and no other food or liquid except necessary medication, up to the age of six months. To assess the practices of EBF of mothers we largely follow Emmanuel and Clow [
60]. This part of the questionnaire contains twelve questions including mother’s self-reports assessed questions about exclusive breastfeeding practices by asking their initiation at the first hour and continued practices at one month, three months and six months of the baby’s age. Questions about pre-plans of EBF practice and feeding after six months up to two years were also included. We followed the same style of questioning for the fathers to assess their plans and activities to support the mother for practicing EBF. The questions are in statement form which give multiple choice answering options with a five-point Likert scale consisting of 1 as strongly disagree to 5 as strongly agree.
3.5.2. Intention to Practice EBF
In the present study, we measured the intention of mothers to exclusively breastfeed the baby as per standard guidelines (from 0–6 months) with the Infant Feeding Intentions scale (IFI) following Nommsen-Rivers and Dewey [
61]. The IFI scale deals with a total of five items whereas the first two items deal with the strength of intentions of mothers to breastfeed and the rest of the items deal with the strength of their willingness to continue exclusive breastfeeding at one, three and six months of age.
3.5.3. EBF Attitude
To explore EBF attitude of mothers and fathers, we applied the “Iowa Infant Feeding Attitude Scale” (IIFAS) developed by Mora, et al. [
62]. This scale is an easily administered scale to reveal the feeding attitude. At the development stage, this scale was applied in three studies by Mora, Russell, Dungy, Losch and Dusdieker [
62] and found to be a valid and reliable instrument with Cronbach’s α ranging from 0.68 to 0.86. The instrument can predict the feeding method choice. The scale is a combination of 17 items out of which 9 are reverse coded items. We adapted the questionnaire with similar language to the original and a 5-point Likert scale to assess the attitude of mothers to breastfeed their babies exclusively. Moreover, to assess the attitude of fathers to support their partners for EBF, we asked a similar set of questions.
3.5.4. Breastfeeding Knowledge and Experience
We followed Osibogun, Olufunlayo and Oyibo [
46] to prepare a knowledge assessment tool. We developed 11-item tool/questionnaire containing statements about different aspects of EBF of which the first one assessed the engagement of the interviewee (father/mother) in breastfeeding talks, i.e., how frequently he/she used to hear about EBF. The subsequent five items assess the knowledge about what EBF is and how it benefits. Items 7–9 assessed knowledge about the expected benefit of EBF up to the first six months of the baby regarding producing energy and prevention from diseases. The next item assessed knowledge about timing of feeding breastmilk. The last item dealt with knowledge of the importance of EBF in comparison to formula feeding. Out of the 11 items, three were reverse coded. We followed the same methodology to assess the knowledge of fathers about EBF. The experience variable is measured about the mother only with a single item construct which is a binary variable i.e., 0 for primiparous mothers and 1 for multiparous mothers. This is done with the belief that multiparous mothers had a prior chance to breastfeed elder children.
3.5.5. Normative Beliefs
We use the TPB guided framework following Giles, Connor, McClenahan, Mallett, Stewart-Knox and Wright [
43] to formulate items for subjective norm construct. The construct contained six items that asked about the perception of people who are important to mother, mother’s mother, family members, husband/partner, doctor and nurse, close friends and colleague about EBF. The items directly asked the surveyed mothers about their beliefs on how the others important peers wanted them to feed their babies (for example “My mother would like me to breastfeed my baby exclusively”). It is noteworthy that this construct was applied for mothers only as this is about their normative beliefs regarding EBF and not about that of fathers’.
3.5.6. Perceived Behavioral Control
Perceived behavioral control (PBC) is determined by perceived ease of difficulty to perform certain behavior. Such control believes or perceived behavioral control constitutes internal and external control factors. The first factor, internal control, emphasizes how a person assumes him/herself to behave while performing some activity. The internal control, termed as self-efficacy, depends largely on the actor’s knowledge, skill, and ability to perform the activity or self-confidence in some activities. On the other hand, external control is the set of factors that control one’s behavioral intention and/or actual behavior due to external factors. One’s family members, friends, colleagues and peers often shape one’s behavioral intention or behavior. We follow Ajzen [
39] and Giles, Connor, McClenahan, Mallett, Stewart-Knox and Wright [
43] to formulate questions for control beliefs. This part of the questionnaire contains 11 questions while three of them represent self-efficacy and the remaining eight represent perceived behavioral control. The self-efficacy part asks three questions about the respondent’s self confidence regarding her internal factors to perform EBF, while PBC part asks seven questions about her self confidence regarding the external factors, such as her confidence to overcome EBF obstacles raised by external affairs. This construct is targeted only to mothers as they perform the primary responsibility to breastfeed their babies.
4. Data Collection, Management and Ethical Considerations
Before the final survey, we conducted a pilot survey on a small sample of 30 participants (mothers and fathers) to check the readability and validity of our questionnaire. We found a necessity for minor revision to enhance its readability and did the revisions accordingly. Moreover, we added translations into Bengali (the language of Bangladesh) of the questions/statements in brackets which were placed adjacent to each sentence/question/answering option. The translation was primarily done by the corresponding author and verified and modified by a professor of Bengali language and literature, Jatiya Kabi Kazi Nazrul, at Islam University, Mymensingh, Bangladesh. A total of 954 pairs of questionnaires were distributed considering parental cases that match our inclusion and exclusion criteria while keeping in mind the quota for each city. We went for such extensive invitation of respondents due to the low response rate (40–50%) by the online survey [
63] which is identified as very low in health care studies [
64,
65]. As described in
Section 3.3 and
Section 3.4, the respondents were invited to volunteer the research firstly by social and news media and secondly by extending the invitation through snowballing technique undertaken via primarily invited respondents according to their convenience. The data collection tool (questionnaire) was prepared using an online form employing ‘Google forms’. The links of the forms were shared to the prospective respondents by the investigators and primarily selected volunteers through online and social media (e.g., Facebook, WeChat, personal emails). At the beginning of the response, the respondents first would find a consent form which they had to respond by yes/no options. If they expressed their consent by selecting “yes”, they could get forward to respond demographic information questions. Upon completion of the demographic information they could see and respond to questions regarding EBF. The participants were able to contact us via email and telephone at any time to ask any question. To maintain the highest level of ethical standards while conducting the research, we followed several steps. Firstly, the respondents responded only on their option to do. Secondly, they could withdraw their response at any point during the study. Thirdly, the confidentiality of their responses were maintained and the data was used only for research purposes. Fourthly, inference is drawn only based upon the findings revealed in standard procedure. A total of 398 pairs of responses were received (single responses were not considered) which was around 42% of the total questionnaires sent. However, the minimum number required for our study was met even after the exclusion of incomplete responses. After the exclusion of invalid and incomplete observations, (inaccurate, duplicate, irrelevant and incomplete observations were removed from the dataset) we were able to retain 332 responses for analysis. While constructing the sample all dimensionalities (e.g., social class) were treated equally, i.e., parental cases from each dimension had the equal chance to be included, despite the issue of convenience sampling. Furthermore, from demographic analysis (presented in
Section 6) we found that participants form all age, profession, income, income, residence, religion and education groups were included in the sample.
7. Discussion
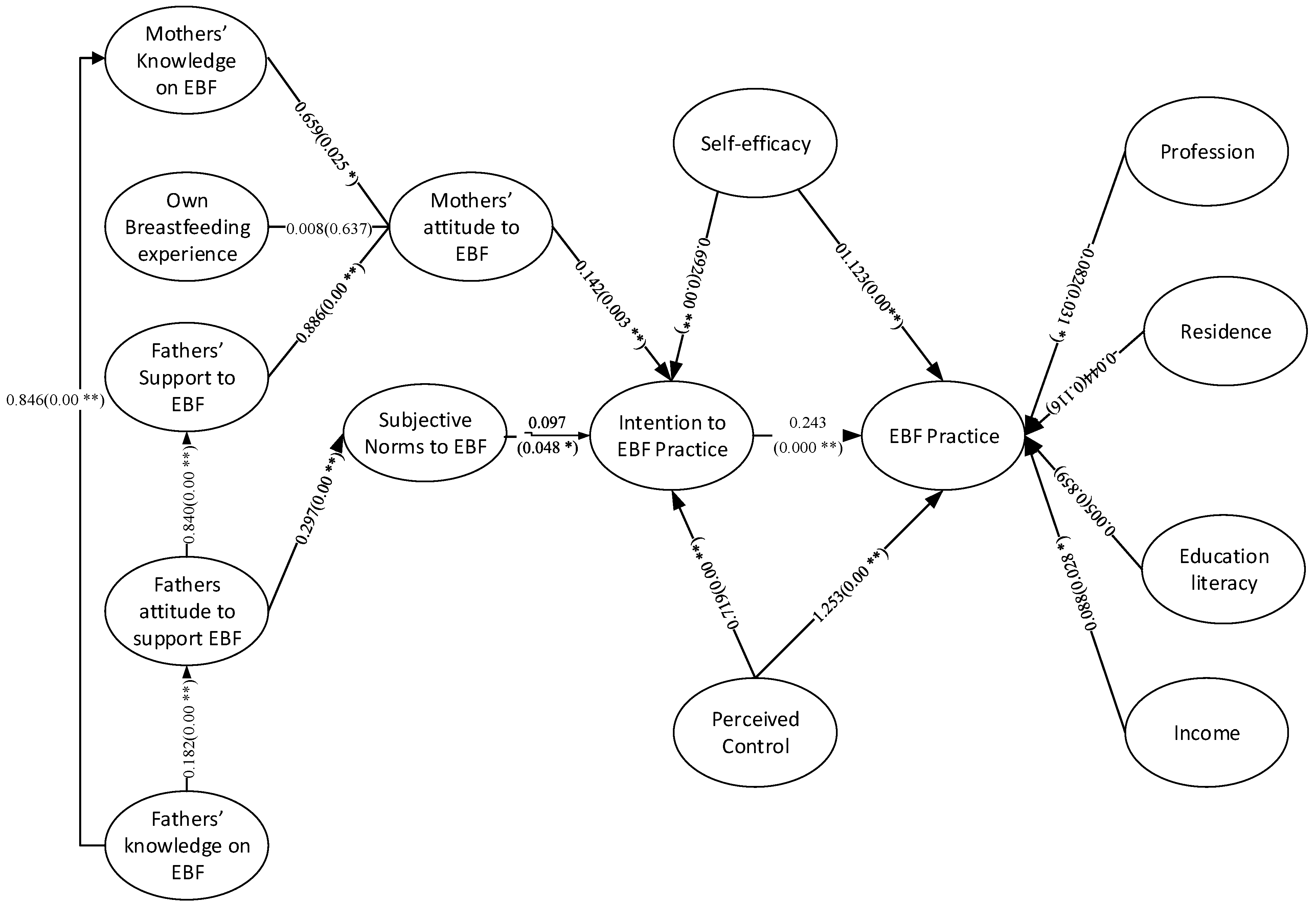
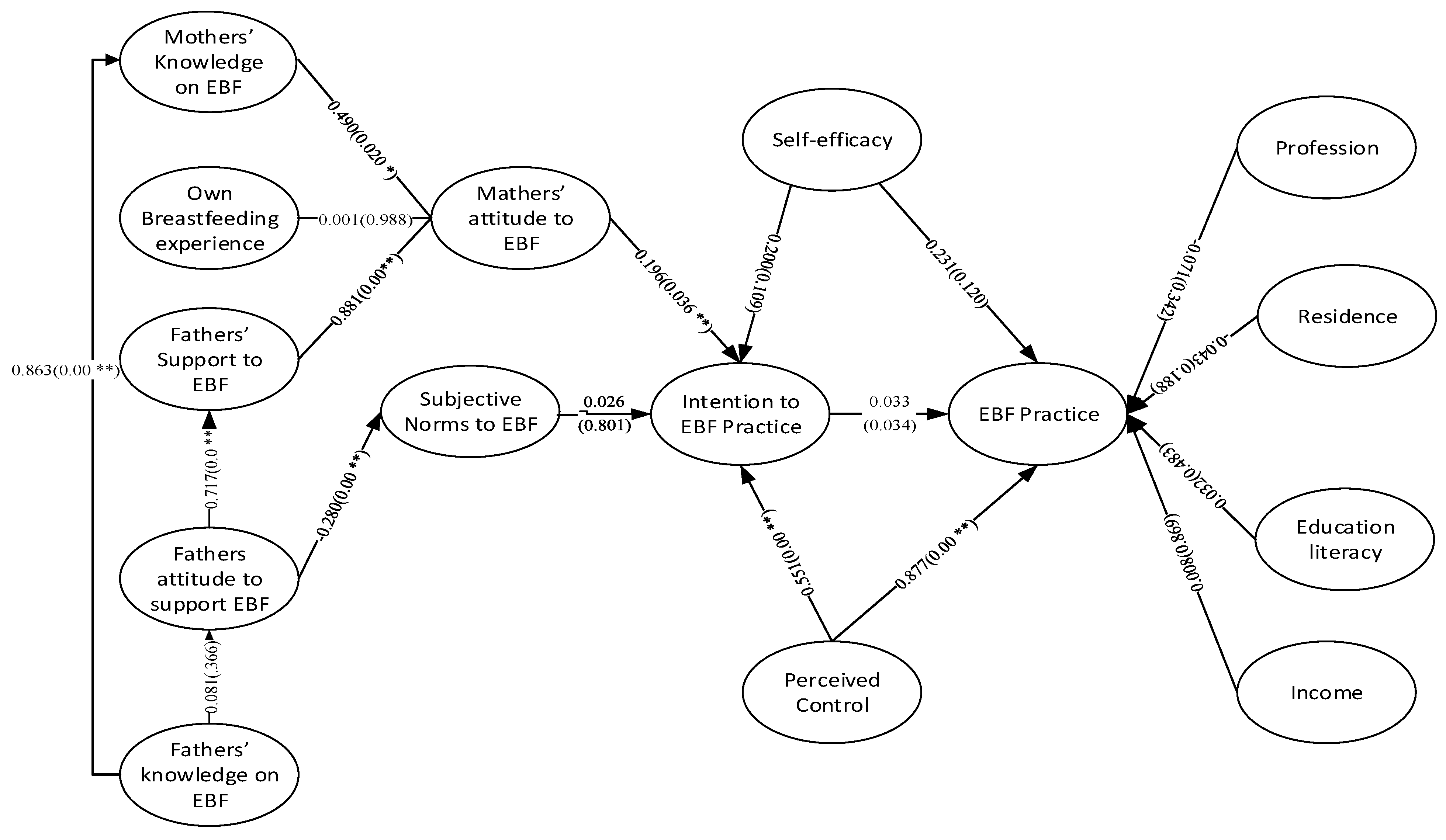
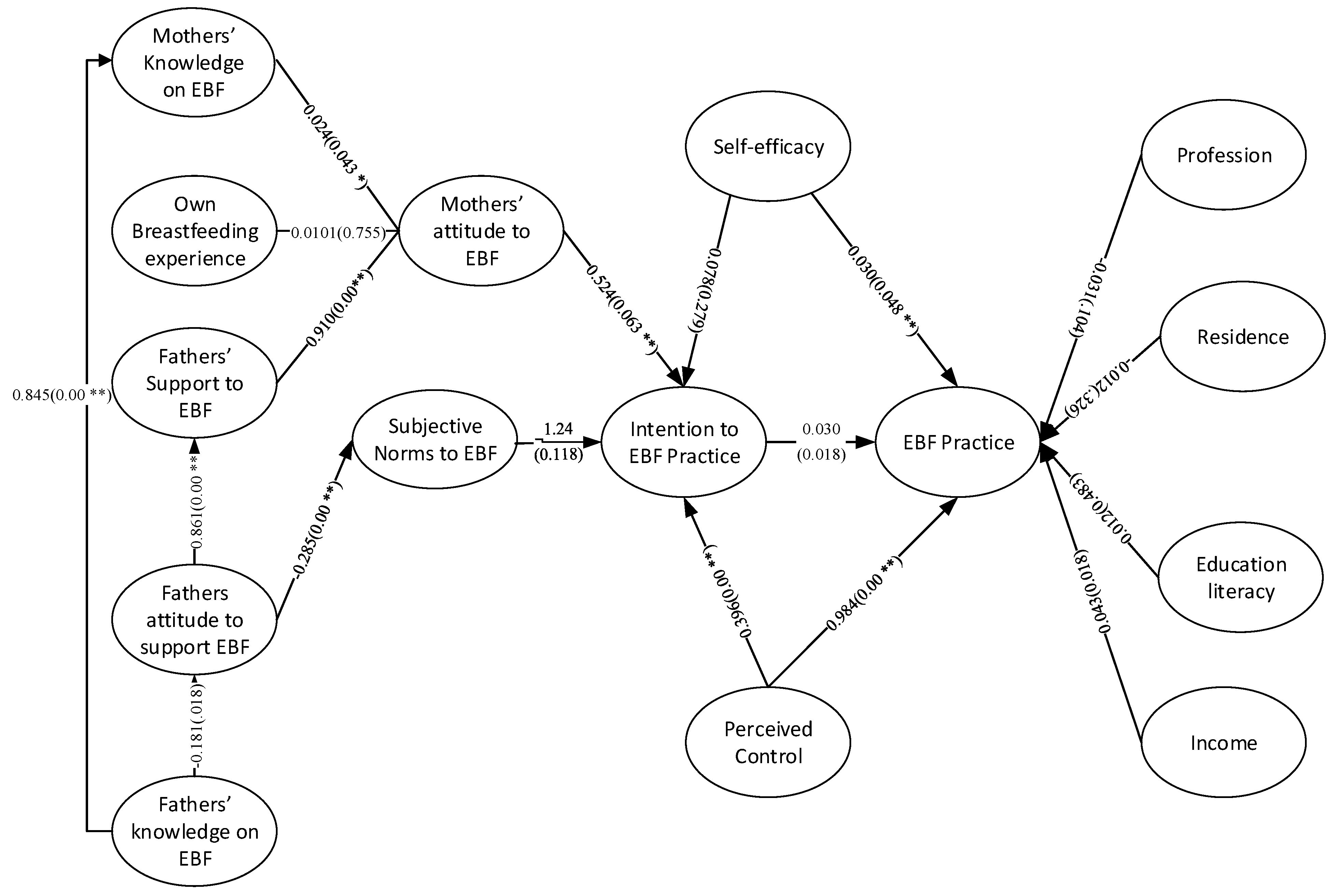
The study, to the best of our knowledge, was the first ever to diagnose the role of fathers’ knowledge about and attitude to support EBF on forming mothers’ knowledge, attitude and practice of EBF based on multi-group SEM. To test the broad aspects, we followed TPB to formulate our research framework that guides us to test Bangladeshi fathers’ knowledge of EBF and attitude to support mothers in practicing EBF on mothers’ knowledge, attitude and practice of EBF. To investigate the facts and figures, following TPB the SEMs relied on a number of principal hypotheses which direct the relationships of fathers’ knowledge and support offered to mothers and other relevant constructs to, finally, practice of EBF by the mothers. The facts revealed are presented in
Figure 2,
Figure 3 and
Figure 4 here below for the complete sample, cesarean delivery cases sub-sample and vaginal delivery cases sub-sample, respectively.
As generally known, any support by knowledge sharing is the greatest support for the recipient entity. That is, if a father can achieve knowledge about EBF, its necessity and strategies and can enlighten his partner i.e., the mother with his achieved knowledge. It is noteworthy that our study found fathers’ knowledge to explain more than 80% of mothers’ knowledge about EBF as we found the coefficient values between these two variables as 0.846 (complete sample); 0.863 (cesarean delivery sub-sample) and 0.845 (vaginal delivery sub-sample). The highly significant coefficient explains the high importance of fathers’ role play in this era. This finding is consistent with Rempel, Rempel and Moore [
21] and Rempel and Rempel [
33] as the authors suggested that a father can equip a mother with proper EBF knowledge.
On the other hand, our findings suggest that fathers’ breastfeeding knowledge enrich his attitude to offer support for EBF to the mother and consequently the enhanced positives attitude result in practical support offered by a father to his partner [
18,
39]. A father’s positive and stronger attitude is also found to directly and positively influence mother’s attitude [
19,
21,
24] and mother’s subjective norms [
32]. The maternal attitude to practice EBF, subjective norms and perceived behavioral control is found to significantly determine maternal intention to practice EBF [
22,
35,
41,
46,
82] whereas the self-efficacy sub-component is found to be of less importance and indirectly determining maternal intention.
Maternal intention being determined by maternal attitude, subjective norms, and perceived behavioral control to EBF, significantly determines actual practice of breastfeeding exclusively. The perceived behavioral control can also directly affect maternal practice of breastfeeding as the perceived behavioral control variable (jointly, self-efficacy and perceived control) is found to have a highly significant and positive coefficient.
However, the demographic instances are not found to have much specific effect on EBF practices. More specifically, however, on the complete sample the variables like profession and income had a significant effect on EBF practices while place or city of residence of mothers and level of education showed insignificant relations. Coming to separated subsamples based on delivery mode we found that all four control variables showed insignificant effects in the case of cesarean delivery subsample and for the normal delivery subsample only income showed some significant and positive relation.
In summary, our findings reveal that for Bangladeshi mothers to practice EBF, her partner’s knowledge, attitude and support are significantly important. Once a father is well educated and knowledgeable about EBF, he can share his knowledge to his wife i.e., the mother, which can enrich EBF practice through enrichment of intention via an enhanced positive attitude towards EBF. The findings are mostly robust in the complete sample and cesarean and normal delivery subsamples. The tables containing path coefficients for the complete sample is presented in
Table 5. However, for brevity path coefficients for subsamples of parental cases based on latest delivery mode of mothers—cesarean and vaginal delivery—are presented in
Table A1 and
Table A2 in
Appendix A respectively.
10. Conclusions
This paper empirically investigates the roles of a mother in practicing exclusive breastfeeding (EBF) and father role in supporting the mother within a framework of the theory of planned behavior and with structural equation modeling. To investigate the issue, we consider Bangladesh, a lower-middle-income country, as a case considering a high fluctuation in the EBF rate prevailing in the country. We endeavor to represent the whole country and conducted a survey in eight divisional cities while each represents a region/division of the country. The survey was undertaken by sending online questionnaire forms to the identified parents while the parents are identified on a joint basis of quota and convenience sampling. A total of 954 parental cases were identified and provided a questionnaire for the survey. However, only 398 questionnaires were returned. After screening and shorting out incomplete or irrationally complete responses, 332 responses were included for analysis purposes.
Analysis of data reveals that a father’s knowledge of EBF is of high importance in strengthening mother’s EBF knowledge and subjective norms in one way while in another way for enhancing the chances of other types of support (emotional and domestic) to be offered to a partner (i.e., the mother) via enhancing his attitude to support EBF. In line with the postulates of the theory of planned behavior, we also find that stronger maternal attitude to EBF, EBF supportive social norms and ease of behavioral control shape a mother’s strength of intention to breastfeed her baby exclusively, while we find that the higher the intention the better is the practice of EBF. Our findings are robust across different methodologies such SEM path analysis. These findings are important for relevant health policymakers. They should formulate and execute proper policies that encourage the health service providers to educate new and expectant fathers about EBF. Likewise, policies also may be adapted to encourage new and expectant fathers to encourage learning about EBF. Moreover, policymakers should formulate and implement policies that create social norms and ease perceived difficulties in practicing EBF, for example., For working and student mothers, proper maternity leave in all types of organization, daycare, and breastfeeding spaces in all types of schools and organizations. Community hospitals, educational institutes, formal and informal social media, and health educators may take responsibility for knowledge enhancement and awareness building by realizing the seriousness of this issue.



{kind=link}
{kind=link}
{kind=link}
{kind=link}



