
Effects of the Small-Sided Soccer Games on Blood Pressure in Untrained Hypertensive Adults: A Systematic Review and Meta-Analysis of Randomized Controlled Trials



Abstract
:1. Introduction
2. Materials and Methods
2.1. Information Sources
2.2. Eligibility Criteria
2.3. Extraction of Data
2.4. Data Items
2.5. Assessment of Methodological Quality
2.6. Summary Measures, Synthesis of Results, and Publication Bias
3. Results
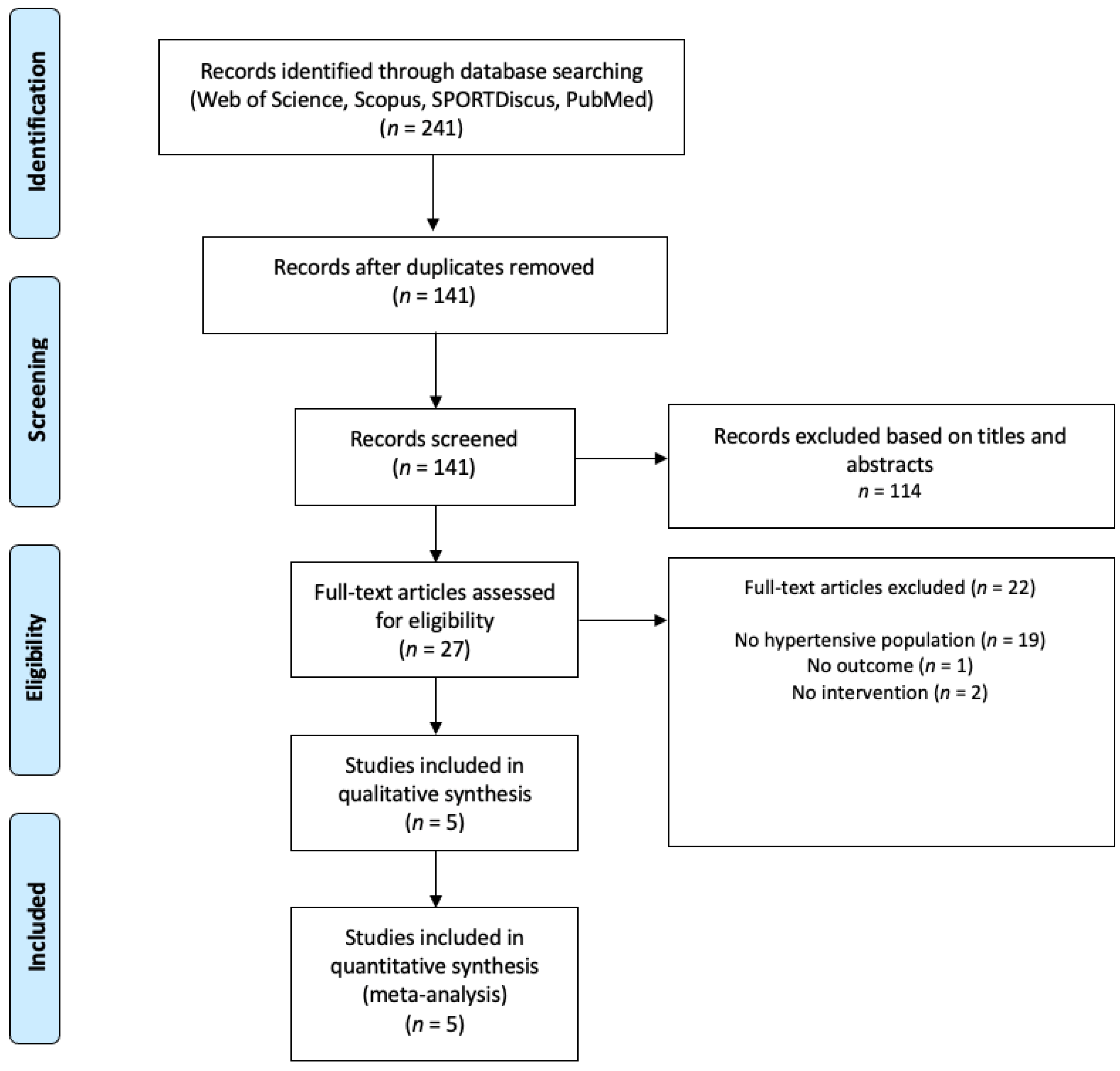
3.1. Study Identification and Selection
3.2. Study Characteristics
3.3. Methodological Quality
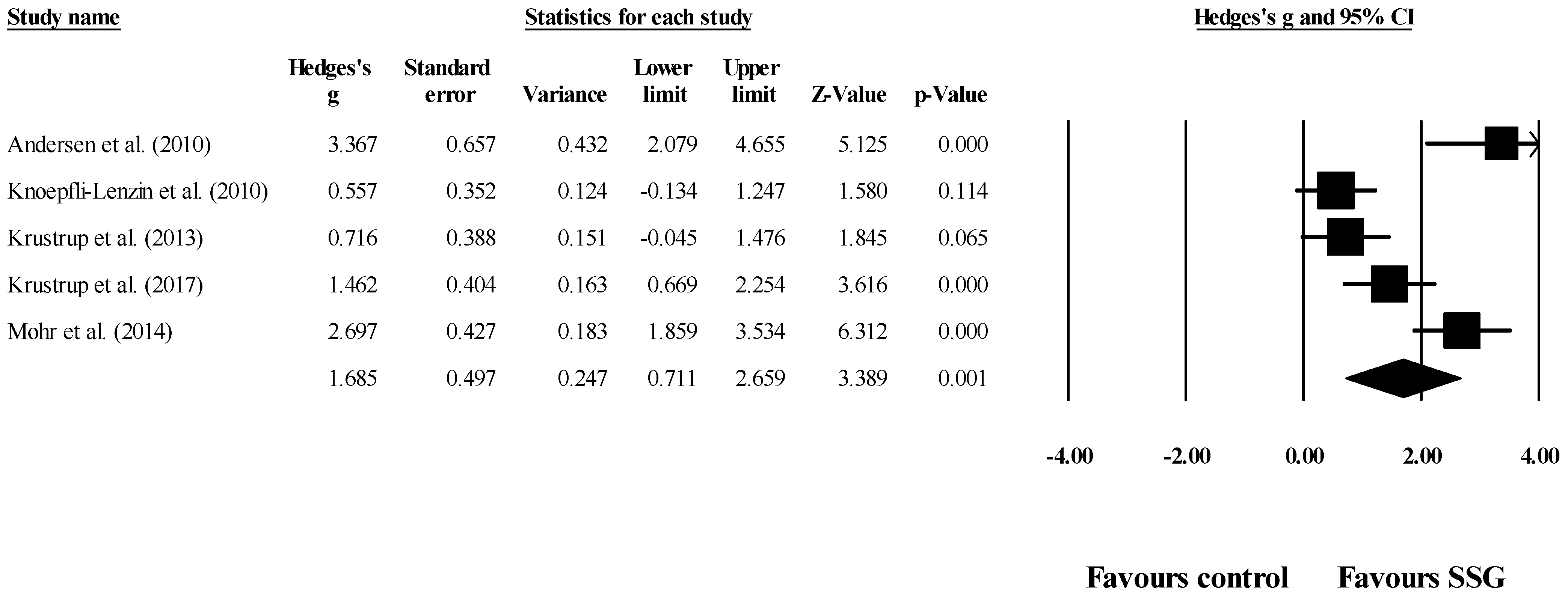
3.4. SSG vs. Control on Systolic Blood Pressure
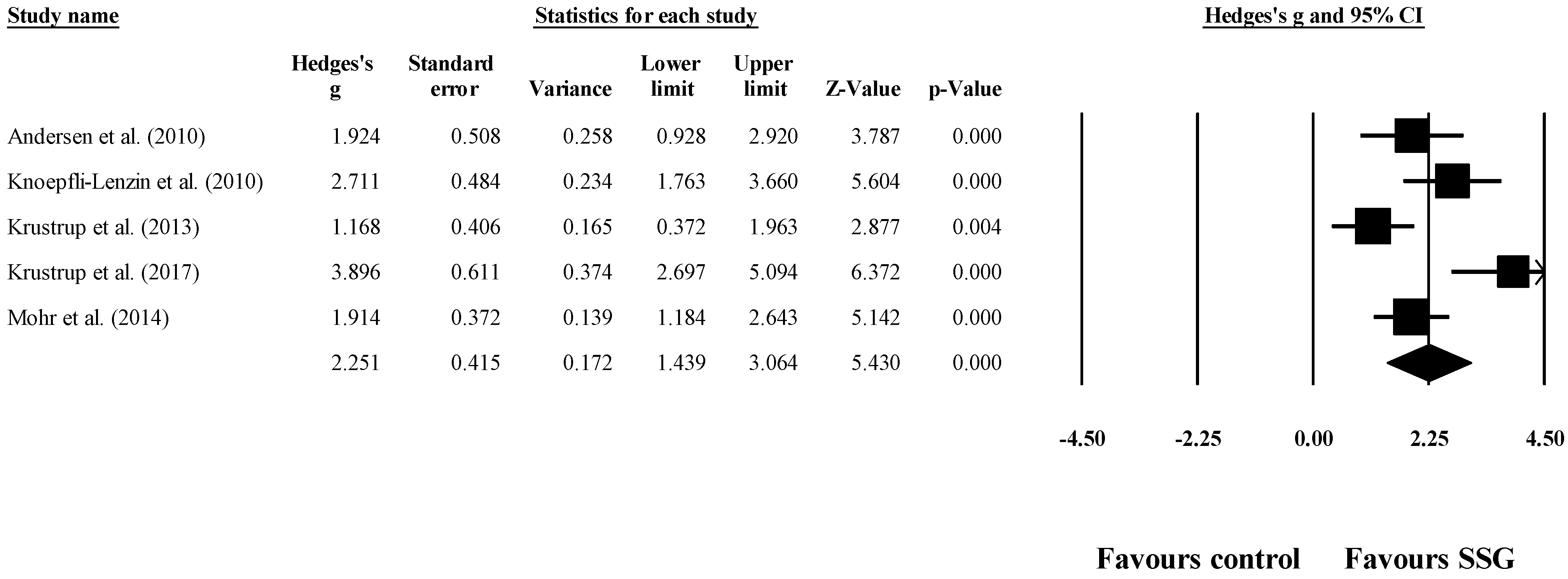
3.5. SSG vs. Control on Diastolic Blood Pressure
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Cornelissen, V.A.; Smart, N.A. Exercise Training for Blood Pressure: A Systematic Review and Meta-analysis. J. Am. Heart Assoc. 2013, 2, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Kjeldsen, S.; Feldman, R.D.; Lisheng, L.; Mourad, J.-J.; Chiang, C.-E.; Zhang, W.; Wu, Z.; Li, W.; Williams, B. Updated National and International Hypertension Guidelines: A Review of Current Recommendations. Drugs 2014, 74, 2033–2051. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chow, C.K. Prevalence, Awareness, Treatment, and Control of Hypertension in Rural and Urban Communities in High-, Middle-, and Low-Income Countries. JAMA 2013, 310, 959. [Google Scholar] [CrossRef] [Green Version]
- Lopez, A.D.; Mathers, C.D.; Ezzati, M.; Jamison, D.T.; Murray, C.J. Global and regional burden of disease and risk factors, 2001: Systematic analysis of population health data. Lancet 2006, 367, 1747–1757. [Google Scholar] [CrossRef]
- Angeli, F.; Reboldi, G.; Trapasso, M.; Gentile, G.; Pinzagli, M.G.; Aita, A.; Verdecchia, P. European and US guidelines for arterial hypertension: Similarities and differences. Eur. J. Intern. Med. 2019, 63, 3–8. [Google Scholar] [CrossRef]
- Mahmood, S.; Shah, K.U.; Khan, T.M.; Nawaz, S.; Rashid, H.; Baqar, S.W.A.; Kamran, S. Non-pharmacological management of hypertension: In the light of current research. Ir. J. Med. Sci. 2019, 188, 437–452. [Google Scholar] [CrossRef]
- Hedayati, S.S.; Elsayed, E.F.; Reilly, R.F. Non-pharmacological aspects of blood pressure management: What are the data? Kidney Int. 2011, 79, 1061–1070. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Whelton, S.P.; Chin, A.; Xin, X.; He, J. Effect of Aerobic Exercise on Blood Pressure. Ann. Intern. Med. 2002, 136, 493. [Google Scholar] [CrossRef] [PubMed]
- Duncan, L.R.; Hall, C.R.; Wilson, P.M.; Jenny, O. Exercise motivation: A cross-sectional analysis examining its relationships with frequency, intensity, and duration of exercise. Int. J. Behav. Nutr. Phys. Act. 2010, 7, 7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sarmento, H.; Manuel Clemente, F.; Marques, A.; Milanovic, Z.; David Harper, L.; Figueiredo, A. Recreational football is medicine against non-communicable diseases: A systematic review. Scand. J. Med. Sci. Sports 2020, 30, 618–637. [Google Scholar] [CrossRef] [PubMed]
- Krustrup, P.; Helge, E.W.; Hansen, P.R.; Aagaard, P.; Hagman, M.; Randers, M.B.; de Sousa, M.; Mohr, M. Effects of recreational football on women’s fitness and health: Adaptations and mechanisms. Eur. J. Appl. Physiol. 2018, 118, 11–32. [Google Scholar] [CrossRef]
- Clemente, F.M.; Afonso, J.; Sarmento, H. Small-sided games: An umbrella review of systematic reviews and meta-analyses. PLoS ONE 2021, 16, e0247067. [Google Scholar] [CrossRef]
- Clemente, F.; Sarmento, H. The effects of small-sided soccer games on technical actions and skills: A systematic review. Hum. Mov. 2020, 21, 100–119. [Google Scholar] [CrossRef] [Green Version]
- Krustrup, P.; Dvorak, J.; Junge, A.; Bangsbo, J. Executive summary: The health and fitness benefits of regular participation in small-sided football games. Scand. J. Med. Sci. Sports 2010, 20 (Suppl. 1), 132–135. [Google Scholar] [CrossRef]
- Clemente, F.M.; Afonso, J.; Castillo, D.; Arcos, A.L.; Silva, A.F.; Sarmento, H. The effects of small-sided soccer games on tactical behavior and collective dynamics: A systematic review. Chaos Solitons Fractals 2020, 134, 109710. [Google Scholar] [CrossRef]
- Diaz, K.M.; Shimbo, D. Physical Activity and the Prevention of Hypertension. Curr. Hypertens. Rep. 2013, 15, 659–668. [Google Scholar] [CrossRef] [Green Version]
- Hammami, A.; Gabbett, T.J.; Slimani, M.; Bouhlel, E. Does Small-sided Games Training Improve Physical-Fitness and Specific Skills for Team Sports? A Systematic Review with Meta-Analysis. J. Sports Med. Phys. Fitness 2018, 58, 1446–1455. [Google Scholar]
- Moran, J.; Blagrove, R.C.; Drury, B.; Fernandes, J.F.T.; Paxton, K.; Chaabene, H.; Ramirez-Campillo, R. Effects of Small-Sided Games vs. Conventional Endurance Training on Endurance Performance in Male Youth Soccer Players: A Meta-Analytical Comparison. Sports Med. 2019, 49, 731–742. [Google Scholar] [CrossRef] [Green Version]
- Kunz, P.; Engel, F.A.; Holmberg, H.-C.; Sperlich, B. A Meta-Comparison of the Effects of High-Intensity Interval Training to Those of Small-Sided Games and Other Training Protocols on Parameters Related to the Physiology and Performance of Youth Soccer Players. Sports Med. Open 2019, 5, 7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Castagna, C.; de Sousa, M.; Krustrup, P.; Kirkendall, D.T. Recreational team sports: The motivational medicine. J. Sport Health Sci. 2018, 7, 129–131. [Google Scholar] [CrossRef] [PubMed]
- Luo, H.; Newton, R.U.; Ma’ayah, F.; Galvão, D.A.; Taaffe, D.R. Recreational soccer as sport medicine for middle-aged and older adults: A systematic review. BMJ Open Sport Exerc. Med. 2018, 4, e000336. [Google Scholar] [CrossRef]
- Milanovic, Z.; Pantelic, S.; Covic, N.; Sporis, G.; Krustrup, P. Is Recreational Soccer Effective for Improving VO2max? A Systematic Review and Meta-Analysis. Sport. Med. 2015, 45, 1339–1353. [Google Scholar] [CrossRef] [Green Version]
- Zouhal, H.; Hammami, A.; Tijani, J.M.; Jayavel, A.; de Sousa, M.; Krustrup, P.; Sghaeir, Z.; Granacher, U.; Ben Abderrahman, A. Effects of Small-Sided Soccer Games on Physical Fitness, Physiological Responses, and Health Indices in Untrained Individuals and Clinical Populations: A Systematic Review. Sports Med. 2020, 50, 987–1007. [Google Scholar] [CrossRef]
- Barbosa, A.; Brito, J.; Figueiredo, P.; Seabra, A.; Mendes, R. Football can tackle type 2 diabetes: A systematic review of the health effects of recreational football practice in individuals with prediabetes and type 2 diabetes. Res. Sports Med. 2020. [Google Scholar] [CrossRef]
- Green, S.; Higgins, J. Cochrane Handbook for Systematic Reviews of Interventions; John Wiley & Sons: Hoboken, NJ, USA, 2005. [Google Scholar]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Cochrane Collaboration. Data Extraction Template for Included Studies. Available online: https://cccrg.cochrane.org/sites/cccrg.cochrane.org/files/public/uploads/det_2015_revised_final_june_20_2016_nov_29_revised.doc (accessed on 2 January 2021).
- Deeks, J.J.; Higgins, J.P.; Altman, D.G. Analysing data and undertaking meta-analyses. In Cochrane Handbook for Systematic Reviews of Interventions; Higgins, J.P., Green, S., Eds.; The Cochrane Collaboration: Oxford, UK, 2008; pp. 243–296. [Google Scholar]
- Kontopantelis, E.; Springate, D.A.; Reeves, D. A Re-Analysis of the Cochrane Library Data: The Dangers of Unobserved Heterogeneity in Meta-Analyses. PLoS ONE 2013, 8, e69930. [Google Scholar] [CrossRef]
- Hopkins, W.G.; Marshall, S.W.; Batterham, A.M.; Hanin, J. Progressive Statistics for Studies in Sports Medicine and Exercise Science. Med. Sci. Sports Exerc. 2009, 41, 3–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgins, J.P.T.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef]
- Egger, M.; Smith, G.D.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duval, S.; Tweedie, R. Trim and Fill: A Simple Funnel-Plot-Based Method of Testing and Adjusting for Publication Bias in Meta-Analysis. Biometrics 2000, 56, 455–463. [Google Scholar] [CrossRef] [PubMed]
- Andersen, L.J.; Randers, M.B.; Westh, K.; Martone, D.; Hansen, P.R.; Junge, A.; Dvorak, J.; Bangsbo, J.; Krustrup, P. Football as a treatment for hypertension in untrained 30-55-year-old men: A prospective randomized study. Scand. J. Med. Sci. Sports 2010, 20, 98–102. [Google Scholar] [CrossRef] [PubMed]
- Knoepfli-Lenzin, C.; Sennhauser, C.; Toigo, M.; Boutellier, U.; Bangsbo, J.; Krustrup, P.; Junge, A.; Dvorak, J. Effects of a 12-week intervention period with football and running for habitually active men with mild hypertension. Scand. J. Med. Sci. Sports 2010, 20, 72–79. [Google Scholar] [CrossRef]
- Krustrup, P.; Randers, M.B.; Andersen, L.J.; Jackman, S.R.; Bangsbo, J.; Hansen, P.R. Soccer Improves Fitness and Attenuates Cardiovascular Risk Factors in Hypertensive Men. Med. Sci. Sport. Exerc. 2013, 45, 553–561. [Google Scholar] [CrossRef]
- Krustrup, P.; Skoradal, M.-B.; Randers, M.B.; Weihe, P.; Uth, J.; Mortensen, J.; Mohr, M. Broad-spectrum health improvements with one year of soccer training in inactive mildly hypertensive middle-aged women. Scand. J. Med. Sci. Sports 2017, 27, 1893–1901. [Google Scholar] [CrossRef]
- Mohr, M.; Lindenskov, A.; Holm, P.M.; Nielsen, H.P.; Mortensen, J.; Weihe, P.; Krustrup, P. Football training improves cardiovascular health profile in sedentary, premenopausal hypertensive women. Scand. J. Med. Sci. Sports 2014, 24, 36–42. [Google Scholar] [CrossRef] [PubMed]
- Faselis, C.; Doumas, M.; Kokkinos, J.P.; Panagiotakos, D.; Kheirbek, R.; Sheriff, H.M.; Hare, K.; Papademetriou, V.; Fletcher, R.; Kokkinos, P. Exercise Capacity and Progression From Prehypertension to Hypertension. Hypertension 2012, 60, 333–338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sharman, J.E.; Smart, N.A.; Coombes, J.S.; Stowasser, M. Exercise and sport science australia position stand update on exercise and hypertension. J. Hum. Hypertens. 2019, 33, 837–843. [Google Scholar] [CrossRef] [Green Version]
- Hagberg, J.M.; Park, J.-J.; Brown, M.D. The Role of Exercise Training in the Treatment of Hypertension. Sports Med. 2000, 30, 193–206. [Google Scholar] [CrossRef] [PubMed]
- Wallace, J.P. Exercise in Hypertension. Sport. Med. 2003, 33, 585–598. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| PICOS Components | Details |
|---|---|
| Population | Untrained hypertensive adult populations of both sexes |
| Intervention | Small-sided games (SSG)-based training programs |
| Comparator | Passive controls |
| Outcomes | Blood pressure, systolic blood pressure, diastolic blood pressure |
| Study design | Randomized controlled trials and controlled trials |
| Study | Mean Age (y) | N | Sex | Training Level | Design | CG | Protocol of Test Used in the Original Studies | Measure Extracted from the Tests in the Original Studies |
|---|---|---|---|---|---|---|---|---|
| Andersen et al. [34] | SSG: 46.7 ± 2.0 CG: 47.8 ± 1.8 | SSG: 13 CG: 9 | M | Untrained | RCT | Only received physician-guided traditional recommendation on cardiovascular risk factor modification | Supine position followed by 15 min rest. Blood pressure was recorded five times in both upper arms. Average values of 10 measurements were presented. | Systolic blood pressure (mm Hg) Diastolic blood pressure (mm Hg) |
| Knoepfli-Lenzin et al. [35] | SSG: 37.0 ± 4.0 CG: 38.0 ± 5.0 | SSG: 15 CG: 17 | M | Untrained | RCT | Continued their sedentary lifestyle | Measured in a sitting position | Systolic blood pressure (mm Hg) Diastolic blood pressure (mm Hg) |
| Krustrup et al. [36] | 46 (range 31–54) | SSG: 20 CG: 10 | M | Untrained | RCT | Only received physician-guided traditional recommendation on cardiovascular risk factor modification | Supine position followed by 15 min rest. Blood pressure was recorded five times in both upper arms. Average values of 10 measurements were presented. | Systolic blood pressure (mm Hg) Diastolic blood pressure (mm Hg) |
| Krustrup et al. [37] | SSG: 45.0 ± 6.0 CG: 45.0 ± 4.0 | SSG: 19 CG: 12 | W | Untrained | RCT | Continued their sedentary lifestyle | Supine position followed by 15 min rest. Blood pressure was recorded five times in both upper arms. Average values of 10 measurements were presented. | Systolic blood pressure (mm Hg) Diastolic blood pressure (mm Hg) |
| Mohr et al. [38] | SSG: 45.0 ± 3.0 CG: 43.0 ± 3.0 | SSG: 21 CG: 20 | W | Untrained | RCT | Continued their sedentary lifestyle | Measured after resting in supine position for 2 h. The average of 4 measurements was used. | Systolic blood pressure (mm Hg) Diastolic blood pressure (mm Hg) |
| Study | Duration (M/W) | d/w | Session/Person Per Week (n) | Total Sessions | SSG Formats | SSG Pitch Dimension (Length × Width) | SSG Area Per Player (m2) | Sets | Reps | Recovery between Sets (min) | Recovery between Sets (Intensity) | Total Work Duration (min) | Work Duration Per Set (min) | Work Intensity |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Andersen et al. [34] | 3 M | 2 | 1.7 ± 0.2 | 22 | 5 vs.5 6 vs.6 7 vs.7 | 45–60 × 30–45 m | ND | 2 | - | 5 | ND | 50 | 25 | ND |
| Knoepfli-Lenzin et al. [35] | 12 W | 3 | 2.4 ± 0.2 | ND | 3 vs.3 4 vs.4 5 vs.5 | ND | ND | ND | ND | ND | ND | 50 | ND | 79.9 ± 4.5% HRmax |
| Krustrup et al. [36] | 6 M | 2 | 1.7 ± 0.5 | 43 | 5 vs.5 6 vs.6 7 vs.7 | 45–60 × 30–45 m | ND | 4 | ND | 2 | - | 48 | 12 | 85.0 ± 7.0% HRmax |
| Krustrup et al. [37] | 12 M | 2 | 2.5 ± 0.4 | 128 ± 29 | 4 vs.4 to 8 vs.8 | ND | ND | 4 | ND | 2 | - | 48 | 12 | ND |
| Mohr et al. [38] | 15 W | 3 | 3.0 ± 0.1 | 45 | 4 vs.4 to 10 vs.10 | ND | ND | ND | ND | ND | ND | ~60 | ND | 80.5 ± 1.1 to 98.9 ± 1.4 HRmax |
| Study | N.1 * | N.2 | N.3 | N.4 | N.5 | N.6 | N.7 | N.8 | N.9 | N.10 | N.11 | Total ** |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Andersen et al. [34] | 1 | 1 | 1 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 7 |
| Knoepfli-Lenzin et al. [35] | 1 | 1 | 1 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 7 |
| Krustrup et al. [36] | 1 | 1 | 1 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 7 |
| Krustrup et al. [37] | 1 | 1 | 1 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 7 |
| Mohr et al. [38] | 1 | 1 | 1 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 7 |
| Study | Group | N | Before Mean ± SD | After Mean ± SD | After–Before (Δ%) |
|---|---|---|---|---|---|
| Andersen et al. [34] | SSG | 13 | 150 ± 3 | 138 ± 2 | −8.0 |
| Knoepfli-Lenzin et al. [35] | SSG | 15 | 136 ± 3 | 124 ± 4 | −8.8 |
| Krustrup et al. [36] | SSG | 20 | 151 ± 10 | 139 ± 9 | −7.9 |
| Krustrup et al. [37] | SSG | 19 | 140 ± 1 | 133 ± 3 | −5.0 |
| Mohr et al. [38] | SSG | 21 | 139 ± 3 | 127 ± 4 | −8.6 |
| Andersen et al. [34] | CG | 9 | 153 ± 3 | 148 ± 2 | −3.3 |
| Knoepfli-Lenzin et al. [35] | CG | 17 | 136 ± 3 | 126 ± 3 | −7.4 |
| Krustrup et al. [36] | CG | 10 | 152 ± 7 | 146 ± 6 | −3.9 |
| Krustrup et al. [37] | CG | 12 | 135 ± 9 | 132 ± 2 | −2.2 |
| Mohr et al. [38] | CG | 20 | 134 ± 4 | 133 ± 4 | −0.7 |
| Study | Group | N | Before Mean ± SD | After Mean ± SD | After–Before (Δ%) |
|---|---|---|---|---|---|
| Andersen et al. [34] | SSG | 13 | 91 ± 2 | 84 ± 2 | −7.7 |
| Knoepfli-Lenzin et al. [35] | SSG | 15 | 87 ± 3 | 76 ± 3 | −12.6 |
| Krustrup et al. [36] | SSG | 20 | 92 ± 7 | 84 ± 5 | −8.7 |
| Krustrup et al. [37] | SSG | 19 | 87 ± 9 | 83 ± 2 | −4.6 |
| Mohr et al. [38] | SSG | 21 | 86 ± 2 | 80 ± 3 | −7.0 |
| Andersen et al. [34] | CG | 9 | 95 ± 2 | 92 ± 2 | −3.2 |
| Knoepfli-Lenzin et al. [35] | CG | 17 | 87 ± 2 | 83 ± 2 | −4.6 |
| Krustrup et al. [36] | CG | 10 | 96 ± 6 | 94 ± 5 | −2.1 |
| Krustrup et al. [37] | CG | 12 | 83 ± 5 | 87 ± 2 | 4.8 |
| Mohr et al. [38] | CG | 20 | 82 ± 3 | 81 ± 2 | −1.2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Clemente, F.M.; Ramirez-Campillo, R.; Sarmento, H. Effects of the Small-Sided Soccer Games on Blood Pressure in Untrained Hypertensive Adults: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Healthcare 2021, 9, 345. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare9030345
Clemente FM, Ramirez-Campillo R, Sarmento H. Effects of the Small-Sided Soccer Games on Blood Pressure in Untrained Hypertensive Adults: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Healthcare. 2021; 9(3):345. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare9030345
Chicago/Turabian StyleClemente, Filipe Manuel, Rodrigo Ramirez-Campillo, and Hugo Sarmento. 2021. "Effects of the Small-Sided Soccer Games on Blood Pressure in Untrained Hypertensive Adults: A Systematic Review and Meta-Analysis of Randomized Controlled Trials" Healthcare 9, no. 3: 345. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare9030345