
Prevention and Treatment of Phlebitis Secondary to the Insertion of a Peripheral Venous Catheter: A Scoping Review from a Nursing Perspective


 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Search Strategy
2.3. Selection Criteria
2.4. Data Collection and Extraction
2.5. Evaluation of Methodological Quality
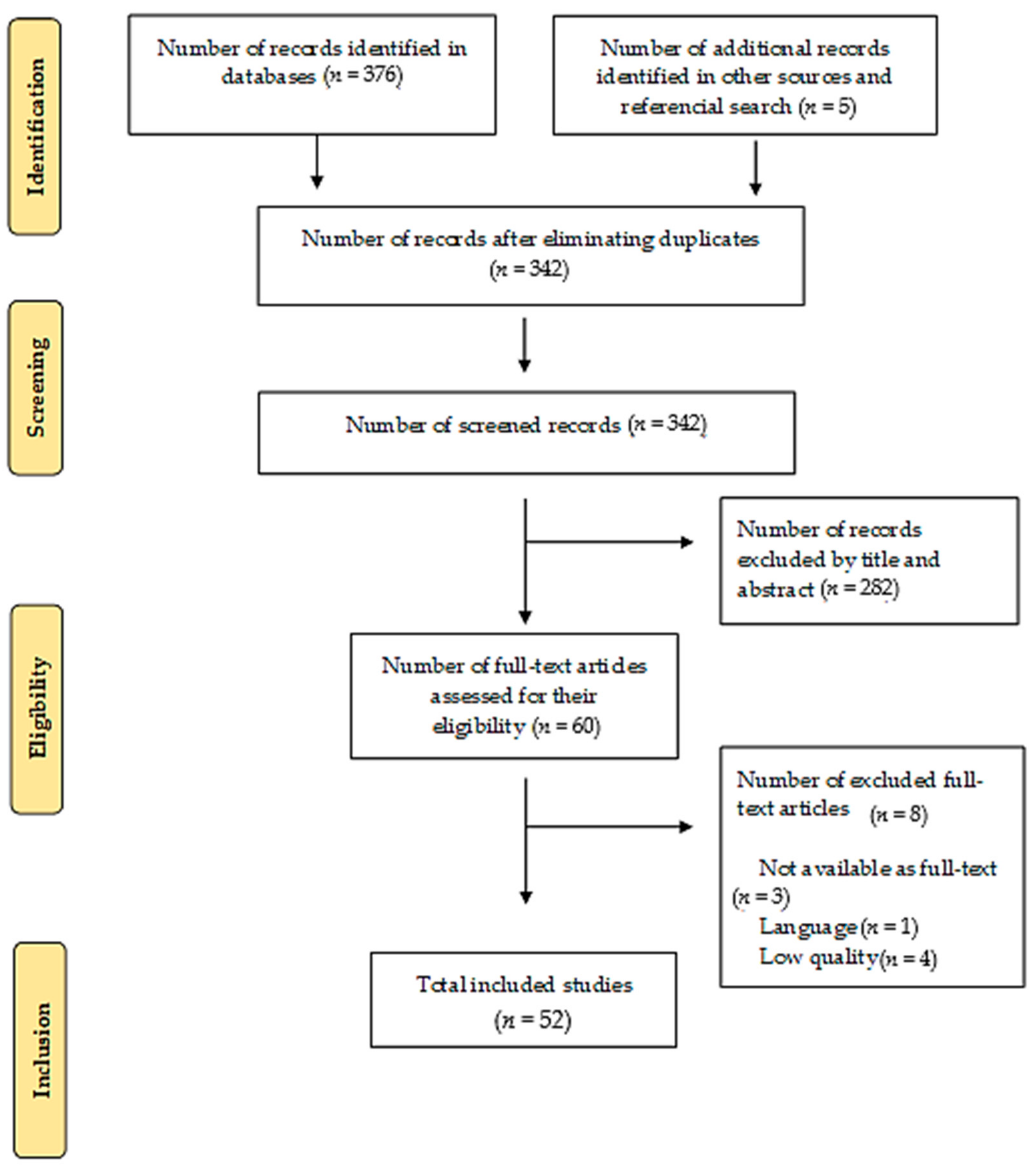
3. Results
3.1. Nursing Interventions for the Prevention of Phlebitis
- For intermittent flushing and locking of PVC, it is recommended to use saline solution (SS) before and after administration of medication by performing the positive pressure technique [4,29]. According to the Flebitis Zero project, flushing heparin is not recommended because it can cause thrombocytopenia [7]. A randomized clinical trial reflected that continuous infusion of heparin into PVCs improved the duration of permeability, reducing infusion failure and phlebitis. However, no statistically significant differences were found when heparin was used intermittently. If PVC is used to obtain a blood sample, the use of diluted heparin is indicated [43]. Double-pump syringes enable both medication and cleaning solution administration to reduce PVC manipulation and complications [40].
- To prevent and treat phlebitis, Aloe vera, Matricaria chamomilla, and Xianchen (composed of some components such as Fritillaria and Bletilla striata) can be used. The application of Moist Exposed Burn Ointment (MEBO) for topical treatment of burn injuries, containing sesame oil, β-sitosterol, Berberine, and other medicinal plants (Coptis chinensis, Scutellaria baicalensis, Phellodendron chinese, and Papaver somniferum) [36] is also effective.
- Not performing a systematic catheter change every 72 to 96 h. It must be changed when clinically justified. There are no significant differences in the percentage of complications (phlebitis, occlusion...) between PVC that have been inserted less than 96 h and those that have been inserted for more than 96 h [4,46,47].
- Avoiding insertion into joint areas, wrist, and antecubital fossa, because there is a higher incidence of mechanical phlebitis related to catheter movement [4].
- Replacing administration systems, extension cords, and accessories with a frequency of more than 96 h and less than 7 days, when dirty or damaged connections are observed, and whenever there is an accidental disconnection of the circuit [4].
- Withdrawing systems of blood administration and of blood products at the end of transfusion [4].
- In adults, an upper-extremity site for catheter insertion must be used. Any catheter inserted in a lower extremity must be replaced to an upper extremity site as soon as possible [4].
- Using a 0.22-micron line filter to remove air and bacteria and small drug particles that were not properly diluted. A filter is also required when the infusion of amiodarone exceeds 24 h [48].
3.2. Asepsis
- Applying antiseptics to clean skin and complying with drying times (2% alcoholic chlorhexidine: 30 s; non-alcoholic chlorhexidine and povidone–iodine: 2 min) [4].
- Hygienic hand washing and usage of clean gloves for both punctures and equipment, hubs, stopcocks, and bio-connectors handling. It is not necessary to wear sterile gloves if the previously disinfected area is not touched again during the technique [4]. Using disposable tourniquets can help reduce PVC contamination rates [49].
- Minimizing handling of connectors for infusion equipment [4].
- Protecting dressing and connectors in activities that may pose a risk of contamination [4].
3.3. Nursing Assessment
- Involving the patient in the choice of PVC and puncture site [2].
- Assessing the status of venous resources. Whenever possible, choose straight, palpable, and well-filled vessels [4].
- Previously identifying comorbidities such as diabetes mellitus due to the changes in the circulatory system caused by this disease [31].
- Asking the patient if there is pain/discomfort, heat, or burning at the insertion site [32].
3.4. Catheter
- Selecting the length and caliber of the catheters based on objective, expected time of use, known infectious or non-infectious complications, experience of those who insert and manage the catheter [7].
- Using the minimum number of three-way stopcocks. Idle ports should always be capped [4].
- Using only one of the ports of the three-way stopcock to place a bio-connector, where medication solutions and bolus will be administered. The results of a prospective experimental study indicate that using SwabCap significantly reduced connector contamination from 43.7% to 0% (p = 0.006) [51]. If this cap is not available, the bio-connector is disinfected with alcoholic chlorhexidine at >0.5% or 70% alcohol for 30 s [4,7].
- Teflon, silicone, or polyurethane elastomer catheters are safer than those of polyethylene, polyvinyl hydrochloride, or steel needles, which might cause tissue necrosis if extravasation occurs [43].
3.5. Dressing
- The dressing should be placed aseptically, with clean or sterile gloves, without excessively touching the adhesive layer and without placing tie-shaped adhesive tapes under the dressing. Wear sterile gloves for central and arterial devices [4].
- Replacing catheter site dressing if the dressing becomes damp, loosened, or visibly soiled [7].
- If the site is bleeding or oozing, use gauze dressing until this is resolved [4].
- Ensuring correct securement or dressing to prevent dislodgement [4].
- Softly removing dressing, without moistening the puncture site [4].
- For catheter securement, products such as CliniFix simultaneously reduce the risk of infection and trauma from cannula movement. Made with hydrocolloid adhesive, not harmful to the skin, that can remain in place for up to 7 days without affecting the integrity of the skin. In the presence of wound oozing, hydrocolloids absorb fluid and form gel to help reduce the spread of infection [42].
- Using skin glue (cyanoacrylate) at the insertion site to improve catheter securement and reduce rates of phlebitis and occlusion. Apply a drop at the insertion site and a drop under the center of the catheter, allow to dry for 30 s, and place a dressing [33].
- Using the “I.V. House UltraDressing” in pediatric patients to increase catheter dwell time, and to protect and stabilize PIVCs [34].
3.6. Nursing Interventions for the Treatment of Phlebitis
- Apply alternating hot and cold compresses to decrease erythema, edema, and pain. The hot compress stimulates vasodilation by inducing optimal blood circulation and promoting a faster wound-healing process. The cold compress stimulates vasoconstriction and reduces edema [35].
- Apply compresses with 0.9% NaCl to stimulate anti-inflammatory response and relieve pain, redness, swelling, and edema [35].
- Apply 10 drops (3 mL) of sesame oil (SO) twice daily for two weeks. Massage for 5 min within 10 cm of the place of phlebitis. Use a finger with a sterile glove to apply a rotary technique. SO contains unsaturated fatty acids (linoleic acid, oleic acid) that relieve pain by reducing prostaglandins and leukotriene. In addition, the SO has lignans responsible for analgesic and anti-inflammatory effects [36].
- Administer chamomile extract (2.5%), as it has anti-inflammatory and anti-edema properties. It is the most effective in the treatment of grade II phlebitis. The use of topical chamomile showed that the incidence of phlebitis in patients treated with amiodarone decreases significantly. Aqueous chamomile extract inhibits the production of prostaglandins by the suppression of cyclooxygenase-2 (COX-2) and direct gene expression of inhibition of COX-2 enzyme activity [37].
- Apply a compress with Burow solution at a temperature between 2 and 8 degrees Celsius, and leave on for 20 min every 8 h. This formulation has as its main component aluminium acetate, which is known for its astringent properties and ability to produce the precipitation of proteins at the topical level. Based on observed results, the Burow solution could be defined as an effective therapeutic alternative in the treatment of post-infusion phlebitis [38].
- Apply marigold ointment every 8 h. Calendula/marigold flavonoids prevent histamine release and prostaglandin production. In addition, they inhibit blood plasma secretion in tissues, reduce the migration of white blood cells to the swelled area, and prevent the growth of bacteria and fungi by reducing capillary permeability. In one study, the application of marigold ointment decreased the severity of phlebitis in a shorter period compared to using a wet and hot compress. It is proven to have anti-inflammatory and antibacterial effects. Although calendula has an anti-inflammatory effect similar to corticoids, it has none of its complications and is safe to use [39].
3.7. Nurses Following Protocols and Guidelines
- Topical treatments with Aloe vera or “Chamomilla Recutita” using wet compresses at 38 degrees Celsius on the affected area. Apply topical diclofenac and "Essaven" heparin gel. Other topical products such as notoginseny and 5 mg nitroglycerin patch accelerate the improvement of phlebitis symptoms, as compared to heparinoid substances [6].
- Dilution of chemotherapeutic agents, immediate catheter removal, intermittent heparin washing, prophylactic antibiotics, transparent dressings, topical application of anti-inflammatory or corticosteroid agents, and application of a hot and/or wet compress are preventive and therapeutic approaches [36].
- There is no definitive treatment to prevent phlebitis; drugs such as heparin, corticosteroids, and piroxicam have been proposed as therapeutic agents [39].
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Urbanetto, J.S.; Peixoto, C.G.; May, T.A. Incidencia de flebitis durante el uso y después de la retirada de catéter intravenoso periférico. Rev. Latino-Am. Enfermagem 2016, 24, e2746. [Google Scholar] [CrossRef] [Green Version]
- Salgueiro-Oliveira, A.S.; Basto, M.L.; Braga, L.M.; Arreguy-Sena, C.; Melo, M.N.; Parreira, P.M. Nursing practices in peripheral venous catheter: Phlebitis and patient safety. Texto Contexto-Enferm 2019, 28, e20180109. [Google Scholar] [CrossRef] [Green Version]
- Enes, S.M.S.; Opitz, S.P.; Faro, A.R.M.d.C.d.; Pedreira, M.d.L.G. Phlebitis associated with peripheral intravenous catheters in adults admitted to hospital in the Western Brazilian Amazon. Rev. Esc. Enferm. USP 2016, 50, 263–271. [Google Scholar] [CrossRef] [PubMed]
- Torres-Muñoz, R.; Marín-Navarro, L.; Gallego-Sánchez, J.C. Cuidados de Enfermería en los Accesos Vasculares. Guía De recomendaciones. Complejo Hospitalario Universitario de Badajoz. Área de Salud de Badajoz. 2018. Available online: https://www.areasaludbadajoz.com/Calidad_y_Seguridad_2016/Cuidados_enfermeria_accesos_vasculares.pdf (accessed on 12 December 2020).
- Tork-Torabi, M.; Namnabati, M.; Allameh, Z.; Talakoub, S. Vancomycin Infusion Methods on Phlebitis Prevention in Children. Iran. J. Nurs. Midwifery Res. 2019, 24, 432–436. [Google Scholar] [CrossRef]
- Martín-Gil, B.; Fernández-Castro, M.; López-Vallecillo, M.; Peña-García, I. Efectividad del tratamiento tópico de la flebitis secundaria a la cateterización periférica: Una revisión sistemática. Enferm. Glob. 2017, 16, 491–507. [Google Scholar] [CrossRef] [Green Version]
- Martínez-Ortega, C.; Suárez Mier, B.; Cantero, M.; Llinás, M.; Plan Nacional Resistencia Antibióticos. Prevención de Complicaciones Relacionadas con Accesos Vasculares de Inserción Periférica. Programa Flebitis Zero. Ministerio de Sanidad, Consumo y Bienestar Social. Agencia Española de Medicamentos y Productos Sanitarios. 2019. Available online: http://www.resistenciaantibioticos.es/es/system/files/content_images/programa_flebitis_zero.pdf (accessed on 12 February 2021).
- Ray-Barruel, G.; Cooke, M.; Mitchell, M.; Chopra, V.; Rickrad, C.M. Implementing the I-DECIDED clinical decision-making tool for peripheral intravenous catheter assessment and safe removal: Protocol for an interrupted time-series study. BMJ Open 2018, 8, e021290. [Google Scholar] [CrossRef] [Green Version]
- Infusion Nurses Society. Infusion Nursing Standards of Practice. J. Infus. Nurs. 2016, 36, 1–159. [Google Scholar]
- Ortiz del Río, C.A.; Pérez de la Blanca, E.B.; Buzón Barrera, M.L.; Calderón Sandubete, E.; Carrero Caballero, M.C.; Carrión Camacho, M.R.; Luna Rodríguez, M.E.d.; García Aguilar, R.; García Díez, R.; García Fernández, F.P.; et al. Guía de Práctica Clínica Sobre Terapia Intravenosa con Dispositivos no Permanentes en Adultos. Ministerio de Sanidad, Servicios Sociales e Igualdad. Agencia de Evaluación de Tecnologías Sanitarias de Andalucía (AETSA). 2014. Available online: https://www.aetsa.org/publicacion/guia-de-practica-clinica-sobre-terapia-intravenosa-con-dispositivos-no-permanentes-en-adultos/ (accessed on 12 February 2021).
- Nickel, B. Peripheral Intravenous Access: Applying Infusion Therapy Standards of Practice to Improve Patient Safety. Crit. Care Nurse 2019, 39, 61–71. [Google Scholar] [CrossRef]
- Atay, S.; Sen, S.; Cukurlu, D. Phlebitis-related peripheral venous catheterization and the associated risk factors. Niger. J. Clin. Pract. 2018, 21, 827–831. [Google Scholar] [CrossRef]
- Eghbali-Babadi, M.; Ghadiriyan, R.; Hosseini, S.M. The effect of saline lock on phlebitis rates of patients in cardiac care units. Iran. J. Nurs. Midwifery Res. 2015, 20, 496–501. [Google Scholar] [CrossRef]
- Milutinović, D.; Simin, D.; Zec, D. Risk factor for phlebitis: A questionnaire study of nurses’ perception. Rev. Lat. Am. Enferm. 2015, 23, 677–684. [Google Scholar] [CrossRef] [Green Version]
- Furlan, M.S.; Costa-Lima, A.F. Direct cost of procedures for phlebitis treatment in an Inpatient Unit. Rev. Esc. Enferm. USP 2020, 54, e03647. [Google Scholar] [CrossRef]
- Chiu, P.C.; Lee, Y.H.; Hsu, H.T.; Fneg, Y.T.; Lu, I.C.; Chiu, S.L.; Cheng, K.I. Establish a perioperative check forum for peripheral intravenous access to prevent the occurrence of phlebitis. Kaohsiung J. Med. Sci. 2015, 31, 215–221. [Google Scholar] [CrossRef] [Green Version]
- Osti, C.; Khadka, M.; Wosti, D.; Gurung, G.; Zhao, Q. Knowledge and practice towards care and maintenance of peripheral intravenous cannula among nurses in Chitwan Medical College Teaching Hospital, Nepal. Nurs. Open 2019, 6, 1006–1012. [Google Scholar] [CrossRef]
- Ministerio de Ciencia e Innovación. Orden Cin/2134/2008, de 3 de Julio, Por la Que se Establecen los Requisitos para la Verificación de los Títulos Universitarios Oficiales que Habiliten para el Ejercicio de la Profesión de Enfermero. BOE Num 174, de 19 de Julio de 2008. Available online: https://www.boe.es/eli/es/o/2008/07/03/cin2134 (accessed on 18 May 2021).
- Herdman, T.H.; Kamitsuru, S. (Eds.) NANDA International Nursing Diagnoses: Definition and Clasification 2018–2020, 11th ed.; Thieme Medical Publishers Inc.: New York, NY, USA, 2017. [Google Scholar]
- Butcher, H.K.; Bulechek, G.M.; Dochrterman, J.M.; Wagner, C. Clasificación de Intervenciones de Enfermería (NIC), 7th ed.; Elsevier: Barcelona, Spain, 2018. [Google Scholar]
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The PRISMA Group. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Santamaría-Olmo, R. Programa de habilidades en Lectura Crítica Español (CASPe). Nefroplus 2017, 9, 100–101. [Google Scholar]
- Berra, S.; Elorza-Ricart, J.M.; Estrada, M.D.; Sánchez, E. Instrumento para la lectura crítica y la evaluación de estudios epidemiológicos transversales. Gac. Sanit. 2008, 22, 492–497. [Google Scholar] [CrossRef]
- Levac, D.; Colquhoun, H.; O’Brien, K.K. Scoping studies: Advancing the methodology. Implement. Sci. 2010, 5, 69. [Google Scholar] [CrossRef] [Green Version]
- Flórez-Gómez, I.D.; Montoya, D.C. Las guías de práctica clínica y el instrumento AGREE II. Rev. Colomb. Ppsiquiat. 2011, 40, 563–576. [Google Scholar] [CrossRef]
- Manterola, C.; Asenjo-Lobos, C.; Otzen, T. Jerarquización de la evidencia: Niveles de evidencia y grados de recomendación de uso actual. Rev. Chil. Infectol. 2014, 31, 705–718. [Google Scholar] [CrossRef] [Green Version]
- Jordan, Z.; Lockwood, C.; Munn, Z.; Aromataris, E. The update Joanna Briggs Institute Model of Evidence Based Healthcare. Int. J. Evid. Based Healthc. 2019, 17, 58–71. [Google Scholar] [CrossRef]
- Reichembach-Danski, M.T.; Mingorance, P.; Athanasio-Johann, D.; Adami-Vayego, S.; Lind, J. Incidence of local complications and risk factors associated with peripheral intravenous catheter in neonates. Rev. Esc. Enferm. USP 2016, 50, 22–28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Braga, L.M.; Parreira, P.M.; Salgueiro-Oliveira, A.S.; Mendes-Mónico, L.S.; Arreguy-Sena, C.; Henriques, M.A. Flebitis e infiltración: Traumas vasculares asociados al catéter venoso periférico. Rev. Lat. Am. Enfermagem 2018, 26, e3002. [Google Scholar] [CrossRef] [Green Version]
- Rosário-Pereira, M.S.; de Oliveria-Cunha, A.T.; Almeida-Lima, E.F.; Ferreira-Santos, T.F.; Batista-Portugal, F. La Seguridad del paciente en el contexto de las flebitis notificadas en un hospital universitario. Rev. Epidemiol. Controle Infecção 2019, 9, 1–7. [Google Scholar] [CrossRef]
- Lim, E.Y.P.; Wong, C.Y.W.; Kek, L.K.; Suhairi, S.S.B.M.; Yip, W.K. Improving the Visibility of Intravenous (IV) Site in Pediatric Patients to Reduce IV Site Related Complications-An Evidence-based Utilization Project. J. Pediatr. Nurs. 2018, 41, e39–e45. [Google Scholar] [CrossRef]
- Bugden, S.; Shean, K.; Scott, M.; Mihala, G.; Clark, S.; Johnstone, C.; Fraser, J.F.; Rickard, C.M. Skin Glue Reduces the Failure Rate of Emergency Department-Inserted Peripheral Intravenous Catheters: A Randomized Controlled Trial. Ann. Emerg. Med. 2016, 68, 196–201. [Google Scholar] [CrossRef]
- Büyükyılmaz, F.; Şahiner, N.C.; Cağlar, S.; Eren, H. Effectiveness of an Intravenous Protection Device in Pediatric Patients on Catheter Dwell Time and Phlebitis Score. Asian Nurs. Res. 2019, 13, 236–241. [Google Scholar] [CrossRef] [Green Version]
- Annisa, F.; Nurhaeni, N.; Wanda, D. Warm Water Compress as an Alternative for Decreasing the Degree of Phlebitis. Compr. Child Adolesc. Nurs. 2017, 40 (Suppl. 1), 107–113. [Google Scholar] [CrossRef]
- Shamloo, M.B.B.; Nasiri, M.; Maneiy, M.; Dorchin, M.; Mojab, F.; Bahrami, H.; Naseri, M.S.; Kiarsi, M. Effects of topical sesame (Sesamum indicum) oil on the pain severity of chemotherapy-induced phlebitis in patients with colorectal cancer: A randomized controlled trial. Complement Ther. Clin. Pract. 2019, 35, 78–85. [Google Scholar] [CrossRef] [PubMed]
- Sharifi-Ardani, M.; Yekefallah, L.; Asefzadeh, S.; Nassiri-Asl, M. Efficacy of topical chamomile on the incidence of phlebitis due to an amiodarone infusion in coronary care patients: A double-blind, randomized controlled trial. J. Integr. Med. 2017, 15, 373–378. [Google Scholar] [CrossRef]
- García-Quintanilla, L.; Otero-Barreiro, M.; González-Barcia, M.; Virgós-Lamela, A.; Rodríguez-Prada, M.; Lamas, M.; Fernández-Ferreiro, A. Estudio de la Utilización, Eficacia y Seguridad de la Solución de Burow en el tratamiento de la flebitis. Rev. Ofil Ibero Lat. Am. J. Health Syst. Pharm. 2018, 28, 199–202. [Google Scholar]
- Jourabloo, N.; Nasrabadi, T.; Ebrahimi-Abyaneh, E. Comparing the effect of warm moist compress and Calendula ointment on the severity of phlebitis caused by 50% dextrose infusion: A clinical trial. Med. Surg. Nurs. 2017, 6, 21–26. [Google Scholar]
- Parreira, P.; Sousa, L.B.; Marques, I.A.; Santos-Costa, P.; Braga, L.M.; Cruz, A.; Salgueiro-Oliveira, A. Double-chamber syringe versus classic syringes for peripheral intravenous drug administration and catheter flushing: A study protocol for a randomised controlled trial. Trials 2020, 21, 78. [Google Scholar] [CrossRef] [Green Version]
- Pérez-Granda, M.J.; Bouza, E.; Pinilla, B.; Cruces, R.; González, A.; Millán, J.; Guembe, M. Randomized clinical trial analyzing maintenance of peripheral venous catheters in an internal medicine unit: Heparin vs. saline. PLoS ONE 2020, 15, e0226251. [Google Scholar] [CrossRef]
- Higgingson, R. IV cannula securement: Protecting the patient from infection. Br. J. Nurs. 2015, 24, S23–S28. [Google Scholar] [CrossRef]
- Chau, J.; Pellowe, C.; Instituto Joanna Briggs. Manejo de los dispositivos intravasculares periféricos. Best Pract. 2008, 12, 1–4, ISSN 1329-1874. [Google Scholar]
- Da Silva-Oliveira, E.C.; Barros-de Oliveira, A.P.; de Oliveira, R.C. Caracterización de flebitis notificada a la gestión de riesgos en la red centinela hospitalaria. Rev. Baiana Enferm. 2016, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Mattox, E.A. Complications of Peripheral Venous Access Devices: Prevention, Detection, and Recovery Strategies. Crit. Care Nurse 2017, 37, e1–e14. [Google Scholar] [CrossRef] [Green Version]
- Webster, J.; Osborne, S.; Rickard, C.M.; Marsh, N. Clinically-indicated replacement versus routine replacement of peripheral venous catheters. Cochrane Database Syst. Rev. 2019, 23, CD007798. [Google Scholar] [CrossRef] [Green Version]
- Gilton, L.; Seymour, A.; Baker, R.B. Changing Peripheral Intravenous Catheter Sites When Clinically Indicated: An Evidence-Based Practice Journey. Worldviews Evid. Based Nurs. 2019, 16, 418–420. [Google Scholar] [CrossRef] [PubMed]
- Oragano, C.A.; Patton, D.; Moore, Z. Phlebitis in Intravenous Amiodarone Administration: Incidence and Contributing Factors. Crit. Care Nurs. 2019, 39, 1–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parreira, P.; Serambeque, B.; Costa, P.S.; Mónico, L.S.; Oliveira, V.; Sousa, L.B.; Gama, F.; Bernardes, R.A.; Adriano, D.; Marques, I.A.; et al. Impact of an Innovative Securement Dressing and Tourniquet in Peripheral Intravenous Catheter-Related Complications and Contamination: An Interventional Study. Int. J. Environ. Res. Public Health 2019, 16, 3301. [Google Scholar] [CrossRef] [Green Version]
- Mandal, A.; Raghu, K. Study on incidence of phlebitis following the use of peripheral intravenous catheter. J. Fam. Med. Prim. Care 2019, 8, 2827–2831. [Google Scholar] [CrossRef]
- Gutiérrez-Nicolás, F.; Nazco-Casariego, G.J.; Viña-Romero, M.M.; González-García, J.; Ramos-Diaz, R.; Perez-Perez, J.A. Reducing the degree of colonisation of venous access catheters by continuous passive disinfection. Eur. J. Hosp. Pharm. 2016, 23, 131–133. [Google Scholar] [CrossRef]
- Corley, A.; Ullman, A.J.; Mihala, G.; Ray-Barruel, G.; Ray-Barruel, G.; Alexandrou, E.; Rickard, C.M. Peripheral intravenous catheter dressing and securement practice is associated with site complications and suboptimal dressing integrity: A secondary analysis of 40,637 catheters. Int. J. Nurs. Stud. 2019, 100. [Google Scholar] [CrossRef] [Green Version]
- Lemos-Alves, J.; Mendes-Rodrígues, C.; Velloso-Antunes, A. Prevalence of Phlebitis in a Clinical Inpatient Unit of a High-complexity Brazilian University Hospital. Rev. Bras. Ciências Saúde 2018, 22, 231–236. [Google Scholar]
- Roman-Ros, A.C.; Ramos-Oliveira, D.; Debon, R.; Scaratti, M. Intravenous therapy in hospitalized older adults: Care evaluation. Cogitare Enferm 2017, 2, e49989. [Google Scholar]
- Lee, S.; Kim, K.; Kim, J.S. A Model of Phlebitis Associated with Peripheral Intravenous Catheters in Orthopedic Inpatients. Int. J. Environ. Res. Public Health. 2019, 16, 3412. [Google Scholar] [CrossRef] [Green Version]
- Loureiro-Buzatto, L.; Pinna-Massa, G.; Sorgini-Peterlini, M.A.; Yamaguchi-Whitaker, I. Factors associated with phlebitis in elderly patients with intravenous infusion. Acta. Paul. Enferm. 2016, 29, 260–266. [Google Scholar] [CrossRef] [Green Version]
- Wei, T.; Li, X.; Yue, Z.; Chen, Y.; Wang, Y.; Yuan, Z.; Lin, Q.; Tan, Y.; Peng, S.; Li, X. Catheter Dwell Time and Risk of Catheter Failure in Adult Patients With Peripheral Venous Catheters. J. Clin. Nurs. 2019, 28, 4488–4495. [Google Scholar] [CrossRef]
- Urbanetto, J.S.; Minuto-Muniz, F.O.; Martis da Silva, R.; Christo de Freitas, A.P.; Ribeiro de Oliveira, A.P.; Ramos dos Santos, J.C. Incidence of phlebitis and post-infusion phlebitis in hospitalised adults. Rev. Gaúcha Enferm. 2017, 38, e58793. [Google Scholar]
- Braga, L.M.; Salgueiro-Oliveira, A.S.; Pereira Henriques, M.A.; Arreguy-Sena, C.; Pianetti Albergaria, V.M.; Dinis-Parreira, P.M. Cateterismo venoso periférico: Comprensión y evaluación de las prácticas de enfermería. Texto Context-Enferm. 2019, 28, e20180018. [Google Scholar] [CrossRef]
- Reichembach Danski, M.T.; Johann, D.A.; Vayego, S.A.; Rodrigues-Lemes de Oliveira, G.; Lind, J. Complications related to the use of peripheral venous catheters: A randomized clinical trial. Acta. Paul. Enferm. 2016, 29, 84–92. [Google Scholar]
- Ray-Barruel, G. Infection Prevention: Peripheral Intravenous Catheter Assessment and Care. Aust. Nurs. Midwifery J. 2017, 24, 34. [Google Scholar]


{kind=link}
| Patient | Patients with Peripheral Venous Catheter |
|---|---|
| Intervention | Evidence-based nursing interventions for the prevention and treatment of phlebitis |
| Comparison | Non-evidence-based routine interventions |
| Outcomes | Use of sterile and transparent dressing, catheter size, use of hot and cold compresses, topical treatment, management and maintenance of intravenous therapy |
| Database | Date (dd/mm/yyyy) | Search Strategy | Found Articles | Pre-Selected Articles |
|---|---|---|---|---|
| Scielo | 7/12/2020 | Phlebitis AND catheter | 19 | 10 |
| Scielo | 02/01/2021 | Phlebitis AND treatment | 5 | 1 |
| Scopus | 7/12/2020 | Phlebitis and nurs* | 20 | 6 |
| Scopus | 02/01/2021 | Phlebitis AND treatment | 6 | 1 |
| Pubmed | 2/12/2020 | Phlebitis and nurs* | 20 | 6 |
| Pubmed | 12/12/2020 | Phlebitis AND intervention AND nurs* | 2 | 1 |
| Pubmed | 21/12/2020 | Phlebitis AND nurs* intervention | 17 | 2 |
| Pubmed | 21/12/2020 | Phlebitis AND assessment measure | 1 | 1 |
| Pubmed | 13/01/2021 | Phlebitis AND prevention AND nurs* | 5 | 1 |
| Pubmed | 25/11/2020 | Competence AND nurs* AND phlebitis | 13 | 5 |
| Dialnet | 13/12/2020 | Phlebitis AND nursing | 13 | 3 |
| Medline | 13/12/2020 | Phlebitis and nursing interventions | 2 | 2 |
| Medline | 19/12/2020 | Phlebitis and nurs* | 64 | 8 |
| Medline | 19/12/2020 | Phlebitis AND treatment OR intervention OR therapy AND nurs* | 41 | 2 |
| WOS | 21/01/2021 | Phlebitis AND nurs* AND prevention | 15 | 5 |
| WOS | 21/01/2021 | Phlebitis AND treatment AND nurs* | 15 | 2 |
| LILACS | 21/12/2020 | Phlebitis AND nursing | 65 | 8 |
| LILACS | 21/12/2020 | Phlebitis and intervention | 3 | 1 |
| CINHAL | 02/01/2021 | Phlebitis AND treatment OR intervention OR therapy AND nurs* | 27 | 5 |
| CINAHL | 02/01/2021 | Phlebitis AND intervention | 23 | 1 |
| Total | 376 | 71 |
| a. RESULTS FROM CLINICAL STUDIES | |||||
|---|---|---|---|---|---|
| Year and Author | Objective | Type of Study | Results | Critical Reading | JBI Synthesis of the Evidence |
| Reichembach-Danski et al., 2016 [29] | Evaluate the incidence of complications related to peripheral intravenous catheter use in neonates and identify associated risk factors. | Prospective cohort study | Protocols with measures such as continuous observation of the insertion site, keeping the catheter insertion site visible, and saline solution infusion prior to the administration of other substances may be used to reduce complications. | 9/11 **** | DE*: 3c DR: A |
| Braga et al., 2018 [30] | Determine the incidence rate and risk factors for phlebitis and infiltration in patients with peripheral venous catheter. | Cohort study | To improve quality of care and prevent phlebitis and infiltrations, the nurse should analyze patient characteristics, prescribed intravenous medications (irritant and/or vesicant, pH, and osmolarity), expected duration of intravenous treatment, and risk factors for complications that can occur before selecting a venous catheter. Evaluate risks and benefits of each type of catheter and consider patient preferences. This test may indicate the use of other venous catheters, such as peripherally inserted central catheter. | 9/11 **** | DE*: 3c DR: A |
| Rosário-Pereira et al., 2019 [31] | Describe cases of phlebitis reported in a university hospital and contribute to possible improvement actions in quality of care and safety. | Retrospective, observational study | Knowing the characteristics of phlebitis favors understanding and minimization of this adverse event so as to establish preventive behaviors and decrease risk and incidence. | Intermediate evidence ***** | DE*: 3e DR: A |
| Lim et al., 2018 [32] | Project to improve visibility of intravenous area through the use of transparent adhesive dressings to achieve frequent and adequate intravenous inspection of the intravenous area and reduce incidence of complications. | Quasi-experimental study | Improved visibility of the intravenous puncture site and nurses’ compliance in frequent testing and monitoring; phlebitis can be detected early, reducing severity of complications. | 8/11 **** | DE*: 2d DR: B |
| Bugden et al., 2016 [33] | Assess whether the use of a skin adhesive glue to secure a peripheral intravenous line improves failure rates compared with standard securing measures | Randomized clinical trial | Adding a drop of cyanoacrylate adhesive helps stabilize the peripheral intravenous catheter. | 9/11 **** | DE*: 1c DR: A |
| Büyükyılmaz et al., 2019 [34] | Evaluate efficacy of I.V UltraDressing to protect peripheral intravenous catheters in pediatric patients. | Randomized clinical trial | I.V House UltraDressing device is useful to increase catheter dwell time and protect and stabilize PVCs in pediatric patients. | 9/11 **** | DE*: 1c DR: A |
| Annisa et al., 2017 [35] | Assess the effectiveness of applying hot compress to reduce the degree of phlebitis. | Quasi-experimental study | A hot water compress is useful in the treatment of phlebitis and could decrease degree of phlebitis in an effective and cost-saving way. | 8/11 **** | DE*: 2d DR: A |
| Bigdeli-Shamloo et al., 2019 [36] | Assess the effects of topical sesame oil on reduced severity of "chemotherapy-induced phlebitis" pain. | Randomized clinical trial | Complementary methods for the treatment of phlebitis symptoms are proposed. Application of sesame oil is effective in reducing severity of chemotherapy-induced phlebitis pain. | 9/11 **** | DE*: 1c DR: A |
| Sharifi-Ardani et al., 2017 [37] | Assess the effect of topical chamomile on phlebitis caused by the administration of amiodarone infusion in PVC. | Randomized clinical trial | Topical chamomile may be effective in decreasing incidence of phlebitis for its anti-inflammatory capacity. | 9/11 **** | DE*: 1c DR: A |
| García-Quintanilla et al., 2018 [38] | Describe the use and assess the efficacy and safety of Burow solution for topical treatment of phlebitis. | Prospective observational study | During the inclusion period for Burow solution in 35 patients with phlebitis, 12 have been excluded for lack of follow-up. 83% (n = 19) have responded to the therapy by reducing the degree of phlebitis by two points after three days of treatment, and 17% (n = 4) were unresponsive, requiring topical applications of Feparil®. | 7/11 **** | DE*: 3e DR: A |
| Jourabloo et al., 2017 [39] | Compare the effect of wet compresses and marigold ointment on the severity of phlebitis caused by dextrose infusion. | Randomized clinical trial | Applying marigold ointment decreased the severity of phlebitis in a shorter period, compared to using a wet, hot compress. This ointment is recommended to reduce phlebitis severity. | 9/11 **** | DE*: 1c DR: A |
| Parreira et al., 2020 [40] | Establish clinical efficacy and safety parameters for double-pump syringes for intravenous medication administration and PVC washing. | Randomized clinical trial | Developing a double-pump syringe makes it easier for nurses to adopt good clinical practices in procedures and administer intravenous medicine to reduce catheter handling. | 8/11 **** | DE: 1c * DR: A |
| Pérez-Granda et al., 2020 [41] | Compare rates of phlebitis and catheter tip colonization between PVC blocked with saline solution and blocked with heparin in patients admitted to internal medicine. | Randomized clinical trial | No statistically significant differences were found in frequency of phlebitis and PVC tip colonisation regarding blockage with saline solution or with heparin. PVC can be maintained with saline solution, and it is safer and cheaper than heparin. | 8/11 **** | DE: 1c * DR: A |
| b. RESULTS FROM REVIEWS | |||||
| Year and Author | Research Question | Methodology | Results | Critical Reading | JBI Synthesis of the Evidence |
| Higgingson, 2015 [42] | Assess complications associated with improperly secured intravenous cannulae, along with examination of fastening devices. | Literature review | Intravenous catheters not secured properly produce higher rates of mechanical phlebitis and infection. Clinical staff need to be educated on PVC stabilization as an important measure to reduce phlebitis. Safety devices are available for their use whenever appropriate. | 8/11 **** | DE*: 4a DR: A |
| Chau and Pellowe, 2008 [43] | Provide summarized evidence on intravascular device management to reduce risk of infection. | Best practice information sheet | Continuous training and evaluation are needed on handling, aseptic technique and hand washing, choosing a catheter based on estimated function, duration, and complications. | Recommended *** | DR: A * |
| Chau and Pellowe, 2008 [43] | Provide summarized evidence on intravascular device management to reduce risk of infection. | Best practice information sheet | Flush stopcocks with saline solution. | Recommended *** | DR: B * |
| Martín-Gil et al., 2017 [6] | Effectiveness of topical treatments in hospitalized patients with phlebitis secondary to peripheral venous catheterisation to improve or resolve signs and symptoms. | Systematic review of clinical trials and reviews | Aloe vera, notoginseny, diclofenac, and heparin gel 1000 IU showed a level of evidence and a moderate degree of recommendation. Heparin gel is the only compound indicated by the Spanish Agency of Medicines and Medical Products to treat post-infusion phlebitis; notoginseny is not marketed in the Western world; and diclofenac is an anti-inflammatory used in various pathologies. | 10/11 **** | DE*: 1b DR: A |
| c. RESULTS FROM QUALITATIVE STUDIES | |||||
| Year and Author | Research Question | Methodology | Results | Critical Reading | JBI Synthesis of the Evidence |
| Salgueiro-Oliveira et al., 2019 [2] | What are the PVC-related nursing practices for identifying deviations from available evidence on phlebitis prevention? | Qualitative study, participants monitoring and interviews | Nursing practices that differ from scientific evidence; influence from institutional dimensions; characteristics of the sick and misinformation about patient safety risk actions. Developing protocols and implementing continuing education are critical to acquiring skills, correcting and providing safe and quality assistance. | 9/11 **** | DE*: 4b DR: A |
| d. RESULTS FROM DESCRIPTIVE STUDIES | |||||
| Year and Author | Research Question | Methodology | Results | Critical Reading | JBI Synthesis of the Evidence |
| Da Silva-Oliveira et al, 2016 [44] | What are the characteristics of phlebitis reported in a hospital of the Sentinel Hospital Surveillance Network? | Descriptive quantitative study | For the prevention of phlebitis, an educational intervention through team training has the potential to reduce 50% of cases in peripheral intravenous therapy. Phlebitis rates/incidence are used as an indicator of nursing quality of care. As best prevention practices, it is suggested to use smaller calibre cannulae, transparent dressings, and professional knowledge of signs and symptoms that warn of possible phlebitis. On the venous access site, a statistical association was found between the back of the hand with more grade I phlebitis, followed by antecubital pit with higher number of grade II and grade III phlebitis. It is advisable to prioritize peripheral catheterisation in upper limb blood vessels, as they are safer. Avoid joint areas with greater mobility, more prone to traumatic mechanical phlebitis formation, and control osmolarity and pH of medication to reduce chemical phlebitis. | HIGH evidence ***** | DE*: 4a DR: A |
| e. RESULTS FROM CLINICAL PRACTICE GUIDELINES | |||||
| Year and Author | Research Question | Methodology | Results | HICPAC Category | AGREE |
| Torres-Muñoz et al., 2018 [4] | Guide to recommendations on nursing care of vascular accesses. | Clinical Practice Guideline | PVC insertion technique: Handwash with antiseptic soap and water if visibly dirty (40–60 s) or alcoholic-based friction (20–30 s) if visibly clean. Avoid joint areas; wrist and antecubital pit, since they have a higher incidence of mechanical phlebitis. To insert a PVC, 10–15 cm compressor above the puncture site, locate vein by palping, and place the limb in decline to favor venous filling. alcoholic chlorhexidine solution at > 0.5% or aqueous chlorhexidine at 2%. In cases of hypersensitivity, use iodine solutions or alcohol at 70%. PVC is covered with transparent sterile dressing. PVC Maintenance: Reduce connections manipulations; handle stopcocks or bio-connectors with hygienic hand washing and clean gloves. | Category IA ** | Recommended *** |
| Torres-Muñoz et al., 2018 [4] | Vascular Access Nursing Care Recommendations Guide | Clinical Practice Guideline |
| Category IB ** | Recommended *** |
| Torres-Muñoz et al., 2018 [4] | Vascular Access Nursing Care Recommendations Guide | Clinical Practice Guideline |
| Category IC ** | Recommended *** |
| Torres-Muñoz et al., 2018 [4] | Vascular Access Nursing Care Recommendations Guide | Clinical Practice Guideline |
| Category II ** | Recommended *** |
| Martínez-Ortega et al., 2019 [7] | Prevention of complications related to peripheral venous catheter for vascular access. | Clinical Practice Guideline | Before inserting a PVC, hand hygiene with alcoholic-based solution or antiseptic soap. Wear clean gloves. Prepare skin with 2% alcoholic chlorhexidine and allow to dry. Cover with sterile, transparent, and semi-permeable dressing to inspect insertion site. Change management systems and connections every 4–7 days, and to reduce risk of infection, clean access port with antiseptic (alcoholic chlorhexidine >0.5% or alcohol at 70%) Remove any PVC that is not essential. | Category IA ** | Recommended *** |
| Martínez-Ortega et al., 2019 [7] | Prevention of complications related to peripheral venous catheter for vascular access. | Clinical Practice Guideline | Select PVC based on objective, expected time of use, and known complications. Select catheter of the smallest caliber and shortest length possible. Avoid areas of the joints (hand, wrist, and antecubital pit), with increased risk of infiltration and injury from extravasation. Dressings will be changed every 7 days, except in pediatric patients, where risk of dislodging PVC is greater than the advantages of changing dressings. Remove PVC if signs of phlebitis, infection, or malfunctioning appear. It is recommended to use The Visual Scale of Phlebitis Assessment (Maddox scale). | Category IB ** | Recommended *** |
| Martínez-Ortega et al., 2019 [7] | Prevention of complications related to peripheral venous catheter for vascular access. | Clinical Practice Guideline | It is recommended to use split septum valves against mechanical ones, which have an increased risk of infection. | Category II ** | Recommended *** |
| Infusion Nurses Society, 2016 [9] | Assessment of the vascular access site, determining type of intervention, education about phlebitis for the patient, and response to treatment | Clinical Practice Guideline | It is recommended to assess our patient’s characteristics regularly, recognize risk factors for bacterial, mechanical, or chemical phlebitis, and consider pharmacological actions, also applying a warm compress and elevating the limb. | Category IB ** | Recommended *** |
| Result | Interventions | Synthesis of the Evidence | NIC [20] |
|---|---|---|---|
| Management and maintenance of intravenous therapy | Protocol monitoring and continuous evaluation | DE*:3c DR*: A | (6520) Health Screening |
| Records need to include date of puncture, securement used, professional performing the procedure. When changing the PVC, record date, site, number of puncture attempts, intravenous medication in use. | DE*: 4a DR: A | (4200) Intravenous therapy (i.v.) | |
| Using sterile saline solution to secure the PVC, to avoid heparin-induced thrombocytopenia. | DE*: 1c DR: A | (2314) Intravascular medication administration (i.v.) | |
| For intermittent flushing and locking, perform the positive pressure technique to avoid a possible suction effect or backflow when extracting the syringe. | DE*: 2c DR: A | (2314) Intravascular medication administration (i.v.) | |
| Flushing stopcocks and hubs with normal saline solution. If PVC is used to obtain a blood sample, the use of diluted heparin is indicated. | DR*: B | (4235) Phlebotomy: Cannulated Vessel | |
| Using double-pump syringes to enable both medication and cleaning solution administration to reduce PVC manipulation and complications. | DE: 1c DR: A | (2314) Intravascular medication administration (i.v.) | |
| To prevent and treat phlebitis, use Aloe vera, Matricaria chamomilla, or Xianchen. | DE*: 1b DR: A DE*: 1c DR: A | (3584) Skin care: topical treatments | |
| Removing any PVC that is not essential. | Category IA ** | (4200) Intravenous therapy (i.v.) | |
| Not performing a systematic catheter change every 72 to 96 h. It must be changed when clinically justified. | Category IB ** | (4200) Intravenous therapy (i.v.) | |
| Avoiding insertion into joint areas, wrist, and antecubital fossa. | Category IA ** | (4190) Intravenous insertion (i.v.) | |
| Replacing administration systems, extension cords, and accessories between 4 and 7 days. | Category IA ** | (4200) Intravenous therapy (i.v.) | |
| Guiding patients and family members on signs and symptoms of phlebitis after removing the catheter and at hospital discharge. | DE*: 3c DR*: A DE*: 1ª DR: A | (6610) Risk identification (5510) Health education | |
| Catheter asepsis | Using alcoholic chlorhexidine solution at > 0.5% or aqueous chlorhexidine at 2% to wash skin. | Category IA ** | (4200) Intravenous therapy (i.v.) |
| Applying antiseptic on clean skin, making circles from inside to outside, and let dry. | Category IB ** | (4200) Intravenous therapy (i.v.) | |
| Handling stopcocks, hubs, ports, and bio-connectors with hygienic hand washing and clean gloves. | Category IA ** | (4200) Intravenous therapy (i.v.) | |
| In cases such as those in emergency areas, replace the catheter as soon as possible if aseptic technique cannot be ensured. | DE: 1c DR: A | (4190) Intravenous insertion (i.v.) (4200) Intravenous therapy (i.v.) | |
| Nursing assessment | Involving the patient in the choice of PVC. | DE*: 3b DR: A | (4190) Intravenous insertion (i.v.) (5510) Health education |
| Analysing patient characteristics, prescribed intravenous medications, expected duration of the treatment, and other risk factors for the onset of phlebitis, before opting for a PVC | DE*: 5a DR: A | (6610) Risk identification (2314) Intravascular medication administration (i.v.) | |
| Assessing osmolarity of treatment and state of venous sources when inserting the PVC. | Category IB ** | (4190) Intravenous insertion (i.v.) | |
| Previously identifying comorbidities such as diabetes mellitus. Educating to provide with knowledge on signs of phlebitis and facilitate early detection and minimize complications. | DE*: 4a DR: A | (6610) Risk identification (5510) Health education | |
| Catheter | Choosing a catheter based on estimated function, duration, and known complications. | DR*: A | (4190) Intravenous insertion (i.v.) |
| Choosing a catheter of the least length and caliber possible, without exceeding vein caliber. | Category IB ** | (4190) Intravenous insertion (i.v.) | |
| Using the minimum number of three-way stopcocks. Idle ports should always be capped. | Category IA ** | (4200) Intravenous therapy (i.v.) | |
| Using only one of the ports of the three-way stopcock to place a bio-connector, where intermittent medication solutions and bolus will be administered. Protect with cap infused with alcoholic solution for one use or, if not possible, disinfect the area with alcoholic solution for 30 s. | Category IA ** | (4235) Phlebotomy: Cannulated Vessel | |
| Dressing | Using transparent adhesive sterile dressing to achieve frequent and adequate intravenous inspection of the intravenous site. | Category IA ** | (4190) Intravenous insertion (i.v.) |
| Dressings will be changed every 7 days, except in pediatric patients, where risk of dislodging PVC is greater than the advantages of changing dressings. | Category IB ** | (4190) Intravenous insertion (i.v.) | |
| Using skin glue (cyanoacrylate) at the insertion site to improve catheter securement and reduce rates of phlebitis and occlusion. | DE*: 1c DR: A | (4190) Intravenous insertion (i.v.) | |
| Using the "I.V. House UltraDressing" in pediatric patients to increase catheter dwell time, and to protect and stabilize PIVCs. | DE*: 1a DR: A | (4190) Intravenous insertion (i.v.) | |
| Nurse as a care prescriber | Applying alternating hot and cold compresses to decrease erythema, edema, and pain. | DE*: 3c DR: A | (1380) Heat/Cold Application |
| Applying compresses with 0.9% NaCl to stimulate anti-inflammatory response and relieve pain, redness, swelling, and oedema. | DE*: 2c DR: A | (1380) Heat/Cold Application | |
| Applying 10 drops (3 mL) of sesame oil (SO) twice daily for two weeks. Massage for 5 min. | DE*: 1c DR: A | (3584) Skin care: topical treatments | |
| Applying Moist Exposed Burn Ointment (MEBO) for topical treatment of burn injuries. | DE*: 1a DR: A | (3584) Skin care: topical treatments | |
| Administering chamomile extract (2.5%), as it has anti-inflammatory and anti-edema properties. | DE*: 1b DR: A | (3584) Skin care: topical treatments | |
| Applying marigold ointment every 8 h for anti-inflammatory effect. | DE*: 1c DR: A | (3584) Skin care: topical treatments | |
| Applying a compress with Burow solution at a temperature between 2 and 8 degrees Celsius, and leave on for 20 min every 8 h. | DE*: 3c DR: A | (3584) Skin care: topical treatments | |
| Nurse following protocols and guidelines | Applying of anti-inflammatory or corticosteroid agents, and application of a hot and/or wet compress. | DE*: 1a DR: A | (3584) Skin care: topical treatments |
| Using corticosteroids and piroxicam to prevent phlebitis. | DE*: 1c DR: A DE*: 1ª DR: A | (2316) Medication Administration: Skin | |
| Applying topical treatments with aloe vera or "Chamomilla Recutita" using wet compresses at 38 degrees Celsius on the affected area. Apply topical diclofenac and “Essaven” heparin gel for the treatment of phlebitis. Topical products such as notoginseny and 5 mg nitroglycerin patch accelerate the improvement of phlebitis symptoms, as compared to heparinoid substances. | DE*: 1a DR: A | (2316) Medication Administration: Skin (3584) Skin care: topical treatments |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guanche-Sicilia, A.; Sánchez-Gómez, M.B.; Castro-Peraza, M.E.; Rodríguez-Gómez, J.Á.; Gómez-Salgado, J.; Duarte-Clíments, G. Prevention and Treatment of Phlebitis Secondary to the Insertion of a Peripheral Venous Catheter: A Scoping Review from a Nursing Perspective. Healthcare 2021, 9, 611. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare9050611
Guanche-Sicilia A, Sánchez-Gómez MB, Castro-Peraza ME, Rodríguez-Gómez JÁ, Gómez-Salgado J, Duarte-Clíments G. Prevention and Treatment of Phlebitis Secondary to the Insertion of a Peripheral Venous Catheter: A Scoping Review from a Nursing Perspective. Healthcare. 2021; 9(5):611. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare9050611
Chicago/Turabian StyleGuanche-Sicilia, Aitana, María Begoña Sánchez-Gómez, María Elisa Castro-Peraza, José Ángel Rodríguez-Gómez, Juan Gómez-Salgado, and Gonzalo Duarte-Clíments. 2021. "Prevention and Treatment of Phlebitis Secondary to the Insertion of a Peripheral Venous Catheter: A Scoping Review from a Nursing Perspective" Healthcare 9, no. 5: 611. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare9050611