
Analysis of General Practitioners’ Attitudes and Beliefs about Psychological Intervention and the Medicine-Psychology Relationship in Primary Care: Toward a New Comprehensive Approach to Primary Health Care


Abstract
:1. The Biopsychosocial Model in Primary Health Care
2. Multidisciplinary Teamwork and Primary Health Care
3. Materials and Methods
4. Results
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
- Do you share your clinic with other GPs?
- ○
- No
- ○
- Yes (How many?) _______
- 2.
- How much has your training in medicine promoted the possibility of a collaboration between medicine and psychology?
- ○
- Not at all
- ○
- A little
- ○
- Moderately
- ○
- A lot
- 3.
- In your opinion, what are the specifics of the intervention of these different professionals:Psychologist
- ○
- Intervention targets
- ○
- Intervention goals
- ○
- Reasons for referral
- Psychotherapist
- ○
- Intervention targets
- ○
- Intervention goals
- ○
- Reasons for referral
- Counselor
- ○
- Intervention targets
- ○
- Intervention goals
- ○
- Reasons for referral
- Psychiatrist
- ○
- Intervention targets
- ○
- Intervention goals
- ○
- Reasons for referral
- 4.
- Have you ever referred patients to a psychologist?
- ○
- No
- ○
- Yes
- 5.
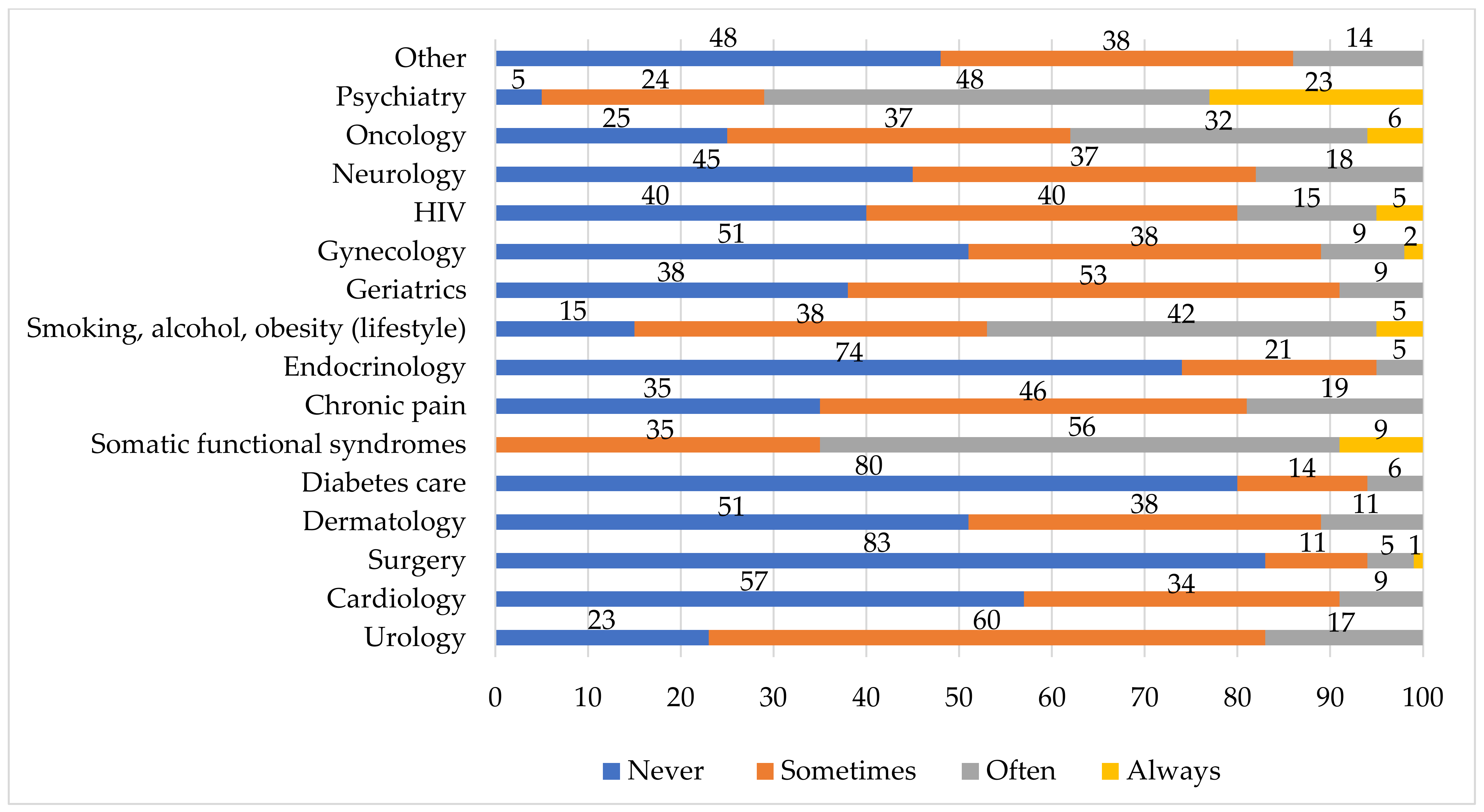
- How often have you referred patients to a psychologist for the following medical areas?
| Never | Sometimes | Often | Always | |
| Urology | ||||
| Cardiology | ||||
| Surgery | ||||
| Dermatology | ||||
| Diabetes care | ||||
| Somatic functional syndromes | ||||
| Chronic pain | ||||
| Endocrinology | ||||
| Smoking, alcohol, obesity (lifestyle) | ||||
| Geriatrics | ||||
| Gynecology | ||||
| HIV | ||||
| Neurology | ||||
| Oncology | ||||
| Psychiatry | ||||
| Other |
- 6.
- Regarding the patients referred, have you received any feedback from the psychologist?
- ○
- No
- ○
- Yes, by phone
- ○
- Yes, in person
- ○
- Yes, other (please specify)
- 7.
- Do you have a network of psychologists you consider “trustworthy”?
- ○
- No, I do not know who to send patients to
- ○
- Yes, within public facilities
- ○
- Yes, within private organizations
- ○
- Yes, professional psychologists (individual or associated)
- 8.
- How often do you prescribe psychotropic drugs?
- ○
- Never
- ○
- Sometimes
- ○
- Often
- ○
- Always
- 9.
- How often do you meet patients who may benefit from psychological intervention?
- ○
- Never
- ○
- Sometimes
- ○
- Often
- ○
- Always
- 10.
- How often do you refer patients who you consider may benefit from psychological intervention to a psychologist?
- ○
- Never
- ○
- Sometimes
- ○
- Often
- ○
- Always
- 11.
- For what reasons did you not propose psychological intervention to someone who would need it?
- ○
- The distress was contained within the doctor-patient relationship
- ○
- I opted for a pharmacological therapy
- ○
- My proposal could have had a negative impact on the patient (“I’m not crazy!”)
- ○
- Patient could have experienced their problem as diminished
- ○
- Patient could have diminished their trust in me because I had not been able to manage the problem directly
- ○
- Patient might have felt abandoned by me
- ○
- I did not know who to refer them to
- ○
- Patient could not economically afford a psychological consultation
- ○
- Other (please specify)
- 12.
- How often do you receive requests for psychological intervention from your patients?
- ○
- Never
- ○
- Sometimes
- ○
- Often
- ○
- Always
- 13.
- How often do your patients complain about physical disorders whose origin is psychological?
- ○
- Never
- ○
- Sometimes
- ○
- Often
- ○
- Always
- 14.
- Which aspects of the relationship with patients are more difficult to manage for you?
- ○
- Aggressiveness
- ○
- Complaints
- ○
- Mistrust
- ○
- Unwarranted criticism
- ○
- Other (please specify)
- 15.
- If you have the opportunity, would you offer psychological interventions to your patients in your clinic?
- ○
- No
- ○
- Yes, individual psychological sessions conducted by a psychologist
- ○
- Yes, visits jointly conducted by doctor and psychologist
- ○
- Yes, group sessions jointly conducted by doctor and psychologist for patients with similar pathologies
- ○
- Yes, other (please specify)
- 16.
- A collaboration with a psychologist:
- ○
- Would help me to manage patients who show little compliance
- ○
- Would help me to manage patients with hypochondriac/psychosomatic symptoms
- ○
- Would shorten the waiting list
- ○
- Would foster a faster recovery of some patients
- 17.
- How much could the psychologist’s work overlap or hinder the doctor’s work?
- ○
- Not at all
- ○
- A little
- ○
- Moderately
- ○
- A lot
- 18.
- Is there a psychologist in your clinic?
- ○
- No
- ○
- Yes
- 19.
- If a psychologist is present in your clinic, how long has the partnership lasted?
- ○
- 0–5 months
- ○
- 6–12 months
- ○
- >12 months
- 20.
- If a psychologist is present in your clinic, how often are they present in a week?
- ○
- Depends on the number of appointments arranged
- ○
- Twice a week
- ○
- >3 times a week
- 21.
- How did the collaboration start?
- ○
- On the initiative of the psychologist
- ○
- On my own initiative to reduce the costs of the clinic
- ○
- On my own initiative to offer an additional service to patients
- ○
- There was an explicit request from patients
- ○
- Other (please specify)
- 22.
- What kind of cooperation is there between you and the psychologist in your clinic?
- ○
- None, s/he is a consultant to whom patients go spontaneously without my referral
- ○
- Referral for psychosomatic/functional disorders
- ○
- Referral for anxiety and depression disorders
- ○
- Referral for adapting to living with a chronic illness
- ○
- Other (please specify)
- 23.
- Response date to this survey:
- 24.
- Gender:
- ○
- Male
- ○
- Female
- 25.
- Year of birth:
- 26.
- Year of graduation:
- 27.
- Year of specialization (specify which one):
- 28.
- Other specialties or masters (specify which one):
- 29.
- In the past, have you worked as a doctor in other public or private organizations?
- ○
- No
- ○
- Yes, in a hospital
- ○
- Yes, in a residence for elderly
- ○
- Yes, in a family counseling center
- ○
- Yes, in a hospice
- ○
- Yes, other (please specify)
- 30.
- Indicate the year in which you started your practice as a general practitioner:
- 31.
- Number of patients assisted:
- 32.
- Health district to which you belong:
References
- Engel, G.L. The clinical application of the biopsychosocial model. Am. J. Psychiatry 1980, 137, 535–544. [Google Scholar] [PubMed]
- Frazier, L.D. The past, present, and future of the biopsychosocial model: A review of The Biopsychosocial Model of Health and Disease: New philosophical and scientific developments by Derek Bolton and Grant Gillett. New Ideas Psychol. 2020, 57, 100755. [Google Scholar] [CrossRef]
- World Health Organization. Ottawa Charter for Health Promotion; WHO: Geneva, Switzerland, 1986. [Google Scholar]
- World Health Organization. The European Mental Health Action Plan 2013–2020; WHO: Geneva, Switzerland, 2015. [Google Scholar]
- Wade, D.T.; Halligan, P.W. The biopsychosocial model of illness: A model whose time has come. Clin. Rehabil. 2017, 31, 995–1004. [Google Scholar] [CrossRef]
- Ward, P. Trust and communication in a doctor-patient relationship: A literature review. Arch Med. 2018, 3, 36. [Google Scholar]
- Hvidt, E.A.; Lykkegaard, J.; Pedersen, L.B.; Pedersen, K.M.; Munck, A.; Andersen, M.K. How is defensive medicine understood and experienced in a primary care setting? A qualitative focus group study among Danish general practitioners. BMJ Open 2017, 7, e019851. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Livio, G.; Padula, A. Defensive medicine in Europe: A ‘full circle’? Eur. J. Health Econ. 2020, 21, 165–170. [Google Scholar]
- Hartman, T.C.O.; Woutersen-Koch, H.; Van der Horst, H.E. Medically unexplained symptoms: Evidence, guidances, and beyond. Br. J. Gen. Pract. 2013, 63, 625–626. [Google Scholar] [CrossRef] [Green Version]
- IAPT Improving Access to Psychological Therapies—IAPT. Available online: https://www.england.nhs.uk/mental-health/adults/iapt/ (accessed on 15 December 2020).
- Wortman, M.S.; Lokkerbol, J.; Van der Wouden, J.C.; Visser, B.; Van der Horst, H.E.; Olde Hartman, T.C. Cost-effectiveness of interventions for medically unexplained symptoms: A systematic review. PLoS ONE 2018, 13, e0205278. [Google Scholar] [CrossRef]
- Fraser, M.W.; Lombardi, B.M.; Wu, S.; de Saxe Zerden, L.; Richman, E.L.; Fraher, E.P. Integrated primary care and social work: A systematic review. J. Soc. Soc. Work Res. 2018, 9, 175–215. [Google Scholar] [CrossRef]
- Craig, S.; Frankford, R.; Allan, K.; Williams, C.; Schwartz, C.; Yaworski, A.; Janz, G.; Malek-Saniee, S. Self-reported patients psychosocial needs in integrated primary health care: A role for social work in interdisciplinary teams. Soc. Work Health Care 2016, 55, 41–60. [Google Scholar] [CrossRef]
- Solano, L. Dal Sintomo Alla Persona; Franco Angeli: Milan, Italy, 2011. [Google Scholar]
- World Health Organization (WHO)/Wonca Joint Report Integrating Mental Health into Primary Care: A Global Perspective. Available online: https://www.who.int/mental_health/policy/services/mentalhealthintoprimarycare/en/ (accessed on 15 December 2020).
- Kusnanto, H.; Agustian, D.; Hilmanto, D. Biopsychosocial model of illnesses in primary care: A hermeneutic literature review. J. Fam. Med. Prim. Care 2018, 7, 497–500. [Google Scholar] [CrossRef]
- Soler, J.K.; Okkes, I. Reasons for encounter and symptom diagnoses: A superior description of patients’ problems in contrast to medically unexplained symptoms (MUS). Fam. Pract. 2012, 29, 272–282. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Houwen, J.; Lucassen, P.L.; Stappers, H.W.; Assendelft, P.J.; Van Dulmen, S. Medically unexplained symptoms: The person, the symptoms and the dialogue. Fam. Pract. 2017, 34, 245–251. [Google Scholar] [CrossRef]
- Liuzzi, M. Per un progetto nazionale di psicologia di cure primarie. Psicol. Della Salut. 2020, 2, 158–175. [Google Scholar]
- Aamland, A.; Malterud, K.; Werner, E.L. Patients with persistent medically unexplained physical symptoms: A descriptive study from Norwegian general practice. BMC Fam. Pract. 2017, 15, 107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mulvale, G.; Embrett, M.; Razavi, S.D. ‘Gearing Up’ to improve interprofessional collaboration in primary care: A systematic review and conceptual framework. BMC Fam. Pract. 2016, 17, 83. [Google Scholar] [CrossRef] [Green Version]
- Das, P.; Naylor, C.; Majeed, A. Bringing together physical and mental health within primary care: A new frontier for integrated care. J. R. Soc. Med. 2016, 109, 364–366. [Google Scholar] [CrossRef] [Green Version]
- Derksen, J. Primary care psychologist in the Netherlands: 30 years of experience. Prof. Psychol. Res. Pract. 2009, 40, 493–501. [Google Scholar] [CrossRef]
- Pereira, M.G.; Fachado, A.A.; Smith, T.E. Practice of Biopsychosocial Medicine in Portugal: Perspectives of Professionals Involved. Span J. Psychol. 2009, 12, 217–225. [Google Scholar] [CrossRef] [Green Version]
- Turpin, G.; Richards, D.; Hope, R.; Duffy, R. Improving access to psychological therapies in: A national initiative to ensure the delivery of high quality evidence-based therapies. Pap. Del Psicólogo 2008, 29, 271–280. [Google Scholar]
- Kates, N. Promoting Collaborative Care in Canada: The Canadian Collaborative Mental Health Initiative. Fam. Syst. Health 2008, 26, 466–473. [Google Scholar] [CrossRef]
- Zealand, T.N. The Wellbeing Budget. Wellington, New Zealand: Treasury New Zealand. Available online: https://treasury.govt.nz/publications/wellbeing-budget/wellbeing-budget-2019 (accessed on 15 December 2020).
- Aru, F.L.; Chiri, L.R.; Menchetti, M.; Gallingani, F.; Filugelli, L.; Antonica, M.R.; Ciotti, E.; Fioritti, A.; Berardi, D. Modelli di integrazione tra psicologia e assistenza sanitaria primaria: Verso la concreta costruzione di una assistenza psicologica di base? G. Ital. Di Psicol. 2019, 46, 179–200. [Google Scholar]
- Legge Regionale n. 23 Del 11 Agosto 2015—Evoluzione Del Sistema Sociosanitario Lombardo: Modifiche al Titolo I e l Titolo II Della Legge Regionale del 30 Dicembre 2009 n. 33 (Testo Unico Delle Leggi Regionali in Materia di Sanità). Available online: http://normelombardia.consiglio.regione.lombardia.it/ (accessed on 15 December 2020).
- Bojadzievski, T.; Gabbay, R.A. Patient-centered medical home and diabetes care. Diabete Care 2011, 34, 1047–1053. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Piano Nazionale Della Cronicità. Available online: http://www.salute.gov.it/imgs/C_17_pubblicazioni_2584_allegato.pdf (accessed on 15 December 2020).
- Allegrante, J.P.; Wells, M.T.; Peterson, J.C. Interventions to Support Behavioral Self-Management of Chronic Diseases. Annu. Rev. Public Health 2019, 40, 127–146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Solano, L.; Magnani, M.; Di Trani, R.; Ferri, R.; Di Monte, C.; Renzi, A. L’esperienza di collaborazione tra psicologi della salute e medici di medicina generale (MMG) della Scuola di Psicologia della Salute di Roma. Psicol. Della Salut. 2020, 1, 79–91. [Google Scholar]
- Compresenza Della Figura Dello “Psicologo di Base” (PdB) Nell’ambito Dell’organizzazione Territoriale Regionale a Supporto Dei Medici di Assistenza Primaria (MAP). Avvio Della Sperimentazione. Available online: https://bur.regione.veneto.it/BurvServices/pubblica/DettaglioDgr.aspx?id=275496 (accessed on 15 December 2020).
- Kaitz, J.E.; Ray, S. Psychologist and Physician Inter-Professional Collaborative Experiences in Primary Care Integration. J. Clin. Psychol. Med. Settings 2020. [Google Scholar] [CrossRef]
- Damasio, A.R. Descartes’ Error: Emotion, Reason, and the Human Brain; Putnam: New York, NY, USA, 1994. [Google Scholar]
- Glaser, B.; Strauss, A. The Discovery of Grounded Theory: Strategies for Qualitative Research; Aldine: Chicago, IL, USA, 1967. [Google Scholar]
- Balint, M. The Doctor, His Patient and the Illness; Churchill Livingstone: London, UK, 2000. [Google Scholar]
- Benincasa, F. Nota Editoriale. In Medico, Paziente e Malattia; Fioriti: Rome, Italy, 2014. [Google Scholar]
- Kainz, K. Barriers and enhancements to physician-psychologist collaboration. Prof. Psychol. Res. Pract. 2002, 33, 169–175. [Google Scholar] [CrossRef]
- Bluestein, D.; Cubic, B.A. Psychologists and Primary Care Physicians: A Training Model for Creating Collaborative Relationships. J. Clin. Psychol. Med Settings 2009, 16, 101–112. [Google Scholar] [CrossRef]
- Solano, L. Tra Mente e Corpo. Come si Costruisce la Salute; Franco Angeli: Milan, Italy, 2001. [Google Scholar]
- Berkel, L.A.; Nilsson, J.E.; Joiner, A.V.; Stratmann, S.; Caldwell, K.K.; Chong, W.W. Experiences of Early Career Counseling Psychologists Working in Integrated Health Care. Couns. Psychol. 2019, 47, 1037–1060. [Google Scholar] [CrossRef]
- McDaniel, S.H.; Belar, C.D.; Schroeder, C.; Hargrove, D.S.; Freeman, E.L. A training curriculum for professional psychologists in primary care. Prof. Psychol. Res. Pract. 2002, 33, 65–72. [Google Scholar] [CrossRef]
- World Health Organization. Declaration of Alma Ata; WHO: Geneva, Switzerland, 1978. [Google Scholar]
- Primary Health Care: Now More Than Ever. Campagna Italiana per un Nuovo Modello di Cure Primarie. Available online: https://2018phc.wordpress.com (accessed on 15 December 2020).
- Ordine Degli Psicologi Della Lombardia, Codice Deontologico. Available online: http://www.opl.it/public/files/945-codice-deontologico-finale-neutro.pdf (accessed on 15 December 2020).
- Negri, A.; Andreoli, G.; Belotti, L.; Barazzetti, A.; Martin, E.H. Psychotherapy trainees’ epistemological assumptions influencing research-practice integration. RIPPO 2019, 22, 344–358. [Google Scholar] [CrossRef] [PubMed]
- Grenier, J.; Chomienne, M.H.; Gaboury, I.; Ritchie, P.; Hogg, W. Collaboration between family physicians and psychologists: What do family physicians know about psychologists’ work? Can Fam. Physician 2008, 54, 232–233. [Google Scholar] [PubMed]
- Sydow, K.V.; Reimer, C. Attitudes toward psychotherapists, psychologists, psychiatrists, and psychoanalysts. Am. J. Psychother. 1998, 52, 463–488. [Google Scholar] [CrossRef] [Green Version]
- Cordella, B.; Greco, F.; Di Trani, M.; Renzi, A.; La Corte, C.; Solano, L. The impact of joint consultation with family physicians on perception of psychologists. Prof. Psychol. Res. Pr. 2016, 47, 102–109. [Google Scholar] [CrossRef]
- Zivin, K.; Pfeiffer, P.N.; Szymanski, B.R.; Valenstein, M.; Post, E.P.; Miller, E.M.; McCarthy, J.F. Initiation of primary care-mental health integration programs in the VA health system: Associations with psychiatric diagnoses in primary care. Med. Care 2010, 48, 843–851. [Google Scholar] [CrossRef]
- Cornwell, B.L.; Brockmann, L.M.; Lasky, E.C.; Mach, J.; McCarthy, J.F. Primary Care-Mental Health Integration in the Veterans Affairs Health System: Program Characteristics and Performance. Psychiatr. Serv. 2018, 69, 696–702. [Google Scholar] [CrossRef] [PubMed]
- Negri, A.; Andreoli, G.; Barazzetti, A.; Zamin, C.; Christian, C. Linguistic markers of the emotion elaboration surrounding the confinement period in the Italian epicenter of COVID-19 outbreak. Front Psychol. 2020, 11, 568281. [Google Scholar] [CrossRef]


{kind=link}
| Thematic Areas | Examples of Questions | Answer Options |
|---|---|---|
| Degree | Year Type and year Type and year No, hospital, family counseling center, hospice, retirement home, other | |
| Education and career information | First specialization | |
| Other specialization | ||
| Previous medical activity in other services | ||
| Patients’ medical conditions and need for psychological interventions | How often do you meet patients who could benefit from psychological intervention? | Never, sometimes, often, always |
| Beliefs and attitudes towards mental health professionals | In your opinion, what are the goals of the intervention of these different professionals: psychologist, psychotherapist, counselor and psychiatrist? | Open-ended |
| Attitudes towards the psychologist | If you had the opportunity, would you offer your patients a psychological intervention in your clinic? | No, yes |
| In case you answered “yes” to the previous question, which psychological intervention would you offer? | Visit jointly conducted by doctor and psychologist, individual psychological/psychotherapy sessions, group posttherapy, other | |
| How much could the psychologist/psychotherapist’s work overlap and hinder the doctor’s work? | Not at all, a little, moderately, a lot | |
| Features of collaborations with psychologists | How often did you refer patients to a psychologist/psychotherapist with symptoms concerning the following medical areas? (urology, cardiology, dermatology, etc.) | Never, sometimes, often, always |
| As for patients you referred to a psychologist/psychotherapist, did you have feedback by the psychologist/psychotherapist? How? | No, yes; by phone, in person, other |
| Professionals | Intervention Targets | Intervention Goals | Reasons for Referral |
|---|---|---|---|
| Psychiatrist | Severe psychic symptoms (major depression, psychosis) | Diagnosis and psychopharmacological treatment | To heal and manage severe psychological symptoms |
| Psychologist | Psychic and functional symptoms | Diagnosis, treatment, and psychological support | To heal and manage mild psychological symptoms |
| Psychotherapist | Psychic and functional symptoms | Diagnosis, treatment, and psychological support | To heal and manage mild psychological symptoms |
| Counselor | Existential and relational difficulties | Personal skills empowerment, promotion of an active role toward their own problems | To help in managing specific life issues |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Negri, A.; Zamin, C.; Parisi, G.; Paladino, A.; Andreoli, G. Analysis of General Practitioners’ Attitudes and Beliefs about Psychological Intervention and the Medicine-Psychology Relationship in Primary Care: Toward a New Comprehensive Approach to Primary Health Care. Healthcare 2021, 9, 613. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare9050613
Negri A, Zamin C, Parisi G, Paladino A, Andreoli G. Analysis of General Practitioners’ Attitudes and Beliefs about Psychological Intervention and the Medicine-Psychology Relationship in Primary Care: Toward a New Comprehensive Approach to Primary Health Care. Healthcare. 2021; 9(5):613. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare9050613
Chicago/Turabian StyleNegri, Attà, Claudia Zamin, Giulia Parisi, Anna Paladino, and Giovanbattista Andreoli. 2021. "Analysis of General Practitioners’ Attitudes and Beliefs about Psychological Intervention and the Medicine-Psychology Relationship in Primary Care: Toward a New Comprehensive Approach to Primary Health Care" Healthcare 9, no. 5: 613. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare9050613