
Impact of Three Strengthening Exercises on Dynamic Knee Valgus and Balance with Poor Knee Control among Young Football Players: A Randomized Controlled Trial


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
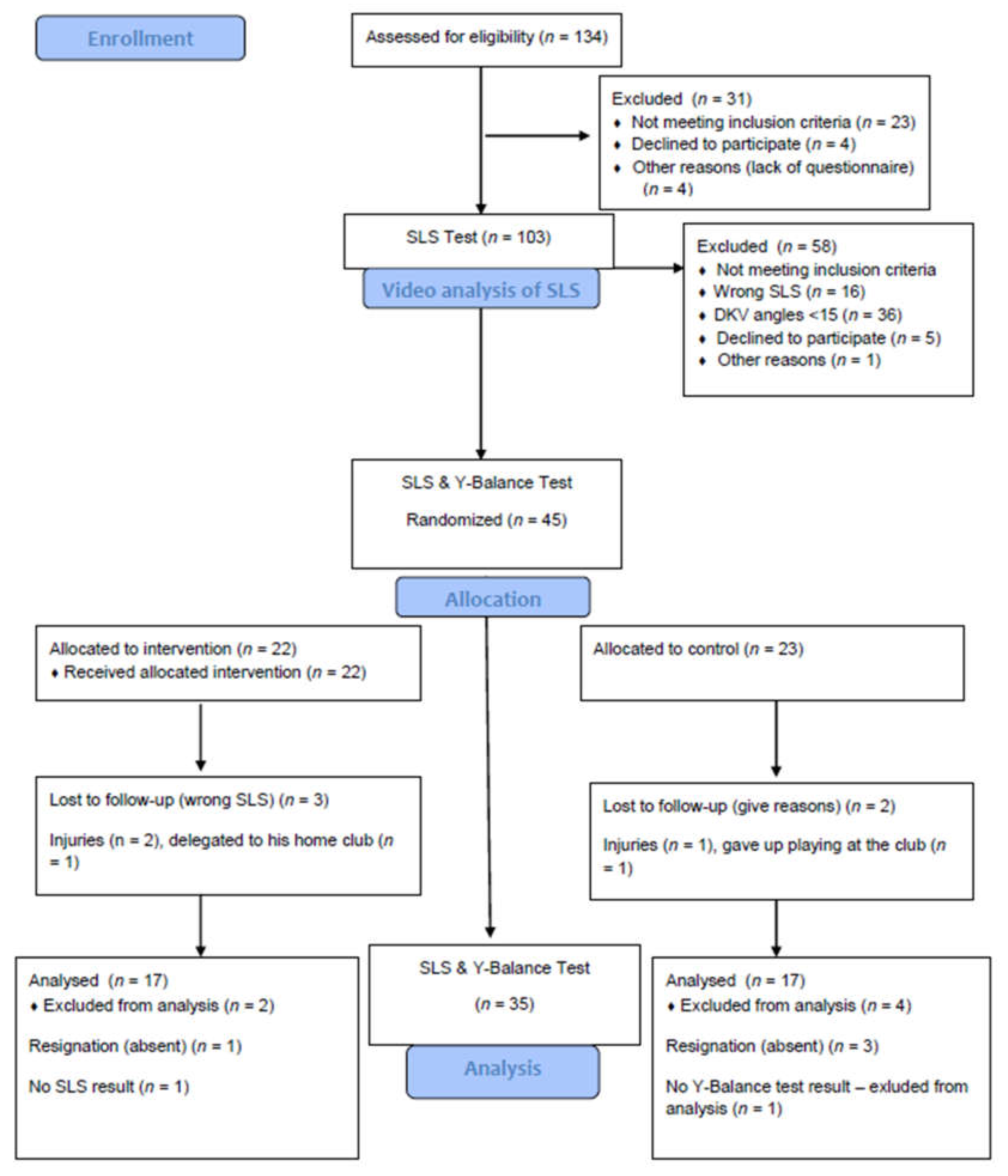
2.2. Study Design
2.3. The Tests and Exercise Supervision among Young Football Players
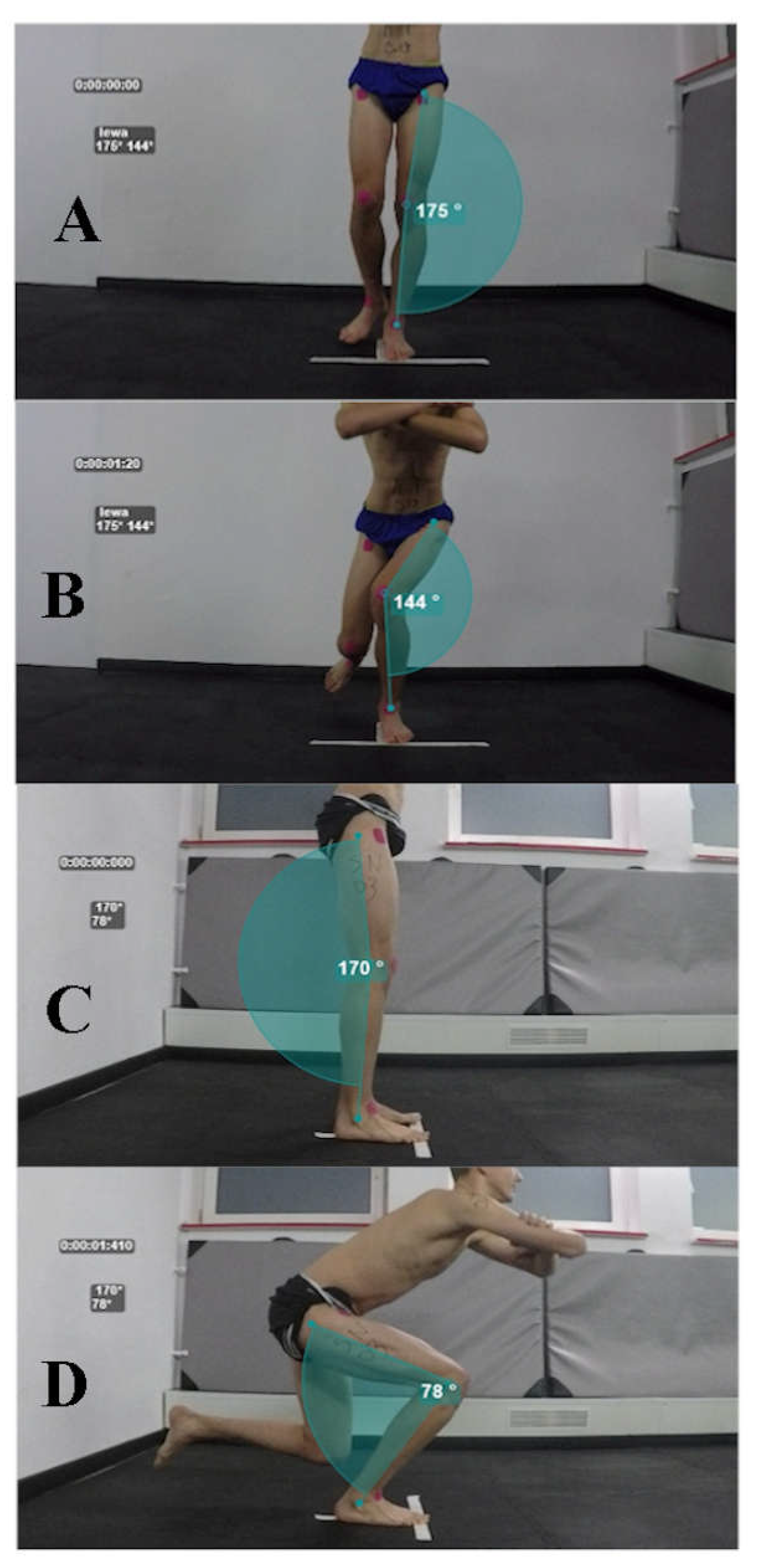
2.3.1. Single Leg Squat
2.3.2. Frontal Plane Projection Angle
2.3.3. Y-Balance Test
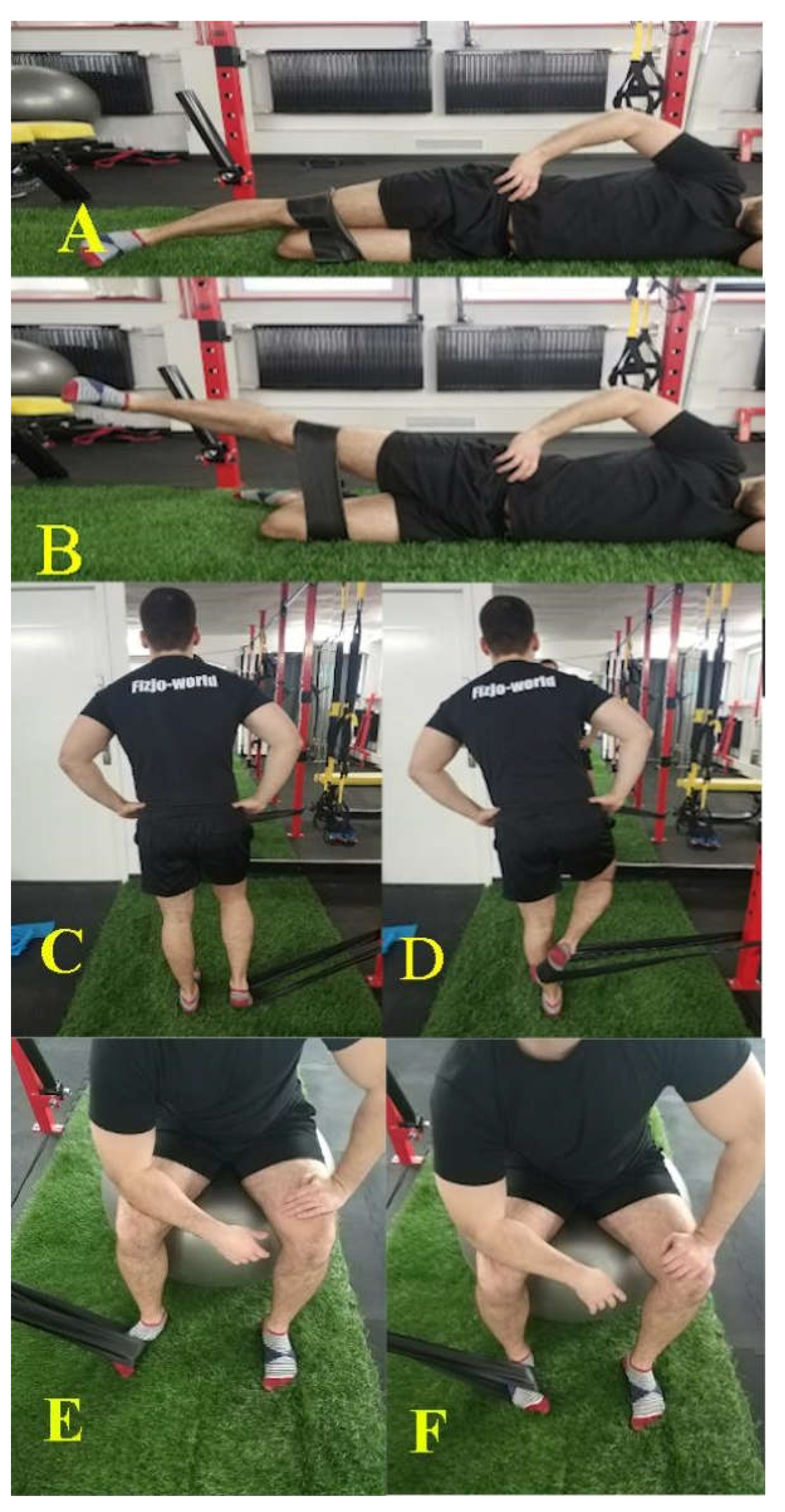
2.4. Exercise Program
2.5. Statistical Methods
3. Results
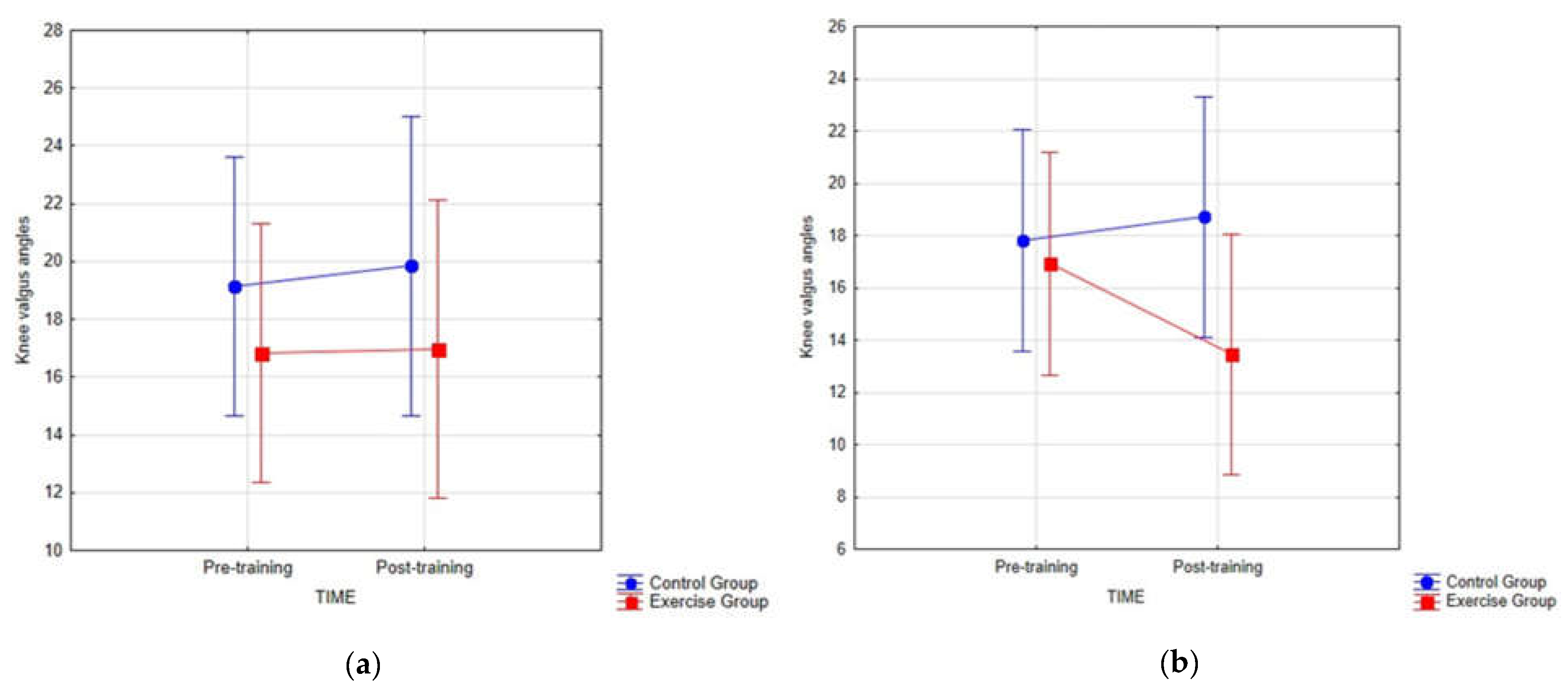
3.1. Primary Outcome
3.2. Secondary Outcome
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- More than Half the World Watched Record-Breaking 2018 World Cup Portal. Available online: https://www.fifa.com/worldcup/news/more-than-half-the-world-watched-record-breaking-2018-world-cup (accessed on 16 March 2021).
- Milanović, Z.; Pantelić, S.; Čović, N.; Sporiš, G.; Krustrup, P. Is Recreational Soccer Effective for Improving V˙O2max? Sports Med. (Auckl. N.Z.) 2015, 45, 1339–1353. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blatter, J.S.; Dvorak, J. Football for health—Science proves that playing football on a regular basis contributes to the improvement of public health. Scand. J. Med. Sci. Sports 2014, 24 (Suppl. S1), 2–3. [Google Scholar] [CrossRef]
- Merkel, D.L. Youth sport: Positive and negative impact on young athletes. Open Access J. Sports Med. 2013, 4, 151–160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Faude, O.; Rößler, R.; Junge, A. Football injuries in children and adolescent players: Are there clues for prevention? Sports Med. (Auckl. N.Z.) 2013, 43, 819–837. [Google Scholar] [CrossRef]
- Ekstrand, J.; Hägglund, M.; Waldén, M. Epidemiology of muscle injuries in professional football (soccer). Am. J. Sports Med. 2011, 39, 1226–1232. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Read, P.; Oliver, J.L.; Ste Croix, M.B.A.; de Myer, G.D.; Lloyd, R.S. Injury risk factors in male youth soccer players. Strength Cond. J. 2015, 37, 1–7. [Google Scholar] [CrossRef]
- Gomes Neto, M.; Conceição, C.S.; de Lima Brasileiro, A.J.A.; de Sousa, C.S.; Carvalho, V.O.; de Jesus, F.L.A. Effects of the FIFA 11 training program on injury prevention and performance in football players: A systematic review and meta-analysis. Clin. Rehabil. 2017, 31, 651–659. [Google Scholar] [CrossRef]
- Bizzini, M.; Dvorak, J. FIFA 11+: An effective programme to prevent football injuries in various player groups worldwide-a narrative review. Br. J. Sports Med. 2015, 49, 577–579. [Google Scholar] [CrossRef]
- Rodríguez, C.; Echegoyen, S.; Aoyama, T. The effects of “Prevent Injury and Enhance Performance Program” in a female soccer team. J. Sports Med. Phys. Fit. 2018, 58, 659–663. [Google Scholar] [CrossRef]
- Beck, N.A.; Lawrence, J.T.R.; Nordin, J.D.; DeFor, T.A.; Tompkins, M. ACL Tears in school-aged children and adolescents over 20 years. Pediatrics 2017, 139, e20161877. [Google Scholar] [CrossRef] [Green Version]
- Werner, B.C.; Yang, S.; Looney, A.M.; Gwathmey, F.W., Jr. Trends in pediatric and adolescent anterior cruciate ligament injury and reconstruction. J. Pediatr. Orthop. 2016, 36, 447–452. [Google Scholar] [CrossRef]
- Hewett, T.E.; Myer, G.D.; Ford, K.R. Reducing knee and anterior cruciate ligament injuries among female athletes: A systematic review of neuromuscular training interventions. J. Knee Surg. 2005, 18, 82–88. [Google Scholar] [CrossRef] [PubMed]
- Wilczyński, B.; Zorena, K.; Ślęzak, D. Dynamic knee valgus in single-leg movement tasks. Potentially modifiable factors and exercise training options. A literature review. Int. J. Environ. Res. Public Health 2020, 17, 8208. [Google Scholar] [CrossRef]
- Hewett, T.E.; Torg, J.S.; Boden, B.P. Video analysis of trunk and knee motion during non-contact anterior cruciate ligament injury in female athletes: Lateral trunk and knee abduction motion are combined components of the injury mechanism. Br. J. Sports Med. 2009, 43, 417–422. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barber-Westin, S.D.; Noyes, F.R. Effect of fatigue protocols on lower limb neuromuscular function and implications for anterior cruciate ligament injury prevention training: A systematic review. Am. J. Sports Med. 2017, 45, 3388–3396. [Google Scholar] [CrossRef] [PubMed]
- Souza, R.B.; Powers, C.M. Differences in hip kinematics, muscle strength, and muscle activation between subjects with and without patellofemoral pain. J. Orthop. Sports Phys. Ther. 2009, 39, 12–19. [Google Scholar] [CrossRef] [PubMed]
- Waldén, M.; Krosshaug, T.; Bjørneboe, J.; Andersen, T.E.; Faul, O.; Hägglund, M. Three distinct mechanisms predominate in non-contact anterior cruciate ligament injuries in male professional football players: A systematic video analysis of 39 cases. Br. J. Sports Med. 2015, 49, 1452–1460. [Google Scholar] [CrossRef] [Green Version]
- Grassi, A.; Smiley, S.P.; Di Roberti Sarsina, T.; Signorelli, C.; Marcheggiani Muccioli, G.M.; Bondi, A.; Romagnoli, M.; Agostini, A.; Zaffagnini, S. Mechanisms and situations of anterior cruciate ligament injuries in professional male soccer players: A YouTube-based video analysis. Eur. J. Orthop. Surg. Traumatol. 2017, 27, 967–981. [Google Scholar] [CrossRef] [PubMed]
- Petersen, W.; Rembitzki, I.; Liebau, C. Patellofemoral pain in athletes. Open Access J. Sports Med. 2017, 8, 143–154. [Google Scholar] [CrossRef] [Green Version]
- Räisänen, A.M.; Pasanen, K.; Krosshaug, T.; Vasankari, T.; Kannus, P.; Heinonen, A. Association between frontal plane knee control and lower extremity injuries: A prospective study on young team sport athletes. BMJ Open Sport Exerc. Med. 2018, 4, e000311. [Google Scholar] [CrossRef]
- Schurr, S.A.; Marshall, A.N.; Resch, J.E.; Saliba, S.A. Two-dimensional video analysis is comparable to 3d motion capture in lower extremity movement assessment. Int. J. Sports Phys. Ther. 2017, 12, 163–172. [Google Scholar]
- Werner, D.M.; Di Stasi, S.; Lewis, C.L.; Barrios, J.A. Test-retest reliability and minimum detectable change for various frontal plane projection angles during dynamic tasks. Phys. Ther. Sport. 2019, 40, 169–176. [Google Scholar] [CrossRef] [PubMed]
- Gwynne, C.R.; Curran, S.A. Quantifying frontal plane knee motion during single limb squats: Reliability and validity of 2-dimensional measures. Int. J. Sports Phys. Ther. 2014, 9, 898–906. [Google Scholar] [PubMed]
- Nilstad, A.; Krosshaug, T.; Mok, K.M.; Bahr, R.; Andersen, T.E. Association between anatomical characteristics, knee laxity, muscle strength, and peak knee valgus during vertical drop-jump landings. J. Orthop. Sports Phys. Ther. 2015, 45, 998–1005. [Google Scholar] [CrossRef]
- Hartley, E.M.; Hoch, M.C.; Boling, M.C. Y-balance test performance and BMI are associated with ankle sprain injury in collegiate male athletes. J. Sci. Med. Sport. 2018, 21, 676–680. [Google Scholar] [CrossRef]
- Smith, C.A.; Chimera, N.J.; Warren, M. Association of y balance test reach asymmetry and injury in division I athletes. Med. Sci. Sports Exerc. 2015, 47, 136–141. [Google Scholar] [CrossRef] [PubMed]
- Booysen, M.J.; Gradidge, P.J.; Watson, E. The relationships of eccentric strength and power with dynamic balance in male footballers. J. Sports Sci. 2015, 33, 2157–2165. [Google Scholar] [CrossRef] [PubMed]
- Dawson, S.J.; Herrington, L. Improving single-legged–squat performance: Comparing 2 training methods with potential implications for injury prevention. J. Athl. Train. 2015, 50, 921–929. [Google Scholar] [CrossRef] [Green Version]
- Sasaki, S.; Tsuda, E.; Yamamoto, Y.; Maeda, S.; Kimura, Y.; Fujita, Y.; Ishibashi, Y. Core-muscle training and neuromuscular control of the lower limb and trunk. J. Athl. Train. 2019, 54, 959–969. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hopper, A.J.; Haff, E.E.; Joyce, C.; Lloyd, R.S.; Haff, G.G. Neuromuscular training improves lower extremity biomechanics associated with knee injury during landing in 11–13 year old female netball athletes: A randomized control study. Front. Physiol. 2017, 8, 883. [Google Scholar] [CrossRef]
- Marshall, A.N.; Hertel, J.; Hart, J.M.; Russell, S.; Saliba, S.A. Visual biofeedback and changes in lower extremity kinematics in individuals with medial knee displacement. J. Athl. Train. 2020, 55, 255–264. [Google Scholar] [CrossRef] [Green Version]
- Attwood, M.J.; Roberts, S.P.; Trewartha, G.; England, M.E.; Stokes, K.A. Efficacy of a movement control injury prevention programme in adult men’s community rugby union: A cluster randomised controlled trial. Br. J. Sports Med. 2018, 52, 368–374. [Google Scholar] [CrossRef]
- Bell, D.R.; Oates, D.C.; Clark, M.A.; Padua, D.A. Two- and 3-dimensional knee valgus are reduced after an exercise intervention in young adults with demonstrable valgus during squatting. J. Athl. Train. 2013, 48, 442–449. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mauntel, T.C.; Begalle, R.L.; Cram, T.R.; Frank, B.S.; Hirth, C.J.; Blackburn, T.; Padua, D.A. The effects of lower extremity muscle activation and passive range of motion on single leg squat performance. J. Strength Cond. Res. 2013, 27, 1813–1823. [Google Scholar] [CrossRef] [Green Version]
- Wyndow, N.; De Jong, A.; Rial, K.; Tucker, K.; Collins, N.; Vicenzino, B.; Russell, T.; Crossley, K. The relationship of foot and ankle mobility to the frontal plane projection angle in asymptomatic adults. J. Foot Ankle Res. 2016, 9, 3. [Google Scholar] [CrossRef] [Green Version]
- Neamatallah, Z.; Herrington, L.; Jones, R. An investigation into the role of gluteal muscle strength and EMG activity in controlling HIP and knee motion during landing tasks. Phys. Ther. Sport 2020, 43, 230–235. [Google Scholar] [CrossRef] [PubMed]
- Ford, K.R.; Nguyen, A.-D.; Dischiavi, S.L.; Hegedus, E.J.; Zuk, E.F.; Taylor, J.B. An evidence-based review of hip-focused neuromuscular exercise interventions to address dynamic lower extremity valgus. Open Access J. Sports Med. 2015, 6, 291–303. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reiman, M.P.; Bolgla, L.A.; Loudon, J.K. A literature review of studies evaluating gluteus maximus and gluteus medius activation during rehabilitation exercises. Physiother. Theory Pract. 2012, 28, 257–268. [Google Scholar] [CrossRef] [PubMed]
- Kulig, K.; Burnfield, J.M.; Requejo, S.M.; Sperry, M.; Terk, M. Selective Activation of Tibialis Posterior: Evaluation by Magnetic Resonance Imaging. Med. Sci. Sports Exerc. 2004, 36, 862–867. [Google Scholar] [CrossRef]
- Nyland, J.; Lachman, N.; Kocabey, Y.; Brosky, J.; Altun, R.; Caborn, D. Anatomy, function, and rehabilitation of the popliteus musculotendinous complex. J. Orthop. Sports Phys Ther. 2005, 35, 165–179. [Google Scholar] [CrossRef] [Green Version]
- Soda, N.; Fujihashi, Y.; Aoki, T. In vivo ultrasound imaging of the popliteus muscle: Investigation of functional characteristics. J. Phys. Ther. Sci. 2016, 28, 979–982. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McLean, S.; Walker, K.; Ford, K.; Myer, G.; Hewett, T.; van den Bogert, A.J. Evaluation of a two dimensional analysis method as a screening and evaluation tool for anterior cruciate ligament injury. Br. J. Sports Med. 2005, 39, 355–362. [Google Scholar] [CrossRef] [Green Version]
- Räisänen, A.M.H.S.; Pasanen, K.; Krosshaug, T.; Avela, J.; Perttunen, J.; Parkkari, J. Single-Leg Squat as a Tool to Evaluate Young Athletes’ Frontal Plane Knee Control. Clin. J. Sport Med. 2016, 26, 478–482. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schulz, K.F.; Altman, D.G.; Moher, D.; CONSORT Group. CONSORT 2010 statement: Updated guidelines for reporting parallel group randomised trials. BMJ 2010, 340, c332. [Google Scholar] [CrossRef] [PubMed]
- Willson, J.D.; Davis, I.S. Utility of the frontal plane projection angle in females with patellofemoral pain. J. Orthop. Sports Phys. Ther. 2008, 38, 606–615. [Google Scholar] [CrossRef]
- Willson, J.D.; Ireland, M.L.; Davis, I. Core strength and lower extremity alignment during single leg squats. Med. Sci. Sports Exerc. 2006, 38, 945–952. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Balsalobre-Fernández, C.; Tejero-González, C.M.; del Campo-Vecino, J.; Bavaresco, N. The concurrent validity and reliability of a low-cost, high-speed camera-based method for measuring the flight time of vertical jumps. J. Strength Cond. Res. 2014, 28, 528–533. [Google Scholar] [CrossRef]
- Puig-Diví, A.; Escalona-Marfil, C.; Padullés-Riu, J.M.; Busquets, A.; Padullés-Chando, X.; Marcos-Ruiz, D. Validity and reliability of the Kinovea program in obtaining angles and distances using coordinates in 4 perspectives. PLoS ONE 2019, 14, e0216448. [Google Scholar] [CrossRef]
- Hébert-Losier, K. Clinical Implications of Hand Position and Lower Limb Length Measurement Method on Y-Balance Test Scores and Interpretations. J. Athl. Train. 2017, 52, 910–917. [Google Scholar] [CrossRef] [Green Version]
- Shaffer, S.W.; Teyhen, D.S.; Lorenson, C.L.; Warren, R.L.; Koreerat, C.M.; Straseske, C.A.; Childs, J.D. Y-balance test: A reliability study involving multiple raters. Mil. Med. 2013, 178, 1264–1270. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pomares-Noguera, C.; Ayala, F.; Robles-Palazón, F.J.; Alomoto-Burneo, J.F.; López-Valenciano, A.; Elvira, J.L.L.; Hernández-Sánchez, S.; De Ste Croix, M. Training Effects of the FIFA 11+ Kids on Physical Performance in Youth Football Players: A Randomized Control Trial. Front. Pediatr. 2018, 6, 40. [Google Scholar] [CrossRef] [Green Version]
- Plisky, P.J.; Gorman, P.P.; Butler, R.J.; Kiesel, K.B.; Underwood, F.B.; Elkins, B. The Reliability of an Instrumented Device for Measuring Components of the Star Excursion Balance Test. N Am. J. Sports Phys Ther. 2009, 4, 92–99. [Google Scholar] [PubMed]
- Ortqvist, M.; Moström, E.B.; Roos, E.M.; Lundell, P.; Janarv, P.-M.; Werner, S.; Broström, E.W. Reliability and reference values of two clinical measurements of dynamic and static knee position in healthy children. Knee Surg. Sports Traumatol. Arthrosc. 2011, 19, 2060–2066. [Google Scholar] [CrossRef] [PubMed]
- Clark, M.A.; Lucett, S.C.; Sutton, B.G. NASM Essentials of Corrective Exervise Training; Jones & Bartlett Learning: Burlington, MA, USA, 2014. [Google Scholar]
- Powden, C.J.; Dodds, T.K.; Gabriel, E.H. The reliability of the star excursion balance test and lower quarter y-balance test in healthy adults: A systematic review. Int. J. Sports Phys. Ther. 2019, 14, 683–694. [Google Scholar] [CrossRef]
- Filipa, A.; Byrnes, R.; Paterno, M.V.; Myer, G.D.; Hewett, T.E. Neuromuscular Training Improves Performance on the Star Excursion Balance Test in Young Female Athletes. J. Orthop. Sports Phys. Ther. 2010, 40, 551–558. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Imai, A.; Kaneoka, K.; Okubo, Y.; Shiraki, H. Effects of two types of trunk exercises on balance and athletic performance in youth soccer players. Int. J. Sports Phys. Ther. 2014, 9, 47–57. [Google Scholar]
- Palmer, K.; Hebron, C.; Williams, J.M. A randomised trial into the effect of an isolated hip abductor strengthening programme and a functional motor control programme on knee kinematics and hip muscle strength. BMC Musculoskelet. Disord. 2015, 16, 1–8. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Exercise | Starting Position | Exercise | Week 1 | Week 2–3 | Week 4–6 |
|---|---|---|---|---|---|
| Gluteus medius [39] | Side-lying, free leg flexed 90° in the knee joint, exercised leg straightened. The hand on the side of the exercised leg lies on the hip. Band tied over the patella. | Hip abduction to an angle of about 30° in the hip joint. | 2 sets 10 reps | 3 sets 10 reps | 3 sets 15 reps |
| Popliteus [41] | Standing on one leg. Hands resting on the hips. Band applied to the forefoot. | Flexion movement in the knee joint with simultaneous external rotation of the thigh and internal rotation of the tibia. | |||
| Tibialis posterior [40] | Sitting position with knees flexed approximately at 90°, the forearm on the side of the exercised leg based on the knee. The heel is in contact with the ground. Band hooked at the forefoot. | Resisted foot adduction and internal rotation of the tibia without femur movement. |
| Characteristics | Exercise Group (n = 22) | Control Group (n = 23) | p-Value |
|---|---|---|---|
| Age, median (IQR), years | 13 (12–15) | 13 (12–15) | 0.847 † |
| Height, mean (SD) centimeters | 157 (10) | 158 (14) | 0.877 ‡ |
| Weight, mean (SD) kilograms | 45 (10) | 45 (12) | 0.943 ‡ |
| BMI, median (IQR) kg/m2 | 17 (16–19) | 18 (16–19) | 0.883 † |
| Skeletal muscle mass, median (IQR) kilograms | 19 (17–23) | 18 (17–28) | 0.892 † |
| Physical Performance Measure (°) | Exercise | Control | Between Groups | p-Value | d Cohen’s | |
|---|---|---|---|---|---|---|
| Dynamic valgus left—mean, (SD) | Pre | 16.07 (8.75) | 18.03 (7.53) | 1.95 | 0.426 | 0.24 |
| Post | 13.45 (6.60) | 18.70 (11.36) | 5.25 | 0.108 | 0.57 | |
| Post-Pre | −2.63 | 0.68 | ||||
| Dynamic valgus right—mean, (SD) | Pre | 16.33 (10.28) | 18.48 (9.41) | 2.14 | 0.469 | 0.22 |
| Post | 16.96 (11.12) | 19.84 (9.73) | 2.88 | 0.427 | 0.27 | |
| Post-Pre | 0.63 | 1.37 |
| Y-Balance Test (LL%) | Exercise Group | Within-Group p-Value | Control Group | Within-Group p-Value | Between-Groups p-Value | d Cohen’s | ||
|---|---|---|---|---|---|---|---|---|
| Pre | Post | Pre | Post | Post | ||||
| ANTERIOR right—median, (IQR) | 69.1 (8.1) | 73.6 (8.3) | 0.038 * | 70.5 (7.0) | 70.3 (9.1) | 0.687 | 0.215 | 0.44 |
| ANTERIOR left—median, (IQR) | 68.3 (7.2) | 71.9 (7.3) | 0.039 * | 72.3 (5.5) | 72.1 (7.7) | 0.831 | 0.757 | 0.11 |
| POSTEROLATERAL right—median, (IQR) | 106.3 (7.8) | 112.9 (4.7) | 0.055 | 105.6 (8.0) | 107.5 (8.2) | 0.381 | 0.054 | 0.71 |
| POSTEROLATERAL left—mean (SD) | 108.3 (8.8) | 111.6 (6.8) | 0.208 | 108.0 (8.1) | 109.3 (6.6) | 0.583 | 0.286 | 0.34 |
| POSTEROMEDIAL right—median (IQR) | 104.3 (12.3) | 110.0 (11.3) | 0.006 * | 105.5 (11.1) | 108.01 (7.9) | 0.831 | 0.352 | 0.33 |
| POSTEROMEDIAL left—mean (SD) | 105.0 (9.0) | 107.2 (6.2) | 0.394 | 108.0 (11.4) | 107.8 (6.5) | 0.959 | 0.654 | 0.09 |
| COMPOSITE RIGHT—median (IQR) | 92.2 (5.9) | 97.9 (6.3) | 0.015 * | 93.8 (7.3) | 95.1 (5.3) | 0.355 | 0.113 | 0.57 |
| COMPOSITE left—mean (SD) | 94.4 (7.19) | 96.8 (5.3) | 0.257 | 95.9 (7.0) | 96.0 (5.6) | 0.966 | 0.605 | 0.15 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wilczyński, B.; Wąż, P.; Zorena, K. Impact of Three Strengthening Exercises on Dynamic Knee Valgus and Balance with Poor Knee Control among Young Football Players: A Randomized Controlled Trial. Healthcare 2021, 9, 558. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare9050558
Wilczyński B, Wąż P, Zorena K. Impact of Three Strengthening Exercises on Dynamic Knee Valgus and Balance with Poor Knee Control among Young Football Players: A Randomized Controlled Trial. Healthcare. 2021; 9(5):558. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare9050558
Chicago/Turabian StyleWilczyński, Bartosz, Piotr Wąż, and Katarzyna Zorena. 2021. "Impact of Three Strengthening Exercises on Dynamic Knee Valgus and Balance with Poor Knee Control among Young Football Players: A Randomized Controlled Trial" Healthcare 9, no. 5: 558. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare9050558