Can Haglund’s Syndrome Be Misdiagnosed as Low Back Pain? Findings from a Case Report in Physical Therapy Direct Access

 , , ,
, , ,  ,
,  ,
,  and
and
Abstract
:1. Introduction
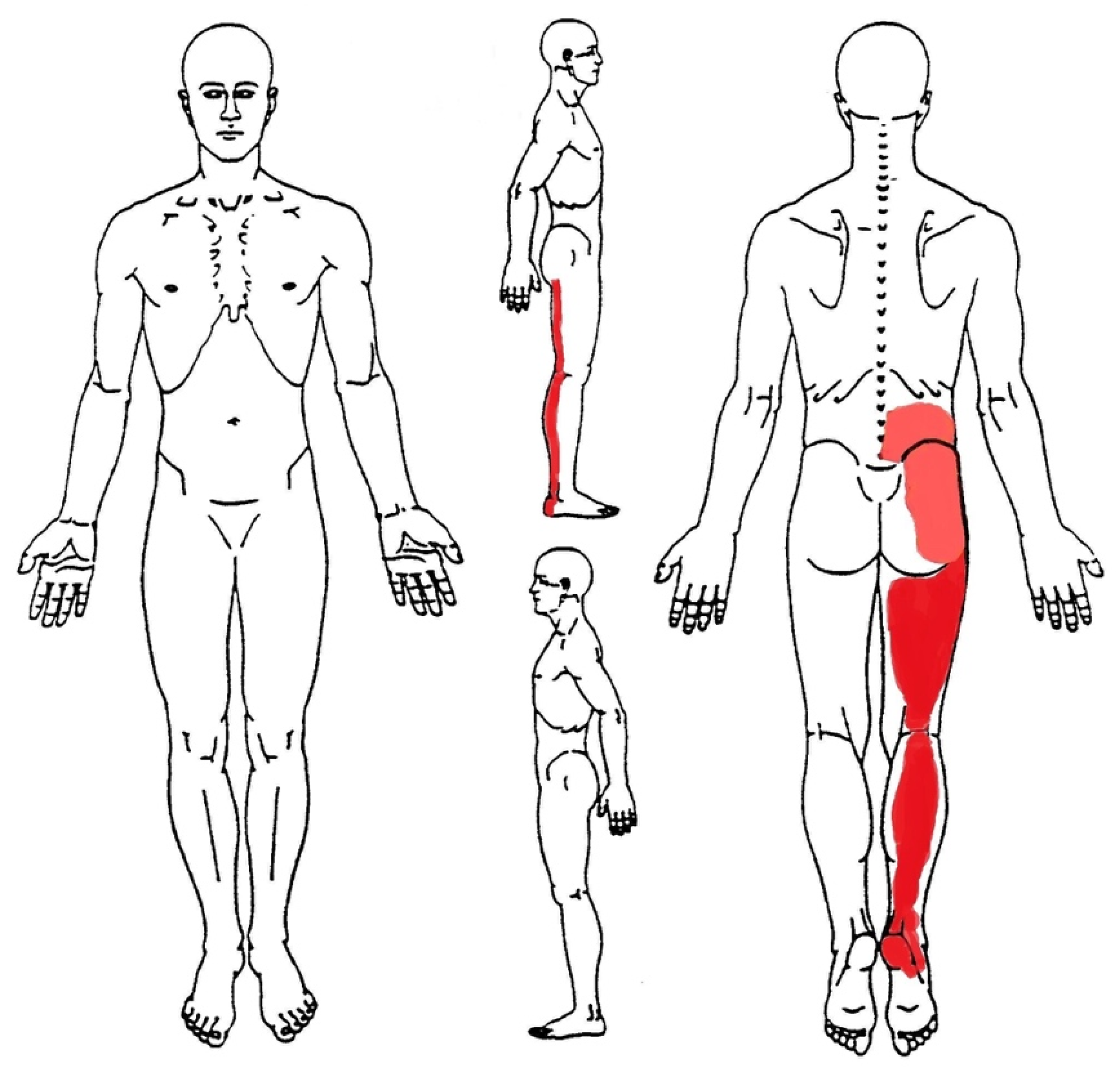
2. Case Presentation
3. Results
3.1. Differential Diagnosis
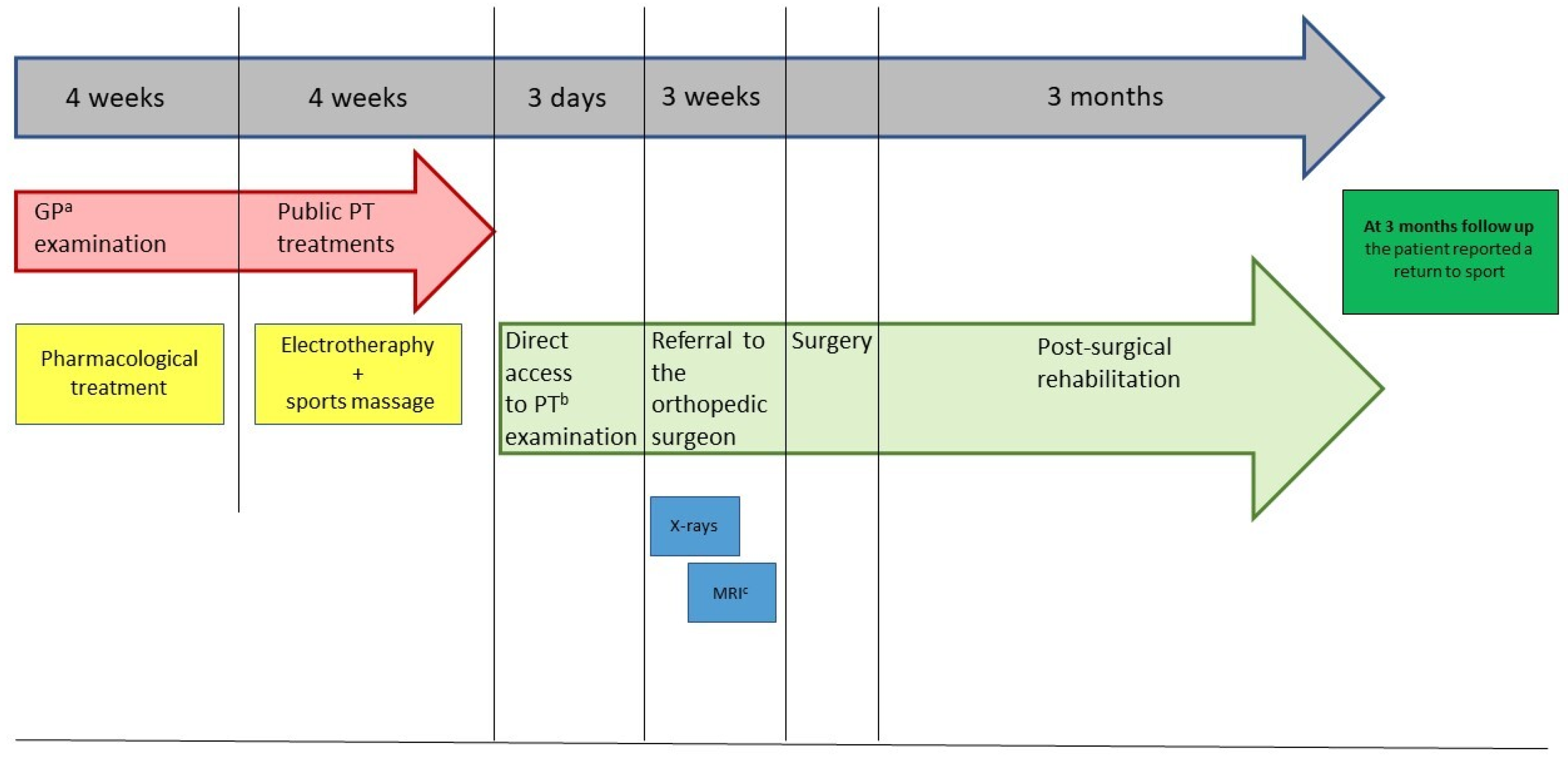
3.2. Treatment
3.3. Outcome and Follow-Up
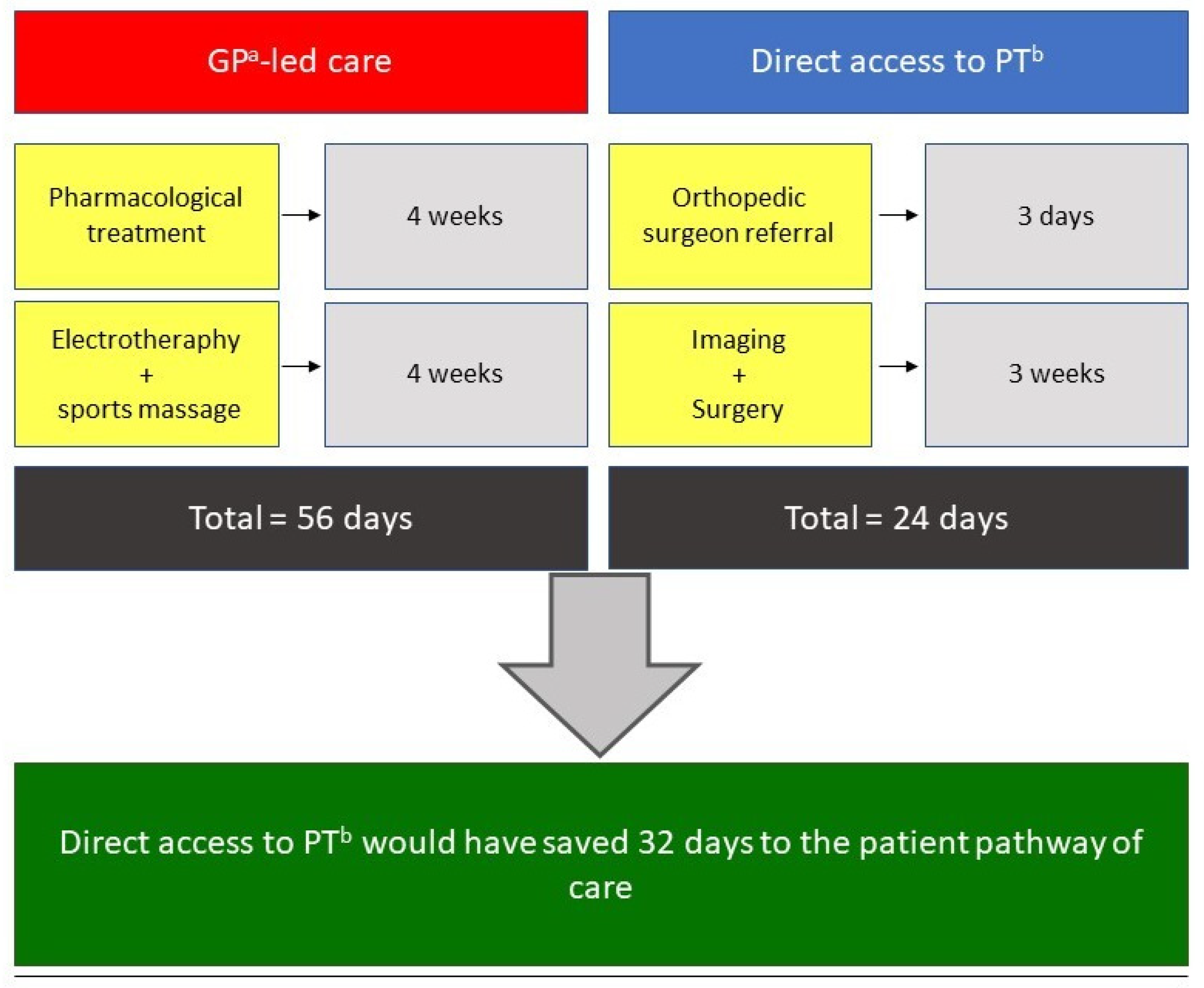
4. Discussion
5. Conclusions
Learning Points
- HS is a common MSK condition that every trained healthcare professional should be able to recognize and properly manage.
- DA to a PT is a safe, cost-effective and time-saving practice for patients with MSK disorders.
- A thorough physical examination within the differential diagnosis process is mandatory in case of patients with MSK disorders.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Oja, P.; Titze, S.; Kokko, S.; Kujala, U.M.; Heinonen, A.; Kelly, P.; Koski, P.; Foster, C. Health benefits of different sport disciplines for adults: Systematic review of observational and intervention studies with meta-analysis. Br. J. Sports Med. 2015, 49, 434–440. [Google Scholar] [CrossRef] [Green Version]
- Hespanhol Junior, L.C.; Pillay, J.D.; van Mechelen, W.; Verhagen, E. Meta-Analyses of the Effects of Habitual Running on Indices of Health in Physically Inactive Adults. Sports Med. 2015, 45, 1455–1468. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Belavý, D.L.; Albracht, K.; Bruggemann, G.P.; Vergroesen, P.P.A.; van Dieën, J.H. Can Exercise Positively Influence the Intervertebral Disc? Sports Med. 2016, 46, 473–485. [Google Scholar] [CrossRef] [PubMed]
- Maselli, F.; Storari, L.; Barbari, V.; Colombi, A.; Turolla, A.; Gianola, A.; Rossettini, G.; Testa, M. Prevalence and incidence of low back pain among runners: A systematic review. BMC Musculoskelet Disord. 2020, 21. [Google Scholar] [CrossRef]
- van der Worp, M.P.; ten Haaf, D.S.M.; van Cingel, R.; de Wijer, A.; Nijhuis-Van Der Sanden, M.W.G.; Bart Staal, J. Injuries in runners; a systematic review on risk factors and sex differences. PLoS ONE 2015, 10. [Google Scholar] [CrossRef] [PubMed]
- Vaishya, R.; Agarwal, A.K.; Azizi, A.T.; Vijay, V. Haglund’s Syndrome: A Commonly Seen Mysterious Condition. Cureus 2016, 8. [Google Scholar] [CrossRef] [Green Version]
- Barr, K.P.; Harrast, M.A. Evidence-based treatment of foot and ankle injuries in runners. Phys. Med. Rehabil. Clin. N. Am. 2005, 16, 779–799. [Google Scholar] [CrossRef]
- Thomas, J.L.; Christensen, J.C.; Kravitz, S.R.; Mendicino, R.W.; Schuberth, J.M.; Vanore, J.V.; Weil, L.S., Sr.; Zlotoff, H.J.; Bouchè, R.; Baker, J. The Diagnosis and Treatment of Heel Pain: A Clinical Practice Guideline-Revision 2010. J. Foot Ankle Surg. 2010, 49. [Google Scholar] [CrossRef]
- Kucuksen, S.; Karahan, A.Y.; Erol, K. Haglund syndrome with pump bump. Medicinski Arhiv. 2012, 66, 425–427. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Piscitelli, D.; Furmanek, M.P.; Meroni, R.; de Caro, W.; Pellicciari, L. Direct access in physical therapy: A systematic review. Clin. Ter. 2018, 169, e249–e260. [Google Scholar] [CrossRef]
- Babatunde, O.O.; Bishop, A.; Cottrell, E.; Jordan, J.L.; Corp, N.; Humpries, K.; Hadley-Barrows, T.; Huntley, A.L.; van der Windt, D.A. A systematic review and evidence synthesis of non-medical triage, self-referral and direct access services for patients with musculoskeletal pain. PLoS ONE 2020, 15. [Google Scholar] [CrossRef] [PubMed]
- Piano, L.; Maselli, F.; Viceconti, A.; Gianola, S.; Ciuro, A. Direct access to physical therapy for the patient with musculoskeletal disorders, a literature review. J. Phys. Ther Sci. 2017, 29, 1463–1471. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leemrijse, C.J.; Swinkels, I.C.; Veenhof, C. Direct access to physical therapy in the Netherlands: Results from the first year in community-based physical therapy. Phys. Ther. 2008, 88, 936–946. [Google Scholar] [CrossRef] [Green Version]
- Moore, J.H.; McMillian, D.J.; Rosenthal, M.D.; Weishaar, M.D. Risk determination for patients with direct access to physical therapy in military health care facilities. J. Orthop. Sports Phys. Ther. 2005, 35, 674–678. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Monteiro, D.P.; Britto, R.R.; de Freitas Fregonezi, G.A.; Dias, F.A.L.; da Silva, M.G.; Pereira, D.A.G. Reference values for the bilateral heel-rise test. Braz J. Phys. Ther. 2017, 21, 344–349. [Google Scholar] [CrossRef] [PubMed]
- Hébert-Losier, K.; Wessman, C.; Alricsson, M.; Svantesson, U. Updated reliability and normative values for the standing heel-rise test in healthy adults. Physiotherapy 2017, 103, 446–452. [Google Scholar] [CrossRef] [PubMed]
- Robinson, J.M.; Cook, J.L.; Purdam, C.; Visentini, P.J.; Ross, J.; Mafulli, N.; Tauton, J.E.; Khan, K.M. The VISA-A questionnaire: A valid and reliable index of the clinical severity of Achilles tendinopathy. Br. J. Sports Med. 2001, 35, 335–341. [Google Scholar] [CrossRef]
- Agyekum, E.K.; Ma, K. Heel pain: A systematic review. Chin. J Traumatol. 2015, 18, 164–169. [Google Scholar] [CrossRef]
- Chimenti, R.L.; Cychosz, C.C.; Hall, M.M.; Phisitkul, P. Current Concepts Review Update: Insertional Achilles Tendinopathy. Foot Ankle Int. 2017, 38, 1160–1169. [Google Scholar] [CrossRef]
- di Chio, F.; Cecere, A.; Troiano, M.; Mardighian, A.; Parisi, S.; Guglielmi, G. Persistent Haglund’s disease after conventional treatments: The innovative role of radiotherapy. BJR Case Rep. 2016, 2, 20150272. [Google Scholar] [CrossRef]
- Sofka, C.M.; Adler, R.S.; Positano, R.; Pavlov, H.; Luchs, J.S. Haglund’s Syndrome: Diagnosis and Treatment Using Sonography. HSS J. 2006, 2, 27-9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jiménez Martín, F.; Alonso Valdazo, M.D.; Díaz Peña, G.; Fernández Leroy, J.; Hernández Herrero, D.; Díaz García, F. Haglund’s syndrome. Two case reports. Síndrome de Haglund. A propósito de 2 casos. Reumatol. Clin. 2017, 13, 37–38. [Google Scholar] [CrossRef]
- Childs, J.D.; Whitman, J.M.; Pugia, M.L.; Sizer, P.S.; Flynn, T.W.; Delitto, A. Knowledge in managing musculoskeletal conditions and educational preparation of physical therapists in the uniformed services. Mil. Med. 2007, 172, 440–445. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mitchell, J.M.; de Lissovoy, G. A comparison of resource use and cost in direct access versus physician referral episodes of physical therapy. Phys Ther. 1997, 77, 10–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Demont, A.; Quentin, J.; Bourmaud, A. Impact of models of care integrating direct access to physiotherapy in primary care and emergency care contexts in patients with musculoskeletal disorders: A narrative review. Rev. Epidemiol. Sante Publique 2020, 68, 306–313. [Google Scholar] [CrossRef] [PubMed]
- Vos, T.; Barber, R.M.; Bell, B.; Bertolozzi-Villa, A.; Biryukov, S.; Bolliger, I.; Charlson, F.; Davis, A.; Degenhardt, L.; Dicker, D.; et al. Global, regional, and national incidence, prevalence, and years lived with disability for 301 acute and chronic diseases and injuries in 188 countries, 1990-2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet 2015, 386, 743–800. [Google Scholar] [CrossRef] [Green Version]
- Garrity, B.M.; McDonough, C.M.; Ameli, O.; Rothendler, J.A.; Carey, K.M.; Cabral, H.J.; Stein, M.D.; Saper, R.B.; Kazis, L.E. Unrestricted Direct Access to Physical Therapist Services Is Associated With Lower Health Care Utilization and Costs in Patients With New-Onset Low Back Pain. Phys. Ther. 2020, 100, 107–115. [Google Scholar] [CrossRef]
- Ojha, H.A.; Snyder, R.S.; Davenport, T.E. Direct access compared with referred physical therapy episodes of care: A systematic review. Phys. Ther. 2014, 94, 14–30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hon, S.; Ritter, R.; Allen, D.D. Cost-Effectiveness and Outcomes of Direct Access to Physical Therapy for Musculoskeletal Disorders Compared to Physician-First Access in the United States: Systematic Review and Meta-Analysis. Phys. Ther. 2021, 101. [Google Scholar] [CrossRef] [PubMed]
- Storari, L.; Barbari, V.; Brindisino, F.; Testa, M.; Filippo, M. An unusual presentation of acute myocardial infarction in physiotherapy direct access: Findings from a case report. Arch. Physiother. 2021, 11, 5. [Google Scholar] [CrossRef] [PubMed]
- Green, C.E.; Pastore, A.; Cronley, L.; Walker, M.D.; Thigpen, C.A.; Cook, C.E.; Givens, D.L. Explanatory multivariate modeling for disability, pain, and claims in patients with spine pain via a physical therapy direct access model of care. Back Musculoskelet Rehabil. 2019, 32, 769–777. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lystad, R.P.; Brown, B.T.; Swain, M.S.; Engel, R.M. Service utilisation trends in the manual therapy professions within the Australian private healthcare setting between 2008 and 2017. Chiropr. Man. Therap. 2020, 28, 49. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Before Surgery | Two-Month Follow-Up | Three-Month Follow-Up |
|---|---|---|
| NPRS: 7/10 at right heel, 6/10 from the heel to the calf, 2/10 in the lower back. | NPRS: 3/10 at right heel, 4/10 from the heel to the calf, 0/10 in the lower back. | NPRS: 0/10 throughout the body. |
| Bilateral heel rise tests were painful (NPRS 5/10) after 20 repetitions | --- | Bilateral heel rise test: 69 repetitions |
| Single heel rise was extremely painful and suspended after 2 repetitions (NPRS 9/10) | --- | Single heel rise test: 29 repetitions |
| VISA-A questionnaire: 45/100 points | --- | VISA-A questionnaire: 95/100 points |
| --- | Rearfoot strike pattern | Midfoot-strike pattern |
| --- | Running pace was on average 6.5 min/km | Running pace was on average 5 min/km |
| --- | Running cadence: 167 steps per minute | Running cadence: 181 steps per minute |
| --- | Ground contact time: 277 ms | Ground contact time: 252 ms |
| --- | Vertical oscillation: 8 cm | Vertical oscillation: 7 cm |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maselli, F.; Storari, L.; Barbari, V.; Rossettini, G.; Mourad, F.; Salomon, M.; Bisconti, M.; Brindisino, F.; Testa, M. Can Haglund’s Syndrome Be Misdiagnosed as Low Back Pain? Findings from a Case Report in Physical Therapy Direct Access. Healthcare 2021, 9, 508. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare9050508
Maselli F, Storari L, Barbari V, Rossettini G, Mourad F, Salomon M, Bisconti M, Brindisino F, Testa M. Can Haglund’s Syndrome Be Misdiagnosed as Low Back Pain? Findings from a Case Report in Physical Therapy Direct Access. Healthcare. 2021; 9(5):508. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare9050508
Chicago/Turabian StyleMaselli, Filippo, Lorenzo Storari, Valerio Barbari, Giacomo Rossettini, Firas Mourad, Mattia Salomon, Mattia Bisconti, Fabrizio Brindisino, and Marco Testa. 2021. "Can Haglund’s Syndrome Be Misdiagnosed as Low Back Pain? Findings from a Case Report in Physical Therapy Direct Access" Healthcare 9, no. 5: 508. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare9050508