
The Empathic Capacity and the Ability to Regulate It: Construction and Validation of the Empathy Management Scale (EMS)

 , and
, and 
Abstract
:1. Introduction
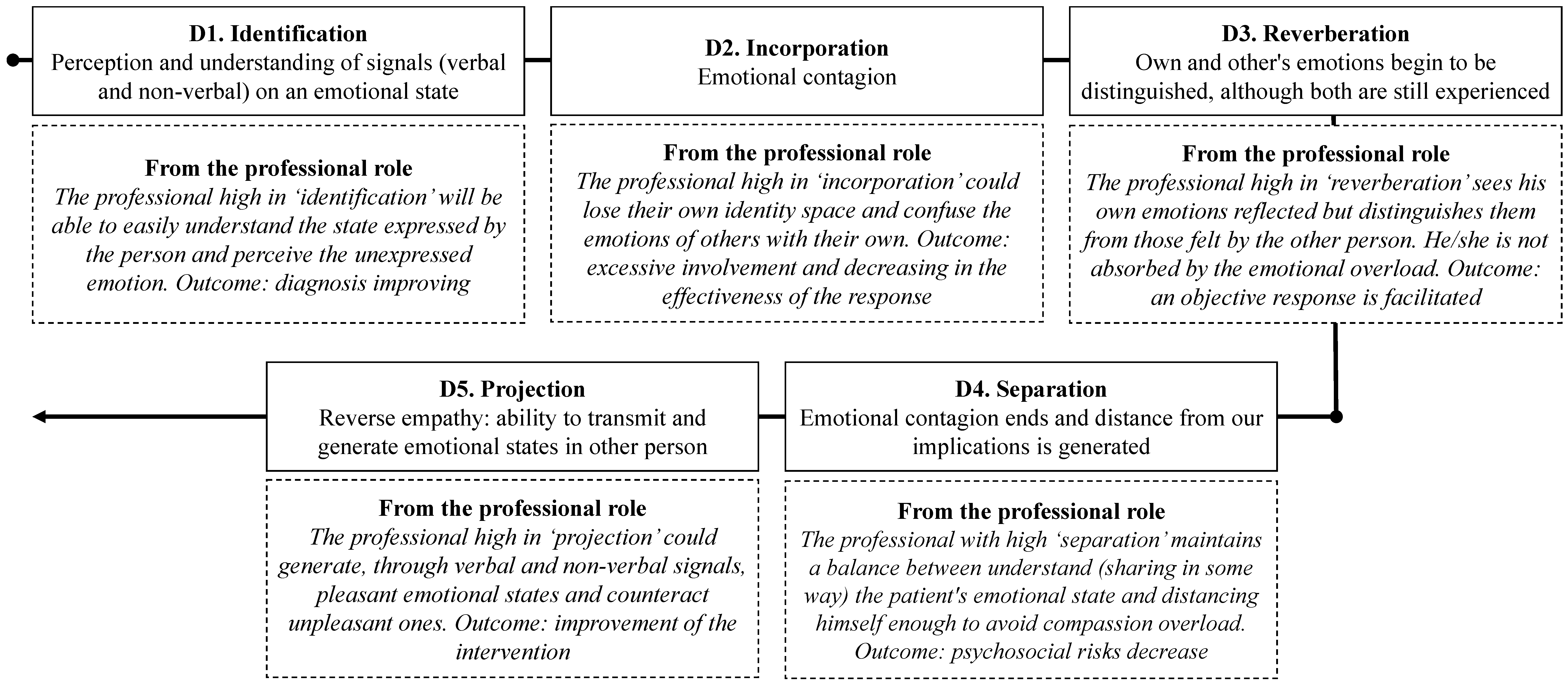
1.1. Overview of the Empathic Process
1.2. Empathy Assessment
1.3. Variables and Instruments Related to Empathy Management
2. Study 1
2.1. Materials and Methods
2.1.1. Participants
2.1.2. Development of Items for the Empathy Management Scale
2.1.3. Procedure
2.1.4. Statistical Analyses
2.2. Results
2.2.1. Construct Validity
2.2.2. Internal Consistency
3. Study 2
3.1. Method and Materials
3.1.1. Participants
3.1.2. Instruments
- EPE [38]. This scale comprises 31 items grouped into five subscales. Three scales were selected due to their relevance to our research goal. (a) Feelings: This subscale assesses the ability to detect others’ feelings, experience the same intensity and clarity of the emotions of others, and project emotions onto others (α = 0.79). (b) “Apata” characteristics: This subscale measures the difficulty to feel or experience others’ emotions (α = 0.79). (c) Separation and reverberation: This subscale concerns the influence of others’ emotions and the difficulty of empathic persons to separate themselves from these emotions (α = 0.69).
- Trait Meta-Mood Scale (TMMS-24) [47]; Spanish adaptation [11]. This scale measures individuals’ knowledge about their own emotional abilities (perceived EI). It comprises three dimensions: (a) emotional attention or the ability to feel and express emotions appropriately (α = 0.79), (b) emotional clarity or the ability to understand our own emotional states (α = 0.78), and (c) emotional repair or the ability to regulate our own emotional states appropriately (α = 0.86).
- Questions about sociodemographic variables were also included in the instrument (sex, age, and formal education).
3.1.3. Procedure
3.1.4. Statistical Analyses
3.2. Results
3.2.1. Construct Validity
3.2.2. Internal Consistency
3.2.3. Convergent Validity
3.2.4. Other Evidence of Construct Validity: Study of Sociodemographic Variables
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
| (1) Previamente a una situación difícil, empleo técnicas para afrontar las emociones que me esperan, como la relajación. | 1 | 2 | 3 | 4 | 5 |
| (2) Es difícil para mí darme cuenta de qué emociones negativas son mías y cuáles provienen de otra persona. | 1 | 2 | 3 | 4 | 5 |
| (3) Soy capaz de darme cuenta de si los sentimientos que experimento son míos o provienen de otra persona. | 1 | 2 | 3 | 4 | 5 |
| (4) Cuando sé que me voy a exponer a una situación emocionalmente negativa e intensa me preparo de alguna manera para distanciarme de esa situación. | 1 | 2 | 3 | 4 | 5 |
| (5) Cuando se trata de emociones positivas me doy cuenta con facilidad de cuáles me las ha contagiado otra persona y cuáles he generado yo. | 1 | 2 | 3 | 4 | 5 |
| (6) Aunque esté con otra persona que se siente mal, no me contagio de su emoción. | 1 | 2 | 3 | 4 | 5 |
| (7) Sé tranquilizar a las personas mediante mi contacto. | 1 | 2 | 3 | 4 | 5 |
| (8) Me contagio tan fácilmente de las emociones negativas de los demás que me afectan como si fueran mías. | 1 | 2 | 3 | 4 | 5 |
| (9) No suelo saber cómo se siente alguien por su comunicación no verbal. | 1 | 2 | 3 | 4 | 5 |
| (10) Cuando otra persona me explica cómo se siente, me resulta difícil entenderla. | 1 | 2 | 3 | 4 | 5 |
| (11) Cuando estoy con otra persona me doy cuenta de qué parte de lo que siento me está generando ella. | 1 | 2 | 3 | 4 | 5 |
| (12) Si alguien está triste, le contagio la alegría. | 1 | 2 | 3 | 4 | 5 |
| (13) Cuando estoy con otra persona que se siente mal termino sintiéndome igual de mal que ella. | 1 | 2 | 3 | 4 | 5 |
| (14) Me resulta difícil;cil generar emociones positivas en una situación difícil. | 1 | 2 | 3 | 4 | 5 |
| (15) Me cuesta trabajo entender cómo se siente otra persona. | 1 | 2 | 3 | 4 | 5 |
| (16) Cuando tengo cerca a una persona que está nerviosa, puedo no saber cómo lo hago, pero la tranquilizo. | 1 | 2 | 3 | 4 | 5 |
| (17) Evito situaciones que impliquen emociones negativas porque no sé cómo deshacerme de ellas. | 1 | 2 | 3 | 4 | 5 |
| (18) Sé cómo separar mis sentimientos de los de los demás. | 1 | 2 | 3 | 4 | 5 |
| 1 = totalmente en desacuerdo, 2 = en desacuerdo, 3 = ni en desacuerdo, ni de acuerdo, 4 = de acuerdo, 5 = totalmente de acuerdo | |||||
References
- Sansó, N.; Galiana, L.; González, B.; Sarmentero, J.; Reynes, M.; Oliver, A.; Garcia-Toro, M. Differential effects of two contemplative practice-based programs for health care professionals. Psicosoc. Interv. 2019, 28, 131–138. [Google Scholar] [CrossRef] [Green Version]
- Yuguero, O.; Melnick, E.R.; Marsal, J.R.; Esquerda, J.; Soler-González, J. Cross-sectional study of the association between healthcare professionals’ empathy and burnout and the number of annual primary care visits per patient under their care in Spain. BMJ Open 2018, 8, e020949. [Google Scholar] [CrossRef] [Green Version]
- McKinnon, J. In their shoes: An ontological perspective on empathy in nursing practice. J. Clin. Nurs. 2018, 27, 3882–3893. [Google Scholar] [CrossRef] [PubMed]
- Mahmoudian, A.; Zamani, A.; Tavakoli, N.; Farajzadegan, Z.; Fathollahi-Dehkordi, F. Medication adherence in patients with hypertension: Does satisfaction with doctor-patient relationship work? J. Res. Med. Sci. 2017, 22, 48. [Google Scholar] [CrossRef] [PubMed]
- Delgado, N.; Bonache, H.; Betancort, M.; Morera, Y.; Harris, L.T. Understanding the Links between Inferring Mental States, Empathy, and Burnout in Medical Contexts. Healthcare 2021, 9, 158. [Google Scholar] [CrossRef]
- Davis, M.H. Measuring individual differences in empathy: Evidence for a multidimensional approach. J. Pers. Soc. Psychol. 1983, 44, 113–126. [Google Scholar] [CrossRef]
- Decety, J. Empathy in medicine: What it is, and how much we really need it. Am. J. Med. 2020, 133, 561–566. [Google Scholar] [CrossRef]
- Hong, H.; Han, A. A systematic review on empathy measurement tools for care professionals. Educ. Gerontol. 2020, 46, 72–83. [Google Scholar] [CrossRef]
- Reik, T. Listening with the Third Ear; Grove Press: New York, NY, USA, 1948. [Google Scholar]
- Davis, M.H. A multidimensional approach to individual differences in empathy. Catal. Sel. Doc. Psychol. 1980, 10, 2–19. [Google Scholar]
- Fernández-Pinto, I.; López-Pérez, B.; Márquez, M. Empatía: Medidas, teorías y aplicaciones en revisión [Empathy: Measurements, theories and applications under review]. An. Psicol. 2008, 24, 284–298. [Google Scholar]
- Mestre, M.V.; Frías, M.D.; Samper, P. Measuring empathy: The Interpersonal Reactivity Index. Psicothema 2004, 16, 255–260. [Google Scholar]
- Wilkinson, H.; Whittington, R.; Perry, L.; Eames, E. Examining the relationship between burnout and empathy in healthcare professionals: A systematic review. Burn. Res. 2017, 6, 18–29. [Google Scholar] [CrossRef] [PubMed]
- Duarte, L.; Pinto-Gouveia, J. Empathy and feelings of guilt experienced by nurses: A cross-sectional study of their role in burnout and compassion fatigue symptoms. Appl. Nurs. Res. 2017, 35, 42–47. [Google Scholar] [CrossRef] [Green Version]
- Mottaghi, S.; Poursheikhali, H.; Shameli, L. Empathy, compassion fatigue, guilt and secondary traumatic stress in nurses. Nurs. Ethics 2020, 27, 494–504. [Google Scholar] [CrossRef]
- Brunero, S.; Lamont, S.; Coates, M. A review of empathy education in nursing. Nurs. Inq. 2010, 17, 65–74. [Google Scholar] [CrossRef]
- Marilaf, M.; San-Martín, M.; Delgado-Bolton, R.; Vivanco, L. Empathy, loneliness, burnout, and life satisfaction in Chilean nurses of palliative care and homecare services. Enferm. Clin. 2017, 27, 379–386. [Google Scholar] [CrossRef]
- Hunt, P.A.; Denieffe, S.; Gooney, M. Burnout and its relationship to empathy in nursing: A review of the literature. J. Res. Nurs. 2017, 22, 7–22. [Google Scholar] [CrossRef]
- Salgado, M.E. Empathy management in consultation-liaison psychiatry. Persp. Psicol. 2015, 12, 44–51. [Google Scholar]
- Zilber, A. Theories about Theory of Mind. The role of cognitive and emotional processes. Rev. Latinoam. Psicol. 2017, 9, 1–12. [Google Scholar] [CrossRef]
- Rogers, C.R. The necessary and sufficient conditions of therapeutic personality change. J. Consult. Psychol. 1957, 21, 95. [Google Scholar] [CrossRef] [Green Version]
- Rogers, C.R. Client-Centered Therapy: Its Current Practice, Implications, and Theory; Houghton-Mifflin: Boston, CT, USA, 1965. [Google Scholar]
- Shamay-Tsooy, S.G.; Aharon-Peretz, J.; Perry, D. Two Systems for empathy: A double dissociation between emotional and cognitive empathy in inferior frontal gyrus versus ventromedial prefrontal lesions. Brain 2009, 132, 617–627. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Repetto, E. Fundamentos de Orientación. La Empatía en el Proceso Orientador [Orientation Fundamentals. Empathy in the Guiding Process]; Morata: Madrid, Spain, 1977. [Google Scholar]
- Repetto, E. Formación en Competencias Socioemocionales [Training in Socio-Emotional Skills]; La Muralla: Madrid, Spain, 2009. [Google Scholar]
- While, A. Touch: Knowledge and considerations for nursing practice. Br. J. Community Nurs. 2021, 26, 190–194. [Google Scholar] [CrossRef]
- Kelly, M.A.; Nixon, L.; McClurg, C.; Scherpbier, A.; King, N.; Dornan, T. Experience of Touch in Health Care: A Meta-Ethnography Across the Health Care Professions. Qual. Health Res. 2018, 28, 200–212. [Google Scholar] [CrossRef] [Green Version]
- Leskowitz, E. Therapeutic touch. In Complementary and Integrative Medicine in Pain Management; Complementary and Integrative Medicine in Pain Management, 1st ed.; Weintraub, M.I., Mamtani, R., Micozzi, M.S., Eds.; Springer Publishing Company: New York, NY, USA, 2008; pp. 163–174. [Google Scholar]
- Hall, J.A.; Schwartz, R. Empathy present and future. J. Soc. Psychol. 2019, 159, 225–243. [Google Scholar] [CrossRef]
- Dymond, R.F. A scale for the measurement of empathic ability. J. Consult. Psychol. 1949, 13, 127–133. [Google Scholar] [CrossRef] [PubMed]
- Hogan, R. Development of an empathy scale. J. Consult. Clin. Psychol. 1969, 33, 307–316. [Google Scholar] [CrossRef] [PubMed]
- Mehrabian, A.; Epstein, N. A measure of emotional empathy. J. Pers. 1972, 40, 525–543. [Google Scholar] [CrossRef]
- Mehrabian, A. Manual for the Balanced Emotional Empathy Scale (BEES); Albert Mehrabian: Monterey, CA, USA, 1996. [Google Scholar]
- Pérez-Albéniz, A.; de Paúl, J.; Etxeberría, J.; Montes, M.P.; Torres, E. Spanish adaptation of the Interpersonal Reactivity Index. Psicothema 2003, 15, 267–272. [Google Scholar]
- López-Pérez, B.; Fernández-Pinto, I.; Abad, F.J. TECA Test de Empatía Cognitiva y Afectiva [Cognitive and Affective Empathy Test]; TEA Ediciones: Madrid, Spain, 2008. [Google Scholar]
- Oceja, L.; López-Pérez, B.; Ambrona, T.; Fernández, I. Measuring general dispositions to feeling empathy and distress. Psicothema 2019, 21, 171–176. [Google Scholar]
- Reniers, R.L.; Corcoran, R.; Drake, R.; Shryane, N.M.; Völlm, B.A. The QCAE: A Questionnaire of Cognitive and Affective Empathy. J. Pers. Assess. 2011, 93, 84–95. [Google Scholar] [CrossRef] [PubMed]
- Aranda, M.; Montilla-Jiménez, G.; Montes-Berges, B. Escala de Personalidad Émpata (EPE) [Empath personality scale]. In Émpatas. La Capacidad de Sentir Como la otra Persona; Montes-Berges, B., Ed.; Ruiz de Aloza: Granada, Spain, 2011; pp. 143–163. [Google Scholar]
- Montes-Berges, B. Émpatas. La Capacidad de Sentir Como la Otra Persona. ¿Por qué Hay Personas Que no Pueden ver el Telediario? [Empaths. The Ability to Feel Like the Other Person. Why are there People who Cannot Watch the News?]; Ruiz de Aloza: Granada, Spain, 2011. [Google Scholar]
- Barrett-Lennard, G.T. Dimensions of the therapist response as causal factors in therapeutic change. Psychol. Monogr. 1962, 76, 1–36. [Google Scholar] [CrossRef]
- La Monica, E.L. Construct validity of an empathy instrument. Res. Nurs. Health 1981, 4, 389–400. [Google Scholar] [CrossRef]
- Hojat, M.; Mangione, S.; Nasca, T.J.; Cohen, M.J.; Gonnella, J.S.; Erdmann, J.B.; Magee, M. The Jefferson scale of physician empathy: Development and preliminary psychometric data. Educ. Psychol. Meas. 2001, 61, 349–365. [Google Scholar] [CrossRef]
- Yu, J.; Kirk, M. Evaluation of empathy measurement tools in nursing: Systematic review. J. Adv. Nurs. 2009, 65, 1790–1806. [Google Scholar] [CrossRef]
- Salovey, P.; Mayer, J.D. Emotional intelligence. Imagin. Cogn. Pers. 1990, 9, 185–211. [Google Scholar] [CrossRef]
- Mayer, J.D.; Salovey, P. What is Emotional Intelligence? In Emotional Development and Emotional Intelligence: Implications for Educator; Salovey, P., Sluyter, D., Eds.; Basic Books: New York, NY, USA, 1997; pp. 3–31. [Google Scholar]
- Muñoz, A.P.; Chaves, L. Empathy: A unique concept? Katharsis 2013, 16, 123–143. [Google Scholar]
- Salovey, P.; Mayer, J.D.; Goldman, S.L.; Turvey, C.; Palfai, T.P. Emotional attention, clarity, and repair: Exploring emotional intelligence using the Trait Meta-Mood Scale. In Emotion, Disclosure and Health; Pennebaker, J.W., Ed.; American Psychological Association: Washington, DC, USA, 1995; pp. 125–154. [Google Scholar]
- Extremera, N.; Fernández-Berrocal, P. Emotional intelligence, quality of interpersonal relationships and empathy in university students. Clin. Health 2004, 15, 117–137. [Google Scholar]
- Mestre, J.M.; Fernández-Berrocal, P. Manual de Inteligencia Emocional [Emotional Intelligence Manual]; Pirámide: Madrid, Spain, 2007. [Google Scholar]
- Meneghini, A.M.; Cunico, L.; Sartori, R. Empathy: Angel or devil? How shared emotions can help or hinder nurses in their relationships with patients. In Psychology and Neurobiology of Empathy; Psychology and Neurobiology of Empathy; Watt, D.F., Panksepp, J., Eds.; Nova Biomedical Books: Hauppauge, NY, USA, 2016; pp. 259–295. [Google Scholar]
- Montes-Berges, B. Émpatas, Empáticos y Ápatas. Claves Para Mejorar tu Empatía [Empatas, Empaths, and Apatas. Keys to Improve Your Empathy; Ruiz de Aloza: Granada, Spain, 2014. [Google Scholar]
- Muñiz, J.; Fonseca-Pedrero, E. Ten steps for test development. Psicothema 2019, 31, 7–16. [Google Scholar] [CrossRef] [PubMed]
- George, D.; Mallery, P. SPSS for Windows Step by Step: A Simple Guide and Reference. 11.0 update, 4th ed.; Allyn & Bacon: Boston, CT, USA, 2003. [Google Scholar]
- Hair, J.F.; Black, W.C.; Babin, B.J.; Anderson, R.E. Multivariate Data Analysis, 7th ed.; Pearson Education: Upper Saddle River, NJ, USA, 2014. [Google Scholar]
- Dimitrov, D.M. Testing for factorial invariance in the context of construct validation. Meas. Eval. Couns. Dev. 2010, 43, 121–149. [Google Scholar] [CrossRef]
- Filippetti, V.; López, M.A.; Richaud, M.C. Neuropsychological Approach to the Empathy Construct: Cognitive and Neuroanatomical Aspects. Cuad. Neuropsicol. 2012, 6, 63–83. [Google Scholar] [CrossRef]
- Gallese, V. The manifold nature of interpersonal relations: The quest for a common mechanism. Philos. Trans. R. Soc. 2003, 358, 517–528. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Abascal, E.G.; Martín-Díaz, M.D. Relations between Dimensions of Emotional Intelligence, Specific Aspects of Empathy, and Non-verbal Sensitivity. Front. Psychol. 2019, 10, 1066. [Google Scholar] [CrossRef]
- Valor-Segura, I.; Expósito, F.; Moya, M. Forgiveness for transgressions in interpersonal relationships. Psicosoc. Interv. 2010, 19, 129–134. [Google Scholar] [CrossRef]
- Baron-Cohen, S. Empathizing, systemizing, and the extreme male brain theory of autism. Prog. Brain Res. 2010, 186, 167–175. [Google Scholar] [CrossRef] [PubMed]
- Hojat, M.; Gonnella, J.S.; Nasca, T.J.; Mangione, S.; Vergare, M.; Magee, M. Physician empathy: Definition, components, measurement, and relationship to gender and specialty. Am. J. Psychiatry 2020, 159, 1563–1569. [Google Scholar] [CrossRef] [Green Version]
- Toccaceli, V.; Fagnani, C.; Eisenberg, N.; Alessandri, G.; Vitale, A.; Stazi, M.A. Adult empathy: Possible gender differences in gene-environment architecture for cognitive and emotional components in a large Italian twin sample. Twin Res. Hum. Genet. 2018, 21, 214–226. [Google Scholar] [CrossRef]
- Stern, J.A.; Cassidy, J. Empathy from infancy to adolescence: An attachment perspective on the development of individual differences. Dev. Rev. 2018, 47, 1–22. [Google Scholar] [CrossRef]
- Suna, B.; Luoa, Z.; Zhangb, W.; Lia, W.; Li, X. Age-related differences in affective and cognitive empathy: Self-report and performance-based evidence. Aging Neuropsychol. C 2017, 1–18. [Google Scholar] [CrossRef]
- Wieck, C.; Kunzmann, U. Age differences in empathy: Multidirectional and context-dependent. Psychol. Aging 2015, 30, 407–419. [Google Scholar] [CrossRef]
- Bailey, P.E.; Brady, B.; Ebner, N.C.; Ruffman, T. Effects of Age on Emotion Regulation, Emotional Empathy, and Prosocial Behavior. J. Gerontol. B Psychol. Sci. Soc. Sci. 2020, 75, 802–810. [Google Scholar] [CrossRef]
- Roth, M.; Altmann, T. The self-other agreement of multiple informants on empathy measures and its relation to empathic accuracy. Pers. Individ. Dif. 2020, 171, e110499. [Google Scholar] [CrossRef]
- McCann, C.; Roberts, R.D. New paradigms for assessing emotional intelligence: Theory and data. Emotion 2008, 8, 540–551. [Google Scholar] [CrossRef] [PubMed]
- Nowicki, S.; Carton, J. The Measurement of Emotional Intensity from Facial Expressions. J. Soc. Psychol. 1993, 133, 749–750. [Google Scholar] [CrossRef] [PubMed]
- Baum, K.M.; Nowicki, S. Perception of emotion: Measuring decoding accuracy of adult prosodic cues varying intensity. J. Nonverbal Behav. 1998, 22, 89–107. [Google Scholar] [CrossRef]

| Item | D1 | D2 | D3 | D4 | D5 |
|---|---|---|---|---|---|
| 17 (8 *) People’s negative emotions are so easily passed on to me that they affect me as if they were my own. | 0.817 | ||||
| 26 (13) When I am next to someone who is upset, I end up feeling the same way. | 0.832 | ||||
| 10 (6r **) When I am next to someone who is upset, their emotions do not transfer to me. | 0.713 | ||||
| 4 (4) When I know I will be exposed to an emotionally negative and intense situation, I prepare to distance myself from the situation. | 0.812 | ||||
| 1 (1) Before a difficult situation, I use some techniques to face the emotions to come, such as relaxation. | 0.807 | ||||
| 18 (17r **) I avoid situations involving negative emotions because I don’t know how to get rid of them. | 0.798 | ||||
| 19 (18) I know how to separate myself from others’ feelings. | 0.736 | ||||
| 2 (2r) It is difficult for me to identify which negatives emotions are my own and which are the other person’s. | 0.802 | ||||
| 3 (3) I am able to determine if the emotions I experience are my own or the other person’s. | 0.800 | ||||
| 23 (11) When I am with someone, I can identify which part of what I am feeling is caused by that person. | 0.701 | ||||
| 5 (5) When it comes to positive emotions, I can easily identify which have been passed on to me by the other person and which are my own. | 0.676 | ||||
| 21 (10r) When someone explains to me how they feel, it is difficult for me to understand it. | 0.771 | ||||
| 28 (15r) I struggle to understand how another person is feeling. | 0.772 | ||||
| 20 (9r) I tend not to understand how someone is feeling by their non-verbal communication. | 0.733 | ||||
| 13 (7) I know how to appease someone. | 0.748 | ||||
| 25 (12) If someone is feeling sad, I pass my joy on to him/her. | 0.750 | ||||
| 30 (16) When someone near me is feeling anxious, I don’t know how but I am able to calm him/her. | 0.671 | ||||
| 27 (14r) It is difficult for me to create positive emotions in a difficult situation. | 0.652 |
| EME Dimensions | Correlations | |||||
|---|---|---|---|---|---|---|
| M (SD) | D1 | D2 | D3 | D4 | D5 | |
| D1Idt | 4.00 (0.92) | 1 | ||||
| D2Inc | 2.67 (0.93) | −0.032 | 1 | |||
| D3Rev | 3.52 (0.86) | 0.112 ** | 0.033 | 1 | ||
| D4Sep | 3.07 (0.88) | −0.056 | 0.053 | 0.293 ** | 1 | |
| D5Proj | 3.17 (0.73) | 0.137 ** | 0.049 | 0.267 ** | 0.375 ** | 1 |
| Subscales | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. EMSiden | 1 | ||||||||||||||
| 2. EMSinc | −0.052 | 1 | |||||||||||||
| 3. EMSrev | 0.125 ** | −0.024 | 1 | ||||||||||||
| 4. EMSsep | −0.027 | −0.032 | 0.243 ** | 1 | |||||||||||
| 5. EMEproj | 0.126 ** | −0.027 | 0.255 ** | 0.343 ** | 1 | ||||||||||
| 6. EPEfeel | 0.342 ** | 0.250 ** | 0.126 ** | 0.264 ** | 0.392 ** | 1 | |||||||||
| 7. EPEsep | 0.114 * | 0.333 ** | 0.099 * | −0.023 | 0.074 | 0.385 ** | 1 | ||||||||
| 8. EPEapat | −0.334 ** | 0.039 | −0.145 ** | −0.022 | −0.140 ** | −0.066 | −0.080 | 1 | |||||||
| 9. TMMSaten | 0.058 | 0.233 ** | 0.095 * | 0.140 ** | 0.143 ** | 0.299 ** | 0.241 ** | 0.151 ** | 1 | ||||||
| 10. TMMSclar | 0.185 ** | −0.075 | 0.103 * | 0.377 ** | 0.308 ** | 0.244 ** | −0.022 | 0.153 ** | 0.130 ** | 1 | |||||
| 11. TMMSreg | 0.087 | −0.180 ** | 0.301 ** | 0.282 ** | 0.407 ** | 0.157 ** | −0.017 | 0.120 ** | 0.043 | 0.301 ** | 1 | ||||
| 12. IRIpers | 0.340 ** | 0.033 | 0.171 ** | 0.165 ** | 0.287 ** | 0.397 ** | 0.206 ** | 0.171 ** | 0.218 ** | 0.248 ** | 0.281 ** | 1 | |||
| 13. IRIfant | 0.207 ** | 0.213 ** | −0.003 | −0.007 | −0.027 | 0.237 ** | 0.193 ** | 0.185 ** | 0.275 ** | −0.006 | −0.084 | 0.137 ** | 1 | ||
| 14. IRIconcer | 0.308 ** | 0.295 ** | 0.048 | 0.079 | 0.168 ** | 0.406 ** | 0.468 ** | 0.141 ** | 0.378 ** | 0.086 | 0.042 | 0.429 ** | 0.241 ** | 1 | |
| 15. IRIdisc | −0.188 ** | 0.355 ** | −0.056 | −0.135 | −0.213 | −0.023 | 0.200 ** | −0.023 | 0.221 ** | −0.256 ** | −0.249 | −0.120 ** | 0.186 ** | 0.134 ** | 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mora-Pelegrín, M.; Montes-Berges, B.; Aranda, M.; Vázquez, M.A.; Armenteros-Martínez, E. The Empathic Capacity and the Ability to Regulate It: Construction and Validation of the Empathy Management Scale (EMS). Healthcare 2021, 9, 587. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare9050587
Mora-Pelegrín M, Montes-Berges B, Aranda M, Vázquez MA, Armenteros-Martínez E. The Empathic Capacity and the Ability to Regulate It: Construction and Validation of the Empathy Management Scale (EMS). Healthcare. 2021; 9(5):587. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare9050587
Chicago/Turabian StyleMora-Pelegrín, Miguel, Beatriz Montes-Berges, María Aranda, María Agustina Vázquez, and Elena Armenteros-Martínez. 2021. "The Empathic Capacity and the Ability to Regulate It: Construction and Validation of the Empathy Management Scale (EMS)" Healthcare 9, no. 5: 587. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare9050587